-
7/31/2019 Orthotics Lower Limb
1/9
1
LOWER EXTREMITY ORTHOTICS TO ENHANCE AMBULATION
INTRODUCTION
The first orthotic objective is to design an orthosis that
addresses the biomechanicalneeds of the client by providing support
and substitution for lost muscle function or provide
control of excessive spasticity. The principle of the
intervention with the least amount of control
necessary is achieved by limiting motion at any joint only if it
will assist in providing improvedjoint stability and creating a
stable base of support. The second objective is to provide a
stableskeletal alignment. Long-term effects of skeletal
misalignment include the acquisition of
pathomechanical deformities. (1) While the biomechanical needs
of the patient are routinelyconsidered, alignment problems leading
to chronic pathomechanical deformities are frequently
overlooked. For example, a patient may be fitted with an off the
shelf posterior leaf spring anklefoot orthosis (AFO) to obtain
clearance of the foot during swing phase but the orthosis may
not
provide adequate support of the subtalar joint during stance
phase once weight is applied to theleg. This alignment will over
time lead to excessive pronation composed of subtalar eversion,
midtarsal depression or pronation and forefoot abduction. In the
patient population wheremuscle loss and imbalance are common,
skeletal alignment as well as muscle stability is of
utmost importance.
GOALS FOR ORTHOTIC INTERVENTION
The most obvious use for an ankle foot orthosis is control of
the ankle joint in the sagittal
plane. The AFO can sustain clearance of the foot during swing
phase if there is inadequatestrength of the ankle dorsiflexors
including the tibialis anterior, extensor hallicus longus, and
extensor digitorum longus. The AFO can also substitute for push
off during stance phase if theankle plantarflexors are weak. Less
obvious goals of an AFO include controlling the position of
the ankle in the sagittal plane to control mild knee
hyperextension, as well as knee flexioninstability, due to weakness
of the quadriceps.
Coronal plane stability of the subtalar joint can be achieved
with a well-designed plastic
AFO as well as coronal plane supination and pronation of the
forefoot. Transverse plane controlmust also be considered when
designing an orthotic system. With proper stabilization of
thesubtalar joint, transverse plane control of forefoot abduction
and adduction can be obtainable.
The more difficult component to control of transverse rotation,
is internal rotation of the femurand tibia, which can be addressed
by careful material selection and design principles. The
materials and components must not allow transverse rotation
structurally to occur and the forcesystems must be appropriately
placed for effective force couple systems to prevent unwanted
movement.Through optimal skeletal alignment of the person along
with appropriate biomechanical
controls in our AFO design, we hope to create a stable base of
support to allow safe and efficientambulation and prevent the
development of future pathomechanical deformities.
-
7/31/2019 Orthotics Lower Limb
2/9
2
BIOMECHANICAL CONTROLS FOR AFOS
Three-Point Force Systems
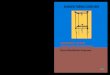
The controls incorporated in orthotic systems are based on
three-point force systems to
affect alignment by controlling two adjacent skeletal segments.
(Fig. 1) The corrective force islocated on the convex side of the
curve at the joint addressed (b). Two counteractive forces are
positioned on the opposite side above (c) and below (a) the
corrective force. As the distance ofthe counteractive force from
the corrective force increases so do the lever arms and therefore
the
effectiveness. Based on the principle, Pressure=Total Force/
Area of Force Application, theobjective is to distribute the forces
over a larger area to decrease the resultant pressures. (2) A
well fitting total contact orthosis avoiding bony prominences
and utilizing effective three-pointforce systems will assist in
achieving this objective.
Fig. 1 Three-Point Force System
-
7/31/2019 Orthotics Lower Limb
3/9
3
To provide mediolateral stability at the subtalar joint and
control excessive subtalar
eversion, the three-point force system (Fig. 2) has the
corrective force applied proximal to themedial malleolus (b) and at
the sustentaculum tali (c). Due to the fact that pressure cannot
be
applied to the bony medial malleolus, the corrective force must
be applied over two adjacentareas. The sustentaculum tali (ST) is
located on the calcaneus and if stabilized correctly by a ST
modification or pad provides a horizontal ledge to support the
talus. (3) The two counteractiveforces at the distal lateral
calcaneus (a) and proximal lateral calf (d) are above and below
the
joint and as far away from the joint as possible to produce
longer lever arms.Subtalar inversion (Fig. 3) from an unopposed
tibialis anterior is controlled by the
corrective force placed proximal to the lateral malleolus (c)
and over the cuboid (b) if possible.Again, we are unable to apply a
direct force over the lateral malleolus and must place the
corrective forces adjacent. The two counteractive forces are
located at the distal medialcalcaneus (a) and the medial proximal
flare (d).
Fig. 2 Subtalar eversion Fig. 3 Subtalar inversion
force system force system
-
7/31/2019 Orthotics Lower Limb
4/9
4
Plantarflexion Stop
A plantarflexion stop or posterior stop in an AFO (Fig. 4) is
designed to substitute forinadequate strength of the ankle
dorsiflexors including the tibialis anterior, extensor hallicus
longus, and the extensor digitorum longus during swing phase of
gait. This stop is effective bylimiting the plantarflexion range of
motion of the talocrural joint. The three-point force system
has the corrective force at the shoe instep or ankle strap and
two counteractive forces, one at theplantar surface at the ball of
the foot and the second on the posterior calf region. An
important
concept when evaluating the ankle position is the tibial angle
to the floor (Fig. 5)
Fig. 4 Articulated AFO with Fig. 5 Tibial angle to floor
a plantarflexion stop
We define the tibial angle to the floor by bisecting the distal
one-third of the tibia in thesagittal plane and measuring this
angle in relationship to the floor. Each shoe has a heel height
or the difference of the height of the heel minus the thickness
of the material at the ball of thefoot. This resultant slope
affects the tibial angle to the floor once the AFO is inserted into
the
shoe. The tibial angle to the floor must be measured with the
shoe on when evaluating thestability and function during
ambulation. This angle will be altered with the use of shoes
with
varying heel heights. For example, a tibia placed in relative
dorsiflexion to the floor whilewearing a shoe produces a knee
flexion moment at loading response and can decrease a mild to
moderate knee hyperextension moment during stance phase of gait
or create knee flexioninstability at loading response when
walking.
-
7/31/2019 Orthotics Lower Limb
5/9
5
Dorsiflexion Stop
A dorsiflexion stop or anterior stop in an AFO (Fig. 6) is used
to simulate push off andsubstitutes for weak ankle plantarflexors.
The stop will limit tibial advancement during
midstance providing stability in the sagittal plane by limiting
the doriflexion range of motion ofthe talocrural joint. Limitation
of dorsiflexion to neutral or in slight plantarflexion also
influences the stability of the knee and is of assistance when
the quadriceps strength is grade fairminus. With restraint of the
tibia, the bodys center of mass moves anterior to the knee joint
axis
and due to the resultant ground reaction force vector a knee
extension moment is created.
Fig. 6 Laminated AFO with a Fig. 7 Articulated AFO with a
dorsiflexion stop dorsiflexion assist
Dorsiflexion AssistA dorsiflexion assist joint can be composed
of a spring arrangement (Fig. 7) or a flexure
joint. Both components function to bring the talocrural joint
through dorsiflexion range ofmotion, thus providing clearance of
the foot during swing phase. They also allow plantarflexion
range of motion at loading response therefore decreasing the
knee flexion moment which maydestabilize the knee and increase the
potential for falls. (7)
-
7/31/2019 Orthotics Lower Limb
6/9
6
AFO DESIGNS
Conventional AFO Designs
A conventional design AFO (Fig. 8) is composed of a shoe,
stirrup, ankle joint,
sidebar/upright, calfband, and calf closure. The control of the
subtalar joint and foot depends onthe stability and integrity of
the shoe. Once the shoe is worn, the effectiveness decreases. A
soleplate extending to the metatarsal heads is added between the
midsole and the outer shoe ofthe shoe to produce an effective lever
arm. Due to the lack of total contact, the conventional
AFO is not an effective design for controlling coronal or
transverse plane motion. A foot insertor UCBL foot orthosis may be
added inside the shoe to improve the control and alignment of
the
subtalar and midtarsal joints.
Fig. 8 Conventional AFO Fig. 9 Double adjustableankle joint
A double adjustable ankle joint (Fig. 9) allows a greater degree
of adjustability. The dual
channel system enables the practitioner to utilize the following
controls at the ankle: 1) fixedposition of the ankle in the
sagittal plane, 2) limited range of motion, 3) controlled
plantarflexion
at loading response due to a spring in the posterior channel and
a dorsiflexion stop via a pin inthe anterior channel as shown in
Figure 9.
-
7/31/2019 Orthotics Lower Limb
7/9
7
Plastic AFO Designs
The biomechanical functions of plastic AFOs are described by
their trimlines. Thetrimlines reflect the rigidity in relationship
to the range of motion they allow at the talocrural
joint. They range from a solid ankle design (Fig. 10)
positioning the ankle in a fixed position to
a posterior leaf spring design (Fig. 11). A solid ankle design
is used with combined dorsiflexionand plantarflexion muscle loss or
weakness with a trimline at the ankle region anterior to
themalleoli. It affords maximal stability in the sagittal, coronal,
and transverse planes at the ankle
joint, subtalar, and midtarsal joints by placing the joint in a
fixed position by utilizing multiplethree-point force systems or
force couples. To safely control the knee with this AFO the
individual will need grade fair strength of the quadriceps and a
tibial angle to the floor of 0-5degrees of relative dorsiflexion
when positioned in the shoe.
A posterior leaf spring AFO is trimmed posterior to the malleoli
allowing 1) controlledplantarflexion at loading response, 2)
dorsiflexion range of motion during late midstance through
terminal stance, and 3) providing clearance of the foot during
swing phase of gait. Many currentpre-fabricated designs are
extremely flexible and offer no stability of the subtalar and
midtarsal
joints during weight bearing. A custom fabricated posterior leaf
spring design AFO can bedesigned to offer a more refined amount of
resistance and improved control of the subtalar and
midtarsal joints by the trimlines and casting features. The most
common function or goal whenusing this AFO design is the limitation
of plantarflexion range of motion during swing phase
when an individual has weakness of the ankle dorsiflexors.
Fig. 10 Solid Ankle AFO Fig. 11 Posterior Leaf Spring AFO
-
7/31/2019 Orthotics Lower Limb
8/9
8
The term, ground reaction AFO (Fig. 12) has historically been
used to describe the plasticAFO composed of a solid ankle design
with a pretibial shell. Ground reaction force vectors
induce a knee extension moment at the end of stance phase when a
dorsiflexion stop or anteriorstop limiting the dorsiflexion range
of motion is incorporated into the design. As the center of
mass of the individual is moving forward and tibial advancement
is limited by the AFO, a kneeextension moment is created. The
tibial angle to the floor contributes to determining knee
stability as well as the length of the foot plate. Stability at
midstance is achieved with the ankleat 90 degrees to the floor or
slightly posteriorly tilted or plantarflexed. A knee flexion
moment
will be accentuated at loading response as the dorsiflexion
angle of the AFO is increased. Thelength of the footplate may be
extended distally past the usual length at the metatarsal heads
to
increase the knee extension moment arm during midstance through
terminal stance. The groundreaction AFO design is indicated with
quadriceps strength of fair minus (4). Another AFO
design offering this control is composed of double adjustable
ankle joints, a footplate, and apretibial shell. (Fig. 13) The
ankle joint may be designed with stops in both channels or a stop
in
the anterior channel and a spring in the posterior channel. As
discussed previously, the spring inthe posterior channel will allow
controlled plantarflexion range of motion at loading response
and will reduce the knee flexion moment that may cause knee
instability.
Figure 12 Solid Ankle Ground Figure 13 AFO with pretibial
shell,Reaction AFO Double adjustable ankle
joints
-
7/31/2019 Orthotics Lower Limb
9/9
9
References
1. Fish DJ, Nielsen JP. Clinical Assessment of Human Gait. JPO
1993; Vol. 5, No. 2: 27-36.
2. Fess EE, Philips CA. Hand Splinting: Principles and Methods,
2nd
Edition St. Louis,MO: C.V. Mosby, 1987; 126.
3. Carlsen MJ, Berglund G. An Effective Orthotic Design for
Controlling the UnstableSubtalar Joint: Orthotics and Prosthetics,
1979; 33 (1): 31-41.
4. Yang GW, Chu DS. Floor Reaction Orthosis: Clinical
Experience. Orthotics andProsthetics 1986; Vol. 40, No. 1,
33-37.