Embed Size (px)
Citation preview

Oral Pharmaceuticals in Anterior Segment Disease
Blair B Lonsberry, MS, OD, MEd., FAAODiplomate, American Board of Optometry
Pacific University College of [email protected]

OSDs are Difficult to Tell Apart: Overlapping Signs/Symptoms
SignsHyperemiaChemosisLid Swelling
SymptomsForeign Body SensationBurningDry, Gritty Ocular SurfaceItchy EyesPhotophobia Tearing

CASE

Case
• 20 year old male presents with a red painful eye– Started that morning when he
woke up– reports a watery discharge, no
itching, and is not a contact lens wearer
• SLE:– See attached image with NaFl
stain

Herpes Simplex Keratitis: Clinical Features
• Characterized by primary outbreak and subsequent reactivation
• Primary outbreak is typically mild or subclinical• After primary infection, the virus becomes latent in
the trigeminal ganglion or cornea• Stress, UV radiation, and hormonal changes can
reactivate the virus• Lesions are common in the immunocompromised
(i.e. recent organ transplant or HIV patients)

Dendritic Ulcers
6

Pediatric HSV Keratitis
• pediatric herpes simplex keratitis has an 80% risk of recurrence, a 75% risk of stromal disease, and a 30% rate of misdiagnosis
• 80% of children with herpes simplex keratitis develop scarring, mostly in the central cornea– results in the development of astigmatism– 25% of children have more than 2 D of astigmatism,
most of which is irregular• consider pediatric HSV when a patient has
unilateral recurrent disease in the anterior segment

Herpes Simplex Keratitis Management
• Topical:– Viroptic (trifluridine) q 2h until epi healed then
taper down for 10-14 days. • Viroptic is toxic to the cornea.
– Zirgan (ganciclovir) available, use 5 times a day until epi healed then 3 times for a week (US only)

Anti-Viral MedicationDrug Mechanism of Action Bioavailability Dosing Side Effects
Acyclovir Acyclovir interferes with DNA synthesis inhibiting viral replication
10-30% gets absorbedShort ½ life*Metabolized in kidneys
Simplex:400 mg 5x/dayZoster: 800 mg 5x/day
Overall very safeNausea, vomiting, headaches,dizziness, confusion
Valacyclovir Acyclovir pro-drug Equivalent to acyclovir but better for pain management
95% converted to acyclovir*Betterbioavailability and longer 1/2 life
Simplex:500 mg tidZoster: 1 g tid
Same as acyclovir
Famciclovir(Famvir)
Inhibits DNA chain elongationIt is metabolized to penciclovir where it is active 10-20x as long as acyclovir
Superior to acyclovir*
Simplex: 250 mgTIDZoster:500 mg TID
Same as acyclovir

HSV Stromal Disease
• HSV Stromal disease is an immune-mediated disease• Increased risk of scarring and high risk of poor visual
prognosis• Requires corticosteroids (HEDS: corticosteroid reduced risk of
progression by 68%)– Without epithelial defect: corticosteroids and prophylactic anti-viral
dosage– With epithelial defect: active infection anti-viral dosage with judicious
corticosteroids

How much to dose steroid?
• HEDS used QID of prednisolone phosphate • Current Recommendations:
– Mod – severe (especially with neo): 1% Prednisolone or Lotemax QID to 6x/day
– Want the lowest dose needed to control the inflammation
– AAO EBM Treatment Guideline 2014• Topical steroid for 10 weeks (this is based on HEDS results) with oral
antiviral

Herpes Simplex Epithelial Keratitis• Treatment Regimen:
– Zirgan 5x/day until the ulcer heals, then 3x/day for one week– Oral Valtrex 500 mg 3x/day for 7-10 days– Artificial tears
– L-Lysine 2 grams daily?• Proven to “slow down” and retard the growth of the herpes virus and
inhibit viral replication– Debride the ulcer?
• Prior to topical antiviral therapy debridement was treatment of choice• Generally try to avoid use of sharp instruments and use of cotton swab
and anesthetic
• RTC 1 day, 4 days, 7 days

Herpes Simplex Keratitis• Prophylactic Treatment:
– Reduces the rate of recurrence of epithelial and stromal keratitis by ≈ 50%
• Acyclovir 400 mg BID• Valtrex 500 mg QD• Famvir 250 mg QD
• L-lysine 1 gram/day:– Proven to “slow down” and retard the growth of
the herpes virus and inhibit viral replication
• Frequent debilitating recurrences, bilateral involvement, or HSV infection in a monocular patient

Prophylaxis??
• Pitfalls to Prophylaxis:– Reduction of recurrence does not persist once drug
stopped– Resistance????
• van Velzen, et. al., (2013) demonstrated that long-term ACV prophylaxis predisposes to ACV-refractory disease due to the emergence of corneal ACVR HSV-1.

Herpes Zoster

Herpes Zoster Ophthalmicus
18

Herpes Zoster
• Presents with:
– pain and tingling in region of skin supplied by V few days before lesions,
– malaise and fever,
– papulomacular then pustular rash,
– mucopurulent conjunctivitis,
– uveitis, glaucoma, episcleritis, keratitis, and retinitis can all occur.
– neurological complications include cranial nerve palsies and optic neuritis.


Herpes Zoster• Associated factors include increasing age, immune deficiency and
stress.• Only people who had natural infection with wild-type VZV or had
varicella vaccination can develop herpes zoster.• Children who get the varicella vaccine appear to have a lower risk
of herpes zoster compared with people who were infected with wild-type VZV.
• A person's risk for herpes zoster increases sharply after 50 years of age.
• Almost 1 out of 3 people in the United States will develop herpes zoster during their lifetime.
• A person’s risk of developing post-herpetic neuralgia also increases sharply with age.

Herpes Zoster• Management includes:
– oral antivirals:• 800mg acyclovir 5x/day • valacyclovir (Valtrex) 1g TID,• famciclovir (Famvir) 500 mg TID
– effectiveness of therapy is best started within 72 hours • Valacyclovir and famciclovir are preferred because of better
bioavailability and convenience– Pain management:
• tricyclic antidepressants, • Gabapentin• oral steroids

Herpes Zoster Ophthalmicus (HZO)
• Topical ganciclovir 5 times a day until healed, and then twice daily for 2 to 4 weeks is effective for dendriform keratitis, even in cases that have been unresponsive to oral antivirals41
• Topical corticosteroids: – management of stromal keratitis and uveitis, – often need to be continued at a low-dose chronically
and – require close monitoring for safety and efficacy

Herpes Zoster Ophthalmicus (HZO)
• Secondary glaucoma (16% to 56%) can occur because of inflammation or topical corticosteroids.
• Neurotrophic keratopathy:– complicated by persistent epithelial defects, – corneal melting with or without perforation, and – microbial superinfection– challenging to manage

Vaccine (Zostavax®)
• The Advisory Committee on Immunization Practices (ACIP) recommends zoster vaccine (Zostavax®) for people aged 60 years and older.
• The vaccine reduced the overall incidence of shingles by 51% and the incidence of PHN by 67%
• Even people who have had herpes zoster should receive the vaccine to help prevent future occurrences of the disease.
• In adults vaccinated at age 60 years or older, vaccine efficacy wanes within the first 5 years after vaccination, and protection beyond 5 years is uncertain



Corneal Ulcers • Infective bacterial and fungal corneal lesions cause severe
pain and loss of vision• Signs and Symptoms:
– Pain, photophobia, tearing– Mucopurulent discharge with generalized conjunctival
injection– Decreased VA (esp if on visual axis)– Possible AC reaction and hypopyon– Dense infiltrate– Satellite lesions around main lesion may indicate fungal
infection

Associated Factors
• Contact lens wear, especially soft and extended wear lens
• Recent history of corneal trauma
• Topical steroid use
• History of exposure to vegetative matter (fungal etiology)

• 1,2,3 Rule:
• 1 mm from visual axis
• 2 infiltrates (or more)
• 3mm or greater in size
• Nosocomial infections
• Immuno-compromised patient
• Post-surgical
When to culture?

Sterile vs Infectious Infiltrates

Peripheral (Sterile) Corneal Ulcer

Infectious Corneal Ulcer

Corneal Ulcers• The Steroids for Corneal Ulcers Trial (SCUT)• Conclusions:
– no overall difference in 3-month BSCVA and no safety concerns with adjunctive corticosteroid therapy for bacterial corneal ulcers
– researchers did find significant vision improvement for one specific subgroup of the study by using steroid therapy on patients with severe ulcers
• Application to Clinical Practice:– Adjunctive topical corticosteroid use does not improve 3-
month vision in patients with bacterial corneal ulcers unless in the severe category
Management• Infective ulcers need to be cultured!• If contact lens wearer, consider culture of
contact lens• Intensive topical antibiotic regimen,
consider fortified preparations, subconjunctival injections.– loading dose of
Vigamox/Moxeza/Zymaxid/Besivance 2gtts q 15 min x 1 hour,
– 1gt q 30 min x 6 hours, – 1 gt q 1 hr until f/u in 24 hours.

ARMOR
• Antibiotic Resistance Monitoring in Ocular Microorganisms (ARMOR)
• Approximately 42% of isolates were determined to be MRSA
• Newer fluoroquinolones have better activity than earlier generations
• Besivance has the lowest MIC values of all the fluoroquinolones
• Vancomycin is drug of choice if MRSA present• Azithromycin had very poor activity against Staph


Anti-inflammatory effects
• Degrade extracellular proteins• Tetracyclines inhibit MMPs• Anti-inflammatory

Pseudomonas case report
“Doxycycline as an adjunctive therapy…may help to stabilize corneal breakdown and prevent subsequent perforation.”
AM. McElvanney750

Anti-inflammatory Efficacy • Cortisol (hydrocortisone) is the standard of
comparison for glucocorticoid potency and is given an anti-inflammatory score of 1
• All of the other medications are given relative scores that allow direct comparison– Prednisone has a relative anti-inflammatory efficacy of 4
• Much easier to compare for systemic medications than topical because of the vast differences in tear films, drop delivery, etc.

Anti-Inflammatory EfficacyGeneric Name of Medication
Anti-Inflammatory Activity
EquivalentDose (mg)
Relative Sodium Retaining Activity
Hydrocortisone 1.0 20 mg 1.0
Prednisone 4.0 5 mg 0.8
Prednisolone 4.0 5 mg 0.8
Triamcinolone 5.0 4 mg 0.0
Methylprednisolone 5.0 4 mg 0.0
Dexamethasone 25.0 0.75 mg 0.0
Betamethasone 25.0 0.75 mg 0.0

Bioavailability of Systemic Steroids• Corticosteroids are readily absorbed from the intestinal
tract which makes oral dosages very effective • They are metabolized by the liver (must consider
function before prescribing) and excreted via the kidneys
• Long term steroid treatment must be tapered to avoid side effects – Even at doses as low as 15 mg of prednisone if the patient
has been dosed for several weeks• High dose oral steroids should be considered for initial
therapy– 1 mg/kg therapy and continued until uveitis has resolved

Systemic Corticosteroids
• Prednisone– Available as Oral: 1, 2.5, 5, 10, 20, 50 mg tablets (1
and 5 mg/mL solution and syrup, if needed)• Ocular Treatment Guidelines
– Mild to Moderate: Initial dose of 20-40 mg– Moderate to Severe: 40 – 60 mg – Severe: 60-100 mg
• IV Methylprednisolone 250 mg IV q6hours for 12 doses for arteritic ischemic optic neuropathy (giant cell arteritis)
• Similar dose given for active optic neuritis 2⁰ to MS

Steroid Treatment Pearls
• Specific type and location of inflammation determine route of administration
• I.e. treat the problem!– Topical, Systemic, Periocular, Intravitreal, etc.
• Must institute treatment immediately and at a high enough dose and frequency to suppress the inflammation

Indications for oral and IV steroids
• Inflammation of the posterior segment, optic nerve, or orbital tissues– Stubborn anterior uveitis – Posterior uveitis and/or chorioretinitis– Scleritis– Arteritic Ischemic Optic Neuropathy – temporal arteritis – Optic neuritis– Orbital inflammatory pseudotumor
• Also recommended for hypersensitivity reactions– Contact dermatitis, etc

Why Taper?
• To prevent rebound inflammation– Corticosteroids reduce the quantity and activity of
leukocytes
– Stopping cold turkey causes these white cells to proliferate and increase the production of inflammatory cytokines
– This means more steroids for a longer period of time which increases the risk of side effects

What is the “right way” to taper oral prednisone?
• Tapering is VERY case specific – no cookie-cutter method
• If the inflammation is mild and a low dose oral steroid is prescribed for less than a week, tapering is usually not needed
• Do NOT start tapering until the inflammation is resolved

Medrol Dosepak
• Methylprednisolone • Dosepaks have six 4 mg tablets that the
patients takes on day one, with the number of tablets reduced by 1 each day over the next 6 days in a tapering schedule (21 tablets total)
• Convenient dosing regimen with built in tapering

Side Effects of Systemic Corticosteroids
• Incidence increases with long-term high-dose therapy
• Length of use has greater link to developing side effects than dosage amount

Side Effects of Systemic Steroids• Metabolic Effects:
– HYPERglycemia can occur– Increased appetite, Weight Gain, and Redistribution of fat – Decreased calcium absorption – leads to Osteoporosis– Hyperlipidemia
• Mineralocorticoid Effects:– Fluid Retention (Increased Sodium Retention)– Hypertension – Edema (If liver/kidneys can’t keep up)
• CNS Symptoms: Euphoria, Insomnia, Psychoses, Depression, and Restlessness

Therapy Considerations• Diabetes
– Educate all Type 2 Diabetes patients that their blood sugar will likely become elevated
– Educate all Type 1 Diabetes patients they made need to alter their insulin levels
• Peptic Ulcers– Consider prescribing an H2 Blocker or a Proton Pump
Inhibitor if prednisone dose ≥60 mg or ≥30 mg over 2 weeks
• PPI’s: Omeprazole (Prilosec), Esomeprazole (Nexium), and Lansoprazole (Prevacid)
• H2 Blockers: Cimetidine (Tagamet), Famotidine (Pepcid), and Ranitidine (Zantac)

Steroid Considerations
• Also use caution in patients with: – Any Infectious disease – Pregnancy (Orals are Category C)– Chronic renal failure– Congestive Heart Failure– Systemic Hypertension– Osteoporosis– Psychoses

Allergic Conjunctivitis

Prevalence of Allergic Conjunctivitis
• Allergies affect as many as 40 to 50 million Americans
• Incidence and prevalence of allergic conjunctivitis has been rising over the last 40 years

Signs and Symptoms of Allergic ConjunctivitisClinical presentation – bilateral
Signs:– Conjunctival edema– Conjunctival hyperemia– Chemosis– Lid edema– Watery discharge
Symptoms:– Itching– Burning– Photophobia– Foreign body sensation– Blurred vision
HyperemiaLid edema and bilateral hyperemia Chemosis

Mast Cell Cascade

Treatment
• Ocular allergy sufferers need;– fast relief of signs and symptoms, – long-lasting therapeutic effects, – comfortable and safe topical drugs, – convenient treatment regimen
• Therapeutic focus is mostly confined to the suppression of mast cells, their degranulation and the effects of histamine and other mast-cell derived mediators.

Treatment of Ocular Allergy
Medications:• Topical OTC drops • Oral antihistamines (prescription and OTC) • Topical NSAID drops • Topical antihistamines• Topical mast cell stabilizers• Topical steroid drops• Topical dual-action drugs (antihistamine/mast cell
stabilizers)

Oral Allergy Medications
• Oral antihistamines (pills and liquids) ease symptoms such as: – swelling, – runny nose, – itchy or watery eyes, and – hives (urticaria).
• Some oral antihistamines may cause dry mouth and drowsiness.
• Older antihistamines such as diphenhydramine (Benadryl), chlorpheniramine (Chlor-Trimeton) and clemastine (Tavist) are more likely to cause drowsiness and slow reaction time. – these sedating antihistamines shouldn't be taken when driving or
doing other potentially dangerous activities.

OTC Allergy Medications
Generic Brand
Diphenhydramine Benadryl
Chlorpheniramine Chlor-Trimeton
Clemastine Tavist
Loratadine Claritin
Cetirizine Zyrtec
Fexofenadine Allegra (both OTC and Rx)

Prescription Allergy Medications
Carbinoxamine maleate ARBINOXA, PALGIC (tabs, solution)
Diphenhydramine HCI BENADRYL Injection
Hydroxyzine HCI HYDROXYZINE HCL (tabs, syrup)
Desloratadine CLARINEX (tabs, ODT, syrup)
Fexofenadine HCl ALLEGRA (tabs, ODT, suspension)
Levocetirizine dihydrochloride XYZAL (tabs, solution)
Montelukast SINGULAIR (tabs, chew tabs, granules)
Cromolyn sodium GASTROCROM (oral solution)
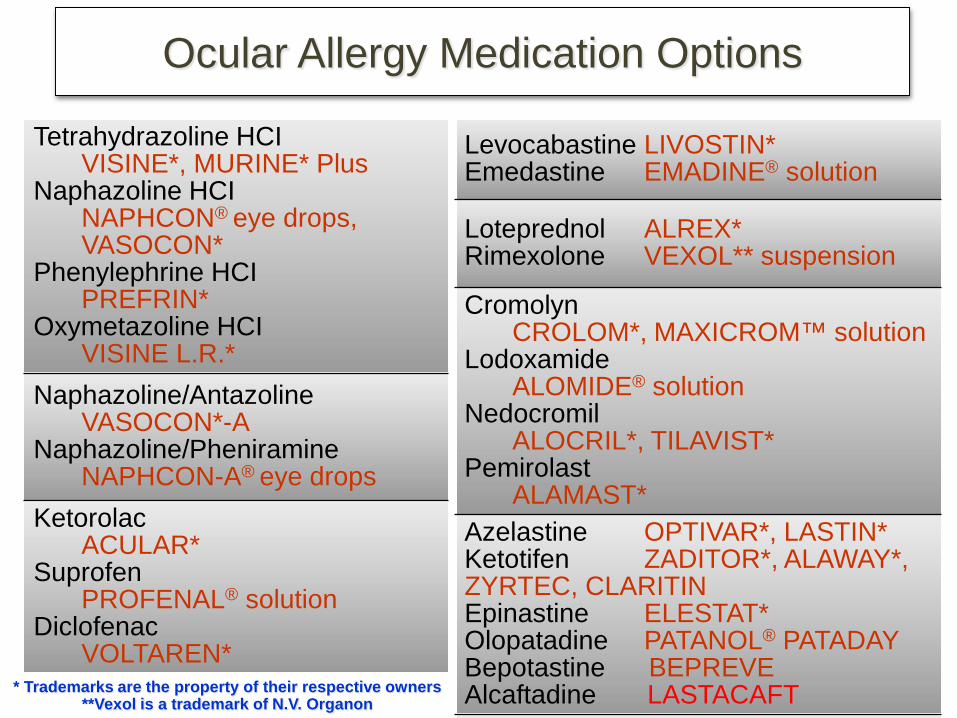
Ocular Allergy Medication Options
Tetrahydrazoline HCIVISINE*, MURINE* Plus
Naphazoline HCINAPHCON® eye drops, VASOCON*
Phenylephrine HCIPREFRIN*
Oxymetazoline HCIVISINE L.R.*
Naphazoline/AntazolineVASOCON*-A
Naphazoline/PheniramineNAPHCON-A® eye drops
KetorolacACULAR*
SuprofenPROFENAL® solution
DiclofenacVOLTAREN*
Levocabastine LIVOSTIN*Emedastine EMADINE® solution
Loteprednol ALREX*Rimexolone VEXOL** suspension
CromolynCROLOM*, MAXICROM™ solution
LodoxamideALOMIDE® solution
NedocromilALOCRIL*, TILAVIST*
PemirolastALAMAST*
Azelastine OPTIVAR*, LASTIN*Ketotifen ZADITOR*, ALAWAY*, ZYRTEC, CLARITINEpinastine ELESTAT*Olopatadine PATANOL® PATADAYBepotastine BEPREVEAlcaftadine LASTACAFT* Trademarks are the property of their respective owners
**Vexol is a trademark of N.V. Organon

Thank You!!!





























