Embed Size (px)
Citation preview
ORAL PATHOLOGY PROJECT
Amanda Mirabello2014
MEDICAL HISTORY
18 year old
Caucasian female
Negative medical history
Non-tobacco user
Adequate home care
INTRA-ORAL EXAMINATION
During routine intra-oral examination a short lingual frenum and splitting of the anterior tip of tongue were noted.
DESCRIPTION
Lingual frenum attached anterior on the tongue.
Tongue splits at anterior one third.
Intra-oral exam WNL
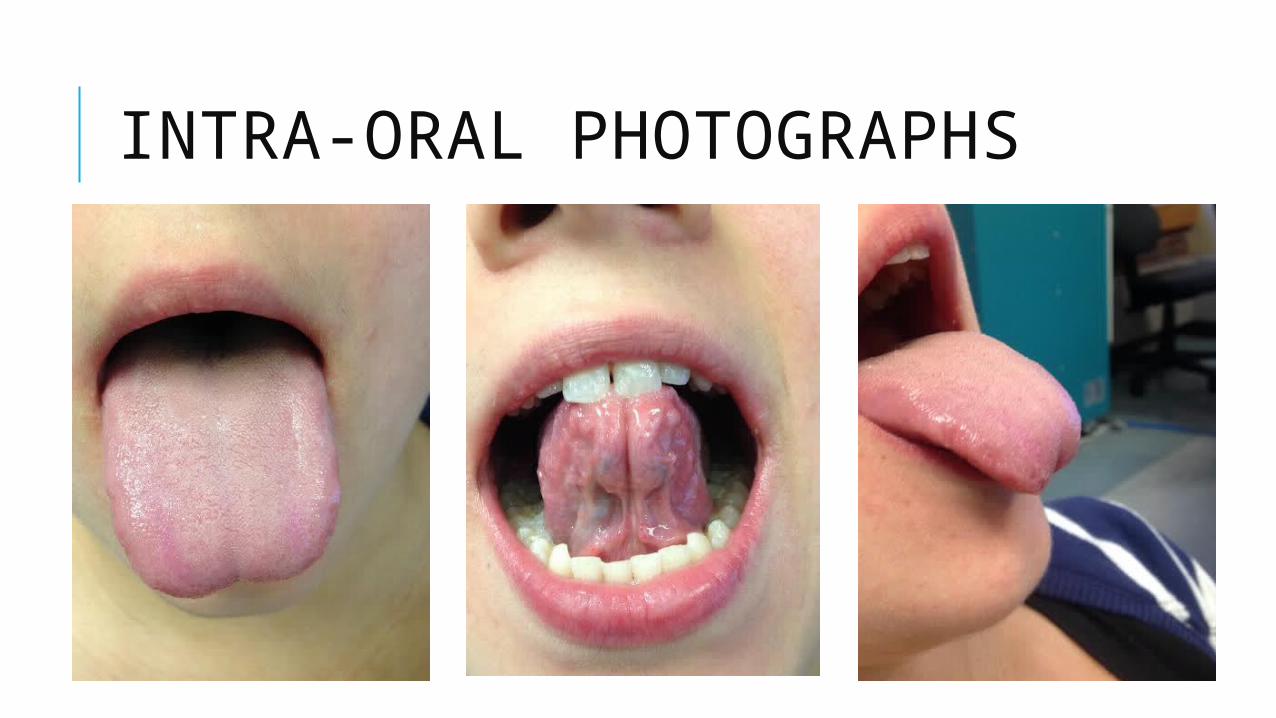
INTRA-ORAL PHOTOGRAPHS

INTRA-ORAL PHOTOGRAPHS
HISTORY OF ABNORMALITY
Patient states that her tongue has been split since birth.
Splitting of tongue has not caused any difficulties in speech, swallowing, or oral hygiene.
No history of trauma or piercings
SYMPTOMS
No pain reported
Normal upon palpation, no masses noted
Salivary glands WNL
Oropharynx and Larynx WNL
Voice WNL
No dysphagia noted
All other intra-oral and extra-oral exam findings WNL
DIFFERENTIAL DIAGNOSIS
1) Ankyloglossia:
- Pulling anteriorly on tongue causing it to appear bifid
- “Tongue Tied”
- Congenital
- Decreases mobility of the tongue tip
- Short, thick lingual frenum
- Mild-Complete
- Affects eating, speech and oral hygiene in more severe cases
DIFFERENTIAL DIAGNOSIS
2) Bifid Tongue:
- Congenital disorder occurring during fetal development in the 4th week
- Divided longitudinally at anterior
- Rare without other orofacial abnormalities
- Commonly seen in conjunction with syndromes and other orofacial abnormalities
DIFFERENTIAL DIAGNOSIS
3) Trauma to tongue:
- Possible biting of tip of tongue, or oral piercing causing splitting and scarring.
- Possible cosmetic surgery to achieve “snake tongue”

DIAGNOSIS PROCESS AND DIAGNOSIS Consulted on call dentist in clinic
Evaluated patient and ruled out any syndromes in conjunction with abnormality
Negative medical history
Bifid tongue in the absence of other orofacial abnormalities/syndromes = very rare.
No history of trauma or piercing to her tongue.
Due to the rarity of this abnormality without other symptoms or syndromes, and lack of trauma/piercing history: Ankyloglossia = diagnosis from the dentist on staff.
Intra-oral photographs were taken and Ankyloglossia bifid tongue was reported under intra-oral exam.
HEALTH PROMOTION METHODS Routine treatment was provided as planned.
Abnormality noted under patient’s intra-oral exam findings.
No effect on speech
No dysphagia
Prognosis abnormality is good.
BIBLIOGRAPHY
DMB Hall, M. R. (2005). Tongue Tie. Retrieved from Archives of Disease in Childhood : http://adc.bmj.com/content/90/12/1211.1.full
Kumar L. K. Surej, N. M. (2010). Isolated Congenital Bifid Tongue . Retrieved from National Journal of Maxillofacial Surgery: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3304211/.
P.S Flemming, T. F. (2005). Bifid Tongue- a complication of tongue piercing. Retrieved from British Dental Journal: http://www.nature.com/bdj/journal/v198/n5/full/4812117a.html
THANK YOU !