-
7/30/2019 Oral Pathology Case Report
1/12
AMELOBLASTOMA
Doloso, Shyra Jane B.
DMD 2- CAD
-
7/30/2019 Oral Pathology Case Report
2/12
Amelobalstoma
A benign, aggressive tumor that is invasive and persistent.
Sometimes its called solid or multicystic ameloblastoma
Adult most commonly affected
Mandibular molar- ramus most commonly affected site
Broad range age range: maen 40 years old
Unilocular or Multilocular
Recurrence rate higher with conservative treatment
No gender predilection
They grow quickly and can change and destroy bone around
them
Radiographically it appears osteolytic,typically found at tooth
bearing areas of jaws and maybeeither unilocular or multilocular.
Margins are usually well defined and sclerotic.
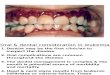
Clinical Features:
facial deformity
difficulty moving your jaw
loosening of your teeth
swelling
-
7/30/2019 Oral Pathology Case Report
3/12
DEFINITION OF TERMS
Ameloblastoma - is a benign odontogenic tumor arising from the
residual epithelial
components of tooth development
Hemimandibulectomy- is a procedure whereby one half of the
mandible is
removed surgically.
Reconstruction of the mandible - mandible is to restore the
shape and function of the face,
the continuity of the mandible and the muscular attachment
Osteotomy is a surgical procedure that involve bone-cutting.
Incision- cutting or surgical cut in the skin or flesh
Hemostasis- act of stopping blood from flowing
Gigli Saw - is another instrument used to carry out osteotomy.
The instrument has two handles,
and a lengthwise twisted stainless-steel wire is hooked to
them.
Suture is a process of joining two surfaces or edges together
along a line by or as if by sewing.
-
7/30/2019 Oral Pathology Case Report
4/12
Patients Information
16 years old
M
Student
Filipino
Complete Patient History
Chief Complain
Namamaga po ang aking baba
My jaw is swelling
History of Present Illness
The patient has history of incision and drainage three years ago
and comes for consult because
of the swelling at the left side of his mandible. He was put on
antibiotics for a week but noticesthere no change. The swelling
becomes bigger and bigger. There is also minimal displacement
of
the teeth. The patient requested X-ray examination of his left
mandible.
Medical History
Never been hospitalized
Not taking any medications
Does not have an allergies
Dental History
No Restorations
No Extractions
-
7/30/2019 Oral Pathology Case Report
5/12
History of incision and drainage
Social History
He doesnt smoke and He doesnt drink alcohol
Patients Dental Chart
-
7/30/2019 Oral Pathology Case Report
6/12
Diagnostic Findings
-
7/30/2019 Oral Pathology Case Report
7/12
-
7/30/2019 Oral Pathology Case Report
8/12
Diagnosis
Preliminary Diagnosis : Ameloblastoma
Tentative Diagnosis : Ameloblastoma
Differential Diagnosis.
Odontogenic Keratocyst
AMELOBLASTOMA
An ameloblastoma is a benign but
locally agressivetumour arising from
the mandible, or less commonly from
the maxilla.
Epidemiology
Ameloblastomas are the second
most common odontogenic
tumor and account for up to a
3rd of such cases.
They are slow growing and tendto present in the 3rd to 5th
decades
of life, with no gender
predilection
Pathology
Ameloblastomas (notsurprisingly) arise from
ameloblasts, (part of the
odontogenic epithelium,responsible for enamel
production and eventual crown
formation).
Radiographic Features
Well defined radiolucent area
Rounded or scalloped margin
Some are unilocular but majority
are multilocular
ODONTOGENIC KERATOCYST
An odontogenickeratocyst
(OKC) is a type of developmental
cyst involving the mandible ormaxilla.
Epidemiology
Odontogenickeratocysts typicallypresent in younger patients (2nd
-
3rd decades), are often multiple,
and may be seen in either the bodyor ramus of mandible
(approximately 70% of all OKCs),
ormaxilla. There may be male
predilection.
Pathology
OKCs originate from epithelialcell rests (stratified
squamous
keratinizing epithelium) found
along the dental lamina and
periodontal margin of the alveolusof the mandible.
http://radiopaedia.org/articles/missing?article%5Btitle%5D=maxillahttp://radiopaedia.org/articles/missing?article%5Btitle%5D=maxilla
-
7/30/2019 Oral Pathology Case Report
9/12
Radiographic Features
Typically rounded. Radiographic
margins are usually well defined
and sclerotic. Multilocular
radiolucencyScalloped
margin.When loculations are large,
the appearance is called as SOAP
BUBBLEappearance
TYPES OF AMELOBLASTOMA
SOLID/ MULTICYSTIC AMELOBLASTOMA
HISTOPATHOLOGICAL SUBTYPES OF SOLID AMELOBLASTOMA
FOLLICULAR
Islands of epithelium resemble dental organ surrounded by mature
connective
stroma.Individual follicles show central mass of stellate
reticulum like cells surrounded by a
single peripheral layer of ameloblast like cells. Nuclei of
peripheral cells are reversely polarized.Within the islands, cyst
formation is common.
PLEXIFORM
Instead of islands, long, anastomosing cords and occasional
sheets of epithelial cells
bounded by columnar cuboidal cells.Cells within cords are more
loosely arranged thanperipheral cells.Supporting stroma is loose
and vascular. Cyst formation occurs, not inside
follicles, but in surrounding stroma.
ACANTHOMATOUS
Central area of follicles show extensive squamous metaplasia,
often associated with
keratin formation.Does not indicate a moreaggressive course of
tumor
Can be confused with squamous cell carcinoma.
GRANULAR CELL
Follicles / sheets of cells show granular cell change.These
cells have abundant cytoplasm filledwith eosinophilic granules.Seen
in younger persons and appears to be more aggressive clinically
BASAL CELL TYPE
Least common typeComposed of nests /sheets of hyperchromatic
basaloid cells.No stellatereticulum present centrally and
peripheral cells tend to be cuboidal rather than tall columnar
-
7/30/2019 Oral Pathology Case Report
10/12
UNICYSTIC AMELOBLASTOMA
SUBTYPES OF UNICYSTIC AMELOBLASTOMA
o LUMINAL
Tumor is confined to luminal surface of cyst.Seen as fibrous
cyst wall with lining
comprised totally / partially of ameloblastic epithelium,
showing a basal layer of columnar /
cuboidal reversely polarized cells .Overlying epithelial cells
are loosely adhesive, resembling thestellate reticulum of dental
organ.
o INTRALUMINAL
This variant shows the tumor from cyst lining protruding into
the lumen of cyst.
Intraluminal projections resemble plexiform ameloblastoma in
most cases, though not always.
o MURAL
In this type, the fibrous wall of the cyst is infiltrated with
typical follicular / plexiform
ameloblastoma.Believed to be more aggressive than other two
variants
-
7/30/2019 Oral Pathology Case Report
11/12
TREATMENT
Hemimandibulectomy and Reconstruction of Mandible
Before Surgery :
Evaluate any other medical problems
Pulmonary function test (PFT)
Cardiac stress test to evaluate your heart.
Anesthetic Requirements
GENERAL ANESTHESIA
Surgery
Incision
Hemostasis
Occlusion setting with wiring
Resection of the lesion
Reconstruction of Mandile
Placement of titanium plates with and without bone Graft
Suturing
After Surgery
* Tubes,Drainage,Catheters and Other Medical Devices
>A humidifier collar placed over your trach tube. It will
provide moist air to your lungs
> The intravenous (IV) line through which you will
receive:
-
7/30/2019 Oral Pathology Case Report
12/12
Fluid.
Antibiotics.
Pain medication.
Anticoagulants (to prevent your body from forming blood clots in
the surgical area).
>A Foley catheter to drain urine from your bladder. It is
removed two or three days after
surgery.
>A feeding tube through your nose into your stomach. You will
get high-protein liquid feedings
and your medicines through this tube. You will not be able to
eat and drink until the swelling
from the surgery goes
down.
*Self Care
*Oral Irrigation
As soon as the rubber bands are removed, you will begin
irrigating (wetting) your mouth
with salt water and baking soda. This helps keep your mouth
clean and moist.
*Diet
Most patients are discharged on a pureed diet. This means that
foods have been put through a
blender
*Follow-up Appointments
COMPLICATIONS
Blood clot
Speech and swallowing
Bleeding
Numbness
Infection