Embed Size (px)
Citation preview

Oral Manifestations of Celiac Disease
Sara Ahmed, DMD Assistant in Pediatric Dentistry ,
Boston Children’s Hospital Instructor in Developmental Biology, Harvard School of Dental Medicine
Disclosure
• I have no relevant financial interest, arrangement, or affiliation with any manufacturers of any commercial products to disclose

Objectives
• Identify common dental presentations in celiac disease
• Recognize causes of dental presentations
• Understand how to treat dental complications of the disease

Celiac Disease – Background
• Schuppan D. Current concepts of celiac disease pathogenesis. Gastroenterology. 2000;119:234–242 • “What is Celiac Disease?” Understanding Celiac Disease Celiac. Disease Foundation. Web. 2 March 2017.
• Celiac Disease (CD): a chronic autoimmune disorder in which predisposed individuals are not capable of digesting gluten
• Gliadin, a protein component of gluten, causes an inflammatory reaction
• Gluten digestion leads to damage of the small intestinal mucosa
• T & B cell mediated immune response leads to flattening of small intestinal villi and eventual atrophy

Rashid, Mohsin, et al. "Oral Manifestations of Celiac disease: A Clinical Guide for dentists." J Can Dent Assoc 77 (2011): b39.
• Healing of the intestinal mucosa is possible with a strict adherence to a gluten–free diet
• 1% of North Americans may have this disease based on serologic studies; however 90% may go undiagnosed
• Oral manifestations can help identify early signs of CD before it progresses
Celiac Disease – Background

Rashid, Mohsin, et al. "Oral Manifestations of Celiac disease: A Clinical Guide for dentists." J Can Dent Assoc 77 (2011): b39.
Oral Manifestations
1) Enamel Defects
2) Recurrent Aphthous Ulcers
3) Dry Mouth Syndrome
4) Delayed Eruption
5) Atrophic Glossitis
6) Oral Lichen Planus
7) Cheilosis

Oral Manifestations
1) Enamel Defects
2) Recurrent Aphthous Ulcers
3) Dry Mouth Syndrome
4) Delayed Eruption
5) Atrophic Glossitis
6) Oral Lichen Planus
7) Cheilosis

Rashid, Mohsin, et al. "Oral Manifestations of Celiac disease: A Clinical Guide for dentists." J Can Dent Assoc 77 (2011): b39.
Enamel Defects
• Most commonly affect the permanent dentition
• Occur symmetrically and chronologically in all four quadrants of the mouth
• Number of teeth affected are directly correlated with time of symptom onset
• The maxillary and mandibular incisors and molars are most affected

• Develop if celiac disease is noted during the development of permanent teeth (during enamel layer formation)
• Develop before the age of 7
• Irreversible
• Not commonly seen in those with adult-onset CD, as onset is after permanent tooth development
Enamel Defects

Dental Growth and Development. American Academy of Pediatric Dentistry. 337
Sequence of Eruption

Enamel Defects - Mechanism
• Immune mediated damage - possible hypothesis states that gluten in the oral cavity stimulates naïve lymphocytes
• Disturbances in nutrient absorption such as hypocalcemia
Rashid, Mohsin, et al. "Oral Manifestations of Celiac disease: A Clinical Guide for dentists." J Can Dent Assoc 77 (2011): b39.

• Rashid, Mohsin, et al. "Oral Manifestations of Celiac disease: A Clinical Guide for dentists." J Can Dent Assoc 77 (2011): b39. • Muggiano F, Quaranta A, Giannantoni I. Major dental clinical pathological manifestation of celiac disease. WebmedCentral Oral Medicine
2013;4(11):WMC004448 • “Stages of Tooth Decay” Favero Family Dental. Web. 12 March 2017.
Enamel Defects - Mechanism
• Hypoplasia and hypomineralization of the enamel leads to discolorations, pitting, grooving and complete loss of enamel
• Alteration in quantitative and qualitative mineralized dental tissue

Enamel Defects – Classification
Aine Classification System (1986) for enamel lesion in CD
• Grade 1: Defect in the color of enamel - single or multiple cream, yellow or brown opacities
• Grade 2: Slight structural defects - rough enamel surface, horizontal grooves, shallow pits
• Grade 3: Evident structural defects - deep horizontal grooves, large vertical pits
• Grade 4: Severe structural defects - shape of tooth may be changed

• Grade I: multiple white and cream opacities with clearly defined margins
• Grade II: rough enamel surface with patchy symmetric opacities and discoloration
Enamel Defects – Classification

http://pocketdentistry.com/enamel-defects-in-the-permanent-dentition-prevalence-and-etiology/
Enamel Defects – Classification
• Grade III: deep horizontal grooves with large pits and linear discoloration
• Grade IV: Severe structural defects; shape of the tooth may change

Enamel Defects - Epidemiology
• Prevalence in mixed or permanent dentition ranges from 9.5% to 95.9% (mean 51.1%)
• Prevalence in primary teeth ranges from 5.8% to 13.3% (mean 9.6%)

Enamel Defects – Differential Dx

Enamel Defects - Treatment
• No treatment
• Composite
• Veneers
• Crowns

• http://www.nature.com/bdj/journal/v215/n9/fig_tab/sj.bdj.2013.1045_F1.html • Patel, M., et al. "Amelogenesis imperfecta-lifelong management. Restorative management of the
adult patient." British dental journal 215.9 (2013): 449-457. • http://www.optimumhealthinstitute.com/cosmetic-dentistry/what-are-dental-veneers/
Veneers

• “Research Evaluation of Lithium Disilicate Restorative System”MarkACruz. Web. • https://www.google.com/search?q=crowns+teeth&source=lnms&tbm=isch&sa=X&sqi=2&ved=0ahUKEwj1gMP4q-
HSAhWj24MKHXCaBbYQ_AUIBigB&biw=1275&bih=697#tbm=isch&q=anterior+porcelain+crowns+images&*&imgdii=q1Ys3snkGXtWFM:&imgrc=TkDwy0j_2VouLM:
Crowns

Oral Manifestations
1) Enamel Defects
2) Recurrent Aphthous Ulcers
3) Dry Mouth Syndrome
4) Delayed Eruption
5) Atrophic Glossitis
6) Oral Lichen Planus
7) Cheilosis

Aphthous Ulcers • Aphthous stomatitis/canker sores
• Painful ulcers located intra orally on the lips, cheek, tongue, palate, or base of gums
• Hard to speak and eat

• Mitchell, Jennifer. “Oral Manifestations of Celiac: Teeth Issues & More.” Colgate. Web. 28 Feb 2017. • Gilliam, Kathryn. “Treating Oral Ulcers.” RDH Mag. Web. 12 February 2017.
Aphthous Ulcers - Mechanism
• Immune mediated (T-cell mediated)
• Malabsorption:
– Vitamins B1, B2, B6, B12 and C
– Nutrients: low serum iron, folic acid, calcium, and selenium

Aphthous Ulcers - Epidemiology
• Canadian study: Prevalence of aphthous ulcers in subjects with biopsy confirmed celiac disease was 16% in children (<16 years) and 26% in adults
• According to the National Institutes of Health (NIH), between 3 and 61% of people with celiac disease have aphthous ulcers

• “Canker Sores-Treatment.” The American Academy of Oral Medicine 2007. Web. 20 February 2017 • Dombrowski, Margie M. “Celiac Teeth: Celiac Disease & Oral Health.” Colgate. Web. 28 February
2017
Aphthous Ulcers - Treatment • Avoid spicy, citric and
acidic foods. Instead consume simple, plain, bland flavored foods (yogurt)
• OTC: Occlusives, anesthetics, cleansing /antiseptic agents
• Prescription: anti-inflammatory or collagenase inhibiting agents

Oral Manifestations
1) Enamel Defects
2) Recurrent Aphthous Ulcers
3) Dry Mouth Syndrome
4) Delayed Eruption
5) Atrophic Glossitis
6) Oral Lichen Planus
7) Cheilosis

Dombrowski, Margie M. “Celiac Teeth: Celiac Disease & Oral Health.” Colgate. Web. 28 February 2017
Dry Mouth Syndrome - Background
• Mouth frequently dry due to insufficient saliva production
• Halitosis, difficult to speak, chew and swallow foods
• Dental concern: Saliva is key to a clean mouth, and hyposalivation leads to an increase in cavities

Trandafir, Laura Mihaela, et al. "Oral manifestations in celiac disease children." Romanian Journal of Oral Rehabilitation 6.1 (2014).
Dry Mouth Syndrome – Mechanism and Epidemiology
• Gluten exposure leads to salivary gland dysfunction resulting in an alteration in the composition of saliva: total protein, IgA, IgM, albumin, amylase, myeloperoxidase
• Lahteenoja et al observed that xerostomia was a consequence of diminished salivary flow
• In a study by Ertekin V et al, 58% of patients with celiac disease presented with xerostomia
• Sjogren’s syndrome is an autoimmune disorder that attacks salivary glands
• 4.5-15% of people with celiac have Sjogren’s Syndrome (according to Beyond Celiac)

Dombrowski, Margie M. “Celiac Teeth: Celiac Disease & Oral Health.” Colgate. Web. 28 February 2017
Dry Mouth Syndrome - Treatments
• Keep mouth hydrated with water or a humidifier at night
• Artificial saliva
• Prescription toothpaste: Gelkam or PreviDent 5000

Oral Manifestations
1) Enamel Defects
2) Recurrent Aphthous Ulcers
3) Dry Mouth Syndrome
4) Delayed Eruption
5) Atrophic Glossitis
6) Oral Lichen Planus
7) Cheilosis

Suri, Lokesh, Eleni Gagari, and Heleni Vastardis. "Delayed tooth eruption: pathogenesis, diagnosis, and treatment. A literature review." American Journal of Orthodontics and Dentofacial Orthopedics 126.4 (2004): 432-445.
Delayed Eruption
• Delayed eruption is a result of deficiency in essential nutrients
• Delay occurs due to inadequate supply of key nutrients during a time of high metabolic demand
• Treatment: Identify the disease as soon as possible and establish a gluten free diet

Oral Manifestations
1) Enamel Defects
2) Recurrent Aphthous Ulcers
3) Dry Mouth Syndrome
4) Delayed Eruption
5) Atrophic Glossitis
6) Oral Lichen Planus
7) Cheilosis

Erriu, Matteo et al. “Idiopathic Atrophic Glossitis as the Only Clinical Sign for Celiac Disease Diagnosis: A Case Report.” Journal of Medical Case Reports 6 (2012): 185. PMC. Web. 18 Mar. 2017.
Atrophic Glossitis - Background
• An inflammatory disorder of the tongue mucosa
• Smooth, glossy, fiery red or pink appearance
• Reamy, Brian V., Richard Derby, and Christopher W. Bunt. "Common tongue conditions in primary care." Am Fam Physician 81.5 (2010): 627-34. • Erriu, Matteo et al. “Idiopathic Atrophic Glossitis as the Only Clinical Sign for Celiac Disease Diagnosis: A Case Report.” Journal of Medical Case Reports 6
(2012): 185. PMC. Web. 18 Mar. 2017. • Images: https://en.wikipedia.org/wiki/Lingual_papillae
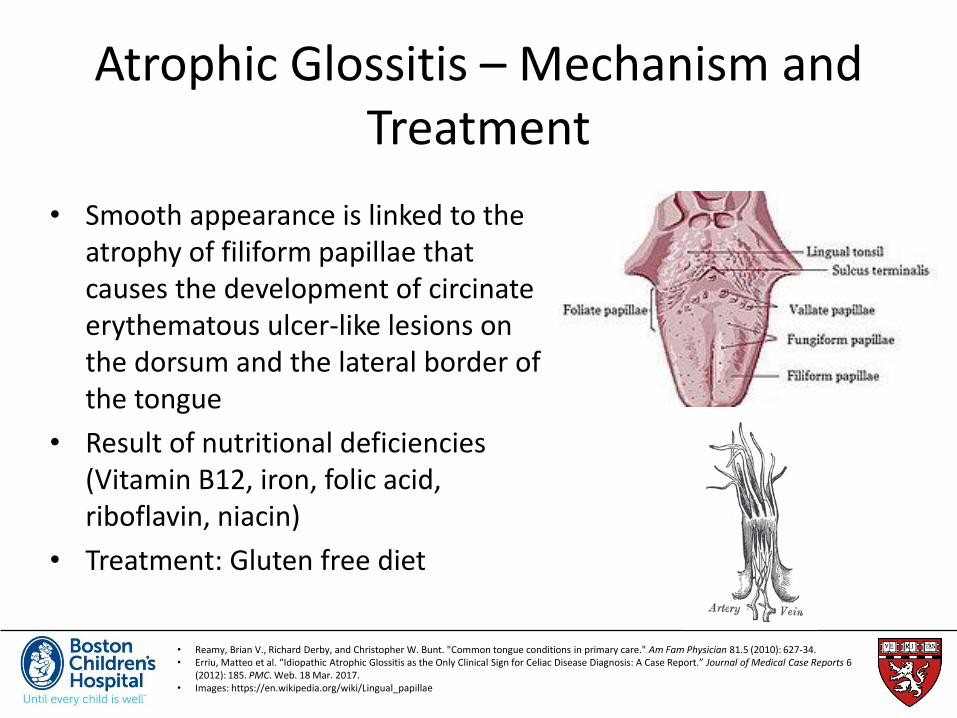
• Smooth appearance is linked to the atrophy of filiform papillae that causes the development of circinate erythematous ulcer-like lesions on the dorsum and the lateral border of the tongue
• Result of nutritional deficiencies (Vitamin B12, iron, folic acid, riboflavin, niacin)
• Treatment: Gluten free diet
Atrophic Glossitis – Mechanism and Treatment
Oral Manifestations
1) Enamel Defects
2) Recurrent Aphthous Ulcers
3) Dry Mouth Syndrome
4) Delayed Eruption
5) Atrophic Glossitis
6) Oral Lichen Planus
7) Cheilosis

Burkhart, N. “Oral Lichen Planus.” The American Academy of Oral Medicine 2013. Web. 20 February 2017
Oral Lichen Planus (OLP) - Background • Mucocutaneous disease that
affects skin and mucosa. • Two primary forms
1) Reticular form: lacy web-like, white threads that are slightly raised (Wikham’s Striae).
2) Erosive (atrophic) pattern: Layer of mucosa is lost. Bright red and uncomfortable
• Most commonly affects the cheek mucosa, tongue and gums

• Muggiano F, Quaranta A, Giannantoni I. Major dental clinical pathological manifestation of celiac disease. WebmedCentral Oral Medicine 2013;4(11):WMC004448
Oral Lichen Planus – Mechanism and Treatment
• Believed to be a reaction to an antigen (allergic reaction)
• OLP and celiac disease possibly share the same autoimmune etiopathogenetic mechanisms
• Autoimmune disorder where white blood cells are attacking epithelial cells
• Potentially a result of malabsorption and malnutrition in mucosal cells that are rapidly dividing
• Treatment: Gluten free diet

Oral Manifestations
1) Enamel Defects
2) Recurrent Aphthous Ulcers
3) Dry Mouth Syndrome
4) Delayed Eruption
5) Atrophic Glossitis
6) Oral Lichen Planus
7) Cheilosis

• Devani, Alim, and Benjamin Barankin. “Answer: Can You Identify This Condition?” Canadian Family Physician 53.6 (2007): 1022–1023.
• Ruessner, Harold T. "archive. is." Am Fam Physician 57.5 (1998): 1023-1034.
Cheilosis • Inflammatory reaction that
presents on either one or both angles of the mouth
• Appears as a painful ulcer
• Common causes: Lip sucking, drooling, bacterial and fungal infections, contact allergy, anemia
• Nutritional deficiencies: Vitamin B2,6,12, iron, ferritin, folate, riboflavin, niacin
• Treatment: repleting nutrients

Sewell, Josalyn. “The Staff of life or a chronic poison?” RDH. 18 Feb 2017
Role of a Dentist in Celiac Disease 1) Celiac disease should be on the differential when enamel defects and aphthous ulcers are detected
2) Ask about other clinical symptoms such as anemia, fatigue, abdominal pain, diarrhea and weight loss
3) Presence of other autoimmune diseases such as type I diabetes and thyroiditis should raise suspicion for celiac disease
4) Having a first or second degree relative with celiac disease increases likelihood of a diagnosis
5) If a dentist suspects celiac disease, laboratory testing should be coordinated with PCP
6) Most dental products are gluten free, but it is always best to confirm with certification or labeling

In summary • Oral cavity is the gateway to the gut
• Those with celiac disease may only present with oral and dental abnormalities
• Several oral manifestations are either a result of an autoimmune reaction or nutritional deficiencies
• Dentists and physicians should recognize these dental abnormalities and can play a significant role in screening for, and early detection of, celiac disease

References

Work Cited
• Burkhart, N. “Oral Lichen Planus.” The American Academy of Oral Medicine 2013. Web. 20 February 2017
• “Canker Sores-Treatment.” The American Academy of Oral Medicine 2007. Web. 20 February 2017
• Dental Growth and Development. American Academy of Pediatric Dentistry. 2011; 337 • Devani, Alim, and Benjamin Barankin. “Answer: Can You Identify This Condition?” Canadian
Family Physician 53.6 (2007): 1022–1023. • Dombrowski, Margie M. “Celiac Teeth: Celiac Disease & Oral Health.” Colgate. Web. 28 February
2017 • Erriu, Matteo et al. “Idiopathic Atrophic Glossitis as the Only Clinical Sign for Celiac Disease
Diagnosis: A Case Report.” Journal of Medical Case Reports 6 (2012): 185. PMC. Web. • Gilliam, Kathryn. “Treating Oral Ulcers.” RDH Mag. Web. 12 February 2017. • Patel, M., et al. "Amelogenesis imperfecta-lifelong management. Restorative management of the
adult patient." British dental journal 215.9 (2013): 449-457. • “What are Dental Venners” Optimum Health Institute. Web. 20 February 2017 • Sewell, Josalyn. “The Staff of life or a chronic poison?” RDH. 18 Feb 2017

Work Cited
• Rashid, Mohsin, et al. "Oral Manifestations of Celiac disease: A Clinical Guide for dentists." J Can Dent Assoc 77 (2011): b39.
• Schuppan D. Current concepts of celiac disease pathogenesis. Gastroenterology. 2000;119:234–242
• Trandafir, Laura Mihaela, et al. "Oral manifestations in celiac disease children." Romanian Journal of Oral Rehabilitation 6.1 (2014).
• Major dental clinical pathological manifestation of Celiac Disease. Dr. Andrea Quaranta et al. (2013)
• Mitchell, Jennifer. “Oral Manifestations of Celiac: Teeth Issues & More.” Colgate. Web. 28 Feb 2017.
• Muggiano F, Quaranta A, Giannantoni I. Major dental clinical pathological manifestation of celiac disease. WebmedCentral Oral Medicine 2013;4(11):WMC004448