Embed Size (px)
Citation preview

Br Heart J 1991;65:239-44
ORIGINAL ARTICLES
Twenty four hour heart rate variability: effects ofposture, sleep, and time of day in healthy controlsand comparison with bedside tests of autonomicfunction in diabetic patients
D J Ewing, J MM Neilson, C M Shapiro, J A Stewart, W Reid
AbstractHeart rate variability was measured in77 healthy controls and 343 diabeticpatients by a count of the number ofbeat-to-beat differences greater than50 ms in the RR interval during a 24 hourambulatory electrocardiogram. In thehealthy controls the lower 95% tolerancelimits for total 24 hour RR intervalcounts were approximately 2000 at age25, 1000 at 45, and 500 at 65 years. Sixcontrols confined to bed after injury hadnormal 24 hour patterns of RR counts,while eight other controls showed loss ofdiurnal variation in both heart rate andRR counts during a period of sleepdeprivation. RR counts in ten controls onand off night duty increased during sleepwhenever it occurred. Nearly half (146)the 343 diabetic patients had abnormal24 hour RR counts. The percentage ofabnormal RR counts increased withincreasing autonomic abnormalityassessed by a standard battery of tests ofcardiovascular autonomic function. Aquarter of those with normal cardiovas-cular reflex tests had abnormal 24 hourRR counts. There were close correlationsbetween 24 hour RR count resuks andthe individual heart rate tests (r = 0-6).The assessment of cardiac para-
sympathetic activity by 24 hour RRcounts was reliable. The diurnal varia-tions in RR counts seen in the controlswere probably related to sleep ratherthan either posture or time of day. Themethod was more sensitive than conven-tional tests of cardiovascular reflexes.
UniversityDepartments ofMedicine, and MedicalPhysics and MedicalEngineering, RoyalInfirmary, EdinburghD J EwingJMM NeilsonCM ShapiroJ A StewartW ReidCorrespondence toDr D J Ewing, Departmentof Medicine, RoyalInfirmary, EdinburghEH3 9YW.
Accepted for publication6 December 1990
Measurements of heart rate variability are
increasingly being used as markers of cardiacautonomic activity. In diabetes and otherclinical disorders affecting the autonomicnervous system their use is now well estab-lished.' The variability in heart rate may be an
independent prognostic marker after myocar-dial infarction,2 and an imbalance of normalcardiac autonomic control mechanisms, withreduced heart rate variation, has beenproposed to explain sudden infant death syn-drome.3 Diurnal variation in the pulse ratewas noted in a medical journal as long ago as
1815,4 but the use of short term heart rate
variation as a clinical test of autonomic func-tion both at rest5 and during a short period ofdeep breathing6 was only developed in the1970s. More recently still, heart rate variationhas been measured over longer periods by 24hour electrocardiographic tape recordings.7 Asa diagnostic clinical test, the maximum -
minimum heart rate during deep breathinghas proved most popular689 but for researchpurposes other methods of analysis, includingthe use of standard deviation25 and spectralanalysis,""'2 have also been used.Though these approaches are valid they also
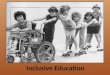
have drawbacks. For example, the "deepbreathing" method has relatively poorreproducibility, is dependent on the subject'scooperation, and only gives information aboutthe brief period during which the heart rate isactually measured. Scrutiny of longer heartrate recordings often shows considerable dis-crepancies in the amount of heart ratevariability present at different times of the dayand night (fig 1). Spectral analysis is based onassumptions about the control of heart ratewhich depend on particular and consistentinput stimuli and on the assumption that itsrhythms can be broken down into discretecomponents, each representing specific anddifferent autonomic activity. Spectral tech-niques are also unable to cope with recordingscontaining frequent ventricular arrhythmias.Standard deviation methods do not distin-guish clearly between parasympathetic andsympathetic components.Because of the limitations of these methods,
we have developed an alternative approach.We noted that there were a large number ofbeat-to-beat changes in heart rate thatoccurred frequently but irregularly in healthycontrols and that they were distinct from thesmaller cyclical changes of respiratory sinusarrhythmia. We devised a method to measurethese larger changes by counting the numberof times successive RR intervals differed bymore than 50 ms during a 24 hour taperecording (referred to subsequently as "RRcounts"). This was first described in 1984when we showed that RR counts reflected theintegrity of cardiac parasympathetic path-ways.7The aim of our present study was to deter-
mine what factors affect heart rate variability-in particular the role of posture, sleep, andtime of day. We evaluated the results from our
239
on August 28, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.65.5.239 on 1 May 1991. D
ownloaded from

Ewing, Neilson, Shapiro, Stewart, Reid
1600-
lnn-
L-
-4o O
C 1600-c:cr
1000-
400-
Day Night.n ,, .- :. --... .
: i , 1. .7
7-
7-
7
-I-5-0 -,,:4! !
_':: : : :.:::::''. ';::.: :,.:.' -*., .' : .:. i. : . : |.... ,, . . . . .-:: z:::' V' I t
jL i Ax 1Et-Wt-0
,- _ M _ .__ ,.
...,T - ; ......... ....... .... ,.-:- . ... :.--- :-t---Jet -::1 -. * . e --| *---
:' :-: .: '':.':::::.[;-:: :.i '...: :. _ w ::X:: :_ a._., _
l
1 min
j_._
Figure 1 Four short RR interval recordings (3 minutes each) takenfrom the samediabetic patient at different times of the day and night, showing considerable differences inRR variation.
larger experience of 24 hour electrocardiogra-phic tape analysis and defined the age relatednormal values for the RR counts. We alsosought to establish how the results of 24 hourelectrocardiographic tape recordings relate toconventional tests of cardiovascular auto-nomic function in a large group of diabeticpatients.
Patients and methodsCONTROLSTwenty four hour electrocardiograms were
recorded from 57 men (aged 18-65 years) and20 women (aged 18-57 years). All were
ambulant and going about their normal dailyroutines. None had any known disease or was
taking regular medications (normal group).Tapes were also recorded from six young men(18-27 years) who were confined to bed withleg and pelvic fractures. The tapes were recor-
ded several days after operation when the menwere fully conscious (orthopaedic group).Eight other healthy young men (aged 19-29years) took part in a sleep deprivation study,during which heart rate was monitored on totape for 24 hours before, for two successive 24hour periods during 48 hours continuoussleep deprivation, and then on two successive24 hour recovery periods of normal sleep(sleep deprived group). The results from thetwo 24 hour tapes measured during sleepdeprivation were averaged as were those fromthe 48 hours recovery period. Ten night nur-ses (three men and seven women, aged 26-47years) had 24 hour tape recordings made dur-ing and after their night duty shifts (nightshift group). Four recordings were made oneach individual: at the beginning and end ofseven days of night duty and at the beginningand end of their seven day recovery period offduty. The 24 hour RR counts in men in thenormal group and the "posture" results in theorthopaedic group have been described brieflybefore'3 but are included here in greaterdetail.
DIABETIC PATIENTSThree hundred and twelve diabetic patients(200 men and 112 women, aged 17-66 years)had 24 hour recordings as part of their assess-ment for autonomic involvement (diabeticgroup). Twenty four hour tape recordings anda standard battery of cardiovascular reflex testswere performed within 24 hours of each otherin all these patients. A further 31 diabeticpatients had an incomplete battery of cardio-vascular tests. Their results are included inthe correlations between the 24 hour taperesults and individual tests.The subjects in the various studies all
agreed to 24 hour ambulatory electro-cardiographic monitoring and the techniquehad the approval of the local hospital ethicsadvisory committee.
METHODSElectrocardiographic recordingsThree chest electrodes were used to recordelectrocardiogram signals on to a cassette tapewith an ambulatory electrocardiographicmonitoring system (Medilog, Oxford Instru-ments or Tracker, Reyndlds Medical). Anadjacent tape track was used to record a simul-taneous time frequency reference signal. Therecordings were continued for 24 hours, whilethe subjects went about their routine dailyactivities, with the tape recorder carried on abelt worn around the waist. They noted mealtimes, unusual events, and the times ofgoing tobed and getting up in a diary.
Analysis ofRR interval variationThe 24 hour tapes were later replayed througha Pathfinder (Reynolds Medical) high speedarrhythmia analyser at 120 times the originalrecording speed. The replay speed was con-trolled to within 0-5% by means of the timereference track recorded on each tape.The trigger section of the analyser detected
individual QRS waves in the electrocardiogramsignal and distinguished them from P and Twaves and from muscle noise and artefact bymeans of a continuously adaptive thresholdderived from the noise components byindependent filtering. The accuracy with whichQRS waves can be detected depends on thequality ofthe recorded electrocardiogram; withtapes of routine quality there were only about12 false positive and false negative errors ofdetection in 24 hours.'4 Excessive noise, such aswould cause QRS waves to be missed,automatically inhibited analysis until the noisesubsided, whereupon analysis was resumed.The Pathfinder detects any QRS waves with ashapethat differs significantly fromthe subject's"normal" QRS complex; a continuouslyupdated example ofthis normal complex is heldin the analyser memory for comparison. Suchabnormal complexes are indicated as ven-tricular extrasystoles. 5 The signal is closelymonitored throughout the analysis by theoperator to exclude tapes with atrial fibrillationand other non-sinus rhythms, and appreciablenumbers of supraventricular extrasystoles.For each electrocardiographic complex in
the recording the Pathfinder generates an ex-
.!:+ 1: .! '!.titti:::.:
.:
-: i:........
..
240
m..Ir
.a
L ^ i
on August 28, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.65.5.239 on 1 May 1991. D
ownloaded from

Twentyfour hour heart rate variability
ternal pulse to signify a beat, and another if thatQRS complex is of normal (sinus) configura-tion. These pulses are passed to a microcom-puter which times the arrival of each beat andcalculates the length of each RR interval andthe difference between each successive beat. Ifthis increases by more than 50 ms betweensuccessive beats a positive count is added to thetotal being accumulated. Likewise, if thechange shows a decrease ofmore than 50 ms thetotal negative count is increased. Because we
found no significant differences betweenpositive and negative counts7 the resultsreported here are positive counts.The program also continuously maintained
time thresholds corresponding to 63% and175% of the prevailing normal RR interval.Beats with intervals outside these limitstogether with all those indicated by the Path-finder as being "not normal" in shape wererejected and the interval calculations were
restarted from the next normal QRS. Theintervals thus excluded and all periods duringwhich the analyser was inhibited were
accumulated and used to calculate the percen-tage of the time actually analysed. Using thistechnique we can now analyse tapes with largenumbers of ventricular extrasystoles.16 Foreach tape the program gave an output of total 24hour RR counts, mean hourly wake and meanhourly sleep RR counts, and mean wake andmean sleep heart rate. Where the tape record-ing is incomplete the results are normalised tothe equivalent of 24 hours. Recordings shorterthan 18 hours or with less than 40% of beatsanalysed were rejected.
Cardiovascular autonomic function testsWe used a standard battery of cardiovascularautonomic function tests to assess all diabeticpatients: the heart rate responses to theValsalva manoeuvre, standing up, and deepbreathing; and the blood pressure responses tostanding up and sustained handgrip. We havedescribed these tests and the grading of severityin detail elsewhere.9 In brief, autonomicinvolvement was categorised as normal (alltests normal), early (one heart rate test abnor-mal), definite (two or more heart rate testsabnormal), severe (abnormal heart rate testsplus one or both blood pressure tests abnor-mal), or atypical (any other combination ofabnormalities). Autonomic scores were derivedby giving each test a score of0 for normal, for
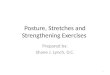
Figure 2 Individual total24 hour RR counts in 57healthy men and 20healthy women. Thebroken lines are the agerelated 95% normaltolerance limits, derivedfrom the counts in the 57men.
100000-
10000-(a
c
o:0
, 1000-
100-
10-
00
000.0 .000 * -
001
- -so- 00 %O~~~~0~~~~~~
*O * w
20 30 40Age (years)
50 60
borderline, and 2 for an abnormal result. Thisgave a total score of between 0 (normal) and 10(most severe).
STATISTICAL ANALYSISConventional statistical methods were appliedto the results as appropriate; we used regressioncalculations and paired t tests. Where the datawere not normally distributed calculationswere performed on the log transformed data.Results are accordingly presented as mean(SD) or geometric mean and range.
ResultsCONTROLSThere were significant inverse correlationsbetween age and total 24 hour (r = -0-55),mean hourly wake (r = -0-54), and meanhourly sleep (r = -0-51) RR counts in the 57male controls. Figure 2 shows the individualtotal 24 hour RR counts in these men and in 20female controls. Because there were no sig-nificant differences between the results of themen and women and because the age distribu-tion of the women was skewed (most were < 30years old), the lower 95% tolerance limits forthe RR counts were calculated from the resultsfor the 57 men. The normal lower 95°%tolerance limits for total 24 hour RR counts are2000 at age 25, 1000 at age 45, and 500 at age 65years. Table 1 shows the equivalent values formean hourly wake and sleep RR counts.
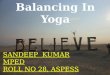
ORTHOPAEDIC GROUPAll six young men confined to bed after injuryhad total 24 hour RR counts well within thenormal range for their age (fig 3). The countsrose appropriately at night during sleep in fivesubjects (geometric mean of hourly wakecounts 235 (84-792) and hourly sleep counts484 (249-716)). All wake and sleep values werein the normal range. Mean heart rate fell from77 (7) beats/min awake to 61 (6) beats/minasleep.
SLEEP DEPRIVED GROUPTable 2 shows the group mean RR counts andheart rate during normal sleep and during sleepdeprivation. There were no significant differ-ences in results between the normal 24 hourperiod before and the 48 hour period after sleepdeprivation. Mean RR counts rose as expectedduring normal sleep from 452 to 614 (+ 36%,p = 0 034), but not at night during sleepdeprivation (460 to 471) (+2%, NS). Heartrate fell substantially during normal sleep, butduring sleep deprivation day and night valuesremained similar. There were, therefore, con-siderable differences between the night time
Table I Approximate normal lower 95% tolerancelimitsfor total 24 hour, mean hourly wake, and meanhourly sleep RR counts related to age
Total 24 hour Mean hourly Mean hourlyAge (yr) counts wake counts sleep counts
25 2000 60 9045 1000 30 4565 500 15 20
241
on August 28, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.65.5.239 on 1 May 1991. D
ownloaded from

Ewing, Neilson, Shapiro, Stewart, Reid
600-
C'500-0
cr 400-
0 300-
c
c
' 200-
100-
0-
. * R R counts|O Heart rate
I I I I I I I I I -110 12 14 16 18 20 22 24 2 4 6 8 14
Time (hours)
Figure 3 Group mean hourly RR counts and hourly heart rate in sixyoung menconfined to bed.
counts (p = 0-059) and heart rates (p < C
during the normal and the sleep depperiods.
NIGHT SHIFT GROUPDuring the first and last night shift peiwhich were separated by six days, the Nsleep pattem was similar, with an averaseven hours sleep on each occasion,between about 9.00 am and 5.00 pm
coming offnight duty, the subjects usuallyduring the day until about 5.00 pm, theup, and went back to bed again aroundmidnight until 7.00 or 8.00 am the follcmorning. This meant that during the firsthey had an average of 13 hours' sleep. Sixlater, the last day shift, the sleep patterrreverted to normal, but in preparation fornext night duty shift, the subjectslonger-an average of 10 hours from midto 10.00 am.The hourly RR counts during these fo
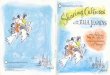
hour periods reflect the wake and sleep pat(fig 4) in that during the two night shift pethe average RR counts were highest durinday when the subjects were asleep (geonmean of hourly counts: wake 123 (13-585140 (35-462); sleep 188 (47-1167) and 234835)). The last day shift period, just beforsubjects restarted night duty, shows a ncday/night pattern ofRR counts (wake 174541); sleep 331 (96-1021)). The first dayperiod, however, shows a somewhat diffipattern, with two periods of higher and
90 periods of lower counts, corresponding to the80 two periods of sleep and waking. This was
coupled with higher and lower mean heart rates70 (geometric mean of hourly counts-wake first60 period 144 (34-673), wake second period 154
(46-640); sleep first period 255 (74-857), sleep50 X second period 344 (82-940) and mean heart40 g rates (beats/min)--wake 78 (10) and 78 (8);
sleep 66 (8) and 62 (5) sleep). Because the30 3 counts were higher during sleep, the mean total20 24 hourRR counts were greatest during the day
shift periods when the subjects slept more (first10 night shift 3583 (582-18119), last night shift0 4168 (811-13514), first day shift 6425 (2182-
o 17644), last day shift 5905 (1922-16191)).
DIABETIC GROUPForty seven per cent (146 subjects) had total 24hour RR count results that were less than thelower 95% tolerance limit for healthy controlsrelated to age. Table 3 shows the proportion of
)-001) normal and abnormal results related both to therived autonomic category and to the autonomic score
(based on results from a standardised battery ofcardiovascular reflex tests done within 24 hoursof the 24 hour tape recording). With increasing
riods, autonomic abnormality there was a higherwake/ percentage ofabnormal 24 hour tape results; so
ge of that alnost all with autonomic dysfunction intaken the "definite" and "severe" categories had. On abnormal total 24 hour counts. The fact thatslept the 24 hour tape method is more sensitive thann got conventional autonomic function tests is shown12.00 by the 24% who had abnormal 24 hour counts)wing despite normal cardiovascular reflexes. Table 3;t day also shows the group mean values for the 24days hour count results related to autonomic
a had category and score. Counts were lower as thetheir autonomic damage increased.slept Table 4 shows the correlation coefficientsnight between the 24 hour total counts, wake and
sleep counts, and the individual cardiovascularur 24 autonomic function tests. In every case the:terns relations were highly significant statistically,riods with the closest correlation between the countsig the and the heart rate tests. There were alsoaetric extremely close correlations between the log) and total 24 hour counts and the log wake counts(32- (r = 0-969) and the log sleep counts
re the (r = 0-957) in this group of diabetic patients.)rmalL(29-shift DiscussionSerent Since we first reported our technique ofI two assessing cardiac parasympathetic activity by
Table 2 Group mean RR counts and heart rates in eight healthy men aged 19-29 years who were deprived ofsleepfor48 hours
RR counts (geometric mean and range) Heart rate (arithmetic mean (SD)) (beats/min)
Mean hourly Mean hourlyTotal 24 h counts wake sleep Wake Sleep
(-p = 0034-5Normal sleep 12333 452 614 79 (8) 57 (8)
(7332-18050) (300-737) (263-877)Significance NS NS p = 0059 NS p < 0-001
Day Night Day Night(8am-12pm) (I2pm-8 am)
Sleep deprived 11194 460 471 77 (8) 76(8)(5951-17723) (217-761) (310-754)
242
on August 28, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.65.5.239 on 1 May 1991. D
ownloaded from

Twenty four hour heart rate variability
500-t Day shifts
400
300
200-
c 100-
o'C .
X 400-
300-
200-
1001
Night shifts
0-
8 10 12
* First night shiftO Last night shift
14 16 18 20 22Time (hours)
24 2 4 6 8
Figure 4 Group mean hourly RR counts in ten healthy individuals (three men andseven women) during and after night duty.
analysing 24 hour electrocardiograms,7 we havegained considerably more experience in bothhealthy individuals and patients. The methodhas also been refined so that we can now excludelarge numbers of ventricular extrasystoleswithout losing the essential data on heart ratevariability.'6 This contrasts with the inability ofspectral analysis methods to handle ventricularextrasystoles. Additionally, analysis can bedone at 120 times real speed so that a full 24hour tape recording can be read through intwelve minutes by the dedicated microcom-puter system we have developed.
In a smaller study we showed that RR countsdecrease with age in healthy individuals. Wehave expanded our normal results and in thepresent study we show the 95% tolerance limitsnot only for the total 24 hour RR counts butalso for the mean hourly wake and mean hourlysleep counts. There was an extremely closecorrelation between these three measures in theresults from the diabetic patients, which meansthat each index can be used to assess variability.We previously reported our data on
repeatability in healthy individuals, diabeticpatients, and patients with cardiac disorders,7 16showing that this RR counts method can beused reliably for treatment and outcome trials.There is normally a characteristic rise in RR
counts at night and we wondered what factorsmight be responsible for this. We found anormal RR counts pattern in a group of fit butimmobile young men. This suggests that beingconfined to bed is not a factor influencing thenumbers of abnormal RR counts recorded.To establish whether the variations in RR
counts were part of a built-in diurnal clock wemeasured RR counts in another group of fityoung men undergoing prolonged periods ofsleep deprivation as part of a different study.Though total 24 hour RR counts were similar,the wake/sleep difference in counts during theperiod of "normal sleep" disappeared duringthe 48 hours of sleep deprivation. Similarly, ina group of nurses the daytime counts were
higher while the nurses were on night shift andsleeping during the day. There is, therefore, nobuilt-in diurnal clock to regulate the RRcounts.The third candidate for modifying RR
counts is that of sleep itself, rather than eitherposture or time of day. The results from boththe sleep deprivation and the night duty studiessupport this mechanism: both periods of sleeptaken by the night duty staff on the same dayincreased the RR counts. Thus the increase inRR counts seen in most individuals occursduring sleep and seems to be due to sleep itself.This would fit in with current concepts of therelative activity of the autonomic nervous sys-tem whereby both sympathetic and parasym-pathetic components are active during the day,whereas at night during periods of non-rapideye movement sleep there is predominantlyparasympathetic activity. This is also reflectedin the changes in heart rate which reciprocatethe changes in RR counts in most individuals.We have not specifically related sleep stages toRR counts but during rapid eye movementsleep there are well documented changes inautonomic activity'7 which may be associatedwith increased RR counts.Do RR counts merely reflect the overall heart
rate? We argued in detail that this is not so7 13 inview of the dissociation between heart rate andheart rate variability in our earlier studies.'8There is a complex interrelation between beat-
Table 3 Number of diabetic patients with abnormal 24 hour RR counts according to autonomic category and score,and group mean values for RR counts
Number with 24 hour RR counts Group mean 24 hour RR counts (geometric mean)
Number with Mean hourly Mean hourlyTotal abnormal counts (%) Total 24 hour wake sleep
All 312 146 (47)By autonomic category:Normal 147 35 (24) 2845 84 170Early 52 25 (48) 866 27 42Definite 32 27 (84) 154 6 7Severe 60 51(85) 114 4 4Atypical 21 8 (38) 1489 48 69
By autonomic score:0-2 175 42 (24) 2756 82 1623-5 67 43 (64) 422 14 196-10 70 61 (87) 112 4 4
N First day shift13 Last day shift
9 I 9 I I I I I I I I -II
243
on August 28, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.65.5.239 on 1 May 1991. D
ownloaded from

Ewing, Neilson, Shapiro, Stewart, Reid
Table 4 Correlation coefficients between individual cardiovascular autonomicfunction tests and total 24 hour RRcounts and mean hourly wake and sleep RR counts
Valsalva 30:15 Max - min BP drop BP rise AutonomicRR counts ratio ratio heart rate on standing with grip score
Log total 24 hour 0 627 0 557 0-625 -0 439 0-314 -0-683(n = 321) (n = 342) (n = 285) (n = 316) (n= 312)
Log mean hourly wake 0 636 0-567 0-637 -0 433 0-297 -0-679(n = 318) (n = 340) (n= 286) (n = 313) (n = 311) (n = 309)
Log mean hourly sleep 0 610 0 539 0-608 -0 444 0-323 -0-692(n = 318) (n = 340) (n = 286) (n = 313) (n = 311) (n = 309)
to-beat differences and prevailing average heartrate, but it is by no means a simple matter of theoverall heart rate determining the amount ofbeat-to-beat heart rate variation, howevermeasured.Though we showed the clear relation be-
tween autonomic damage and RR counts in ouroriginal article7 and briefly in a small group ofdiabetic patients"9 we have not hitherto repor-ted in detail on the relation between conven-tional non-invasive tests. of cardiovascularautonomic function and 24 hour RR counts inlarge numbers of diabetic patients. Our resultsclearly show not only the very close correla-tions achieved between individual cardiovas-cular tests (particularly the heart rate tests) andRR counts, but also the differing proportions ofnormal and abnormal results with increasingseverity of autonomic damage. About 85% ofthose in whom definite or severe damage wasdetected by cardiovascular testing had abnor-mal RR counts. Because 24% of diabeticpatients with apparently normal cardiovascularreflexes had abnormal RR counts we believethat the RR counts method is more sensitivethan conventional tests of cardiovascularreflexes.What are the clinical applications of this
method? It is reliable and sensitive and gives anobjective measure of cardiac parasympatheticactivity.7 Simple bedside tests of autonomicfunction in diabetes are widely available todiagnose autonomic neuropathy,'9 but ourmethod of analysing 24 hour electrocardio-graphic tape recordings reveals earlier abnor-malities of cardiac parasympathetic function.There has recently been increasing interest inthe effect of autonomic influences on prognosisafter myocardial infarction. With our method itshould be possible to see whether low heart rate
variability is indeed an adverse prognosticindicator. One such study has already beenpublished,2 and further studies are currently inprogress by our own group and others. Con-ventional bedside tests are also inappropriate inthe sudden infant death syndrome, where therehas been evidence that reduced heart ratevariation may be a factor.'20 Objective assess-
ment of other conditions such as chronic renalfailure, liver disease, and congestive cardiacfailure may also be possible with this method of24 hour electrocardiographic tape recording.Other work in progress suggests thatmeasurement of RR counts may also be ofrelevance in assessing the effect of drugs on thecardiovascular system.'6 21
These studies were supported by grants from the WellcomeTrust, British Diabetic Association, Chest Heart and StrokeAssociation (Scotland), and the Scottish Home and HealthDepartment.
1 Ewing DJ. Recent advances in the non-invasive investiga-tion of diabetic autonomic neuropathy. In: Bannister R,ed. Autonomicfailure. A textbook of clinical disorders of theautonomic nervous system. 2nd ed. Oxford: Oxford Univer-sity Press, 1988:667-89.
2 Kleiger RE, Miller JP, Bigger JT, Moss AJ, and theMulticenter Post-Infarction Research Group. Decreasedheart rate variability and its association with increasedmortality after acute myocardial infarction. Am J Cardiol1987;59:256-62.
3 Schwartz PJ. The quest for mechanisms ofthe sudden infantdeath syndrome: doubts and progress. Circulation1987;75:677-83.
4 Knox R. On the relation subsisting between the time of theday, and various functions of the human body; and on themanner in which pulsations of the heart and arteries areaffected by muscular exertion. Edin Med Surg J1815;11:52-65 and 164-7.
5 Murray A, Ewing DJ, Campbell IW, Neilson JMM, ClarkeBF. RR interval variations in young male diabetics. BrHeart J 1975;37:882-5.
6 Wheeler T, Watkins PJ. Cardiac denervation in diabetes. BrMedJ 1973;iv:584-6.
7 Ewing DJ, Neilson JMM, Travis P. New method forassessing cardiac parasympathetic activity using 24 hourelectrocardiograms. Br Heart J 1984;52:396-402.
8 Hilsted J, Jensen SB. A simple test for autonomicneuropathy in juvenile diabetes. Acta Med Scand1979;205:385-7.
9 Ewing DJ, Martyn CN, Young RJ, Clarke BF. The value ofcardiovascular autonomic function tests: 10 yearsexperience in diabetes. Diabetes Care 1985;8:491-8.
10 Axelrod S, Gordon D, Madwed JB, Snydman NC, ShannonDC, Cohen RJ. Hemodynamic regulation: investigationby spectral analysis. Am J Physiol 1985;249:H867-75.
11 Pomeranz B, Macaulay RJB, Caudhill MA, et al. Assessmentof autonomic function in humans by heart rate spectralanalysis. Am JPhysiol 1985;248:H151-3.
12 Pagani M, Lombardi F, Guzzetti S, et al. Power spectralanalysis ofheart rate and arterial pressure variabilities as amarker of sympatho-vagal interaction in man and cons-cious dog. Circ Res 1986;59:178-93.
13 McAreavey D, Neilson JMM, Ewing DJ, Russell DC.Cardiac parasympathetic activity during the early hours ofacute myocardial infarction. Br Heart J 1989;62:165-70.
14 Neilson JMM. Detection of QRS waves in ambulatorymonitoring signals. In: Hombach V, Hilger HH, eds.Holter monitoring technique. Stuttgart and New York:Schatteur, 1985:15-25.
15 Neilson JMM. Computer detection of ventricular ectopicbeats: on line and off. Computers in Cardiology, Bethesda,USA, IEEE Cat No 75CH 1b18-1C, 1975:33-5.
16 Zuanetti G, Latini R, Neilson JMM, Schwartz PJ, EwingDJ. Heart rate variability in patients with ventriculararrhythmias: effect of antiarrhythmic drugs. J Am CollCardiol 1991 (in press).
17 Shapiro CM. Autonomic dysfunction during REM sleep.In: Peter JH, Podszus T, von Wichert P, eds. Sleep andhealth risk. Berlin: Springer-Verlag, 1991 (in press).
18 Ewing DJ, Hume L, Campbell IW, Murray A, NeilsonJMM, Clarke BF. Autonomic mechanisms in the initialheart rate response to standing. J Appl Physiol1980;49:809-14.
19 Matthews DM, Martyn CN, Riemersma RA, Clarke BF,Ewing DJ. Noradrenaline response to edrophonium (ten-silon) and its relation to other autonomic tests in diabeticsubjects. Diabetes Res 1987;6:175-80.
20 Cauchemez B, Peirano P, Samson-Dolfus D, et al. Theautonomic nervous system in sudden infant death syn-drome. Analysis of heart rate and heart rate variability onHolter recordings. Arch Mal Coeur 1989;82:745-52.
21 Flapan AD, Nolan J, Neilson JMM, Ewing DJ. Captopriltherapy increases parasympathetic activity in patientswith congestive cardiac failure [Abstract]. Circulation1990;82(suppl 3):382.
244
on August 28, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.65.5.239 on 1 May 1991. D
ownloaded from

















![BBC VOICES RECORDINGS€¦ · BBC Voices Recordings) ) ) ) ‘’ -”) ” (‘)) ) ) *) , , , , ] , ,](https://img.pdfslide.us/doc/110x75/5f8978dc43c248099e03dd05/bbc-voices-recordings-bbc-voices-recordings-aa-a-a-a-.jpg)







