Embed Size (px)
Citation preview

Oral Cavity and Oropharyngeal Cancer: A New Staging System for 2017
Masanari G. Kato, B.S., Terry A. Day, M.D.
Introduction Historically, squamous cell carcinomas of the oral cavity (OCSCC) and oropharynx (OPSCC) have been grouped together as similar diseases with the terms “oral” and “oropharyngeal” used synonymously. The use of these terms interchangeably has since become obsolete, as translational and clinical research has distinguished one from the other in many respects other than just anatomic site, such as by risk factors, patient demographics, etiopathogenesis, and management. These, among other emerging findings, have resulted in evidence that the 7th ed. (2010) American Joint Committee on Cancer (AJCC) staging system may not accurately reflect the differences in stage-related prognosis as a resource to guide treatment. Recently, the AJCC released the 8th ed. of the cancer staging manual, effective January 1st 2017. With this new staging system, notable modifications taken from the more recent published research have occurred and are expected to influence current management guidelines.
Background Anatomy The anatomic separation of the subsites and borders of the oral cavity and oropharynx are often confused, though important to the diagnosis and management of OCSCCs and OPSCCs. The former begins at the mucocutaneous junction of the lips and extends posteriorly, including the alveolar ridge and gums, the anterior two-thirds of the tongue, floor of the mouth, buccal mucosa, retromolar trigone, and hard palate (Figure 1). The oropharynx begins superiorly at the junction of the soft and hard palate, and inferiorly at the circumvallate papilla of the tongue. Subsites of the oropharynx include the soft palate, tonsillar pillars, tonsils, base (posterior 1/3) of the tongue, vallecula, and the pharyngeal walls, and is bounded superiorly by the lower surface of the soft palate and inferiorly by the epiglottis (Figure 1).

Figure 1. The anatomy of the oral cavity and the oropharynx (used with permission from artist, Lauren Visserman). Epidemiology Head and neck cancers (HNC) make up 3% of all cancers in the United States, with a favorable, downward trend in its overall occurrence.1,2 The rates of OCSCCs has paralleled this pattern while OPSCC incidence has been accelerating (Figures 2A, 2B).1 This observation is due to the surge in human papilloma virus (HPV) associated OPSCCs, approaching 60-80% of all OPSCCs, a subset now often referred to as an “epidemic” in the head and neck community.3,4 Of note, the incidence of “tongue” cancer is inferred to account for both the oral tongue and base of tongue by both the Surveillance, Epidemiology, and End Results (SEER) database and American Cancer Society, and its rise due to increasing rates of the latter, which is a distinct subsite of the oropharynx (Figure 2A). Thus, Figure 2A shows rising “tongue” cancer, which appears to be primarily a result of the increase in base of tongue as can be appreciated in Figure 2B. Researchers are optimistic that future national databases will separate tongue into
the “oral” part of the tongue and separate the “base of tongue” into the oropharynx. Between OCSCC and OPSCC, the American Cancer Society estimates nearly 50,000 new cases will develop, leading to almost 10,000 deaths in the US for 2016 alone.2

Figure 2. Age-adjusted SEER incidence rates by subsite in the U.S., all races, both sexes from 1975-2013. A. OCSCC declining overall.1 Of note, the incidence of tongue cancer is inferred to account for the oral tongue and base of tongue, and its rise due to increasing rates of the latter, a distinct subsite of the oropharynx B. Rates of OPSCC rising rapidly.1 Patient Demographics and Clinical Characteristics It is interesting that HPV-positivity in the oropharynx patients represent a unique entity, as the HPV- OPSCC and all OCSCC patients appear to be similar in demographics. This distinction along with other clinical characteristics of each is summarized below (Table 1). Table 1. Common Demographics and Clinical Characteristics of OCSCCs and OPSCCs
Cancer Site Oral Cavity Oropharynx
HPV(-) HPV(+)
Demographics5
Smoker/drinker
Older
More African-Americans
Lower SES
Lower education
Smoker/drinker
Older
More African-Americans
Lower SES
Lower education
Nonsmoker
Male
Younger
Caucasian
Multiple partners
Higher SES
Higher education
Common Locations
6
Oral Tongue Pharyngeal wall
Soft Palate
Tonsil
Base of tongue
Common Presentations
6
Soreness with red or white spots
Sore throat
Dysphagia
Otalgia
Painless neck mass
Diagnosis The initial workup of these patients involves a physical exam, visualizing the primary tumor by fiberoptic endoscopy in the outpatient clinic, and sampling the primary tumor with a tissue biopsy or neck mass with fine needle aspiration to confirm the disease. Currently, testing for HPV status is routine for oropharyngeal lesions. Immunostaining for p16 protein is the most popular method. Following diagnosis, imaging modalities such as

MRI, CT, and CT-PET are often utilized to determine the extent of disease, namely, nodal involvement and the presence of distant metastasis. The authors feel that contrasted CT combined with the CT-PET fusion is a useful and beneficial imaging study that provides information on primary tumor proximity to the lingual neurovascular bundle, the carotid and jugular vascular structures, along with mandible and pterygoid muscles, which aids in accurate staging (Figure 3A).
Additionally, contrasted imaging reveals lymph nodes that may be suspicious for harboring regional metastasis even when they are normal by size criteria (Figure 3B). As noted earlier, HPV+ OPSCC commonly involves the base of tongue (Figure 4A) and advanced nodal disease is more likely present, typically appearing large and cystic (Figure 4B).
Figure 3. Imaging of Advanced OCSCC. A. CT-PET showing uptake of primary gingival SCC involving the mandible (green arrow) with nodal metastasis (yellow arrows) B. Contrast CT showing a lymph node less than 1cm in size (red arrow) with metastatic OCSCC.
Formatted: Font: Bold
Formatted: Font: Bold
Formatted: Tab stops: 2.18", Left

Figure 4. Imaging of Advanced OPSCC. A. CT-PET showing uptake of primary base of tongue SCC with nodal metastasis (yellow arrows) B. Contrast CT showing a cystic lymph node (red arrow) with metastatic OCSCC. Add Green arrow to base of tongue in A Staging The clinical assessments outlined above then translate to the clinical stage of the cancer. Like most cancers, OCSCCs and OPSCCs are staged by the TNM (tumor, node, metastasis) staging system, a classification established by the AJCC to categorize cancer patients based on prognostic differences. The resulting alphanumeric code (T0-4,
N0-3, M0-1) then corresponds to stage grouping (I to IV). EMERGING CONCEPTS
Since the implementation of the previous AJCC staging system (7th ed., 2010), treatment standards, patient demographics, and cancer knowledge have evolved. A number of these findings relate to improving the accuracy of the staging system, while others shed light on future strategies to undertake the HPV+ OPSCC epidemic. Changes in staging have resulted from studies revealing predictive prognostic indicators that impact treatment, locoregional control, and survival. Oral Cavity Cancer Findings related to OCSCCs vary,7-11 though notably, the depth of invasion (DOI) of the primary tumor was found to be an independent prognostic measure for both nodal metastasis and survival in OCSCCs.12-14 The DOI is measured histologically by utilizing the basement membrane of normal adjacent tissue as reference. Incorporating the DOI by increments of 5mms help to categorize patients by survival more effectively compared to the 7th ed. staging system.12,13
Formatted: Font: (Default) Arial, 11 pt
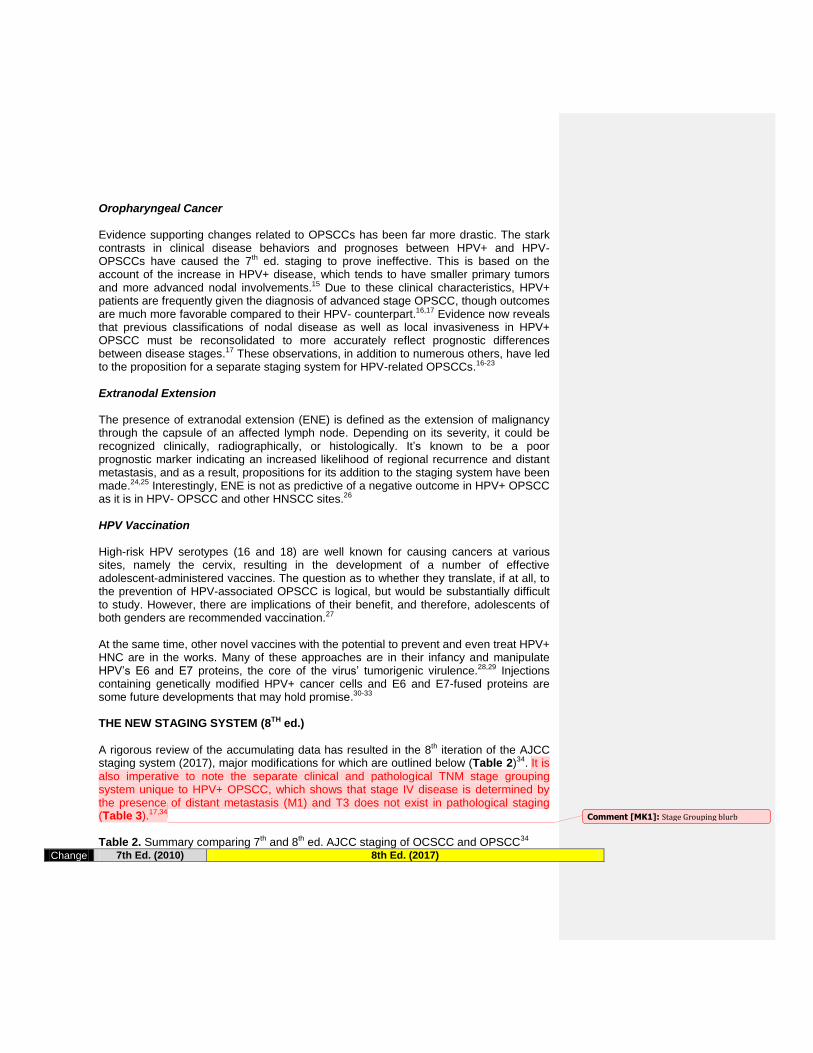
Oropharyngeal Cancer Evidence supporting changes related to OPSCCs has been far more drastic. The stark contrasts in clinical disease behaviors and prognoses between HPV+ and HPV- OPSCCs have caused the 7th ed. staging to prove ineffective. This is based on the account of the increase in HPV+ disease, which tends to have smaller primary tumors and more advanced nodal involvements.15 Due to these clinical characteristics, HPV+ patients are frequently given the diagnosis of advanced stage OPSCC, though outcomes are much more favorable compared to their HPV- counterpart.16,17 Evidence now reveals that previous classifications of nodal disease as well as local invasiveness in HPV+ OPSCC must be reconsolidated to more accurately reflect prognostic differences between disease stages.17 These observations, in addition to numerous others, have led to the proposition for a separate staging system for HPV-related OPSCCs.16-23 Extranodal Extension The presence of extranodal extension (ENE) is defined as the extension of malignancy through the capsule of an affected lymph node. Depending on its severity, it could be recognized clinically, radiographically, or histologically. It’s known to be a poor prognostic marker indicating an increased likelihood of regional recurrence and distant metastasis, and as a result, propositions for its addition to the staging system have been made.24,25 Interestingly, ENE is not as predictive of a negative outcome in HPV+ OPSCC as it is in HPV- OPSCC and other HNSCC sites.26 HPV Vaccination High-risk HPV serotypes (16 and 18) are well known for causing cancers at various sites, namely the cervix, resulting in the development of a number of effective adolescent-administered vaccines. The question as to whether they translate, if at all, to the prevention of HPV-associated OPSCC is logical, but would be substantially difficult to study. However, there are implications of their benefit, and therefore, adolescents of both genders are recommended vaccination.27 At the same time, other novel vaccines with the potential to prevent and even treat HPV+ HNC are in the works. Many of these approaches are in their infancy and manipulate HPV’s E6 and E7 proteins, the core of the virus’ tumorigenic virulence.28,29 Injections containing genetically modified HPV+ cancer cells and E6 and E7-fused proteins are some future developments that may hold promise.30-33 THE NEW STAGING SYSTEM (8TH ed.)
A rigorous review of the accumulating data has resulted in the 8th iteration of the AJCC staging system (2017), major modifications for which are outlined below (Table 2)34. It is also imperative to note the separate clinical and pathological TNM stage grouping system unique to HPV+ OPSCC, which shows that stage IV disease is determined by the presence of distant metastasis (M1) and T3 does not exist in pathological staging (Table 3).17,34 Table 2. Summary comparing 7th and 8th ed. AJCC staging of OCSCC and OPSCC34
Change 7th Ed. (2010) 8th Ed. (2017)
Comment [MK1]: Stage Grouping blurb

Oral Cavity HPV- Oropharynx HPV+ Oropharynx
T-s
tage
T0: no primary
T1: size ≤2cm T2: size 2-4cm T3: size >4cm
T4: o T4a: moderately
advanced (extrinsic tongue muscle involvement constituted T4a)
o T4b: very
advanced
T0 deleted
T1: size <2cm and DOI <5mm
T2: size <2cm and DOI 5-10mm or size 2-4cm and DOI <10mm
T3: size >4cm or >10mm DOI
T4a extrinsic tongue muscle
infiltration now deleted
T0 deleted
T0 if proven p16+ disease without evidence of primary tumor
All locally advanced combined to T4
N-s
tage
N0: no LN involved
N1: single ipsi LN
≤3cm in size N2: o N2a: single ipsi LN,
3-6cm in size o N2b: multiple ipsi
LNs, all ≤6cm in size
o N2c: any bi or ctr
LNs, all ≤6cm in size
N3: any LN >6cm in size
Clinical N-stage
N1-N2 is same as previous and ENE(-)
N3 now with subcategories:
o N3a is previous N3 (size >6cm) and ENE(-)
o N3b is any ENE(+), either clinical or radiographic
Previous N1, N2a combined to N1 (<6cm with or without ENE)
Previous N2b, N2c combined to N2
Pathological N-stage
Microscopically evident ENE(+) LNs results in upstaging
N1: <4 LNs involved
N2: >4 LNs involved
N3 deleted
Sta
ge
gro
upin
g
Clinical or pathological TNM
used for same grouping system
Same as previous
Separate clinical and pathological TNM
groupings
DOI – depth of invasion, LN – lymph node, ENE(+) – extranodal extension present, ENE(-) extranodal extension absent, ipsi – ipsilateral, bi – bilateral, ctr - contralateral Table 3. Changes in Stage Grouping for HPV+ OPSCC34
7th ed. TNM Grouping 8
th ed. cTNM Grouping 8
th ed. pTNM Grouping
N0 N1 N2 N3
N0 N1 N2 N3 N0 N1 N2
T1 I III IVA IVB T0 I I II III T0 I I II
T2 II III IVA IVB T1 I I II III T1 I I II
T3 III III IVA IVB T2 I I II III T2 I I II
T4a IVA IVA IVA IVB T3 II II II III T3 II II III
T4b IVB IVB IVB IVB T4 III III III III T4 II II III
M1 IVC IVC IVC IVC M1 IV IV IV IV M1 IV IV IV
Comment [MK2]: Stage grouping table – necessary?

CHANGES IN MANAGEMENT
Current therapies for OCSCCs and OPSCCs include isolated or various combinations of surgery, radiation therapy, chemotherapy, and immunotherapy. In general, all oral cavity cancer is treated with surgery unless metastatic, unresectable, or there are constraindications to surgery. However, oropharyngeal cancer can be treated with surgery(TORS) or radiation therapy alone for early stage(I or II) while combined therapy using Surgery + Radiation Therapy(SRT) or Chemoradiation(CRT) is the standard for advanced stage(III or IV). (Ref NCCN, etc) The management has historically been stage-dependent, with therapies increasing in intensity with higher stage. However, recent evidence suggests the need to individually tailor treatment practices as overtreatment has been a topic of concern, particularly for early-stage OCSCCs and OPSCCs.17,35 Consequently, prospective studies are currently underway to minimize morbidities and de-intensifying treatment in patients undergoing aggressive multimodal regimens.22 SUMMARY OCSCC and OPSCC are clinically and pathologically distinct diseases. While the overall decrease in incidence of all HNCs is favorable, the rise in HPV+ OPSCCs has become an important issue in the diagnosis, prevention, and treatment of these cancers. This evolving landscape in the modern era has culminated in the release of the 8th ed. of the AJCC staging system, which incorporates critical parameters to improve prognostic categorization. Highlights include the incorporation of depth of invasion in oral tongue cancers, separation of OPSCC staging by HPV status, and inclusion of extranodal extension in nodal staging. By more accurately reflecting the differences in patient prognoses, cancer management is sure to adapt with time. Furthermore, translational research is showing potential in the realm of HPV prevention, diagnostics, and unique therapeutics, adding to the collective efforts to tackle this epidemic. REFERENCES
1. Surveillance, Epidemiology, and End Results (SEER) Program (http://www.seer.cancer.gov) SEER*Stat Database: Populations - Total U.S. (1969-2014).
2. American Cancer Society. Cancer Facts & Figures 2016, 2016. 3. Polednak AP. Using Data on Tumor Grade in Cancer Registries to Enhance
Surveillance of Oropharyngeal Cancers in Relation to the Human Papillomavirus Epidemic. Journal of registry management 2016; 43:29-35.
4. Mehanna H, Beech T, Nicholson T, et al. Prevalence of human papillomavirus in oropharyngeal and nonoropharyngeal head and neck cancer--systematic review and meta-analysis of trends by time and region. Head Neck 2013; 35:747-755.
5. Gillison ML, D'Souza G, Westra W, et al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst 2008; 100:407-420.
6. McIlwain WR, Sood AJ, Nguyen SA, Day TA. Initial symptoms in patients with HPV-positive and HPV-negative oropharyngeal cancer. JAMA Otolaryngol Head Neck Surg 2014; 140:441-447.
Comment [MK3]: Fix all formatting

7. Patel SG, Amit M, Yen TC, et al. Lymph node density in oral cavity cancer: results of the International Consortium for Outcomes Research. Br J Cancer 2013; 109:2087-2095.
8. Ebrahimi A, Gil Z, Amit M, et al. The prognosis of N2b and N2c lymph node disease in oral squamous cell carcinoma is determined by the number of metastatic lymph nodes rather than laterality: evidence to support a revision of the American Joint Committee on Cancer staging system. Cancer 2014; 120:1968-1974.
9. Ebrahimi A, Gil Z, Amit M, et al. Comparison of the American Joint Committee on Cancer N1 versus N2a nodal categories for predicting survival and recurrence in patients with oral cancer: Time to acknowledge an arbitrary distinction and modify the system. Head Neck 2016; 38:135-139.
10. Boland PW, Pataridis K, Eley KA, Golding SJ, Watt-Smith SR. A detailed anatomical assessment of the lateral tongue extrinsic musculature, and proximity to the tongue mucosal surface. Does this confirm the current TNM T4a muscular subclassification? Surg Radiol Anat 2013; 35:559-564.
11. Kuk SK, Yoon HJ, Hong SD, Hong SP, Lee JI. Staging significance of bone invasion in small-sized (4cm or less) oral squamous cell carcinoma as defined by the American Joint Committee on Cancer. Oral Oncol 2016; 55:31-36.
12. Ebrahimi A, Gil Z, Amit M, et al. Primary tumor staging for oral cancer and a proposed modification incorporating depth of invasion: an international multicenter retrospective study. JAMA Otolaryngol Head Neck Surg 2014; 140:1138-1148.
13. Hubert Low TH, Gao K, Elliott M, Clark JR. Tumor classification for early oral cancer: re-evaluate the current TNM classification. Head Neck 2015; 37:223-228.
14. Kane SV, Gupta M, Kakade AC, A DC. Depth of invasion is the most significant histological predictor of subclinical cervical lymph node metastasis in early squamous carcinomas of the oral cavity. Eur J Surg Oncol 2006; 32:795-803.
15. Marur S, D'Souza G, Westra WH, Forastiere AA. HPV-associated head and neck cancer: a virus-related cancer epidemic. Lancet Oncol 2010; 11:781-789.
16. Huang SH, Xu W, Waldron J, et al. Refining American Joint Committee on Cancer/Union for International Cancer Control TNM stage and prognostic groups for human papillomavirus-related oropharyngeal carcinomas. J Clin Oncol 2015; 33:836-845.
17. O'Sullivan B, Huang SH, Su J, et al. Development and validation of a staging system for HPV-related oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICON-S): a multicentre cohort study. Lancet Oncol 2016; 17:440-451.
18. Rios Velazquez E, Hoebers F, Aerts HJ, et al. Externally validated HPV-based prognostic nomogram for oropharyngeal carcinoma patients yields more accurate predictions than TNM staging. Radiother Oncol 2014; 113:324-330.
19. Beitler JJ, LeCraw Mikell J, Switchenko J. Human Papillomavirus-Related Oropharyngeal Cancer: Agree With a New Staging System, but the Devil Is in the Details. J Clin Oncol 2015; 33:3217-3218.

20. Keane FK, Chen YH, Neville BA, et al. Changing prognostic significance of tumor stage and nodal stage in patients with squamous cell carcinoma of the oropharynx in the human papillomavirus era. Cancer 2015; 121:2594-2602.
21. Dahlstrom KR, Garden AS, William WN, Jr., Lim MY, Sturgis EM. Proposed Staging System for Patients With HPV-Related Oropharyngeal Cancer Based on Nasopharyngeal Cancer N Categories. J Clin Oncol 2016; 34:1848-1854.
22. Horne ZD, Glaser SM, Vargo JA, et al. Confirmation of proposed human papillomavirus risk-adapted staging according to AJCC/UICC TNM criteria for positive oropharyngeal carcinomas. Cancer 2016; 122:2021-2030.
23. Keane FK, Chen YH, Tishler RB, et al. Population-based validation of the recursive partitioning analysis-based staging system for oropharyngeal cancer. Head Neck 2016.
24. Wreesmann VB, Katabi N, Palmer FL, et al. Influence of extracapsular nodal spread extent on prognosis of oral squamous cell carcinoma. Head Neck 2016; 38 Suppl 1:E1192-1199.
25. Wenzel S, Sagowski C, Kehrl W, Metternich FU. The prognostic impact of metastatic pattern of lymph nodes in patients with oral and oropharyngeal squamous cell carcinomas. Eur Arch Otorhinolaryngol 2004; 261:270-275.
26. Sinha P, Lewis JS, Jr., Piccirillo JF, Kallogjeri D, Haughey BH. Extracapsular spread and adjuvant therapy in human papillomavirus-related, p16-positive oropharyngeal carcinoma. Cancer 2012; 118:3519-3530.
27. Lowy DR, Herrero R, Hildesheim A. Primary endpoints for future prophylactic human papillomavirus vaccine trials: towards infection and immunobridging. Lancet Oncol 2015; 16:e226-233.
28. Dyson N, Howley PM, Munger K, Harlow E. The human papilloma virus-16 E7 oncoprotein is able to bind to the retinoblastoma gene product. Science 1989; 243:934-937.
29. Scheffner M, Werness BA, Huibregtse JM, Levine AJ, Howley PM. The E6 oncoprotein encoded by human papillomavirus types 16 and 18 promotes the degradation of p53. Cell 1990; 63:1129-1136.
30. Mikyskova R, Indrova M, Simova J, Bieblova J, Bubenik J, Reinis M. Genetically modified tumour vaccines producing IL-12 augment chemotherapy of HPV16-associated tumours with gemcitabine. Oncol Rep 2011; 25:1683-1689.
31. Mansilla C, Berraondo P, Durantez M, et al. Eradication of large tumors expressing human papillomavirus E7 protein by therapeutic vaccination with E7 fused to the extra domain a from fibronectin. Int J Cancer 2012; 131:641-651.
32. Venuti A, Curzio G, Mariani L, Paolini F. Immunotherapy of HPV-associated cancer: DNA/plant-derived vaccines and new orthotopic mouse models. Cancer Immunol Immunother 2015; 64:1329-1338.
33. Yin W, Duluc D, Joo Het al. Therapeutic HPV Cancer Vaccine Targeted to CD40 Elicits Effective CD8+ T-cell Immunity. Cancer Immunol Res 2016; 4:823-834.
34. AJCC Cancer Staging Manual. In: Amin MB, Edge S, Greene FL, Byrd DR, Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR, Sullivan DC, Jessup JM, Brierley JD, Gaspar LE, Schilsky RL, Balch CM, Winchester DP, Asare EA, Madera M, Gress DM, Meyer LR, eds.: Springer International Publishing, 2017.
35. Cracchiolo JR, Baxi SS, Morris LG, et al. Increase in primary surgical treatment of T1 and T2 oropharyngeal squamous cell carcinoma and rates of

adverse pathologic features: National Cancer Data Base. Cancer 2016; 122:1523-1532.
1. Surveillance, Epidemiology, and End Results (SEER) Program (www.seer.cancer.gov) SEER*Stat Database: Populations - Total U.S. (1969-2014).
2. American Cancer Society. Cancer Facts & Figures 2016, 2016. 3. Polednak AP. Using Data on Tumor Grade in Cancer Registries to Enhance
Surveillance of Oropharyngeal Cancers in Relation to the Human Papillomavirus Epidemic. Journal of registry management 2016; 43:29-35.
4. Mehanna H, Beech T, Nicholson Tet al. Prevalence of human papillomavirus in oropharyngeal and nonoropharyngeal head and neck cancer--systematic review and meta-analysis of trends by time and region. Head Neck 2013; 35:747-755.
5. Gillison ML, D'Souza G, Westra Wet al. Distinct risk factor profiles for human papillomavirus type 16-positive and human papillomavirus type 16-negative head and neck cancers. J Natl Cancer Inst 2008; 100:407-420.
6. McIlwain WR, Sood AJ, Nguyen SA, Day TA. Initial symptoms in patients with HPV-positive and HPV-negative oropharyngeal cancer. JAMA Otolaryngol Head Neck Surg 2014; 140:441-447.
7. Patel SG, Amit M, Yen TCet al. Lymph node density in oral cavity cancer: results of the International Consortium for Outcomes Research. Br J Cancer 2013; 109:2087-2095.
8. Ebrahimi A, Gil Z, Amit Met al. The prognosis of N2b and N2c lymph node disease in oral squamous cell carcinoma is determined by the number of metastatic lymph nodes rather than laterality: evidence to support a revision of the American Joint Committee on Cancer staging system. Cancer 2014; 120:1968-1974.
9. Ebrahimi A, Gil Z, Amit Met al. Comparison of the American Joint Committee on Cancer N1 versus N2a nodal categories for predicting survival and recurrence in patients with oral cancer: Time to acknowledge an arbitrary distinction and modify the system. Head Neck 2016; 38:135-139.
10. Boland PW, Pataridis K, Eley KA, Golding SJ, Watt-Smith SR. A detailed anatomical assessment of the lateral tongue extrinsic musculature, and proximity to the tongue mucosal surface. Does this confirm the current TNM T4a muscular subclassification? Surg Radiol Anat 2013; 35:559-564.
11. Kuk SK, Yoon HJ, Hong SD, Hong SP, Lee JI. Staging significance of bone invasion in small-sized (4cm or less) oral squamous cell carcinoma as defined by the American Joint Committee on Cancer. Oral Oncol 2016; 55:31-36.
12. Ebrahimi A, Gil Z, Amit Met al. Primary tumor staging for oral cancer and a proposed modification incorporating depth of invasion: an international multicenter retrospective study. JAMA Otolaryngol Head Neck Surg 2014; 140:1138-1148.
13. Hubert Low TH, Gao K, Elliott M, Clark JR. Tumor classification for early oral cancer: re-evaluate the current TNM classification. Head Neck 2015; 37:223-228.
14. Kane SV, Gupta M, Kakade AC, A DC. Depth of invasion is the most significant histological predictor of subclinical cervical lymph node metastasis in early squamous carcinomas of the oral cavity. Eur J Surg Oncol 2006; 32:795-803.
15. Marur S, D'Souza G, Westra WH, Forastiere AA. HPV-associated head and neck cancer: a virus-related cancer epidemic. Lancet Oncol 2010; 11:781-789.
16. Huang SH, Xu W, Waldron Jet al. Refining American Joint Committee on Cancer/Union for International Cancer Control TNM stage and prognostic groups for human papillomavirus-related oropharyngeal carcinomas. J Clin Oncol 2015; 33:836-845.
17. O'Sullivan B, Huang SH, Su Jet al. Development and validation of a staging system for HPV-related oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICON-S): a multicentre cohort study. Lancet Oncol 2016; 17:440-451.
18. Rios Velazquez E, Hoebers F, Aerts HJet al. Externally validated HPV-based prognostic nomogram for oropharyngeal carcinoma patients yields more accurate predictions than TNM staging. Radiother Oncol 2014; 113:324-330.
19. Beitler JJ, LeCraw Mikell J, Switchenko J. Human Papillomavirus-Related Oropharyngeal Cancer: Agree With a New Staging System, but the Devil Is in the Details. J Clin Oncol 2015; 33:3217-3218.
20. Keane FK, Chen YH, Neville BAet al. Changing prognostic significance of tumor stage and nodal stage in patients with squamous cell carcinoma of the oropharynx in the human papillomavirus era. Cancer 2015; 121:2594-2602.
21. Dahlstrom KR, Garden AS, William WN, Jr., Lim MY, Sturgis EM. Proposed Staging System for Patients With HPV-Related Oropharyngeal Cancer Based on Nasopharyngeal Cancer N Categories. J Clin Oncol 2016; 34:1848-1854.
22. Horne ZD, Glaser SM, Vargo JAet al. Confirmation of proposed human papillomavirus risk-adapted staging according to AJCC/UICC TNM criteria for positive oropharyngeal carcinomas. Cancer 2016; 122:2021-2030.
23. Keane FK, Chen YH, Tishler RBet al. Population-based validation of the recursive partitioning analysis-based staging system for oropharyngeal cancer. Head Neck 2016.
24. Wreesmann VB, Katabi N, Palmer FLet al. Influence of extracapsular nodal spread extent on prognosis of oral squamous cell carcinoma. Head Neck 2016; 38 Suppl 1:E1192-1199.
25. Wenzel S, Sagowski C, Kehrl W, Metternich FU. The prognostic impact of metastatic pattern of lymph nodes in patients with oral and oropharyngeal squamous cell carcinomas. Eur Arch Otorhinolaryngol 2004; 261:270-275.
26. Sinha P, Lewis JS, Jr., Piccirillo JF, Kallogjeri D, Haughey BH. Extracapsular spread and adjuvant therapy in human papillomavirus-related, p16-positive oropharyngeal carcinoma. Cancer 2012; 118:3519-3530.

27. Lowy DR, Herrero R, Hildesheim A. Primary endpoints for future prophylactic human papillomavirus vaccine trials: towards infection and immunobridging. Lancet Oncol 2015; 16:e226-233.
28. Dyson N, Howley PM, Munger K, Harlow E. The human papilloma virus-16 E7 oncoprotein is able to bind to the retinoblastoma gene product. Science 1989; 243:934-937.
29. Scheffner M, Werness BA, Huibregtse JM, Levine AJ, Howley PM. The E6 oncoprotein encoded by human papillomavirus types 16 and 18 promotes the degradation of p53. Cell 1990; 63:1129-1136.
30. Mikyskova R, Indrova M, Simova J, Bieblova J, Bubenik J, Reinis M. Genetically modified tumour vaccines producing IL-12 augment chemotherapy of HPV16-associated tumours with gemcitabine. Oncol Rep 2011; 25:1683-1689.
31. Mansilla C, Berraondo P, Durantez Met al. Eradication of large tumors expressing human papillomavirus E7 protein by therapeutic vaccination with E7 fused to the extra domain a from fibronectin. Int J Cancer 2012; 131:641-651.
32. Venuti A, Curzio G, Mariani L, Paolini F. Immunotherapy of HPV-associated cancer: DNA/plant-derived vaccines and new orthotopic mouse models. Cancer Immunol Immunother 2015; 64:1329-1338.
33. Yin W, Duluc D, Joo Het al. Therapeutic HPV Cancer Vaccine Targeted to CD40 Elicits Effective CD8+ T-cell Immunity. Cancer Immunol Res 2016; 4:823-834.
34. AJCC Cancer Staging Manual. In: Amin MB, Edge S, Greene FL, Byrd DR,
Brookland RK, Washington MK, Gershenwald JE, Compton CC, Hess KR,
Sullivan DC, Jessup JM, Brierley JD, Gaspar LE, Schilsky RL, Balch CM,
Winchester DP, Asare EA, Madera M, Gress DM, Meyer LR, eds.: Springer International Publishing, 2017.
35. Cracchiolo JR, Baxi SS, Morris LGet al. Increase in primary surgical treatment of T1 and T2 oropharyngeal squamous cell carcinoma and rates of adverse pathologic features: National Cancer Data Base. Cancer 2016; 122:1523-1532.