Embed Size (px)
Citation preview

Osmotic Diuretic Treatment of Refractory EdemaBy LIONEL M. BERNSTEIN, M.D., PH.D., BERNARD BLUMBERG, M.D., AND
MURRAY C. ARKIN, M.D.
Many patients with edema of congestive cardiac failure, nephrosis, and cirrhosis becomerefractory to all diuretic therapy. Theoretically, the use ia adequate dosage of osmoticdiuretics whose action is dependent upon physical factors should augment sodium, chlo-ride, and water excretion from whatever level exists prior to their use. In refractoryedema, the effect of other diuretics (via alteration of the imetabolie, actively resorbingmechanisms of the tubular cells) on tubular rejection of sodium, chloride, and watershould be increased by osmotic diuretics. Mannitol was administered intravenously inlarge doses to test the effectiveness of osmotic diuretics in refractory edema.
OSMOTIC diuretics exert their actionthrough physical rather than cellular
metabolic effects.'-3 Osmotic diuretic actiondepends upon the presence of nonabsorbableparticles within the isosmotic proximal tubule.These nonabsorbable particles cause retentionof water within the proximal tubule to main-tain a constant total osmolar concentration of310 mOsM. per Lj. As compared with the pre-osmotic diuretic baseline, the water that is soretained progressively dilutes the sodium inthe fluid as it traverses the proximal tu-bule. Thus, an unchanged cell surface areacontaining the active metabolic sites for so-dium resorption is exposed to a fluid of pro-gressively lesser sodium concentration.' Theabsorbing sites being less saturated, less so-dium particles are absorbed (despite unal-tered avidity of the individual cell sites),and more sodium particles passed on distally.Within the proximal tubule the additionalnonabsorbed sodium and accompanying an-ions behave as osmotic diuretic particles4 andretain water that also is passed on distally.In the distal convoluted tubule, absolutequantities absorbed, even when maximal, are
small fractions of the increased total quan-tities presented and explain the inability ofthe distal tubule greatly to modify the natureof the fluid presented to it.1-3 Urine duringsuch marked osmotic diuresis is similar to thefluid leaving the proximal tubule in total con-
centration, pH, and individual ion concentra-
From the Medical Service and the Medical Re-
search Division, V.A.H., Hines, Ill.
tions. During such osmotic diuresis, the ad-ministration of a hypertonic solution (suchas 1500 mOsM. per L.) coupled with excre-tion of urine with a 300 to 350 mOsM. perL. concentration indicates a net loss of solute.
Osmotic diuretics have been tried in refrac-tory edema, both successes5'6 and failures7having been reported. However, the spar-sity of data and the infrequency of their usesuggest that they have not been generallyeffective. From theoretical considerations,the limiting factor for their effectiveness isthe presence of an adequate filtration rate toallow enough osmotic diuretic particles toreach the tubular lumen. Mercurial and os-motic diuretics potentiate each other 's ef-feets.5'8
Mannitol, regarded as an almost inert, non-toxic hexose, excreted by glomerular filtra-tion alone, is an osmotic diuretic available forparenteral injection. The experience withmannitol administered intravenously withand without a mercurial diuretic in the treat-ment of refractory edema is the basis of thisreport.
METHODS
Subjects were chosen who had marked edemaof nephrosis, cardiac failure, or cirrhosis thatwas refractory to dietary salt restriction (less than500 mg. of sodium per day) plus the usual diu-retics, singly and in combination. In all patients,use of mercurial diuretics, aminophylline, am-monium chloride, and Diamox was unsuccessful.In the 2 cardiac patients, digitalis was used forboth; ACTH priming and alcohol were used forone (case 2). Because of prolonged refractory
Circulation, Volume XVII, June 19581013
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

BERNSTEIN, BLUMBERG, AND ARKIN
t 1311
, 1291
c 127
101% 99
7196
I, 5
-No
-Cl
K
-Monnitol-Urine flow
-Na
K
20 v-16 z
12 \
8
4;..t
k.oTime 9AM 10 1i N 1PM 2 3 4 5
t 2mi Thiomerin 1. V.
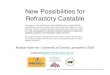
FIG. 1. Case 1, Exp. D., nephrotic edema. Serumelectrolyte concentrations and urinary excretion ratesof sodium, potassium, chloride, mannitol, and waterduring mannitol-Thiomerin treatments.
edema, diuresis with mannitol' administered intra-venously, was attempted. The dietary sodium con-tent was constant for several weeks before, during,and after mannitol administration in all cases.Water intake was ad libitum. Patients were treatedwith infusions of 25 per cent mannitol intrave-nously in amounts up to 2,000 ml. (500 Gm.) overperiods of 4 to 8 hours. Usually a priming dosewas followed by a slower infusion. Interruptionsof the infusions occurred occasionally. As far aspossible, after initial exploratory experiments on1 patient, a standard approach was roughly fol-lowed. Daily outputs of water, sodium, potassium,and chloride were determined immediately before,during, and immediately after administration ofmannitol. When mannitol and a mercurial diu-retic were given together, the outputs were com-pared with those without treatment, and withmercurial diuretic treatment alone.A mercurial diuretic (Thiomerin) was given
intravenously as single 2-ml. doses, or as 2 1-ml.doses 3 to 5 hours apart. In several cases, urinaryspecific gravity and the rate of urine flow (for 10-to 60-minute periods) were measured throughoutthe course of mannitol administration. In 1 case,the excretions of mannitol, water, and electrolyteswere measured during the course of a day ofmannitol plus mercurial treatment.
Urinary creatinine exeretions were measured bythe method of Bonsnes and Taussky.9Sodium and potassium were analyzed with the
Perkin-Elmer flame photometers chloride by themethod of Sendroy, as modified by Van Slyke and
*The mannitol used in this study was provided byMerck, Sharp and Dohme, Rahway, N. J.
Hiller," and mannitol by the method of Corcoranand Page.'2 Freezing point determinations wereperformed with the Fiske osmometer, by means ofa sodium chloride standard curve.'3
RESULTS
Treatment of Nephrotic Edema. The ini-tial, exploratory studies were made on a pa-tient with refractory nephrotic edema of sev-eral months duration (case 1, table 1).Intravenous administration of 100 to 200 Gm.of mannitol with and without 2 ml. of Thio-merin suggested (1) that mannitol alonecaused greater water as compared with so-dium loss than did Thiomerin alone (Exp.A and C, table 1); (2) that mannitol com-bined with Thiomerin caused much greaterwater and sodium losses than did eitheralone (Exp. A) ; and (3) that combined man-nitol and Thiomerin administration signifi-cantly increased water and sodium excretionabove control nontreatment levels (Exp. Band C).
Following a 2-week period without treat-ment, a critical test was performed. Excre-tions were studied for each of 5 consecutivedays on which there were, respectively, notreatment, 2 ml. of Thiomerin, 2 ml. of Thio-merin plus 250 Gm. of mannitol, 2 ml. of Thi-omerin, and no treatment (Exp. D, table 1).The sodium excretion on the mannitol plusThiomerin day was increased 480 mEq. abovethe average of the days immediately pre-ceding and following with Thiomerin alone.Generally, chloride excretion followed sodiumexcretion as the major accompanying anion.Potassium excretion was not altered by man-nitol or Thiomerin administration or both.Total daily urinary output was increasedabout 800 ml. per day by Thiomerin as com-
pared with no treatment; it was increased an
additional 5,600 ml. by the administration of250 Gm. of mannitol (in 1000 ml. of water)with Thiomerin. Figure 1 shows the rates ofexcretion per minute during the mannitolplus Thiomerin treatment day. The parallel-ism of sodium, chloride, and mannitol excre-
tions (in milliosmoles per minute) and urineflow rates is clear. The failure of potassiumexcretion to increase during the osmotic di-
.ol' 1
1014
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

OSMOTIC DIURETIC TREATMENT OF EDEMA 1015
TABLE 1.-Response of Refractory Edema Cases to Intravenously Administered Mannitol andMercurial Diuretics
Treatment
Thiomerin Mannitol(ml.) (Gm.)
22
2
22
222
222
222
2222
2
22
2
100100
200
200100
250
400
440
350
475
Volume(ml./day)
3 2605,1201,990
1,4804,7252,480
1,9154,4853,8101,250
2,2353,4408,6852,5552,060
1,3601,9806,6201,4601,820940
7,0201,4401,400
1,1201,500
8,0601,140600
1,780
9901,8008,0751,2701,100
Urine
Total amounts/day
Na(mEq.)
75.0297.084.6
35.5224.054.8
49.477.1133.024.8
87.8259.0660.397.139.8
6.675.2
264.0.0.0.3
82.5.0.4
15.613.4
356.84.0.4
22.8
1.252.4469.1
.89.9
K (mEq.) Cl (mEq.)_ _1 _
89.689.160.1
74.9106.898.0
78.5110.3102.555.6
104.298.4106.088.496.0
93.2159.0210.820.730.46.0
139.519.257.1
53.168.0152.051.454.6133.9
27.163.486.036.486.6
__ __ __ _ __ __ __- _ __ __ _
Case 1~~~~~~~~~~~~~~~~~~~~~~~~~~~~Case 1Exp. A
Exp. B
Exp. C
Exp. D
Case 2
Case 3
Case 4
Day
1234
78910
1112131415
272829303132
12345678910
1234567
123456
105.6366.3100.6
31.9181.532.5
21.154.9
137.113.7
94.0275.0639.192.528.6
58.0149.0254.4
2.1.0
1.2193.825.4
.5
62.751.4465.020.61.6
30.9
6.892.2459.5
Creatinine(Gm.)
1.831.541.47
1.041.321.49
1.391.441.521.13
1.201.031.561.021.15
1.582.342.111.462.551.692.111.443.25
.35
.90
.851.02.84
1.14
.79
.90
.49
.53
.12
Bodyweight(lbs.)
188186183Y2182Y2
176177176176
176175Y2174173174
17817812176167Y2167169
198M2198197188Y2189191191186Y2187187
175175172Y2163166Y2167Y2168
153152150132Y2134134
Weightchangeper day(lbs.)
-2-2'2-1
+1-10
-1'2-1-1+1
+
21-12y
+2
-½-1
-812
+2+20
-4V2+V
0
-2½2-9½2+3V2+1+12
-1-2- 1712+1'20
.,
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

BERNSTEIN, BLUMBERG, AND ARKIN
uresis is also evident. During this diuresis,there were no clinically significant changes inserum electrolyte levels.
Table 1 reveals daily body weight losses upto only 21/2 pounds despite urinary volumesup to 5 L. per day in experiments A toC, indicating possible incomplete controlof this ambulatory patient's water (and salt)intake. In experiment D, the massive outputof water and sodium on Thiomerin plus man-nitol treatment was accompanied by an 81/2-pound loss. During the course of this treat-ment day, the gross edema of penis, scrotum,and lower extremities could be seen to disap-pear gradually, there remaining only a traceof edema at the end of the treatment day.Thirst was excessive throughout treatment.The combined mannitol and Thiomerin treat-inent effected great loss of water, sodium, andchloride, without adverse effects.
Treatment of Cardiac Edema. Two cases ofrefractory cardiac edema were treated withmannitol plus Thiomerin. The first (case 2)was a patient with primary pulmonary hyper-tension in a state of extreme, hopeless decom-pensation refractory to treatment for severalmonths. The first control day studied re-vealed an output of only 6.6 mEq. of sodium,and 1,360 ml. of water (table 1). Thiomerinalone increased the sodium output to 75 mEq.and the urine volume to 1,980 ml., whereasThiomerin plus 400 G-m. of mannitol in-creased the sodium excretion to 264 mEq.,and the urine volume to 6,620 ml. Thislarge urinary output was accompanied by an
8/-pound weight loss, despite which the pa-tient's clinical condition improved negligibly.Following this, the urinary excretion of so-dium fell to zero, whether or not Thiomerinwas given. A second trial on Thiomerin plus440 Gm. of mannitol increased the sodiumoutput from zero to 82.5 mEq. with a urinaryvolume of 7,020 ml. per day, and caused a
41/2-pound weight loss, again with very minorclinical improvement.
In this patient, potassium excretion was
clearly and significantly elevated by the Thi-omerin-mannitol treatment. Chloride excret-ing generally increased when potassium andsodium excretions increased.
The weight losses were rough measures ofedema loss. The cardiac failure of this pa-tient was not secondarily aggravated by theaccumulated peripheral edema. Mobilizationand excretion of this edema, while relievingthe patient of some discomfort, did not basi-cally alter his state of cardiac decompensation.There was definite, increased pulmonary con-gestion and dyspnea during the mannitol in-fusions related to an increase in extracellularfluid and blood volumes. The rate of manni-tol infusion was decreased as pulmonary con-gestion increased. Pulmonary congestion wasdecreased within an hour after discontintua-tion of mannitol infusion.Ten days later, a third infusion of manni-
tol was attempted. Thirty minutes after tlieinfusion was begun acute pulmonary edemaoccurred. The mannitol infusion wasstopped, usual measures were taken, and thepulmonary edema terminated. Eight hourslater another episode of pulmonary edemaoccurred, did not respond to the usual thera-py as had the numerous previous episodes ofacute pulmonary edema and the patient died.
The second cardiac patient (case 3) treatedwith mannitol had coronary artery diseasewith refractory congestive failure. At rest,he had neither dyspnea nor findings of pul-monary congestion. Marked pitting edema ofhis lower extremities was present, whichcould not be mobilized. Table 1 demon-strates very small sodium and water excre-tions, even with daily Thiomerin. Infusionof 350 Gm. of mannitol with the Thiomerinincreased the 24-hour sodium excretion by350 mEq., increased the urinary output to8,075 ml, and effected a 91/2-pound weightloss. As in case 2, potassium excretion was
increased during mannitol-Thiomerin diure-sis. Chloride excretion followed as the mainion accompanying sodium and potassium.During the mannitol infusion, pulmonary
congestion and dyspnea occurred. These sub-sided as the mannitol infusion was slowed or
stopped. At the end of the treatment day, allbut a trace of the edema of the lower extrem-
ities was gone. Since this was the main mani-festation of his cardiac decompensation, the
1016
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

OSMOTIC DIURETIC TREATMENT OF EDEMA
mannitol-Thiomerin treatment was a clinicalsuccess in this instance.Treatment of Cirrhotic Edema. One patient
(case 4), with typical Laennec 's cirrhosis,marked emaciation, and marked ascites (butwithout edema elsewhere) that was refractoryto diuretic therapy was treated with mannitolplus Thiomerin. Table 1 summarizes thedata. Control excretion of sodium was 1.2mEq. per day. Thiomerin alone increasedsodium excretion to 50 mEq. whereas infusionof 475 Gm. of mannitol with Thiomerin in-creased the sodium loss to 469 mEq. Thishuge increase in sodium excretion was ac-companied by a urinary volume of 8,075 ml.,and a weight loss of 171/2 pounds. The largeurinary losses were derived primarily frommobilized ascitic fluid, since no other edemawas present. Potassium excretion was unaf-fected by mannitol administration. Chlorideexcretion followed sodium excretion as theaccompanying anion. At the end of the in-fusion, the patient developed muscular rigi-dity of his extremities and flapping motionsof his hands. These disappeared within anhour after the infusion was terminated, anddid not recur. Dryness of the mouth andthirst were present throughout the mannitol-Thiomerin treatment day.Treatment Failures. In 2 patients, one
with cirrhotic edema (case 5), and one withnephrotic edema due to lupus erythematosus(case 6), single attempts with mannitol plusThiomerin did not significantly increase so-dium and water outputs, and failed to causeloss of edema fluid. The data are not pre-sented. In both cases, diminished renal func-tion (markedly decreased filtration rates withazotemia) and small doses of mannitol limitedthe numbers of osmotic diuretic particlesreaching the tubular lumens. Thus, these 2failures may reasonably be attributed to bothinadequate dosage and the limiting factor oflow filtration rates.Mechanism of Osmotic Diuresis. Mannitol,
in adequate dosage, and in combination withThiomerin, was a very effective diuretic incases of refractory edema. In cases 1 to 4,peak urine flows reached were, respectively,18, 24, 25, and 35 ml. per minute. Study of
Time 7AM 8 9 10 11 N 1PM 2 3 4 5
?I-mi Thiomerin I.V.t ,i-m Thiomerin VV.
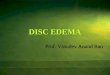
FIG. 2. Case 3, cardiac edema. Rates of urinaryflow as related to time of intravenously administeredThiomerin and mannitol.
individual urine specimens revealed that withincreasing excretory loads and urine volumesthe urine total osmolar concentration (asmeasured by freezing point depression) de-creased asymnptomatically toward 310 mOsM.per L.; and the urine specific gravity asymp-tomatically toward 1.010. These conform tothe characteristics of urine under osmotic di-uretic circumstances.' 3The much greater natriuretic and diuretic
effects of mannitol and Thiomerin combinedas compared with either alone are demon-strated by the data in table 1, and are clearlyshown by the time course of urinary flowrates in relation to the Thiomerin and manni-tol administration in figure 2 (case 3). Thefirst peak excretion rate (A) represents themaximal effect of the first Thiomerin injectionat a time of constant mannitol infusion. Thefirst nadir (B) represents the lessened effectof the first Thiomerin injection with the man-
nitol infusion unchanged. The second peak(C) represents the combined effects of thesecond Thiomerin injection and high manni-tol plasma levels. (The mannitol infusionhad been stopped, but significant removal byexcretion or utilization of the extracellularlydistributed mannitol had not yet occurred.That peripheral utilization of mannitol con-
tributes significantly to fall in plasma manni-tol levels is indicated by total recoveries ofonly 34 and 43 per cent, respectively, of the
1017
W
z
P 12.1_i
X 8a
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

1BERNSTEIN, BLUMBERG, AND ARKIN
TABLE 2.-Serum Electrolyte Concentrations beforeand after Mannitol Plus Mercurial Diuretics
Case 2
Case 3
Case 4
Day
2
378
-3-2t
36
-4t34
Treat-men'day
XX
X
X
Serum concentration (mEq./L.) t
Na
121
120121
145
144
132
139
K
5.8
4.43.6
5.74.8
4.5
3.7
3.1
Cl
868587
9593
92
100
99
* Treatment with mannitol plus Thiomerin.t Fasting a.m. levels.t Days before day 1 of table 1.
total doses administered in cases 1 and 4.)The second nadir (D) occurred during theeffect of the second Thiomerin injection afterthe plasma mannitol level had become loweredby excretion and utilization following cessa-
tion of the mannitol infusion. The thirdpeak (E) occurred following the restartingof mannitol infusion while the effect of thesecond Thiomerin injection was still present.Thus, nadir B represents the diuretic effectprimarily of mannitol, and nadir D repre-
sents the effect primarily of Thiomerin;whereas peaks A, C, and E each represent thecombined effects of mannitol and Thiomerin.
DISCUSSIONThese data demonstrate the effectiveness of
an osmotic diuretic combined with a mercu-
rial diuretic in treatment of refractory ede-ma. In 1 nephrotic patient, mannitol withThiomerin was effective and without adversereactions. In 2 cardiac patients, as was pre-
dicted, the mannitol infusion caused pulmo-nary edema during the osmotic diuresis. In1 cirrhotic patient, marked diuresis was fol-
lowed by early signs of central nervous sys-
tem symptoms of hepatic insufficiency. In 2
other patients, one with Laennec's cirrhosis,the other with the nephrotic syndrome of
lupus erythematosus, diuresis failed to occurbecause of both inadequate dosage andmarkedly reduced filtration rates. The effectof mannitol in nonrefractory edema14 was notstudied.The increased effectiveness of the combina-
tion of an osmotic and a mercurial diuretic5' 8probably can be explained by their knowndifferent actions. Mannitol, by its water-retaining and sodium-diluting action, de-creases the numbers of sodium-absorbing sitesof the tubular cells that are exposed to so-dium ;1 Thiomerin reduces the avidity of eachof these decreased numbers of sites for sodi-um resorption.5' 6, 15 The combined effects re-sult in great proximal tubular rejection ofsodium (and accompanying anions). Bothmannitol2' 3 and nonabsorbed sodium4 (dueto mercurial effects on tubular cells) havebeen shown to act as osmotic diuretics. Thenonabsorbed ionS4 and the mannitol retainwater isosmotically in the proximal tubluleand thus present excessive amounts of waterand electrolytes to the distal tubule whichare followed by excess excretion. It wouldbe expected that any osmotic diuretic couldbe effectively combined with any metabolicdiuretic that acted directly on the active cellmechanism for sodium transport. The fac-tors influencing excretion of sodium are sonumerous and variable that no absolute val-ues of sodium excretion may be expected forgiven doses of mercurials, osmotic diuretics,or combinations of diuretics. What is dem-onstrated is the ability of osmotic diureticsto increase the tubular rejection of sodiumfrom whatever level of rejection existed im-mediately prior to their use.4 6, 15-17
Despite the great losses of water, sodium,and chloride during the course of combinedmannitol-Thiomerin treatment (table 1) no
clinically significant changes of serum sodi-um, potassium, chloride, or bicarbonate con-
centrations occurred, as is demonstrated byvalues during treatment in case 1 (fig. 1) or
before and after treatment in cases 2 to 4(table 2).No substantial difference was found be-
tween the natriuretic or diuretic effects of
1018
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

OSMOTIC DIURETIC TREATMENT OF EDEMA
mannitol plus Thiomerin in the patients withrefractory edema of renal, cardiac, or hepat-ic origin. The diuretics were effective inshifting toward greater tubular rejection ofsodium and water. The similarity of diu-retic effects conforms with the concept thatin these different states excessive sodium re-sorption by tubular cells, due mainly to in-creased aldosterone effect, is the final com-mon pathway for the development of edema.18The clinical value of osmotic diuretics in
refractory edema must be evaluated by moreextended studies. The hazards of pulmonaryedema in cardiac patients may be minimizedby use of adequate doses of urea or otherosmotic diuretics that are distributed through-out body water rather than extracellular fluidalone. In cirrhotic patients, the effects ofrepeated treatment gradually to remove ex-tensive ascites and peripheral edema mustbe evaluated.The use of (physical) osmotic diuretics in
large adequate doses in combination with(metabolic) tubular cell sodium resorptionblocking diuretics should be considered whenedema states are refractory to all other di-uretic therapy.
SUMMARYMannitol, a typical osmotic diuretic, was
administered intravenously in large doses(up to 475 Gm. in 8 hours) to a small num-ber of patients with edema refractory to otherdiuretic therapy. Whatever the previouslevels of sodium, chloride, and water excre-tion, the administration of mannitol marked-ly increased those levels of excretion.The combination of mannitol and a mer-
curial diuretic was much more effective thaneither alone in increasing excretion of sodi-um (up to 660 mEq. per day) and water (upto 8,685 ml. per day), and causing weight(edema) losses whether the edema was ofrenal, cardiac, or hepatic origin. Negligibleto very large weight losses occurred, beingdetermined by both exeretions and simultane-ous intakes. Diuretic responses were notnecessarily accompanied by clinical benefits.The excretions were not accompanied by clini-
cally significant alterations in serum electro-lyte concentrations.The data conclusively demonstrate the abil-
ity of an osmotic diuretic markedly to in-crease the urinary excretion of water, sodium,and chloride in cases of refractory edema. Themechanism by which this is accomplished isdiscussed. The hazard of inducing pulmo-nary edema by administering osmotic diuret-ics to cardiac patients is recognized. Theclinical value of osmotic diuretics must be de-termined by additional studies.
ACKNOWLEDGMENT
The authors wish to thank Drs. Smith Freemanand Lyle A. Baker for their contributions to thiswork, and E. E. Bond, J. X. Wheeler, G. Phillips,and D. Perry for their important technical as-sistance.
SUMMARIO IN INTERLINGUAMannitol, un typic diuretico osmotic, esseva
administrate per via intravenose in grandedoses (de usque a 475 g in 8 horas) a unmicre numero de patientes con edema queesseva refractori a altere formas de therapiadiuretic. Sin reguardo al previe valores delexcretion de natrium chloruro, e aqua, le ad-ministration de mannitol augmentava ille val-ores marcatemente.Le combination de mannitol con un diure-
tico mercurial esseva multo plus efficace quele un o le altere sol in augmentar le excre-tion de natrium (usque a 660 mEq per die)e de aqua (usque a 8.685 ml per die) e incausar perdiates de peso (de edema), sin re-guardo a si le edema esseva de origine renal,cardiac, o hepatic. Le perditas de peso vari-ava inter negligibile e multo pronunciate eesseva determinate per le factores del excre-tion e del ingestion contemporanee. Le re-sponsas diuretic non esseva necessarimenteaccompaniate de beneficios clinic. Le excre-tiones non esseva accompaniate de clinica-mente significative alterationes in le concen-trationes del electrolytos seral.
Lie datos demonstra conclusivemente le fac-to que un diuretico osmotic es capace a in-ducer marcate augmentos del excretion uri-nari de aqua, natrium, e chloruro in casos deedema refractori. Le mechanismo que resul-
1019
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

BERNSTEIN, BLUMBERG, AND ARKIN
ta in iste effecto es discutite. Le risco de in-ducer edema pulmonar per le administrationde diureticos osmotic a patientes cardiac esrecognoscite. Le valor clinic de diureticososmotic debe esser determinate per studiosadditional.
REFERENCES1. SHANNON, J. A.: The renal reabsorption and
excretion of urea under conditions of ex-treme diuresis. Am. J. Physiol. 123: 182,1938.
2. RAPOPORT, S., BRODSKY, W. A., WEST, C. D.,AND MACKLER, B.: Urinary flow and ex-cretion of solutes during osmotic diuresisin hydropenic man. Am. J. Physiol. 156:433, 1949.
3. -, WEST, C. D., AND BRODSKY, W. A.: Ex-cretion of solutes and osmotic work duringosmotic diuresis of hydropenic man. Theideal and the proximal and distal tubularwork; the biological maximum of work.Am. J. Physiol. 157: 363, 1949.
4. BRODSKY, Wy. A., AND GRAUBARTH, H. N.:Mechanism of mercurial diuresis in hydro-penie dogs. Am. J. Physiol. 172: 67, 1953.
5. VOGL, A.: Diuretic Therapy. Baltimore, TheWilliams & Wilkins Co., 1953.
6. SMITH, H. W.: The Kidney. Structure andFunction in Health and Disease. New York,Oxford University Press, 1951.
7. LUETSCHER, J. A.: A study of the mechanismof nephrotic edema. J. Clin. Invest. 26:1189, 1947.
8. MUDGE, G. H., FOULKS, J., AND GILMAN, A.:
Effect of urea diuresis on renal excretionof electrolytes. Am. J. Physiol. 158: 218,1949.
9. BONSNES, R. W., AND TAUSSKY, H. H.: Colo-rimetric determination of creatinine by theJaffe reaction. J. Biol. Chem. 158: 581,1945.
10. Instruction Manual, Flame Photometer Model52-C, Perkin-Elmner Corp., Glenbrook,Conn.
11. HAWK, P. B., OSER, B. L., AND SUMMERSON,W. H.: Practical Physiological Chemistry.Ed., 12, Philadelphia, Blakiston Co., 1948.
12. CORCORAN, A. C., AND PAGE, I. H.: A imiethodfor the determination of mnannitol in plasmaand urine. J. Biol. Chein. 170: 165, 1947.
13. Instruction Manual, Osmoineter Model B,Fiske Associates, Inc., Boston, Mass.
14. LAST, J. H., MCDONALD, G. 0., JONEs, R. A.,AND BOND, E. E.: Rates of equilibrium ofinulin and mannitol between plasma andinterstitial water in edematous states. J.Lab. & Clin. Med. 39: 62, 1952.
15. SMITH, H. W.: Principles of Renal Physi-ology. New York, Oxford University Press,1956.
16. SIMMoNs, D. H., HARVEY, R. B., AND Ho-SHIKO, T.: Effect of sodium intake on sodi-unm loss due to mannitol diuresis. Am. J.Physiol. 178: 182, 1954.
17. CIZEK, L. J., AND HOLMES, J. H.: Chlorideexcretion during osmotic diuresis in thedog. Am. J. Physiol. 160: 536, 1950.
18. BARTTER, F. C.: The role of aldosterone innormal homneostasis and in certain diseasestates. Metabolism 5: 369, 1956.
9~It is with the living that medicine has to do. The living man must be studied in health
as in disease; to the physician or surgeon the sick or wounded man is as the mineralto the geologist, as the star to the astronomer.-William Stokes His Life and Work(1804-1878) by his son WILLIAM STOKES. London T. Fisher Unwin, MDCCCXCVIII,p. 162.
1020
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from

LIONEL M. BERNSTEIN, BERNARD BLUMBERG and MURRAY C. ARKINOsmotic Diuretic Treatment of Refractory Edema
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1958 American Heart Association, Inc. All rights reserved.
75231is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TXCirculation
doi: 10.1161/01.CIR.17.6.10131958;17:1013-1020Circulation.
http://circ.ahajournals.org/content/17/6/1013located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer
of the Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle columnClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on May 19, 2018
http://circ.ahajournals.org/D
ownloaded from