Embed Size (px)
Citation preview

DRUG THERAPY Drugs & Aging 1996 Dec; 9 (6): 418-437 11 70-229X/96/0012-0418/SIO.00/0
© AdlS Inte rno tionoll1mlfe d . All rightS reseN 9 d .
Oral Antidiabetic Drug Use in the Elderly Rubin Bressler and David G. Johnson
Departments of Medicine and Pharmacology, University of Arizona Health Sciences Center, Tucson, Arizona, USA
Contents Summary 1. Sulphonylureas
1 .1 Efficacy . 1.2 Tolerability 1.3 Drug Interactions
2. Combination Drug Therapy . 3. Metformin ..
3.1 Efficacy 3.2 Toxicity
4. Troglitazone 5. Acarbose . 6. Conclusion
418 420 423 424 425 425 426 427 428 428 429 430
Summary Non-insulin-dependent diabetes mellitus (NIDDM) is a metabolic disease that is common in the elderly, and is characterised by insulin insufficiency and resistance. Measures such as bodyweight reduction and exercise improve the metabolic defects, but pharmacological therapy is the most frequently used and successful therapy. The sulphonylureas stimulate insulin secretion. Metformin and troglitazone increase glucose disposal and decrease hepatic glucose output without causing hypoglycaemia. Acarbose is a dietary aid that spreads the dietary carbohydrate challenge to endogenous insulin over time. These pharmacological agents, either alone or in combination, should improve blood glucose regulation in patients with NIDDM.
It has been well established that the incidence of non-insulin-dependent diabetes mellitus (NIDDM) and impaired glucose tolerance (IGT) increase with aging.[1 -9] NIDDM is a common disorder
characterised by defects in both insulin secretion and insulin action,[I ,IO-13] and typically occurs in
overweight patients aged 2:40 years. Both genetic and environmental factors playa
role in the pathogenesis of NIDDM, and it is not certain whether impairment of tissue sensitivity to
insulin (insulin resistance), impairment of insulin
response to glucose (insulin secretory defect) or both represent the initiating genetic abnormality in NIDDM.[I,8,11 ,12,14-26]
Studies have been carried out to ascertain the metabolic defect or defects in individuals genetically predisposed to NIDDM, Several such investigations have shown that decreased glucose-induced insulin output is a predictor of NIDDM.!II-1 3,27-30]
The exact basis of insulin resistance is not

Oral Antidiabetics in the Elderly
known, but can be contributed to by a decreased level of physical activity and increased body fat. [5,S,9,27,3 1-34] Moreover, many drugs used by eld-
erly patients may contribute to glucose intolerance. These include thiazide diuretics, glucocorticoids, adrenergic blocking agents, nicotinic acid and phenytoin. [5,35]
Whereas a deficient insulin output and insulin resistance in response to a glucose challenge are characteristic of and predictive of NIDDM, the biochemical sequence of changes involved in the transition of these metabolic abnormalities to overt disease is still unknown.[11.12,21] However, insulin
resistance increases as a function of aging, obesity, decreased physical activity and probably other unknown factors. Increased insulin resistance results in deterioration of glucose tolerance.
The increased blood glucose levels caused by both insulin resistance and a delay in the early phase of insulin secretion eventually stimulates increased insulin secretion, which limits the increased blood glucose levels. In time, the insulin secretory response declines and blood glucose
levels rise because of augmented gluconeogenesis and insulin insufficiency. [1 .8,11, I 5, 16,36-39J Hyper-
glycaemia itself is a causal factor in the decreased insulin output, and in insulin resistance.lS,40,41]
Diabetes mellitus can be viewed as an abnormal metabolic state characterised by glucose overproduction and underutilisation.ll.S, 10,12,30,36-39] These
abnormalities are the result of insufficient insulin secretion in response to glucose, and tissue insensitivity to the actions of insulin.[I,S,30,39]
Controlled studies of the effects of blood glucose regulation on the complications of NIDDM have not been carried out. The major causes of death and disability in elderly patients with NIDDM are atherosclerotic and arteriosclerotic vascular diseases .[42-45] In patients with NIDDM, coronary
artery disease is the leading cause of death regardless of the duration of the disease, gender or ethnic/racial origins.l42-44] There is a higher incidence of all clinical varieties of macrovascular disease, including peripheral and cerebral vascular
© Adis International Umited. All rights reserved.
419
disease, in patients with NIDDM compared with the general population.l42-44]
Poorly controlled blood glucose levels in NIDDM result in a dyslipidaemia, which constitutes an additional coronary artery disease risk factorJ44-46] The dyslipidaemia consists of low levels of high density lipoprotein (HDL)-cholesterol, elevated levels of low density lipoprotein (LDL)cholesterol and very low density lipoprotein (VLDL)cholesterol, and increased levels of apolipoproteins Band E.l45-47] These abnormalities are ameliorated by improved blood glucose controJ.l45,4S-50]
This discussion of the treatment of NIDDM in the elderly focuses on agents that increase in'sulin secretion, drugs that increase insulin sensitivity, and an agent that helps the dietary control of blood glucose.
1. Sulphonylureas
Patients with NIDDM have been shown to have defects in both target-tissue sensitivity to insulin and to glucose-induced insulin outputJI ,S,II,12,19,21 ,22]
The goal of drug therapy is to ameliorate or correct both of these abnormalities in the elderly patient with NIDDM.
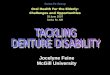
The sulphonylureas have been the primary drug therapy of NIDDM for 4 decades. The sulphonylureas that were available at the time of this review are shown in figure 1. The chemical differences between the drugs are responsible for their differing pharmacokinetic profiles, which are shown in table P51]
Recently, glimepiride, a long-acting sulphonylurea available outside the US, was approved for use in the US. [53] This agent is similar to glipizide and glibenclamide (glyburide) in terms of its potency and duration of action, and is efficacious at daily dosages of I to 6mg, although lower dosages are recommended in the elderly and in those with renal or hepatic disease. The agent is metabolised by the liver and its principle metabolite accounts for 30% of the activity of glimepiride. Maximal activity occurs 2 to 3 hours after administration, and efficacy persists for 24 hoursJ53,54] Glimepiride is an effective drug that appears to offer no
Drugs & Aging 1996 Dec; 9 (6)

420
proven advantage over currently available drugs for the treatment of NIDDM.l53,54]
The sulphonylureas stimulate insulin secretion by the pancreatic ~-cells, thereby correcting one of the 2 deficits present in NIODM. The mechanism of action is the same for all the sulphonylureas, although the potency of the second-generation drugs is greater (table 1).151 .58] The stimulatory effect of sulphonylureas has been demonstrated both in vitro and in vivo.[57·60] In many patients, control of elevated blood glucose levels by sulphonylureas may also increase the sensitivity of target tissues to insulin by removing glucose toxicity.[1,8,40,41]
The sulphonylureas have no stimulatory effect on insulin secretion in patients with insulin-de-
Bressler & Johnson
pendent diabetes mellitus (IODM) or in pancreatectomised diabetic patients. [51 ,57,58.61·64]
Untreated NIDDM patients have elevated fasting and postprandial blood glucose levels and low plasma insulin levels compared with nondiabetic individuals. Sulphonylurea therapy lowers blood glucose and raises plasma insulin to above pretreatment levels. Over a period of months, the efficacy of the sulphonylurea is evidenced by improved fasting and postprandial blood glucose levels. However, the plasma insulin falls to a level that is above the pretreatment level, but below the level achieved soon after initiation of sulphonylurea therapy.[8,65] This reduction in insulin secretion reflects the improvement in blood glucose levels pro-
Tolbutamide
CH3-C0-o-S02-NH-CO-NH-D Acetohexamide
C,,-o-So,-NH-CO-NH-{]
CI--O-S02-NH-CO-NH-CH2-CH2-CH3
CH'~-=>-CO-NH-C"-CH,-o-so,-.a<-CO-NH-D CI
< )-CO-NH-CH,-C,,-o-so,-NH-CO-NH-D
CH3-o-S02-NH-CO-NH-NCD
Tolazamide
Chlorpropamide
Glipizide
Glibenclamide
Gliclazide
Fig. 1. Commonly used sulphonylurea drugs. The first generation sulphonylureas are tolbutamide, acetohexamide, tolazamide and chlorpropamide. The second generation sulphonylureas are glipizide, glibenclamide (glyburide) and gliclazide.
© Adis International Umited. All rights reserved . Drugs & Aging 1996 Dec; 9(6)

Oral Antidiabetics in the Elderly
duced by the sulphonylurea therapy. If the blood glucose level is raised to pretreatment values, the insulin secretory response is greater than it was before treatment. [65-67]
To stimulate insulin secretion, sulphonylureas must bind to pancreatic ~-cells. The sulphonylurea receptor has been described and its physiological function characterised (fig. 2) .[65-68] Recently, the sulphonylurea receptor has been cloned, providing further insight into its function.[69-71] It has been
shown that the occupation by a sulphonylurea of its pancreatic ~-cell high-affinity receptor inhibits an adenosine triphosphate (ATP)-dependent potassium channel, KATP, which determines resting ~cell membrane potential. The resultant decreased potassium efflux causes ~-cell depolarisation and the activation of L-type calcium channeis.[65.66.69] The consequent calcium influx stimulates insulin secretion.[65-70]
421
The sulphonylurea receptor is situated in the KATP domain, thereby linking the sulphonylurea receptor with openers of the K+ channel functionally and anatomically.l69] Stimulation of insulin secretion by sulphonylureas and glucose is shown in figure 2.[72]
The stimulation of insulin secretion by glucose and amino acids occurs by a similar physiological mechanism to that of the sulphonylureas.l59.65.66,69,701
In the case of glucose, its metabolism produces ATP, which raises the intracellular ATP: adenosine diphosphate (ADP) ratio. This closes the ATPsensitive K+ channel, decreasing K+ efflux (fig. 2) and causing cell membrane depolarisation. As a result, the voltage-sensitive Ca++ channel opens, promoting Ca++ influx[59,67,69] and causing insulin
secretion. Thus, glucose and sulphonylureas stimulate in
sulin secretion via similar actions on ion flux and
Table I. Pharmacokinetic properties and clinical data on sulphonylureas (modified from GerichI51))
Characteristic Drug
tolbutamide tolazamide chlorpropamide glipizide glibenclamide (glyburide)
Relative potency 5 6 100 150
Duration of action (h) 6-10 16-24 24-72 16-24 18-24
Protein binding
type Ionic/non ionic lonic/nonionic Ionic/non ionic Nonionic Nonionic
extent (%) 98 98 95 98 98
Activity of hepatic Weak One active, others Weak Weak One active, others metabolites inactive inactive
Daily dosage (mg)
range 500-3000 100-1000 100-500 2.5-40' 1.25-20
average 1500 250 250 10 7.5
No. of doses per day 2-3 1-2 1-2 1-2
Usual initial daily 500 100 100 5 2.5 dosage (mg)
Dosage forms 250,500 100,250, 500 100,250 5, 10 1.25, 2.5, 5b
available (mg)
Diuretic effect? Yes Yes No No Yes
Antidiurelic effect? Yes No Yes No No
Disulfiram effect? No No Yes No No
Frequency of severe 1 1 4-6 2-4 4-6 hypoglycaemia (%)
Overall frequency of 3 4 9 6 7 adverse effects (%)
a Studies have shown that the maximum effective dosage of glipizide is 10mg daily. Dosages above this may have reduced efficacy.l521
b Glibenclamide is available worldwide as better absorbed micronised preparations. These preparations are available in 1 .5, 1.75, 3, 3.7 and 6mg tablets.
© Adis International Lirnited. All rights reserved. Drugs & Aging 1996 Dec; 9 (6)

422 Bressler & Johnson
Depolarises ---m-'e-'m""'b-ra-ne---.~ CaH
Closes K+
channel K+
ATP/ADP
o o
o o
o ' ''''Ii' ---O vesicles o ... Insulin and C peptide
Fig. 2. Mechanism of insulin secretion by pancreatic ~-cells. In the basal state, an adenosine triphosphate (ATP)·modulated K+ channel is open, maintaining polarisation of the plasma membrane. At the same time, a voltage-dependent Ca++ channel is closed. The entry of glucose into the cell via Glut 2 transporters, and its subsequent metabolism, increases ATP production. An increase in the ATP/adenosine diphosphate (ADP) ratio causes closure of the K+ channel. The level of K+ increases at the plasma membrane, causing depolarisation, which opens the voltage-dependent Ca++ channel and allows Ca++ to enter the cell. The resultant increase in the cytosolic Ca++ level stimulates the secretion of insulin.
membrane depolarisation, but they differ metabolically.l59,69.71] Glucose stimulates proinsulin bio
synthesis, causing both phase I (the initial rapid peak) and phase 2 (later prolonged) insulin release, whereas sulphonylureas induce only phase I insulin release and do not stimulate insulin biosynthesis.[57,58,72,73]
Sulphonylureas augment insulin secretion, but have no direct effect on insulin sensitivity. In addition, they are not effective in IDDM since there is no functioning residual insulin secretory system,P4.80] A number of studies have proposed that sulphonylureas have extrapancreatic effects that contribute to their antidiabetic efficacy. These have recently been summarised.l72]
The sulphonylureas are well absorbed from the gastrointestinal tractJ57,58,81 ,82] Absorption may be
© Adis International Limited. All rights reserved.
slowed by age, diabetic gastric atony and dilatation, hyperglycaemia and the presence of food. [35,57,58,72,81,82]
All sulphonylureas are cleared by both the liver and kidneys, and some undergo hepatic transformation into weakly active or inactive metabolites. For example, one metabolite of acetohexamide is more active than the parent molecule. Because hepatic inactivation is the primary route of clearance of sulphonylureas, standard dosages can cause hypoglycaemia in older patients and those with liver disease.
Renal disease can also result in toxic levels of sulphonyJureas that have active or partially active metabolites (table I). The active metabolites of several sulphonylureas[57,58] are eliminated by renal
excretion. Although its metabolites have only weak
Drugs & Aging 1996 Dec; 9 (6)

Oral Antidiabetics in the Elderly
antidiabetic activity (table I), chlorpropamide is contraindicated in patients with renal disease. Sulphonylureas are highly bound to plasma proteins.[83-85]
The potency of sulphonylureas is based on their effects on insulin secretion. The characterisation of the sulphonylurea receptor has permitted quantification of intrinsic activity in terms of binding constants.[65,68,69,86] The second generation sulphonylureas (e.g. glipizide and glibenclamide) are up to 100 times more potent than the first generation agents (tolbutamide, tolazamide, acetohexamide and chlorpropamide). However, the maximal activity of all of the sulphonylureas is approximately the same. [51 ,55,56,86·90]
The duration of action of the sulphonylureas determines drug dosage schedules. The use of sulphonylureas in elderly patients with NIDDM is complicated by decreased renal function, decreased liver size and liver blood flow, and decreased plasma albumin levels.l35] These changes impede sulphonylurea clearance and predispose the patient to excessive drug activity. Sulphonylureas with longer durations of action (e.g. chlorpropamide) are more likely to cause hypoglycaemia. [57,58,91 ,92J
Although the sulphonylureas ameliorate the deficiency in glucose-stimulated insulin output to some degree, they are frequently not capable of restoring the NIDDM patient to a euglycaemic state. The recognition of the metabolic defects that occur in NIDDM has suggested the development of antidiabetic drugs that aid in dietary control (uglucosidase inhibitors), increase tissue sensitivity to insulin (metformin, thiazolinediones) and decrease hepatic glucose production (metformin). These drugs are being used in conjunction with sulphonylurea therapy because they act via separate mechanisms[93] that will be discussed in sections 4 to 6.
1.1 Efficacy
The efficacy of sulphonylureas in NIDDM depends to a great extent on the selection of suitable patients for such therapy. Ideal patients for
© Adis International Limited. All rights reserved.
423
sulphonylurea therapy are those with NIDDM whose blood glucose level cannot be regulated by dietary modification and physical activity alone.[57,58,88,94-96] The clinical efficacy of sulpho-
nylurea therapy is greatest in patients with NIDDM of 5 years' duration.[57,58,95-IOO] However,
data on the efficacy of sulphonylureas are complicated by uncertainty about patients' suitability for sulphonylurea therapy, and by the lack of suitable placebo controls in most studies.l57,58,101,102] The
apparent efficacy of sulphonylureas may be greater than in reality because of the lack of placebocontrolled crossover studies, especially in newly diagnosed patients.l57,58,101,102] Because NIDDM
responds to dietary modification, exercise and bodyweight loss, placebo effects may be prominent. [101-103]
Sulphonylurea therapy is ineffective in inducing a significant decrease in blood glucose levels in between 15 and 20% of patients with recent-onset (i.e. within the previous 12 months) NIDDM.l57,58,97,99,101,102,104] This is termed 'pri-
mary failure'. About 50% of sulphonylurea-treated patients achieve normal or near-normal blood glucose levels, and the remainder have lesser, varying degrees of blood glucose controP57,58,97-106] In a proportion of NIDDM patients who have an initial clinical response to sulphonylureas, treatment failure occurs after months to years. This has been designated 'secondary failure' .[76,97,101,102,107,108]
The attribution of lack of efficacy to the drug alone is complicated by inadequate selection of suitable candidates for sulphonylurea therapy, patient noncompliance with dietary modifications and prescribed drugs, the use of inadequate drug dosages, and other confounding factors.l57,58,107]
The annual secondary failure rate has been reported to be as high as 3 to 5%.[76,97,107,108]
An effective response to a sulphonylurea is characterised by a reduction in the fasting and postprandial blood glucose levels. These changes in blood glucose are brought about by an increase in ~-cell insulin output; the insulin is transported to the liver, where it decreases hepatic glucose output, and to the periphery, where it stimulates glucose
Drugs & Aging 1996 Dec; 9 (6)

424
uptake and utilisation. The resulting lower blood glucose level sensitises peripheral target tissues to insulin, leading to glucose uptake and utilisation, and the p-cells to glucose, leading to insulin secretion. [1,8,37,39-41, I 09-111]
There is a lack of evidence that successful regulation of blood glucose with sulphonylureas decreases the retinal, renal and neurological complications associated with NIDDM. A large prospective study is ongoing in the UK to ascertain whether better blood glucose control decreases the morbidity and mortality of NIDDM, and to determine whether insulin or oral antidiabetic drugs are more effective.l I04,105] Interim data from the study, collated at I year, showed that dietary modification failed to control blood glucose in 83% of patients, and that sulphonylureas and insulin were about equally effective in reducing fasting blood glucose and glycated haemoglobin (HbAlc) levels.l 104,105]
Follow-up studies at 3 to 6 years revealed that 85% of sulphonylurea-treated NIDDM patients had good diabetic control (mean fasting blood glucose level 7.2 mmoIlL), although 10% also required metformin and 5% were switched to insulin.l 112] The average nonfasting blood glucose level in the insulin-treated group (i.e. those initially treated with insulin, as opposed to a sulphonylurea) was the same as that in the sulphonylurea-treated group (7.2 mmoI/L), whereas the level in the placebo group was 9.1 mmol/L.
By the sixth year of the study, 20% of the patients who were initially treated with sulphonylureas required the addition of metformin to their regimen, and 12% had been changed to insulin therapy.! I 13] The efficacy of sulphonylurea therapy was found to diminish progressively with time. The percentage of sulphonylurea-treated patients with a fasting blood glucose of >7.0 mmollL was 50% at 3 years and 65% at 6 years. The investigators noted that the likelihood of sulphonylurea failure at 6 years was correlated with higher blood glucose levels at the start of the study. [113]
The main reason for primary failure in sulphonylurea therapy is probably insulin insufficiency. [75,108] There are a number of reversible causes
© Adis International Limited. All rights reserved.
Bressler & Johnson
of secondary failure,[107,114] including obesity, lack of physical activity, underdosage and poor compliance with sulphonylureas.[51,55,57,58,72]
1.2 Tolerability
The frequency of adverse effects of sulphonylureas is low. The most common adverse effects are gastrointestinal disorders and skin rashes.!57,58,86, 114, 115] Infrequent cases of haemato-
logical , liver and immunological abnormalities have been reported.!57,58,101] Water retention and hyponatraemia occur with the use of chlorpropamide (6.3% ).[116,117] The cause of this hyponatraemia is the increased secretion and activity of antidiuretic hormone,[118] which is unique to chlorpropamide among the sulphonylurea agents. Risk factors for this adverse effect are old age and the coadministration of thiazide diuretics. [I 19]
Some patients receiving chlorpropamide experience an intense flushing after alcohol (ethanol) consumption.!120] The flushing reaction is of uncertain aetiology and is not seen with the secondgeneration sulphonylurea agents. However, the effect is dose-dependent, and patients who are not affected may experience flushing if their dosage is increased'! 120]
1.2.1 Hypoglycaemia Hypoglycaemia is the most frequent and serious
adverse effect of sulphonylurea therapy.[91 ,92] The frequency of this effect is unknown because most episodes are treated at home, and the incidence from primary and hospital care data is therefore an underestimate. Moreover, many NIDDM patients are elderly, and the signs and symptoms of hypoglycaemia may not be recognised by these patients. Symptoms of weakness, tiredness, confusion, light-headedness and tachycardia may not be recognised as hypoglycaemia.
Symptomatic hypoglycaemia occurred in 20.2% of 40- to 65-year-old NIDDM patients who were treated with sulphonylureas over a 6-month surveillance period.[121] The risk of sulphonylureainduced hypoglycaemia is increased in elderly patients with multiple medical problems, such as poor renal function and inadequate nutrition,
Drugs & Aging 1996 Dec; 9 (6)

Oral Antidiabetics in the Elderly
and in those who are being treated with multiple drugs. [35,57,58,91,92,122,123] Chlorpropamide and
glibenclamide are more frequently associated
with prolonged hypoglycaemia than tolbutamide and gIipizideJI21-125] Glibenciamide has
been identified as the most frequent cause of
sulphonylurea-induced coma and death in Western Europe.[I22,1 24-1 26] However, it is also the most
commonly used sulphonylurea in Western Europe.
Other studies have shown that sulphonylureas are
the major cause of drug-induced hypoglycaemia
requiring hospitalisation (59% of 840 cases), with
9% resulting in death or permanent neurological injury.[9I ,92] Sulphonamide-induced hypoglycae
mic episodes may occur even at standard dosagesJ124,125] In elderly patients with NIDDM, it is
prudent to increase the dosage of sulphonylurea slowly, since these patients may have multiple
other conditions for which drug therapy has been
prescribed.
7.2.2 Cardiofoxicity The University Group Diabetes Program
(UGDP) was a large study that was designed to ascertain whether control of blood glucose could
decrease vascular complications in patients with NIDDM. The study was discontinued because of a
perception that there was a higher incidence of death from cardiovascular causes among patients receiving tolbutamide.[I27,128] However, the study
was criticised on a number of grounds, including
the use of fixed dosages of sulphonylureas, inappropriate selection of patients,[129.130] and poor
study design. Controversy has continued over the
study and the cardiovascular issue for many years.[I02,129,130] The supposed increase in cardio
vascular risk associated with sulphonylureas has
not been substantiated by other studies. In a 1979 policy publication,[1 31] the American Diabetes As
sociation stated that the decision not to use sul
phonylureas based on the UGDP findings should be 'held in abeyance' .[1 31] Thus, evidence that sul
phonylureas are cardiotoxic is lacking.
© Adis International limited. All rights reserved ,
425
Table II. Clinically important drug interactions with sulphonylureas (from Lebovitz & Melander,ll'll with permission)
Interacting drug(s)
Increase in hypoglycaemia Aspirin (acetylsalicylic acid), fibrates, trimethoprim
Alcohol (ethanol), histamine H2 receptor antagonists, anticoagulants
Probenecid, allopurinol
Alcohol, aspirin
Nature of interaction
Displacement of sulphonylurea from albumin binding sites
Competitive inhibition of sulphonylurea metabolism
Inhibition of urinary sulphonylurea excretion
Concomitant use of drugs with hypoglycaemic activity
~-Blockers, sympatholytic drugs Antagonism of counter-regulatory hormones
Worsening of glycaemic control Barbiturates, rifampiCin (rifampin)
Thiazide and loop diuretics, ~-blockers, phenytoin
Corticosteroids, growth hormone, estrogens, catecholamines
1 .3 Drug Interactions
Stimulation of sulphonylurea metabolism
Inhibition of insulin secretion
Inhibition of insulin action
Elderly patients with NIDDM are likely to have other chronic diseases that require drug therapy.[35] NIDDM patients treated with sulphonylureas may be exposed to both pharmacokinetic and pharmacodynamic drug interactions. [35,5 I ,57,58,72,10 I ,132,133]
Sulphonylureas can interact with a number of drugs, resulting in an alteration of the effect of either the sulphonylurea or the interacting drug.[35,5I,57,58,72,IOI ,132,133] Table II lists the mech-
anisms by which some sulphonylureas interact with other drugs.[57,58, 134,135] There have been
many reports of drug interactions between sulphonylureas and drugs commonly used by elderly patients. [57 ,58, I 33-14 I]
2. Combination Drug Therapy
The use of sulphonylureas plus subcutaneous insulin in patients with NIDDM has been studied by several investigators using various regimens. This therapy, although it did not achieve euglycaemia in patients with NIDDM, improved blood glucose control in many patients, including those with sulphonylurea failure .[142-148]
Drugs & Aging 1996 Dec; 9 (6)

426
The 'dawn phenomenon' is characterised by an increase in blood glucose levels in the early morning hours in the absence of a preceding hypoglycaemic episode. It has been described in patients with IDDM and those with NIDDM.l149.15I) A combination of daytime sulphonylurea therapy and intermediate-acting insulin at night has become commonly used to improve fasting blood glucose levels through better control of nocturnal glycogenolysis and gluconeogenesis.[1O,36,37.152,153) Sim-
ilarly, combination therapy with sulphonylureas and metformin has been used to improve blood glucose control. [154·157]
Acarbose is an a-glucosidase inhibitor that limits and delays the postprandial hyperglycaemia resulting from orally ingested sucrose and starch in patients with NIDDM.[93] Acarbose is effective in both NIDDM and IDDM, since its effects are not dependent on insulin secretion.1158.159) Acarbose is rarely used alone; it is usually combined with insulin, sulphonylureas or metformin.
3. Metformin
Metformin (fig. 3) is a biguanide that has been used worldwide for the treatment of NIDDM since 1957, but has only recently been approved for use in the US. This antihyperglycaemic drug has several unique characteristics that are suited to the therapy of NIDDM in elderly patients.l156.16o.163] The efficacy of metformin monotherapy in the treatment of NIDDM has been well documented, as has its augmentation of the blood glucose lowering effects of sulphonylureas when they are used together. I 154, 155, 157,161 -164)
Metformin is an amphoteric compound (pKa of 2.8 and 11 .5) that is protonated at physiological pH and therefore has a low degree of lipid solubility.[161-163) The oral bioavailability of metformin is
Fig. 3. Structural formula of metformin (1 , 1-dimethylbiguanide).
© Adis International Limited. All rights reserved.
Bressler & Johnson
around 50 to 60%.[162,163) After oral administration, most of the drug is absorbed within 6 hours of ingestion, with peak plasma concentrations being reached after 2 to 3 hours. The proportion of a dose that is absorbed is lower at higher doses.l165-169) Metformin is not protein bound, nor is it metabolised. 1156,160,165,166,169] It has an elimination half-
life of 1.5 to 5h, and is primarily eliminated via renal tubular secretion.[166.168,169) Because of the risk of drug accumulation, metformin is contraindicated in patients with renal insufficiency.
Because of the potential for lactic acidosis with biguanides, metformin should not be used in patients with renal or hepatic disease.l156.170-172] Renal disease results in the elevation of blood lactate levels, and cases of lactic acidosis have occurred in patients with NIDDM and renal insufficiency who were treated with metforminJI56,17o,173,174]
Metformin causes small, postprandial increases in plasma lactate levels.1164,175] Metformin accumulates in the intestine, resulting in the production of lactate from ingested carbohydrateJI63,176.I77) In individuals with normal hepatic function, the liver efficiently extracts and metabolises the lactate produced by the intestines.l161.176.177] However, in patients with severe liver disease, the liver may not extract the intestinal lactate and peripheral plasma levels may rise.l 156,171,178)
Metformin does not increase lactate production by muscle or other peripheral tissues.1156,16I) Diseases that predispose to decreased tissue perfusion cause hypoxia, resulting in increased lactate production, but renal impairment is the most frequent underlying complication in metformin-induced lactic acidosis.1156.171-174] Overdoses of metformin can be treated using haemodialysis, which has been used in patients with lactic acidosisJI79)
In patients with normal renal function, metformin is absorbed more slowly than it is eliminated, and accumulation does not occurJI60.162.163.168]
3.1 Efficacy
Metformin has demonstrated antihyperglycaemic effects in the therapy of obese and lean NIDDM patients whose diabetes has not been con-
Drugs & Aging 1996 Dec; 9 (6)

Oral Antidiabetics in the Elderly
trolled with diet modification alone.fI56.172,173,ISO-IS5]
The efficacy of metformin as an antihyperglycaemic agent has been confirmed by a number of double-blind, placebo-controlled randomised trials,1161 -164,IS6] and is about equal to that of the
sulphonylureas in newly diagnosed NIDDM patients. fISI ,ls4,IS7-190] When used in combination,
metformin and sulphonylureas exhibit synergistic antihyperglycaemic effects. f 154, 157, 164.191-196]
The mechanisms of action of metformin are unknown at the molecular level, and there is controversy about the quantitative importance of its various physiological and biochemical antihyperglycaemic actions.[161 ,164] Metformin has been
studied extensively in patients with NIDDM in whom acceptable blood glucose control has not been achieved with diet modification alone. The efficacy of metformin as monotherapy has been attributed to several effects,f I61 ,164,197.200] in-
cluding: (a) a reduction in the rate of gastrointestinal glu
cose absorption, reducing the intensity of the glucose challenge to insulin secretion;
(b) a decreased rate of hepatic glucose production, attributed by many investigators to a decrease in hepatic gluconeogenesis; f 161,156,164,199,200]
(c) increased peripheral glucose utilisation with a concomitant decrease in the plasma insulin level. Although it has been claimed that metformin sensitises peripheral tissues to insulin,fI61 ,200,201 ,202]
other studies have shown that metformin sensitises the peripheral tissues to glucose- rather than insulin-mediated glucose uptake.f 161 ,199,197,19S] In a
recent studyfl99] performed with the use of a 6.9 mmollL (blood glucose level) hyperglycaemic clamp, peripheral glucose uptake was increased in metformin-treated obese or lean NIDDM patients. In contrast, in a euglycaemic insulin clamp studyl199] increased glucose uptake was seen only in obese patients;
(d) a decrease in plasma total cholesterol, LDL-cholesterol and triglyceride levels, and a slight increase in the HDL-cholesterol leveJ.l156,164,172,201,203-205] These changes may be
separate from the effect of metformin on blood glu-
© Adis International Urnited. All rights reserved.
427
cose, but are consonant with the bodyweight loss associated with metformin use;[156,161 ,164,ISS,IS9,200]
(e) a decrease in fasting and postprandial blood glucose and HbA lc levels in around 80% of newly diagnosed patients.l 162, 163]
Primary failure rates with metformin are around 12%, and secondary failure rates range from 5 to 10% per year.l 162, 163,206,207] Decreases in the blood
glucose level on initiating therapy are around 20%, and are accompanied by an improvement in oral glucose tolerance.[l60, 164, lSI ,200,201]
Metformin is suitable as the sole antihyperglycaemic agent for elderly NIDDM patients because it does not cause hypoglycaemia and results in some bodyweight loss. Moreover, patients with NIDDM often have elevated blood lipids and lowered HDL-cholesterol levels, which are risk factors for arteriosclerotic heart disease. f20S] These dyslipidaemias are often improved by metformin therapy.
Sulphonylureas and metformin have similar efficacy as monotherapy in NIDDM. Combination therapy is often used in patients with NIDDM in whom satisfactory control of blood glucose levels is not achieved with either drug alone. In studies in which maximal dosages of sulphonylureas failed to control blood glucose adequately, the addition of metformin (850 to 2500 mg/day) decreased mean fasting and postprandial blood glucose levels, HbA lc levels, serum lipid levels and bodyweight. f ISS, 191 -193,209]
Two randomised, parallel-group, double-blind studies of 29 weeks' durationfl64] have compared: (i) metformin 2500mg versus placebo; and (ii) metformin 2500mg or glibenclamide 20mg versus the combination. At 29 weeks, patients in the glibenclamide group had an increase in both fasting plasma glucose (0.8 ± 0.2 mmoIlL) and HbA lc (0.2 ± 0.1 %) levels. Patients who had received metformin had slight decreases in both fasting plasma glucose (0.1 ± 0.3 mmollL) and HbA lc (0.4 ± 0.1 %) levels . Patients who received both drugs showed a large decrease in fasting blood glucose (from 14.6 ± 0.2 to 10.5 ± 0.2 mmol/L) and HbA lc (8.7 ± 0.1 to 7.1 ± 0.1 %) levels compared with
Drugs & Aging 1996 Dec; 9 (6)

428 Bressler & Johnson
Table III. Reductions in plasma lipid levels following treatment with metformin 2500 mg/day, either as monotherapy or in combination with glibenclamide (glyburide) 20 mg/day. Data are from a 29-week study in patients with non-in sui in-dependent diabetes mellitus"641
Lipid Metformin Metformin plus glibenclamide
reduction in mg/dl reduction in mmollL reduction in mg/dl reduction in mmollL
Total cholesterol
Low density lipoprotein cholesterol
Triglycerides
4 ±2'
6±2"
16±r
0.10 ± 0.05'
0.16±0.OS··
0.1S ± O.OS·
10 ± 2'
S ± 2'
20±r
0.25 ± 0.05'
0.21 ±O.OS·
0.23 ±O.OS·
Symbols: • p < 0.001 ; •• p < 0.019.
baseline. Metformin used as monotherapy or in combination with a sulphonylurea reduced plasma lipids significantly (table III). In contrast, glibenclamide monotherapy had no beneficial effect on plasma lipids. [1M] Bodyweight decreased by 3.8 ± 0.2kg in the metformin group, and increased by 0.4 ± 0.2kg in the glibenclamide group (p < 0.001).[164] There was no significant decrease
in fasting plasma insulin levels in the metformin group.
3.2 Toxicity
The adverse effects of metformin are mainly gastrointestinal in nature. Around 5 to 20% of patients started on the drug experience transient nausea, diarrhoea and anorexia.[181,1 82,210-212] These
effects can be avoided in part by slowly increasing the metformin dosage, and by taking the drug with food . Around 4.2% of patients who begin therapy with metformin discontinue taking it because of adverse gastrointestinal effects. [ 173.21 3.214] In addi
tion, the drug decreases the absorption of vitamin BI2 (cyanocobalamin),lI56.173.212,215,216] but this is
seldom of clinical importance. As discussed on page 426, lactic acidosis is an exceedingly rare
CH, 0-CH, 0
CH'WO CH,o CH'r-( SyNH HO
o CH,
Fig. 4. Structural formula of troglitazone, (±)-all-rac-5-{p-((6-hydroxy-2,5,7,8-tetramethyl-2-chromanyl)methoxy)benzyl)-2, 4-thiazolidinedione.
© Adis International Limited. All rights reserved .
event that may occur in susceptible patients (e.g. those with renal failure) .
Drug interactions with metformin, a number of which are pharmacodynamic in nature, are infrequent. ~-Blockers may cause dyslipidaemia and decrease glucose tolerance on their own, thereby possibly overcoming the triglyceride-lowering effects of metformin. These effects are more pronounced with the nonselective agents (e.g. propranolol).[1 34,2171 They may also delay recovery from hypoglycaemia, and tachycardia deriving from hypoglycaemia,lI34,2171 in patients treated with metformin plus sulphonylureas or insulin. When given as monotherapy, metformin does not cause hypoglycaemia.
Cimetidine has been shown to cause an elevation of plasma metformin levels, probably via competition for renal tubular secretion. l351
Sulphonylureas and metformin have additive blood glucose-lowering effects. Thus, their concomitant use increases the potential for hypoglycaemia to occur.
4. Troglitazone
The thiazolinediones have been studied as antidiabetic agents for over a decade.l218-2201 During the past 5 years, studies in insulin-resistant individuals with NIDDM and/or obesity have proven the efficacy of this class of drugs. At present, troglitazone (fig. 4) is the thiazolinedione that has undergone most clinical investigation in the US.
Thiazolinediones have been tested in a number of animal models of insulin resistance. These include the KK mouse and db/db mouse, which are spontaneously diabetic obese models, and the ob/ob mouse and the Wi star and Zucker fatty rats, which are insulin-resistant obese models.l218-2231
Drugs & Aging 1996 Dec; 9 (6)

Oral Antidiabetics in the Elderly
These animals models respond to oral thiazolinediones with a fall in blood glucose, an increase in glucose tolerance and decreases in plasma insulin and triglyceride levels.1218-223] The agents are
efficacious in insulin-resistant, but not insulindeficient, animals.[218-223] The thiazolinediones
have not been shown to cause hypoglycaemia in normal animals.1218-223]
In vitro, troglitazone has been shown to increase glucose utilisation in muscle and decrease glucose production by liver tissue.[218,221,224]
The animal studies suggest that thiazolinediones increase tissue sensitivity to insulin, which would enhance glucose utilisation by adipose tissue and skeletal muscle. The drugs produce a decrease in plasma insulin levels, causing a decrease in insulin resistance.[2 1 8,224.225] The initial response
is a fall in blood glucose levels, followed by a decrease in plasma insulin.
Studies of the effect of thiazolinediones on gluconeogenesis have had conflicting results.l226-2281 In studies where gluconeogenesis inhibition was shown, the changes were small and are unlikely to be the major factor in the antihyperglycaemic action of the drugsP291
The molecular mechanism of action of the thiazolinediones is unknown, but some studies have suggested that these drugs act at an intracellular site subsequent to the binding of insulin to its receptor.[21 8,22I] The decrease in blood glucose appears to be a consequence of increased glucose utilisation rather than decreased hepatic glucose production. [218,230,231]
Troglitazone has been studied in both NIDDM and in nondiabetic obese insulin-resistant patients.l222,225,232,2331 In a placebo-controlled study
in II patients with NIDDM,[2221 troglitazone 400
mg/day lowered the fasting blood glucose level in 8 patients, with an improvement in the 7-hour meal tolerance test in the entire group. Interestingly, the fall in fasting blood glucose level occurred after 2 to 3 weeks of therapy, with maximal responses usually occurring 2 weeks after the initial response.
© Adis International Limited. All rights reserved.
429
In a study in 18 nondiabetic obese individuals, 9 of whom had impaired glucose tolerance, 12 weeks' treatment with troglitazone 200mg twice daily decreased insulin resistance and improved glucose tolerance to oral glucose and to mixed meals.l222,233]
5. Acarbose
Dietary control of blood glucose is considered an essential part of therapy in patients with NIDDM. Studies in which multiple small meals were compared with fewer, larger meals showed that the former were associated with better blood glucose control in diabetic patients.[234,235] Pharmacological approaches to delaying the digestion and absorption of complex carbohydrates have been made over the past several decades.1236] The development of acarbose and its sister compound miglitol (fig. 5) was the culmination of successful attempts to regulate the activity of the intestinal enzymes involved in the digestion of carbohydrates such as starch, sucrose and maltose.[237-241] Delayed digestion of complex carbohydrates leads to the delayed absorption of end-product monosaccharides throughout the small intestineP42] The absorption of dietary monosaccharides, such as glucose, is not affected by acarbose or miglitoI. 1236,242] Acarbose inhibits intestinal brush border a-glucosidases and, when administered orally, is effective in attenuating postprandial rises in blood glucose in diabetic patients.1236-239,242-244]
Chemically, acarbose is an oligosaccharide produced by cultured strains of actinomycetes. It is a competitive inhibitor that has a high affinity for sucrase and a lower affinity for glucoamylase and pancreatic amylase.l236,237] Acarbose is administered with food intake, therefore it must be taken 3 or more times a day. When a meal containing sucrose or starches is ingested, acarbose decreases the postprandial rise in blood glucose through inhibition of intestinal disaccharidases. [236,238,245,246]
Clinical studies with acarbose in both IDDM and NIDDM patients have shown that the drug attenuates the postprandial rise in blood glucose levels and reduces urinary glucose excretion.[245-247]
Drugs & Aging 1996 Dec; 9 (6)

430 Bressler & Johnson
HO""'7=\,. CH, HO~N--\--\--O\
Ho~a~CH20H 0
o la CH20H
HO OH 0+\----0,
Acarbose LJr\~OH HO OH
HO
H
Miglitol
Fig. 5. Structural formulae of the a-glucosidase inhibitors acarbose and miglitol.
However, the overall improvement in blood glucose control is modest. [244.248.249] Acarbose does not decrease hepatic glucose outpUt.[236]
The dosages of acarbose that have been used in most clinical studies are 50 to 250mg with each large meal, and correspondingly smaller doses with snacks. The most common adverse effects are increased flatulence, abdominal bloating and, less commonly, diarrhoea.[244.250] The combined use of low-dose acarbose with guar gum crispbread was reported to decrease postprandial glycaemia with fewer adverse effects.[251] Because its mechanism of action differs from that of other antidiabetic agents, acarbose can be combined with them to produce addi ti ve efficacy. [252]
6. Conclusion
NIDDM has a high incidence in elderly people. It is a disease conditioned by hereditary factors and confounded by age, obesity and decreased physical activity. NIDDM is characterised by both insulin
© Adis International Limited. All rights reserved.
resistance and, in its fully expressed stages, by insulin insufficiency.[1.8.9] If untreated or inadequately treated, NIDDM is associated with a number of organ and tissue impairments resulting from nerve, renal, retinal and cardiovascular damage.
In this review of the oral antidiabetic drugs currently available for the treatment of NIDDM, we have focused on the place of drug therapy in dealing with disease pathophysiology. The available drugs remedy, to some extent, the insulin insufficiency and the insulin resistance found in NIDDM.
The oral sulphonylureas stimulate pancreatic phase I output of insulin. The consequent lowering of blood glucose levels relieves the insulin resistance engendered by glucose toxicity; thus, stimulation of insulin output indirectly decreases insulin resistance.
Metformin decreases blood glucose levels in patients with NIDDM in several ways. It delays glucose absorption, thereby decreasing the intensity of the challenge to endogenous insulin. It sensitises
Drugs & Aging 1996 Dec; 9 (6)

Oral Antidiabetics in the Elderly
peripheral tissues to glucose-induced glucose uptake, thereby reducing blood glucose and plasma lipid levels, and decreases hepatic glucose production (via glycogenolysis and/or gluconeogenesis). Most recent clinical studies suggest that decreased hepatic glucose output, rather than the enhancement of peripheral glucose uptake, is the dominant effect of metformin in humans.
Troglitazone sensitises tissues to the actions of insulin. It stimulates insulin-induced glucose removal in skeletal muscle and adipose tissue by magnifying the insulin effect. It also has some effect in decreasing hepatic gluconeogenesis. The (X
glucosidase inhibitors serve as an aid to the dietary control of blood glucose levels by delaying the digestion of complex dietary carbohydrates. This decreases the physiological rise in blood glucose levels, thereby reducing the need for insulin. The absorption of dietary glucose and other monosaccharides is not affected.
Metformin, troglitazone and acarbose all have proven efficacy in NIDDM patients, but require endogenous insulin because they do not stimulate its secretion. They are well tolerated in elderly patients with NIDDM, partly because of the lack of hypoglycaemia that occurs with the use of these drugs.
References I. DeFronzo RA. The triumvirate: ~-cell, muscle, liver: a collu
sion responsible for NIDDM. Diabetes 1988; 37: 667-87 2. Shinmukata H, Muller DC, Fleg JL, et a!. Age as an independent
determinant of glucose tolerance. Diabetes 1991; 40: 44-51 3. Harris MI. Epidemiology of diabetes mellitus among the el
derly in the United States. Clin Geriatr Med 1990; 6: 703-19 4. Andres R. Aging and diabetes. Med Clin North Am 1971 ; 55:
835-46 5. Morrow LA, Halter JB. Treatment of the elderly with diabetes.
In: Kahn CR, Weir GC, editors. Joslin 's diabetes mellitus. 13th ed. Philadelphia: Lea and Febiger, 1994: 552-9
6. Harris MI, Hadden WC, Knowler WC, et a!. Prevalence of diabetes and impaired glucose tolerance and plasma glucose levels in U.S. population ages 20-74 years. Diabetes 1987; 136: 523-34
7. King H, Rewers M. WHO Ad Hoc Diabetes Reporting Group: global estimates for prevalence of diabetes mellitus and impaired glucose tolerance in adults. Diabetes Care 1993; 16: 157-77
8. DeFronzo RA, Bonadonna RC, Ferrannini E. Pathogenesis of NIDDM: a balanced overview. Diabetes Care 1992; 15: 318-68
© Adis International Limited. All rights reserved.
431
9. Hamman R. Genetic and environmental determinants of noninsulin dependent diabetes mellitus (NIDDM). Diabetes Metab Rev 1992; 8: 287 -338
10. Consoli A, Nurjhan N, Capani F, et a!. Predominant role of gluconeogenesis in increased hepatic glucose production in NIDDM. Diabetes 1989; 38: 550-7
II . Bogardus C, LiIIioja S, Nyomba BL, et a!. Distribution of in vivo insulin action in Pima Indians as a mixture of three normal distributions. Diabetes 1989; 38: 1423-32
12. Lillioja S, Molt DM, Spraul M, et a!. Insulin resistance and insulin secretory dysfunction as precursors of non-insulin dependent diabetes mellitus. N Engl J Med 1993; 329: 1988-92
13. Warran JH, Martin BC, Krolewski AS, et a!. Slow glucose removal rate and hyperinsulinemia precede the development of type II diabetes in the offspring of diabetic parents. Ann Intern Med 1990; 113: 909-15
14. Eriksson J, Franssila-Kallunki A, Ekstrand A, et a!. Early metabolie defects in persons at increased risk for non-insulin-dependent diabetes mellitus. N Engl J Med 1989; 321 (6): 337-43
15. Turner R, Mathews D, Clark A, et a!. Pathogenesis ofNIDDM: a disease of deficient insulin secretion. BaiIIieres C1in Endocrinol Metab 1988; 2: 327-42
16. Gerich J. Role of insulin resistance in the pathogenesis of type II (non-insulin dependent) diabetes mellitus. Baillieres Clin Endocrinol Metab 1988; 2: 307-26
17. Taylor S, Accilli D, Imai Y. Insulin resistance or insulin deficiency: which is the primary cause of NIDDM? Diabetes 1994; 43: 735-40
18. Yki-Harvinsen H. Pathogenesis of non-insulin dependent diabetes mellitus. Lancet 1994; 343: 91-5
19. Pi menta W, Korytkowski M, Mitra A, et a!. Pancreatic ~-cell dysfunction as the primary genetic lesion in NIDDM. JAMA 1995; 273: 1855-61
20. Martin B, Warram J, Rosner B, et a!. Familial clustering of insulin sensitivity. Diabetes 1992; 41: 850-4
21. Weir Gc. Which comes first in non-insulin dependent diabetes mellitus: insulin resistance or ~-cell failure? Both come first. JAM A 1995; 273: 1878-9
22. Vaag A, Henriksen JE, Madsbad S, et a!. Insulin secretion, insulin action and hepatic glucose production in identical twins discordant for non-insulin dependent diabetes mellitus. J Clin Invest 1995; 95: 690-8
23. Iselius L, Lindsten J, Morton N, et a!. Genetic regulation of the kinetics of glucose-induced insulin release in man. Clin Genet 1985; 28: 8-15
24. Meneilly GS, Dawson K, Tessier D. Alterations in glucose metabolism in the elderly patient with diabetes. Diabetes Care 1993; 16: 1241-8
25. Chen M, Bergman RN, Pauni G, et a!. Pathogenesis of age-related glucose intolerance in man: insulin resistance and decreased ~-cell function. J Clin Endocrinol Metab 1985; 60: 13-20
26. Zavaroni I, Dall' Aglio E, Bruschi F, et a!. Effect of age and environmental factors in glucose tolerance and insulin secretion in a worker population. J Am Geriatr Soc 1986; 34: 271-5
27. Saad MF, Knowler WC, Pettitt DJ , et a!. A two step model for development of non-insulin dependent diabetes. Am J Med 1991; 90: 229-35
28. Sicree R, Zimmet PZ, King HOM, et a!. Plasma insulin response among Naurvans: prediction of deterioration in glucose tolerance over 6 years. Diabetes 1987; 36: 179-86
29. Charles MA, Fontbonne A, Eschwegs E. Risk factors of type 2 (non-insulin dependent) diabetes in a caucasian population [abstract]. Diabetologia 1988; 31 : 479A
Drugs & Aging 1996 Dec; 9 (6)

432
30. Bruce DG, Chisholm DJ, Storlien LH, et al. Physiological importance of deficiency in early prandial insulin secretion in NIDDM. Diabetes 1988; 37: 736-44
31. Laws A, Reaven GM. Effect of physical activity on age-related glucose intolerance. Clin Geriatr Med 1990; 6: 849-63
32. O ' Dea K. Obesity and diabetes in 'the land of milk and honey'. Diabetes Metab Rev 1992; 8: 373-88
33. Kriska AM, Bennett PH. An epidemiological perspective of the relationship between physical activity and NIDDM : from activity assessment to intervention. Diabetes Metab Rev 1992; 8: 355-72
34. Tuomilehto J, Knowler WC, Zimmet P. Primary prevention of non-insulin dependent diabetes mellitus. Diabetes Metab Rev 1992; 8: 339-53
35. Bressler R. Adverse drug reactions in geriatric pharmacology. In: Bressler R, Kates MD, editors. Geriatric pharmacology. New York: McGraw-Hili, 1993: 41-62
36. DeFronzo RA, Ferrannini E. Regulation of hepatic glucose metabolism in humans. Diabetes Metab Rev 1987; 3: 415-59
37. DeFronzo RA, Ferrannini E, Simonson DC Fasting hyperglycemia in non-insulin dependent diabetes mellitus: contributions of excessive glucose production and impaired tissue glucose uptake. Metabolism 1989; 38: 387-95
38. Ferrannini E, Simonson DC, Katz LD, et al. The disposal of an oral glucose load in patients with non-insulin dependent diabetes, Metabolism 1988; 37: 79-85
39. Mitrakou A, Kelley D, Yeneman T, et al. Contribution of abnormal muscle and liver glucose metabolism to postprandial hyperglycemia in NIDDM. Diabetes 1990; 39: 1381-90
40. Leahy JL, Cooper HE, Deal DA, et al. Chronic hyperglycemia is associated with impaired glucose influence on insulin secretion: a study in normal rats using chronic in vivo glucose infusions. J Clin Invest 1986; 77: 908-15
41. Rossetti L, Giaccari A, DeFronzo RA. Glucose toxicity. Diabetes Care 1990; 13: 610-30
42. Kannel WB, McGes DL. Diabetes and cardiovascular disease: the Framingham study. JAMA 1979; 241: 2035-8
43. Pyiirala K, Laakso M, Uusitupa M. Diabetes and atherosclerosis: an epidemiologic view. Diabetes Metab Rev 1987; 3: 463-524
44. Chait A, Bierman EL. Pathogenesis of macrovascular disease in diabetes. In: Kahn CR, Weir GC, editors. Joslin 's diabetes mellitus. 13th ed. Philadelphia: Lea and Febiger, 1994: 648-64
45. Howard BY, Howard WJ. The pathophysiology and treatment of lipid di sorders in diabetes mellitus. In: Kahn CR, Weir GC editors. Joslin's diabetes mellitus. 13th ed. Philadelphia: Lea and Febiger, 1994: 372-96
46. Howard B V. Lipoprotein metabolism in diabetes mellitus. J Lipid Res 1987; 28: 613-28
47. Barakat HA, Carpenter JW, McLendon YO, et al. Influence of obesity, impaired glucose tolerance, and NIDDM on LDL structure and composition: possible link between hyperinsulinemia and atherosclerosis. Diabetes 1990; 39: 1527-33
48. Chen YDI, Jeng CY, Reaven GM. HDL metaboli sm in diabetes. Diabetes Metab Rev 1987; 3: 653-68
49. Dunn FL. Treatment of lipid disorders in diabetes mellitus. Med Clin North Am 1988; 72: 1379-98
50. DeFronzo RA, Ferrannini E. Insulin resistance: a multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia and atherosclerotic cardiovascular disease. Diabetes Care 1991 ; 14: 173-94
51. Gerich JE. Oral hypoglycemic agents. N Engl J Med 1989; 321: 1231-45
© Adis International Limited. All rights reserved .
Bressler & Johnson
52. Steinman S, Mellander A, Groop P-H, et al. What is the benefit of increasing the sulfonylurea dose? Ann Intern Med 1993; 118: 169-72
53. Glimepiride for NIDDM. Med Lett 1996; 38: 47-8 54. Draeger E. Clinical profile of glimepiride. Diabetes Res Clin
Pract 1995; 28 Suppl. E: 139-46 55. Melander A, Bitzen P-O, Faber 0 , et al. Sulphonylurea anti
diabetic drugs: an update of their clinical pharmacology and rational therapeutic use . Drugs 1989; 37: 58-72
56. Marchetti P, Navalesi R. Pharmacokinetic-pharmacodynamic relationships of oral hypoglycaemic agents: an update. Clin Pharmacokinet 1989; 16: 100-28
57. Jackson JE, Bressler R. Clinical pharmacology of sulfonylurea hypoglycemic agents: I. Drugs 1981; 22: 211-45
58. Jackson JE, Bressler R. Clinical pharmacology of sulfonylurea hypoglycemic agents: II. Drugs 1981; 22: 295-320
59. Malaisse WJ , Lebrun P. Mechanism of sulfonylurea induced insulin release. Diabetes Care 1990; 13 Suppl. 3: 9-17
60. Pfeifer MA, Halter JB, Judzewitsch RG, et al. Acute and chronic effect of sulfonylurea drugs on pancreas islet function in man. Diabetes Care 1984; 7 Suppl. I: 25-34
61. Loubatieres A. The hypoglycemic sulfonamides: history and development of the problem from 1942 to 1945. Ann N Y Acad Sci 1957; 71: 4-11
62. Houssay BA, Penhos JC Action of the hypoglycemic sulfonyl compounds in hypophysectomized, adrenalectomized and depancreatized animals. Metabolism 1958; 5: 727 -32
63. Mirsky lA, Lerisutti G, Jinks R. Ineffectiveness of sulfonylureas in alloxan diabetic rats. Proc Soc Exp Bioi Med 1956; 91: 475-7
64. Joffe BI , Jackson WPU, Bank S, et al. Effect of oral hypoglycemic agents on glucose tolerance in pancreatic diabetes. Gut 1972; 13: 285-8
65. Kolterman OG, Gray RX, Shapiro G, et al. The acute and chronic effects of sulfonylurea therapy in type II diabetic subjects. Diabetes 1984; 33: 346-54
66. Nelson TY, Gaines KL, Rajan AS, et al. Increased cytosolic calcium: a signal for sulfonylurea-stimulated insulin release from beta cells. J Bioi Chern 1987; 262: 2608-12
67. Boyd III AE. Sulfonylurea receptors, ion channels, and fruit flies. Diabetes 1988; 37: 847-50
68. Gaines KL, Hamilton S, Boyd III AE. Characterization of the sulfonylurea receptor on beta cell membranes. J Bioi Chern 1988; 263: 2589-92
69. Aguilar-Brywn L, Nichols CG, Wechsler SW, et al. Cloning of the cell high-affinity sulfonylurea receptor: a regulator of insulin secretion. Science 1995; 268: 423-6
70. Thomas PM, Cote GJ, Wohllk N, et al. Mutations in the sulfonylurea receptor gene in familial persistent hyperinsulinemic hypoglycemia of infancy. Science 1995; 268: 426-9
71. Wollheim CB, Biden TJ. Signal transduction in insulin secretion: comparison between fuel stimuli and receptor agonists. Ann N Y Acad Sci 1986; 488: 317-33
72. Lebovitz H. Oral hypoglycemic agents. In: Kahn CR, Weir GC, editors. Joslin's diabetes mellitus. 13th ed. Philadelphia: Lea and Febiger, 1994: 508-29
73. Yalow RS, Black H, Yillazon M, et al. Comparison of plasma insulin levels following administration of tolbutamide and glucose. Diabetes 1968; 9: 356-62
74. Sartor G, Ursing D, Nilsson-Ehle P, et al. Lack of primary effect of sulphonylurea (glipizide) on plasma lipoproteins and insulin action in former type I diabetics with attenuated insulin secretion. Eur J Clin Pharmacol 1987; 33: 279-82
Drugs & Aging 1996 Dec; 9 (6)

Oral Antidiabetics in the Elderly
75. Snehalatha C, Ramachandran A, Mohan V, et al. Beta cell function in long term NIDDM (type 2) patients and its relation to treatment. Horm Metab Res 1986; 18: 391-4
76. Groop LC, Pelkonen R, Koskimies S, et al. Secondary failure of treatment with oral antidiabetic agents in non-insulin dependent diabetes. Diabetes Care 1986; 9: 129-33
77. Castillo M, Scheen AJ , Paolisso G, et al. The addition of glipizide to insulin therapy in type-II diabetic patients with secondary failure to sulfonylureas is useful only in the presence of a significant residual insulin secretion. Acta Endocrinol 1987; 116: 364-72
78. Grunberger G, Ryan J, Gorden P. Sulfonylureas do not affect insulin binding or glycemic control in insulin-dependent diabetics. Diabetes 1982; 3 I: 890-6
79. Ratzmann KP, Schulz B, Heinke P, et al. Tolbutamide does not alter insulin requirement in type I (insulin-dependent) diabetes. Diabetologia 1984; 27: 8-12
80. Simonson DC, Delprato S, Castellino P, et al. Effect of glyburide on glycemic control , insulin requirement, and glucose metabolism in insulin-treated diabetic patients. Diabetes 1987; 36: 136-46
81. Sartor G, Melander A, Schersten B, et al. Influence of food and age on the single dose kinetics and effects of tolbutamide and chlorpropamide. Eur J Clin Pharmacol 1980; 17: 285-93
82. Antal EJ , Gillespie WR, Phillips JP, et al. The effect of food on the bioavailability and pharmacodynamics of tolbutamide in diabetic patients. Eur J Clin Pharmacol 1982; 22: 459-62
83. Crooks MJ, Brown KF. The binding of sulphonylureas to serum albumin. J Pharm Pharmacol 1974; 26: 304-11
84. Crooks MJ, Brown KF. Interaction of glipizide with human serum albumin. Biochem Pharmacol 1975; 24: 298-9
85. Brown KF, Crooks MJ. Displacement of tolbutamide, glibenclamide and chlorpropamide from serum albumin by anionic drugs. Biochem Pharmacol 1976; 25: 1175-8
86. Lebovitz HE. Glipizide: a second-generation sulfonylurea hypoglycemic agent: pharmacology, pharmaCOkinetics and clinical use. Pharmacotherapy 1985; 5: 63-77
87. Groop L, Wahiin-Boll E, Goop P-H, et al. Pharmacokinetics and metabolic effects of glibenclamide and glipizide in type 2 diabetics. Eur J Clin Pharmacol 1985; 28: 697-704
88. Melander A, Lebovitz HE, Faber OK. Sulfonylureas: why, which, and how? Diabetes Care 1990; 13 Suppl. 3: 18-25
89. Ferner RE, Chaplin S. The relationship between the pharmacokinetics and pharmacodynamic effects of oral hypoglycemic drugs. Clin Pharmacokinet 1987; 12: 379-401
90. Clarke BF, Campbell IW. Long term comparative trial of glibenclamide and chlorpropamide in diet-failed, maturityonset diabetics. Lancet 1975; I: 246-8
91. Ferner RE, Neil HAW. Sulphonylureas and hypoglycaemia. BMJ 1988; 296: 940-9
92. Seltzer HS. Drug-induced hypoglycemia: a review of 1418 cases. Endocrinol Metab Clin North Am 1989; 18: 163-83
93. Johnson DG, Bressler R. New pharmacologic approaches. In: Rifkin H, Porte Jr 0, editors. Diabetes mellitus: theory and practice. New York: Elsevier, 1990: 887-95
94. Alberti KGMM, Gries FA. Management of non-insulin dependent diabetes mellitus in Europe: a consensus view. Diabet Med 1988; 5: 275-81
95. Asmal AC, Marble A. Oral hypoglycaemic agents: an update. Drugs 1984; 28: 62-7
96. Nathan OM, Roussell A, Godine JE. Glyburide or insulin for metabolic control in non-insulin-dependent diabetes mellitus: a randomized double-blind study. Ann Intern Med 1988; 108: 334-40
© Adis International Limited. All rights reserved.
433
97. Balodimos MC, Camerini-Davalos RA, Marble A. Nine years experience with tolbutamide in the treatment of diabetes. Metabolism 1966; 15: 957-70
98. Powell T, Howells L. Diabetes mellitus treated with chlorpropamide and tolbutamide: a four-year clinical study. Diabetes 1966; 15: 269-75
99. Berhhard H. Long-term observations of oral hypoglycemic agents in diabetes: the effect of carbutamide and tolbutamide. Diabetes 1965; 14: 59-70
100. Cervantes-Amezcua A, Naldjian S, Camerini-Davalos R, et al. Long-term use of chlorpropamide in diabetes. JAMA 1965; 193: 759-62
101. Shen SW, Bressler R. Clinical pharmacology of oral antidiabetic agents. N Engl J Med 1977; 296: 493-6, 787-93
102. Boyden T, Bressler R. Oral hypoglycemic agents. Adv Intern Med 1979; 24: 53-70
103. Singer DL, Hurwitz D. Long term experience with sulfonylureas and placebo. N Engl J Med 1967; 277: 450-6
104. Turner RC, Mann JI, leeton G, et al. UK prospective study of therapies of maturity-onset diabetes: I. Effect of diet, sulphonylurea, insulin or biguanide therapy on fasting plasma glucose and body weight over one year. Diabetologia 1983; 24: 404-11
105. Turner RC, Mann JI , Oakes S, et al. UK Prospective Diabetes Study II. Reduction in HbAlc with basal insulin supplement sulfonylurea or biguanide therapy in maturity-onset diabetes. Diabetes 1985; 34: 793-8
106. Muller R, Bauer G, Schroder R, et al. Summary report of clinical investigation of the oral antidiabetic drug HB 419 (glibenclamide). Horm Metab Res 1969; I Suppl.: 88-92
107. Pontiroli AE, Calderara A, Pozza G. Secondary failure of oral hypoglycaemic agents: frequency, possible causes and management. Diabetes Metab Rev 1994; 10: 31-43
108. Turner RC, Holman RR, Matthews DR. Sulfonylurea failure and inadequacy. In: Cameron 0, Colagiuri S, Heding L, et aI. , editors. Non-insulin dependent diabetes mellitus. Hong Kong: Excerpta Medica, 1989: 52-5
109. Yki-Jiirvinen H, Helve E, Koivisto VA. Hyperglycemia decreases glucose uptake in type I diabetes. Diabetes 1987; 36: 892-6
110. Garvey WT, Olefsy JM, Griffin J, et al. The effect of insulin treatment on insulin secretion and insulin action in type II diabetes mellitus. Diabetes 1985; 34: 222-34
III. Rossetti L, Smith 0, Shulman GI , et al. Correction ofhyperglycemia with phlorizin normalizes tissue sensitivity to insulin in diabetic rats. J Clin Invest 1987; 79: 1510-5
112. UK Prospective Diabetes Group. Perspectives in diabetes: UK Prospective Diabetes Study 16. Overview of 6 years ' therapy of type II diabetes: a progressive disease. Diabetes 1995; 44: 1249-58
113. Turner R, Cull C, Holman R. United Kingdom prospective diabetes study 17: a 9-year update of a randomized, controlled trial on the effect of improved metabolic control on complications in non-insulin dependent diabetes mellitus. Ann Intern Med 1996; 124 (I): 136-45
114. Holmes B, Heel RC, Brogden RN, et al. Gliclazide: a preliminary review of its pharmacodynamic properties and therapeutic efficacy in diabetes mellitus. Drugs 1984; 27: 301-27
115. O'Donovan CJ. Analysis of long-term experience with tolbutamide (orinase) in the management of diabetes. Curr Ther Res 1959; I: 69-87
116. Weissman PN, Shenkman L, Gregerman RI. Chlorpropamide hyponatremia: drug-induced inappropriate antidiuretic hormone activity. N Engl J Med 1971; 284: 65-71
Drugs & Aging 1996 Dec; 9 (6)

434
117. Kadowaki T, Hagura R, Kajinuma H, et al. Chlorpropamide-induced hyponatremia: incidence and risk factors. Diabetes Care 1983; 6: 468-71
118. Moses AM, Numann P, Miller M. Mechanism of chlorpropamide-induced antidiuresis in man: evidence for release of ADH and enhancement of peripheral action . Metabolism 1973; 22: 59-66
119. Kadowaki T, Hagura R, Kajin H, et al. Chlorpropamide-induced hyponatremia: incidence and risk factors . Diabetes Care 1983; 6: 468-71
120. Jerntorp P, Almer LO, Ohlin H, et al. Plasma chlorpropamide: a critical factor in chlorpropamide-alcohol flush. Eur J Clin Pharmacol 1983; 24 (2): 237-42
121. Jennings AM, Wilson RM, Ward JD. Symptomatic hypoglycemia in NIDDM patients treated with oral hypoglycemic agents. Diabetes Care 1989; 12: 203-8
122. Berger W, Caduff F, Pasquel M, et al. Die relativ Haufigkeit der schweren Sulfonylharnstoff - Hypoglykamie in den letzen 25 Jahren in der Schweiz. Schweiz Med Wochenschr 1986; 116: 145-51
123. Asplund K, Wiholm B-E, Lithner F. Glibenclamide-associated hypoglycaemia: a report on 57 cases. Diabetologia 1983; 24: 412-7
124. Berger W. Incidence of severe side effects during therapy with sulfonylureas and biguanides. Horm Metab Res 1985; 17 Suppl. 15: 111-5
125. Pearson JG, Antal EJ, Raehl CL, et al. Pharmacokinetic disposition of 14C-glyburide in patients with varying renal function. Clin Pharmacol Ther 1986; 39: 318-24
126. Paice BJ, Paterson KR, Lawson DH. Undesired effects of the sulfonylurea drugs. Adverse Drug React Acute Poisoning Rev 1985; I: 23-36
127. University Group Diabetes Program. A study of the effects of hypoglycemic agents on vascular complications in patients with adult-onset diabetes: mortality results. Diabetes 1970; 19 Suppl. 2: 785-830
128. Biometric Society. Report of committee for assessment of biometric agents of controlled trials of hypoglycemic agents. JAM A 1975; 231: 583-608
129. Kilo C, Miller JP, Williamson JR. The crux of UGDP: spurious results and biologically inappropriate data analysis. Diabetologia 1980; 18: 179-85
130. Feinstein AR. How good is statistical evidence against oral hypoglycemic agents? Adv Intern Med 1979; 24: 71-95
131. American Diabetes Association. Policy statement: UGD controversy. Diabetes 1979; 28: 168-70
132. Logie AW, Galloway DG, Petrie Jc. Drug interactions and longterm anti-diabetic therapy. Br J Clin Pharmacol 1976; 3: 1027-32
133. Hansen M, Christensen LK. Drug interactions with oral sulphonylurea hypoglycaemic drugs. Drugs 1977; 13: 24-34
134. Bressler P, DeFronzo RA. Drugs and diabetes. Diabetes Rev 1994; 2: 53-84
135. Balant L. Clinical pharmacokinetics of sulfonylurea hypoglycemic drugs. Clin Pharmacokinet 1981 ; 6: 215-41
136. Jackson WPU. Sulphonylureas in the management of human diabetes. In: Campbell GD, editor. Oral hypoglycemic agents: pharmacology and therapeutics. New York: Academic Press, 1969: 137-92
137. Rojdmark S, Andersson DEH. Influence of verapamil on human glucose tolerance. Am J Cardiol 1986; 57: 39D-43D
138. Dey NG, Castleden CM, Ward J, et al. The effect of cimetidine on tolbutamide kinetics. Br J Clin Pharmacol 1983; 16: 438-40
© Adis International Limited. All rights reserved.
Bressler & Johnson
139. Charles S, Ketelslegers JM, Buysschaert M, et al. Hyperglycemic effect of nifedipine. BMJ 1981; 283: 19-20
140. Jackson JE. Sulfonylurea hypoglycemic agents. Drug Ther 1990; 20: 39-53
141. Lebovitz HE, Melander A. Sulfonylureas: basic and clinical aspects. In: Alberti KGMM , DeFronzo RA, Keen H, et aI. , editors. International textbook of diabetes mellitus. London: Wiley Bros, 1992: 745-72
142. Scheen AJ , Lefebvre PJ. Insulin versus insulin plus sulfonylureas in type 2 diabetic patients with secondary failure to sulfonylureas. Diabetes Res Clin Pract 1989; 6 (4): S33-43
143. Groop LC, Groop P-H, Stenman S. Combined insulin-sulfonylurea therapy in treatment ofNIDDM. Diabetes Care 1990; 13 Suppl. 3: 47-52
144. Lebovitz HE, Pasmantier RM. Combination insulin sulfonylurea therapy. Diabetes Care 1990; 13: 667-75
145. Bailey TS, Mezitis NHE. Combination therapy with insulin and sulfonylureas for type II diabetes. Diabetes Care 1990; 13: 687-95
146. Peters AL, Davidson MB. Insulin plus a sulfonylurea agent for treating type 2 diabetes. Ann Intern Med 1991; 115: 45-53
147. Trischitta V, Italia S, Borzi V, et al. Low-dose bedtime NPH insulin in treatment of secondary failure to glyburide. Diabetes Care 1989; 12: 582-5
148. Del Prato S, Vigili de Kreutzenberg S, Riccio A, et al. Partial recovery of insulin secretion and action after combined insulin-sulfonylurea treatment in type 2 (non-insulin-dependent) diabetic patients with secondary failure to oral agents. Diabetologia 1990; 33: 688-95
149. Campbell P, Bolli G, Cryer P, et al. Pathogenesis of the 'dawn phenomenon ' in patients with insulin-dependent diabetes mellitus. N Engl J Med 1985; 312: 1473-9
150. Bohli G, Gerich J. The 'dawn phenomenon ' , a common occurrence in both non-insulin-dependent and insulin-dependent diabetes mellitus. N Engl J Med 1984; 31: 746-50
151 . Dimitriadis G, Vlachonikolis IG, Hatziagellaki E, et al. The 'dawn phenomenon' in patients with type II diabetes mellitus. Diabetes Nutr Metab 1988; I: 37-41
152. Riddle MC, Hart JS, Bouma DJ, et al. Efficacy of bedtime NPH insulin with daytime sulfonylurea for subpopulation of type II diabetic subjects. Diabetes Care 1989; 12: 623-9
153. Taskinen M-R, Sane T, Helve E, et al. Bedtime insulin for suppression of overnight free-fatty acid blood glucose and glucose production in NIDDM. Diabetes 1989; 38: 580-8
154. Clarke BF, Duncan UP. Combined metformin-chlorpropamide therapy in 108 diabetic sulphonylurea failures. Lancet 1965; I: 1248-51
155. Hermann LS. Biguanides and sulfonylureas as combination therapy in NIDDM. Diabetes Care 1990; 13 Suppl. 3: 37-41
156. Vigneri R, Goldfine 10. Role of metformin in treatment of diabetes mellitus. Diabetes Care 1987; 10: 118-22
157. Herman L, Schersten B, Bitzen PO, et al. Therapeutic comparison of metformin and sulfonylurea, alone and in various combinations. Diabetes Care 1994; 17: 1100-9
158. Dimitriadis G, Hatziagellaki E, Alexopoulos E, et al. Effects of a-glucosidase tolerance and timing of insulin administration in patients with type I diabetes mellitus. Diabetes Care 1991; 14: 393-8
159. Schnack E, Prager RJF, Winkler J, et al. Effects of an 8-week a-glucosidase inhibition on metabolic control , C peptide secretion, hepatic glucose output, and peripheral insulin sensitivity in poorly controlled type II diabetic patients. Diabetes Care 1989; 12: 537-43
Drugs & Aging 1996 Dec: 9 (6)

Oral Antidiabetics in the Elderly
160. Dunn CJ, Peters DH. Metformin: a review of its pharmacological properties and therapeutic use in diabetes mellitus. Drugs 1995; 49: 721-49
161. Bailey CJ. Metformin: an update. Gen Pharmacol 1993; 24: 1299-1309
162. Garber AJ. Metformin therapy for type II diabetes mellitus. Pharm Ther 1995; 20: 568-83
163. Chow MSS. Focus on metformin. Formulary 1995; 30: 383-7 164. DeFronzo RA, Goodman AM, the Multicenter Metformin Study
Group. Efficacy of metformin in patients with non-insulindependent diabetes mellitus. N Engl J Med 1995; 333: 541-9
165. Hermann LS, Melander A. Biguanides: basic aspects and clinical uses. In: Alberti KGMM, DeFronzo RA, Keen H, et aI., editors. International textbook of diabetes mellitus. New York: Wiley & Sons, 1994: 773-95
166. Sinori C. Franceschini G, Galli-Kienle M, et al. Disposition of metformin (N,N-dimethylbiguanide) in man. Clin Pharmacol Ther 1978; 24: 683-93
167. Pentikainen PJ. Bioavailability of metformin: comparison of solution, rapidly dissolving tablet, and three sustained release products. Int J Clin Pharmacol Ther Toxicol 1986; 24: 213-20
168. Pentikainen PJ, Neuvonen PJ, Penttila A. Pharmacokinetics of metformin after intravenous and oral administration to man. Eur J Clin Pharmacol 1979; 16: 195-202
169. Tucker GT, Casey C, Phillips PJ, et al. Metformin kinetics in healthy subjects and in patients with diabetes mellitus. Br J Clin Pharmacol 1981; 12: 235-46
170. Assan R, Heuclin C, Ganeval D, et al. Metformin-induced lactic acidosis in the presence of acute renal failure. Diabetologia 1977; 13: 211-7
171 . Hutchison SMW, Callerall JR. Metformin and lactic acidosis: a reminder. Br J Clin Pract 1987; 41: 673-4
172. Lucis OJ. The status of metformin in Canada. Can Med Assoc J 1983; 128: 24-6
173. Clarke BF, Duncan UP. Biguanide treatment in the management of insulin independent (maturity-onset) diabetes: clinical experience with metformin. Res Clin Forum 1979; I: 53-63
174. Phillips PJ, Scicchitano R, Clarkson AR, et al. Metformin associated lactic acidosis. Aust N Z J Med 1978; 8: 281-4
175. Lalau JD, Lacroix C, Compagnon P, et al. Role of metformin accumulation in metformin-associated lactic acidosis. Diabetes Care 1995; 18: 779-84
176. Wilcock C, Bailey CJ. Sites of metformin-stimulated glucose metabolism. Biochem Pharmacol 1990; 39: 1831-4
177. Bailey CJ, Wilcock C, Day C. Effect of metformin on glucose metabolism in the splanchnic bed. Br J Pharmacol 1992; 105: 1009-15
178. Campbell IW. Metformin and the sulphonylureas: the comparative risk. Horm Metab Res 1985; 15: 105- 11
179. Lalau JD, Andrejak M, Moniniere P, et al. Hemodialysis in the treatment of lactic acidosis in diabetics treated by metformin: a study of metformin elimination. Int J Clin Pharmacol Ther Toxicol 1989; 27: 285-8
180. Shenfield GM, Bhalla IP, Steel JM , et al. Metformin in the treatment of obese diabetics. Practitioner 1977; 219: 745-9
181. Clarke BF, Duncan LPJ. Comparison of chlorpropamide and metformin treatment on weight and blood-glucose response of uncontrolled obese diabetics. Lancet 1968; I: 123-6
182. Lim P, Khoo OT. Metformin compared with tolbutamide in the treatment of maturity-onset diabetes mellitus. Med J Aust 1970; I: 271-3
© Adis International Umited. All rights reserved.
435
183. Siitonen 0, Aro A, Hullunen JK, et al. Effect of discontinuation of biguanide therapy on metabolic control in maturity-onset diabetics. Lancet 1980; I: 217-20
184. Clarke BF, Campbell IW. Comparison of metformin and chlorpropamide in non-obese, maturity-onset diabetics uncontrolled by diet. BMJ 1977; 2: 1576-8
185. Hermann LS. Metabolic effects of metformin in relation to clinical effects and side effects: international congress symposium series: biguanide therapy today. J R Soc Med 1984; 48: 3-13
186. Doman TL, Heller SR, Peck GM, et al. Double-blind evaluation of efficacy and tolerability of metformin in NIDDM. Diabetes Care 1991; 14: 342-4
187. Elkeles RS. The effects of oral hypoglycemic drugs on serum lipids and lipoproteins in non-insulin-dependent diabetes (NIDDM). Diabete Metab 1991 ; 17: 197-200
188. Hermann LS, Bitzen PO, Kjellstrom T, et al. Comparative efficacy of metformin and glibenclamide in patients with non-insulin-dependent diabetes mellitus. Diabete Metab 1991; 17: 201-8
189. Hermann LS, Schersten B, Bitzen PO, et al. Therapeutic comparison of metformin and sulfonylurea, alone and in various combinations: a double-blind controlled study. Diabetes Care 1994; 17: 1100-9
190. Noury J, Nandeuil A. Comparative three-month study of the efficacies of metformin and gliclazide in the treatment of NIDDM. Diabete Metab 1991 ; 17: 209-12
191 . Clarke BF, Marshall A, McGill RC, et al. A 3-year evaluation of combined sulphonylurea-metformin treatment in 200 diabetic ketoacidosis resistant sulphonylurea failures. In: Butterfield WJH, Van Westering W, editors. Tolbutamide . . . after ten years. New York: Excerpta Medica, 1967: 312-20
192. Nattrass M, Hinks L, Smythe P, et al. Metabolic effects of combined sulphonylurea and metformin therapy in maturity-onset diabetics . Horm Metab Res 1979; II: 332-7
193. Capretti L, Bonora E, Coscelli C, et al. Combined sulphonylurea-biguanide therapy for non-insulin-dependent diabetics: metabolic effects of glibenclamide and metformin or phenformin in newly diagnosed obese patients. Curr Med Res Opin 1982; 7: 677-83
194. Reaven GM, Johnston P, Hollenbeck CB, et al. Combined metformin-sulfonylurea treatment of patients with noninsulin-dependent diabetes in fair to poor glycemic control. J Clin Endocrinol Metab 1992; 74: 1020-6
195. Haupt E, Knick B, Koschinsky T, et al. Oral antidiabetic combination therapy with sulfonylureas and metformin. Diabete Metab 1991; 17: 224-31
196. Trischitta V, Italia S, Mazzarino S, et al. Comparison of combined therapies in treatment of secondary failure to glyburide. Diabetes Care 1992; 15: 539-42
197. Hother-Nielsen 0 , Schmitz 0, Andersen PH, et al. Metformin improves peripheral but not hepatic insulin action in obese patients with type II diabetes. Acta Endocrinol 1989; 120: 257-65
198. Klip A, Leiter LA. Cellular mechanism of action of metformin. Diabetes Care 1990; 13: 696-704
199. DeFronzo RA, Barzilai N, Simonsen DC. Mechanism of metformin action in obese and lean non-insulin-dependent diabetic subjects. J C1in Endocrinol Metab 1991; 73: 1294-301
200. Stumvoll M, Nurjhan N, Perriello G, et al. Metabolic effects of metformin in non-insulin-dependent diabetes mellitus. N Engl J Med 1995; 333: 550-4
201. Bailey CJ. Biguanides and NIDDM. Diabetes Care 1992; 15: 755-72
Drugs & Aging 1996 Dec: 9 (6)

436
202. Nosadini R, Avogaro A, Trevisian R, et al. Effect of metformin on insulin-stimulated glucose turnover and insulin binding to receptors in type II diabetes. Diabetes Care 1987; 10: 62-7
203. Jeppesen J, Zhou MY, Chen YDI, et al. Effect of metformin on postprandial lipemia in patients with fairly to poorly controlled NIDDM. Diabetes Care 1994; 17: 1093-8
204. Sirtori CR, Weber G , Losi M, et al. Metformin and lipid metabolism. Res Clin Forum 1979; I: 117-22
205. Wu MS, Johnston P, Sheu WHH, et al. Effect of metformin on carbohydrate and lipoprotein metabolism in NIDDM patients. Diabetes Care 1990; 13: 1-8
206. Collier A, Watson HH, Patrick AW, et al. Effect of glycaemic control, metformin and gliclazide on platelet density and aggregability in recently diagnosed type 2 (non-insulin-dependent) diabetic patients. Diabete Metab 1989; 15: 420-5
207. Genuth S. Management of the adult onset diabetic with sulfonylurea drug failure. Endocrinol Metab Clin North Am 1992; 21: 351-71
208. Howard BY, Howard WJ. Dyslipidemia in non-insulin-dependent diabetes mellitus. Endocr Rev 1994; 15: 263-74
209. Hermann LS. Biguanides and sulfonylureas as combination therapy in NIDDM. Diabetes Care 1990; 13 Suppl. 3: 37-41
210. Josephkutty S, Potter JM. Comparison of tolbutamide and metformin in elderly diabetic patients. Diabetic Med 1990; 7: 510-4
211. Stowers JM, Borthwick LJ. Oral hypoglycaemic drugs: clinical pharmacology and therapeutic use. Drugs 1977; 14: 41-7
212. Menzies DG, Campbell IW, McBain A, et al. Metformin efficacy and tolerance in obese non-insulin dependent diabetics: a comparison of two dosage schedules. Curr Med Res Opin 1989; II: 273-8
213. Dandona P, Fonseca Y, Mier A, et al. Diarrhea and metformin in a diabetic clinic. Diabetes Care 1983; 6: 472-4
214. Pagano G, Tagliaferro Y, Carta Q, et al. Metformin reduces insulin requirement in type I (insulin-dependent) diabetes. Diabetologia 1983; 24: 351-4
215. Berchtold P, Dahlquist A, Gustafson A, etal. Effects ofabiguanide (metformin) on vitamin BI2 and folic acid absorption and intestinal enzyme activities. Scand J Gastroenterol 1971; 6: 751-4
216. Sterne J, Junien JL. Metformin: pharmacological mechanisms of the antidiabetic and anti lipid effects and clinical consequences: international congress symposium series: biguanide therapy today. J R Soc Med 1984; 48: 3-13
217. Stein PP, Black HR. Treatment of hypertension in patients with diabetes mellitus. Diabetes Care 1991; 14 (6): 425-48
218. Co1ca JR, Morton DR: antihyperglycaemic thiazolidinediones: ciglitazone and its analogues. In: Bailey CJ, Flatt PR, editors. New antidiabetic drugs. London: Smith-GordonlNishimura, 1990: 255-61
219. Fujita T, Sugiyama Y, Taketomi S, et al. Reduction of insulin resistance in obese and/or diabetic animals by 5-[4-(methy1cyclohexylmethoxy) benzyllthiazolidine-2 (ADD-3878, U-63 ,287 , ciglitalOne), a new antidiabetic agent. Diabetes 1983; 32: 804-10
220. Chang A Y, Wyse BM, Gilchrist BJ. CiglitalOne, a new hypoglycemic agent: I. Studies in ob/ob and db/db mice, diabetic Chinese hamsters, and normal and streptozotocin-diabetic rats. Diabetes 1983; 32: 830-8
221. Sugiyama Y, Taketomi S, Shimura Y, et al. Effects of pioglitazone on glucose and lipid metabolism in Wistar fatty rats. Arzneimittelforschung 1990; 40: 263-7
© Adis International Umited. All rights reserved.
Bressler & Johnson
222. Suter SL, Nolan JJ, Wallace P, et al. Metabolic effects of new and hypoglycemic agent CS-045 in NIDDM subjects. Diabetes Care 1992; 15: 193-203
223. Fujiwara T, Yoshioka S, Yoshioka T, et al. Characterization of new oral antidiabetic agent CS-045: studies in KK and ob/ob mice and Zucker fatty rats. Diabetes 1988; 37: 1549-58
224. Ciarladi TP, Gilmore A, Olefsky J, et al. 111 vitro studies on the action of CS-045, a new antidiabetic agent. Metabolism 1990; 39: 1056-62
225. Iwamoto Y, Kuzuya T, Matsuda A, et al. Effects of new oral antidiabetic agent CS-045 on glucose tolerance and insulin secretion in patients with NIDDM. Diabetes Care 1991 ; 14: 1083-6
226. Sugiyama Y, Shimura Y, Ikeda H. Effects of pioglitazone on hepatic and peripheral insulin-resistance in Wistar fatty rats. Arzneimittelforschung 1990; 40: 436-40
227. Chang AY, Gilchrist BJ, Wyse BM. CiglitalOne, a new hypoglycemic agent: 3. Effect on glucose disposal and gluconeogenesis ill vivo in C57BL/6J-ob/ob and +I? mice. Diabetologia 1983; 25: 514-20
228. Shargill NS, Tatoyan A, Fukushima M, et al. Effect of ciglitazone on glucose uptake and insulin sensitivity in skeletal muscle of the obese (ob/ob) mouse: distinct insulin and glucocorticoid effects. Metabolism 1986; 35: 64-70
229. Steiner KE, Lien EL. Hypoglycemic agents which do not release insulin. Prog Med Chem 198; 24: 209-48
230. Kuehnle HF. New therapeutic agents for the treatment of NIDDM . ExpClin Endocrinol Diabetes 1995; 104: 93-101
231. Hofmann CA, Colca JR. New oral thiazolidinedione antidiabetic agents act as insulin sensitizers. Diabetes Care 1992; 15: 1075-8
232. Kosaka K, Kuzuya T, Akanuma Y, et al. Clinical evaluation of a new oral hypoglycemic drug, CS-0045, in patients with noninsulin-dependent diabetes poorly controlled by sulfonylureas - a double blind placebo controlled study. J Clin Ther Med 1993; 9 Suppl. 3: 95-126
233. Nolan JJ, Ludvik B, Beerdsen P, et al. Improvement in glucose tolerance and insulin resistance in obese subjects treated with troglitazone. N Engl J Med 1994; 331: 1188-93
234. Jenkins DJA, Wolever TMS, Vuksan Y, et al. Nibbling versus gorging: metabolic advantages of increased meal frequency. N Engl J Med 1989; 321: 929-34
235. Jenkins DJA, Wolever TMS, Ocana AM, et al. Metabolic effects of reducing rate of glucose ingestion by single bolus versus continuous sipping. Diabetes 1990; 39: 775-81
236. Taylor RH. Alpha-glucosidase inhibitors. In: Bailey CJ, Flatt PR, editors. New antidiabetic drugs. London: Smith-Gordon/Nishimura, 1990: 119-32
237. Schmidt DD, Frommer W, Junge B, et al. New complex oligosaccharides of microbial origin . Naturwissenschaften 1977; 64: 535-6
238. Puis W, Keup U, Krause HP, et al. Glucosidase inhibition: a new approach to the treatment of diabetes, obesity, and hyperlipoproteinaemia. Naturwissenschaften 1977; 64: 536-7
239. Caspary WF. Sucrose malabsorption in man after ingestion of a-glucosidehydrolase inhibitor. Lancet 1978; I: 1231-3
240. Hillebrand I, Boehme K, Frank G, et al. The effects of the -glucosidase inhibitor BAY g 5421 (acarbose) on meal-stimulated elevations of circulating glucose, insulin, and triglyceride levels in man. Res Exp Med (Berl) 1979; 175: 81-6
241. Hillebrand I, Boehme K, Frank G, et al. The effects of the uglucosidase inhibitor BAY g 5421 (acarbose) on postprandial blood glucose, serum insulin, and triglyceride levels: dose-
Drugs & Aging 1996 Dec; 9 (6)

Oral Antidiabetics in the Elderly
time-response relationships in man. Res Exp Med (Berl) 1979; 175: 87-94
242. Joubert PH, Venter HL, Foukaridis GN. The effect of miglitol and acarbose after an oral glucose load: a novel hypoglycaemic mechanism? Br J Clin Pharmacol 1990; 30: 391-6
243. Schnack C, Prager RJF, Winkler J, et al. Effects of 8-week a-glucosidase inhibition on metabolic control, C-peptide secretion, hepatic glucose output, and peripheral insulin sensitivity in poorly controlled type II diabetic patients. Diabetes Care 1989; 12: 537-43
244. Hanefeld M, Fischer S, Schulze J, et al. Therapeutic potential of acarbose as first-line drug in NIDDM insufficiently treated with diet alone. Diabetes Care 1991 ; 14: 732-7
245. Vierhapper H, Bratusch-Marrain A, Waldausl W. a-Glucoside hydrolase inhibition in diabetes [letter]. Lancet 1978; II: 1386
246. Walton RJ , Sherif IT, Noy GA, et al. Improved metabolic profiles in insulin-treated diabetic patients given an alphaglucosidehydrolase inhibitor. BMJ 1979; I: 220-1
247. Requejo F, Uttenthal LO, Bloom SR. Effects of alphaglucosidase inhibition and viscous fibre on diabetic control and postprandial gut hormone responses. Diabet Med 1990; 7: 515-20
248. Tuomilehto J. Acarbose monotherapy in the treatment of noninsulin dependent diabetes mellitus: a review. In: Creutzfeldt W, editor. Acarbose for the treatment of diabetes mellitus: 2nd
© Adis International Limited. All rights reserved.
437
International Symposium on Acarbose. Berlin: SpringerVerlag, 1988: 104-18
249. Lebovitz HE. Oral antidiabetic agents: the emergence of a glucosidase inhibitors. Drugs 1992; 44 Suppl. 3: 21-8
250. PuIs W, Bischoff H. The pharmacological rationale of diabetes mellitus therapy with acarbose . In: Creutzfeldt W, editor. Acarbose for the treatment of diabetes mdlitus: 2nd International Symposium on Acarbose . Berlin: Springer-Verlag, 1988: 29-38
251. Jenkens DJA, Taylor RH, Nineham R, et al. Combined use of guar and acarbose in reduction of postprandial glycaemia. Lancet 1979; II: 924-7
252. Sachse G. Acarbose in non-insulin-dependent diabetes - Iongterm studies in combination with oral agents. In: Creutzfeldt W, editor. Acarbose for the treatment of diabetes mellitus: 2nd International Symposium on Acarbose. Berlin: Springer-Verlag, 1988: 92-103
Correspondence and reprints: Dr Rubin Bressler, Department of Medicine, Arizona Health Sciences Center, University of Arizona, PO Box 245031, Tucson, AZ 85724-5031, USA.
Drugs & Aging 1996 Dec: 9 (6)