Embed Size (px)
Citation preview

ORIGINAL ARTICLE
East–West gradient in the incidence of inflammatorybowel disease in Europe: the ECCO-EpiCominception cohortJ Burisch,1 N Pedersen,1 S Čuković-Čavka,2 M Brinar,2 I Kaimakliotis,3 D Duricova,4
O Shonová,5 I Vind,6 S Avnstrøm,6 N Thorsgaard,7 V Andersen,8,9,10 S Krabbe,8
J F Dahlerup,11 R Salupere,12 K R Nielsen,13 J Olsen,13 P Manninen,14 P Collin,14
E V Tsianos,15 K H Katsanos,15 K Ladefoged,16 L Lakatos,17 E Björnsson,18
G Ragnarsson,18 Y Bailey,19 S Odes,20 D Schwartz,20 M Martinato,21
G Lupinacci,22,23 M Milla,24 A De Padova,25 R D’Incà,21 M Beltrami,26
L Kupcinskas,27 G Kiudelis,27 S Turcan,28 O Tighineanu,29 I Mihu,29 F Magro,30,31,32
L F Barros,33 A Goldis,34 D Lazar,34 E Belousova,35 I Nikulina,35 V Hernandez,36
D Martinez-Ares,36 S Almer,37,38 Y Zhulina,39 J Halfvarson,39,40 N Arebi,41
S Sebastian,42 P L Lakatos,17 E Langholz,43 P Munkholm,1 for the EpiCom-group
▸ Additional material ispublished online only. To viewplease visit the journal online(http://dx.doi.org/10.1136/gutjnl-2013-304636).
For numbered affiliations seeend of article.
Correspondence toDr J Burisch, Digestive DiseaseCentre, Medical Section, HerlevUniversity Hospital, HerlevRingvej 75, CopenhagenDK-2730, Denmark;[email protected]
Received 4 February 2013Accepted 26 March 2013
To cite: Burisch J,Pedersen N, Čuković-Čavka S, et al. GutPublished Online First:[please include Day MonthYear] doi:10.1136/gutjnl-2013-304636
ABSTRACTObjective The incidence of inflammatory boweldisease (IBD) is increasing in Eastern Europe. Thereasons for these changes remain unknown. The aim ofthis study was to investigate whether an East–Westgradient in the incidence of IBD in Europe exists.Design A prospective, uniformly diagnosed, populationbased inception cohort of IBD patients in 31 centresfrom 14 Western and eight Eastern European countriescovering a total background population of approximately10.1 million people was created. One-third of thecentres had previous experience with inception cohorts.Patients were entered into a low cost, web basedepidemiological database, making participation possibleregardless of socioeconomic status and prior experience.Results 1515 patients aged 15 years or older wereincluded, of whom 535 (35%) were diagnosed withCrohn’s disease (CD), 813 (54%) with ulcerative colitis(UC) and 167 (11%) with IBD unclassified (IBDU). Theoverall incidence rate ratios in all Western Europeancentres were 1.9 (95% CI 1.5 to 2.4) for CD and 2.1(95% CI 1.8 to 2.6) for UC compared with EasternEuropean centres. The median crude annual incidencerates per 100 000 in 2010 for CD were 6.5 (range0–10.7) in Western European centres and 3.1 (range0.4–11.5) in Eastern European centres, for UC 10.8(range 2.9–31.5) and 4.1 (range 2.4–10.3), respectively,and for IBDU 1.9 (range 0–39.4) and 0 (range 0–1.2),respectively. In Western Europe, 92% of CD, 78% of UCand 74% of IBDU patients had a colonoscopy performedas the diagnostic procedure compared with 90%, 100%and 96%, respectively, in Eastern Europe. 8% of CDand 1% of UC patients in both regions underwentsurgery within the first 3 months of the onset of disease.7% of CD patients and 3% of UC patients from WesternEurope received biological treatment as rescue therapy.Of all European CD patients, 20% received only5-aminosalicylates as induction therapy.Conclusions An East–West gradient in IBD incidenceexists in Europe. Among this inception cohort—including
indolent and aggressive cases—international guidelinesfor diagnosis and initial treatment are not beingfollowed uniformly by physicians.
Significance of this study
What is already known on this subject?▸ The incidence of inflammatory bowel disease
(IBD) is increasing worldwide.▸ Recent studies from Eastern Europe have
reported sharp increases in incidence in somecentres comparable with Western Europeanincidence rates, whereas in other EasternEuropean centres IBD incidence has not beeninvestigated. Whether these increases representtrue increases in incidence remains unknown.
▸ Few population based inception cohorts inadults and paediatric onset IBD exist fromEastern Europe.
What are the new findings?▸ A prospective, population based, web based
inception cohort in 31 European centrescovering a background population of 10.1million people.
▸ A West–East gradient of 2 in IBD incidenceexists in Europe. The highest incidence in theworld is found on the Faroe Islands.
▸ The patient populations in Eastern and WesternEurope are identical in terms patientcharacteristics, disease extent and phenotype,smoking habits and diagnostic delay.
▸ In this inception cohort, the initial surgery ratesseemed unchanged despite the introduction ofbiological therapy in IBD treatment.
Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636 1
Inflammatory bowel disease Gut Online First, published on April 20, 2013 as 10.1136/gutjnl-2013-304636
Copyright Article author (or their employer) 2013. Produced by BMJ Publishing Group Ltd (& BSG) under licence.
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

INTRODUCTIONThe incidence of inflammatory bowel diseases (IBDs), consistingof Crohn’s disease (CD) and ulcerative colitis (UC), is subject toconsiderable variation worldwide. Incidences of UC and CDvary between 0 and 24.3/100 000 inhabitants and 0 and 20.2/100 000 inhabitants, respectively,1 with IBD more common inindustrialised countries than in non-industrialised countries.Until recently, few population based cohort data were availableon the epidemiology of IBD in Eastern Europe. However,recent studies from Hungary and Croatia have reported sharpincreases in IBD incidence that means they are now comparablewith Western European countries.2 3
The reported increase could be due to methodological bias inprevious studies from Eastern Europe, rising awareness of thedisease, differences in diagnostic practices or they could reflecttrue changes in IBD incidence.4 To investigate whether there isan East–West gradient in the incidence of IBD across Europeancountries, 31 medical centres from Eastern and Western Europeparticipated in the European Crohn’s and Colitis Organisation’s(ECCO) Epidemiological Committee (EpiCom) study; a pro-spective population based cohort of unselected IBD cases diag-nosed in 2010 within well described geographical areas wascollated by capturing clinical data throughout a 5 year period(2010–2015). Epidemiological findings on incidence, phenotypeand initial treatment are presented here.
METHODSStudy centresFollowing an initial meeting in Vienna in 2006 and anannouncement in an ECCO newsletter,5 31 centres from 14Western and eight Eastern European countries covering a totalbackground population of approximately 10.1 million people(6.8 million from Western and 3.3 million from Eastern Europe)agreed to participate in this study. The classification of centresas being situated in either Western or Eastern European coun-tries was based on the socioeconomic status of that countrybefore 1990. A well defined primary catchment area with up todate population data, including age and gender distribution, wasa prerequisite for participation. Similarly, participation requiredan established network of gastroenterologists, colorectal sur-geons and general practitioners within the uptake area to ensurecomplete coverage and inclusion of patients.
A study steering committee has organised twice yearlyEpiCom group meetings since 2006 where participants havebeen educated in case ascertainment in order to achieve consist-ency of methods as well as being trained in how to enter data in
the EpiCom database. Ten centres had previously organisedpopulation based cohorts. Furthermore, participants have beenable to influence the development and improvement of the webbased database, constructed by HD Support LLC, Denmark.6
The low cost, web based epidemiological concept made partici-pation possible for every country in Europe, regardless of socio-economic status and prior experience.
Case definitionIncident cases diagnosed with IBD between 1 January and 31December 2010 and living in the predefined catchment areas atthe time of diagnosis were prospectively included. Cases wererequired to meet the Copenhagen Diagnostic Criteria for CD7
and UC8 (see web appendix available online only). Cases inwhich not of all criteria for either CD or UC were fulfilled andyet in which subsequent relevant IBD treatment was necessarywere classified as IBD unclassified (IBDU).7–9 Fulfilment of theaforementioned criteria was ensured by the participating physi-cians. Diagnostic criteria were locked into the database securingthat the required criteria for CD, UC or IBDU were met.General practitioners, specialists, other IBD units and patientself-help groups in the study areas were contacted twice duringthe inclusion period to ensure complete prospective recruitmentof patients. Patients younger than 15 years were included aspaediatric patients in the paediatric centres, with the exceptionof the centre from the Czech Republic which included patientsyounger than 18 years. The age limit of 15 years was the referralage and was decided on by agreement between all centres.Disease phenotype classification by disease extent for UC, aswell as disease location and behaviour for CD, were definedaccording to the Montreal classification10 which has previouslybeen shown to have overall good interobserver agreement.11 12
Induction therapy was defined as any medical or surgicaltreatment for IBD initiated within the first 3 months after diag-nosis. Medical treatment was categorised as: 5-aminosalicylates(5-ASA) (oral and/or topical 5-ASA treatment±topical steroids),steroids (oral steroids±azathioprine, 6-mercaptopurine, 5-ASAor topical steroids), immunomodulators (azathioprine,6-mercaptopurine, ciclosporin±steroids or methotrexate±steroids) or biological therapy (infliximab or adalimumab in com-bination with any of the above). Surgical treatment was definedas any surgery due to IBD within the first 3 months after diagno-sis (regardless of medical treatment prior to surgery).
Data collection and validityData regarding demographics, disease course, therapy and bloodsamples were collected at diagnosis and every third monththroughout the follow-up period, and data were prospectivelyentered by physicians and/or IBD specialist trained nurses intothe EpiCom database,13 a unique, tailor made and secure webbased inception cohort database, facilitating remote data inputfrom around the world in a cost effective way. Participants weretrained in using the database at the biannual EpiCom meetingsprior to and during the study. Furthermore, participants tookpart in the construction and validation process of the database.Built-in control and validation tests were used to enhanceinternal data validity. All data were standardised manually by JBto further improve data quality, and centres were asked tocorrect inconsistent information and to provide any missingdata if necessary.
A running overview bar of the cumulative number of regis-tered patients and corresponding annual incidence rates for eachcentre was implemented at the project website14 to encourageresearchers in entering the data and to meet the deadlines.
Significance of this study
How might it impact on clinical practice in theforeseeable future?▸ In this European population based cohort, diagnostic
procedures and initial medical treatment were not inaccordance with current guidelines.
▸ Follow-up of the EpiCom cohort will reveal the impact oftreatment choices on disease course.
▸ This web based epidemiological methodology has beenshown to be feasible and affordable regardless of priorexperience and cost constraints, and should be furtherdeveloped.
2 Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

Audits of case ascertainment and data quality were performedrandomly at 24 of 31 centres, followed by corrections if neces-sary. The centre from Finland was unable to supply full data onmedical treatment due to local restrictions.
Ethical considerationsThe study was approved by the local ethics committees accord-ing to local regulations.
Statistical methodsStatistical analyses were performed using SAS software V.9.2. Ageand gender standardised annual incidence rates for the adult popu-lation were obtained using the European Standard population15
with the age groups 0–14, 15–44, 45–64 and 65+years. The pur-chasing power parity (PPP) version of gross domestic product(GDP) was obtained for 2011 from the World Bank data service.16
For analysis of a possible GDP effect on IBD incidence, for each
centre the GDP (PPP version) of the corresponding country versusthe centre wise standardised IBD incidence rate (per 100 000population per year) was depicted. A p value of <0.05 was consid-ered statistically significant. The incidence gradient was analysedusing log linear (multiplicative) Poisson regression.
RESULTSA total of 1515 patients aged 15 years or older were diagnosedwith IBD in 2010. Of these, 535 (35%) patients were diagnosedwith CD, 813 (54%) with UC and 167 (11%) with IBDU. Intotal, 1259 (83%) patients were diagnosed in Western Europeanand 256 (17%) in Eastern European centres. Paediatric IBD wasdiagnosed in 45 patients (see web appendix available onlineonly). Patient demographics (table 1) were similar in the two geo-graphic regions, except for educational status. Nearly all cases ofIBDU (96%) were diagnosed in Western European centres.Disease classification (figures 1, 2) and smoking habits at
Table 1 Demographic characteristics of incident adult and paediatric patients with inflammatory bowel disease
Western European centres Eastern European centres**
Adult patients (≥15 years) CD UC IBDU CD UC IBDU
No of patients (n (%)) 430 (34) 668 (53) 161 (13) 105 (41) 145 (57) 6 (2)Males (n (%)) 220 (51) 375 (56) 78 (48) 63 (60) 82 (57) 4 (67)Age (years) (median (range; IQR)) 34 (16–89; 26) 39 (15–89; 27) 38 (16–84; 28) 32 (15–78; 21) 36 (18–81; 26) 30 (20–34; 5)Time from symptoms to diagnosis (months)(median (range; IQR))
4.6 (0–31 years;10 months)
2 (0–21 years;4.2 months)
2.4 (0–30 years;5.5 months)
3.4 (0–20 years;6.5 months)
2.2 (0–5 years;4.6 months)
2.7 (0–3 years;8.6 months)
Never smoker (n (%)) 170 (43) 311 (56) 70 (51) 39 (38) 77 (54) 4 (67)Current smoker (n (%)) 142 (36) 52 (9) 20 (15) 39 (38) 16 (11) 2 (33)Former smoker (n (%)) 88 (21) 196 (35) 46 (34) 25 (24) 51 (35) 0 (0)
Adult patients (≥15 years) Western European centres Eastern European centres
Educational status (n (%))*Completed academic education 191 (18) 53 (21)Completed non-academic education 564 (55) 131 (52)Currently in education 151 (15) 57 (23)No education 128 (12) 12 (5)
Employment status (n (%))**Employed 557 (53) 137 (54)Self-employed 63 (6) 12 (5)Unemployed 121 (11) 26 (10)Student 161 (15) 42 (17)Retired 157 (15) 36 (14)
Extraintestinal complications at diagnosis (n (%))**None 1085 (88) 221 (85)Skin 19 (2) 3 (1)Eyes 18 (2) 3 (1)
Joints 86 (7) 27 (10)Primary sclerosing cholangitis 5 (0) 2 (1)Pancreatitis 3 (0) 2 (1)Other 13 (1) 3 (1)
Western European centres Eastern European centres**
Paediatric patients CD UC IBDU CD UC IBDU
No of patients (n (%)) 9 (45) 9 (45) 2 (10) 6 (24) 18 (72) 1 (5)Males (n (%)) 5 (56) 3 (33) 1 (50) 3 (50) 8 (44) 1 (100)Age (years) (median (range; IQR)) 11 (6–14; 2.1) 12 (1–14; 1.9) 10 (7–14; 3.9) 10 (2–16; 6.2) 4 (1–16; 9.1) 9Time to diagnosis (months) (median(range; IQR))
4.1 (0.3–12.4; 2.2) 2.3 (0.6–5.8; 1.9) 1.9 (1.5–2.2; 0.3) 3.6 (2.0–17.0; 2.6) 2.7 (1.2–104.3; 4.3) 3.5
*p<0.01; **NS. p Values are given for comparison between the geographic regions.CD, Crohn’s disease; IBD, inflammatory bowel disease; IBDU, IBD unclassified; UC, ulcerative colitis.
Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636 3
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

diagnosis did not differ. In both Western and Eastern Europeancentres, more CD patients (36% and 38%) than UC patients (9%and 11%) were current smokers at the time of diagnosis(p<0.01) while more UC patients (35% and 35%) than CDpatients (21% and 24%) were former smokers (p<0.01).
Incidence in EuropeThe crude as well as age and gender adjusted incidence rates(per 100 000 per year) for UC, CD and IBDU in the selected
study areas are shown in table 2 and illustrated in figure 3. Theregional annual incidence rates for IBD combined, and for CD,UC and IBDU separately, differed significantly between Easternand Western Europe (p<0.01). The highest incidence of IBDwas found on the Faroe Islands (81.5 per100 000). The overallannual incidence rates in all Western European centres wereroughly twice as high as rates in all Eastern European centresfor CD (incidence rate ratio (IRR)=1.9, 95% CI 1.5 to 2.4) andUC (IRR=2.1, 95% CI 1.8 to 2.6). The median crude annualincidence rate for CD was 6.5 (range 0–10.7) in WesternEuropean centres and 3.1 (range 0.4–11.5) in Eastern Europeancentres whereas the median annual incidence rates for UC were10.8 (range 2.9–31.5) and 4.1 (range 2.4–10.3), respectively,and the median annual rates for IBDU were 1.9 (range 0–39.4)and 0 (range 0–1.2), respectively.
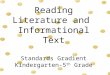
The observed incidences correlated with the GDP of eachcountry. The highest incidences were observed in countrieswith high GDP—that is, Western European centres (NorthernEurope and the Mediterranean region)—compared withregions with lower GDP (Eastern European centres) (figure 4).Analysing incidence rates depending on age, gender, regionand GDP, the IRR for IBD was 0.4 (95% CI 0.2 to 0.7) whencomparing Eastern with Western European centres for thesame age/gender group and GDP. High concordance prohibitedthe separation of the effects of GDP and geographic region inthis analysis. The variation in rates could thus be ascribed toeither factor.
Diagnostic proceduresAll UC patients were diagnosed using endoscopy (see web appen-dix available online only). A full colonoscopy was performed in524 (78%) UC patients from Western Europe compared with
Figure 2 Disease location andbehaviour at diagnosis for adultpatients with Crohn’s disease (NS).
Figure 1 Extent of disease at diagnosis for adult patients withulcerative colitis (UC) (NS).
4 Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

130 (90%) from Eastern European countries (p<0.01) while theremaining patients had a sigmoidoscopy performed as part oftheir diagnostic investigations (proctosigmoiditis patients, wherethe investigator reached normal tissue). For CD, 402 (93%)patients in Western and 101 (96%) in Eastern European countrieshad a colonoscopy performed, while 1% in both Western andEastern European countries only had a sigmoidoscopy per-formed during the diagnostic investigation (NS). For patientswith IBDU, 119 (74%) from Western Europe had a colonoscopycompared with six (100%) from Eastern Europe.
TreatmentThe initial treatment in Western and Eastern European centresduring the first 3 months of disease is shown in figure 5. Theobserved regional differences for UC and CD patients were signifi-cant (p<0.01). 5-ASA monotherapy was chosen as the initial treat-ment for 75 (18%) CD patients in Western Europe and for 33(31%) in Eastern Europe, with most patients receiving oral 5-ASAonly (66 (92%) and 29 (88%), respectively, NS). Of these patients,25 (35%) in Western Europe and six (18%) in Eastern Europe hadcolonic CD (NS). Of CD patients receiving steroids as the initial
Table 2 Incidence rates per 100 000 for inflammatory bowel disease, Crohn’s disease, ulcerative colitis and inflammatory bowel diseaseunclassified in Europe for patients aged 15 years or older in 2010
No ofpatients
IBDcrude
IBD adjusted(SE)
CDcrude
CD adjusted(SE)
UCcrude
UC adjusted(SE)
IBDUcrude
IBDU adjusted(SE)
Western European centresCyprus, Nicosia 27 11.2 11.4 (2.2) 6.2 6.3 (1.6) 2.9 3.0 (1.1) 2.1 2.2 (1.0)Denmark, Aarhus 55 21.2 20.7 (2.8) 8.5 8.2 (1.8) 10.8 10.6 (2.0) 1.9 1.8 (0.8)Denmark, Amager 23 17.2 16.3 (3.4) 5.2 4.8 (1.8) 7.5 7.4 (2.4) 4.5 4.1 (1.7)Denmark, Funen 123 30.7 33.4 (3.1) 10.7 11.4 (1.8) 18.7 20.1 (2.4) 1.2 1.4 (0.7)Denmark, Herlev 48 22.4 24.4 (3.6) 6.5 7.0 (1.9) 7.5 8.3 (2.1) 8.4 9.2 (2.2)Denmark, Herning 49 21.2 22.5 (3.3) 6.5 7.1 (1.9) 12.6 13.0 (2.5) 2.2 2.3 (1.1)Denmark, Viborg 37 24.6 26.7 (4.5) 8.6 9.6 (2.7) 14.6 15.7 (3.4) 1.3 1.4 (1.0)Faroe Islands 31 81.5 83.1 (15.0) 10.5 11.1 (5.6) 31.5 31.8 (9.3) 39.4 40.2 (10.5)Finland, Pirkanmaa 107 26.2 27.7 (2.7) 4.4 5.0 (1.2) 17.1 18.0 (2.2) 4.7 4.7 (1.1)Greece, Ioanninia 15 9.2 10.2 (2.6) 3.1 3.5 (1.6) 5.5 6.0 (2.0) 0.6 0.7 (0.7)Greenland 9 24.0 19.6 (6.6) 0.0 0 (0) 24.0 19.6 (6.6) 0.0 0 (0)Iceland 72 28.7 28.5 (3.4) 5.6 5.6 (1.5) 17.9 17.8 (2.7) 5.2 5.1 (1.4)Ireland, Adelaide and
Meath36 13.2 12.9 (2.2) 4.8 4.3 (1.2) 4.4 4.2 (1.2) 4.0 4.4 (1.4)
Israel, Beer Sheva 51 13.2 13.0 (1.9) 8.6 8.4 (1.5) 4.4 4.4 (1.1) 0.3 0.2 (0.2)Italy, Northern Italy 182 10.9 11.6 (0.9) 3.9 4.3 (0.5) 6.1 6.4 (0.7) 0.8 0.9 (0.3)Portugal, Vale de Sousa 31 11.1 10.8 (2.0) 7.2 7.0 (1.6) 3.9 3.8 (1.2) 0.0 0 (0)Spain, Vigo 102 20.4 21.4 (2.1) 10.2 10.8 (1.5) 9.0 9.4 (1.4) 1.2 1.2 (0.5)Sweden, Linköping 55 38.3 40.0 (5.4) 9.8 10.1 (2.7) 16.0 16.5 (3.5) 12.5 13.5 (3.2)Sweden, Örebro 39 26.5 28.3 (4.6) 7.5 8.3 (2.5) 15.6 16.1 (3.4) 3.4 3.9 (1.8)UK, Brent and Harrow 76 19.9 19.3 (2.2) 2.6 2.4 (0.8) 15.9 15.6 (2.0) 1.3 1.3 (0.6)UK, Hull and EastYorkshire
91 18.1 18.6 (2.0) 8.4 8.9 (1.4) 8.2 8.3 (1.3) 1.6 1.4 (0.5)
Eastern European CentresCroatia, Zagreb 12 6.3 6.6 (1.9) 3.1 3.3 (1.3) 3.1 3.3 (1.4) 0.0 0 (0)Czech Republic, Prague 22 12.2 12.7 (2.8) 5.5 5.6 (1.8) 5.5 5.8 (1.9) 1.1 1.3 (0.9)Czech Republic, SouthBohemia
42 7.7 7.9 (1.2) 3.8 3.9 (0.9) 3.8 3.9 (0.9) 0.0 0 (0)
Estonia, SouthernEstonia
30 10.3 11.0 (2.0) 5.2 5.4 (1.4) 5.2 5.7 (1.5) 0.0 0 (0)
Hungary, Veszpremprovince
58 23.0 24.0 (3.2) 11.5 12.0 (2.2) 10.3 10.7 (2.1) 1.2 1.3 (0.7)
Lithuania, Kaunas 32 8.5 9.1 (1.6) 2.4 2.6 (0.9) 6.1 6.5 (1.4) 0.0 0 (0)Moldova, Chisinau 10 4.3 3.9 (1.2) 0.4 0.4 (0.4) 3.9 3.5 (1.2) 0.0 0 (0)Romania, Timis 24 4.1 4.2 (0.9) 1.7 1.7 (0.5) 2.4 2.5 (0.7) 0.0 0 (0)Russia, Moscow 26 5.1 5.3 (1.1) 0.8 0.9 (0.5) 4.1 4.2 (0.9) 0.2 0.2 (0.2)
Regional incidence ratesNo ofpatients IBD (95% CI) CD (95% CI) UC (95% CI) IBDU (95% CI)
All Western Europeancentres
1259 18.5 (17.5 to 19.5)* 6.3 (5.7 to 6.9)* 9.8 (9.1 to 10.6)* 2.4 (2.0 to 2.8)*
All Eastern Europeancentres
256 8.1 (7.2 to 9.2) 3.3 (2.7 to 4.0) 4.6 (3.9 to 5.4) 0.2 (0.1 to 0,4)
All centres 1515 15.2 (14.4 to 16.0) 5.4 (4.9 to 5.8) 8.2 (7.6 to 8.7) 1.7 (1.4 to 1.9)
*Difference in incidence between the geographic regions p<0.01.CD, Crohn’s disease; IBD, inflammatory bowel disease; IBDU, IBD unclassified; UC, ulcerative colitis.
Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636 5
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

treatment, 152 (67%) in Western Europe and 53 (93%) in EasternEurope received prednisolone while the remaining patients weretreated with budesonide (p<0.01). Of patients receiving budeso-nide, 44 (58%) in Western Europe and two (50%) in EasternEurope had disease located in the terminal ileum (NS). Forpatients treated with prednisolone, these numbers were 45% inWestern Europe and 51% in Eastern Europe (NS). Most patientswith UC were treated with 5-ASA monotherapy as the initial treat-ment. Sixty-nine (44%) patients with left-sided colitis and19 (23%) with extensive colitis in Western Europe received com-bination therapy with oral and topical 5-ASA compared with21 (42%) and six (22%), respectively, in Eastern Europe. Of UCpatients with proctitis, 11 (11%) in Western Europe and five(19%) in Eastern Europe received oral 5-ASA only.
Biological therapyBiological treatment was administered to 29 (7%) CD patientsfrom Western European centres: 24 (83%) were treated withinfliximab and five (17%) with adalimumab. Five (17%) patients
were treated ‘top down’, with no medical treatment precedingbiological therapy, while the remaining patients were treatedwith combinations of steroids and either azathioprine and/or5-ASA. An equal proportion of six (21%) patients had strictur-ing or penetrating disease. In 20 (69%) cases, biological treat-ment was initiated due to refractoriness to other treatments.Only two (2%) CD patients from Eastern Europe receivedinfliximab due to refractoriness to other treatments. Of the 16(3%) UC patients from Western European centres who receivedbiological treatment, all received infliximab: three (19%) didnot receive any treatment before starting on biologicals whilethe remaining patients were treated with combinations of ster-oids and either azathioprine and/or 5-ASA or azathioprinealone. The indication for starting biological treatment wasrefractoriness to other treatments in 14 (88%) cases. Mostpatients (10 (63%)) had extensive colitis at diagnosis while theremaining patients had left-sided colitis. Four (3%) patients withIBDU received infliximab because of refractoriness to othertreatments (two patients), maintenance of remission (onepatient) or steroid dependency (one patient). Three patientsreceived steroids prior to starting biological treatment while onepatient received 5-ASA monotherapy. No association betweensmoking status at diagnosis and biological treatment wasobserved in any patient.
SurgeryResections were performed in 34 (8%) Western European CDpatients (including three hemicolectomies and one total colec-tomy) compared with eight (8%) Eastern European CD patients(one hemicolectomy). Stricturing disease occurred in 14 (41%)Western European patients and penetrating disease in 14 (41%)compared with two (26%) and five (63%), respectively, forEastern European patients (NS). The majority of patients(24 (73%) and 7 (88%)) received no medical treatment beforeundergoing surgery (NS). Seven (1%) Western European UCpatients (one with left-sided colitis and six with extensivecolitis) underwent a colectomy at diagnosis or during the first3 months of disease compared with one (1%) patient with
Figure 3 Incidence rates (/100 000) of cases aged 15 years or older for inflammatory bowel disease (IBD) in selected areas in Europe in 2010.
Figure 4 Inflammatory bowel disease (IBD) (Crohn’s disease/ulcerative colitis/inflammatory bowel disease unclassified) standardisedincidence rates versus 2010/2011 purchasing power parity (PPP) versionof gross domestic product (GDP).
6 Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

extensive colitis from Eastern Europe. All UC patientswere treated medically with steroids with or without immuno-modulators before undergoing surgery. No association betweensmoking status at diagnosis and risk of surgery was observed foreither CD or UC patients (NS). Two (1%) patients with IBDUfrom Western Europe had a total colectomy at diagnosis orduring the first 3 months of disease.
DISCUSSIONWe have presented what we believe is the first multicentre webbased inception cohort study of the incidence of IBD in Europe.The overall age and gender adjusted annual incidence rates per100 000 per year were 5.4 for CD, 8.2 for UC and 1.7 for IBDU.The combined annual incidence rates for CD and UC in allWestern European centres were twice as high as the rates in allEastern European centres. This gradient was smaller than origin-ally expected compared with the North–South gradient
previously observed17; this might be explained by a bias concern-ing case ascertainment in previous Eastern European studies.
All 31 participating centres performed a population basedstudy capturing all incident IBD patients in the catchment areaduring 2010. Several measures were used in order to secure thequality and validity of the incidence rates recorded. Diagnosticcriteria used for case definition, the time period of inclusion,the recorded patient data and the method of case ascertainmentwere standardised and consistent, and catchment areas were pre-cisely defined. The unification of methods constitutes a majorstrength of population based inception cohorts compared with,for example, Health Administrative Databases, where issues ofdata incompleteness compared with clinical records and codingerrors of diagnoses exist.18 19 Furthermore, by contacting alldepartments of gastroenterology, practising gastroenterologistsand general practitioners in the uptake areas during the inclu-sion period, prospective inclusion of all patients in the regionsdiagnosed with IBD was ensured. Audit visits and built-in data
Figure 5 Initial treatment during thefirst 3 months of disease in Easternand Western European centres.
Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636 7
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

control in the database guaranteed project protocol adherence,as well as extensive training of participating physicians andnurses in methodology prior to and during the study period atthe biannual EpiCom group meetings.
The reported IBD incidence rate on the Faroe Islands (81.5per 100 000 per year) is, to our knowledge, the highestreported incidence rate to date. Median age at diagnosis andtime to diagnosis did not differ from other Western Europeancentres (data not shown) and incidence rates for 2011 and 2012in the Faroe Islands did not differ significantly from the inci-dence rate found in 2010 (K Nielsen, personal communication).A previous study found a mean incidence rate of 23.9 per100 000 for 1981–198820 on the Faroe Islands. The presentmajor increase in incidence could have been caused by environ-mental factors21 (eg, special dietary habits) in combination witha genetic burden.22 Another interesting observation was theHungarian incidence of IBD (23 per100 000), which was thehighest Eastern European incidence and equalled WesternEuropean incidences. This finding is in line with previousreports,2 and as Hungary is one of the wealthier EasternEuropean countries in terms of GDP, may be the result of amore westernised way of life. The analysis suggests that lifestylevariations, expressed by geographic lifestyle differences com-bined with PPP, influence IBD incidence and suggests that therisk of IBD is linked to the developmental status of the geo-graphic region/country.
Additionally, previous population based studies have shownthat 5–7% of all cases of IBD occur in children <15 years ofage.23 24 In this inception cohort, however, only 45 (3%) out of1560 IBD cases were paediatric onset IBD cases. As many centresparticipating in the study are low incidence areas, and since thepaediatric incidence rates observed during 2010 do not differfrom previously reported rates from the same countries orregions,25 26 the observed number of incident paediatric onsetIBD patients is likely to resemble the true number of cases.
The geographic regions of Eastern and Western Europe weresurprisingly similar in terms of sociodemographic characteristics,time to diagnosis and smoking habits. In accordance with theavailable literature, more CD patients were smokers at the timeof diagnosis and more UC patient were former smokers,27 28
and this was the case in both regions. In addition, the anatom-ical location, disease extent and behaviour at the time of diagno-sis showed little overall difference. The diagnostic approach forCD and UC seemed similar in Eastern and Western Europe andin accordance with the international guidelines for IBD29–34 asalmost 90% of all IBD patients had a full colonoscopy per-formed as part of the diagnostic workup. However, only 78%of Western European UC patients and 73% of IBDU patientshad a full colonoscopy performed, compared with 90% and100% in Eastern Europe.
The IBD patients included in this population based inceptioncohort were unselected and represented the broad spectrum ofdisease from indolent to severe cases. It is therefore unsurprisingthat international guidelines for the diagnosis and treatment ofIBD are not being followed at ‘the clinical frontier’. The obser-vation that 21% of CD patients were treated with 5-ASA mono-therapy for induction offers one such example: the efficacy of5-ASA for inducing remission in CD patients remains uncer-tain35 and consequently current guidelines do not recommend5-ASA for CD.34 36 In a Danish cohort of CD patients, a mildphenotype of patients was recognised as responders to 5-ASAand were furthermore characterised as dependent on 5-ASAtreatment, thus benefiting from monotherapy for a median of3 years.37 38 Also, budesonide, recommended as the first choice
of treatment for ileocaecal CD,36 has recently not shown super-iority to 5-ASA,38 and 5-ASA is recommended during pregnancydue to its low toxicity,39 40 which could partly explain theobserved high frequency of 5-ASA as the initial treatment in CDpatients.
With regards to steroid treatment in CD, 33% of WesternEuropean and 7% of Eastern European patients were treatedwith budesonide. Yet only 62% and 50%, respectively, had thedisease located in the terminal ileum. Furthermore, althoughcurrent guidelines recommend topical therapy with 5-ASA foractive proctitis, and combined therapy with both oral andtopical 5-ASA for mildly to moderately active left-sided andextensive colitis,41 these were not followed uniformly by partici-pating physicians. Socioeconomic considerations regarding treat-ment options influence the choice of treatment, just as patientpreferences do, and these might be influenced by psychologicaldistress, patient beliefs about medication or a discordantdoctor–patient relationship.42 Also, differences in disease man-agement are strongly linked to extra-medical considerations andnot necessarily linked to the disease itself, while the comparisonmight be further complicated by major differences betweenhealth systems across Europe.
Surgery rates for CD have been declining in the past twodecades.43 In a Danish population based cohort, 12% of CDpatients diagnosed between 2003 and 2005 had a resection per-formed within the first year after diagnosis.9 Similarly, in apopulation based study from Hungary, CD patients diagnosedbetween 2002 and 2006 reported a surgery rate of 9.8% after1 year.44 The present study found that surgery rates within thefirst 3 months were already close to what is seen at 1 year ofdiagnosis, representing unavoidable surgeries. Biological treat-ment within the first 3 months of disease was administered in7% of CD and 3% of UC patients from Western Europe. Thisrapid escalation of therapy might be the result of the ‘era ofmucosal healing’ as an important treatment goal45 as well as theuse of biological as medical rescue therapy.46 Almost 20% ofboth CD and UC patients treated with biologicals were treated‘top down’ and did not receive any other treatment prior tobiologicals.
In the present study we have shown that it is possible toperform a large, entirely web based, epidemiological populationbased cohort study throughout Europe in 31 centres. The data-base is inexpensive with low maintenance costs, is easy to useand facilitates direct remote data input. Most centres had notperformed population based inception cohort studies before butthis innovative methodology enabled participation regardless ofprior experience and cost constraints. The web based epidemio-logical concept is feasible and the data it generates are valid,robust and consistent.
The EpiCom study has created this inception cohort, as wellas the related database, as a framework for more epidemio-logical studies to further analyse the impact of treatment choiceson disease course during follow-up observation in 2010–2015of the EpiCom cohort, as well as the impact of environmentalfactors.
Author affiliations1Digestive Disease Centre, Medical Section, Herlev University Hospital, Copenhagen,Denmark2Division of Gastroenterology and Hepatology, University Hospital Centre Zagreb,University of Zagreb School of Medicine, Zagreb, Croatia3Nicosia private practice, Nicosia, Cyprus4IBD Centre ISCARE, Charles University, Prague, Czech Republic5Gastroenterology Department, Hospital České Budějovice, České Budějovice,Czech Republic
8 Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

6Department of Medicine, Amager Hospital, Amager, Denmark7Department of Medicine, Herning Central Hospital, Herning, Denmark8Medical Department, Viborg Regional Hospital, Viborg, Denmark9Medical Department, Hospital of Southern Jutland, Aabenraa, Denmark10University of Southern Denmark, Odense, Denmark11Department of Medicine V (Hepatology and Gastroenterology), Aarhus UniversityHospital, Arhus, Denmark12Division of Endocrinology and Gastroenterology, Tartu University Hospital, Tartu,Estonia13Medical Department, The National Hospital of the Faroe Islands, Torshavn,Faroe Islands14Department of Gastroenterology and Alimentary Tract Surgery, Tampere UniversityHospital, Tampere, Finland151st Division of Internal Medicine and Hepato-Gastroenterology Unit, UniversityHospital, Ioannina, Greece16Medical Department, Dronning Ingrids Hospital, Nuuk, Greenland171st Department of Medicine, Semmelweis University, Budapest, Hungary18Department of Internal Medicine, Section of Gastroenterology and Hepatology,The National University Hospital, Reykjavik, Iceland19Department of Gastroenterology, Adelaide and Meath Hospital, TCD, Dublin,Ireland20Department of Gastroenterology and Hepatology, Soroka Medical Centre andBen Gurion University of the Negev, Beer Sheva, Israel21UO Gastroenterologia, Azienda Ospedaliera—Università di Padova, Padova, Italy22UO di Medicina e Gastroenterologia, Az Ospedaliera Ospedale di Cremona,Cremona, Italy23UO di Gastroenterologia e Endoscopia Digestiva, Az Ospedaliera OspedaleMaggiore di Crema, Crema, Italy24Gastroenterology Unit, Careggi Hospital, Florence, Italy25UO Gastroenterologia ed Endoscopia Digestiva, Ospedale Morgagni—Pierantoni,Forlì, Italy26UO Medicina 3° e Gastroenterologia, Azienda Ospedaliera Arcispedale S MariaNuova, Reggio Emilia, Italy27Institute for Digestive Research, Lithuanian University of Health Sciences, Kaunas,Lithuania28Department of Gastroenterology, State University of Medicine and Pharmacy of theRepublic of Moldova, Chisinau, Republic of Moldova29Department of Paediatric Gastroenterology, Centre of Mother and Child, Chisinau,Republic of Moldova30Department of Gastroenterology, Hospital de São João, Porto, Portugal31Institute of Pharmacology and Therapeutics, Oporto Medical School, Porto,Portugal32Institute for Molecular and Cell Biology, University of Porto, Porto, Portugal33Hospital de Vale de Sousa, Porto, Portugal34Clinic of Gastroenterology, University of Medicine ‘Victor Babes’, Timisoara,Romania35Department of Gastroenterology, Moscow Regional Research Clinical Institute,Moscow, Russia36Gastroenterology Department, Complexo Hospitalario Universitario de Vigo, Vigo,Spain37Division of Gastroenterology and Hepatology, Department of Clinical andExperimental Medicine, Linköping University, Linköping, Sweden38Department of Gastroenterology/UHL, County Council of Östergötland, Linköping,Sweden39Department of Medicine, Division of Gastroenterology, Örebro University Hospital,Örebro, Sweden40School of Health and Medical Sciences, Örebro University, Örebro, Sweden41Sir Alan Park's Physiology Unit, St Mark's Hospital, Imperial College London,London, UK42Hull and East Yorkshire NHS Trust and Hull and York Medical School, Hull RoyalInfirmary, Hull, UK43Department of Medical Gastroenterology, Gentofte Hospital, Copenhagen,Denmark
Acknowledgements We are thankful for the academic support from the head ofthe former EC-IBD group Professor R Stockbrügger. We are grateful to B Vucelic(Croatia), N Turk (Croatia), N Procopiou (Cyprus), B Järventaus (Finaland), V Tsianos(Greece), K Stroggili (Greece), Z Vegh (Hungary), S Kramli (Hungary), P Bodini(Cremona, Italy), A Santini (Florence, Italy), D Valpiani (Forlì, Italy), S Lombardini(Reggio Emilia, Italy), L Jonaitis (Lithuania), I Valantiene (Lithuania), L Sanromán(Spain), C Salgado (Spain), UB Widén (Sweden) and C Tysk (Sweden) for theircontribution to patient inclusion and entering of data. Furthermore, we wish tothank HD Support LLC for their work on developing the web based interactivedatabase solution in Europe, experienced from the Danish Crohn Colitis Database(DCCD), as well as Henrik Wachman, Larix Ltd, for statistical support.
Contributors All authors have made significant contributions to the researchdescribed in this manuscript. JB carried out the study, collected and analysed the
data, and drafted the manuscript. All authors collected and entered data, andrevised the draft of the manuscript. PM took part in the planning and designing ofthe study, and revised the draft of the manuscript. All authors read and approvedthe final manuscript. JB, PM, PLL, NP, ST, LK, RS, EVT, MM, ADP, Patrizia Politi,Alessia Santini and MB performed the audit visits.
Funding The authors thank the Danish Colitis Crohn Patients Organisation (CCF), theVibeke Binder and Povl Riis’ Foundation, the Scientific Council at Herlev Hospital, theSigrid Rigmor Moran Foundation, Aage and Johanne Louis-Hansens Foundation, theMunkholm Foundation, the CC Klestrup and Henriette Klestrup Foundation, the Knudand Dagny Gad Andresens Foundation, the Else and Mogens Wedell-WedellsborgsFoundation, the Direktør Jacob Madsen and Olga Madsens Foundation, ScanVet, theTorben og Alice Frimodt Foundation, Bengt Ihre’s Foundation, Nanna Svartz’Foundation, Örebro University Hospital Research Foundation, Örebro County ResearchFoundation, the Swedish Foundation for Gastrointestinal Research, the SwedishResearch Council, the Swedish Society of Medicine, the Research Council of South-EastSweden, the County Council of Östergötland, the Swedish Organization for the study ofinflammatory bowel disease and the European Crohn’s and Colitis Organisation’s(ECCO) for their unrestricted grant support.
Competing interests None.
Ethics approval The study was approved by the local ethics committees accordingto local regulations.
Provenance and peer review Not commissioned; externally peer reviewed.
REFERENCES1 Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the
inflammatory bowel diseases with time, based on systematic review.Gastroenterology 2012;142:46–54. e42; quiz e30.
2 Lakatos L, Mester G, Erdelyi Z, et al. Striking elevation in incidence and prevalenceof inflammatory bowel disease in a province of western Hungary between 1977–2001. World J Gastroenterol 2004;10:404–9.
3 Sincić BM, Vucelić B, Persić M, et al. Incidence of inflammatory bowel disease inPrimorsko-goranska County, Croatia, 2000–2004: a prospective population-basedstudy. Scand J Gastroenterol 2006;41:437–44.
4 Burisch J, Jess T, Martinato M, et al. The burden of inflammatory bowel disease inEurope. J Crohn’s Colitis 2013;7:322–37.
5 Burisch J, Munkholm P. Is there an east west incidence gradient in IBD in Europecaused by environmental factors and vitamin D level? ECCO News 2009;10–1.
6 HD-Support LLC. http://www.hd-support.dk/ (accessed 1 Feb 2013).7 Munkholm P. Crohn’s disease—occurrence, course and prognosis. An epidemiologic
cohort-study. Dan Med Bull 1997;44:287–302.8 Langholz E. Ulcerative colitis. An epidemiological study based on a regional
inception cohort, with special reference to disease course and prognosis. Dan MedBull 1999;46:400–15.
9 Vind I, Riis L, Jess T, et al. Increasing incidences of inflammatory bowel disease anddecreasing surgery rates in Copenhagen City and County, 2003–2005: a population-based study from the Danish Crohn colitis database. Am J Gastroenterol2006;101:1274–82.
10 Silverberg MS, Satsangi J, Ahmad T, et al. Toward an integrated clinical, molecularand serological classification of inflammatory bowel disease: Report of a WorkingParty of the 2005 Montreal World Congress of Gastroenterology. Can JGastroenterol 2005;19(Suppl A):5–36.
11 Riis L, Munkholm P, Binder V, et al. Intra- and interobserver variation in the use ofthe Vienna classification of Crohn’s disease. Inflamm Bowel Dis 2005;11:657–61.
12 Krishnaprasad K, Andrews JM, Lawrance IC, et al. Inter-observer agreement forCrohn’s disease sub-phenotypes using the Montreal Classification: how good arewe? A multi-centre Australasian study. J Crohn’s Colitis 2012;6:287–93.
13 Burisch J, Cukovic-Cavka S, Kaimakliotis I, et al. Construction and validation of aweb-based epidemiological database for inflammatory bowel diseases in Europe AnEpiCom study. J Crohn’s Colitis 2011;5:342–9.
14 EpiCom project website. http://www.epicom-ecco.eu (accessed 1 Feb 2013).15 Ahmad OB, Boschi-pinto C, Lopez AD. Age standardization of rates: a new WHO
standard. Geneva: World Health Organization, 2001.16 World Bank. World development indicators database. data.worldbank.org (accessed
9 Jul 2012).17 Shivananda S, Lennard-Jones J, Logan R, et al. Incidence of inflammatory bowel
disease across Europe: is there a difference between north and south? Results ofthe European collaborative study on inflammatory bowel disease (EC-IBD). Gut1996;39:690–7.
18 Majholm B, Bartholdy J, Christoffersen JK, et al. Poor agreement between data fromthe national patient registry and the Danish Patient Insurance Association. Dan MedJ 2012;59:A4430.
19 Agergaard P, Hebert A, Bjerre J, et al. Children diagnosed with congenital cardiacmalformations at the national university departments of pediatric cardiology:positive predictive values of data in the Danish National Patient Registry. ClinEpidemiol 2011;3:61–6.
Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636 9
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

20 Róin F, Róin J. Inflammatory bowel disease of the Faroe Islands, 1981–1988.A prospective epidemiologic study: primary report. Scand J Gastroenterol Suppl1989;170:44–6.
21 Weihe P, Joensen HD. Dietary recommendations regarding pilot whale meat andblubber in the Faroe Islands. Int J Circumpolar Health 2012;71:18594.
22 Als TD, Jorgensen TH, Børglum AD, et al. Highly discrepant proportions of femaleand male Scandinavian and British Isles ancestry within the isolated population ofthe Faroe Islands. Eur J Hum Genet: EJHG 2006;14:497–504.
23 Langholz E, Munkholm P, Krasilnikoff PA, et al. Inflammatory bowel diseases withonset in childhood. Clinical features, morbidity, and mortality in a regional cohort.Scand J Gastroenterol 1997;32:139–47.
24 Auvin S, Molinié F, Gower-Rousseau C, et al. Incidence, clinical presentation andlocation at diagnosis of pediatric inflammatory bowel disease: a prospectivepopulation-based study in northern France (1988–1999). J Pediatr GastroenterolNutr 2005;41:49–55.
25 Jakobsen C, Paerregaard A, Munkholm P, et al. Paediatric inflammatory boweldisease during a 44-year period in Copenhagen County: occurrence, course andprognosis—a population-based study from the Danish Crohn Colitis Database. Eur JGastroenterol Hepatol 2009;21:1291–301.
26 Martín-de-Carpi J, Rodríguez A, Ramos E, et al. Increasing incidence of pediatricinflammatory bowel disease in Spain (1996–2009): The SPIRIT Registry. InflammBowel Dis 2013;19:73–80.
27 Thomas GA, Rhodes J, Green JT. Inflammatory bowel disease and smoking—areview. Am J Gastroenterol 1998;93:144–9.
28 Higuchi LM, Khalili H, Chan AT, et al. A prospective study of cigarette smoking andthe risk of inflammatory bowel disease in women. Am J Gastroenterol2012;107:1399–406.
29 Dignass A, Eliakim R, Magro F, et al. Second European evidence-based consensuson the diagnosis and management of ulcerative colitis part 1: definitions anddiagnosis. J Crohn’s Colitis 2012;6:965–90.
30 Van Assche G, Dignass A, Panes J, et al. The second European evidence-basedconsensus on the diagnosis and management of Crohn’s disease: definitions anddiagnosis. J Crohn’s Colitis 2010;4:7–27.
31 Kornbluth A, Sachar DB. Ulcerative colitis practice guidelines in adults: AmericanCollege of Gastroenterology, Practice Parameters Committee. Am J Gastroenterol2010;105:501–23.
32 Lichtenstein GR, Hanauer SB, Sandborn WJ. Management of Crohn’s disease inadults. Am J Gastroenterol 2009;104:465–83.
33 Turner D, Levine A, Escher JC, et al. Management of pediatric ulcerative colitis: jointECCO and ESPGHAN evidence-based consensus guidelines. J Pediatr GastroenterolNutr 2012;55:340–61.
34 Mowat C, Cole A, Windsor A, et al. Guidelines for the management ofinflammatory bowel disease in adults. Gut 2011;60:571–607.
35 Ford AC, Kane S V, Khan KJ, et al. Efficacy of 5-aminosalicylates in Crohn’sdisease: systematic review and meta-analysis. Am J Gastroenterol2011;106:617–29.
36 Dignass A, Van Assche G, Lindsay JO, et al. The second European evidence-basedconsensus on the diagnosis and management of Crohn’s disease: currentmanagement. J Crohn’s Colitis 2010;4:28–62.
37 Duricova D, Pedersen N, Elkjaer M, et al. 5-Aminosalicylic acid dependency inCrohn’s disease: a Danish Crohn Colitis Database study. J Crohn’s Colitis2010;4:575–81.
38 Tromm A, Bunganič I, Tomsová E, et al. Budesonide 9 mg is at least as effective asmesalamine 4.5 g in patients with mildly to moderately active Crohn’s disease.Gastroenterology 2011;140:425–34.
39 Van der Woude CJ, Kolacek S, Dotan I, et al. European evidenced-basedconsensus on reproduction in inflammatory bowel disease. J Crohn’s Colitis2010;4:493–510.
40 Vermeire S, Carbonnel F, Coulie PG, et al. Management of inflammatory boweldisease in pregnancy. J Crohn’s Colitis 2012;6:811–23.
41 Dignass A, Lindsay JO, Sturm A, et al. Second European evidence-based consensuson the diagnosis and management of ulcerative colitis Part 2: current management.J Crohn’s Colitis 2012;6:991–1030.
42 Elkjaer M, Moser G, Reinisch W, et al. IBD patients need in health quality of careECCO consensus. J Crohn’s Colitis 2008;2:181–8.
43 Bernstein CN, Loftus E V, Ng SC, et al. Hospitalisations and surgery in Crohn’sdisease. Gut 2012;61:622–9.
44 Lakatos L, Kiss LS, David G, et al. Incidence, disease phenotypeat diagnosis, and early disease course in inflammatorybowel diseases in Western Hungary, 2002–2006. Inflamm Bowel Dis2011;17:2558–65.
45 Neurath MF, Travis SPL. Mucosal healing in inflammatory bowel diseases: asystematic review. Gut 2012;61:1619–35.
46 Järnerot G, Hertervig E, Friis-Liby I, et al. Infliximab as rescue therapy in severe tomoderately severe ulcerative colitis: a randomized, placebo-controlled study.Gastroenterology 2005;128:1805–11.
10 Burisch J, et al. Gut 2013;0:1–10. doi:10.1136/gutjnl-2013-304636
Inflammatory bowel disease
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

doi: 10.1136/gutjnl-2013-304636 published online April 20, 2013Gut
J Burisch, N Pedersen, S Cukovic-Cavka, et al. ECCO-EpiCom inception cohortinflammatory bowel disease in Europe: the
West gradient in the incidence of−East
http://gut.bmj.com/content/early/2013/04/19/gutjnl-2013-304636.full.htmlUpdated information and services can be found at:
These include:
Data Supplement http://gut.bmj.com/content/suppl/2013/04/18/gutjnl-2013-304636.DC1.html
"Supplementary Data"
References http://gut.bmj.com/content/early/2013/04/19/gutjnl-2013-304636.full.html#ref-list-1
This article cites 41 articles, 4 of which can be accessed free at:
P<P Published online April 20, 2013 in advance of the print journal.
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
CollectionsTopic
(980 articles)Ulcerative colitis � (612 articles)Endoscopy �
(1113 articles)Colon cancer � (846 articles)Crohn's disease �
Articles on similar topics can be found in the following collections
(DOIs) and date of initial publication. publication. Citations to Advance online articles must include the digital object identifier citable and establish publication priority; they are indexed by PubMed from initialtypeset, but have not not yet appeared in the paper journal. Advance online articles are Advance online articles have been peer reviewed, accepted for publication, edited and
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from

Notes
(DOIs) and date of initial publication. publication. Citations to Advance online articles must include the digital object identifier citable and establish publication priority; they are indexed by PubMed from initialtypeset, but have not not yet appeared in the paper journal. Advance online articles are Advance online articles have been peer reviewed, accepted for publication, edited and
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on April 21, 2013 - Published by gut.bmj.comDownloaded from