Embed Size (px)
Citation preview

ORAL SURGERY INVOLVING THE MAXILLARY SINUSCharles Tomes Lecture delivered at the Royal College of Surgeons of England
on20th July 1956
by
B. W. Fickling, F.R.C.S., F.D.S.Dental Surgeon, St. George's Hospital and Royal Dental Hospital; Senior Dental
Surgeon, Mount Vernon Centre for Plastic and Jaw Surgery
INTRODUCTION
I AM DEEPLY conscious of the honour which has been conferred upon me,upon the medical and dental schools in which I trained and work, andupon my teachers, by my nomination as the Charles Tomes Lecturer forthis year. The name of Tomes will for ever command respect in the pro-fession of this country for two most vital contributions, the establishmentof dental surgery as a profession based on medicine and the developmentof a scientific approach. While John Tomes was the originator and primemover in these changes, his son Charles nobly carried on the tradition.Both had an incalculable influence in ensuring that dentistry should berecognised among the great professions.
In choosing as subject the oral surgery of the maxillary sinus I am onlytoo aware that this is border territory between two great specialties ofsurgery. It is possible, however, that each has something to learn fromthe experience of the other and I trust my remarks will be accepted inthis spirit. This paper is limited to oral surgery; the effect of dentalconditions on the sinus or of sinus diseases on dental surgery are confinedto this aspect.
I do not need to stress to a gathering such as this the close relation ofthe maxillary sinus to the roots of the teeth. Perhaps I may use the wordsand illustrations of Nathaniel Highmore from his Corporis HumaniDisquisitio Anatomica, published at The Hague in 1651.
" This single antrum is covered by thin bone or bony scale; indeed the bonewhich encloses it and which separates it from the sockets of the teeth does notmuch exceed a piece of wrapping paper in thickness (Fig. la, d.d.). In its floorcertain noticeable prominences are visible (Plate 16, Fig. 2a, a, a, a, a,) by whichthe roots of the teeth are enclosed (b.b.b.). The tooth sockets are carved inthe lower margin of this bone (Fig. la, c.c.c.)."
Although given the credit for this description, it was not the firstaccount. This is made quite clear in the remarks of William Cowper,a brilliant English surgeon, who devised and described a treatment forinfection of the sinus which persisted for two hundred years. In hisAnatomy of Humane Bodies, published in 1698, in a description of the
13

B. W. FICKLING
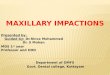
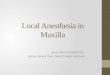
Fig. 1. Leonardo da Vinci's drawing of the maxillary sinus with marginal notesprepared about 1489.
fourth bone of the upper jaw (the maxilla) illustrated in the ninety-secondtable, the following words appear:
" This Cavity is call'd Antst,iii MAaxillace Superioris: by some call'd AntrulnHighlnorianum, for what reason I know not, since 'twas described long beforeDr. Higlunore, as Appears by Vesaililis, Coluitmbuls, Baulimlis etc."Vesalius had indeed described the cavity in 1543 in De Humalni Colpolris
Fabrica.Many of you, however, know that the maxillary sinus was drawn and
even described in marginal notes about 1489 by that remarkable manLeonardo da Vinci (Fig. 1). O'Malley and Saunders give this translation:
" The Cavity of the Orbit and the cavity of the bone which supports thecheek are of equal depth ... each of these cavities is about as long as the thirdpart of a man's face, that is, from the chin to the hair. The eye is hidden in the
14

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
cavity above, and in that below is the humour which nourishes the roots ofthe teeth."
William Cowper described his operation in a chapter " Of the Nose,"contributed to " A new System of Anatomy" by James Drake in 1707.Describing how the nasal opening is at the upper part of the antrum hewrites:" by all which it appears with what difficulty any peccant Humour lodg'd ineither of these Cavities, can be discharg'd by the Foramina Narium since thesecavities must either be fill'd to the top ready to run over first, or the Headmust be held down to procure the discharge. This induced me to put in practicean Operation, I being convinced it might be done without ha7ard to the Patient.After the fore-most Dens Molaris was taken out, and not finding an Aperturefrom its Alveolus into this Antrum, which in other instances I have seen happen,with a convenient Instrument I bor'd the whole of the Alveolus through into theAntrum Genae, whereby the Pus which before lay in the Antrum readily ran out,and the Medicines that were daily injected by this Aperture, pass'd into theNostrils, whereby the Patient was cured."
This approach, which became known as Cowper's operation, becamethe standard treatment of sinus infection for nearly two hundred years.Samuel Cooper in 1807, Charles Bell in 1809, James Syme in 1863, Roseand Carless in 1898 and St. Clair Thomson in 1911 all described the methodwith variants.
It was natural therefore for Tomes in his System of Dental Surgery todescribe the operation. In the first edition of 1859 only three pages aredevoted to diseases of the antrum and Cowper's method is described.In the second edition of 1873 the chapter amounts to ten pages and includesan illustration of an apical abscess on a molar palatal root presentingon the floor of the antrum, with the wording in the text " was in myfather's collection." This is evidence I think that Charles Tomes wasresponsible for enlarging this chapter.
In the third edition of 1887 he writes:the operation may be done with far less disturbance ... by a large spear-head
in the dental engine.... When there are no diseased teeth a sound first molarmay be extracted, or the puncture made near the malar process, or backwardsfrom the canine fossa.... It has been recommended that a gold tube with astopper be fitted to the opening and secured to the neighbouring teeth; but inmost cases a plug of soft wax will be found to answer the purpose."
Among the instruments I inherited in my practice is an antral awl, stillbeautifully sharp, which however I have never used. Alfred Colemandevised an antral awl with a stop which is described in his book publishedin 1881. He saw the disadvantages of the alveolar approach and advocatedpuncture with his instrument in front of the malar buttress.The catalogue of Claudius Ash for 1916 includes a complete set of
instruments designed by Mr. Ackland, dental surgeon to the BristolRoyal Infirmary, for the alveolar approach to the antrum, completewith metal antrum tube, cap and two-way cannula.
15

B. W. FICKLING
Gradually the disadvantages of Cowper's operation became apparentand it was replaced by an approach through the canine fossa and laterthe modern intranasal antrostomy in the inferior meatus became standardpractice.Thomas Bell in his Anatomy, Physiology, and Diseases of the Teeth,
first edition, published in London in 1829, seems to have been one of thefirst to describe a method to assist closure of an oro-antral fistula:" The opening will generally close without any assistance. I have, however,seen cases in which this has not taken place; in these I have found it necessaryto remove a small circular portion of gum, as high up as possible within thetube, and then direct the lips of the opening to be as constantly as possiblekept pressed against each other. A very efficient mode ofproducing the necessarygranulation for filling up the opening, is by affording a mechanical support tothe edges of the tube, by means of a small gold plate."He goes on to inveigh against the principle of keeping anything in the
track and describes a case in which he achieved closure of a fistulawhich was a quarter of an inch in diameter.Coleman in 1881 writes that he had found that all fistulae closed
spontaneously when the antral tube or plug was removed even whenwashing out had continued for several years. " Larger openings theresult of necrosis," he writes, " we have closed by paring the edges anddrawing them together by silver wire sutures."
I have devoted some time to this historical introduction for severalreasons. Firstly to show that the close relation of the teeth to the sinusled to the realisation of its presence and then of its importance as a siteof disease. Secondly to show how this close relationship led to a methodof treatment of a diseased antrum at the time effective but now criticised.Thirdly to indicate the very real contribution to the subject made bydental surgeons of an earlier generation.
THE AETIOLOGY AND TREATMENT OF ORO-ANTRAL FISTULA
It is possible that the disadvantages of alveolar drainage, and the factthat it was used for cases where the maxillary sinus was already acutelyinfected, and where there were often many grossly decayed teeth, haveled to the view that the sinus must never be approached by this access.For a traumatic fistula of dental origin, repeated washouts by nasalpuncture are advised and often a nasal antrostomy is performed.
There still lingers a view that in a large proportion of cases perforationduring extraction occurs because the bone in the region of the apices issoftened or even necrosed as a result of infection from the tooth. Whateverthe conditions fifty years ago this is not the normal cause to-day. Pre-extraction radiographs are available in many cases and the liability tobilateral perforation points to an anatomical rather than a pathologicalcause. In many of the cases under discussion the fistula is an unfortunateaccident involving a healthy sinus. If infection supervenes, as it may do,the lining is irritated, but no irreversible change occurs. Washing out with
16

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
a suitable cannula through the fistula is far less traumatic than puncturein the inferior meatus. Whether the fistula will heal without operationdepends on its width, on its depth and on the original state of the antralmucosa, rather than on the site of irrigation.The surprising number of cases of oro-antral fistulae now being seen
is possibly due to a tendency to consider that every apex must be removedonce an extraction is commenced and to the use of fine apical elevators.The blind use of such instruments in the depth of a narrow molar rootsocket will result in the instrument pushing the root ahead of it in a pro-portion of cases. My records include two instances in which such instru-ments broke leaving a portion in the antrum. The treatment in one casewas as unusual as it was effective. Being seen in London and beingphysically quite fit, the patient was ordered to travel by British Railwaysfor admission to a special centre and removal of the portion of instrument.After fifteen miles of modern railway travel the foreign body was shakenthrough the fistula into the mouth. The fistula healed after a short periodof conservative treatment.
If the smaller fragments of roots are to be removed, and I think thereare indications for leaving some of them in situ in the absence of evidenceof apical or sinus infection, they must be exposed surgically from a lateralapproach and winkled out sideways or downwards under vision. Thisimplies the raising of a flap which when approximated by suture will gofar to exclude the possibility of a fistula.An exactly similar surgical exposure with precise approximation of
flaps should be employed when pre-operative radiographs indicate thatthe antrum may well be opened.
It is taught that every extracted tooth should be examined to see thatthe roots are complete. On occasion this inspection will reveal that a largeor small plate of bone with a smooth compact surface has remainedattached to the roots on the antral aspect. The antral mucosa may or maynot have separated in the process. This accounts, I think, for somegenuine cases in which no fistula is present immediately after operationbut develops a few days later. Due to failure of the socket healingmechanism the unsupported antral mucosa is later ruptured, probablyin blowing the nose. Whenever this appearance on the root is seen, thetests for fistula should be instituted. Fistulae tend to be valvular andseveral tests may be negative. The injection of a radio-opaque fluid isthe most positive test.The immediate simple treatment of an oro-antral fistula should be
approximation of the socket margins by suture, and completion of occlusionby the use of a ribbon gauze cover and not pack. Without appreciableraising and even undercutting of flaps or alternatively without removal ofa considerable height of the alveolar bone, it is not possible to achievecomplete closure of a large proportion of extraction wounds. Someremoval of the buccal alveolar crest is valuable. Simple sutures are tiedacross the socket anteriorly and posteriorly. Another suture is inserted
17

B. W. FICKLING
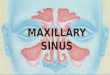
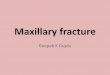
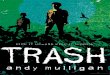
Fig. 2. Immediate simple treatment of an oro-antral fistula. The margins areapproximated with sutures and occlusion completed with a loose cover of ribbon
gauze tied into the opening of the socket.
across the middle of the socket, taking a slightly deeper bite of the tissues.A strip of half-inch ribbon gauze about two inches long is impregnatedwith whatever long acting bacteriostatic the dental surgeon has. I favouracriflavine emulsion, excess emulsion being removed and the gauze thenrolled in penicillin and sulphathiazole powder. Whitehead's varnish,idoform, or the practitioner's favourite socket sedative may be used.The gauze is folded into a flat cover the size of the socket and tied over theopening and just into any gap with the middle suture (Fig. 2). This ensuresocclusion and provides a scaffolding on which blood clot may organise.The gauze pack is removed on the second to the fifth day depending on thematerial incorporated in it, and the sutures on the fifth to the seventh day.If a denture is available it can be extended to cover the area.
The practitioner who has not the facilities for suture should not packthe socket or use antibiotic cones for there is a great tendency for part orall of the pack to enter the antrum, infection resulting. Radiographs areavailable showing zinc oxide and eugenol paste in the antrum, whichdeveloped an acute infection.
Should the patient be seen by an oral surgeon within thirty hours,primary closure with a buccal flap as later described should be performed.After this interval primary closure becomes less satisfactory, but might beattempted where the gingival tissue is suitable for suture, after irrigationof the sinus and the instillation of penicillin solution at the moment ofclosure. Where full facilities are available many of these patients canhave a general anaesthetic permitting complete and precise closure ofraw tissue to raw tissue.
Cases first seen with gross sinusitis are given a parenteral antibioticand the sinus washed out through thefistula with normal saline. A swab
18

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
is taken to check sensitivity to antibiotics. In most cases 2 ccs. of asolution of penicillin are left in the sinus after irrigation and this regimeis repeated several times daily for four to five days. Irrigation is continueduntil the sinus is clear.The patient presenting with an established fistula is treated conserva-
tively, the sinus being irrigated at intervals and watch kept for evidenceof infection. There are possible advantages in the use of a denture orbase plate to occlude the fistula so long as it is well fitting.A number of cases heal spontaneously, depending upon the size and
shape of the fistula, a deep socket being obviously more favourable.Cases may be observed for six to twelve weeks. The closure of very smallepithelialised tracks may be assisted by light cauterising of the surface.When healing is delayed operative closure is indicated and should
always be advised whenever there has been acute infection.Closure of oro-antral fistula by operationThe sinus is washed out from the mouth several times before operation.
Occipito-mental and dental radiographs are obtained, to assess the con-dition of the sinus and the presence of roots or other foreign bodies.A general anaesthetic is preferable.The operation is performed as follows: A circular incision just around
the fistula is made without cutting too deeply, and from this a buccalflap is outlined extending into the sulcus. When there is ample attachedmucoperiosteum on the buccal side this can be shaped symmetrically as forexposure of the buccal roots of a molar (Fig. 3). When the fistula is verymuch to the buccal side of the alveolus the flap may be based anteriorly
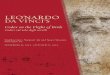
Fig. 3. Symimetrical wedge-shaped incisions outlining a buccal flap. The ink-well has already been dissected free and inverted.
19

B. WV. FICKLING
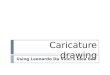
Fig. 4(a). An inkwell incision has been made around the fistula and a flap out-lined. In this case it is based anteriorly.
or posteriorly according to the tooth involved (Fig. 4). When the posteriorteeth are missing it can be based on the tuberosity. These incisions aredeepened to bone and the margin of the bony defect defined. This enablesthe operator to deepen the circular incision and dissect the fistula trackfrom its bony margins, leaving it attached deeply. Wlhen quite free twocatgut sutures are inserted with the knots on the inside of the fistulatrack, which when tied invert the fistula in the form of an unspillableinkwell (Fig. 5).An attempt is now made to draw the flap across the enlarged defect,
but it will not normally approximate without great tension. The flap isturned back and the periosteum only deliberately incised right across thebase of the flap. The site of this undercutting must be above the reflectionof the mucosa and must leave a free rectangle of periosteum of greaterextent than the bony defect. Incised vessels in the undercut must beclipped and if necessary tied. On two occasions the wound has had to bereopened when this was not efficiently performed initially. After thisincision of the periosteum, which is the only limiting membrane, thedegree to which the flap can be advanced and rotated has to be seen to beappreciated. As the incision is well above the reflection there is ampletissue in the base of the flap to ensure its viability. The margins of thedefect and of the flap are trimmed for perfect adaptation and approxi-
20

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
mated by at least four perfect horizontal mattress sutures of black silk-all inserted and held in forceps before one is tied. There is no place forcatgut as a suture material for oral mucoperiosteum. Special care istaken to close the vulnerable gap at the necks of adjacent teeth by usingsutures to wrap the soft tissue round the neck of the tooth.The creation of an inkwell not only provides some form of antral
floor, but indirectly ensures that the ultimate suture line is not placeddirectly over the original defect. Only in the larger defects, more than7 mm. across, can the inversion, as depicted in the diagram, be properlycarried out. Often the bony defect is also very small, and in such casesone only achieves close approximation of the epithelial walls of the trackwithout inversion, the sutured stump being pushed up and covered likethe appendix stump. The raw surface, however, is immediately in contactwith the periosteum of the new flap and healing is rapid. When the bonyopening permits, a fistula can be incised along a diameter to create alinear defect, which can then be inverted more correctly. Although
Fig. 4(b). The method of inverting the inkwell is shown. The incisions are madedown to bone and the flap advanced by undercutting the periosteum, well out in
the sulcus, where there is adequate thickness and blood supply.
21

B. W. FICKLING
*''11'' \\Fig. 4(c). The margins of the flap are trimmed for perfect adaptation and
approximated with numerous mattress sutures.
Fig. 5. Diagrammatic cross-section through an oro-antral fistula to show theinversion of the inkwell and the site and result of undercutting the periosteum.
22

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
sometimes the tissues are extremely friable every effort should be made toinvert some form of antral floor.A nasal antrostomy is performed only if there is persistent infection on
irrigation rather than on radiographic evidence of opacity or thickenedmucosa. In this case a tube is brought out of the nostril to permit dailyinstillations of penicillin solution. More rarely when roots or foreignbodies are present the anterior incision is carried upwards and forwardsto allow the sinus to be opened as described for the removal of roots.The chronic infection associated with a fistula causes some reaction of
the lining which will return to normal when the fistula is closed. Onlygross changes warrant an intranasal antrostomy or an opening to permitan inspection of the interior. Far from easing tension on the oral sutureline, a nasal antrostomy increases haemorrhage and later permits changes
Fig. 6(a). Oro-antral fistula 61 socket, mucosal thickening in right maxillary sinus.
23

B. W. FICKLING
Fig. 6(b). Closure as described. No antrostomy. Sinus clear.
in intranasal pressure to be transmitted more efficiently to the sinusfloor, so that breakdown as a result of an incautious sneeze or blow morereadily occurs.The follow-up has shown that this conservative attitude is justified, with
correspondingly less discomfort for the patient in the immediate post-operative phase (Fig. 6).The special features of the operation I have described are as follows.
Firstly, the attempt to create an antral floor by inverting, in inkwell form,the margins of an established fistula instead of paring them away. Second-ly, a buccal flap with periosteum on its deep surface, advanced by completeundercutting of the periosteum and therefore based on mucosa andsubmucosa. Thirdly, the general avoidance of an intranasal antrostomy
24

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
unless it is very strongly indicated. Fourthly, that while the provisionof a prosthetic cover and protection seems sound in principle, it has beenproved unnecessary when the surgery is equally sound. There is noquestion of sacrifice of alveolar contour to assist in approximation of theflap other than the normal oral surgical rounding of prominent margins.
After this operation had been developed, a review of the literatureshowed that various steps have been recorded previously, but, so far ascan be ascertained, not combined. Guthrie (1932) gave an excellentreview of alternative sites of flaps. Peet (1953) also reviewed operativeprocedures and strongly recommended a full Caldwell-Luc approach,a nasal antrostomy and a palatal flap, because of its valuable lining ofperiosteum. Most books on oral surgery also show the palatal flap aswell as a buccal flap (Archer, 1952).An inkwell operation adapted for fistulae following the Caldwell-Luc
approach was described by Claoue in 1929 while Zange in 1926 dissectedout the fistula and turned it in like an appendix stump. Berger, a dentalsurgeon, whose book in 1923 describes the subject well, in 1939 describedthe undercutting of the periosteum with a dental type buccal flap. Headvocated a series of small, shallow, spaced cuts lest the blood supplyof the flap be endangered. I have always incised right across the perios-teum well out above the reflection which gives much greater relief oftension. I have lost only one flap, when it was based on a recent Caldwell-Luc incision by another surgeon. This proved the efficacy of the inkwellmanoeuvre, for no fistula developed for thirty-six days in spite of the lossof oral mucosal cover.Through the courtesy of my colleagues at the Royal Dental Hospital,
I am able to quote an analysis of operations for oro-antral fistulae in theyears 1952-1956. For further comparison an analysis by Reading,Harrison and Dinsdale (1955) is also shown. The results of the techniqueI have described, performed by myself and my registrars, are included(Table I).
TABLE IOPERATIONS FOR CLOSURE OF ORO-ANTRAL FISTULAE MORE THAN ONE WEEK OLD
Average U 0 Ca ~~s~ uetgSeries No. Duration z c c ' ofFistula i a
of Fistula r. S* and simple =.2-~~~~ - ~~~~ Closure z-
Reading, Harrison, 102 94 65 ?65 8 58 58 %Dinsdale, 1951-1955 94% 65%
Staff of Royal Dental 35 5 months 28 31 29 20 4 29 83%Hospital, 1952-1956 and 2 at 88% 83%
8 yearsand over
Series now reported, 29 5 months 21 12 3 - Operation 28 96%1946-1956 ,. and 6 at 41% 10% as
5 years describedand over 23
253

B. W. FICKLING
Breakdown in the Royal Dental Hospital series occurred in those casesin which the lining had been curetted in a Caldwell-Luc operation. As aresult of their figures, Reading, Harrison and Dinsdale advocate a lesstraumatic operation with avoidance of the Caldwell-Luc exposure. I gofurther and urge the elimination of the antrostomy whenever possible.The relatively few antrostomies and very few Caldwell-Luc operations inmy series is emphasised.The cases were followed-up by examination, dental impressions and
radiographs or by questionnaire, with these results:Operation for closure of fistula
Examined .. .. .. 25Questionnaire .. .. 5Lost or died .. .. .. 4
Total . . 34
Average interval before follow-up just over two years (six months toeight years).Two cases referred to a rhinologist. One was washed out, which was
clear, and the symptoms subsided. One had a nasal discharge due topolypi which were said to be unrelated.
Three complained of excess colds or catarrh.
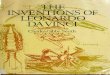
Fig. 7. An extension of the normal exposure for the buccal roots of an uppermolar with removal of outer alveolar plate over the displaced apex has exposedthe root in the antral floor. Such an incision must be carefully closed as already
described.
26

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
One complained of infra-orbital pain. There had been five previousattempts at closure elsewhere, closed by me at one operation.An assessment of the loss of sulcus is shown in Fig. 7.
Tooth roots displaced through the sinus floorTomes included an important section on roots displaced into the
antrum, and cites cases recorded by Cattlin (1859), who wrote a very fullarticle on the subject illustrated with specimens, some of which are stillin the College museum.The root may be entirely free in the sinus, it may be in the sinus but
lodged and attached to one wall by blood clot or inspissated secretions,it may be between the antral mucosa and the bony wall, it may be barelydisplaced from the socket or it may even be in the buccal soft tissues,outside the bony sinus wall altogether. It is not easy to establish byradiology the exact site of the root, even by stereoscopic methods. Thenormal canine fossa exposure does not give a good view of the floor ofthe sinus and might fail to find a root merely displaced outside the lining,a not uncommon site. As the patient has lost one tooth and often hasbone loss exposing the sinus at one site there is no good reason for openingthe sinus in another area with chance of damage to the roots of otherteeth and the infra-orbital nerve. The oral surgeon learns to removeapices of upper teeth which lie in the closest proximity to the sinus by adental approach. An extension of this approach upwards and forwardsand the removal of bone in a pyriform manner above the tooth involvedopens the sinus, but also provides access to the root should it lie in anyof the other tissue planes already described. The root is often immediatelyvisible only very little removed from its socket (Fig. 7). When free in thesinus it may be removed on the suction nozzle, in other cases the patienthas been elevated to an almost sitting position on the operating table andthe root washed out of the antrum through the alveolar hole which is atthe most dependant point. By enlarging the opening upwards and for-wards an access very similar to a Caldwell-Luc is obtained, but preferable,as it is at a lower level and inspection is much facilitated. In cleancases no antrostomy is performed. The sulcus incision is closed asdescribed for an oro-antral fistula, there being no inkwell. If there is anytension the buccal flap is advanced by undercutting the periosteum. Itfollows that this alveolar approach should only be employed by those whohave acquired the technique of closure and can be certain of success.The approach is suitable for any tooth from canine to second molar.A more anterior opening is required for the third molar. Operation shouldonly be undertaken when the root can be seen in radiographs obtained ashort while before operation. Dental films often give insufficient coverand occipito-mental films are almost useless.
IAn intact first molar tooth wholly displaced into the sinus, was similarlyremoved by enlarging the buccal side of the socket until the tooth couldbe rotated into the correct plane and withdrawn. The patient was agedeighteen and the model of the mouth three years later showed that the
273-2

B. W. FICKLING
TABLE IIOPERATIONS FOR ROOTS DISPLACED INTO THE MAXILLARY SINUS
Intervalbefore Site of Root
Operation * E . 838 .
StaffofRoal Detal129W 10 8 11 11 to All
-~~~~ - - -.2 ~~~~~~~~~n
2
C4)0E
4)4W W34 4 0 o0 0 060 >5 80 *;0r'O=00
0 0 a
Staff of Royal Dental 1 3 2 9 1 10 8 II1 1 1 8 AllHospital (average
34 840//months)
Series now reported 19 9 10 4 15 3 4 None None All(average
54 21%weeks)
second molar had moved forward as would normally occur, and the sulcuswas very little reduced.
Table II compares a series treated as described with a similar seriesanalysed by the courtesy of my colleagues at the Royal Dental Hospital.The cases were followed-up with these results:
Operation for root in antrumExamined .. .. .. 13Questionnaire .. .. .. 2Lost .. .. .. 3
Total .. .. .. 18
Average interval before follow-up just under three years (four and ahalf months to ten years).
All symptomless, except one complaining of some pain and catarrhalthough the root was outside the lining and was removed at seven weeks.
It may be emphasised that a fistula was made at operation in each ofthese cases and that healing was complete in every case.
The effect on the buccal sulcusThe loss of sulcus at the site of operation for both fistula and root in
antrum was assessed in the follow-up. The degree of loss of sulcus canbe demonstrated in cross-sections of models cast from muscle trimmedimpression of treated cases, cut through the area showing the greatestloss of sulcus (Fig. 8).The loss of buccal sulcus is minimal and is considered to be much less
than occurs with the more usual mucosal flap. It is possible that healingof the periosteal gap draws the sulcus tissues up to the bone whereas amucosal flap gives transverse scarring between cheek and alveolus.
28

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
Fracture of the maxillary tuberosityDuring the attempted extraction of an upper molar it is not uncommon
for a fracture of the bone of the tuberosity to occur, instead of the toothseparating from the bone as intended. Cattlin and Tomes describe severalremarkable cases of this type. It is usual to find that the sinus has extendedinto the tuberosity, which is thus weakened, and may be only a shell ofbone.
A AOperation this side Operation this side
Fig. 8. Cross-sections of models cast from muscle-trimmed impressions oftreated cases, cut through the area showing the greatest loss of sulcus.
When the fracture is diagnosed, a simple forceps extraction should notbe continued, for an oro-antral fistula is almost certain and may be com-plicated by extensive laceration of mucoperiosteum rendering repairdifficult. An attempt should be made to assess the size of the alveolarfragment. Radiographs are valuable and may reveal hypercementosisand attachment of adjacent or unerupted teeth.
It is usual in such cases to complete the removal of the tooth andfragment by raising a buccal flap, completing the dissection and closingthe defect by careful suturing, a general anaesthetic often being employed.With the larger fragments there is considerable loss of tuberosity contourand a liability to fistula. Fractures of the maxillary tuberosity occurringas a result of crashes and blows are treated conservatively by normal
29

B. W. FICKLING
methods of fracture treatment. After six to eight weeks teeth can beextracted surgically from the bony fragment with no fistula and with betterbony denture support. This conservative approach can be applied insuitable cases for the larger fragments of bone fractured during a dentalextraction.
TEETH DEVELOPING IN THE MAXILLARY SINUSRadiographs occasionally reveal teeth which are situated within the
anatomical boundaries of the sinus. Before deciding upon treatment thefull resources of radiology should be employed to determine the site andpathology involved. If changes suggesting a dentigerous cyst can bedetected then operation is indicated and is described later. A dischargingsinus may develop and require operative interference. Without suchobvious indications removal of an ectopic tooth in such a site should notlightly be undertaken, lest there be post-operative pain, and lest an oro-antral fistula develop. When operation is indicated an approach mustbe made via the antero-lateral wall of the sinus with meticulous closureof the oral incision. When the ectopic tooth lies just above an eruptedtooth removal of both teeth may well be indicated.FRACTURES OF THE FACE INVOLVING THE MAXILLARY SINUSThe maxillary sinus is involved in all fractures of the zygomatic bone
and in fractures of the maxillae along the lines Le Fort I and Le Fort II.Only brief reference can be made to this aspect of the subject. The opaqueantrum, and the break in continuity of the readily visualised lateral walland infra-orbital margin, as depicted in an occipito-mental radiograph,are the main radiological features. In treatment, the maxillary sinus isregarded as a means of access and support, and receives almost no specialconsideration. At operation the sinus is frequently entered through anincision in the labial sulcus and the zygomatic bone lifted with anelevator. When the orbital floor requires support, or the displacementrecurs, the sinus is commonly packed with ribbon gauze by the sameapproach, for ten to eighteen days.Dawson and Fordyce (1953) analysed 190 maxillary fractures and
Mansfield (1949) reviewed 153 zygomatic fractures treated at the centrein which I work. In only seven out of a total of 343 cases was there acuteinfection in the antrum, roughly 2 per cent. An oro-antral fistula with lowgrade infection persisted in 22 per cent. of the cases which were packed.That persistent infection and oro-antral fistula seldom follow thiscombination of traumatic and operative maltreatment is a measure of therecuperative resources of the sinus, especially as a nasal antrostomy isnot normally performed. These findings materially influenced me inreducing the number of occasions on which antrostomy was performedfor lesser trauma.WAR INJURIES INVOLVING THE MAXILLARY SINUS AND ALVEOLUS
Although more strictly a part of maxillo-facial surgery it is importantto include a reference to war injuries of the maxillary sinus. In the early
30

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
treatment of these cases the oral surgeon assists the plastic surgeon in thepreservation of all possible tissue and in maintaining a bony or prostheticscaffold on which the soft tissues may be supported. In the First WorldWar repair was often assisted by collapse of the bony fragments. In thelast conflict brilliant results were achieved by maxillo-facial teams who inthe earliest stages maintained viable jaw fragments in correct relationship,mainly by dental attachments. In the maxillae this can result in largealveolar or palatal defects and in marked adhesions joining cheek topalate. The replacement of tissue in the maxillae still lags behind thetechniques developed for the mandible, so that in many cases these defectswere ultimately filled with large prostheses. Recent work on the use oftubed flaps in palatal repair will be applied to these cases with improvedresults and bone grafting of the maxilla which is now being developedwill assist in providing a more firm base for prostheses.
Chronic infection in the maxillary sinus, and late separation of frag-mented or sequestrating bone undoubtedly delayed treatment in a numberof cases. Oro-antral fistulae in the labial sulcus in such cases can bedifficult to close owing to the great amount of scar tissue and the attemptmay lead to further development of adhesions. The late repair of such acase necessitates a high epithelial inlay and great skill is required to findthe correct plane between the maxillary sinus and the cheek tissues lestan oro-antral fistula be recreated. The sinus may, however, be largelyobliterated by scar tissue.
ORAL TUMOURS INVOLVING THE SINUSUnder this heading also come many cases which may be considered
outside the province of the oral surgeon, but some general principles maybe expressed. Apart from cysts, a mixed salivary tumour is most likely tolead the oral surgeon into the sinus. The palatal aspect of the tuberosity,centred on the greater palatine foramen, must be considered a relativelycommon site for this neoplasm, which may be of a sufficiently soft rubberyconsistency as to be mistaken for a cyst. Owing to the difficulty of radio-graphy in the region the lack of true bony outline may not be detected.A wide oro-antral fistula is very likely to follow operation, which shouldbe a wide excision owing to the tendency to recurrence.
In planning the wide removal of all tumours which will thus join thesinus to the oral cavity the possibility of covering the raw surfaces with asplit skin graft should be considered. In the maxilla an epithelial inlay istrouble-free and reduces post-operative pain, maintains contour and pro-vides very much better prosthetic retention. A large fistula occluded by awell-fitting prosthesis is preferable to a small fistula and an ill-fittingdenture.
CYSTS IN PROXIMITY TO THE SINUSThe differential diagnosis and treatment of radiolucent areas in the
region of the maxillary sinus provide some of the most difficult problemsin oral surgery. There is no doubt that the earlier writers on occasion
31

B. W. FICKLING
mistook cysts of the maxilla for collections of fluid in the sinus. One ofCowper's illustrations depicts a cyst or polyp in the sinus of unusualtype. The term hydrops antri was a cloak for some of these problems,a paper by Frank Coleman in 1942 doing much to clarify the position.Mural cysts in the antral mucosa still present a problem in diagnosis(Lindsay, 1942; Wright, 1946).Thomas Bell describes an infected cyst bulging into the antrum which
he caused to disperse by repeated puncture through an alveolar approach.In another case he resorted to washing out with neat Port wine, a solutionmuch favoured at that time by the surgeons, and probably by the patients.Improved techniques in radiology are giving increasing help in differen-
tial diagnosis. Whenever there is doubt, a medium gauge needle should beinserted by a valvular approach into the area, under local anaesthesia.In most cases this can be made to penetrate through any thin lamina ofbone if present. Contents are aspirated, tests for an oro-antral connectionare made and a radio-opaque fluid injected. After postero-anterior, truelateral and other radiographs the patient should adopt a sinus drainageposition for a short period and an occipito-mental view taken in theprone position. This may well demonstrate that the cavity communicateswith the nose.By such means the cases can be divided into four groups.1. A cyst, either dental or dentigerous, can be predicted.2. Some cystic outline seems apparent but a nasal connection is
demonstrated.3. The cavity is the maxillary sinus, possibly larger than normal.
The case should be transferred to a rhinologist.4. A solid tumour occupies the area. The treatment has been briefly
discussed.In the treatment of maxillary cysts, every effort must be made to prevent
an oro-antral fistula, which in these cases is usually large, troublesometo patient and operator, and largely avoidable.
Quite small cysts may be completely enucliated and the oral incisionclosed. Two main methods of treatment are available for larger cysts.The cyst cavity may be laid open to the mouth or be joined to the sinusand nose and the oral incision closed.The opening of the larger maxillary cyst to the mouth is widely prac-
tised. The cyst lining should be carefully inspected and the portionremoved for access always sent for histo-pathological examination.In the great proportion of cases the cyst lining should be left in situ onthe deeper aspect. It is a stratified squamous epithelium, very normalin appearance when cleaned of cyst debris and its retention limits the rawarea which is the cause of pain in post-operative treatment. The laminaof bone between the wall of a large cyst and the sinus may be very thinand is often absent, in which case a plane of cleavage may not be defined.The routine removal of cyst wall leads to a high percentage of fistulae.
32

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
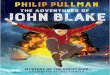
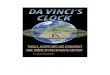
Fig. 9. A large cyst cavity almost obliterating the maxillary sinus treated by theParstch technique of opening to the mouth. It has been filled with radiopaquematerial for demonstration. The follow-up films after eighteen months show
regression of the cavity below the level of the palate.
The oral opening may be large or small, saucerised or the Parstchtechnique followed, depending on the shape of the cavity and the proxi-mity of teeth. The raw margin left at operation soon heals, and the cavity,which is easily cleaned, causes no trouble. Follow-up of cases treated inthis way has shown that the cavity fills in approximately eighteen tothirty-six months (Fig. 9).
Should the appearance of the cyst lining require its removal and afistula be present or possible, then the second method of treatment shouldbe followed which implies that the original incision should be capable ofclose suture.
33

B. W. FICKLING
The alternative treatment of opening maxillary cysts into the sinusand the nose and closing the oral opening is strongly advocated by somesurgeons.At this operation the cyst is exposed by an incision along the gingival
margin, or alveolar crest in edentulous cases, for it is essential that theultimate oral suture line should rest on bone to assist closure. The cystis exposed and opened and after bone removal the antral wall is completelyremoved so as to make one large cavity. The lining may or may not beenucliated. A large nasal antrostomy is a prerequisite of the operation,the oral approach being then closed. I am indebted to Mr. J. W. E.Snawdon who allowed me to see a series of cases treated by this method,the patients being free from all symptoms and the alveolar contourbeing excellent.Apart from certain specific indications for this operation my personal
preference favours the opening of cysts to the mouth, so that the cavitycan be kept under observation, lest a change in pathology or recurrencedevelop.
I have been fortunate in working in close association with plasticsurgeons, whose precise and often advanced techniques have colouredmy work. At first meeting the sinus as a complication, I found that theapplication of sound principles of plastic and oral surgery led to excellentresults. It was a natural step to extend these principles to establishedcases of sinus involvement of dental origin, with results which I haveattempted to describe.
I naturally desire to express my appreciation of the help I have at alltimes received from my colleagues, and to thank those who have workedwith me on these cases. In particular I wish to mention Mr. Fordyce formuch stimulating discussion and assistance and Mr. Boobyer and Mr.Herod for help in preparing the analysis. I am indebted to the photo-graphic staff of three hospitals for the illustrations.
SYNOPSIS(1) Historical introduction. The development of the oral approach to the
sinus and the contribution of dental surgeons.(2) The aetiology and treatment of oro-antral fistula:
(a) Emergency treatment;(b) Treatment when the sinus is infected;(c) Spontaneous closure;(d) Operative closure. The antral floor is reconstructed by means of an
inkwell dissection and a buccal flap carrying periosteum is advancedby undercutting. A nasal antrostomy is not normally performed anda full Caldwell-Luc exposure very rarely indeed. The literature isbriefly reviewed and operative results and follow-up described.
(3) Tooth roots displaced through the sinus floor. An oral surgical approachis described with minimal disturbance of the sinus and nose.
(4) Teeth developing in the sinus.
34

ORAL SURGERY INVOLVING THE MAXILLARY SINUS
(5) Fractures of the maxillary tuberosity and fractures of the facial bones.Sinus involvement in these cases is described and the implicationsdiscussed.
(6) War injuries are briefly reviewed.(7) The oral surgery of certain tumours involving the sinus.(8) The differential diagnosis and treatment of cysts and other radiolucent
areas in the sinus area. Careful pre-operative diagnosis is essential andfor most cases a conservative oral approach is advised.
REFERENCESARCHER, W. H. (1952) Manual of Oral Surgery. Saunders, Philadelphia, p. 322.AXHAUSEN, G. (1930) Dtsch. Mschr. Zahnheilk 48, 193.BELL, C. (1809) A System of Operative Surgery. Longman, London 2, 43.BELL, T. (1829) Anatomy, Physiology, and Diseases of the Teeth, London, p. 267.BERGER, A. (1923) The Principles and Technique of Oral Surgery. Dent. Items Pub. Co.,
Brooklyn, p. 191.(1939) Arch. Otolaryng. (Chicago) 30, 400.
CATTLIN, W. A. (1859) Trans. Odont. Soc. Lond. 2, 17.CLAOUI, C. (1929) J. Mid. Bordeaux 106, 178.COLEMAN, A. (1881) Manual of Dental Surgery and Pathology. Smith Elder, London,
p. 327.COLEMAN, F. (1942) Dent. Rec. 62, 124.COOPER, S. (1807) First Lines of the Practice of Surgery. London, p. 234.COWPER, W. (1707) In J. Drake. A New System ofAnatomy. S. Smith and B. Walford,
London 2, 536.-- (1698) The Anatomy of Humane Bodies. Oxford, for S. Smith and B.
Walford, London. Table 92.DAWSON, R. L. G., and FORDYCE, G. L. (1953) Brit. J. Surg. 41, 254.GUTHRIE, D. (1932) J. Laryng. 47, 459.HIGHMORE, N. (1651) Corporis Humani Disquisitio Anatomica. S. Brown, The Hague,
p. 226.LINDSAY, J. R. (1942) Laryngoscope (St. Louis) 52, 84.LEONARDO DA VINCI (1543) On the Human Body, edited by C. D. O'Malley and J. B.
de C. M. Saunders (1952). Schuman, New York, p. 44.MANSFIELD, 0. T. (1949) Brit. J. plast. Surg. 1, 123.PEET, E. (1953) Brit. J. plast. Surg. 6, 32.READING, P., HARRISON, D. F. N., and DINSDALE, R. C. W. (1955) J. Laryng. 69, 729.
- - -(1956) Brit. dent. J. 100, 233.ROSE, W., and CARLESS, A. (1898) A Manual of Surgerv. Bailliere, London, p. 669.SNAWDON, J. W. E. (1950) Dent. Practit. 1, 105.SYME, J. (1863) Principles of Surgery, 5th edition. Murray, London, p. 535.THOMSON, ST. C. (1911) Diseases of the Nose and Throat. Cassell, London.TOMES, J. (1859) System of Dental Surgery. London, p. 539.
and TOMES, C. S. (1887) System of dental surgery, 3rd edition. Churchill,London, p. 516.
VESALIUS, A. (1543) De Humani Corporis Fabrica. Oporinus, Basel.WRIGHT, R. W. (1946) Laryngoscope (St. Louis) 56, 455.ZANGE, J. (1926) Beitr. Anat., etc., Ohr. 23, 685.
DONATIONSRestoration and Development Fund:
£105 Mr. David Mitchell, F.R.C.S.
General Fund:£1,000 International Congress of Gastroenterology.£1,000 The Corporation and Members of Lloyd's and Lloyd's
Brokers.£50 Mr. C. H. Livingstone (per Professor C. A. Wells).
35