Embed Size (px)
Citation preview

Oral Nutrition Support in Cancer- Does it help?
By Artika Datta Specialist Dietitian
Head and Neck Oncology and Home Enteral Nutrition
Addenbrookes Hospital, Cambridge
Email: [email protected]

Agenda
Why nutrition? Objectives of nutrition support Assessment Oral nutrition supplements – what is the
evidence Novel supplements Summary References

Malnutrition
Affects 40-80% of cancer patients
Prevalance factors
46- 61% of patients with lung cancer and
mesothelioma experience weight loss before
diagnosis and treatment (Brown and Radke, 1998)
Approx 80% of patients in advanced stages
have cancer cachexia (Goo and Hill, 2003)

Why Nutrition ?
Up to 85% of patient with GI tumours are
malnourished (Stratton et al., 2003)
Head and Neck Cancer – the incidence can range from
40 - 58% (Connally, 2004; Grobbelaar et al., 2004)
Risk increases with multi-modality treatments
75-80% of patients with H&N cancer have
significant weight loss (>10% of BW) during treatment
period (Hammerlid et al., 1998; Lopez et.al., 1994)

Consequences
BMI of <18.5 kg/m2 and/or unintentional weight loss of > 10% (over the preceding 3 mths) associated with increased risk of perioperative complications (NICE, 2006)
Reduced QOL
Increased length of hospital stay
Increased risk of death
Up to 20% of cancer patients die of the effects of malnutrition rather than of the malignancy itself (Ottery, 2004)

Objectives of Nutrition Support
To maintain physical strength and optimise status within the confines of the disease during treatment and in many cases for
several months post discharge
prevent or correct nutritional depletion reduce the nutrition-related side effects and
complications Improve tolerance of, and response to cancer
treatment maintain strength and energy maintain quality of life Reduce period of hospital stay

Nutrition Screening
Early identification and intervention can
Promote recovery
Improve prognosis
Cost effective
Reduces complication rates
Reduces length of hospital stay

Assessment
Subjective global assessment (SGA) – simple, reliable and inexpensive
Assesses nutritional status based on the features of:
a history
physical examination

Oral Nutrition Supplements
A simple, non-invasive method of increasing
nutrient intake
Most ONS are nutritionally complete
Majority contain 1-1.5 kcal/ml, but also
available as ‘concentrated’ feed (2kcal/ml)
Protein content varies from 4 to 10g/100ml
Available in liquid form, soups, powders, and
other consistencies such as puddings
Compliance is dependent on appetite and taste

Oral Nutrition Supplements
Appropriate prescription
Studies limited in cancer patients
May improve energy and protein intake
ONS significantly increased dietary
intake (381 kcal/day, 95% CI 193 to 569
in 3 RCTs) in patients undergoing
radiotherapy (Elia M et al, 2006)

Impact on Nutrition Outcome
75 patients with Head and Neck cancer Referred for Radiotherapy (RT) Randomised to:
Group 1 (n=25) patients who received dietary counseling with regular foods
Group 2 (n = 25), patients who maintained usual diet plus supplements
Group 3 (n = 25), patients who maintained intake ad lib
Ravasco et.al, 2005 Head and Neck, 27, 659-68.

Methods and study design
Inclusion criteria : Referral for RT and absence of renal disease and/or diabetes mellitus
Study design:
Total Patients
Men Women Mean Age
Stage I/II
Stage III/IV
75 60 15 60+/- 11
yrs 30
Patients 45
Patients

Methods and study design
ONS used were ready-to-use, high protein,
energy-dense liquid formulations
Each 200ml can provided 20 g of protein and
200 kcal
Amount of ONS – 2 cans/d, which covered the
calculated requirement

Study measures
Evaluated the following at baseline, at the
end of RT, and at 3 months:
Nutritional intake
Nutritional status
QOL

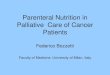
Results: Nutritional Intake

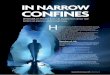
Results: Nutritional Status

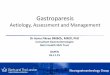
Results: QOL
At end of RT
Group 1 – all function scores improved and
proportional to an increase in Energy and
Protein intake
Group 2 – all function scores improved but
proportional to an increase in Protein intake
Group 3 – all function scores worsened

Results: QOL
At 3 months follow up
Group 1 - all maintained or improved overall
QOL
Group 2 – all maintained or experienced
decline in QOL
Group 3 – function scores further
deteriorated

Discussion
Nutrition intervention was central
ONS not as effective as dietary counselling
Impact of ONS on energy intake short lived

Novel Supplements
n-3 fatty acids arginine, glutamine, nucliec
acids, and antioxidants
Immmuno-modulatory effects
Perioperative supplementation with arginine,
ribonucleic acids and n- fatty acid resulted in
fewer wound infections than control group in
patients with laryngeal and oral cancers
( Casas-Rodera P et al 2008)

Novel Supplements
ONS containing n-3 PUFA beneficially affected nutritional status of patients with Stage III Non-Small Cell Lung Cancer during Multimodality treatment (Van der Meij Bs et al, 2010)
Limited evidence to support the use of fish oils for
management of cachexia
Fearon KC et al (2006) in their double blind, placebo
controlled trial of 518 weight-losing patients with
advanced gastrointestinal or lung cancer showed no
statistically significant benefit from single agent
EPA (2g or 4g) in treatment of cancer cachexia

A Cochrane review
5 trials (involving 587 participants) met the inclusion criteria 3 trials compared EPA at different doses with
placebo 2 two trials compared different doses of EPA with
an active matched control (but without EPA) Outcomes measured
Primary outcomes- weight gain, body composition, median survival
Secondary outcome - functional or performance status, improvement in quality of life, energy expenditure, reduction in fatigue, nutritional status, compliance rates, side effects, adverse events
Dewey et.al (2007) Cochrane Database Syst Rev, 24(1)

Conclusion
Insufficient data.
No evidence that EPA improves symptoms
Need to conduct further research

Summary
Little or no beneficial effects of ONS in
terms of weight gain
Some evidence that ONS can increase total
energy intake and improves QOL indices
Inconsistent results on the effects of EPA
ONS prescription
Dietary counseling

References
Brown JK and Radke KJ (1998). Nutritional assessment, intervention and evaluation of weight loss in patients with non small cell lung cancer. Oncology Nursing forum, 25, 547-553.
Casas-Rodera P, Gomez-Candela C, Benitez S, et al (2008) Immonuenhanced enteral nutrition formulas in head and neck cancer surgery: a prospective, randomised clinical trial. Nutr Hosp, 23(2), 105-10.
Connally, C (2004). Head and Neck cancer: preventing malnutriiton. World of Irish Nursing, 12 (8), 27-28.
Del Fabbro E, Baracos V, Denmark-Wahnefried W, Bowling T, Hopkinson J and Bruera E (2010) Nutrition and the Cancer Patient: Oxford University press Inc., New York
Dewey A et.al (2007) Eicosapentaenoic acid (EPA, an omega-3 fatty acid from fish oils) for the treatment of cancer cachexia. Cochrane, January 2007
Elia, M. A.E. Van Bokhorst-de van der Schueren, J. Garvey, A. Goedhart, K. Lundholm, G. Nitenberg, R. J. Stratton (2006) Enteral (oral or tube administration) nutritional support and eicosapentaenoic acid in patients with cancer: A systematic review. International Journal of Oncology, 28: 5-23
Fearon KC, Barber MD, Moses AG et al (2006) double-blind, placebo-controlled, randomised study of eicosapentaenoic acid diester in patients with cancer cachexia. Journal of Clinical Oncology, 24(21), 3401-7.
Goo, C and Hill, D (2003). Nutrition Support in Cancer. Clinical Nutrition Update, 8, 3-5. Grobbelaar, EJ, Owen S, Torrance AD and Wilson JA (2004). Nutritional challenges in head
and neck cancer. Clinicla Otolaryngology and Allied Sciences, 29 (4), 307-313. Hammerlid E, Wirblad B, Sandin C, Mercke C, Edstrom S, Kaasa S, Sullivan M and Westin
(1998). Malnutrition and food intake in relation to Quality of life in Head and Neck cancer patients. Head &Neck, 20(6), 540-548.

References
Kern KA & Norton JA (1988): Cancer cachexia. J. Parenter. Enteral Nutr. 12, 286 – 298. Lopez, MJ, Robinbson P, Madden T and Highbarger, T(1994). Nutritional support and
prognosis in patients with head and neck cancer. Journal of Surgical Oncology, 55 (1), 33-36 Massad LS, Vogler G, Herzog TJ, Mutch DG (1993). Correlates of length of stay in
gynecologic oncology patients undergoing inpatient surgery. Gynecol Oncol 51, 214–218. Obermair A, Hagenauer S, Tamandl D, Clayton RD, Nicklin JL, Perrin LC et al. (2001). Safety
and efficacy of low anterior en bloc resection as part of cytoreductive surgery for patients with ovarian
cancer. Gynecol Oncol 83, 115–120. Ollenschlager G, Viell B, Thomas W, Konkol K & Burger B (1991): Tumour anorexia: causes,
assessment, treatment. Rec. Results Cancer Res. 121, 249 – 259. Ottery FD. Cancer cachexia: prevention, early diagnosis, and management.Cancer Pract
1994;2:123–31 Shike M (1996): Nutrition therapy for the cancer patient. Hematol. Oncol. Clin. N. Am. 10,
221 – 234. Stratton RJ, Green CJ, and Elia, M (2003). Disease-related malnutrition: an evidence based
approach to treatment. Wallingford: CABI Publishing. Van der Meij BS, Langius JA, Smit EF, Spreeuwenberg MD et al (2010) Oral Nutritional
Supplements containing (n-3) Polyunsaturated fatty acids affect the nutritional status of patients with stage III Non-Small Cell Lung Cancer during Multimodality Treatment. Journal of Nutrition, Aug 25 (Epub ahead of print)