Embed Size (px)
Citation preview

Organization ofOrganization of Health Care Health Care
Presentation to ITTP ClassPresentation to ITTP Class
January 7, 2004January 7, 2004
John E. Billi, M.D.John E. Billi, M.D.
Professor, Internal Medicine and Medical EducationProfessor, Internal Medicine and Medical Education
Associate Dean, Clinical AffairsAssociate Dean, Clinical Affairs
Associate Vice President, Medical AffairsAssociate Vice President, Medical Affairs
[email protected]@umich.edu

Organization of Health CareOrganization of Health Care
Who are the players and what Who are the players and what are their interests?are their interests?
Who are the patients?Who are the patients? How is care funded?How is care funded? Who employs the doctors?Who employs the doctors? Who owns the facilities?Who owns the facilities? Who is at financial risk?Who is at financial risk? Who is accountable for quality Who is accountable for quality
and cost effectiveness of care?and cost effectiveness of care?

Ten Issues Will Shape the Future of Ten Issues Will Shape the Future of Health CareHealth Care
The economyThe economy Medical scienceMedical science Education in the health professions, shortages Education in the health professions, shortages Technology, innovation and communicationTechnology, innovation and communication Population shifts – baby boomers and the elderlyPopulation shifts – baby boomers and the elderly Consumerism, choice and informationConsumerism, choice and information Organization and financing of health careOrganization and financing of health care The shrinking world - globalizationThe shrinking world - globalization The environmentThe environment AccountabilityAccountability
Source: Adapted from W. Peck, M.D., Washington Univ.

Organization of Health Care:Organization of Health Care:The PlayersThe Players
Patient&
Family
Source: Marilynn Rosenthal, Ph.D.
PhysiciansM.D.s & D.OsNurses
OtherAllied HealthProfessionals
Hospitals Nursing Homes, SNFs
Pharmacists
Dentists
NPs, RNs, LPNs, MAs, Aides
Ambulatory Surgery Centers
Physician Offices
Home Care
PAs
ChiropractorsOptometrists
Employers$$$
Insurers[$]
Government$$$
TBIUnit
Urgent Care Center
Social Workers
Individuals$
Podiatrists

New Roles for Health New Roles for Health ProfessionalsProfessionals
Nursing shortageNursing shortage- Medical Assistants Medical Assistants
Mid-level providersMid-level providers- Nurse Practitioners, Midwives, AnesthetistsNurse Practitioners, Midwives, Anesthetists- Physician AssistantsPhysician Assistants- Optometrists, PsychologistsOptometrists, Psychologists
Technicians: surgery, radiology…Technicians: surgery, radiology… Care managersCare managers Home care providersHome care providers Complementary / ”integrated” medicine providersComplementary / ”integrated” medicine providers
Health Care Expenditures Health Care Expenditures (Year 2001)(Year 2001)
$1.4 trillion $1.4 trillion 14.1% of Gross Domestic Product (GDP)14.1% of Gross Domestic Product (GDP) $5,035 per capita = $420/month (or PMPM)$5,035 per capita = $420/month (or PMPM) Hospital spending accounts for largestHospital spending accounts for largest
share (32%)share (32%) Drugs $ are fastest-growing category (14%)Drugs $ are fastest-growing category (14%) Spending growth in health careSpending growth in health care continues tocontinues to
outpace growth of GDPoutpace growth of GDP
Source: http://www.cms.hhs.gov/statisticsHighlights---National Health Expenditures 2001

8
10
12
14
16
1980 1984 1988 1992 1996 2000
Source: CMS, Office of the Actuary, National Health Statistics Group.
Calendar Years
Pe
rce
nt
of
GD
P
Period of accelerated growth
Period of stabilization
Rapid growth in the health spending share of GDP stabilized beginning in 1993.
National Health Expenditures as a Share National Health Expenditures as a Share of Gross Domestic Product (GDP)of Gross Domestic Product (GDP)
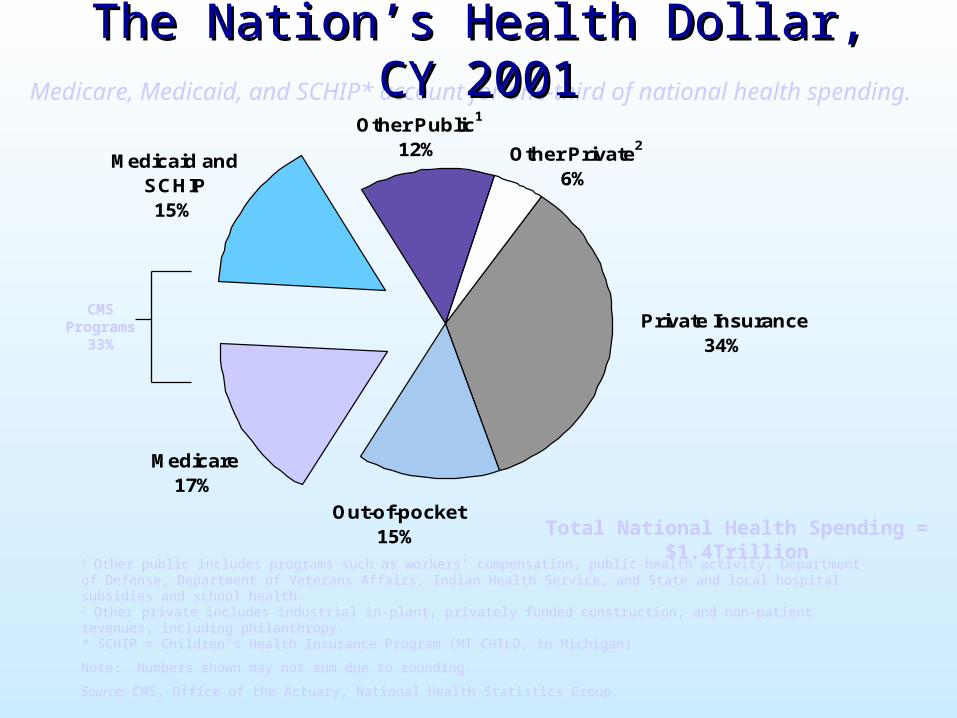
Private Insurance34%
Other Public1
12% Other Private2
6%Medicaid and
SCHIP15%
Out-of-pocket15%
Medicare17%
1 Other public includes programs such as workers’ compensation, public health activity, Department of Defense, Department of Veterans Affairs, Indian Health Service, and State and local hospital subsidies and school health.2 Other private includes industrial in-plant, privately funded construction, and non-patient revenues, including philanthropy.* SCHIP = Children’s Health Insurance Program (MI CHILD, in Michigan)
Note: Numbers shown may not sum due to rounding.
Source: CMS, Office of the Actuary, National Health Statistics Group.
CMSPrograms
33%
Medicare, Medicaid, and SCHIP* account for one-third of national health spending.
Total National Health Spending = $1.4Trillion
The Nation’s Health Dollar, CY 2001The Nation’s Health Dollar, CY 2001

Health Care ExpendituresHealth Care Expenditures (Year 2001)(Year 2001)
Hospital Care32%
Physician & Clinical Services
22%
Other (dental, home heath,
DME…)23%
Program Admin.
6%
Prescription Drugs10%
Nursing Homes
7%
Source: CMS, Office of the Actuary, National Health Statistics Group

National Health Expenditures -National Health Expenditures -Accelerating GrowthAccelerating Growth
Health care spending increasedHealth care spending increased 8.7 percent in 2001 8.7 percent in 2001
Accelerating growth factors:Accelerating growth factors:- rising health sector wagesrising health sector wages- increased Medicare spendingincreased Medicare spending- increasing insurance premiumsincreasing insurance premiums- more technology, more costly drugsmore technology, more costly drugs- consumer demand for less restrictive consumer demand for less restrictive
insurance plansinsurance plans
Source: http://www.cms.gov.stats

Accelerating Growth: Accelerating Growth: ImplicationsImplications
Public/private initiatives to slow pace of Public/private initiatives to slow pace of spending growthspending growth
Trade-offs between health care and Trade-offs between health care and competing prioritiescompeting priorities
Consumers asked to contribute more Consumers asked to contribute more towards coveragetowards coverage
Choice of plans, providers and benefits Choice of plans, providers and benefits may be narrowedmay be narrowed
Source: http://cms.hhs.gov/statistics
The Coming Train WreckThe Coming Train Wreck......
Aging, growing population Dramatic advances in clinical capabilities Information technology requirements 43 million uninsured Unbounded patient demands
vs. Taxpayer, employer, individual
willingness to pay

Health Care Paradigm ShiftHealth Care Paradigm Shift
PhysiciansPhysicians
Solo PracticeSolo Practice
HospitalsHospitals
Free-standing,Free-standing,
communitycommunity
InsuranceInsurance
IndemnityIndemnity
PurchasersPurchasers
PassivePassive
Group Practice orEmployed
Networks & IntegratedDelivery Systems
Managed Care
“Prudent Purchaser”as Proactive Partner(cost shifts, drop insurance)
Performance- based Models(more choice, PPOs)
Privatized

Health Care Paradigm ShiftHealth Care Paradigm Shift
PhysiciansPhysicians
Solo PracticeSolo Practice
HospitalsHospitals
Free-standing,Free-standing,
communitycommunity
InsuranceInsurance
IndemnityIndemnity
PurchasersPurchasers
PassivePassive
Group Practice orEmployed
Networks & IntegratedDelivery Systems
Managed Care
“Prudent Purchaser”as Proactive Partner(cost shifts, drop insurance)
Performance- based Models(more choice, PPOs)
Privatized
Physician RolesPhysician Roles
Traditional:Traditional: Self-employedSelf-employed
Solo practiceSolo practice Single specialty groupsSingle specialty groups Fee-for-service Fee-for-service
reimbursement for care reimbursement for care of individual patientsof individual patients
Open access to any Open access to any doctordoctor
AutonomyAutonomy
Managed Care Era:Managed Care Era: Employed (then Employed (then
privatized)privatized) Group practiceGroup practice Multi-specialty groups Multi-specialty groups Capitated for care ofCapitated for care of
a populationa population(shared $ (shared $
risk)risk) Primary care Primary care
physician gatekeeperphysician gatekeeper(wax and wane)(wax and wane)
AccountabilityAccountability
Physician Payment ModelsPhysician Payment Models
Traditional: fee-for-serviceTraditional: fee-for-service““Do more - make more”Do more - make more”
Capitation: fixed payment per member Capitation: fixed payment per member per month (pmpm)per month (pmpm)““Do less - make more”Do less - make more”
Future: fee-for-benefit &Future: fee-for-benefit &performance-based contractingperformance-based contracting““Do the right thing”Do the right thing”

Evolution of Evolution of Physician OrganizationsPhysician Organizations
Early structure:Early structure:- Group PracticeGroup Practice
• single specialty single specialty • multispecialtymultispecialty
Managed care contracting organizations:Managed care contracting organizations:- IPA - Independent Practice AssociationsIPA - Independent Practice Associations- Physician Organizations (POs)Physician Organizations (POs)- Physician Hospital Organizations (PHOs)Physician Hospital Organizations (PHOs)
Recent developments:Recent developments:- Second Generation Physician Organizations Second Generation Physician Organizations - Physicians within Integrated Delivery SystemsPhysicians within Integrated Delivery Systems

What should Physician What should Physician Organizations do?Organizations do?
Traditional roles:Traditional roles: Contract negotiations with HMOsContract negotiations with HMOs Negotiations with hospitalsNegotiations with hospitals Support office operations, billing…Support office operations, billing…
Emerging roles - Assist physicians to:Emerging roles - Assist physicians to: Improve efficiencyImprove efficiency Improve quality of careImprove quality of care
ToolsTools Physician profiling (quality and appropriateness)Physician profiling (quality and appropriateness) Evidence-based practice guidelinesEvidence-based practice guidelines Disease management programsDisease management programs

Traditional CareTraditional Care
Episodic, uncoordinatedEpisodic, uncoordinated Focused on the acutely illFocused on the acutely ill Patient initiatedPatient initiated Patient education is sporadicPatient education is sporadic Communication among clinicians is sporadicCommunication among clinicians is sporadic
- Information scattered on paperInformation scattered on paper Process of care is variable Clinicians’ Clinicians’ opinionsopinions drive decisions drive decisions ExpensiveExpensive

““Crossing the Quality Chasm”Crossing the Quality Chasm”
Health care should be:Health care should be: SafeSafe EffectiveEffective Patient-centeredPatient-centered TimelyTimely EfficientEfficient Equitable - not vary due to gender, ethnicity, Equitable - not vary due to gender, ethnicity,
geography, socioeconomic statusgeography, socioeconomic status
Source: Crossing the Quality Chasm: A New Health System for the 21st Century, Institute of Medicine, National Academy of Sciences, 2000.

Professional Values - EnduringProfessional Values - Enduring Altruism Altruism
- patients’ interests come firstpatients’ interests come first Commitment to self-improvementCommitment to self-improvement
- master and incorporate new knowledgemaster and incorporate new knowledge- contribute to the knowledge base of the contribute to the knowledge base of the
disciplinediscipline Peer reviewPeer review
- collective sense of responsibility and collective sense of responsibility and accountability among medical professionals accountability among medical professionals for the conduct of colleaguesfor the conduct of colleagues
Source: D Blumenthal, Health Affairs, Spring (I) 1994

Health Care Paradigm ShiftHealth Care Paradigm Shift
PhysiciansPhysicians
Solo PracticeSolo Practice
HospitalsHospitals
Free-standing,Free-standing,
communitycommunity
InsuranceInsurance
IndemnityIndemnity
PurchasersPurchasers
PassivePassive
Group Practice orEmployed
Networks & IntegratedDelivery Systems
Managed Care
“Prudent Purchaser”as Proactive Partner(cost shifts, drop insurance)
Performance- based Models(more choice, PPOs)
Privatized

Hospitals and Health SystemsHospitals and Health Systems
Traditional:Traditional: Community hospitalsCommunity hospitals
- Not-for-profitNot-for-profit- IndependentIndependent
Teaching hospitalsTeaching hospitals Specialized hospitalsSpecialized hospitals
- PsychiatricPsychiatric- Children’sChildren’s
VA and other government VA and other government facilitiesfacilities
Managed Care Era :Managed Care Era : Hospital systemsHospital systems
- Horizontal integrationHorizontal integration- Vertical integrationVertical integration- For-profit chains (Tenet)For-profit chains (Tenet)
PHOsPHOs Specialized: Heart, Hernia...Specialized: Heart, Hernia... IntegratedIntegrated Delivery Systems Delivery Systems Academic health systemsAcademic health systems VA “regional networks”VA “regional networks”

New Care SettingsNew Care Settings
Urgent care sitesUrgent care sites Ambulatory surgical centers (Ambulatory surgical centers (++ MD investors) MD investors) Mobile imaging (MRI, mammography…)Mobile imaging (MRI, mammography…) Psychiatric partial hospitalization & intensive Psychiatric partial hospitalization & intensive
outpatient programsoutpatient programs Home care Home care
All less costly, but shift care out of hospitalAll less costly, but shift care out of hospitale.g., Deep Venous Thrombosis as an outpatient e.g., Deep Venous Thrombosis as an outpatient
- Drug costs higher- Drug costs higher- - TotalTotal costs lower costs lower

Major Trends in Hospitals Major Trends in Hospitals 1990s & 2000s1990s & 2000s
Acquisitions & MergersAcquisitions & MergersDownsizing & ClosuresDownsizing & Closures
IntegrationIntegrationManaged CareManaged Care
Clinical RedesignClinical RedesignMalpractice RiskMalpractice Risk
----Increased Volume & Complexity----Increased Volume & Complexity
Source: Adapted from R. Lichtenstein

Integrated Delivery SystemsIntegrated Delivery Systems
Organized Organized systemsystem of care of care Integrates:Integrates:
- Providers (doctors, nurses, …)Providers (doctors, nurses, …)- Facilities Facilities (tertiary and community hospitals, clinics, home care)(tertiary and community hospitals, clinics, home care) - (Health plan – HMO, PPO)(Health plan – HMO, PPO)
Full spectrum of services Full spectrum of services (primary to tertiary)(primary to tertiary)
Geographic coverageGeographic coverage Economically viable scale (contracting clout)Economically viable scale (contracting clout) Ultimate goals: improve quality, lower costUltimate goals: improve quality, lower cost
- Harder to do in reality than the “paper merger”Harder to do in reality than the “paper merger”

Source: Adapted from R Lichtenstein
Accountability for Cost and QualityAccountability for Cost and QualityIntegrated Health Systems Integrated Health Systems shouldshould:: Promote clinical effectiveness researchPromote clinical effectiveness research Only use effective procedures, therapies, tests: Only use effective procedures, therapies, tests:
Evidence-based MedicineEvidence-based Medicine Develop and use clinical guidelines, clinical pathwaysDevelop and use clinical guidelines, clinical pathways Follow principles of Continuous Quality Improvement Follow principles of Continuous Quality Improvement
(CQI)(CQI) Strive to improve patient safetyStrive to improve patient safety Report quality & safety data to stakeholdersReport quality & safety data to stakeholders
SEE HAND-OUT PACKET FOR SAMPLE SEE HAND-OUT PACKET FOR SAMPLE “REPORT CARD”“REPORT CARD”

Evidence-Based MedicineEvidence-Based Medicine SystematicSystematic process to encourage process to encourage allall
practitioners to apply the appropriate practitioners to apply the appropriate scientific scientific evidenceevidence to individual clinical to individual clinical decisions.decisions.
Evidence Evidence isis::- scientific studies and meta-analysesscientific studies and meta-analyses- published in peer-reviewed journalspublished in peer-reviewed journals- with appropriate methods and populationswith appropriate methods and populations- showing significant outcomesshowing significant outcomes
Distilled into evidence-based practice Distilled into evidence-based practice guidelinesguidelines

Practice GuidelinesPractice Guidelines Prospective agreement among clinicians for the Prospective agreement among clinicians for the
management of typical casesmanagement of typical cases Synthesis of knowledge of diagnoses & therapySynthesis of knowledge of diagnoses & therapy Tool to improve appropriateness and efficiencyTool to improve appropriateness and efficiency Documentation of excellent process of careDocumentation of excellent process of care Evidence-basedEvidence-based
SEE HAND-OUT PACKET FOR SAMPLESEE HAND-OUT PACKET FOR SAMPLEPRACTICE GUIDELINEPRACTICE GUIDELINE

Continuous Quality ImprovementContinuous Quality Improvement
The Approach to Better HealthcareThe Approach to Better Healthcare
A process for continuous improvement:A process for continuous improvement:- evidence based- evidence based- consensus building - consensus building - data driven- data driven
Can be used to address:Can be used to address:- overuse- overuse- underuse- underuse- misuse- misuse
Quality Concerns• UnderuseUnderuse
– 60% of diabetic patients w/o HbAlc test in 199860% of diabetic patients w/o HbAlc test in 1998– Only 59% / 65% of GM women are receiving Only 59% / 65% of GM women are receiving
recommended screenings for cervical / breast cancerrecommended screenings for cervical / breast cancer
• OveruseOveruse– Cardiac surgery and hysterectomy rate in Flint MI 80% Cardiac surgery and hysterectomy rate in Flint MI 80%
higher than Kaiser Permanente (a West Coast HMO)higher than Kaiser Permanente (a West Coast HMO)
– catheterization rate in all catheterization rate in all majormajor MI, OH, IN areas at least MI, OH, IN areas at least 160% higher than Kaiser160% higher than Kaiser
• MisuseMisuse– 60% of cold / URI / bronchitis patients receive antibiotics60% of cold / URI / bronchitis patients receive antibiotics
Source: Bruce Bradley, General Motors

Health Care Paradigm ShiftHealth Care Paradigm ShiftPhysiciansPhysicians
Solo PracticeSolo Practice
HospitalsHospitals
Free-standing,Free-standing,
communitycommunity
InsuranceInsurance
IndemnityIndemnity
PurchasersPurchasers
PassivePassive
Group Practice orEmployed
Networks & IntegratedDelivery Systems
Managed Care
“Prudent Purchaser”as Proactive Partner
Performance- based Contracting

2004 Megatrends2004 Megatrends
Medicare Drug BillMedicare Drug Bill Medicare HMOs and PPOs returnMedicare HMOs and PPOs return
- - - maybe - - - maybe Health savings accountsHealth savings accounts Uninsured riseUninsured rise

Health InsuranceHealth Insurance Employment-based groupsEmployment-based groups
- Traditional Indemnity Traditional Indemnity (e.g., Blue Cross/Blue Shield and for-profit )(e.g., Blue Cross/Blue Shield and for-profit )
- Managed care (HMOs, PPOs, POS, etc.)Managed care (HMOs, PPOs, POS, etc.) Government-sponsored programsGovernment-sponsored programs
- Medicare (federal): Medicare (federal): elderlyelderly, disabled, ESRD, disabled, ESRD- Medicaid (state/federal match): Medicaid (state/federal match):
some of the some of the poorpoor, disabled, disabled Individual coverageIndividual coverage
- Limited availability; high cost; excludesLimited availability; high cost; excludespre-existing conditionspre-existing conditions
Uninsured – safety net programsUninsured – safety net programs

Sample Insurance ConditionsSample Insurance Conditions Deductible: amount that is paid by patient,
before insurance begins paying anything (e.g., after patient pays $500 cumulative medical costs/yr, then insurance begins paying some of costs)
Co-pay/coinsurance: portion of charge that patient must pay for service (e.g., patient pays $10 copay for visit, or pays 20% coinsurance of physician charge)
Discount: % less than charges that MD or hospital agrees to accept from insurer (e.g., agree to accept 50% of charges as full payment, & not balance bill the patient for the remainder)

How Do Deductibles and Copays How Do Deductibles and Copays Work? The Medicare Drug BillWork? The Medicare Drug Bill
Starting 2006, Medicare beneficiary must pay:Starting 2006, Medicare beneficiary must pay: Pay $35/month ($450/yr)Pay $35/month ($450/yr) $450$450 PremiumPremium Pay first $250Pay first $250 $250$250 DeductibleDeductible Pay 25% of next $2000Pay 25% of next $2000$500$500 CoinsuranceCoinsurance Pay next $2850Pay next $2850 $2850$2850 “Donut Hole”“Donut Hole” Pay 5% from there onPay 5% from there on Stop LossStop Loss Discounts begin 2004 (~15%)Discounts begin 2004 (~15%) DiscountsDiscountsTotal cost to person w/ $5100/year drug cost = $4050 (79%) Total cost to person w/ $5100/year drug cost = $4050 (79%) Total cost to person w/ $7500/year drug cost = $4170 (56%)Total cost to person w/ $7500/year drug cost = $4170 (56%)
SEE HAND-OUT PACKET FOR SUMMARY OF SEE HAND-OUT PACKET FOR SUMMARY OF MEDICARE DRUG BILLMEDICARE DRUG BILL

How realistic are these drug costs?How realistic are these drug costs?$5100/year = $425/month$5100/year = $425/month$7500/year = $625/month$7500/year = $625/month
Monthly costs: Monthly costs: NexiumNexium $119$119Pravachol Pravachol $124$124ZoloftZoloft $72$72FosamaxFosamax $65$65ClarinexClarinex $76$76
$456$456CoregCoreg $97$97CelebrexCelebrex $78$78
$631$631

How realistic are these drug costs?How realistic are these drug costs?$5100/year = $425/month$5100/year = $425/month$7500/year = $625/month$7500/year = $625/month
Monthly costs: Monthly costs: NexiumNexium $119$119 omeprazole OTC $15omeprazole OTC $15Pravachol Pravachol $124$124 lovastatin lovastatin $68$68ZoloftZoloft $72$72 fluoxetinefluoxetine $30$30FosamaxFosamax $65$65 Fosamax Fosamax $65$65ClarinexClarinex $76$76 loratidine OTCloratidine OTC $10$10
$456$456 $188$188CoregCoreg $97$97 atenololatenolol $5$5CelebrexCelebrex $78$78 ibuprofenibuprofen $3$3
$631$631 $196$196https://ummcpharmweb.med.umich.edu/internal/ambulatory/umhs_fgp_prefdrugs.asphttps://ummcpharmweb.med.umich.edu/internal/ambulatory/umhs_fgp_prefdrugs.asp

Health Insurance TrendsHealth Insurance Trends Rising premium costs Rising premium costs (slowed, now rising fast)(slowed, now rising fast)
More temporary and part-time work More temporary and part-time work (without health care coverage)(without health care coverage)
Growth of managed care---especially PPOsGrowth of managed care---especially PPOs Reduction in comprehensive coverage:Reduction in comprehensive coverage:
Cost shiftingCost shifting and and benefit limitsbenefit limits-cap on pharmaceutical coverage, triple tier formularies;-cap on pharmaceutical coverage, triple tier formularies;-higher copays, percent co-insurance, deductibles;-higher copays, percent co-insurance, deductibles;-limits on number of services [PT, psych];-limits on number of services [PT, psych];-more stringent authorization requirements-more stringent authorization requirements
Source: Adapted from Kuttner, NEJM1999;34:163-168

The UninsuredThe Uninsured
Uninsured rising despite economic “recovery”Uninsured rising despite economic “recovery” 43.3 million nonelderly Americans were without 43.3 million nonelderly Americans were without
health insurance in 2002 health insurance in 2002 (17.3% of U.S. population)(17.3% of U.S. population)
The number of nonelderly uninsured grew The number of nonelderly uninsured grew almost 10% between 2000 and 2002almost 10% between 2000 and 2002
Low income families are at greatest risk of losing Low income families are at greatest risk of losing health care insurancehealth care insurance
Source: The Kaiser Commission on Medicaid and the Uninsured

Managed Care - What is it?Managed Care - What is it?
“ “Means of providing health care services within Means of providing health care services within a defined a defined networknetwork of health care providersof health care providers responsible for responsible for managingmanaging and providing and providing quality quality, , cost-effectivecost-effective health care”. health care”.
Source: Vogel, DE. The Physician and Managed Care. Chicago, AMA, 1993.

What are the goals ofWhat are the goals of managed care? managed care?
Efficient screening and prevention Efficient screening and prevention programsprograms
Efficient & accurate diagnosisEfficient & accurate diagnosis Efficient & effective treatment and Efficient & effective treatment and
managementmanagement High patient satisfactionHigh patient satisfaction

What do managed care plans What do managed care plans expect from physicians?expect from physicians?
Low costLow cost High qualityHigh quality Patient-satisfying carePatient-satisfying care
Source: C Krause, Family Medicine, June 1995

Managed Care CompetenciesManaged Care Competencies Understanding of health care needs of populationsUnderstanding of health care needs of populations Clinical preventionClinical prevention Management of health risks at home and workManagement of health risks at home and work Clinical decision-making in managed careClinical decision-making in managed care
(Including ethics of resource allocation)(Including ethics of resource allocation) Effective communication with panels of patientsEffective communication with panels of patients Continuous quality improvementContinuous quality improvement Professional satisfactionProfessional satisfaction Team work and practice leadershipTeam work and practice leadership Practice managementPractice management
SOURCE: GT Moore, Report to COGME, 1993

ABCs of Managed CareABCs of Managed Care
HMO - Health Maintenance OrganizationHMO - Health Maintenance Organization- Comprehensive benefit planComprehensive benefit plan
(including screening and preventive services)(including screening and preventive services)- Usually uses “gate-keeper”Usually uses “gate-keeper”- Usually “capitated” or shared financial riskUsually “capitated” or shared financial risk- Out-of-network services not coveredOut-of-network services not covered
PPO - Preferred Provider OrganizationPPO - Preferred Provider Organization- Limited provider network, but no “gatekeeper”Limited provider network, but no “gatekeeper”- Discounted fee-for-service Discounted fee-for-service - No (or low) risk sharingNo (or low) risk sharing- Out-of-network coverage at lower benefit levelOut-of-network coverage at lower benefit level
ABCs of Managed CareABCs of Managed Care POS - Point of Service PlanPOS - Point of Service Plan
- Hybrid of HMO & PPOHybrid of HMO & PPO- Patient chooses how to use benefit optionsPatient chooses how to use benefit options- Some coverage for out-of-network servicesSome coverage for out-of-network services
““Managed” IndemnityManaged” Indemnity- ““Managed care” tools used in a fee-for-service planManaged care” tools used in a fee-for-service plan
• Pre-certification of hospital staysPre-certification of hospital stays• Disease management programsDisease management programs• Prior authorization of high cost proceduresPrior authorization of high cost procedures
Customized Health Savings Account (HSAs)Customized Health Savings Account (HSAs)- High deductible, $$ set aside, keep if don’t useHigh deductible, $$ set aside, keep if don’t use
• Most attractive to those without medical problemsMost attractive to those without medical problems• Leaves the sicker families in the traditional plansLeaves the sicker families in the traditional plans• Access to doctor/hospital report cards (profiles)Access to doctor/hospital report cards (profiles)

Managed CareManaged CareSpectrum of ManagementSpectrum of Management
High Provider Risk Low Provider Risk
High Management Low Management
HMO POS PPO
Indemnity

HMO ModelsHMO Models
Staff ModelStaff Model - HMO employs physicians - HMO employs physicians Group ModelGroup Model - HMO contracts with a - HMO contracts with a
physician group practicephysician group practice IPA and Network ModelsIPA and Network Models - HMO - HMO
contracts multiple physician groupscontracts multiple physician groups Mixed ModelsMixed Models

Funds Flow - Traditional ModelFunds Flow - Traditional Model
people employers
insurers
doctors hospitals

Funds Flow - Capitation Funds Flow - Capitation Physician Hospital Org. Model Physician Hospital Org. Model
HMO1
PHO
Physician Organization
M.D. M.D. M.D. M.D. D.O. M.D.
Group Practice Hospital
HMO2

people employers
HMO
Funds Flow – Funds Flow – Shared Risk ModelShared Risk Model
Primary Care Fund
Specialty CareFund
HospitalFund
PharmacyFund
Other
PCPs PCPs & Specialists
PCP/Specialists/HMO

Health Care Paradigm ShiftHealth Care Paradigm Shift
PhysiciansPhysicians
Solo PracticeSolo Practice
HospitalsHospitals
Free-standing,Free-standing,
communitycommunity
InsuranceInsurance
IndemnityIndemnity
PurchasersPurchasers
PassivePassive
Group Practice orEmployed
Networks & IntegratedDelivery Systems
Managed Care
“Prudent Purchaser”as Proactive Partner(cost shifts, drop insurance)
Performance- based Models(more choice, PPOs)
Privatized

Health Care PurchasersHealth Care Purchasers EmployersEmployers
- Large employers (GM, Detroit Edison, UofM)Large employers (GM, Detroit Edison, UofM)- Small employers (Angelo’s, Ulrich’s)Small employers (Angelo’s, Ulrich’s)
GovernmentGovernment- For aged (thru Medicare)For aged (thru Medicare)- For some indigent (thru Medicaid)For some indigent (thru Medicaid)- Federal, state, local employeesFederal, state, local employees
Health Care CoalitionsHealth Care Coalitions IndividualsIndividuals
- growing due to cost shifts from employersgrowing due to cost shifts from employers

What do purchasers want?What do purchasers want? ValueValue = quality/cost = quality/cost Care that is:Care that is:
- High qualityHigh quality- AppropriateAppropriate- CoordinatedCoordinated- AccessibleAccessible- Cost effectiveCost effective
Healthy, satisfied employees/membersHealthy, satisfied employees/members Ability to hold “suppliers” accountableAbility to hold “suppliers” accountable Lately, they want out!Lately, they want out!

Strategies that create an environment
where motivation and incentives reward
consumers, providers and payers for
behaviors that result in improved:• Quality and outcomes of care • Productivity and cost.
Managed CareManaged Care(One Large Employer’s View of What the (One Large Employer’s View of What the
Definition Definition ShouldShould Be) Be)
Source: Bruce Bradley, General Motors

Purchasers - New RolesPurchasers - New Roles Active Active partners with providerspartners with providers in design of health care in design of health care
and quality improvement:and quality improvement:- Partnership Health (Ford/UM), Active Care (GM/UM) Partnership Health (Ford/UM), Active Care (GM/UM) - Medicaid HMOs Medicaid HMOs - Medicare HMOs (were shrinking, subsidies in new bill)Medicare HMOs (were shrinking, subsidies in new bill)- GDAHC Quality Forum (GDAHC Quality Forum (Greater Detroit Area Health Council)Greater Detroit Area Health Council)
Reporting quality and costsReporting quality and costs::- GDAHC RFI (Request for Information): HMO report cardGDAHC RFI (Request for Information): HMO report card- Hospital safety reports (Leapfrog- employer QI group)Hospital safety reports (Leapfrog- employer QI group)
Working with providers as Working with providers as “suppliers”“suppliers” to improve to improve clinical workflow (PICOS - GM)clinical workflow (PICOS - GM)
Carve outsCarve outs (UM pays directly for Pharmacy) (UM pays directly for Pharmacy) Drop insuranceDrop insurance coverage for dependents/workers coverage for dependents/workers

Employee & Community Health
Value Purchasing
Evolution of Employers’Evolution of Employers’ Management of Health Plans Management of Health Plans
Pay Premiums
Selection / Negotiation
Quality Leadership
Source: Bruce Bradley, General Motors

Impact on PhysiciansImpact on Physicians
More uninsured patientsMore uninsured patients Insured patients pay more (cost share/shift)Insured patients pay more (cost share/shift) More complexity in drug prescribingMore complexity in drug prescribing
- Multiple preferred drug lists, restrictions, prior authsMultiple preferred drug lists, restrictions, prior auths- Patients and doctors lobbied by PHARMAPatients and doctors lobbied by PHARMA
Less PCP gatekeepingLess PCP gatekeeping Zero-sum-game in healthcareZero-sum-game in healthcare
- More money in one area means less in the restMore money in one area means less in the rest- Harder to get coverage for new procedures, Harder to get coverage for new procedures,
technology, or drugstechnology, or drugs

Services that are:Services that are:- High quality, patient-friendly, accessibleHigh quality, patient-friendly, accessible
Choice of physicians, health plan, Choice of physicians, health plan, hospitalshospitals
Continuity of care, coordinated careContinuity of care, coordinated care Low out-of-pocket costsLow out-of-pocket costs No “red tape” and administrative hassleNo “red tape” and administrative hassle Confidentiality/privacyConfidentiality/privacy
What do patients want?What do patients want?

Patient Empowerment: Patient Empowerment: Age of the ConsumerAge of the Consumer
Care co-manager (the true PCP)Care co-manager (the true PCP) Informed consumerInformed consumer
- Report cards: physician, HMO, & hospital Report cards: physician, HMO, & hospital - Increased availability of health care information [50% Increased availability of health care information [50%
web users = health]web users = health]- Marketing directly to patients: hospitals, health plans, Marketing directly to patients: hospitals, health plans,
pharmaceutical companiespharmaceutical companies Role transition (passive active)Role transition (passive active)
- From “receiver of decision”From “receiver of decision”- To “participant in decision-making” To “participant in decision-making” - To “decision-maker”, even “payer” in some new modelsTo “decision-maker”, even “payer” in some new models
CustomerCustomer with service expectations with service expectations

What do physicians want?What do physicians want?
Professional autonomy Professional autonomy - ability to practice and provide high quality care ability to practice and provide high quality care
without undue interferencewithout undue interference Ability to do what’s best for patient and to Ability to do what’s best for patient and to
develop patient-physician relationships develop patient-physician relationships characterized by trustcharacterized by trust
Minimal “red tape” and administrative Minimal “red tape” and administrative hassleshassles
Reasonable reimbursementReasonable reimbursement

What do hospitals & What do hospitals & health systems want?health systems want?
Contracts with payers to lock-in businessContracts with payers to lock-in business Reasonable reimbursementReasonable reimbursement
“No Margin = No Mission”“No Margin = No Mission” Achieve a size/scale to be competitiveAchieve a size/scale to be competitive Satisfied stakeholdersSatisfied stakeholders
- patients patients - physiciansphysicians- payerspayers- communitycommunity

Next Model of Health CareNext Model of Health Care Coordinated careCoordinated care Integrated delivery systemsIntegrated delivery systems Population-basedPopulation-based
- Outreach initiated by plan/physiciansOutreach initiated by plan/physicians- Incorporates prevention and patient educationIncorporates prevention and patient education
Communication among providers & patientsCommunication among providers & patients- Facilitated by information technologyFacilitated by information technology
Standardized, Standardized, evidence-basedevidence-based process process- Guidelines, pathways, disease managementGuidelines, pathways, disease management
Performance-based contractingPerformance-based contracting- Clinical outcomesClinical outcomes- CostCost

Next Model of Health Care: Next Model of Health Care: AccountabilityAccountability
Who?Who?- Physician, hospital, group practice, PO, Physician, hospital, group practice, PO,
PHO, health plan, hospital, IDS, patientPHO, health plan, hospital, IDS, patient For What?For What?
- QualityQuality- AccessAccess- CostCost
By Whom?By Whom?- Employers, consumers, labor, government, Employers, consumers, labor, government,
communitycommunity
Health Trends 2004 Health Trends 2004 Shifting Accountability DownwardShifting Accountability Downward
Performance-based contractingPerformance-based contracting Report cards: outcomes, costsReport cards: outcomes, costs Defined contribution health plansDefined contribution health plans Individualized Medical Savings Individualized Medical Savings
Accounts, with provider report cardsAccounts, with provider report cards Differential copays for high cost Differential copays for high cost
hospitals/groupshospitals/groups

Crossing the Quality Chasm:10 Rules
1. Care based or continuous healing relationshipsa. 24 hour availabilityb. Face-to-face and remote
2. Customized based on needs and values, choice and preference 3. Patient as source of control 4. Shared knowledge and free flow of information
Patients - their own information & medical knowledge 5. Evidence-based decision making 6. Safety as a system property 7. Transparency - consumers and employers data on systems (safety, evidence-based practice, satisfaction) 8. Anticipation of needs 9. Continuous decrease in waste10. Cooperation among clinicians (coordination)

ENDEND
PopulationsPopulations
Healthy Stable chronic disease
and stable at riskHigh risk orunstablechronic disease
Hospitalized
Acutely ill
University of Michigan Medical School
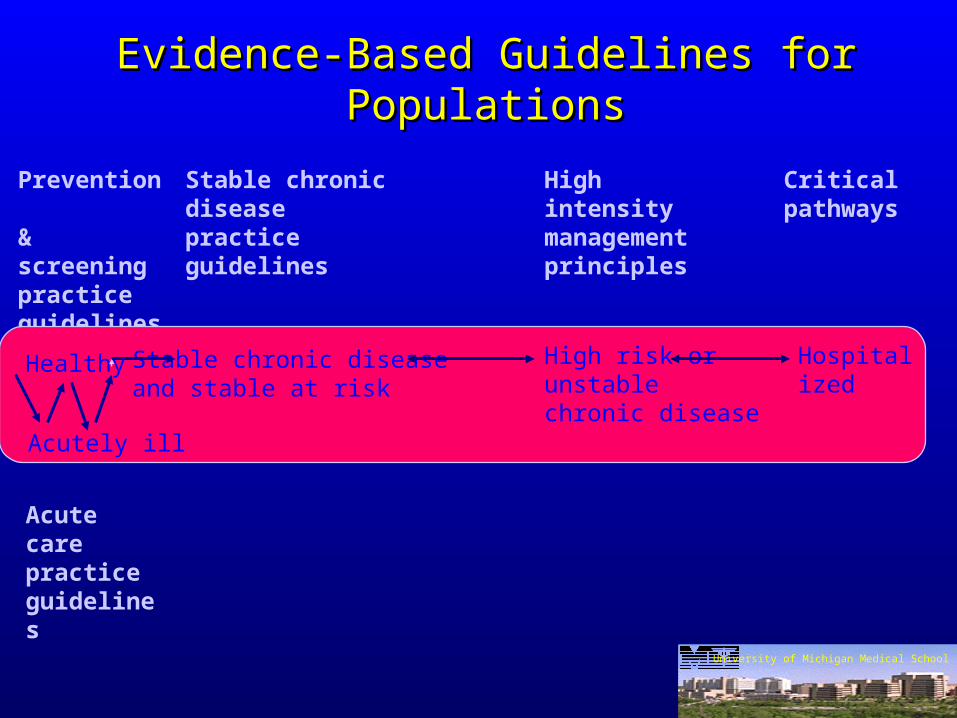
Evidence-Based Guidelines for PopulationsEvidence-Based Guidelines for Populations
Prevention & screeningpracticeguidelines
Stable chronic diseasepractice guidelines
High intensitymanagement principles
Criticalpathways
Acute carepracticeguidelines
University of Michigan Medical School
Healthy
Acutely ill
HospitalizedStable chronic diseaseand stable at risk
High risk orunstablechronic disease

Specialist (& PCP)
Prevention &screeningpractice guidelines
Acute care practice guidelines
Stable chronic diseasepractice guidelines
High intensity management principles
Critical pathways
Prevention/Screeningmanagement program
Acute illnessmanagement program
Chronic/stable illnessmanagement program
High intensitycase management &tracking program
Inpatient practice management
PCP (& Specialist)
PCP & Specialist Specialist (& PCP)
Medical Management Strategies
TEAM APPROACH(Physicians, Nurse Practitioners, Social Work…)
University of Michigan Medical School
Healthy
Acutely Ill
Stable chronic diseaseand stable at risk
High risk or unstable chronic disease
Hospitalized

Specialist(& PCP)
Hospitalized
Healthy Stable chronic diseaseand stable at risk
High risk or unstablechronic disease
Acutely ill
Prevention & screeningpractice guidelines
Acute carepractice guidelines
Stable chronic diseasepractice guidelines
High intensity management principles
Critical pathways
Prevention/Screeningmanagement program
Acute illnessmanagement program
Chronic/stable illnessmanagement program
High intensitycase management &tracking program
Inpatientpracticemanagement
PCP (& Specialist)
PCP & Specialist Specialist (& PCP)
Health Plan Design StrategiesHealth Plan Design Strategies
Principal Physician
Hospitalist
TEAM APPROACH(Physicians, Nurse Practitioners, Social Work)
Access to Specialists
Risk factoridentification, HRA
Patient educationcovered
Specialized management programs covered
Full preventiveservices covered
Targeted health behaviorprograms
Patient advocateHome contactsBenefit expansion

Identify Areas of Practice
Identify Areas of Practice
Process for Practice Guideline Adaptation & ImplementationProcess for Practice Guideline Adaptation & Implementation
Define OptimalClinical Practice
Define OptimalClinical Practice
Teams Design and Implement
Interventions
Teams Design and Implement
Interventions
Assess OutcomesAssess Outcomes
Health Care DatabaseHealth Care Database
Redesign Process, if Necessary
Redesign Process, if Necessary
Institutional ActivitiesInstitutional Activities
External AgenciesExternal AgenciesWise, Billi. Jt. Comm. J. Q. Imp. 1995;21:465-476.
Characteristics of Delivery System
Characteristics of Delivery System
CQI Process
CQI Process CQI Process
CQI Process
CQI Process

Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Define Optimal Clinical Practice & Systems Processes
* Clinical panels adapt guidelines to local practice
* Collaborative critical pathways * Case management
Define Optimal Clinical Practice & Systems Processes
* Clinical panels adapt guidelines to local practice
* Collaborative critical pathways * Case management
Teams Design and Implement
Interventions
Teams Design and Implement
Interventions
Assess OutcomesAssess Outcomes
Health Care DatabaseHealth Care Database
Redesign Process, if Necessary
Redesign Process, if Necessary
Institutional ActivitiesInstitutional Activities
External AgenciesExternal Agencies
Characteristics of Delivery System
Characteristics of Delivery System
CQI Process
CQI Process CQI Process
CQI Process
CQI Process
Teams Design & Implement Interventions
• Data feedback• MIS-based intervention• Administrative interventions• Financial interventions• Educational models• Patient empowerment• Clinician empowerment• Other
Process for Practice Guideline Adaptation & ImplementationProcess for Practice Guideline Adaptation & Implementation

Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Teams Design & Implement Interventions* Data feedback* MIS-based intervention* Administrative interventions* Financial interventions* Educational models* Patient empowerment* Clinician empowerment* Other
Teams Design & Implement Interventions* Data feedback* MIS-based intervention* Administrative interventions* Financial interventions* Educational models* Patient empowerment* Clinician empowerment* Other
Assess OutcomesAssess Outcomes
Health Care DatabaseHealth Care Database
Redesign Process, if Necessary
Redesign Process, if Necessary
Institutional ActivitiesInstitutional Activities
External AgenciesExternal Agencies
Characteristics of Delivery System
Characteristics of Delivery System
CQI Process
CQI Process CQI Process
CQI Process
CQI Process
Define Optimal Clinical Practice Guideline
•Begin with best evidence-based guideline•Clinical panels adapt guidelines to local practice•Modify based on medical evidence, not opinion
•Practice guidelines•Case management principles•Collaborative critical pathways
Define Optimal Clinical Practice Guideline
•Begin with best evidence-based guideline•Clinical panels adapt guidelines to local practice•Modify based on medical evidence, not opinion
•Practice guidelines•Case management principles•Collaborative critical pathways
Process for Practice Guideline Adaptation & ImplementationProcess for Practice Guideline Adaptation & Implementation

Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Identify Areas of Practice• High cost• High volume• Practice variation• High risk• Marketing factors• Regulatory factors• Guidelines available• Local clinical champion(s)• Other
Process for Practice Guideline Adaptation & ImplementationProcess for Practice Guideline Adaptation & Implementation
Teams Design & Implement Interventions•Data feedback • MIS-based intervention•Administrative interventions•Financial interventions•Educational models•Patient empowerment•Clinician empowerment•Other
Teams Design & Implement Interventions•Data feedback • MIS-based intervention•Administrative interventions•Financial interventions•Educational models•Patient empowerment•Clinician empowerment•Other
Institutional Activities Develop financial packages Planning & Marketing Regulatory reporting
Institutional Activities Develop financial packages Planning & Marketing Regulatory reporting
External Agencies Payers Public Corporations Corporate alliances Government agencies
External Agencies Payers Public Corporations Corporate alliances Government agencies
Characteristics of Delivery System• Process driven
• collaboration of caregivers• process of care defined
•Variation reduced (“optimal practice”)• Predictable costs (cost-effectiveness)• Outcomes - optimal outcomes defined & measured
Characteristics of Delivery System• Process driven
• collaboration of caregivers• process of care defined
•Variation reduced (“optimal practice”)• Predictable costs (cost-effectiveness)• Outcomes - optimal outcomes defined & measured
CQI Process
CQI Process CQI Process
CQI Process
CQI Process
Define Optimal Clinical Practice Guideline
•Begin with best evidence-based guideline•Clinical panels adapt guidelines to local practice•Modify based on medical evidence, not opinion
•Practice guidelines•Case management principles•Collaborative critical pathways
Define Optimal Clinical Practice Guideline
•Begin with best evidence-based guideline•Clinical panels adapt guidelines to local practice•Modify based on medical evidence, not opinion
•Practice guidelines•Case management principles•Collaborative critical pathways
Redesign Process, if Necessary
•Identify barriers•Fine tune guidelines
Redesign Process, if Necessary
•Identify barriers•Fine tune guidelines
Assess Outcomes•Clinical•Process•Costs (cost / benefit)•Patient satisfaction•Return to work, days off, days ill
Assess Outcomes•Clinical•Process•Costs (cost / benefit)•Patient satisfaction•Return to work, days off, days ill
Health Care Database• Clinical• Demographic• Economic• Nursing• Outcomes: function, satisfaction, productivity
Health Care Database• Clinical• Demographic• Economic• Nursing• Outcomes: function, satisfaction, productivity
Practice GuidelinesPractice Guidelines““I can’t keep all that evidence in my head…”I can’t keep all that evidence in my head…”
PG = A distillation of scientific PG = A distillation of scientific evidenceevidence into a into a practical guidepractical guide to to assistassist a clinician a clinician in the in the managementmanagement of a problem. of a problem.
A A prospective agreement among cliniciansprospective agreement among clinicians to use in the care of similar cases.to use in the care of similar cases.
To reduce variation -- To reduce variation -- toward optimaltoward optimal
While permitting a doctor to vary -- While permitting a doctor to vary -- with a with a reason!reason!

8 Characteristics of Good 8 Characteristics of Good Practice GuidelinesPractice Guidelines
OpenOpen development process (who development process (who
developed it, why?)developed it, why?) Focused on improving Focused on improving importantimportant, ,
targeted health targeted health outcomesoutcomes.. Specify the most important questionSpecify the most important question SystematicSystematic use of the peer-reviewed use of the peer-reviewed
medical literature to support key steps.medical literature to support key steps.

8 Characteristics of Good 8 Characteristics of Good Practice GuidelinesPractice Guidelines
Full Full disclosure of the level of evidencedisclosure of the level of evidence for for
each step in the guideline.each step in the guideline. ““Expert opinionExpert opinion” minimized and labeled.” minimized and labeled. Include a Include a care algorithmcare algorithm and and key pointskey points.. Make Make availableavailable: supporting materials, text : supporting materials, text
rationales, literature reviews, evidence tables, rationales, literature reviews, evidence tables, patient education materials and bibliography.patient education materials and bibliography.
UMHS Guidelines: http://cme.med.umich.edu/iCMEUMHS Guidelines: http://cme.med.umich.edu/iCME

12 Characteristics of 12 Characteristics of Good UsesGood Uses of Practice Guidelinesof Practice Guidelines
Start with Start with good guidelinesgood guidelines, including the , including the source(s).source(s).
Use the guidelines nested in a Use the guidelines nested in a constructiveconstructive, , educationally-oriented quality improvement educationally-oriented quality improvement model.model.
In the In the local endorsement processlocal endorsement process, involve true , involve true representatives of the clinicians whose practice representatives of the clinicians whose practice the guideline covers.the guideline covers.
Allow Allow local adaptation, with justificationlocal adaptation, with justification and and documentation. Focus on aspects which may documentation. Focus on aspects which may not be feasiblenot be feasible..

12 Characteristics of 12 Characteristics of Good UsesGood Uses of Practice Guidelinesof Practice Guidelines
Carefully design implementationCarefully design implementation programs to programs to encourage encourage educationeducation, dialogue and constructive , dialogue and constructive use of data. use of data.
The guidelines and supporting materials, literature The guidelines and supporting materials, literature reviews and evidence tables must be broadly reviews and evidence tables must be broadly availableavailable..
Help clinicians measure their performance with a Help clinicians measure their performance with a ““measure to improvemeasure to improve” rather than a “measure to ” rather than a “measure to judge” philosophy. judge” philosophy.
Measure onlyMeasure only key stepskey steps supported by high grade supported by high grade scientific evidence. Don’t sweat the small stuff!scientific evidence. Don’t sweat the small stuff!

12 Characteristics of 12 Characteristics of Good UsesGood Uses of Practice Guidelinesof Practice Guidelines
Assess Assess barriersbarriers to successful practice to successful practice improvement. Make changes to overcome improvement. Make changes to overcome them.them.
Activate Activate alliesallies to help with the changes: to help with the changes: staff, patients, payers, employers, other staff, patients, payers, employers, other physicians.physicians.
Plan to Plan to modifymodify the guidelines based on their the guidelines based on their use, as experience grows.use, as experience grows.
Plan to Plan to updateupdate guidelines formally and guidelines formally and regularly.regularly.

Disease ManagementDisease Management
Disease Management is:Disease Management is:A systematic program to identify A systematic program to identify members with a disease and to members with a disease and to intervene to improve quality of intervene to improve quality of care and outcomes. care and outcomes.
Disease ManagementDisease Management
Simplest Versions:Simplest Versions: Multidisciplinary subspecialty clinicMultidisciplinary subspecialty clinic Office nurseOffice nurse

Elements of Superb Elements of Superb Disease Management ProgramsDisease Management Programs
Coordination of careCoordination of care Communication about careCommunication about careComprehensive careComprehensive care PreventionPreventionCollaborative/MultidisciplinaryCollaborative/Multidisciplinary Case managementCase management Provider educationProvider education Patient educationPatient education Patients
with a particular
disease

Features of Superb Features of Superb Disease Management ProgramsDisease Management Programs
Population basedPopulation based Disease specificDisease specific Define the spectrum of disease handledDefine the spectrum of disease handled Excellent case identification methodsExcellent case identification methods Explicitly enroll the membersExplicitly enroll the members Able to manage geographically dispersedAble to manage geographically dispersed Therefore uses long distance managementTherefore uses long distance management
(calls to patients, calls to physicians, home visits)(calls to patients, calls to physicians, home visits)
Features of Superb Features of Superb Disease Management ProgramsDisease Management Programs
Evidence based principlesEvidence based principles Collect and analyze outcomesCollect and analyze outcomes Excellent information systems Excellent information systems
- registry registry - phone logs integrated with clinical and use phone logs integrated with clinical and use
infoinfo- all data retrievable as patient specificall data retrievable as patient specific
Time prompts able to be set variably Time prompts able to be set variably

VALUE
Rate Proposals
Health Plan
Site Visits
Foundation for Accountability
(FACCT) Measures
NCQA/CAHPSSatisfaction
Survey
GM Health CareInformation andAnalysis System
HEDIS Quality Measures
Quality Initiatives
NCQAAccreditation
Health PlanRequests
for Information
BenefitLevelAccess
ClinicalMeasures
PatientSatisfaction
FunctionalOutcomes
.
Cost
Value: Employer’s DefinitionValue: Employer’s Definition
Source: Bruce Bradley, General Motors

Low HighCost Effectiveness
Managed Care ContinuumD
egre
e o
f M
anag
emen
t
an
d I
nte
gra
tio
nL
ow
H
igh
Unmanaged Indemnity
Managed Indemnity
PPO
POS HMO
IPA HMO
Group/Staff HMOHighly Integrated IPA
Corp. SponsoredFacility / Systems
Source: Bruce Bradley, General Motors





























