Embed Size (px)
Citation preview
Washington University School of MedicineDigital Commons@Becker
Open Access Publications
3-1-2010
Orthopaedic surgeons and the medical deviceindustry: The threat to scientific integrity and thepublic trustRichard H. GelbermanWashington University School of Medicine in St. Louis
David SamsonWolff and Samson PC
Sohail K. MirzaDartmouth-Hitchcock Medical Center
John J. CallaghanUniversity of Iowa Health Care
Vincent D. PellegriniUniversity of Maryland School of Medicine
Follow this and additional works at: http://digitalcommons.wustl.edu/open_access_pubs
Part of the Medicine and Health Sciences Commons
This Open Access Publication is brought to you for free and open access by Digital Commons@Becker. It has been accepted for inclusion in OpenAccess Publications by an authorized administrator of Digital Commons@Becker. For more information, please contact [email protected].
Recommended CitationGelberman, Richard H.; Samson, David; Mirza, Sohail K.; Callaghan, John J.; and Pellegrini, Vincent D., ,"Orthopaedic surgeons andthe medical device industry: The threat to scientific integrity and the public trust." The Journal of Bone and Joint Surgery.92,3.765-777. (2010).http://digitalcommons.wustl.edu/open_access_pubs/1047
the
Orthopaedicforum
An AOA Symposium
Orthopaedic Surgeons and theMedical Device Industry
The Threat to Scientific Integrity and the Public Trust
By Richard H. Gelberman, MD, David Samson, Esq, Sohail K. Mirza, MD, MPH, John J. Callaghan, MD,and Vincent D. Pellegrini Jr., MD
The purpose of this article is to relaterecent actions by the United StatesDepartment of Justice, the Institute ofMedicine, the Association of Ameri-can Medical Colleges (AAMC), andothers to the specific challenges con-fronting the specialty of orthopaedicsurgery. Further, it strives to reconcilethe duty and value propositionsassociated with the orthopaedicsurgeon-medical device company re-lationship, with the persistent risks
that are attendant to that relation-ship, and to develop a new path—onethat strives to restore the integrity ofscientific investigation and day-to-day clinical decision making, whileproviding justification for futurephysician-industry interaction. Toconsider the topic in perspective, it isinteresting to assess the origins ofthe current model of physician-industry interaction as they relatespecifically to the issues currently
confronting the specialty of ortho-paedic surgery.
In 1980, novel legislation in thefield of intellectual property, the Bayh-Dole Act, for the first time alloweduniversities and nonprofit organizationsto replace the government as theprincipal beneficiaries of commercialdevelopment resulting from basic-science and clinical research. In essence,the act transferred the ownership ofdiscoveries made with the help of
Disclosure: The authors did not receive any outside funding or grants in support of their research for or preparation of this work. One or more of theauthors, or a member of his or her immediate family, received, in any one year, payments or other benefits in excess of $10,000 or a commitment oragreement to provide such benefits from commercial entities (Medartis, Wright Medical, Lippincott Williams & Wilkins, University of Washington[royalties], and DePuy [consultation, intellectual property, and royalty agreement]).
765
COPYRIGHT � 2010 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2010;92:765-77 d doi:10.2106/JBJS.I.01164

federal research grants to the universi-ties and small businesses where thosediscoveries were made. On the face of it,the Bayh-Dole Act made sense. Con-vinced that government ownership haddeterred the development of incentivesnecessary to promote innovation andhad severely inhibited productivity,supporters saw the act as a remedy forthe depressed American economy in the1970s. The goal of the act was specific—to address the concern that Americanfirms were not using academic researchefficiently for commercialization—and it intended to remedy that short-coming by facilitating patenting andlicensing by U.S. universities of inven-tions from federally funded research. Ifsuccessful, it could help to usher ina new era of innovation in America. Itwas an interesting concept—one thatsupporters claim led to a very positivechain of events and to years of U.S.leadership in a variety of fields. Thepharmaceutical and medical device in-dustries led the way, dramatically in-creasing licenses and patents in the yearsthat followed the adoption of thelegislation.
For the medical profession, theresult was, according to one observer,a modern alchemy, where ‘‘. . . ivorytowers were being turned into gold andsociety was benefiting from hundredsof novel treatments introduced fora host of diseases.’’1 While that viewmay have been accurate for a time,a series of increasing concerns de-veloped over the years following pas-sage of the Bayh-Dole Act. In what hasbeen termed one of the most seriousunintended consequences of a majorpiece of legislation, physician scien-tists and their universities evolvedgradually from noble, highly trustedinstitutions into something closer toventure capital firms1. The increase insubstantial financial conflicts of in-terest between clinical investigatorsand industry rose to such a remarkablelevel that, by 2007, a large percentageof physicians2 and almost two-thirdsof the department chairs in America3,4
had important personal relationshipswith industry, serving as consultants,
members of scientific advisory boards,and paid speakers. With regard to theintegrity of decision making, however,the resultant risks were slow to beappreciated.
Only recently have academicmedical centers and professional so-cieties begun to address, in a system-atic way, the core issue—thetemptation of physicians to deviatefrom their professional obligations foreconomic or other personal gain2,3,5,6.Gradually, it became clear that thepresence of self-interest associatedwith sponsored research substantiallydistorts how individuals makechoices—in the clinic, in the class-room, and in the laboratory. Veryrecently, leaders of some professionalsocieties and academic medical centershave taken on the challenge of de-termining how scientific objectivitycan be maintained in the face ofpotentially compromising relation-ships ensuing from grants, royalties,and equity holdings provided to in-dividual investigators and to academicinstitutions7-14.
Despite some early efforts at self-regulation, the complications associatedwith the industry-physician partnershipbecame so severe in the early 2000sthat the Department of Justice enteredcriminal conspiracy complaints againstfive orthopaedic medical device com-panies, alleging violations of the FederalAnti-Kickback Statute. The governmentaccused the companies of ‘‘using con-sulting agreements with orthopedicsurgeons as inducements to use a par-ticular company’s artificial hip and kneereconstruction and replacement prod-ucts.’’15 Furthermore, the investigationrevealed that it was common practiceacross America, from the late 1990sthrough 2006, for physicians, whoperformed work of little or no value, tobe rewarded with consulting contracts,lavish trips and other perquisites15. Inaddition, it found that physician con-sultants failed to disclose the existenceof their relationships to the centerswhere the surgeries were performed andto the patients who were under theircare.
Compliance in the Wake of the ‘‘BigFive’’ Nonprosecution and DeferredProsecution AgreementsIn 2007, Zimmer, DePuy Orthopae-dics, Biomet, Smith and Nephew, andStryker Orthopaedics (a division ofHowmedica Osteonics) were identifiedby the U.S. Department of Justice asproviding improper financial incentivesto orthopaedic surgeons to induce theirselection of hip and knee devices. Toavoid criminal prosecution, these com-panies entered into nonprosecution anddeferred prosecution agreements pur-suant to which they agreed to eighteenmonths of federal monitoring to ensuretheir implementation of corporatecompliance procedures. Because thesecompanies together account for nearly95% of the market for hip and kneesurgical implants16, this innovativeprosecutorial arrangement sought tochange the way an entire industry didbusiness.
Alleged violations of the FederalAnti-Kickback Statute17 were the basis ofthis unprecedented industry-wide en-forcement effort. The companies hadbeen accused of providing financialinducements to orthopaedic surgeonsthrough consulting agreements and di-rect financial perquisites. At the crux ofthese allegations was the underlyingconflict of interest that the Anti-KickbackStatute is designed to prevent: the con-flict between what is in the surgeon’sfinancial interest and what is in the bestinterest of the patient.
The nonprosecution and deferredprosecution agreements have nowended, successfully marking a new erafor the orthopaedic device industry. Asthe federal monitor for Smith andNephew, one of us (D.S.) personallyobserved the important complianceimprovements and industry transfor-mation achieved by this processthroughout 2007 to 2009. The strictcompliance measures mandated by thenonprosecution and deferred prosecu-tion agreements in areas of (1) de-termination of the need for health-careprofessional consultants, (2) paymentsto health-care professional consultants,(3) disclosure and transparency
766
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY

regarding financial arrangements withhealth-care professionals, and (4) com-pliance training and hotline reportinghave all fostered an industry-wideculture of improved compliance andaccountability. Of course, whether theindustry will continue on this positivepath remains to be seen, but thestructural sea changes have occurredand corporate policies are in place toensure continued success.
Although the nonprosecution anddeferred prosecution agreements pro-cess explicitly applied directly to onlythe companies, the unacceptable trans-actions and relationships that were thesubject of the federal proceeding alwaysinvolved two parties: a company anda professional. Now with the expirationof the nonprosecution and deferredprosecution agreements, the health-care professional side of the arrange-ment will continue to be addressed. Itis certain that public scrutiny is farfrom over because, as stated by DavidRothman, PhD, professor at ColumbiaUniversity and president of ColumbiaUniversity’s Institute on Medicine asa Profession, ‘‘the rules of the game havechanged.’’18 The Department of Healthand Human Services Office of InspectorGeneral will expand enforcement effortsby targeting individual orthopaedicphysicians who are as culpable asmedical device companies for enteringinto illegal arrangements18, and theseexpanded enforcement efforts will likelyresult in negative public perception as tothe professional side of the subjectrelationships. Now that device manu-facturers have been identified and theircompliance practices have substantiallyimproved, there is a new challenge tocounter any negative public view andbuild on the progress achieved withinthe past eighteen months. To do this,it is imperative that physicians adoptand follow the strictest policies andcodes of ethics regarding their interac-tions with the industry to avoidboth actual and apparent conflicts ofinterest.
Inappropriate interactions be-tween physicians and the medical de-vice and pharmaceutical industries
have threatened scientific integrity anddiminished the public trust. Whilemuch progress has been achieved, inthis environment of welcome scrutinyand awareness—where a hotline reportcan result in a full investigation orwhistle-blower suit—physicians mustbe increasingly sensitive to publicperception and be proactive in theirapproach to compliance to avoid sus-picion and to maintain the integrity ofthe profession and its relationship withpatients and its work products. Thisrequires adherence to the most strin-gent codes of ethics and conflict-of-interest policies, particularly those thataim to avoid the appearance of im-propriety by placing reasonable re-straints on physician-industryinteractions.
Throughout the deferred prose-cution agreement process, a number ofhotline reports concerning medical de-vice company interactions with health-care professionals were received. Theyranged from allegations of nepotism tothe providing of a free boat, expensivemeals, basketball tickets, and a day ofpheasant shooting. While it may beargued that these kinds of activities arede minimis and could not possibly resultin any inducement to use a certainproduct, such an argument appears tobe at odds with current opinion.
Several recent studies have dem-onstrated that offerings such as freelunches, subsidized trips, and evensmall gifts may influence a surgeon’smedical judgment19. Physicians them-selves have cited these studies and haveproposed the adoption of much stricterlimitations on interactions with thepharmaceutical and medical device in-dustries. For instance, on April 2, 2009,a group of physicians issued a specialcommunication in the Journal of theAmerican Medical Association that, inpart, advised medical associations tomove toward a complete ban on in-dustry funding20. The reasoning for thisstringent and progressive proposal isthat current policies are not adequatelydetailed to prevent real or apparentundue influence or bias and that lackof strong uniform controls threatens
to undermine the reputation of theprofession.
The movement to adopt morestringent policies is in direct response toincreasing public concern over physi-cian conflicts of interest caused byindustry ties and is consistent with anoverall trend to further regulate andcontrol physician-industry interactions.The AAMC has recommended strictconflict-of-interest policies that placelimitations on faculty-industry rela-tionships21. Institutions such as JohnsHopkins22 and Partners HealthCare23
(a system that consists of Harvard-affiliated facilities such as MassachusettsGeneral Hospital and Brigham andWomen’s Hospital) have recentlyannounced more stringent conflict-of-interest policies that restrict physician-industry ties. There have also beenrecent legislative initiatives such asa Massachusetts law requiring pharma-ceutical and device manufacturers toadhere to a strict marketing code ofconduct24; the Massachusetts law alsomandates disclosure of informationrelated to pharmaceutical and devicemanufacturers’ financial arrangementswith health-care professionals, as doesa recently announced policy of theStanford University School of Medi-cine25 and a recently proposed federallaw 26.
Stringent policies such as thosesuggested in the Journal of the AmericanMedical Association proposal and ad-vanced in other recent initiatives estab-lish bright-line rules to avoid bothactual and perceived conflicts of interestand, ultimately, allegations of illegality.Courts have widely held that, regardlessof best intentions, if merely even onepurpose of an arrangement is to inducefederal health-care program referrals,the Anti-Kickback Statute is violated27-30.The determination of intent or purposeis highly subjective; what is a kickbackto one may not be a kickback to another.Without strict rules that seek to avoidappearances of impropriety, it is diffi-cult to consistently determine theboundaries of acceptability in physician-industry interactions, particularly inareas such as the provision of gifts,
767
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY

entertainment, meals, and hospitality;the existence or extent of inducement touse a particular product will dependon the circumstances and individualsinvolved.
To address the inherent subjec-tivity regarding physician-industry in-teractions and overcome the publicstigma, physicians should adopt theapproach taken in the Journal of theAmerican Medical Association proposaland other recent initiatives to adhere tothe strictest codes of ethics and conflict-of-interest policies. The revised Adva-Med (Advanced Medical TechnologyAssociation) Code of Ethics on In-teractions with Health Care Profes-sionals31 serves as a useful standard thataims to avoid negative perceptions. Forexample, its recommendations include(1) placing a blanket prohibition on theprovision of entertainment (includingactivities such as theater, sportingevents, and hunting); (2) setting forthstricter limitations on the provision ofmeals in terms of purpose and settingor location; and (3) prohibiting gifts,other than the occasional provision ofitems that benefit patients or servea genuine educational function and—except for medical textbooks or ana-tomical models used for educationalpurposes—have a fair market value ofless than $100; notably, unlike theprevious AdvaMed Code, the revisedCode does not permit any type ofnoneducational branded promotionalitem, even if such an item is of minimalvalue and related to the health-careprofessional’s work or for the benefit ofpatients (such as pens, notepads, andmugs).
Physicians should strongly con-sider adopting even stricter policies,such as a complete prohibition on theacceptance of industry gifts regardlessof purpose or value. In addition,although it would not appear to beprohibited under the AdvaMed Codefor a health-care professional to attenda baseball game with a sales represen-tative if the health-care professional ispaying his or her own way, it may beregarded as inappropriate by others. Toavoid any perception of impropriety,
these kinds of situations should beavoided.
The orthopaedic device industryhas made considerable progress towardinstilling a commitment to compliance;however, the public perception of theintegrity of the profession is still at risk,and there is a long way to go to elevatethe industry’s reputation.
The Duty Proposition: How FinancialEntanglements Can Blur theDistinction Between Tradeand ProfessionGuided by the Department of Justice,industry has made progress over thepast few years toward managing con-flicts effectively. Many surgeons, onthe other hand, continue to defenda culture of entitlement and exception32,a defense that is increasingly ineffectiveagainst a public perception of greedydoctors perpetuated by the lay press.Headlines of major newspapers high-light financial payments from industryto physicians, without a balanced ex-planation of context33. Public trust hasbeen eroded further by headlines link-ing profit motives to the provision ofcare. For instance, an article entitled ‘‘AnOperation to Ease Back Pain Bolstersthe Bottom Line, Too’’ states that ‘‘inthe absence of better data, critics in thefield point to a different reason for thefusion operation’s fast rise: money.’’33
Another article quotes a patient whowarned, ‘‘When an orthopedist says youneed surgery and you are in terriblepain, you assume he is right. . . . Thinklong and hard.’’34 It has become in-creasingly clear that, in the context offinancial conflicts, damaged perceptionmatters more than nuanced reality.
At its core, the clinical relation-ship of physician and patient is a re-ciprocal ‘‘clinical fidelity.’’35 Patientsshare sensitive information with theirdoctors, rely on advice provided, andcomply with treatments recommended.In exchange, they expect undividedloyalty from their physicians. In a vul-nerable state of sickness, patients yearnto believe that their doctors are caringprofessionals—practitioners whomaintain their patients’ well-being
ahead of conflicting self-interest andthe interest of any other party 35. In anera when orthopaedic surgeons earnmore by performing surgery than bytreating patients nonoperatively, thechoice of providing advice to patientsregarding surgery compared with theact of performing the procedure con-stitutes a fundamental conflict. Yet,solutions that call for the separationof the decision-making process fromthe surgery itself are not feasible36-38.A more appropriate outcome wouldhave physicians reengage in medicineas a profession, not as a trade—a goalthat is facilitated by distancing patient-care decisions, as much as possible,from extraneous financialarrangements39.
Tainted ScienceIndustry funding in orthopaedics isstrongly associated with favorableoutcomes, even for the scientific goldstandard of randomized clinical trials.Results are favorable to the implantmanufacturer in 73% of industry-sponsored studies compared with 44%of independent studies40 (odds ratio,3.3; 95% confidence interval, 2.4 to4.5) for spine implants; 93% and 37%,respectively, for hip implants; and75% and 20% for knee implants41. Apattern of results favorable to thestudy sponsor is also observed moregenerally in biomedical research.Structured reviews of published stud-ies have shown a results bias favoringthe sponsor, with an odds ratio of 8.0(95% confidence interval, 1.1 to 53.2)for studies funded by drug manufac-turers, 3.6 (95% confidence interval,2.6 to 4.9) for studies funded bybiomedical suppliers, and 5.3(95% confidence interval, 2.0 to 14.4)for studies funded by for-profitorganizations42.
True innovation deserves to berewarded. The long process from con-cept to prototype, to investigationaldevice, to device approval, and to thedelivery of the device to the marketplacedepends on the personal drive andsacrifice of the inventor and the riskborne by the sponsor. Federal granting
768
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY
agencies and foundations rarely supportthe process. Successful innovation de-serves financial reward limited by mar-ket valuation rather than arbitrarythresholds. The problem is that trueinnovation is rare.
A report by the National In-stitute for Healthcare ManagementResearch and Educational Foundationanalyzed 1035 new drug applicationsapproved by the U.S. Food and DrugAdministration between 1989 and200043. Of those drugs, 361 (35%)had a new active ingredient, but 674(65%) had an active ingredient thatwas already marketed; 558 (54%)offered the ingredient in a differentdosage route of administration ora combination with other drugs; and116 (11%) had the identical productalready available. The average priceof a new version was twice the price ofthe older version. Device innovationmay be even more rare—with pro-liferation of ‘‘me too’’ products flood-ing the market with each new deviceapproval.
Myths and False BeliefsSocial science research has providedimportant principles related to financialconflicts of interest. We are all subject toself-serving bias44. When individualshave a stake in the outcome, they tendto weigh arguments differently than if
the outcome is independent of personalgain45.
The first myth is that conflicts ofinterest are avoidable. Conflicts ofinterest are unavoidable. There areinherent conflicts between professionalvalues and self-interest. Routine activ-ities such as recommending tests orprocedures have a conflict of interest ifthe recommending physician is alsoperforming the same tests and pro-cedures (Table I). Recommendingparticipation in a clinical trial is oftenassociated with being paid for referringpatients to the trial. Support for re-search can be contingent on furtherfunding only if positive results areproduced. Writing prescriptions fordrugs often leads to a courtship by thedrug company. Using a specific productis often associated with receiving giftsor being paid by the company. Theseare intrinsic conflicts associated withmedical practice. Unavoidable intrinsicconflicts include the desire to obtainnoteworthy findings, the desire topublish in academic journals, the needto increase the number of researchpublications, and the ambition toadvance a national reputation46. Facultyin academic centers often seek toadvance their careers, vindicate intel-lectual biases, receive accolades frompeers, and win research prizes. There isalso satisfaction in being the first tofulfill the promise of a new procedure.These are some of the intrinsic un-
avoidable conflicts associated withresearch.
The second false belief is that biasis a deliberate choice. Bias is nota deliberate choice. Deliberate mis-representation of data and findings isfraud47. Fraud is rare, but self-servingbias is pervasive. It affects individualsin their evaluations of themselves.Individuals often overestimate theirown contribution to joint tasks48. Theabove-average effect, where morethan half of the individuals rate them-selves within the top 50%, has beenidentified in ethics discussions, mana-gerial adeptness, productivity, andhealth administration. Success is oftenattributed to skill, and failure, to badluck48.
Individuals manifest differentnotions of fairness49. When workinghard is compared with working longhours, the individuals who workmore generally believe they shouldearn more and those who workless believe they should be paidequally45.
The third false belief is that thebiasing effects of gifts can be controlled.In a study of physicians, 76% believedstrongly that drug advertisements andsales personnel were minimally impor-tant in influencing their prescribinghabits, yet 49% changed their prescrib-ing habits on the basis of drug pro-motions50. This discrepancy suggestseither an unwillingness to admit in-
TABLE I Conflict of Interest
Ethical orProfessional
Interest Self-Interest
Recommendingtests or procedures
Performing thesame tests orprocedures
Recommendingparticipation in aclinical trial
Being paidfor referringpatients to aclinical trial
Support for research Further fundingonly if positiveresults
Writing prescriptionsfor drugs
Being courtedby the company
Using a specificproduct
Receiving giftsor being paidby the company
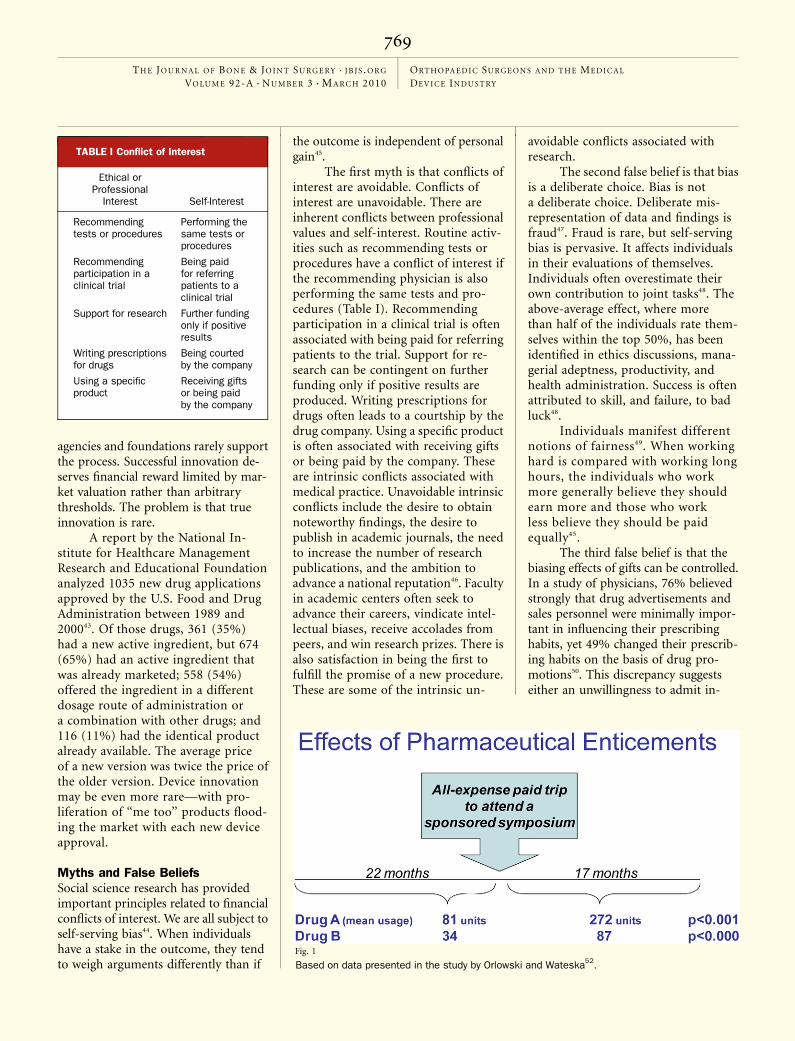
Fig. 1
Based on data presented in the study by Orlowski and Wateska52.
769
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY

fluence or a lack of awareness ofinfluence.
The biasing effect is also prom-inent among physicians who attendsponsored lectures. After attendinggrand rounds sponsored by a drugcompany, the medical residents pre-scribed the company’s drug favorably,with an odds ratio of 8.4 (95% confi-dence interval, 2.1 to 38.9)51. They alsoprescribed inappropriately, with anodds ratio of 7.8 (95% confidenceinterval, 1.6 to 45.5). There was nodifference in drug choice between thosewho remembered the sponsor and thosewho did not.
Some physicians strongly believethat attending a sponsored symposiumdoes not influence them. Recent find-ings of the effects of paid attendance ata conference have indicated, however,that the prescription of drugs increasedfrom eighty-one units in the twenty-twomonths preceding a conference to 272units in the seventeen months followingthe conference52. Study of another drugshowed that prescriptions changedfrom thirty-four units in the precedingtwenty-two months to eighty-sevenunits in the subsequent seventeenmonths (Fig. 1).
The fourth myth is that small giftsdo not matter. Social science researchhas shown that what is considered
inappropriate depends on the individ-ual’s perspective. In one study, 85% ofmedical students believed that it wasinappropriate for a public official toaccept a $50 gift from a contractor;however, only 46% of the medicalstudents believed it was inappropriatefor one of them to accept a $50 gift froma drug firm53. Nearly all (97%) of nursepractitioners thought it was inappro-priate for a public official to accept a giftfrom a contractor, and most (64%)thought it was inappropriate for amedical student to accept a gift froma drug company. Only 30%, however,believed that it was inappropriate fora nurse practitioner to accept a $50gift from a drug company 53.
Physicians and patients have dif-ferent attitudes toward gifts. Patients aremore likely than physicians to considergifts as inappropriate and influential.Even small gifts, such as trips, dinners,pocket knives, lunches, mugs, drugsamples, textbooks, pens, and videos,are more often considered inappropri-ate and influential by patients than byphysicians (Table II)54.
The fifth false belief is that bias isrecognizable. Bias is difficult to recog-nize. In a survey of resident physicians,61% stated that industry promotionsand context did not influence their ownprescribing, but only 16% believed that
other physicians were similarly unaf-fected55. Every medical resident whoconsidered lunches and pens inappro-priate had accepted these gifts55. Thedifference shows inconsistency in phy-sician attitudes of self compared withothers.
The sixth false belief is thateducation reduces bias. Social scienceresearch has shown that awareness andknowledge about the biasing effect ofgifts do not lead to a reduction in theeffects of gifts44,56.
Limits of DisclosureDisclosure, as a method for managingconflicts, has limitations. An underlyingfundamental problem, termed morallicense, holds that, like confession,disclosure provides the surgeon investi-gator a feeling of absolution withoutcleansing the potentially tainted mes-sage56. Disclosure creates the false im-pression that biased advice is fair play.Professional medical associations oftenpay lip service to disclosure throughunenforced and ineffective policies;members participating in the meetingsfrequently treat it casually as an oblig-atory burdensome step. Despite stan-dards of professionalism establishedby the American Academy of Ortho-paedic Surgeons (AAOS), the programfor the 2007 Annual Meeting disclosedonly 71.2% (245) of 344 paymentsreported by the five arthroplasty im-plant manufacturers on their web sites.While the AAOS program disclosuresdid not include dollar amounts, in-dustry web sites provided more detailedinformation, indicating that forty-sevenconsultants were paid over $1 milliona year57-62. Christopher J. Christie Jr.,when he was U.S. Attorney for theDistrict of New Jersey, stated franklythat the target would be shifted fromindustry squarely to the orthopaedicsurgeon: ‘‘I’ve dealt with the supplyissue, now I need to deal with thedemand issue.’’63 Legal action and ex-ternal policing of this sort indicates howwe and how our professional associa-tions may have failed to protect thehealth of the public and the integrityof the profession.
TABLE II Attitudes of Patients and Physicians Toward Gifts*
Inappropriate (%) Influential (%)
Gift Patients Physicians Patients Physicians
Trip 59 75 56 42
Dinner 47 33 48 24
Pocketknife 38 49 28 12
Lunch 23 10 29 12
Mug 23 18 31 8
Drug sample 22 26 42 55
Major textbook 20 29 38 10
Pen 19 4 31 8
Video 18 12 38 22
Small textbook 16 17 37 9
*Based on data in the study by Gibbons et al.54.
770
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY

In a concept described as an-choring, individuals have difficulty un-learning, ignoring, or suppressing theuse of knowledge even if, subsequently,it becomes apparent that the data areinaccurate56. When evidence on whichbeliefs are made is discredited, thebeliefs do not revert to their originalstate. They show the persistent effectsof the discredited evidence. This phe-nomenon has been described as the‘‘curse of knowledge’’ or the ‘‘failureof evidentiary discreditation.’’56
The Association of AmericanMedical Colleges RecommendationsThe AAMC published guidelines tofacilitate the development of institu-tional policies related to financialconflicts64,65. The guidelines offer prin-ciples for examining and redesigningrelationships with industry to conformto standards of medical professional-ism. A report, issued in February 2008,entitled ‘‘Protecting Patients, Preserv-ing Integrity, Advancing Health: Ac-celerating the Implementation of COIPolicies in Human Subjects Research’’called on all medical schools and majoruniversities to develop and implementconflict-of-interest policies within twoyears66.
While orthopaedic surgeons arerequired to work closely with the deviceindustry for research and product in-novation, industrial sponsorship of re-search differs from federal funding inseveral important ways. The subject ofresearch in federal funding is typicallyfundamental science, whereas the sub-ject for industry funding is product-based science. The application processfor federal funding is complex com-pared with, typically, a simple one totwo-page proposal for many industrialgrants. The application review process ispeer review for federal funding andbusiness review for industry funding.The degree of difficulty in obtainingfunding is different. Federal funding iscompetitive, and industry funding istypically noncompetitive. Responsetime to the funding application isprolonged in federal grants comparedwith a rapid review and response in
industry support. The contact betweenthe sponsor and researcher is rare infederal support, whereas it is frequentin industry support. The timing foraccrual of research data is not typicallyspecified in federal funding, whereasit can be discreetly specified in industryfunding. Access to all research datafor all study sites is usually not re-stricted in federal funding. Typically, itis very restricted in industry funding.The relationship between a sponsorand the study findings is disinterestedfor federal funding, whereas thesponsor is typically invested in theresearch outcomes for industry fund-ing. Other factors include differencesin protected time for researchers andinvestigators, salary support for in-vestigators, and the ability to usefunding for academic promotion oracademic reputation.
Policies related to research activ-ities have typically not addressed com-mon relationships between investigatorsand sponsors. Investigators frequentlyreport direct payments from industry,holding office in the company, orreceiving gifts from sponsors. However,these types of activities are rarelyaddressed in institutional policies64,65,67.Our professional associations must de-velop methods of providing clinicalcontext for device manufacturers whileshielding individual patient-care deci-sions from undue commercial influ-ence. Options include the developmentof scientific review processes for thedistribution of industry research andeducation funds, the creation of regis-tries to measure end results of im-planted devices, and the provision oftransparent taxation mechanisms toallow device manufacturers to sponsorthe development of continuing educa-tion courses.
International Committee of MedicalJournal Editors RecommendationsThe International Committee of MedicalJournal Editors (ICMJE) published uni-form requirements for manuscriptssubmitted to biomedical journals68.These requirements are aimed to protectthe integrity of the research process and
the investigators. They require that theinvestigators retain access to all trial data,control all editorial and publicationdecisions, and fully disclose the role ofthe sponsor. ICMJE has advocated fora ‘‘‘rebuttable presumption’ standard bywhich an investigator is presumed to beineligible to conduct human subjectsresearch in which he or she has a signif-icant financial interest, unless that in-vestigator is uniquely qualified to do so,
TABLE III International Committee
of Medical Journal Editors
Uniform Disclosure
Requirements for Potential
Conflicts of Interest*
1. Board membership
2. Consultancy
3. Employment
4. Expert testimony
5. Gifts
6. Grants and/or grants pending
7. Honoraria
8. Payment for manuscript preparation
9. Patents (planned, pending, or issued)
10. Royalties
11. Payment for development ofeducational presentations includingservice on speakers’ bureaus
12. Stock and/or stock options
13. Travel and/or accommodationexpenses covered or reimbursed
14. Other (err on the side of fulldisclosure)
*According to Drazen et al.71, disclosureapplies to financial and nonfinancialrelationships involving the author, insti-tution, spouse or partner, and childrenunder eighteen years of age. Any per-sonal, professional, political, institutional,religious, or other associations that areasonable reader would want to know inrelation to the submitted work, includingall sources of revenue and any entitythat could broadly be considered rele-vant for the thirty-six months prior tosubmission of the work, and all rela-tionships outside the thirty-six-monthwindow that readers may want to knowand could reasonably criticize an authorfor not disclosing. Public funding sources,such as the National Institutes of Healthor the Medical Research Council, neednot be disclosed.
771
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY
and even then, only under carefullymonitored conditions.’’69 The ICMJE hasalso introduced uniform requirementsfor disclosure70-73. While dollar amountsare not required, sponsors are identifiedfor fourteen explicit categories of finan-cial support (Table III)70-72,74.
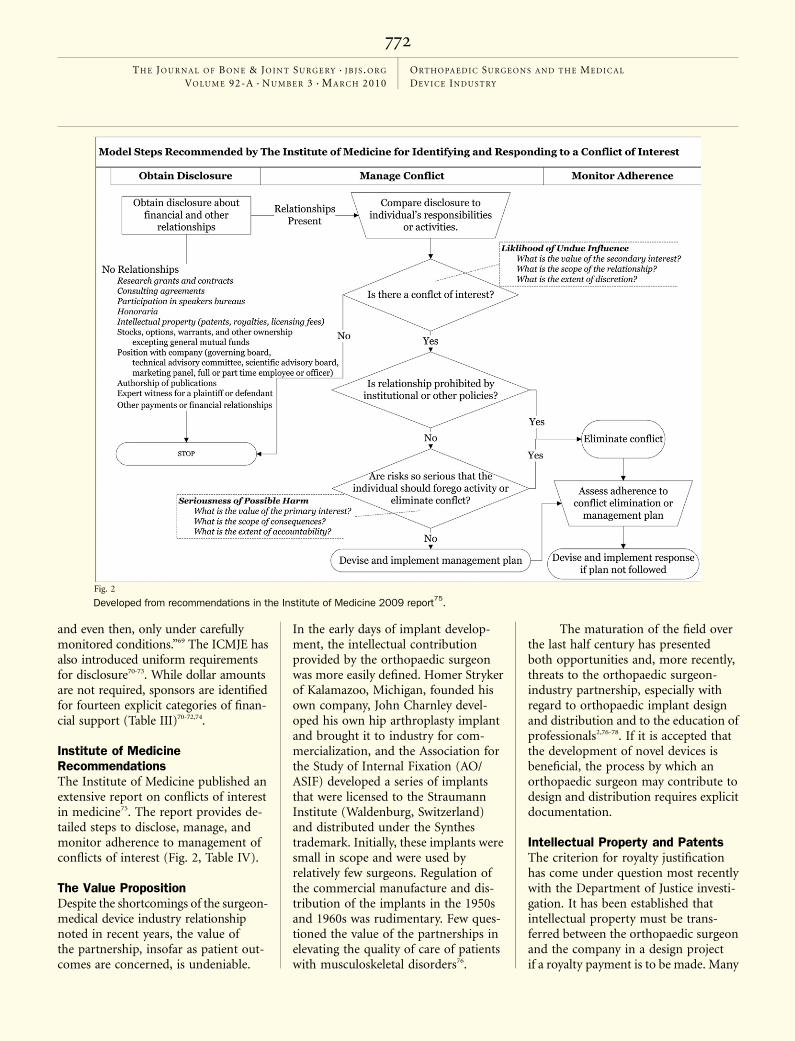
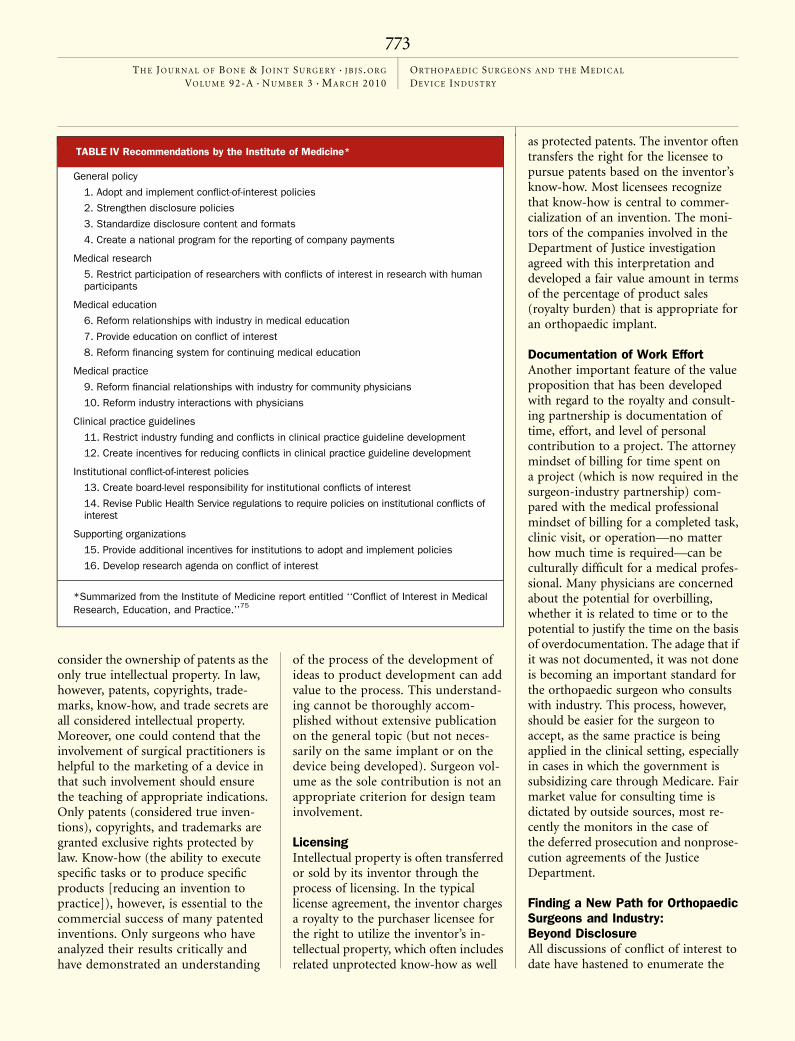
Institute of MedicineRecommendationsThe Institute of Medicine published anextensive report on conflicts of interestin medicine75. The report provides de-tailed steps to disclose, manage, andmonitor adherence to management ofconflicts of interest (Fig. 2, Table IV).
The Value PropositionDespite the shortcomings of the surgeon-medical device industry relationshipnoted in recent years, the value ofthe partnership, insofar as patient out-comes are concerned, is undeniable.
In the early days of implant develop-ment, the intellectual contributionprovided by the orthopaedic surgeonwas more easily defined. Homer Strykerof Kalamazoo, Michigan, founded hisown company, John Charnley devel-oped his own hip arthroplasty implantand brought it to industry for com-mercialization, and the Association forthe Study of Internal Fixation (AO/ASIF) developed a series of implantsthat were licensed to the StraumannInstitute (Waldenburg, Switzerland)and distributed under the Synthestrademark. Initially, these implants weresmall in scope and were used byrelatively few surgeons. Regulation ofthe commercial manufacture and dis-tribution of the implants in the 1950sand 1960s was rudimentary. Few ques-tioned the value of the partnerships inelevating the quality of care of patientswith musculoskeletal disorders76.
The maturation of the field overthe last half century has presentedboth opportunities and, more recently,threats to the orthopaedic surgeon-industry partnership, especially withregard to orthopaedic implant designand distribution and to the education ofprofessionals2,76-78. If it is accepted thatthe development of novel devices isbeneficial, the process by which anorthopaedic surgeon may contribute todesign and distribution requires explicitdocumentation.
Intellectual Property and PatentsThe criterion for royalty justificationhas come under question most recentlywith the Department of Justice investi-gation. It has been established thatintellectual property must be trans-ferred between the orthopaedic surgeonand the company in a design projectif a royalty payment is to be made. Many
Fig. 2
Developed from recommendations in the Institute of Medicine 2009 report75.
772
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY
consider the ownership of patents as theonly true intellectual property. In law,however, patents, copyrights, trade-marks, know-how, and trade secrets areall considered intellectual property.Moreover, one could contend that theinvolvement of surgical practitioners ishelpful to the marketing of a device inthat such involvement should ensurethe teaching of appropriate indications.Only patents (considered true inven-tions), copyrights, and trademarks aregranted exclusive rights protected bylaw. Know-how (the ability to executespecific tasks or to produce specificproducts [reducing an invention topractice]), however, is essential to thecommercial success of many patentedinventions. Only surgeons who haveanalyzed their results critically andhave demonstrated an understanding
of the process of the development ofideas to product development can addvalue to the process. This understand-ing cannot be thoroughly accom-plished without extensive publicationon the general topic (but not neces-sarily on the same implant or on thedevice being developed). Surgeon vol-ume as the sole contribution is not anappropriate criterion for design teaminvolvement.
LicensingIntellectual property is often transferredor sold by its inventor through theprocess of licensing. In the typicallicense agreement, the inventor chargesa royalty to the purchaser licensee forthe right to utilize the inventor’s in-tellectual property, which often includesrelated unprotected know-how as well
as protected patents. The inventor oftentransfers the right for the licensee topursue patents based on the inventor’sknow-how. Most licensees recognizethat know-how is central to commer-cialization of an invention. The moni-tors of the companies involved in theDepartment of Justice investigationagreed with this interpretation anddeveloped a fair value amount in termsof the percentage of product sales(royalty burden) that is appropriate foran orthopaedic implant.
Documentation of Work EffortAnother important feature of the valueproposition that has been developedwith regard to the royalty and consult-ing partnership is documentation oftime, effort, and level of personalcontribution to a project. The attorneymindset of billing for time spent ona project (which is now required in thesurgeon-industry partnership) com-pared with the medical professionalmindset of billing for a completed task,clinic visit, or operation—no matterhow much time is required—can beculturally difficult for a medical profes-sional. Many physicians are concernedabout the potential for overbilling,whether it is related to time or to thepotential to justify the time on the basisof overdocumentation. The adage that ifit was not documented, it was not doneis becoming an important standard forthe orthopaedic surgeon who consultswith industry. This process, however,should be easier for the surgeon toaccept, as the same practice is beingapplied in the clinical setting, especiallyin cases in which the government issubsidizing care through Medicare. Fairmarket value for consulting time isdictated by outside sources, most re-cently the monitors in the case ofthe deferred prosecution and nonprose-cution agreements of the JusticeDepartment.
Finding a New Path for OrthopaedicSurgeons and Industry:Beyond DisclosureAll discussions of conflict of interest todate have hastened to enumerate the
TABLE IV Recommendations by the Institute of Medicine*
General policy
1. Adopt and implement conflict-of-interest policies
2. Strengthen disclosure policies
3. Standardize disclosure content and formats
4. Create a national program for the reporting of company payments
Medical research
5. Restrict participation of researchers with conflicts of interest in research with humanparticipants
Medical education
6. Reform relationships with industry in medical education
7. Provide education on conflict of interest
8. Reform financing system for continuing medical education
Medical practice
9. Reform financial relationships with industry for community physicians
10. Reform industry interactions with physicians
Clinical practice guidelines
11. Restrict industry funding and conflicts in clinical practice guideline development
12. Create incentives for reducing conflicts in clinical practice guideline development
Institutional conflict-of-interest policies
13. Create board-level responsibility for institutional conflicts of interest
14. Revise Public Health Service regulations to require policies on institutional conflicts ofinterest
Supporting organizations
15. Provide additional incentives for institutions to adopt and implement policies
16. Develop research agenda on conflict of interest
*Summarized from the Institute of Medicine report entitled ‘‘Conflict of Interest in MedicalResearch, Education, and Practice.’’75
773
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY

‘‘do nots’’ in physician relationshipswith industry7,11,14. Short of acknowl-edging the need to preserve a positiveinteraction between medicine and in-dustry, however, none have sought todefine the parameters that would char-acterize such a relationship. Such shouldalso be our task.
In order to establish the newparameters of a constructive relationshipwith industry, one first acknowledgesthat a relationship is important, if notessential, but that the current iteration isflawed. The critical error lies in the tooliberal assignment of value to casual,nonsubstantive interactions that sur-geons have with device manufacturers.More holes in an acetabular shell, a 5�increase in the screw angle of a volardistal radial plate, or an additional cross-link between spinal rods do not nec-essarily constitute material productimprovements worthy of compensation.Secondly, while some of the errors havebeen egregious, the demonization of anyrelationship with industry overshoots themark and may lead to considerable harmin the long run. Some have proposeda ‘‘zero financial interest tolerance’’ forphysicians in critical positions that relateto industry and provide potential forpersonal gain20,79,80. Elimination of in-dividuals from important tasks andgroups because they receive appropriatecompensation for critical contributionshandicaps the process and risks com-promise of the quality of the finalproduct. The contributions of those withsuch conflicts should be preserved byeffective management of the relation-ship rather than by complete dismissalof the individual. Further, it is in-cumbent on our profession to repairany perception of disrepute insofar asindustry relationships are concerned.Modifications in physician behavior arethe requisite for a healthy physician-industry relationship, framed by theneed to move beyond simple disclosurein protecting ourselves from the perilsof conflicts of interest. In the words ofDavid Korn, MD, ‘‘Disclosure is es-sential but not sufficient,’’ in charac-terizing the relationship betweenmedical professionals and industry 81.
Components of a HealthyPhysician-Industry RelationshipThe futuristic approach to the construc-tive and ethically acceptable surgeon-industry relationship is predicated onfour fundamental principles:
1. Complete Disclosure andTransparency of ConflictsAs has been articulated by some, adetailed and complete disclosure offinancial and other substantive relation-ships is the starting point81. Specificdollar amounts received from industryfor efforts related, directly or indirectly,to the matter at hand are disclosed12,82,83.This is most effectively accomplished ona web site in the public domain; indeed,most of the pertinent companies and anincreasing number of universities al-ready have such a policy. Objectivereporting, such as income noted on U.S.Internal Revenue Service form 1099,should be the basis for such declara-tions. An unwillingness to disclose suchrelationships in this manner constitutesa basis for exclusion from any relatedposition, task, or group. Moreover,surgical consent forms for an operationshould disclose the existence of suchsurgeon-industry relationships to pa-tients prior to the operative procedurebeing performed; some institutionshave already adopted such a policy andstandardized form. This provides a con-text within which every observer mayjudge the potential bias of each re-spective contributor when presenting ata meeting, publishing a paper, orparticipating in a group discussion.
2. Realistic Assessment ofActual Value AddedThe material value of a surgeon-innovator’s contribution is assessed bysome dispassionate third party, a groupcomprising representative individualsfrom industry as well as a medical peergroup. It is anticipated that there will befar fewer substantive compensable con-tributions as a result of this process.Likewise, it is assumed that this will bethe cornerstone of a more credible,ethical, and consistent system of rewardfor surgeon designers.
3. Objective Third-PartyDetermination of ‘‘Fair Market Value’’As the term implies, market forcesappropriately determine fair compensa-tion for intellectual property transfer andconsulting activity subsequent to a de-termination of real value added. It isexpected that the royalty load for a givenproject varies within some range de-pendent on the magnitude and impact ofeach contribution and the relative suc-cess of the product in the marketplace.Similarly, natural market forces, overseenand approved by an objective third party,should govern hourly remuneration ratesfor consulting activities. This is con-trasted with the current state, wherea predetermined hourly rate for consult-ing activities and fixed percent of royaltyload is set arbitrarily, independent ofmarket forces, by regulators who them-selves may be conflicted.
4. Removal of Linkage fromPatient-Care Decision MakingAny conflict of interest, be it real orperceived, derives from the associationof personal gain of the individualphysician with the selection of a productwhich the physician participates in oreven directs on behalf of the patient.Disclosure is no longer thought toconfer immunity to being influenced84.If the role of the physician in thedevelopment process is to be preservedbecause he or she adds value, it thenstands to reason that the triangleconnecting the physician, the patient,and the vendor must be interrupted.The physician is either dissociated fromthe patient or from industry in thistriangle; any role in device selection onbehalf of the patient or the potentialfor personal gain by the physician(through reciprocity with the vendor) iseliminated. While at first blush thedisconnection of the physician from thedecision-making process for any in-dividual patient appears contrary to thealtruistic role of the physician, manyhealth-care systems in the UnitedStates have already compromised thesurgeon’s ability to choose on behalfof the patient (e.g., by limiting implantsto those supplied by certain vendors
774
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY

chosen by the institution, most oftenbased on favorable pricing consider-ations). Common practice currentlyprecludes a royalty benefit to a design-ing surgeon based on patients cared forin the surgeon’s home institution, butsome would claim a serious conflictpersists if the surgeon’s payment re-mains correlated with the use of anyspecific implant. An alternative hybridscenario might create a third-party-administered ‘‘innovator pool’’ thatprovides a reimbursement premium tosurgeon-innovators whenever the pro-cedure in question is performed, irre-spective of which implant is used in anyparticular patient or which companymanufactured it. Under such a system,the surgeon-designer is rewarded forparticipation in the product develop-ment process in a manner not con-nected with the use of any specificdevice in any particular patient. Forexample, the predetermined ‘‘royaltyload’’ of a given device from eachmanufacturer might be paid to anindependently governed fund ratherthan to any individual designing sur-geon. The aggregate pool of royaltypayments related to surgeon-designeddevices would then be distributed toparticipating surgeon innovators on thebasis of relevant metrics such as thetime spent on projects and the successof the devices, rather than havingpayment linked to the success of anyspecific implant with which the surgeonmay be involved. This approach wouldretain a more general incentive for thesurgeon-innovator while separating thedirect surgeon link to industry; ittherefore also potentially preserves thephysician role as agent in decisionmaking for the individual patient.Likewise, the establishment of sucha ‘‘medical device tax’’ could alsoperpetuate industry sponsorship of re-search and education, considering thatthe incentive for industry to continue itssupport of such activities is diminishedby removal of its direct link to thesurgeon who makes implant-purchasingdecisions.
No matter how the surgeon-designer is removed from the conflict-of-
interest triangle (e.g., eliminating theprospect of financial gain as was thecase in the early history of implantdevelopment, or divorcing the physician-innovator from the process of deviceselection for any individual patient),there will be at least a temporary periodwhen review of these situations bya dispassionate third party (an ethicist)will add considerable value in reassuringthe public that the medical professionhas adopted an ethical and transparentapproach to relationships with industry.It is likely that there will be increasingdemand for such individuals providingcounsel to academic health centers in theyears to come. Beyond the role ofadvisor, a principal function of suchan individual might be to provide abinding review and adjudication ofconflict-of-interest disclosure as well as adetermination of the appropriate re-lationship structure between industryand physician-innovators as we moveforward.
Whatever approach is adopted toraise our profession from the presentquagmire must ensure ethical relation-ships between industry and the medicalcommunity and must restore the pub-lic trust in the treating physician ashaving the welfare of the patient as theprincipal motive. A thoughtful andreflective dialogue involving medicine,the lay public, and industry is essential.Elements of such a relationship includecomplete and full disclosure, a realisticassessment of value added, an inde-pendent determination of fair marketvalue, and elimination of any linkageof the surgeon to either specific patientdecision making or a relationship withindustry that provides for personal gain.Amid all of this, we strive to protect theethical interaction between medicineand industry that has fueled propermedical advances over the years. For allthose who partake in the discussion,nothing less than genuine altruism willbe required, as well as a clear andirrevocable understanding that whatis past has passed and the future ofall relationships with industry willlook very different. Our choice issimple; we can elect to be part of the
solution or a continuing part of theproblem.
Richard H. Gelberman, MDDepartment of Orthopaedic Surgery,Washington University School of Medicine,660 South Euclid, Campus Box 8233,St. Louis, MO 63110.E-mail address: [email protected]
David Samson, EsqWolff and Samson PC, The Offices atCrystal Lake, One Boland Drive,West Orange, NJ 07052
Sohail K. Mirza, MD, MPHDepartment of Orthopaedics,Dartmouth-Hitchcock Medical Center,One Medical Center Drive,Lebanon, NH 03756-0001
John J. Callaghan, MDDepartment of Orthopaedic Surgery,University of Iowa Health Care, 200 HawkinsDrive, 01073 JPP, Iowa City, IA 52242
Vincent D. Pellegrini Jr., MDDepartment of Orthopaedics, University ofMaryland School of Medicine, 22 South GreeneStreet, Suite S11B, Baltimore, MD 21201.E-mail address: [email protected]
References1. Leaf C. The law of unintended consequences.Fortune. 2005;152:250-2, 254, 258.
2. Campbell EG, Gruen RL, Mountford J, Miller LG,Cleary PD, Blumenthal D. A national survey ofphysician-industry relationships. N Engl J Med.2007;356:1742-50.
3. Bekelman JE, Li Y, Gross CP. Scope and impact offinancial conflicts of interest in biomedical research:a systematic review. JAMA. 2003;289:454-65.
4. Campbell EG, Weissman JS, Ehringhaus S, RaoSR, Moy B, Feibelmann S, Goold SD. Institutionalacademic industry relationships. JAMA. 2007;298:1779-86.
5. Boyd EA, Bero LA. Assessing faculty financialrelationships with industry: a case study. JAMA.2000;284:2209-14.
6. McCrary SV, Anderson CB, Jakovljevic J, Khan T,McCullough LB, Wray NP, Brody BA. A national survey ofpolicies on disclosure of conflicts of interest inbiomedical research. N Engl J Med. 2000;343:1621-6.
7. Rothman DJ. Academic medical centers andfinancial conflicts of interest. JAMA. 2008;299:695-7.
8. Johns MM, Barnes M, Florencio PS. Restoringbalance to industry-academia relationships in an eraof institutional financial conflicts of interest: pro-
775
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY

moting research while maintaining trust. JAMA.2003;289:741-6.
9. Studdert DM, Mello MM, Brennan TA. Financialconflicts of interest in physicians’ relationships withthe pharmaceutical industry—self-regulation in theshadow of federal prosecution. N Engl J Med.2004;351:1891-900.
10. Campbell EG. Doctors and drug companies—scrutinizing influential relationships. N Engl J Med.2007;357:1796-7.
11. Brennan TA, Rothman DJ, Blank L, Blumenthal D,Chimonas SC, Cohen JJ, Goldman J, Kassirer JP,Kimball H, Naughton J, Smelser N. Health industrypractices that create conflicts of interest: a policyproposal for academic medical centers. JAMA.2006;295:429-33.
12. Steinbrook R. Disclosure of industry payments tophysicians. N Engl J Med. 2008;359:559-61.
13. Abelson R. Cleveland Clinic discloses doctors’industry ties. New York Times. 2008 Dec 3;B1.
14. Ehringhaus SH, Weissman JS, Sears JL, GooldSD, Feibelmann S, Campbell EG. Responses ofmedical schools to institutional conflicts of interest.JAMA. 2008;299:665-71.
15. U.S. Department of Justice. Press release: mon-itoring and deferred prosecution agreements termi-nated with companies in hip and knee replacementindustry. 2009 Mar 30. http://www.usdoj.gov/usao/nj/press/press/files/pdffiles/hips0330%20rel.pdf. Accessed 2009 Apr 20.
16. U.S. Department of Justice. Press release: fivecompanies in hip and knee replacement industryavoid prosecution by agreeing to compliance rulesand monitoring. 2007 Sep 27. http://www.usdoj.gov/usao/nj/press/files/pdffiles/hips0927.rel.pdf.Accessed 2009 Apr 20.
17. Social Security Act, §1128, 42 U.S.C. 1320a-7b.Criminal penalties for acts involving Federal healthcare programs. 1997 Sep 23.
18. Harris G. Crackdown on doctors who takekickbacks. New York Times. 2009 Mar 4;A14.
19. Demske GE. Examining the relationship betweenthe medical device industry and physicians. Testi-mony before the Senate Special Committee on Aging.2008 Feb 27. Corrected 2008 May 22. http://oig.hhs.gov/testimony/docs/2008/demske_testimony022708.pdf. Accessed 2009 Apr 20.
20. Rothman DJ, McDonald WJ, Berkowitz CD,Chimonas SC, DeAngelis CD, Hale RW, Nissen SE,Osborn JE, Scully JH Jr, Thomson GE, Wofsy D.Professional medical associations and theirrelationships with industry: a proposal for controllingconflict of interest. JAMA. 2009;301:1367-72.
21. Association of American Medical Colleges.Industry funding of medical education: report of an AAMCtask force. 2008 Jun. https://services.aamc.org/publications/showfile.cfm?file=version114.pdf&prd_id=232. Accessed 2009 Apr 20.
22. Rubenstein S. Johns Hopkins bans free drugsamples, gifts from industry. Wall Street JournalBlogs. 2009 Apr 8. http://blogs.wsj.com/health/2009/04/08/johns-hopkins-bans-free-drug-samples-gifts-from-industry/. Accessed 2009 Apr 20.
23. Goldstein J. Harvard-affiliated hospitals to limitdocs’ industry ties. Wall Street Journal Blogs.2009 Apr 10. http://blogs.wsj.com/health/2009/04/10/harvard-affiliated-hospitals-to-limit-docs--industry-ties/. Accessed 2009 Apr 20.
24. Massachusetts Disclosure Law. Mass Gen Lawsch. 111N §§ 1-7. 2009 Jan 1.
25. Spector R. Stanford medical school to provideonline disclosure of faculty’s consulting activities.2009 Apr 1. http://med.stanford.edu/news_releases/2009/april/disclosure.html. Accessed 2009 Apr 20.
26. Physician Payments Sunshine Act of 2009.S.301, 111th Cong.
27. United States v. Greber, 760 F.2d 68 (3rd Cir.),cert. denied, 474 U.S. 988 (1985).
28. United States v. Davis, 132 F.3d 1092 (5th Cir.1998).
29. United States v. Kats, 871 F.2d 105 (9th Cir.1989).
30. United States v. McClatchey, 217 F.3d 823(10th Cir. 2000).
31. AdvaMed. Code of ethics on interactions withhealth care professionals. http://www.advamed.org/NR/rdonlyres/61D30455-F7E9-4081-B219-12D6CE347585/0/AdvaMedCodeofEthicsRevisedandRestatedEffective20090701.pdf. Accessed10 Dec 2009.
32. Callaghan JJ, Crowninshield RD, Greenwald AS,Lieberman JR, Rosenberg AG, Lewallen DG. Sympo-sium: introducing technology into orthopaedic prac-tice. How should it be done? J Bone Joint Surg Am.2005;87:1146-58.
33. Abelson R, Petersen M. An operation to easeback pain bolsters the bottom line, too. New YorkTimes. 2003 Dec 31;A1.
34. Langreth R. Operation! Is elective surgery over-done? Forbes. 2003;172:246-54.
35. Bloche MG. Clinical loyalties and the socialpurposes of medicine. JAMA. 1999;281:268-74.
36. Luft HS, Bunker JP, Enthoven AC. Shouldoperations be regionalized? The empirical relationbetween surgical volume and mortality. 1979. ClinOrthop Relat Res. 2007;457:3–9.
37. Luft HS. Health care reform—toward morefreedom, and responsibility, for physicians. N EnglJ Med. 2009;361:623-8.
38. Luft HS. Economic incentives to promote in-novation in healthcare delivery. Clin Orthop Relat Res.2009;467:2497-505.
39. Smith JW. The dignity of the medical professionis upheld. Illinois Med J. 1907;11:672-3.
40. Shah RV, Albert TJ, Bruegel-Sanchez V, VaccaroAR, Hilibrand AS, Grauer JN. Industry support andcorrelation to study outcome for papers publishedin Spine. Spine (Phila Pa 1976). 2005;30:1099-105.
41. Bhandari M, Busse JW, Jackowski D, Montori VM,Schunemann H, Sprague S, Mears D, Schemitsch EH,Heels-Ansdell D, Devereaux PJ. Association betweenindustry funding and statistically significant pro-industryfindings in medical and surgical randomized trials.CMAJ. 2004;170:477-80.
42. Lexchin J, Bero LA, Djulbegovic B, Clark O.Pharmaceutical industry sponsorship and researchoutcome and quality: systematic review. BMJ.2003;326:1167-70.
43. Changing patterns of pharmaceutical innovation.A research report by The National Institute for HealthCare Management Research and Educational Foun-dation. Washington, DC: NIHCM; 2002. http://www.nihcm.org/pdf/innovations.pdf.
44. Cain DM, Detsky AS. Everyone’s a little bit biased(even physicians). JAMA. 2008;299:2893-5.
45. Dana J, Loewenstein G. A social scienceperspective on gifts to physicians from industry.JAMA. 2003;290:252-5.
46. Sollitto S, Hoffman S, Mehlman M, Lederman RJ,Youngner SJ, Lederman MM. Intrinsic conflicts ofinterest in clinical research: a need for disclosure.Kennedy Inst Ethics J. 2003;13:83-91.
47. Scott J. Withdrawal of a paper. J Bone Joint SurgBr. 2009;91:285-6.
48. Babcock L, Loewenstein G. Explaining bargainingimpasse: the role of self-serving biases. J EconPerspect. 1997;11:109-26.
49. Messick DM, Sentis KP. Fairness and prefer-ence. J Exp Soc Psychol. 1979;15:418-34.
50. Avorn J, Chen M, Hartley R. Scientific versuscommercial sources of influence on the prescribingbehavior of physicians. Am J Med. 1982;73:4-8.
51. Spingarn RW, Berlin JA, Strom BL. Whenpharmaceutical manufacturers’ employees presentgrand rounds, what do residents remember? AcadMed. 1996;71:86-8.
52. Orlowski JP, Wateska L. The effects of pharma-ceutical firm enticements on physician prescribingpatterns. There’s no such thing as a free lunch.Chest. 1992;102:270-3.
53. Palmisano P, Edelstein J. Teaching drug pro-motion abuses to health profession students. J MedEduc. 1980;55:453-5.
54. Gibbons RV, Landry FJ, Blouch DL, Jones DL,Williams FK, Lucey CR, Kroenke K. A comparison ofphysicians’ and patients’ attitudes toward pharma-ceutical industry gifts. J Gen Intern Med. 1998;13:151-4.
55. Steinman MA, Shlipak MG, McPhee SJ. Ofprinciples and pens: attitudes and practices ofmedicine housestaff toward pharmaceutical industrypromotions. Am J Med. 2001;110:551-7.
56. Cain DM, Loewenstein G, Moore DA. The dirt oncoming clean: perverse effects of disclosing conflictsof interest. J Legal Stud. 2005;34:1-25.
57. Biomet. Company consultants—identificationand payments, 2008. http://www.biomet.com/corporate/consultant_disclosure.cfm. Accessed 2009May 12.
58. DePuy Orthopaedics. 2008 payment disclosure.http://www.depuyorthopaedics.com/Attachment%20Documents/depuydisclosure.pdf. Accessed 2009May 12.
59. Zimmer. Disclosure of U.S. hip and kneeconsultants and payments, 2007-2008. http://www.zimmer.com/web/enUS/pdf/Company_Consultants_033109.pdf. Accessed 2009 May 12.
60. Smith and Nephew. Company consultants—identification and payments. http://www.smithnephewdpacompliance.com. Accessed2009 May 12.
61. Stryker. Surgeon consultants. http://www.stryker.com/meetourconsultants/consultants/consultants.php. Accessed 2009 May 12.
62. Okike K, Kocher MS, Wei EX, Mehlman CT,Bhandhari M. Accuracy of conflict-of-interest disclo-sures reported by physicians. N Engl J Med. 2009;361:1466-74.
63. Feder BJ. Subpoenas seek data on orthopedicsmakers’ ties to surgeons. New York Times. 2005 Mar31;C12.
64. AAMC Task Force on Financial Conflicts ofInterest in Clinical Research. Protecting subjects,preserving trust, promoting progress II: principles andrecommendations for oversight of an institution’sfinancial interests in human subjects research. AcadMed. 2003;78:237-45.
776
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY
65. AAMC Task Force on Financial Conflicts ofInterest in Clinical Research. Protecting subjects,preserving trust, promoting progress I: policy andguidelines for the oversight of individual financialinterests in human subjects research. Acad Med.2003;78:225-36.
66. Association of American Medical Colleges. Pro-tecting patients, preserving integrity, advancinghealth: accelerating the implementation of COIpolicies in human subjects research. A report ofthe AAMC-AAU Advisory Committee on FinancialConflicts of Interest in Human Subject Research.Washington, DC: Association of American MedicalColleges; 2008.
67. AAMC Task Force on Financial Conflicts ofInterest in Clinical Research. Protecting subjects,preserving trust, promoting progress—policy andguidelines for the oversight of individual financialinterests in human subjects research. 2001 Dec.http://www.aamc.org/research/coi/firstreport.pdf.Accessed 2005 May 23.
68. Davidoff F, DeAngelis CD, Drazen JM, Hoey J,Højgaard L, Horton R, Kotzin S, Nicholls MG, NylennaM, Overbeke AJ, Sox HC, Van Der Weyden MB, WilkesMS. Sponsorship, authorship, and accountability.Lancet. 2001;358:854-6.
69. Cohen JJ, Siegel EK. Academic medical centersand medical research: the challenges ahead. JAMA.2005;294:1367-72.
70. Drazen JM, Van Der Weyden MB, Sahni P,Rosenberg J, Marusic A, Laine C, Kotzin S, Horton R,Hebert PC, Haug C, Godlee F, Frizelle FA, de LeeuwPW, Deangelis CD. Uniform format for disclosure ofcompeting interests in ICMJE journals. Lancet.2009;374:1395-6.
71. Drazen JM, Van Der Weyden MB, Sahni P,Rosenberg J, Marusic A, Laine C, Kotzin S, HortonR, Hebert PC, Haug C, Godlee F, Frizelle FA, deLeeuw PW, Deangelis CD. Uniform format fordisclosure of competing interests in ICMJE jour-nals. Ann Intern Med. 2009 Oct 13 [Epub ahead ofprint].
72. Drazen JM, Van Der Weyden MB, Sahni P,Rosenberg J, Marusic A, Laine C, Kotzin S, Horton R,Hebert PC, Haug C, Godlee F, Frizelle FA, de LeeuwPW, Deangelis CD. Uniform format for disclosure ofcompeting interests in ICMJE journals. JAMA.2010;303:75-6.
73. Drazen JM, Van Der Weyden MB, Sahni P,Rosenberg J, Marusic A, Laine C, Kotzin S, Horton R,Hebert PC, Haug C, Godlee F, Frizelle FA, de LeeuwPW, Deangelis CD. Uniform format for disclosure ofcompeting interests in ICMJE journals. N Engl J Med.2009;361:1896-7.
74. Drazen JM, Van Der Weyden MB, Sahni P,Rosenberg J, Marusic A, Laine C, Kotzin S, Horton R,Hebert PC, Haug C, Godlee F, Frizelle FA, de LeeuwPW, Deangelis CD. Uniform format for disclosure ofcompeting interests in ICMJE journals. CMAJ.2009;181:565.
75. Institute of Medicine. Conflict of interest inmedical research, education, and practice. A focus onmedical research. Washington, DC: National Acade-mies Press; 2009.
76. Crowninshield RD, Callaghan JJ. The orthopaedicprofession and the industry partnership. Clin OrthopRelat Res. 2007;457:73-7.
77. Heckman JD. Patient care, professionalism, andrelationships with industry. J Bone Joint Surg Am.2008;90:225.
78. Khan MH, Lee JY, Rihn JA, Cassinelli EH, LimMR, Kang JD, Donaldson WF 3rd. The surgeon asa consultant for medical device manufacturers:what do our patients think? Spine (Phila Pa 1976).2007;32:2616-8.
79. The Blue Ridge Academic Health Group. Manag-ing conflict of interest in AHCs to assure healthyindustrial and societal relationships. Report 10. 2006Sep. http://whsc.emory.edu/blueridge/_pdf/blue_ridge_report_10_2006sep.pdf. Accessed 2009May.
80. National Institutes of Health. Frequently askedquestions. Responsibility of applicants for promotingobjectivity in research for which PHS funding is sought(42 CFR Part 50 Subpart F, grants; and responsibleprospective contractors, 45 CFR Part 94, contracts).http://grants.nih.gov/grants/policy/coifaq.htm.Accessed 2009 Mar.
81. Korn D. Council of Academic Societies workshop:academic and scientific society interactions withindustry. 2007 Nov 2. Washington, DC.
82. Steinbrook R. Online disclosure of physician-industry relationships. N Engl J Med. 2009;360:325-7.
83. Steinbrook R. Physician-industry relations—willfewer gifts make a difference? N Engl J Med. 2009;360:557-9.
84. Association of American Medical Colleges. Thescientific basis of influence and reciprocity: a sympo-sium. Korn D, Ehringhaus S, editors. 2007 Jun 12.https://services.aamc.org/publications/showfile.cfm?file=version106.pdf&prd_id=215&prv_id=262&pdf_id=106. Accessed 2009 May.
777
TH E J O U R N A L O F B O N E & JO I N T SU R G E RY d J B J S . O R G
VO LU M E 92-A d NU M B E R 3 d M A R C H 2010ORT H O PA E D I C SU RG E O N S A N D T H E ME D I C A L
DEV I C E IN D U S T RY