Embed Size (px)
Citation preview
OSHAWatchJanuary/February 2003 Volume 5, No. 1
Quality America: We Make Compliance Easy! 1-800-946-9956
How your practice can losethousands of dollars:ignore three simple rules
– See Avoid mistakes, Page 2
Inside...Types of OSHA violations............... 4
ContestingOSHA violations............... 6
Take the mysteryout of MSDS ................. 8
Smallpox Vaccine .......... 11
Plus...
Give us 5 minutes – we’ll give you a better
newsletter.
Got a few thousand dollars to spare? Want to keep those bucks for your practice, or give ‘em to the Feds? Hmmmm…that’s a tough one.
A four-physician internal medicine practice chose the latter and wrote a fat check to OSHA. Yet, they could have kept every dollar (or at least most of them) if their staff had followed three simple rules of conduct during an OSHA inspection.
In this true case study, a disgruntled employee of the practice complained to OSHA that her employer had not switched to safety needles. Her complaint resulted in an OSHA inspection. While the practice was found to be out of compliance in several areas, it was how the staff handled the inspection itself (or mis-handled it, as it were) that racked up the OSHA fines.
A case of too much customer service
It all began when an OSHA inspector walked in unannounced through the doors of Dunnville Medical Center*. He was greeted warmly by the office receptionist. After showing his credentials, he asked to be escorted back to the clinical area. The staff allowed
*Name changed to protect the identity of the practice
him to wander freely around the practice.
Three hours later, the inspector exited those same welcoming doors with a briefcase full of citations amounting to several thousand dollars. The physicians and staff were shocked and surprised two weeks later when they received a 15-page list of citations and penalties assessed against them. They wrote a check to OSHA that week.
Could this happen to you??
Three big mistakes and how to avoid making them
Dunnville Medical Center could have avoided or minimized these
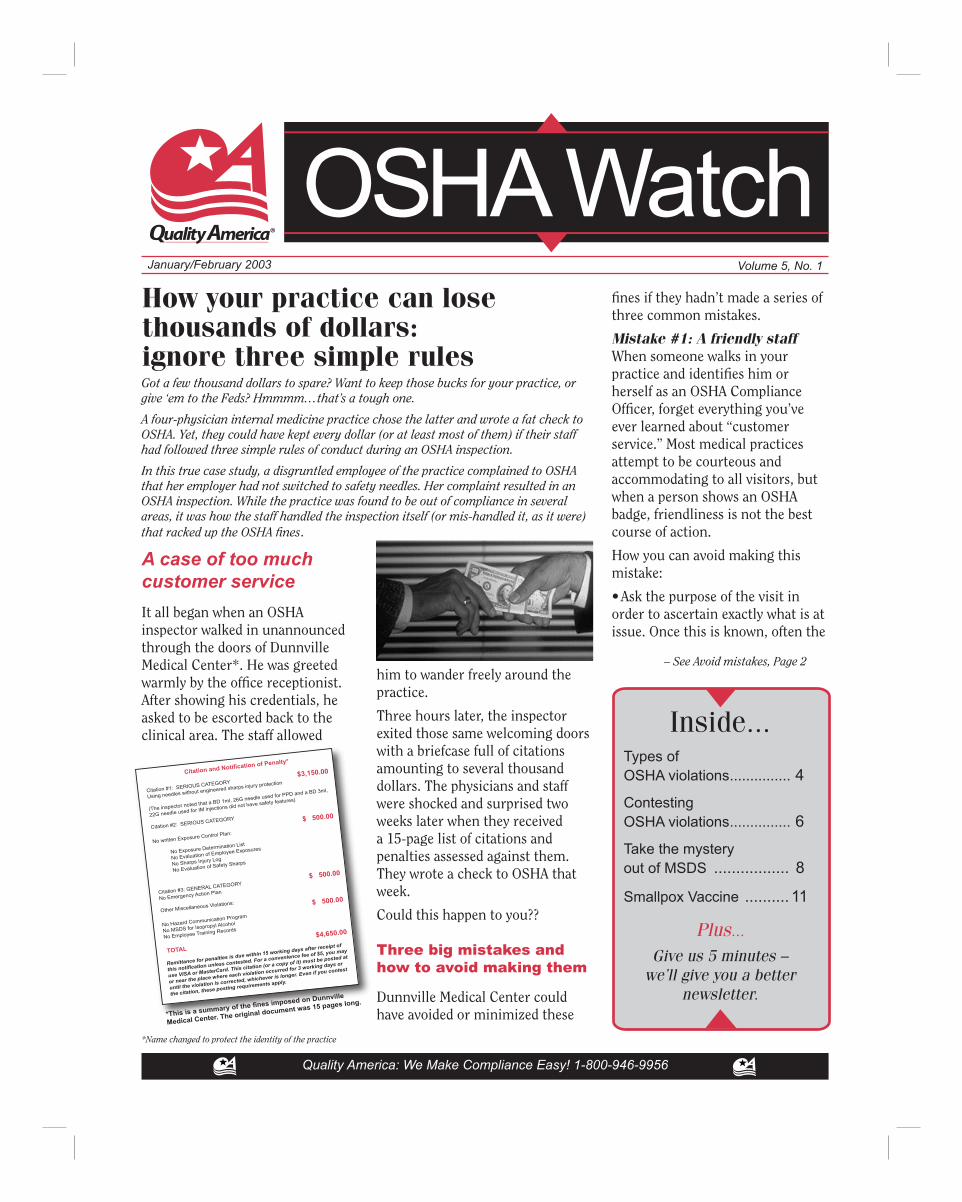
Citation and Notification of Penalty*
Citation #1: SERIOUS CATEGORY $3,150.00
Using needles without engineered sharps injury protection
(The inspector noted that a BD 1ml, 26G needle used for PPD and a BD 3ml,
22G needle used for IM injections did not have safety features)
Citation #2: SERIOUS CATEGORY
$ 500.00
No written Exposure Control Plan:
No Exposure Determination List
No Evaluation of Employee Exposures
No Sharps Injury Log
No Evaluation of Safety Sharps
Citation #3: GENERAL CATEGORY $ 500.00
No Emergency Action Plan
Other Miscellaneous Violations:
$ 500.00
No Hazard Communication Program
No MSDS for Isopropyl Alcohol
No Employee Training Records
TOTAL
$4,650.00
Remittance for penalties is due within 15 working days after receipt of
this notification unless contested. For a convenience fee of $5, you may
use VISA or MasterCard. This citation (or a copy of it) must be posted at
or near the place where each violation occurred for 3 working days or
until the violation is corrected, whichever is longer. Even if you contest
the citation, these posting requirements apply.
*This is a summary of the fines imposed on Dunnville
Medical Center. The original document was 15 pages long.
fines if they hadn’t made a series of three common mistakes.
Mistake #1: A friendly staffWhen someone walks in your practice and identifies him or herself as an OSHA Compliance Officer, forget everything you’ve ever learned about “customer service.” Most medical practices attempt to be courteous and accommodating to all visitors, but when a person shows an OSHA badge, friendliness is not the best course of action.
How you can avoid making this mistake:
• Ask the purpose of the visit in order to ascertain exactly what is at issue. Once this is known, often the

www.quality-america.com
OSHA Watch January/February 2003Page 2
www.quality-america.com
OSHA Watch January/February 2003 Page 3
inspector may be kept focused only on that exact circumstance.
• Ask the OSHA inspector to take a seat in the waiting area. Gather together your management team, including your practice’s OSHA Safety Officer.
Mistake #2: An unescorted inspector
In this case, the friendly reception staff not only neglected to ask the inspector the purpose of the visit, but they let him proceed into the clinical area without arranging an escort.
How you can avoid making this mistake:
• Always provide an escort to any inspector that enters the practice, to keep him focused on the exact purpose of the visit.
• Never allow an inspector to wander freely.
Mistake #3: No closing conference
After the inspection, the doctor’s office did not ask for a closing conference, nor did they contest the fines.
How you can avoid making this mistake:
• Always request a closing confer-ence before the OSHA Compliance Officer leaves the facility. During this conference, the inspector will explain any violations noted.
• Attempt to correct any violations on the spot, without admitting guilt.
Types of OSHA Violations
Violation Circumstances Penalties
Willful The employer knew that a hazardous condition existed but $5,000 -$70,000 per made no reasonable effort to eliminate it. willful violation
Serious A workplace hazard could cause injury or illness that would Up to $7,000 per most likely result in death or serious physical harm, unless the violation employer did not know or could not have known of the violation.
Other-Than- A situation in which the most serious injury or illness would Up to $7,000 per Serious be likely to result from a hazardous condition cannot reasonably violation be predicted to cause death or serious physical harm to exposed employees, but does have a direct and immediate relationship to their safety and health.
De Minimis Violations that have no direct or immediate relationship to safety N/A or health and do not result in citations.
Other A violation that has a direct relationship to job safety and health N/A but is not serious in nature.
Failure-to-Abate Issued when the employer has not corrected a violation for which Up to $7,000 per day OSHA previously issued a citation, and for which the abatement per violation date has passed.
Repeated Issued when an employer has been cited for a violation in the Up to $70,000 for each past and a substantially similar condition continues to exist. violation
• Contest the citation or penalty amount.
$56,000+ in fines to
medical practices
In the last five years, OSHA has inspected more than 1,000 physician offices. Almost half had violations but escaped penalties. The most common citations were for violations of the Bloodborne Pathogens Standard, followed
Federal OSHA Citations for Medical Offices & Clinics*OSHA Standard # Cited Penalty $Bloodborne Pathogens 142 $48,815.00
Hazard Communication 39 2,552.50
Formaldehyde 6 1,072.50
Log & Summary of Occupational Injuries & Illnesses 5 350.00 (no longer required in 2002)
Compressed Gases 2 250.00
Emergency Plans & Fire Prevention Plans 1 250.00
Eye & Face Protection 1 375.00
Sanitation 1 1,575.00
Portable Fire Extinguishers 1 700.00
Total 198 $55,940.00*(Oct. 2000-Sept.2001). Inspection data from 24 states with State OSHA plans are not available, so numbers
above presumably reflect less than half of all OSHA inspections in medical practices.
by the Hazard Communication Standard.
Federal OSHA agents inspect only about half of U.S. states; the remaining inspections are conducted by State agents, under a “state plan.” For just the doctors’ offices in states without state OSHA plans, nearly $56,000 in penalties were fined 2001, according to data on OSHA’s website (www.osha.gov). Since state plan statistics are not
Avoid mistakes during an OSHA inspection–from page 1
In the last five years, OSHA has inspected more than 1,000 physician offices.
www.quality-america.com
OSHA Watch January/February 2003Page 2
www.quality-america.com
OSHA Watch January/February 2003 Page 3
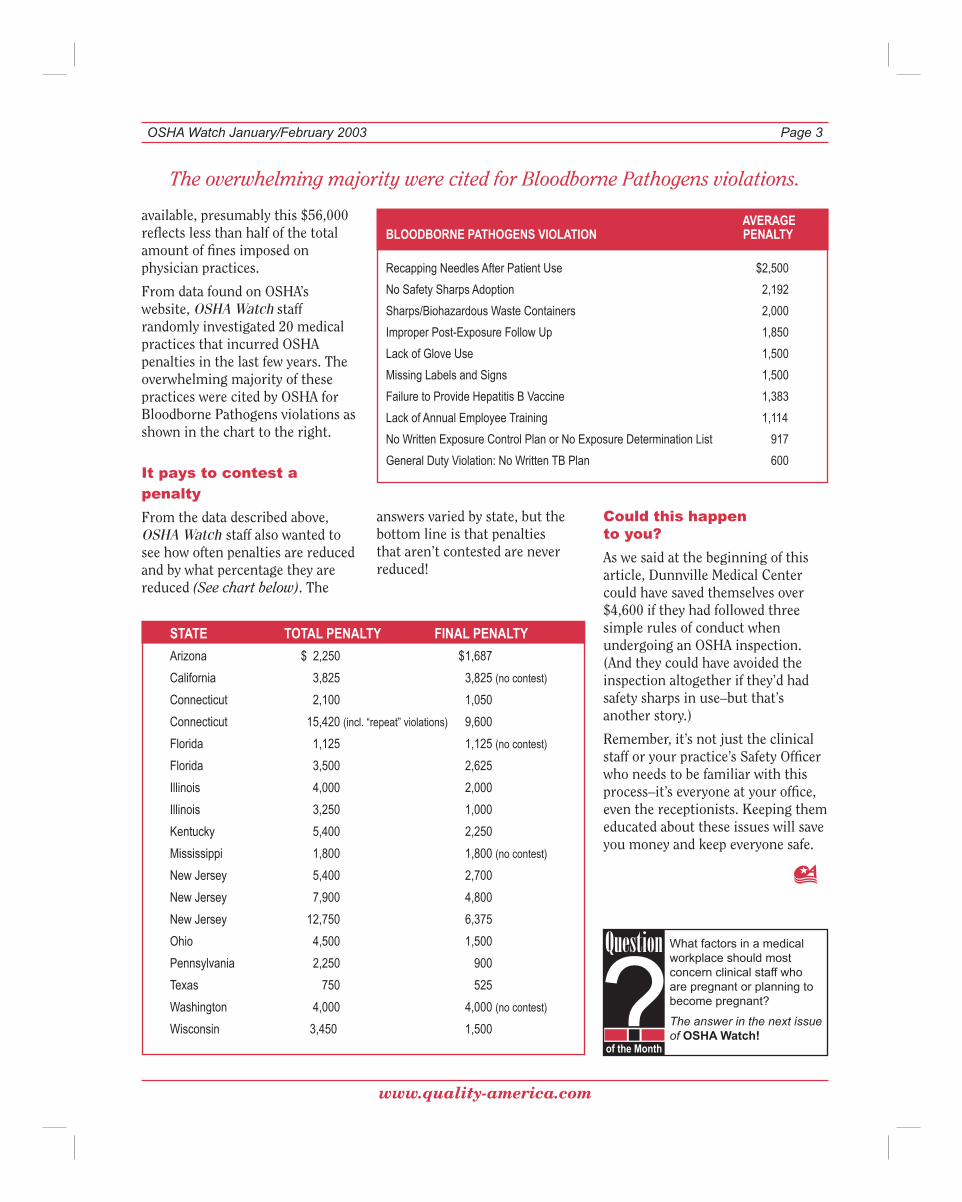
AVERAGEBLOODBORNE PATHOGENS VIOLATION PENALTY
Recapping Needles After Patient Use $2,500
No Safety Sharps Adoption 2,192
Sharps/Biohazardous Waste Containers 2,000
Improper Post-Exposure Follow Up 1,850
Lack of Glove Use 1,500
Missing Labels and Signs 1,500
Failure to Provide Hepatitis B Vaccine 1,383
Lack of Annual Employee Training 1,114
No Written Exposure Control Plan or No Exposure Determination List 917
General Duty Violation: No Written TB Plan 600
available, presumably this $56,000 reflects less than half of the total amount of fines imposed on physician practices.
From data found on OSHA’s website, OSHA Watch staff randomly investigated 20 medical practices that incurred OSHA penalties in the last few years. The overwhelming majority of these practices were cited by OSHA for Bloodborne Pathogens violations as shown in the chart to the right.
It pays to contest a
penalty
From the data described above, OSHA Watch staff also wanted to see how often penalties are reduced and by what percentage they are reduced (See chart below). The
The overwhelming majority were cited for Bloodborne Pathogens violations.
STATE TOTAL PENALTY FINAL PENALTY
Arizona $ 2,250 $ 1,687
California 3,825 3,825 (no contest)
Connecticut 2,100 1,050
Connecticut 15,420 (incl. “repeat” violations) 9,600
Florida 1,125 1,125 (no contest)
Florida 3,500 2,625
Illinois 4,000 2,000
Illinois 3,250 1,000
Kentucky 5,400 2,250
Mississippi 1,800 1,800 (no contest)
New Jersey 5,400 2,700
New Jersey 7,900 4,800
New Jersey 12,750 6,375
Ohio 4,500 1,500
Pennsylvania 2,250 900
Texas 750 525
Washington 4,000 4,000 (no contest)
Wisconsin 3,450 1,500
Question
of the Month
What factors in a medical workplace should most concern clinical staff who are pregnant or planning to become pregnant?
The answer in the next issue of OSHA Watch!
answers varied by state, but the bottom line is that penalties that aren’t contested are never reduced!
Could this happen to you?
As we said at the beginning of this article, Dunnville Medical Center could have saved themselves over $4,600 if they had followed three simple rules of conduct when undergoing an OSHA inspection. (And they could have avoided the inspection altogether if they’d had safety sharps in use–but that’s another story.)
Remember, it’s not just the clinical staff or your practice’s Safety Officer who needs to be familiar with this process–it’s everyone at your office, even the receptionists. Keeping them educated about these issues will save you money and keep everyone safe.
www.quality-america.com
OSHA Watch January/February 2003Page 4
www.quality-america.com
OSHA Watch January/February 2003 Page 5
New drugs for hepatitis C, B and anthrax
Hepatitis C – An estimated 4 million Americans have hepatitis C, the leading cause of liver transplants and the killer of over 10,000 people each year in this country. That annual toll is expected to triple by 2010.
But a new combination of drugs for hepatitis C promises a 56% cure rate and causes fewer side effects than current drugs. It includes weekly injections of Pegasys, a long-acting form of interferon called pegylated interferon, Peg-Intron and the antiviral, ribavirin.
Hepatitis B – A new drug for hepatitis B called adefovir dipivoxil is awaiting formal FDA approval. Originally developed for HIV and then rejected because it damages the kidneys, it has proven effective against hepatitis B in lower, safer doses.
Anthrax – EluSys Therapeutics, a New Jersey biotech firm, won a $2.8 million federal grant to help refine technology to destroy toxins released into the bloodstream by anthrax bacteria. The one-year grant is the first given by the government for an agent to rapidly clear anthrax from the blood. EluSys expects to speed up its research and
begin human safety testing of the drug within two years. It could take at least another year to win approval from the FDA to sell the drug.
Meanwhile, two more antibiotics, gatifloxacin and levofloxacin, may help prevent and treat anthrax infections during a biological attack. Both drugs belong to a newer class of antibiotics called fluoroquinolones, a class that includes ciprofloxacin. The FDA currently endorses three antibiotics for anthrax treatment: penicillin, doxycycline, and ciprofloxacin.
FDA to require glove manufacturers to report powder amounts
The Food and Drug Administration continues its push to regulate latex gloves as medical devices. The FDA’s proposal, which may change with the final rule, requires glove manufacturers to measure powder on latex gloves, says Joseph Sheehan, the head of regulatory staff at the FDA’s Center for Devices and Radiological Health.
Currently about 10%-12% of all healthcare workers have some type of allergy to latex, and this number is increasing. Unfortunately, even those workers who do not actually wear gloves can develop a latex allergy by breathing in the powder particles that carry the latex antigen.
Blood-filled syringes as street weapons
A rash of attacks and incidents involving contaminated needles and blood-filled syringes has authorities concerned about a new trend in street
weaponry and the safety of children who play in public places. The horror stories include:
Boise, ID: A man robs a TCBY store by holding a hypodermic needle in a clerk’s face, telling her that he has AIDS and has used the needle. He threatens to stick the clerk with the supposedly contaminated needle if she doesn’t comply with his demand for cash.
Interlochen, MI: An intoxicated man squirts a syringe of his blood on another man in his own home. Prosecutors believe the man is HIV positive and charges him with aggravated assault.
Town Hall, CT: A mother claims her daughter reached down on the ground near a trashcan in a local park and was stuck by a syringe. Her attorney claims that town officials failed to reasonably inspect the area for garbage and debris and to provide adequate lighting.
England: A 43-year-old man is stabbed in the ribs with a syringe during a fight. In another case, a cab driver is stabbed in the wrist with a hypodermic needle when he attempts to collect the fare from a passenger. The cabbie is tested for hepatitis and HIV and begins taking prophylactic drugs to reduce the risk of HIV infection.
Foam as bioterrorism buster
A newly developed foam is the latest technology in battling the culprits of chemical or biological warfare. Researchers at the Department of Energy’s Sandia National Laboratories in New Mexico have created a lather-like substance that neutralizes dangerous compounds, viruses and bacteria. Generically known as “decon foam,” it expands to 100 times its liquid volume when sprayed through a special nozzle that mixes it with air. It adheres to airborne chemical and germ agents before settling as a foam on the ground, and in a few hours it returns to a liquid state. It also can be dispensed through building sprinkler systems.
IN THE NEWS
A microscopic view of anthrax

www.quality-america.com
OSHA Watch January/February 2003Page 4
www.quality-america.com
OSHA Watch January/February 2003 Page 5
It isn’t harmful to people and doesn’t leave a poisonous or corrosive residue.
In laboratory tests, the foam destroyed mustard gas simulants as well as anthrax–among the most dangerous of all biological agents. Researchers say the foam is a cocktail of ordinary substances found in common household products and can be produced for about 15 cents a pound.
Source: Tampa Tribune (10/14/02) http://tampatrib.com/Business/MGA27JDH97D.html
OraQuick, a health worker pricks a person’s finger, drops a spot of blood into a vial of developing solution and drops in the stick-like testing device. The dipstick gives results similar to common pregnancy tests: One reddish line means no HIV, two reddish lines mean the person may be infected and needs a confirmatory test to be sure.
Studies show OraQuick is 99.6% accurate, but those who test positive still need to get a traditional Western blot test to confirm infection.
OraQuick is not CLIA-waived at this time, but the test is so simple that Health and Human Services Secretary Tommy Thompson urged manufacturer OraSure Technologies Inc. to submit the paperwork to attain a CLIA waiver. This would make the test applicable to all doctors’ offices, as well as mobile testing vans and HIV counseling centers.
The company, in partnership with Abbott Laboratories, has begun selling OraQuick for less than the $20 it costs to perform traditional laboratory HIV tests.
OraQuick’s speed and simplicity could also be applied to post-exposure testing of healthcare workers who have sustained a needlestick. Source patients could be tested on the spot for HIV infection, so that healthcare workers can learn right away if they need prophylactic HIV treatment.
OraQuick also may help when the government begins offering the smallpox vaccine to healthcare workers and others as protection against a possible bioterrorist attack. While such vaccine plans aren’t final yet, smallpox inoculations pose life-threatening risks to anyone with the AIDS virus (see related story, page 11) . A rapid test could prove critical in screening out potential vaccine recipients who don’t know they have HIV.
More and better HIV tests are expected in the near future. The FDA is close to approving an OraSure competitor, MedMira Inc.’s Reveal test. OraSure also plans to seek FDA approval soon
to use OraQuick to test a swab from a patient’s gums instead of blood.
Disgruntled Florida employee shoots two, then self
A disgruntled employee entered the office of Radiological Services, a division of the Florida State Department of Health in downtown Jacksonville, early one morning and shot and wounded two male coworkers and then fatally shot himself with his own handgun. The four-story building, which was not staffed by security guards but has security cameras, also houses Quest Diagnostics, the Northeast Florida AIDS Network and the Duval County Medical Society. About 200 people work in the office building.
FDA approves rapid HIV test
In November 2002, the Food and Drug Administration (FDA) approved a 20-minute HIV test that AIDS experts say is so easy to use that it will greatly cut the number of people who unknowingly carry and spread the disease. Today’s routine HIV tests take up to two weeks to provide results, and at least 8,000 people a year who test positive at public clinics never return to get the news.
The new OraQuick test should slash that number and encourage even more of the almost quarter-million Americans who don’t know they’re infected to seek testing. To use
West Nile update
On Oct. 25, 2002, the FDA issued guidance for blood product safety for cases of known or suspected West Nile Virus infection. The agency is against changes to standard donor screening or blood collection procedures, but it does urge collection centers to actively encourage blood donors to report post-donation illness that could be associated with West Nile infection.
HIV in healthcare workers
A whopping 23,473 healthcare workers have or had AIDS. The vast majority of these cases were not related to workplace transmission.
QAFACToid

www.quality-america.com
OSHA Watch January/February 2003Page 6
www.quality-america.com
OSHA Watch January/February 2003 Page 7
ASK THE EXPERT
Guns, needlesticks, noise, ...oh, my!On gun-toting patients
Q: We suspect that a patient in our waiting area was carrying a gun. What is the most safe and tactful course of action to take in this circumstance?
A: OSHA regulations do not address this situation, and guidance that the Joint Commission on Accreditation of Healthcare Organizations (JCAHO) provides is geared towards hospitals and other large healthcare facilities that have the luxury of having security guards. If your facility doesn’t have security personnel, contact law enforcement. If you do have security guards, contact them and direct them to ask the individual to empty his pockets. If the person is unwilling, call local law enforcement. If the person reveals a weapon, ask for the permit allowing him or her to carry it. If he or she has a permit, explain that your policy prohibits weapons in your facility, and direct the person to turn in the weapon while in your facility. If the person does not have a permit, call local law enforcement.Many practices put signs on their
doors that notify patients and visitors that weapons in the facility are prohibited. While this may not be a deterrent in some cases, it may serve as a reminder to others who enter the building, regardless of whether they have a permit to carry a gun.
Violence among coworkers
Q: I was physically assaulted by another employee and reported it to my supervisor. Instead of resolving the problem, the practice manager decided to remove me as the problem, presumably just for bringing it up. The termination was called “at will.” Now, I find out that they kept my attacker. What are my rights?
A: First, you have the right to go to the police and file a criminal
complaint for assault against the person who hit you. Second, under federal law, you have the right to a safe workplace, and you cannot be retaliated against for complaining about unsafe working conditions. You can file a complaint with OSHA. (There’s plenty of information on workplace violence on OSHA’s website www.osha.gov.) You have only 30 days to report retaliation to your local OSHA office. Finally, you have the right to file for workers’ compensation if you needed any medical treatment as a result of the workplace assault.
Contacting Uncle Sam about needlesticks
Q: Do we have to report needlestick info to OSHA?
A: No, but keep a Sharps Injury Log with the required information with your OSHA records.
Paperwork on eyewash maintenance?
Q: Must eyewashes be inspected? If so, how often?
A: OSHA doesn’t directly address this, but rather refers us to the American National Standard for Emergency Eyewash and Shower Equipment (ANSI Z358.1-1998, Section 5: Plumbed and Self-Contained Eyewash Equipment). Squeeze bottle eyewashes could become contaminated with bacteria and plumbed eyewashes could emit metals from unused pipes. ANSI says to inspect and maintain eyewashes “in accordance with manufacturer’s instructions” for squeeze bottle-type
Answers from
Dr. Sheila DunnPresident and CEO
Quality America
www.quality-america.com
OSHA Watch January/February 2003Page 6
www.quality-america.com
OSHA Watch January/February 2003 Page 7
eyewashes. For eyewashes connected to a faucet, “turn them on once per week to verify proper operation.” Rather than creating a new form (….ugh) to document this, Quality America’s OSHA Safety Program Manual includes weekly eyewash maintenance as a check-off item on the Monthly OSHA Checklist.
ANSWER TO LAST MONTH’S
Question of the MonthWhat testing or treatment is required for an employee who is stuck with a needle when the source patient is unknown (e.g., a stick from a sharp in a sharps container) or the patient refuses to be tested?
ANSWER: Since the source patient cannot be tested, the exposed employee must be presumed to have been exposed to the most common bloodborne pathogens–hepatitis B, hepatitis C and HIV–and tested and treated accordingly.
For additional information and charts illustrating testing and treatment, visit Quality America online. Click on the Question of the Month button on the home page of the site to view and download this information.
www.quality-america.com
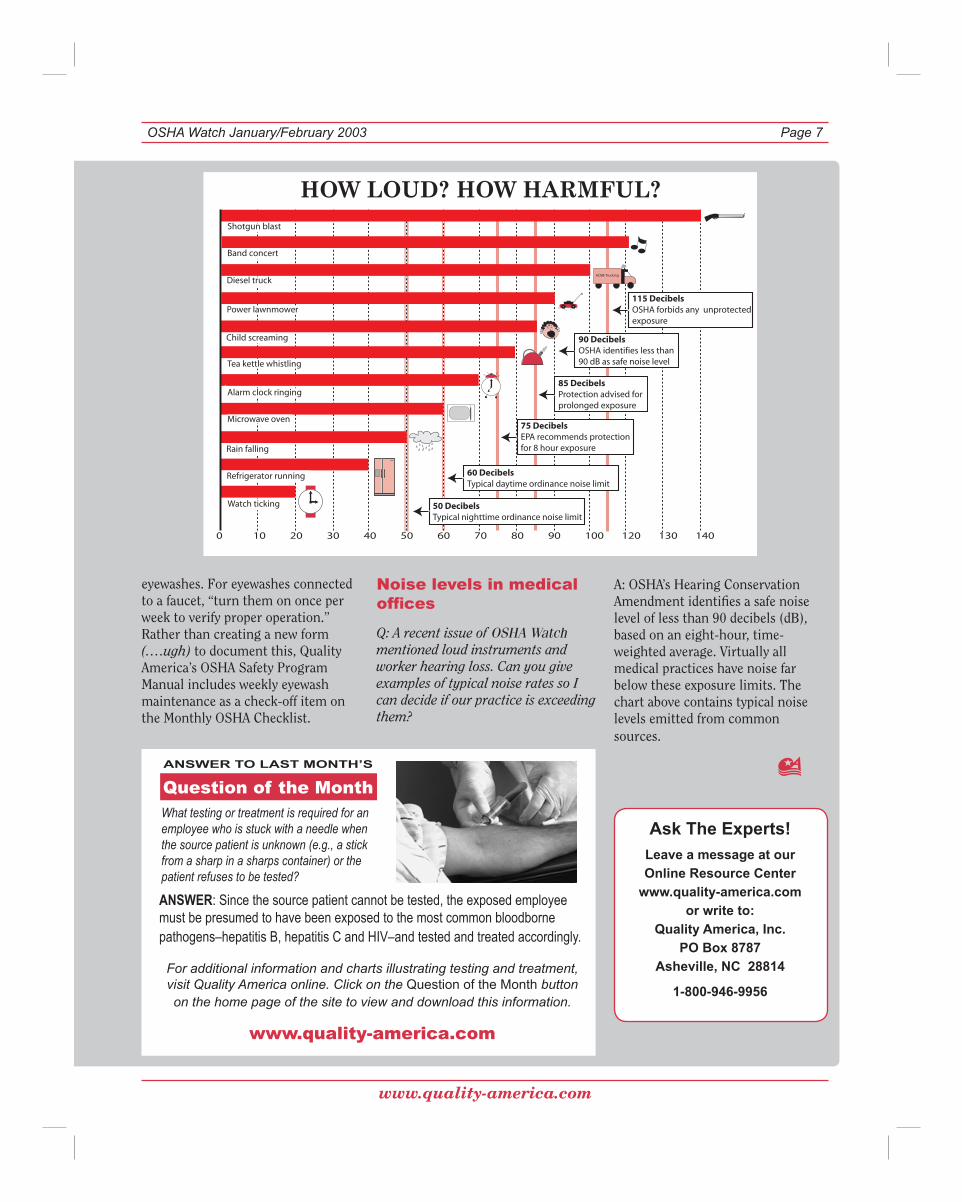
Noise levels in medical offices
Q: A recent issue of OSHA Watch mentioned loud instruments and worker hearing loss. Can you give examples of typical noise rates so I can decide if our practice is exceeding them?
Ask The Experts! Leave a message at our Online Resource Center
www.quality-america.comor write to:
Quality America, Inc.PO Box 8787
Asheville, NC 28814
1-800-946-9956
A: OSHA’s Hearing Conservation Amendment identifies a safe noise level of less than 90 decibels (dB), based on an eight-hour, time-weighted average. Virtually all medical practices have noise far below these exposure limits. The chart above contains typical noise levels emitted from common sources.
0 10 20 30 40 50 60 70 80 90 100 120 130 140
Watch ticking
Refrigerator running
Rain falling
Microwave oven
Alarm clock ringing
Tea kettle whistling
Child screaming
Power lawnmower
Diesel truck
Band concert
Shotgun blast
50 DecibelsTypical nighttime ordinance noise limit
60 DecibelsTypical daytime ordinance noise limit
75 DecibelsEPA recommends protectionfor 8 hour exposure
85 DecibelsProtection advised for prolonged exposure
115 DecibelsOSHA forbids any unprotected exposure
ACME Trucking
90 DecibelsOSHA identifies less than 90 dB as safe noise level
www.quality-america.com
OSHA Watch January/February 2003Page 8
www.quality-america.com
OSHA Watch January/February 2003 Page 9
Working safely with...
Hazardous chemicalsTake the mystery out of MSDS
Just about every medical setting uses hazardous chemicals, from mild cleaning products to dangerous acids. Many can cause injury or illness if not handled properly.
Until 1987, there was no guarantee that workers would be told about the chemical hazards they might face on the job, so OSHA created the Hazard Communication Standard (HazCom). Its purpose? To give every employee across the nation a “right to know” which hazards the job may expose them to, and how to protect themselves against these chemicals.
Specifically, the standard requires employers to teach employees to recognize, understand, and use labels and Material Safety Data Sheets (MSDS), and to follow safety procedures when working with hazardous substances.
Chemicals are Everywhere!
Chemicals aren’t just found in chemical companies or factories. Drugs, solvents, pesticides, oven cleaners, toner in the office copier, detergents and cleaning products are all used on a daily basis in every clinical setting. Some of these compounds are covered under the Hazard Communication Standard; some aren’t.
Chemicals that can be bought for general use in the home are not considered “hazardous” if they meet two criteria:
1) The chemical is used with the same
By law all chemical manufacturers have to let users know about hazards by providing a container label and a MSDS for the product. Labels give a quick overview about the chemical; MSDS provide more extensive information.
Deciphering MSDS
Before they begin a task, employees need to identify hazards and take the proper precautions. The key to working safely with hazardous chemicals is to read the MSDS. Although most Material Safety Data Sheets contain copious amounts of technical scientific jargon on an often poorly copied piece of paper, everything you ever wanted to know (and possibly more) about a chemical is on the MSDS. They are the only way to meet the intent of the HazCom Standard, telling staff in advance what could go wrong and what to do about it, then how and where to get help.
The most common hazardous chemical used in medical practices is glutaraldehyde. In response to the demand for safer high-level disinfectants, manufacturers are now offering glutaraldehyde-free chemicals. To demonstrate how to use MSDS for practical purposes, two MSDS are compared and contrasted on the next page. One is for Metricide 28™ (2.5% glutaraldehyde) and the other for Compliance™ (hydrogen peroxide and peracetic acid). Both are high-level disinfectants.
We suggest highlighting pertinent information on MSDS used in your
Visit Quality America’s Online Resource Center for:
• Sharps Evaluation Forms & Instructions• Sharps Injury Log• Glutaraldehyde Policies & Procedures• Eyewash Recommendations• Gas Cylinder Safety• Glass Capillary Tube Advisory• Latex Allergy Advisory• Hepatitis Test Information• Links for Downloading MSDS & OSHA Regulations
www.quality-america.com
Common substancesrequiring MSDS
• Bleach• Glutaraldehyde & other high-level disinfectants• Alcohol• Peroxide• Aerosol & injectable drugs, especially chemotherapy agents• Medical gases• Ethylene oxide• Mercury• X-ray developer
frequency as a consumer would use it.
2) The chemical is used according to the label instructions.
Any chemical that bears a hazard warning label and does NOT meet the criteria above needs a Material Safety Data Sheet.
To determine whether a drug needs a MSDS, the following criteria must be met:
1) The drug must be hazardous or dangerous.
2) An employee must be exposed to it. This is why tablets, pills and boxes of sample medications do not require MSDS.
www.quality-america.com
OSHA Watch January/February 2003Page 8
www.quality-america.com
OSHA Watch January/February 2003 Page 9
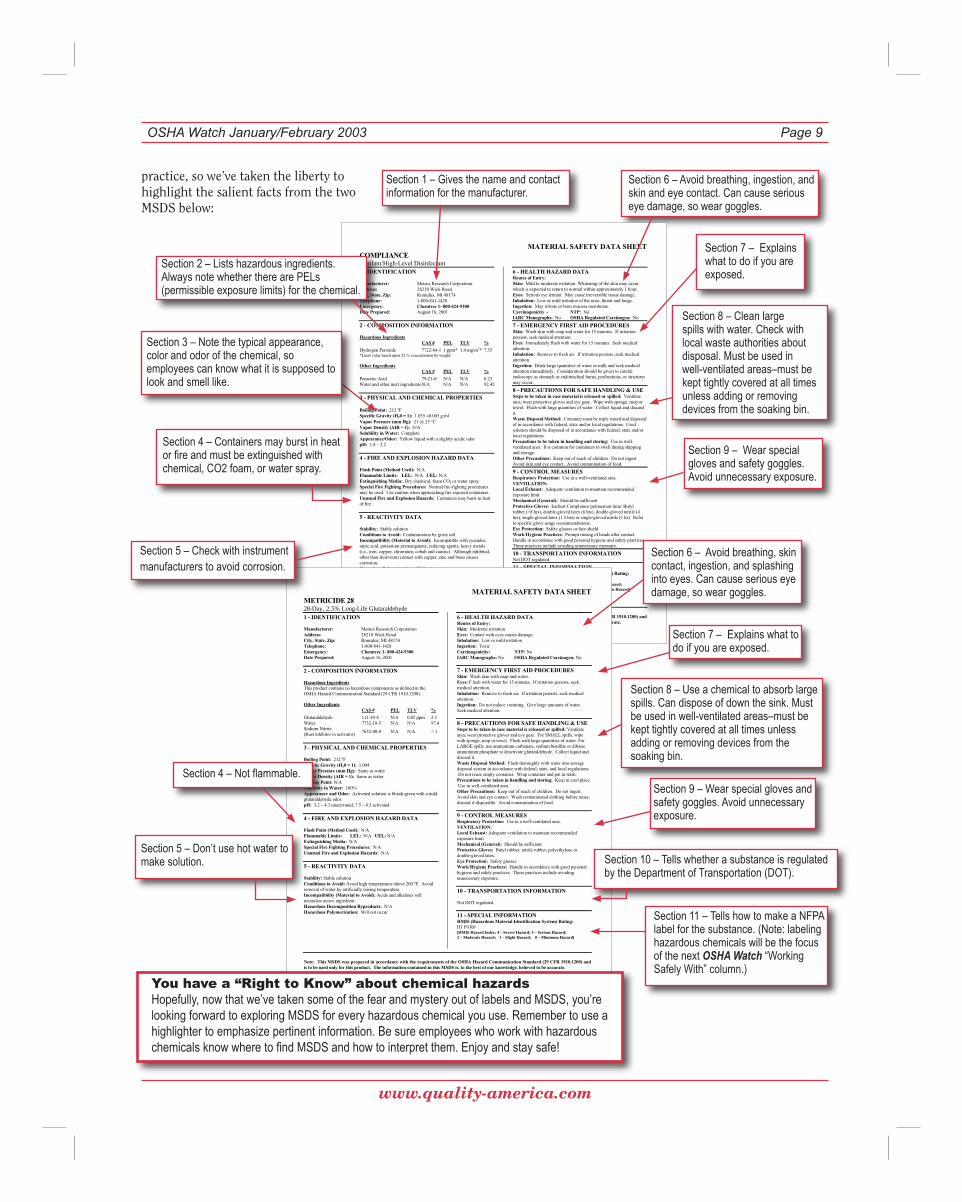
practice, so we’ve taken the liberty to highlight the salient facts from the two MSDS below:
MATERIAL SAFETY DATA SHEET COMPLIANCESterilant/High-Level Disinfectant
Note: This MSDS was prepared in accordance with the requirements of the OSHA Hazard Communication Standard (29 CFR 1910.1200) andis to be used only for this product. The information contained in this MSDS is, to the best of our knowledge, believed to be accurate.
1 - IDENTIFICATION
Manufacturer: Metrex Research Corporation Address: 28210 Wick Road City, State, Zip: Romulus, MI 48174 Telephone: 1-800-841-1428Emergency: Chemtrec 1- 800-424-9300Date Prepared: August 16, 2001
2 - COMPOSITION INFORMATION
Hazardous Ingredients CAS # PEL TLV %
Hydrogen Peroxide 7722-84-1 1 ppm* 1.4 mg/m3* 7.35 *Limit value based upon 52 % concentration by weight.
Other Ingredients CAS # PEL TLV %
Peracetic Acid 79-21-0 N/A N/A 0.23 Water and other inert ingredients N/A N/A N/A 92.42
3 - PHYSICAL AND CHEMICAL PROPERTIES
Boiling Point: 212 ºF Specific Gravity (H20 = 1): 1.035 ±0.005 g/ml Vapor Pressure (mm Hg): 21 @ 25 °CVapor Density (AIR = 1): N/A Solubility in Water: CompleteAppearance/Odor: Yellow liquid with a slightly acidic odor pH: 1.8 – 2.2
4 - FIRE AND EXPLOSION HAZARD DATA
Flash Point (Method Used): N/A Flammable Limits: LEL: N/A UEL: N/A Extinguishing Media: Dry chemical, foam CO2 or water spray. Special Fire Fighting Procedures: Normal fire-fighting procedures may be used. Use caution when approaching fire exposed containers. Unusual Fire and Explosion Hazards: Containers may burst in heat of fire.
5 - REACTIVITY DATA
Stability: Stable solution Conditions to Avoid: Contamination by gross soil Incompatibility (Material to Avoid): Incompatible with cyanides, nitric acid, potassium permanganate, reducing agents, heavy metals (i.e., iron, copper, chromium, cobalt and caustic). Although inhibited, other than short-term contact with copper, zinc and brass causes corrosion.Hazardous Polymerization: Will not occur
6 - HEALTH HAZARD DATA Routes of Entry: Skin: Mild to moderate irritation. Whitening of the skin may occur which is expected to return to normal within approximately 1 hour. Eyes: Serious eye irritant. May cause irreversible tissue damage. Inhalation: Low or mild irritation of the nose, throat and lungs. Ingestion: May irritate or burn mucosa membrane. Carcinogenicity - NTP: No IARC Monographs: No OSHA Regulated Carcinogen: No
7 - EMERGENCY FIRST AID PROCEDURES Skin: Wash skin with soap and water for 15 minutes. If irritation persists, seek medical attention. Eyes: Immediately flush with water for 15 minutes. Seek medical attention.Inhalation: Remove to fresh air. If irritation persists, seek medical attention.Ingestion: Drink large quantities of water or milk and seek medical attention immediately. Consideration should be given to careful endoscopy as stomach or endotracheal burns, perforations, or strictures may occur.
8 - PRECAUTIONS FOR SAFE HANDLING & USE Steps to be taken in case material is released or spilled: Ventilate area; wear protective gloves and eye gear. Wipe with sponge, mop or towel. Flush with large quantities of water. Collect liquid and discard it.Waste Disposal Method: Container must be triple rinsed and disposed of in accordance with federal, state and/or local regulations. Used solution should be disposed of in accordance with federal, state and/or local regulations. Precautions to be taken in handling and storing: Use in well-ventilated area. It is common for containers to swell during shipping and storage.Other Precautions: Keep out of reach of children. Do not ingest. Avoid skin and eye contact. Avoid contamination of food.
9 - CONTROL MEASURES Respiratory Protection: Use in a well-ventilated area. VENTILATION:Local Exhaust: Adequate ventilation to maintain recommended exposure limit Mechanical (General): Should be sufficient Protective Gloves: Earliest Compliance permeation time: Butyl rubber (>8 hrs), double-gloved latex (6 hrs), double-gloved nitrile (4 hrs), single-gloved latex (1.5 hrs) or single-gloved nitrile (1 hr). Refer to specific glove usage recommendations. Eye Protection: Safety glasses or face shield Work/Hygiene Practices: Prompt rinsing of hands after contact.Handle in accordance with good personal hygiene and safety practices. These practices include avoiding unnecessary exposure.
10 - TRANSPORTATION INFORMATION Not DOT regulated.
11 - SPECIAL INFORMATION HMIS (Hazardous Material Identification System) Rating: H3 F0 R1 [HMIS Hazard Index: 4 – Severe Hazard; 3 – Serious Hazard; 2 – Moderate Hazard; 1 – Slight Hazard; 0 – Minimum Hazard]MATERIAL SAFETY DATA SHEET
METRICIDE 2828-Day, 2.5% Long-Life Glutaraldehyde
Note: This MSDS was prepared in accordance with the requirements of the OSHA Hazard Communication Standard (29 CFR 1910.1200) andis to be used only for this product. The information contained in this MSDS is, to the best of our knowledge, believed to be accurate.
1 - IDENTIFICATION
Manufacturer: Metrex Research Corporation Address: 28210 Wick Road City, State, Zip: Romulus, MI 48174 Telephone: 1-800-841-1428Emergency: Chemtrec 1- 800-424-9300Date Prepared: August 16, 2001
2 - COMPOSITION INFORMATION
Hazardous IngredientsThis product contains no hazardous components as defined in the OSHA Hazard Communication Standard (29 CFR 1910.1200).
Other IngredientsCAS # PEL TLV %
Glutaraldehyde 111-30-8 N/A 0.05 ppm 2.5Water 7732-18-5 N/A N/A 97.4 Sodium Nitrite (Rust inhibitor in activator)
7632-00-0 N/A N/A < 1
3 - PHYSICAL AND CHEMICAL PROPERTIES
Boiling Point: 212 ºF Specific Gravity (H20 = 1): 1.004 Vapor Pressure (mm Hg): Same as water Vapor Density (AIR = 1): Same as water Melting Point: N/A Solubility in Water: 100%Appearance and Odor: Activated solution is bluish-green with a mild glutaraldehyde odor. pH: 3.2 – 4.3 unactivated; 7.5 – 8.5 activated
4 - FIRE AND EXPLOSION HAZARD DATA
Flash Point (Method Used): N/A Flammable Limits: LEL: N/A UEL: N/A Extinguishing Media: N/A Special Fire Fighting Procedures: N/A Unusual Fire and Explosion Hazards: N/A
5 - REACTIVITY DATA
Stability: Stable solution Conditions to Avoid: Avoid high temperatures above 200 ºF. Avoid removal of water by artificially raising temperature. Incompatibility (Material to Avoid): Acids and alkalines will neutralize active ingredient. Hazardous Decomposition Byproducts: N/A Hazardous Polymerization: Will not occur
6 - HEALTH HAZARD DATARoutes of Entry: Skin: Moderate irritation Eyes: Contact with eyes causes damage. Inhalation: Low or mild irritation Ingestion: Toxic Carcinogenicity: NTP: No IARC Monographs: No OSHA Regulated Carcinogen: No
7 - EMERGENCY FIRST AID PROCEDURES Skin: Wash skin with soap and water. Eyes: F lush with water for 15 minutes. If irritation persists, seek medical attention. Inhalation: Remove to fresh air. If irritation persists, seek medical attention.Ingestion: Do not induce vomiting. Give large amounts of water.Seek medical attention.
8 - PRECAUTIONS FOR SAFE HANDLING & USE Steps to be taken in case material is released or spilled: Ventilate area; wear protective gloves and eye gear. For SMALL spills, wipe with sponge, mop or towel. Flush with large quantities of water. For LARGE spills, use ammonium carbonate, sodium bisulfite or dibasic ammonium phosphate to deactivate glutaraldehyde. Collect liquid and discard it.Waste Disposal Method: Flush thoroughly with water into sewage disposal system in accordance with federal, state, and local regulations. Do not reuse empty container. Wrap container and put in trash. Precautions to be taken in handling and storing: Keep in cool place. Use in well-ventilated area.Other Precautions: Keep out of reach of children. Do not ingest. Avoid skin and eye contact. Wash contaminated clothing before reuse; discard if disposable. Avoid contamination of food.
9 - CONTROL MEASURES Respiratory Protection: Use in a well-ventilated area. VENTILATION:Local Exhaust: Adequate ventilation to maintain recommended exposure limit. Mechanical (General): Should be sufficient Protective Gloves: Butyl rubber, nitrile rubber, polyethylene or double-gloved latex. Eye Protection: Safety glasses Work/Hygiene Practices: Handle in accordance with good personal hygiene and safety practices. These practices include avoiding unnecessary exposure.
10 - TRANSPORTATION INFORMATION
Not DOT regulated.
11 - SPECIAL INFORMATION HMIS (Hazardous Material Identification System) Rating: H1 F0 R0 [HMIS Hazard Index: 4 – Severe Hazard; 3 – Serious Hazard; 2 – Moderate Hazard; 1 – Slight Hazard; 0 – Minimum Hazard]
Section 1 – Gives the name and contact information for the manufacturer.
Section 6 – Avoid breathing, ingestion, and skin and eye contact. Can cause serious eye damage, so wear goggles.
Section 2 – Lists hazardous ingredients. Always note whether there are PELs (permissible exposure limits) for the chemical.
Section 3 – Note the typical appearance, color and odor of the chemical, so employees can know what it is supposed to look and smell like.
Section 7 – Explains what to do if you are exposed.
Section 7 – Explains what to do if you are exposed.
Section 8 – Use a chemical to absorb large spills. Can dispose of down the sink. Must be used in well-ventilated areas–must be kept tightly covered at all times unless adding or removing devices from the soaking bin.
Section 9 – Wear special gloves and safety goggles. Avoid unnecessary exposure.
Section 9 – Wear special gloves and safety goggles. Avoid unnecessary exposure.
Section 8 – Clean large spills with water. Check with local waste authorities about disposal. Must be used in well-ventilated areas–must be kept tightly covered at all times unless adding or removing devices from the soaking bin.
Section 11 – Tells how to make a NFPA label for the substance. (Note: labeling hazardous chemicals will be the focus of the next OSHA Watch “Working Safely With” column.)
Section 5 – Don’t use hot water to make solution.
Section 4 – Not flammable.
Section 6 – Avoid breathing, skin contact, ingestion, and splashing into eyes. Can cause serious eye damage, so wear goggles.
Section 10 – Tells whether a substance is regulated by the Department of Transportation (DOT).
You have a “Right to Know” about chemical hazardsHopefully, now that we’ve taken some of the fear and mystery out of labels and MSDS, you’re looking forward to exploring MSDS for every hazardous chemical you use. Remember to use a highlighter to emphasize pertinent information. Be sure employees who work with hazardous chemicals know where to find MSDS and how to interpret them. Enjoy and stay safe!
Section 5 – Check with instrument manufacturers to avoid corrosion.
Section 4 – Containers may burst in heat or fire and must be extinguished with chemical, CO2 foam, or water spray.
www.quality-america.com
OSHA Watch January/February 2003Page 10
www.quality-america.com
OSHA Watch January/February 2003 Page 11
HOT FINDSand Cool Websites
Bioterrorism planninghttp://bioprn.advancepcsmdnet.com/new_splash.html
A patient comes into your facility complaining of high fever, nausea, vomiting and shortness of breath after inhaling a white powder when opening an envelope at her job two days ago. Could this be a victim of a bioterrorism attack? Now what do you do?
The Bioterrorism Practical Readiness Network (Bio-PRN) has a quick reference and intervention guide for clinicians and healthcare administrators. It outlines the steps to take in two possible emergency scenarios and offers sample scripts for addressing each crisis. There’s also a section for clinicians that features diagrams for differentiating biological terrorism cases from common diseases, such as influenza. Go to http://bioprn.advancepcsmdnet.com/new_splash.html
Help for OSHA inspectionswww.osha.gov/Publications/osha3000.pdf
OSHA’s new booklet, “Employer Rights and Responsibilities Following an OSHA Inspection,” explains the types of violations and suggests appropriate legal actions to minimize penalties and avoid repeat violations. Available at www.osha.gov/Publications/osha3000.pdf
Rapid HIV testwww.orasure.com
For more information about the new rapid HIV test, visit OraSure Technologies Inc.: www.orasure.com
Smallpox response guidelineswww.cdc.gov/smallpox
The CDC has updated the Smallpox Response Plan and Guidelines that were released in November 2001. The clinic guide assists in planning for larger-scale, post-event vaccination when exposure circumstances indicate the need to supplement the ring vaccination approach with broader protective measures. It also describes the activities and staffing needs associated with large-scale smallpox vaccination clinics, including suggested protocols for vaccine safety monitoring and treatment.
The clinic guide provides an example of a model smallpox clinic and provides samples of pertinent clinic consent forms and patient information sheets that would be used at a clinic. Visit www.cdc.gov/smallpox.
Revamped OSHA standardwww.access.gpo.gov/su_docs/aces/aces140.html
The Exit Routes, Emergency Action Plans, and Fire Prevention Plans Standard was recently published in the Federal Register (11/7/02, pp. 67950-67965). The next issue of OSHA Watch will review the important components of OSHA requirements for exits and fire prevention. Review this document at www.access.gpo.gov/su_docs/aces/aces140.html.
www.quality-america.com
OSHA Watch January/February 2003Page 10
www.quality-america.com
OSHA Watch January/February 2003 Page 11
Routine smallpox vaccination ended in this country in 1972 as the disease was being wiped out. Now, fearing a bioterrorist attack, the U.S. is preparing to vaccinate hundreds of thousands of soldiers and healthcare workers, and is considering whether to offer the vaccine to the public.
Smallpox can kill 30% of its victims, but the vaccine to prevent the disease has long been
eczema or even a history of it, is occasionally fatal. The worst cases tended to occur in people with active eczema when they were exposed to vaccinia.
Nearly 69% of the infections in contacts occurred in children younger than five whose sibling or close relative had been recently vaccinated. But one baby was infected by a nurse, and two children by contacts at daycare. Several adults were infected by vaccinated children, and one woman developed eczema vaccinatum after sleeping with a recently vaccinated soldier. A wrestler infected his opponent.
More risk than in the past
The risks today may be higher than when smallpox vaccinations were administered in the past because more people than ever have disorders of the skin or
Smallpox vaccine: how risky?
– See Smallpox vaccine, page 12
Key Smallpox Vaccine Concerns
§ Who will make up Regional Smallpox Response Teams?
§ How to care for the vaccination site?
§ Should administrative leave be given for vaccinated healthcare workers?
§ How to screen for atopic dermatitis, pregnancy and HIV before vaccination?
immune system. These conditions predispose them to adverse effects from the vaccine or from close contact with those who have been vaccinated.
For example, eczema is now two to three times more common than in the past (the reason for this is not known). Also, more people have lowered immunity from HIV or other immune system diseases, or from drugs used to treat cancer or prevent transplant rejection.
One of the study authors noted that the risks of vaccination are real, whereas the threat of a smallpox attack is theoretical–no one knows for certain whether a country or a terrorist group has the virus. He warned of the threat of a potentially fatal condition called progressive vaccinia, in which the sore at the vaccination site keeps growing and spreading, and systemic illness develops. There is no cure.
Source: CDC’s Smallpox Response Plan and Guidelines, http://www.cdc.gov
regarded as the most dangerous of all immunizations, both to recipients and their close contacts. A major concern is the possibility that newly vaccinated people might inadvertently infect others, particularly people with a high risk of being harmed by vaccinia, the virus used in the smallpox vaccine.
To help clarify the risk of smallpox vaccination, the September 2002 Journal of the American Medical Association reported on an analysis of smallpox vaccination data from the 1960s.
Analyzing the most dangerous of all vaccines
The analysis, based on rates of adverse reactions in 11.8 million Americans vaccinated for the first time in 1963 and 1968, concluded that for every 1 million smallpox vaccine recipients, 15 will have life-threatening reactions, including one or two deaths. Hundreds will have severe rashes or other illnesses.
For every 100,000 people vaccinated for the first time, the study found, vaccinia spread by close contact to two to six others who had not been vaccinated. Most unvaccinated people who got the virus developed “accidental infections”–sores that healed on their own and most likely acted like secondhand vaccinations, giving them immunity.
But one or two became very ill with a condition called eczema vaccinatum, which can cause fever and a severe, extensive rash with scarring. The condition, which affects some people who have the skin disorder
www.quality-america.com
OSHA Watch January/February 2003Page 12
Coming Next Issue
Look for the March/April 2003
edition of OSHA Watch with all your favorite features, including...
Ask The Expert
In The News
Hot Finds and Cool Websites
plus these special features…
Emergency Building Evacuation
Fire Extinguishers: Where and How Many?
Chemical Labeling
…and much more!
���������������� ���� ���������� �����
OSHA Watch Published Bimonthly
by
Dr. Sheila Dunn, President & CEOPO Box 8787 • Asheville, NC 28814
1-800-946-9956
www.quality-america.com
Subscription Rates:1 Year - $79 | 2 Years - $145
3 Years - $199
© 2003, Quality America®, Inc. All rights reserved. No part of this publication may be reproduced, stored in any retrieval system, or transmitted in any form or by any means–elec-tronic, mechanical, photocopying, recording or otherwise–without the prior written permission of the publisher, Quality America®, Inc.
His specific concern was related to the number of immunocompromised people who could contract progressive vaccinia. The Centers for Disease Control and Prevention (CDC) estimates that 300,000 Americans have HIV and do not know it, and more than 23,000 healthcare workers have AIDS. Therefore, an alarming number of undiagnosed people with immune disorders could be at risk if they were vaccinated when they should not be, or if they came in contact with other vaccinated people.
Newly issued CDC guidelines say people should not be vaccinated for smallpox if they have had eczema or a related disorder, atopic dermatitis, or have lived with someone who did. Other skin conditions that rule out vaccination include impetigo or pustules, unhealed burns, contact dermatitis; and chickenpox. But people with such risk factors may have to be vaccinated if there is an attack and they are exposed to the disease.
The debate continues
The American Academy of Pediatrics says the nation’s smallpox plan should involve limited vaccinations if a case occurs, not universal inoculations before there’s even an attack. According to a policy statement issued by the Academy, potential side effects on children are too severe. The group also warned that available vaccines have not been tested on children, who may be at higher risk for bad reactions.
The debate on the risks versus the benefits of the smallpox vaccine rages on, but one thing is certain: If a confirmed smallpox outbreak occurs
Smallpox vaccine: the debate continues– from page 11
within the U.S., rapid, voluntary vaccination of some people will be required to contain it. Those definitely asked to acquire the vaccination would be close contacts of infected patients and people closely associated with those contacts.
CLOSE TO HOME © 2002 John McPherson. Reprinted with permission of UNIVERSAL PRESS SYNDICATE. ALL RIGHTS RESERVED.