Embed Size (px)
Citation preview

Int J Clin Exp Med 2016;9(9):18098-18103www.ijcem.com /ISSN:1940-5901/IJCEM0032998
Original Article Extratemporal facial nerve schwannoma: are computed tomograghy findings predictive?
Yan Wang1, Yixin Qiao2, Wen Li2
1State Key Laboratory of Oral Diseases, Department of Orthodontics, West China College of Stomatology, Sichuan University, Sichuan, China; 2Department of Otolaryngology, Head and Neck Surgery, West China Hospital, Sichuan University, Sichuan, China
Received May 30, 2016; Accepted August 4, 2016; Epub September 15, 2016; Published September 30, 2016
Abstract: Objectives: To investigate the predictive value of computed tomography imaging in diagnosis of extra-temporal facial nerve schwannoma. Materials and methods: Computed tomography records of eight patients with extratemporal facial nerve schwannoma managed from 2007~2015 were reviewed. Tumors of all cases were totally removed surgically. Intraoperative frozen section examination was employed. Results: computed tomography of one patient whose tumor derived from buccal branch demonstrated imaging of a round mass with clear margin; four out of five patients whose tumors derived from facial nerve trunk revealed a significant tail pointing to the stylomastoid foramen with one exception; one patient whose tumor located at the margin of parotid gland demonstrated round mass just outside the stylomastoid foramen deep to the mastoid process with a tail pointing to the parotid gland; one case of synchronous schwannomas took place in the parotid gland and parapharyngeal space presented ob-scure tail-like imaging. Diagnoses of schwannoma were inclined in all intraoperative frozen section examinations. There was no tumor relapse in all cases after one to three years follow-up while the tumor-involved facial nerve or nerve branches were disturbed in all cases. Conclusion: Computed tomography findings can provide some useful in-formation for the diagnosis of extratemporal facial nerve schwannoma especially for those derived from nerve trunk.
Keywords: Facial nerve, schwannoma, computed tomography, diagnosis
Introduction
Extratemporal facial nerve schwannoma (ETFNS) is rarer than those take place intratem-porally [1, 2]. Because most of ETFNS are quite similar to other primary parotid gland neoplasm such as mixed tumor, an early diagnosis is chal-lenging. It is reported that both magnetic reso-nance imaging and computed tomography (CT) could offer some evidence for the diagnosis of intratemporal facial nerve schwannoma (ITFNS) in several papers, while a very few have talked about ETFNS and never reached an agreed cri-teria of diagnosis based on radiological findings [3-5]. Here we report some radiological findings which might favor a diagnosis of ETFNS.
Materials and methods
Eight patients with ETFNS managed from 2007~2015 in West China Hospital, were retro-spectively studied. They are aged from 40 to 65
years old with the mean age of 48. There is only one male among them. All patients presented with a painless parotid mass with normal facial nerve function. CT of eight cases was evaluat-ed. Complex facial nerve schwannoma involving both temporal bone and parotid gland were excluded. Tumors of all cases were totally removed surgically. Intraoperative frozen sec-tion examination was employed.
Results
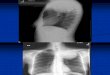
CT of one patient whose tumor located at the margin of parotid gland, demonstrated round mass just outside the stylomastoid foramen deep to the mastoid process with a tail pointing to the parotid gland (Figure 1A); four of five patients with ETFNS derived from facial nerve trunk, revealed a significant tail pointing to the stylomastoid foramen (Figure 1B-D), except one with no tail-like imaging (Figure 2A); one patient of ETFNS derived from buccal branch

CT of extratemporal facial nerve schwannoma
18099 Int J Clin Exp Med 2016;9(9):18098-18103
demonstrated a round mass with clear margin; one patient of synchronous schwannomas took place in the parotid gland and parapharyngeal space, presented obscure tail-like imaging, the schwannoma was also derived from facial nerve trunk (Figure 3A). Pathological diagnoses of schwannoma were inclined in all intraopera-tive frozen section examinations based on the well-differentiated spindle cells accumulation. The final pathological diagnosis of schwanno-ma was also established by routine histology and immunohistochemistry.
Tumors of all cases were totally removed surgi-cally. Superficial parotidectomy was performed
in seven cases and total parotidectomy was performed in one case. Superficial parotidec-tomy and partial mastoidectomy was per-formed for the tumor deep to the mastoid pro-cess. Facial nerve trunk was spared in four cases including three cases of eccentric lesion of the trunk, and one case derived from the buccal branch, at the same time, Schwann membraneous “sac” was also spared (Figure 2B-D). The facial nerve trunk could not spared in the other four cases because the tumor could not strip from a clear facial nerve trunk, or facial nerve trunk was found terminated, then the facial nerve defect was repaired with greater auricular nerve grafting (Figure 3B-D).
Figure 1. Computed tomography of ETFNS ETFNS locating outside the stylomastoid foramen and deep to the mas-toid process with a tail pointing to the parotid gland (A), typical imaging of ETFNS derived from facial nerve trunk, revealing a significant tail pointing to the stylomastoid foramen (B-D).

CT of extratemporal facial nerve schwannoma
18100 Int J Clin Exp Med 2016;9(9):18098-18103
There was no tumor relapse in all cases after one to three years follow-up while the tumor-involved facial nerve or nerve branches were more or less disturbed in all cases.
Discussion
Parotid tumor is common in surgical practice. Of all parotid tumors, 82% are benign and, most of them are pleomorphic adenomas. Schwannoma is rare in the parotid gland, with approximately 160 cases described to date,
and most of them are so-called intraparotid schwannoma as the facial nerve enters the parotid gland immediately upon leaving the sty-lomastoid foramen [2-4, 6]. In this case series, because only one case derived from facial nerve trunk was not embedded in the parotid gland, instead, it located just behind the parot-id gland, so the topic of this paper was accord-ingly changed from intraparotid facial nerve schwannoma to ETFNS. Even though there was a clear boundary presenting between the tumor and parotid gland, surgical exploration has con-
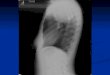
Figure 2. ETFNS derived from facial nerve trunk CT demonstrating a round mass with clear margin (white arrow) but without a tail, enhanced outer layer of the tumor and obvious hypointense region inside (A), intraoperative view demonstrating the tumor at the bifurcation of the trunk (black arrow) and Schwann membranous sac (black triangle) (B); the yellowish content of the tumor accorded to the hypointense region of CT (C); the tapered-off facial nerve trunk eventually became into membranous sac which was still spared during surgery for good nerve function recovery( white arrow) (D).

CT of extratemporal facial nerve schwannoma
18101 Int J Clin Exp Med 2016;9(9):18098-18103
firmed a contact relationship between parotid gland and the tumor. Schwannoma in the tem-poral bone with or without extracranial exten-sion is more common than solely intraparotid ones [7].
Preoperative diagnosis of ETFNS is difficult. Fine needle aspiration biopsy is theoretically the most feasible method but practically incon-clusive [8]. This may be explained by limited cell specimen or pathological complexity of salivary gland tumor. Such as spindle cell type of myo-epidermoid tumor can be taken for schwanno-ma, or epithelioid schwannoma can also be masqueraded as pleomorphic adenoma [9]. In
addition, needle track implantation also make repeated fine needle biopsies controversial. Intraoperative frozen section examination pro- ved to be more accurate than fine needle aspi-ration before surgery, and its routine applica-tion is recommended.
Facial nerve dysfunction occurred in only about 20% patients in a review of 53 ETFNS patients [10]. Whenever facial weakness presents, it mostly implies a primary or metastatic malig-nancy of parotid gland rather than a facial nerve schwannoma. For instance, adenoid cys-tic carcinoma and mucoepidermoid carcinoma are two kinds of primary parotid malignancies
Figure 3. Synchronous schwannomas took place in parapharyngeal space (A) and in the parotid gland (B) Obscure tail-like imaging revealing between the upper belly of digastric muscle and anterior border of sternocleidomastoid muscle (white arrow) (a); intraoperative view demonstrating the nerve trunk terminating at the surface of the tumor (b); demonstration of tapered facial nerve trunk after tumor removal (c); demonstration of Schwann membranous sac of the proximal end of the facial nerve trunk (d).

CT of extratemporal facial nerve schwannoma
18102 Int J Clin Exp Med 2016;9(9):18098-18103
that may easily invade facial nerve thus result in facial nerve weakness or paresis. The weak-ening process of facial nerve is slow and grad-ual, and the presence of slow and gradual facial nerve weakness could not tell different stories about adenoid cystic carcinoma or mucoepidermoid carcinoma from a facial nerve schwannoma. Facial elctroneurography can perform little differential function likewise.
Medical imaging techniques such as ultrason-ic, CT and MR are widely used for diagnosis of parotid tumor including ETFNS, among which MR is regarded as most valuable for facial nerve schwannoma. ETFNS can mimic a pleo-morphic adenoma clinically, as well as on imag-ing [11, 12]. Though pleomorphic adenomas may extremely rarely show extension to the sty-lomastoid foramen, perineural spread of parot-id malignancies should also be included in the differential diagnosis of an ETFNS showing extension along the stylomastoid foramen. In this case series report, a tail of imaging extend-ing to the stylomastoid foramen favor the diag-nosis of an ETFNS. It is supposed to be the result of sub-Schwann membraneous growth of the tumor. MR is thought to be the better technique in diagnosis of ITFNS, it presents a typically fusiform solid tumors with well-circum-scribed smooth margins in the facial nerve canal, or may acquire a dumbbell-shape when it shows multisegmental involvement. They appear iso- to hypointense on T1-weighted imaging and hyperintense on T2-weighted imaging. Cystic degeneration and hemorrhage may result in heterogeneous enhancement, it may also present with typical or classical imag-ing in enhanced CT (Figure 2A). The tumor usu-ally grows along the path of least resistance, but this property could not be demonstrated good enough outside the osseous tissue such as in the parotid gland. Presence of a target sign on T2-weighted images, if seen, excludes the possibility of a pleomorphic adenoma. Parotid malignancies often have infiltrating margins and heterogeneous appearance on T2-weighted images [13]. In this case series, we could conclude that ETFNS derived from facial nerve trunk is very likely to have a tail pointing to the stylomastoid foramen; those not derived from nerve trunk may reveal typical picture because of cystic degeneration and hemorrhage; solitary tumors locating deep to the mastoid process or upper sternocleido-
mastoid muscle with clear margin shall also arouse suspicion of facial nerve schwannoma.
Owing to the rarity of facial nerve schwannoma and its benign and slow-growing nature, there is no universally accepted management. As to the treatment plan for a ITFNS, surgically total removal with facial nerve repair is usually the standard management for patients with poor facial function (House-Brackmann grade III or worse); In patients presenting with normal or near-normal facial nerve function, both of initial observation with periodic examination and early surgical intervention are recommended in different papers. Radiotherapy especially ste-reotactic radiotherapy can be also applied to tumors of small size to avoid surgery and get possible arrest of tumor growth. Meanwhile malignant transformation after radiotherapy has been reported in literature [4, 7, 14]. The diagnosis of ITFNS by medical imaging is easier than that of ETFNS especially via a long term radiological follow-up. For ETFNS with normal facial nerve function and recognizable nerve trunk, which is also named as eccentric, nerve-sparing approach can grant postoperative fa- cial nerve function; in patients with unrecogniz-able nerve trunk, which is also named as con-centric, nerve-resection and grafting approach can rarely keep the facial nerve function satis-factory after tumor removal. Inevitable sacrifice of facial nerve followed by reconstruction may gain some degree recovery, but the facial nerve function has never been better than House-Brackmann grade III [5-7].
In conclusion, computed tomography findings can provide some useful information for the diagnosis of ETFNS especially for those derived from nerve trunk. Early surgical intervention is recommended regardless the facial nerve func-tion, in this manner, postoperative facial nerve function recovery may be easier to gain, and delayed management of primary parotid malig-nancy may be avoided.
Acknowledgements
Financial support: This study was supported by NSFC (No. 81100778). NSFC: national natural science fund of China. PS: The fund belongs to the first author of this paper.
Disclosure of conflict of interest
None.

CT of extratemporal facial nerve schwannoma
18103 Int J Clin Exp Med 2016;9(9):18098-18103
Address correspondence to: Wen Li, Department of Otolaryngology, Head and Neck Surgery, West China Hospital, Sichuan University, Chengdu 610041, China. E-mail: [email protected]
References
[1] Ma Q, Song H, Zhang P, Hou R, Cheng X, Lei D. Diagnosis and management of intraparotid fa-cial nerve schwannoma. J Craniomaxillofac Surg 2010; 38: 271-3.
[2] Gross BC, Carlson ML, Moore EJ, Driscoll CL, Olsen KD. The intraparotid facial nerve schwannoma: a diagnostic and management conundrum. Am J Otolaryngol 2012; 33: 497-504.
[3] Thompson AL, Aviv RI, Chen JM, Nedzelski JM, Yuen HW, Fox AJ, Bharatha A, Bartlett ES, Symons SP. Magnetic resonance imaging of facial nerve schwannoma. Laryngoscope 2009; 119: 2428-36.
[4] McCarthy WA, Cox BL. Intraparotid schwanno-ma. Arch Pathol Lab Med 2014; 138: 982-5.
[5] Lee DW, Byeon HK, Chung HP, Choi EC, Kim SH, Park YM. Diagnosis and surgical outcomes of intraparotid facial nerve schwannoma show-ing normal facial nerve function. Int J Oral Maxillofac Surg 2013; 42: 874-9.
[6] Lin QJ, Shi J. Clinical retrospective analysis of 19 cases of intraparotid facial nerve schwan-noma. Shanghai Kou Qiang Yi Xue 2013; 22: 99-103.
[7] Bacciu A, Nusier A, Lauda L, Falcioni M, Russo A, Sanna M. Are the current treatment strate-gies for facial nerve schwannoma appropriate also for complex cases? Audiol Neurootol 2013; 18: 184-91.
[8] Chong KW, Chung YF, Khoo ML, Lim DT, Hong GS, Soo KC. Management of intraparotid facial nerve schwannomas. Aust N Z J Surg 2000; 70: 732-4
[9] Ciau N, Eisele DW, van Zante A. Epithelioid schwannoma of the facial nerve masquerad-ing as pleomorphic adenoma: a case report. Diagn Cytopathol 2014; 42: 58-62.
[10] Bretlau P, Melchiors H, Krogdahl A. Intraparotid neurilemmoma. Acta Otolaryngol 1983; 95: 382-4.
[11] Kim KH, Sung MW, Yun JB, Han MH, Baek CH, Chu KC, Kim JH, Lee KS. The significance of CT scan or MRI in the evaluation of salivary gland tumors. Auris Nasus Larynx 1998; 25: 397-402.
[12] Gritzmann N, Rettenbacher T, Hollerweger A, Macheiner P, Hubner E. Sonography of the salivary glands. Eur Radiol 2003; 13: 964-975.
[13] Mundada P, Purohit BS, Kumar TS, Tan TY. Imaging of facial nerve schwannomas: diag-nostic pearls and potential pitfalls. Diagn Interv Radiol 2016; 22: 40-46.
[14] Husseini ST, Piccirillo E, Sanna M. Malignant transformation of acoustic neuroma/vestibu-lar schwannoma 10 years after gamma knife stereotactic radiosurgery. Skull Base 2011; 21: 135-8.


![Accessory Nerve Schwannoma Extending to the · PDF fileAccessory Nerve Schwannoma Extending to the ... [6] [7]. The most common ... Routing use of inferior cranial nerves monitoring](https://img.pdfslide.us/doc/110x75/5a7c15aa7f8b9a563b8c9eea/accessory-nerve-schwannoma-extending-to-the-nerve-schwannoma-extending-to-the.jpg)