Identification/Demographic Data
Name: Mr. Ariyono Sukat
Age: 41 years old
Sex: Male
Race: Indonesian
Status: Single
Address: Sibu, Sarawak
Date of admission: 23 March 2015
Chief Complaint
Mr. Ariyono was admitted to Hospital Sibu on 23rd March 2015 for
pain and open wounds on his right leg due to alleged workplace
accident.
History of Presenting Illness
Mr. Ariyono, a 41-year old Indonesian gentleman was admitted to
the ward with complaint of pain at the right leg due to alleged
workplace accident. He claimed that both his leg was caught in a
wood cutting machine. He was not wearing any personal protective
equipment as required during the time of the accident. He tried to
pull out his leg but did not managed to do so. The stopped the
machine and immediately brought him to the hospital via car. He
said there was severe pain which is more at his right leg. He also
noticed bleeding but was not sure of the amount. They also had
previously bandaged him at the factory with a cloth to stop the
bleeding. He also said that his bones can be seen along with his
muscles. He was not able to ambulate and also did not have loss of
consciousness. Otherwise, he does not have any other injury and no
nausea or vomiting also.On admission at emergency department, there
was 2 open wound seen on his right leg with bleeding. The wound was
over the medial aspect of the right tibia. Sensation was also
intact. His vital signs was also stable on admission. X-rays show
tibia and fibula fracture on his right leg.Currently, he underwent
immediate surgical operation after admission which was wound
exploration, debridement, external fixation and muscle repair. He
is also afebrile and unable to ambulate. There was no dysuria and
no hematuria. He also underwent blood transfusion twice since his
admission.
Past medical history This was his first admission to hospital.
There is no relevant past medical history. Past surgical
historyThere is no relevant past surgical history.Drug historyNo
known drug allergy. Does not taking any traditional drugs.Family
historyBoth parents are alive and well. They currently staying in
Pontianak, Indonesia. There is also no family history of malignancy
in the familyAllergy historyNo known food or drugs allergySocial
historyHe is currently in Sibu for work and send money to his
parents. He is staying in hostel with his colleague as provided by
the employee. He is also a smoker and smokes 1 pack per day for
almost 20 years. He does not drink alcohol and does not take any
illicit drugs.
PHYSICAL EXAMINATION:General Examination:He is lying
comfortably, alert and conscious. He is not septic looking or
dyspnoeic. There was a branula inserted on his left hand. His right
leg is under bandage from ankle to mid tibia level with an external
fixation.
Vital Signs:Blood Pressure- 138/76 mmHgPulse Rate - 92 beats/m
(normal volume, regular rhythm)Respiratory Rate - 19 per
minuteTemperature - 37 C
Face, head, neck & limbs examinationAppearance: Normal
placed eyes, nose and ears, no deformities of lips and nose.Shape
of head: Normal head shape.Hair: No hair loss, no bald spotFace: No
cyanosis, no pallor and no facial deformitiesOral cavity: Good oral
hygiene, moist mucous membrane, no ulcers and no central
cyanosisEyes: No pallor and no jaundice.Ear, mouth & throat: No
ear and nose discharge, no throat swelling and redness.Neck: No
thyroid enlargementSkin: pink, no rash, no lesionsImpression: No
abnormalities
SYSTEMIC EXAMINATION:Lower limbs examinationOn inspection,
patient right lower limb is seen with bandage from ankle to mid
tibia level. There was also external fixation seen on his right
leg. Meanwhile, the left leg was normal. There was no scar seen and
no other wound seen. There was also no leg length discrepancies. On
palpation of the right lower limb, there is mild tenderness over
the bandage area. Capillary refill time is less than 2 seconds.
Sensation is intact but lessen as compared to the left leg.
Dorsalis pedis artery and posterior tibial artery is palpable. On
left lower limbs, no tenderness felt and sensation was intact.
Dorsalis pedis artery and posterior tibial artery is
palpableMovement was limited due to bandage and external fixation
for his right leg. Gross movement and sensation of left lower limb
was intact.Cardiovascular system examination
On inspection, his chest moves symmetrically with
respiration.
On palpation, apex beat was felt at left 5th intercostals space,
mid-clavicular line. There was no left parasternal heaves and no
thrills at left sternal edge, pulmonary area and aortic area.On
auscultation, normal 1st and 2nd heart sound was heard. There was
no additional heart sound or murmur.
Respiratory system examination
On inspection, the chest moves symmetrically with respiration on
both sides.
On palpation, the trachea was centrally located and chest
expansion was symmetrical on both sides. On auscultation, the air
entry was adequate and equal on both sides of the lung. Normal
vesicular breath sound was heard with no abnormal sounds.
Nervous System
He is alert and cooperative with GCS score of 15. His thought is
coherent and he is oriented to person, place and time. For upper
limbs on both sides, there was good muscle bulk and tone at 5/5.
Reflex was normal on both sides. Sensation was intact. Right lower
limbs was restricted due to bandages and external fixation.
Provisional diagnosis41 years old male with open right distal
1/3 tibia and fibula fracture with Gustillo 3b open fracture.Reason
for diagnosisHis right leg was caught in a wood cutting machine.
There was two wound seen over the medial aspect of the tibia of his
leg. There was also bones and muscle flap seen from the wound with
bleeding. It was an open wound with no extensive bleeding. X-ray
shows tibia and fibula fracture of his right lower limb.
General investigationIndication: To monitor general condition of
the patient and screen the patients status and if there is any
abnormal platelet count and white blood cells count.
TestsResultUnitNormal rangeImpression
White Blood Cell 9.410^3 L2-20Normal
Red Blood Cell2.5810^6 L4.5-6Low
RBC Distribution Width35.4Fl30-100Normal
Hemoglobin7.9g/dl10-20Low
Hematocrit24.0%30-45Low
Mean Cell Hemoglobin30.6Pg27-31Normal
Mean Cell Volume93.0Fl70-86Normal
Mean Cell Hemoglobin Concentration32.5g/dl27-33Normal
Platelet count19910^3 L150-400Normal
Urea & ElectrolytesIndication: To assess the extent of
electrolytes loss that might compromise renal function
TestResultUnitNormal rangeImpression
Urea3.6mmol/L1.7-6.4Normal
Sodium140mmol/L135-150Normal
Potassium4.0mmol/L3.5-5.1Normal
Creatinine56.1umol/L27-62Normal
Chloride101.0mmol/L98.0-107.0Normal
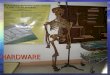
X-ray of right tibia (AP view)
The X-ray above is an anteroposterior (AP) view of the right
tibia of Mr Ariyono Sukat taken on 23rd March 2015. There is an
obvious abnormalities seen. There is an oblique fracture of both
distal 1/3 of tibia and fibula seen. The fractures are completely
displaced medially. There is also shortening seen for both tibia
and fibula. No other abnormalities seen.Impression: Distal 1/3
fracture of right tibia and fibula.
Final Diagnosis 41 years old male with open right distal 1/3
tibia and fibula fracture (Gustillo Grade IIIB)ManagementHe was
immediately sent for surgical intervention upon admission to
emergency department of Hospital Sibu. He underwent wound
exploration, debridement, external fixation and muscle repair.
Operative findings is:1. Open fracture grade IIIB of right distal
1/3 of tibia and fibula. Tibialis anterior partially cut at
musculotendinious junction.Postoperative plan1. For X-ray recheck
of right tibia and fibula.2. Continue IV Flagyl 500mg TDS and IV
Cefuroxime 750mg TDS3. Continue analgesia IV Tramadol 50mg TDS4.
Daily neurovascular charting of both lower limbs5. Elevate
bilateral lower limbs6. Allow orallyDiscussionOpen fractures of the
tibia are the commonest of open long-bone fractures, perhaps
because of its thin anteromedial soft-tissue coverage.They are
caused by various mechanisms, ranging from low-energy twisting
forces to high-energy motor vehicle crashes or penetrating injuries
(gun shots, blasts). Although the principles of management for open
tibial fractures are constant, the path to the final result may
vary.Open tibial fractures can present as isolated injuries or in
the context of a multiply injured patient. The patients clinical
status must dictate the primary and ongoing treatment of the open
tibial fracture. Thorough evaluation of the entire patient is
essential before focusing on the injured leg.Clsiification of open
fractures
Factors affecting tibial fracture managementEach aspect of an
open tibial fracture must be considered in planning initial and
definitive management. The entire patient, the injured extremity
and the specific details of the open fracture itself must each be
considered. Associated arterial injury must be identified and
treated urgently to salvage the limb. Wound debridement will be
necessary. Its thoroughness appears to be more important than how
quickly it is done. The severity of the injuries to soft tissues,
bone and neurovascular structures must be identified and used for
treatment planning.Emergency managementAs in all open fracture
injuries, the patient must receive anti-tetanus prophylaxis and
appropriate antibiotic coverage. Antibiotics should be given
intravenously as soon as possible.Generally, all open fractures are
treated with coverage for typical skin bacteria, often a 1st
generation cephalosporin. Higher grade open fracture wounds will
require additional coverage for gram-negative organisms. With soil
or barnyard injuries, high-dose penicillin should be added to cover
possible clostridial infection (gas gangrene).After initial
inspection the wound should be covered with a sterile dressing
which should not be removed until it is taken down in the OR. A
digital photograph of the wound, before dressing, will remove the
temptation for successive attendant to expose the wound for
inspection.A temporary splint may be applied to protect the soft
tissues while awaiting the availability of an operating
room.Definitive classification of the open fracture is best done in
the OR.Dbridement Patient preparation. The patient is positioned
supine in the OR or in a position that allows best access to the
open fracture wounds. Skin preparation and draping should include
access to the major proximal vessels in case their exposure becomes
necessary. Tourniquets should be avoided when possible to prevent
additional ischemic injury to the soft tissues.General principles
of debridement.It is important to perform a thorough surgical
dbridement in an organized manner. Starting with the skin, each
layer is debrided systematically. One can imagine a clock face;
wound dbridement starts at the 12 oclock position and continues in
a clockwise manner around the circumference of the wound. This is
repeated for each layer down to the level of the bone. Necrotic
tissue is removed and only viable tissue is left behind. The
exception is skin, where none is removed unless obviously necrotic.
The quality of the muscle tissue is assessed using the classic 4
Cs: Color (red or brown) Consistency (how does the muscle feel)
Capillary Circulation (does it bleed?) Contractility (responds to
pinch or electro-cautery)IrrigationAfter removing visible dirt and
necrotic tissue, irrigation with several liters of fluid is a key
component of the decontamination of the injury zone. If available,
a balanced salt solution is routinely used. In more austere
environments, any water that is clean enough to drink is
acceptable. Controversies exist regarding the optimal volume and
delivery methods. We recommend large volumes, with low pressure to
avoid additional tissue injury. Gravity flow, with large-bore
cystoscopy tubing, is a well accepted method.Fracture
stabilizationExternal fixation. External fixation can be applied
using either modular or uniplanar techniques. The modular frames
have the advantage of being more versatile, avoiding the complex
wounds that are often seen. The disadvantage of a modular frame is,
that it is less rigid than the uniplanar fixator because of its
multiple connections. Pin placement outside of the anticipated zone
of the definitive implant is a consideration, although not always
possible. Reduce the fracture as well as possible, to avoid
soft-tissue tension.Definitive treatmentDefinitive fixation is
considered, when: The patients clinical status is optimized The
wounds are healthy and the soft-tissue envelope will allow for
chosen surgical approach A good preoperative plan has been
created.














![Ortho NCLEX Questions[1]](https://img.pdfslide.us/doc/110x75/5537936a55034650678b4eb8/ortho-nclex-questions1.jpg)