Embed Size (px)
Citation preview
“Disaster plans do work”
OR staffs respond to Hyatt casualties
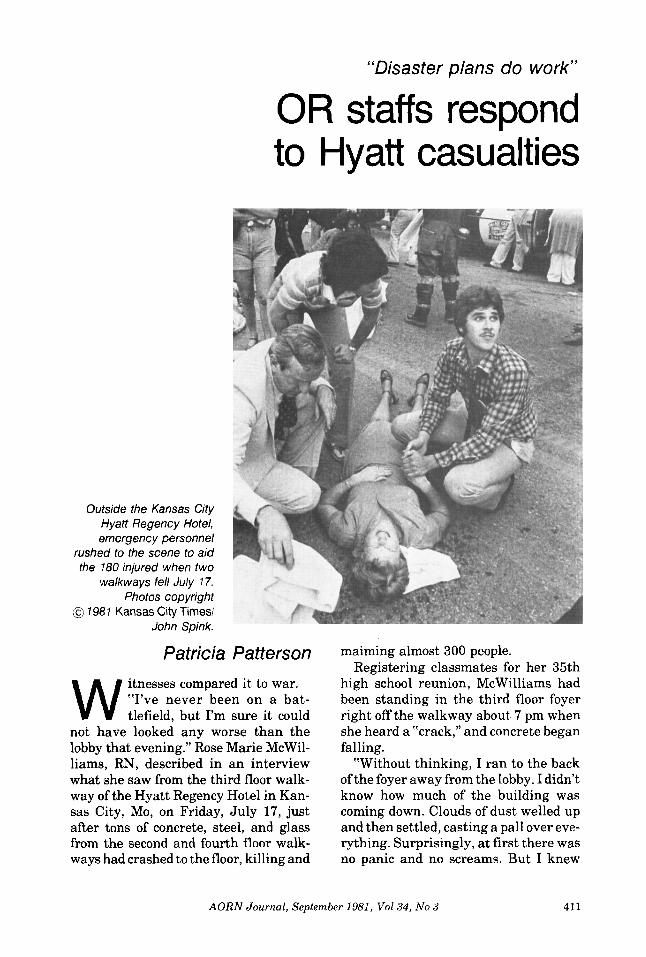
Outside the Kansas City Hyatt Regency Hotel, emergency personnel
rushed to the scene to aid the 180 injured when two
walkways fell July 7 7. Photos copyright
@ 1987 Kansas City Times/ John Spink.
Patricia Patterson
W itnesses compared it to war. “I’ve never been on a bat- tlefield, but I’m sure it could
not have looked any worse than the lobby that evening.” Rose Marie McWil- liams, RN, described in an interview what she saw from the third floor walk- way of the Hyatt Regency Hotel in Kan- sas City, Mo, on Friday, July 17, just after tons of concrete, steel, and glass from the second and fourth floor walk- ways had crashed to the floor, killing and
maiming almost 300 people. Registering classmates for her 35th
high school reunion, McWilliams had been standing in the third floor foyer right off the walkway about 7 pm when she heard a “crack,” and concrete began falling.
“Without thinking, I ran to the back of the foyer away from the lobby. I didn’t know how much of the building was coming down. Clouds of dust welled up and then settled, casting a pall over eve- rything. Surprisingly, at first there was no panic and no screams. But I knew
AORN Journal, September 1981, Vol34, No 3 411
what I would see as I looked over the balcony .”
What she saw was total devastation that would disturb her sleep despite more than 25 years of operating room experience. “The dismemberments. There were arms. There were legs. The groans and cries.” From the amount of blood on the floor within a few minutes, McWilliams sensed the magnitude of human destruction.
A Kansas City native, McWilliams is associate director of nursing service in charge of the operating room, recovery room, and staff development at Univer- sity Hospital of the University of Col- orado Health Sciences Center, Denver.
Gas was escaping, and water gushed from a broken main. Unable to get down the stairs to the second floor, she urged others to get moving, and they left by the third floor terrace. McWilliams worked her way to the front of the build- ing, where she went to work alongside emergency personnel, putting pressure on wounds and calming frightened people.
To her “it seemed like an eternity” before help began arriving, but within a few minutes, the city’s disaster plan had swung into action.
In one of six “mobile response units” in the emergency radio network, Ron Norman of the Kansas City Area Hospi-
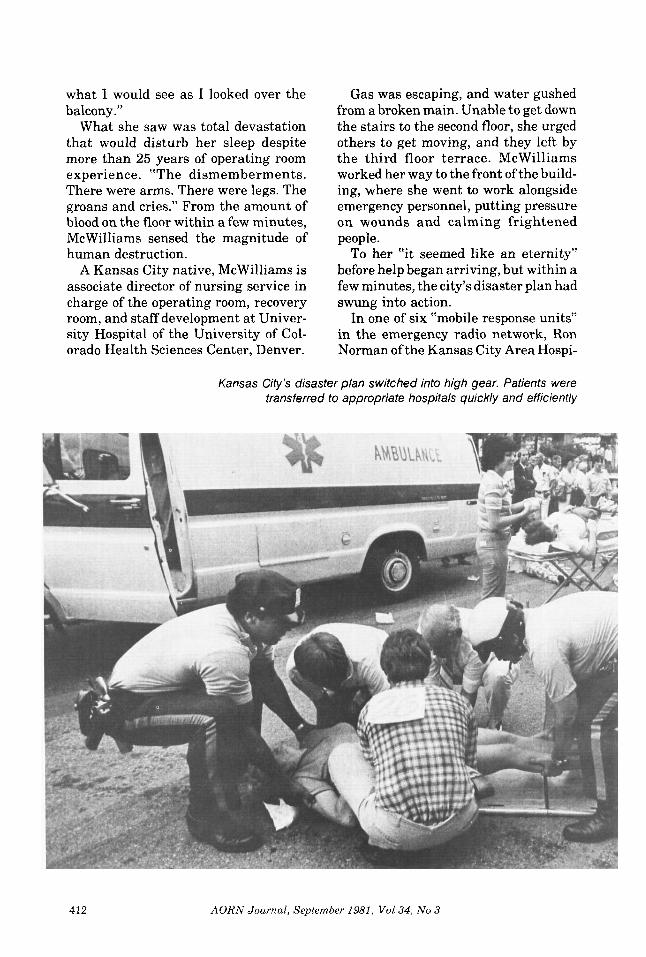
Kansas City’s disaster plan switched into high gear. Patients were transferred to appropriate hospitals quickly and efficiently
412 AORN Journal, September 1981, Vol34, No 3

tal Association (KCAHA) was on his way to the scene. He would spend the next ten hours working with triage of- ficers sending victims to area hospitals.
In hospitals all over the city, operat- ing room nurses were showing up with- out being called. Closest to the hotel, Truman Medical Center, St Mary’s Hospital, Trinity Lutheran Hospital, and St Luke’s Hospital, would receive most of the critically injured patients. They would find that the stress of re- sponding to the disaster did not end that night but stretched into the next two weeks as severely injured patients con- tinued coming to the OR for further surgery.
The first concern was getting victims to hospitals best suited to care for them without overloading any institution.
Leadership and communication are keys to this operation, and it appears that Kansas City had both. KCAHA and 14 major hospitals are connected in the HEAR (Hospital Emergency Ad- ministrative Radio) system. Baptist Memorial Hospital is the hub, responsi- ble for issuing alerts, monitoring the network, and disciplining use of the air waves.
Baptist received first word of the ac- cident within five minutes, but had re- ports of only about 35 minor injuries. Dispatchers issued a low-level alert and began collecting information about hospital “assets”-their current capa- bility to handle disaster victims.
Ten minutes later, Baptist got word of mass casualties. A call went out to the “mobile response units”-officials with radios in their private cars. Closest to the Hyatt, Norman headed for the hotel and checked in at triage. Meanwhile, Baptist switched to its highest alert. This implemented the city’s disaster plan, and the center inventoried all hospitals for their capabilities.
“We were almost astonished a t how well the system worked,” Norman said in a phone interview five days later. “Disaster planners say that simplicity is the key, and that was verified in this case.”
“The plan relied on flexibility and communication-beyond that you have to play it by ear. Every disaster is unique. You have to know what capabil- ities the system has and adjust to the situation,” he observed.
“The four hospitals got most of the victims because they were reporting the ability t o handle critical patients.” He said that medical personnel did not at- tempt to stabilize patients at the scene but concentrated on transporting them to the appropriate hospital as quickly as possible.
The injured came in three waves. Pa- tients transported in the first hour were
AORN Journal, September 1981, V o l 3 4 , No 3 413

“They heard the news at restaurants, at home, or wherever they were and simply came in without being called. ”
those not trapped by wreckage who could be easily removed. In the second and third hours, victims were dug from under the top layer of debris. After another three hours, the lowest section of the second floor bridge was moved, and the last group of victims was found.
The ratio of deaths to injuries did not fit the expected disaster pattern, Nor- man said. “I’m told you can expect 15% to 20% deaths. We had about 40%. The only higher death rate would probably be from a plane crash.” About 180 were hurt, and 11 1 had died within the first five days.
“Injuries we saw go beyond the term trauma-bodies crushed, mangled, and smashed flat. They did an amputation with a chain saw to extricate someone. I was in Vietnam and never saw such butchery in such a concentrated space,” Norman said.
Truman Medical Center, a trauma center, is within walking distance of the Hyatt. The dead and the most critically injured patients were sent there. Re- sponding to the immediate disaster was not a problem for Karen Lundell, assis- tant director of nursing/OR, and her staff in the eight-room OR suite. Their emergency plan came off “without a hitch,” she said, better in fact than the drill they had had two weeks before.
The evening call crew was already there and just finishing a case when they got word of the accident. The first call for more staff went out a t 7:20 pm, and the first staff member arrived by
7:40 pm, even before s t reets were blocked around the Hyatt and the hospi- tal. By 9 pm, 67% of the staff was on hand, a “fantastic response,” Lundell said. “They heard the news at restau- rants, at home, or wherever they were and simply came in without being call- ed.”
Excellent triage a t the scene was a considerable help, too. “We did not re- ceive a massive number of patients,” she related. “We admitted only 18, but none was in less than serious condition. They didn’t send us the minor lacera- tions. Those went to hospitals farther away . ”
Due to the hospital’s trauma center designation, “Our crew is used to mobilizing, and they are used to dealing with critically injured patients, al- though not in this magnitude,” she said. “The staff did not need much direction, which was tremendous for me and a real credit to them. They were really calm.”
Six procedures were done that night. Almost all patients had orthopedic oper- ations. There were also a thoracotomy, exploratory laparotomies for repair of a transected ureter and repair of a left renal vein, drainage of a right iliac hematoma, fracture debridements, and fasciotomies. Later that night, one pa- tient came back in acute renal failure to have a shunt put in. In short, “Nothing very exotic,” Lundell said.
“The aftermath is what I didn’t an- ticipate.” Throughout the next week, four or five Hyatt victims came to surgery each day. These were the less critical orthopedic cases and patients who needed to be stabilized before they could have surgery. Three Harrington rod procedures were scheduled for the week after that.
‘‘It’s not so much what you do that night. You just get through and do the most critical cases,” Lundell com- mented. “The problem is what happens to your schedule for the rest of the week.
414 AORN Journal, September 1981, Vol34, No 3
You need t o anticipate, to look at how you can provide for staffing and how you can expand your regular schedule to handle these extra patients.”
On a case cart system, the depart- ment did not have instrument prob- lems. Many carts are available, and they always have a room ready to go, with only sterile supplies to open.
You also have to be prepared to let instruments go out of the department, she discovered. Skull tongs went to the ER and were applied there. Amputation trays were sent to orthopedic surgeons at the Hyatt who were amputating limbs to extricate patients from the wreckage.
Another thing a disaster plan cannot anticipate is the emotional impact of the incident on the staff and community. Even a veteran staff and the strongest nurses are stunned by the loss and grief. “We kept wondering if the next patient they brought up would be someone we knew,” Lundell said. “We’re all ex- hausted, and I’m sure a lot of it is emo- tional strain.”
One on-call nurse was there all Fri- day night and into Saturday. She was back Monday and Tuesday. “She is one of my strongest nurses, so she was as- signed to the heavy cases,” Lundell explained. “Finally, she came in Tues- day afternoon and said, ‘Please assign me to some lighter cases. I can’t handle another victim.’ This is something you need to keep in mind, too, in planning.”
With morgue facilities, Truman also received the dead. Social workers and medical records staff had the most draining experience, Lundell said, find- ing children of parents who had been killed and assisting families who had to identify badly mutilated bodies. Police took photographs to spare relatives as much as possible from having to view the victims. The hospital is also provid- ing staff with emotional assistance as part of its postdisaster evaluation.
At St Mary’s Hospital, also a few blocks from the hotel, OR supervisor Dale Keith, RN, and her staff were re- ceiving patients with heavy orthopedic trauma. As a t Truman and Trinity Lutheran, many nurses came to the hospital Friday night without being called.
Keith opened four of the eight ORs that evening and had enough staff to open one more. Understaffed for the last four or five months, Keith was also working with nurses new to the staff. Half of the RNs had been in the OR four
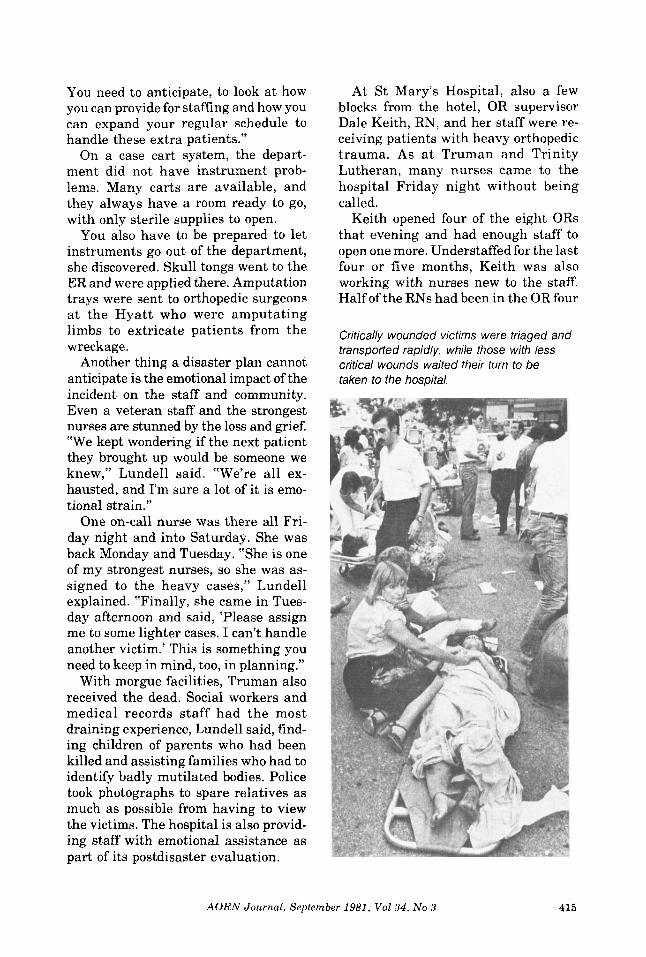
Critically wounded victims were triaged and transported rapidly, while those with less critical wounds waited their turn to be taken to the hospital.
AORN Journal, September 1981, Vol34 , No 3 415
months or less. “The OR and recovery room staffs did
an excellent job,” she added. “I’m really proud of them.”
Ten patients came to surgery that night and the next day. The heavy schedule of disaster victims continued into the next week and the following week.
“This has been my hardest week ever in the OR,” Keith said seven days after the tragedy. “We’re doing surgery on at least two disaster victims a day.” Proce- dures included debridements, dressing changes, pinnings, and insertion of Hoffmann devices.
“It’s hard to get up each day to see more injuries,” she said. “The staff is emotionally and physically fatigued.” Earlier in the week, a man was brought to surgery the same morning his wife was being buried. “That’s difficult for the staff to handle.” A hospital task force was planning emotional support for personnel in the OR, the orthopedic floor, and the intensive care units.
Scheduling the complicated fracture cases was frustrating. Inevitably, the procedures took longer than allotted as surgeons ran into unanticipated prob- lems. Keeping up with supplies was another challenge. “My chief concern on Monday was running an orthopedic and suture inventory, although normally I wouldn’t think of doing it then,” Keith said. (That was the only day that week that no disaster cases came to the OR.) Salesmen from orthopedic companies “have really been super,” she added. One was on hand all night Friday and others expedited orders.
Close cooperation between operating room and recovery room staffs was another morale booster. Recovery room nurses backed up the OR staff by assist- ing with blood and arterial lines. Then when patients went to recovery, OR nurses helped out there.
In general, Keith found that the hos-
pital’s disaster plan worked well. One change she would make is to have more personnel for transporting and lifting patients and holding extremities. Not enough male staff were available to as- sist with these tasks, so Keith and the head nurse brought their husbands in to act as orderlies.
“Disaster plans do work,” was Janett Propst’s assessment. “Victims were triaged so well that no hospital got over- crowded.” She is associate director of nurses and director of the OR and recov- ery room at Trinity Lutheran Hospital, where 17 patients were sent. Five had surgery, primarily orthopedic proce- dures.
Propst was attending a meeting in Columbia, Mo, more than two hours’ drive from Kansas City, when she heard of the disaster. “I called in to see if I should come back and found everything under control. The crew was there and functioning well.” She had praise for the “giving attitude” of the whole staff-OR nurses who showed up without being called, a recovery room nurse who was at the Hyatt and stayed there to assist, housekeepers who transported patients from triage and stayed late into the night to clean operating rooms.
She found the response from the community heartwarming as well. “Within minutes, the blood bank was inundated with volunteers, and they were drawing blood all weekend,” she said. “They not only met the demand from the accident but kept the blood bank from having to deplete its supply for routine cases.”
“Operating room personnel in the city responded beautifully,” McWilliams commented after visiting OR nurses at St Mary’s early in the week after the accident. “The nurses talked about how it brought them together. Disasters, it’s sad to say, unite people at all levels- physicians, anesthesia personnel, nurses.”
416 AORN Journal, September 1981, Val 34, No 3