Embed Size (px)
Citation preview
OPTOMETRY VISION SCIENCE
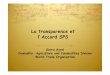
Eyeball
Refractive system
the basic conditions of clear vision:
• 1. transparence
• 2. Imaging on fovea
• 3. Intact visual pathway
• Refractive system• Cornea • Aqueous humor• Lens • Vitreous
Refraction : the process of imaging on retina that lights enter eye through refractive system
Refractive system
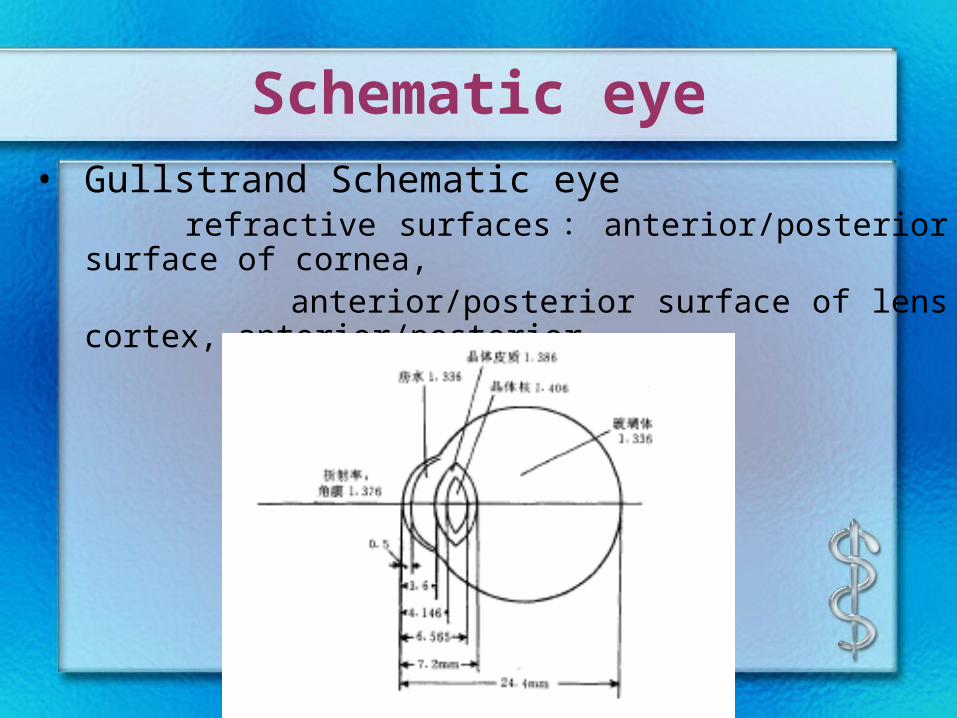
Schematic eye• Gullstrand Schematic eye refractive surfaces : anterior/posterior surface of cornea, anterior/posterior surface of lens cortex, anterior/posterior surface of lens nucleus
Refractive system
• Gullstrand Refractive system
– Total refractive power of eye : 58.64D ,
on maximum accommodation : 70.57D
– Refractive power of cornea : 43.05D
– Refractive power of lens : 19.11D
– Axis of eye : 24mm
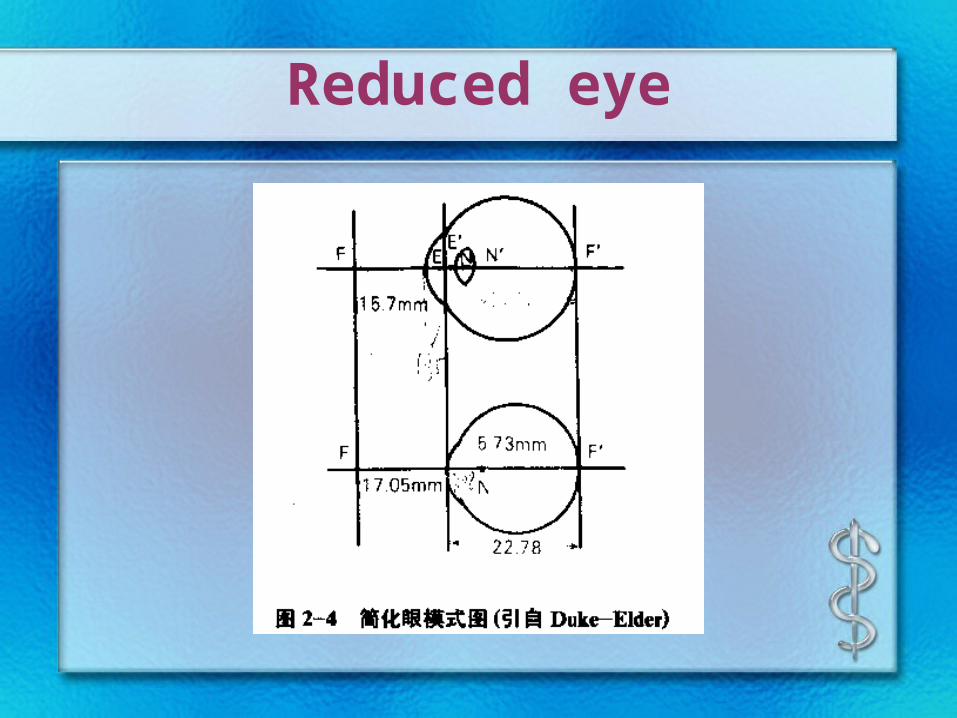
Reduced eye
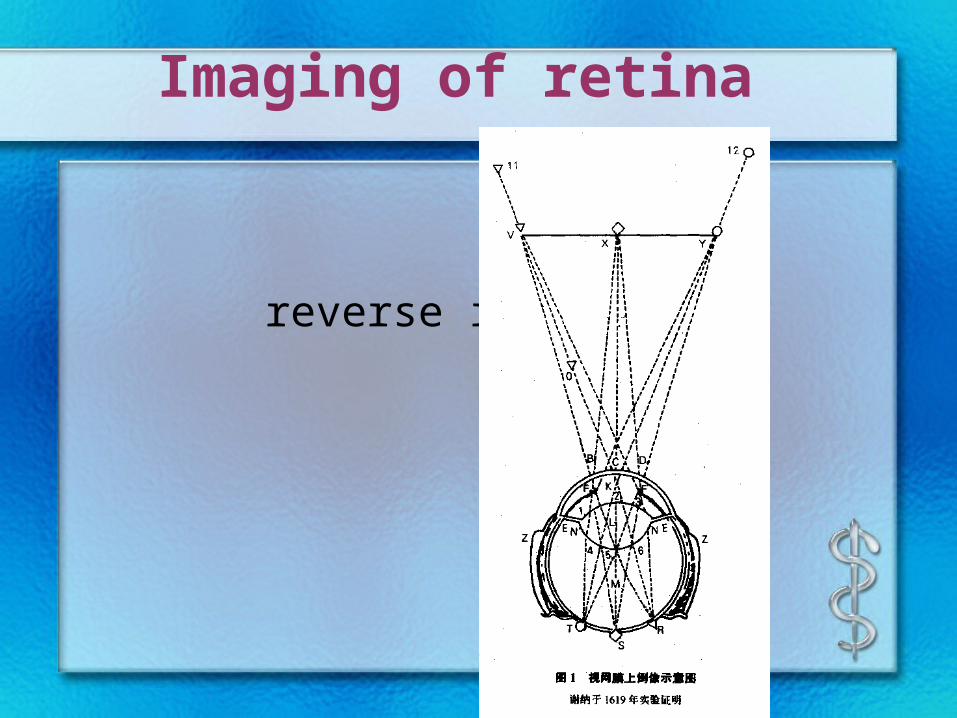
Imaging of retina
reverse imaging
Emmetropia
• Emmetropia : the refractive condition in focus on fovea that parallel lights enter eye through refractive system without accommodation
• Punctum remotum of emmetropia: infinite
Accommodation
• Accommodation
the capability that eyes change refractive
condition in order to acquire clear
near sight
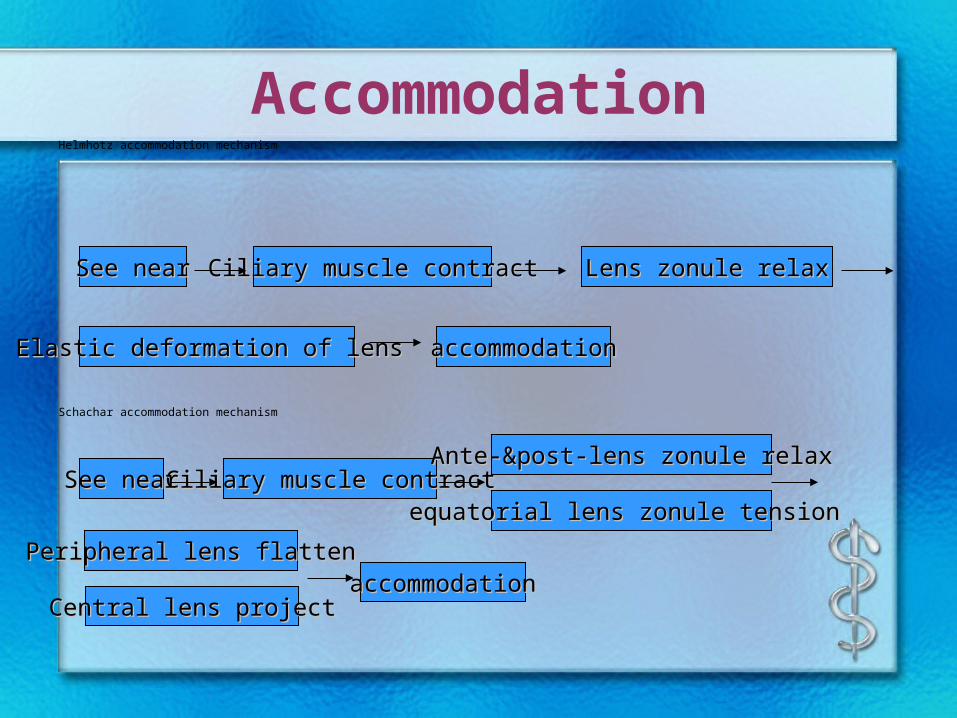
AccommodationHelmhotz accommodation mechanism
Schachar accommodation mechanism
Ciliary muscle contractCiliary muscle contract Lens zonule relaxLens zonule relax
accommodationaccommodationElastic deformation of lens Elastic deformation of lens
See nearSee near
Ciliary muscle contractCiliary muscle contractAnte-&post-lens zonule relaxAnte-&post-lens zonule relax
accommodationaccommodationPeripheral lens Peripheral lens flattenflatten
See nearSee nearequatorial equatorial lens zonule tension lens zonule tension
Central lens Central lens projectproject
Accommodation
• punctum remotum
• Diopter = 1 / distance of punctum remotum
• Static refraction
• Dynamic refraction
Accommodation
• Accommodation = diopter for far - diopter for near
• Range of accommodation = distance of far point — distance of near point
Accommodation & convergence
• Triad Phenomena of eye
– accommodation
– convergence
– Contraction of pupil
Ametropia
• Ametropia : the refractive condition out of focus on fovea that parallel lights enter eye through refractive system on static refraction
• classification– myopia– hyperopia– astigmatism
Myopia
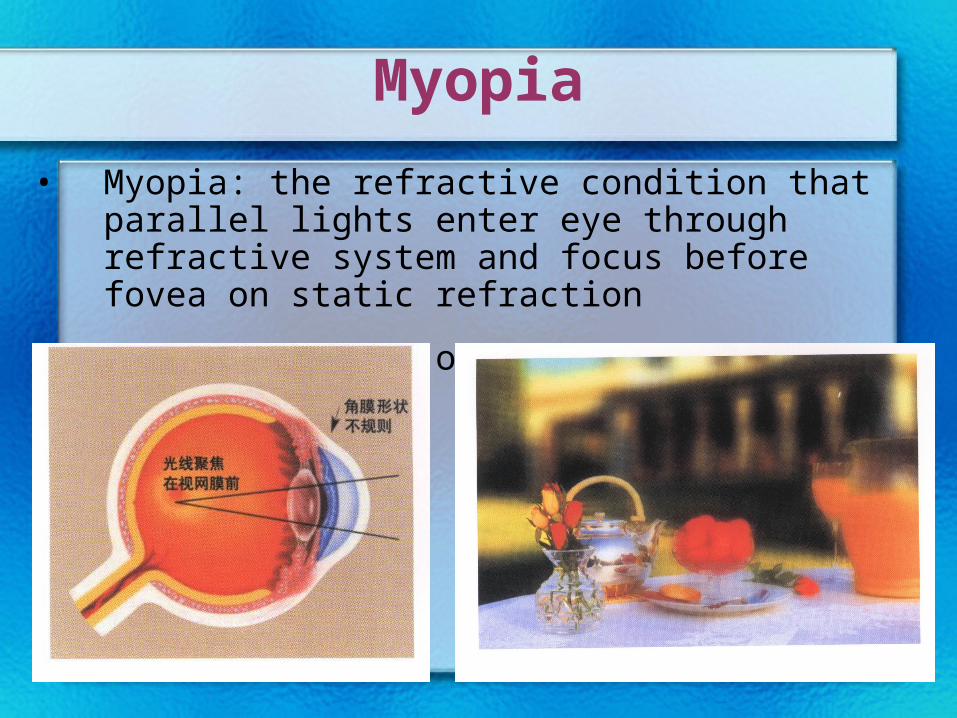
• Myopia: the refractive condition that parallel lights enter eye through refractive system and focus before fovea on static refraction
• Punctum remotum of myopia: a point before eye
Myopia classification
• Function
– Simple myopia
– Pathologic myopia
• Refractive factor
– Axis myopia
– Refractive myopia
• Degree
– mild : < -3.00D
– middle: -3.00D~-6.00D
– severe: > -6.00D
• Accommodation
– Pseudomyopia
(accommodative myopia)
– nonaccommodative myopia
– Mixed myopia
Myopia
• Clinical manifestation
– vision : far sight
– Asthenopia
– strabismus : exophoria / exotropia
– Change of eyeball : long eye axis , exophthalmos
– Change of fundus : tessellation ; myopic conus ;change of macula ; posterior scleral staphyloma ;change of peripheral fundus
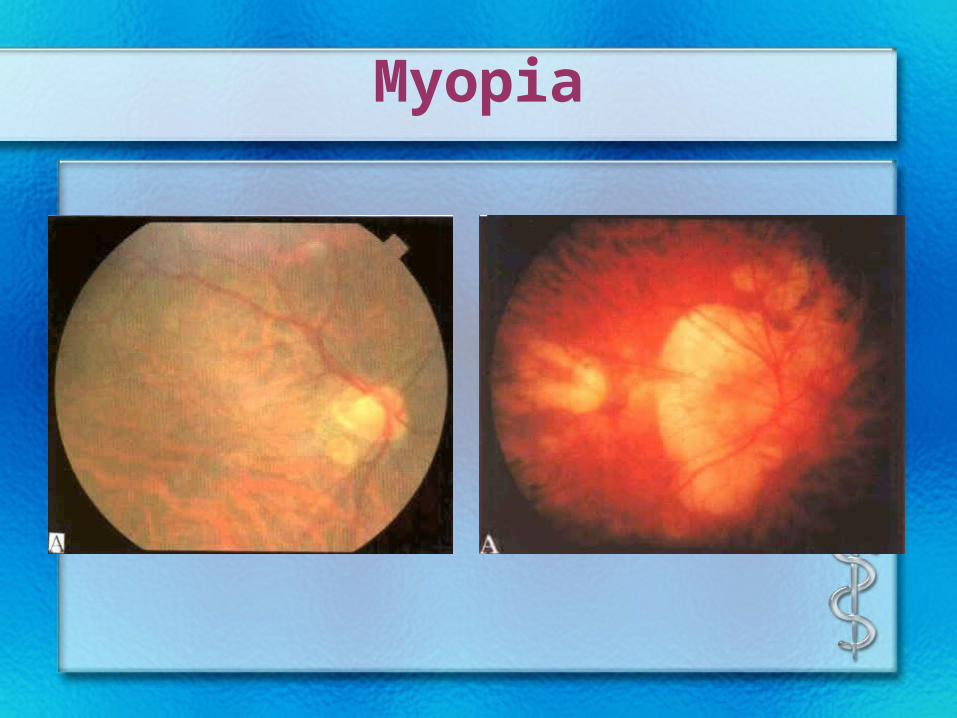
Myopia
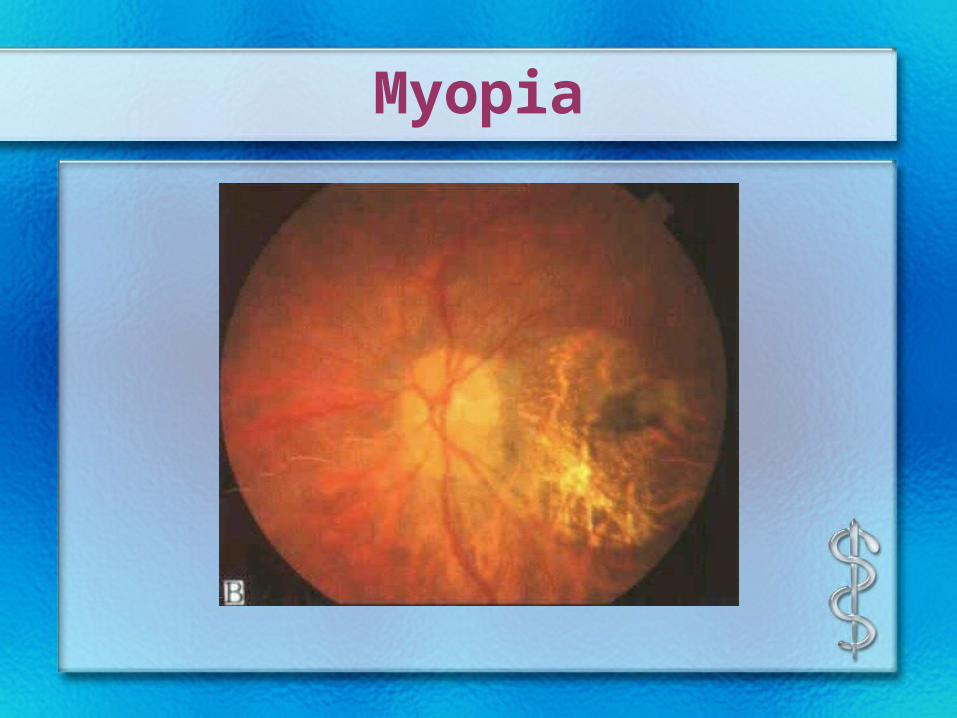
Myopia
• Complications
– Disorder of vitreous body
– Retinal detachment
– glaucoma
– cataract
Myopia
• Treatment
– Spectacles: concave lens
– principle : the lowest diopter for BCVA
– contact lens
– Refractive operation
– Treatment of complications
Myopia

Myopia
Hyperopia
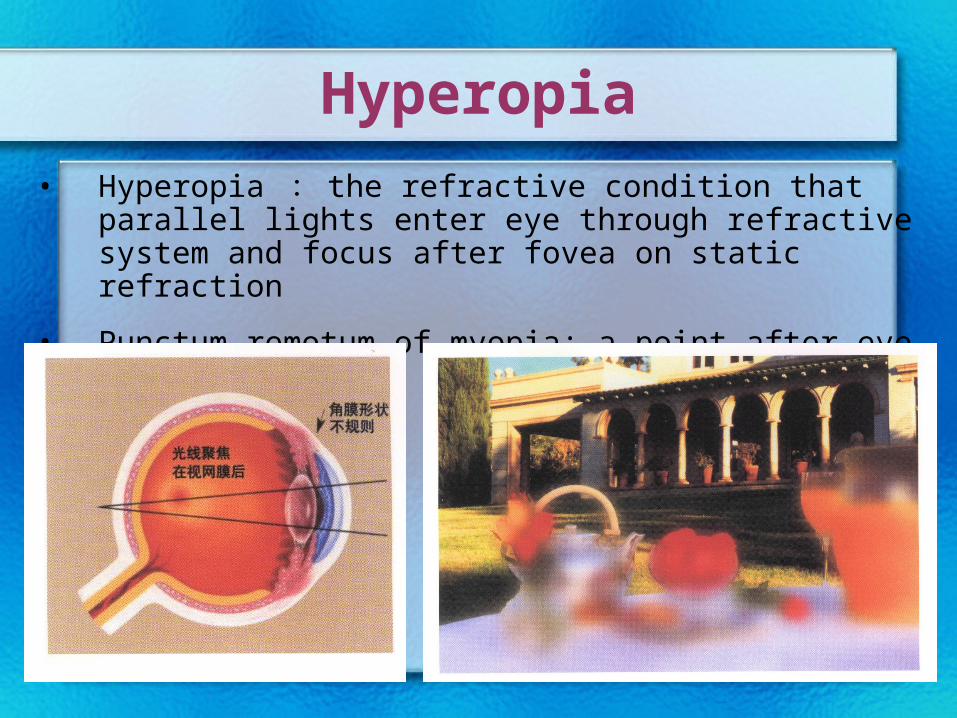
• Hyperopia : the refractive condition that parallel lights enter eye through refractive system and focus after fovea on static refraction
• Punctum remotum of myopia: a point after eye
• Refractive factor
• Axis hyperopia
• Refractive hyperopia
• Degree
• mild : < + 3.00D
• middle: + 3.00D~ + 6.00D
• severe: > + 6.00D
Hyperopia
• Clinical manisfestation
• sight
• degree of hyperopia, accommodation, amblyopia
• Asthenopia
• Esotropia
• Pathological change
Hyperopia
• Correction: convex lens
– Infant and adolescent : dilation pupil to examine eyesight
– adult : best sight , comfort
Hyperopia
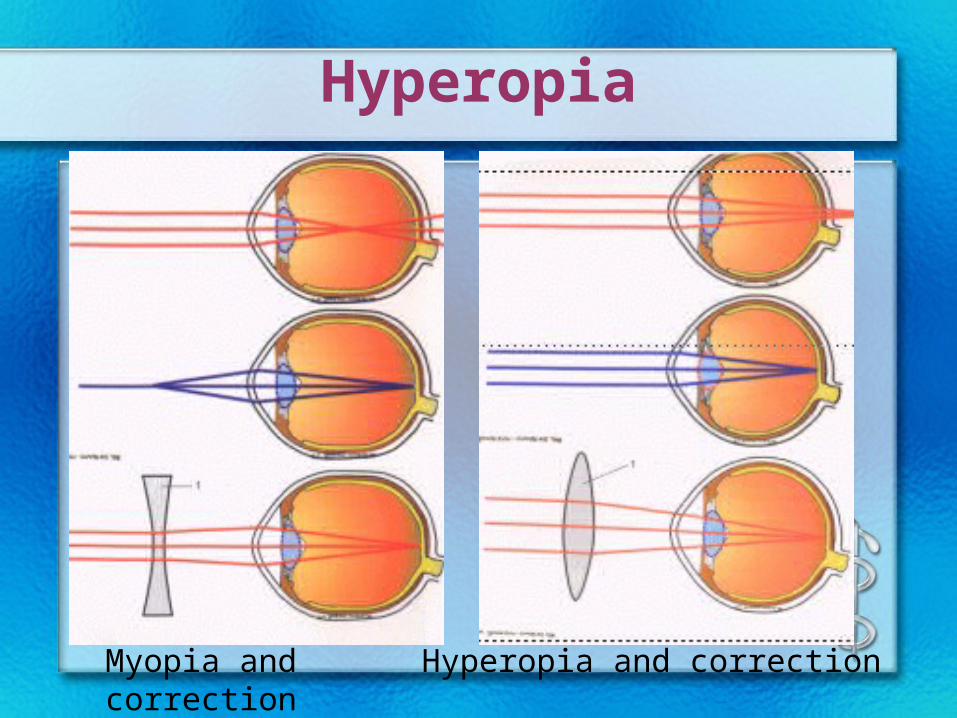
Myopia and correction Hyperopia and correction
Hyperopia

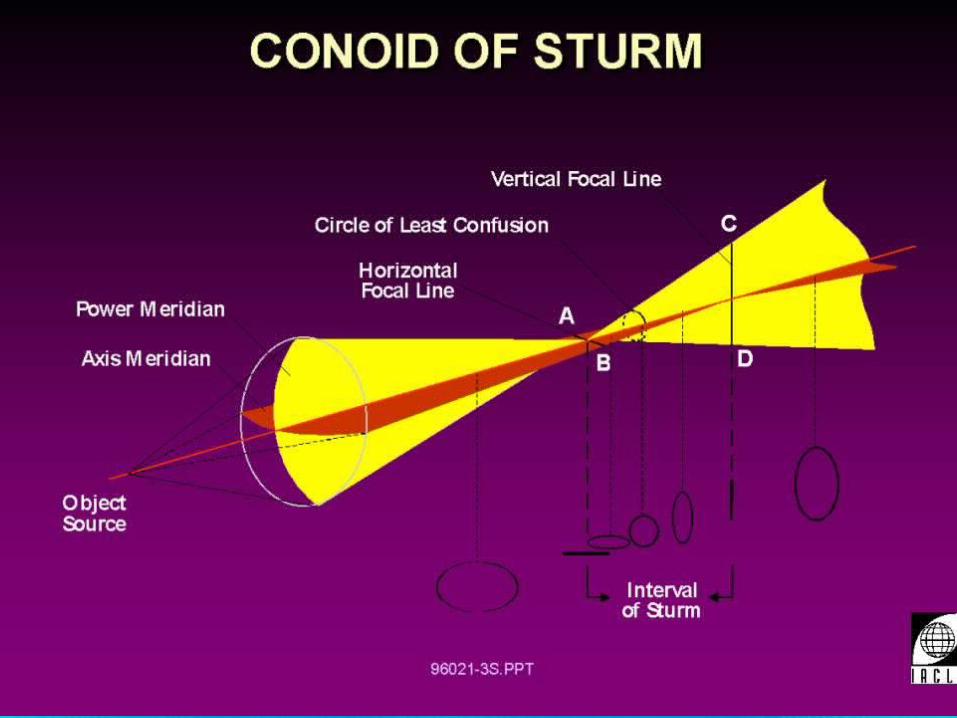
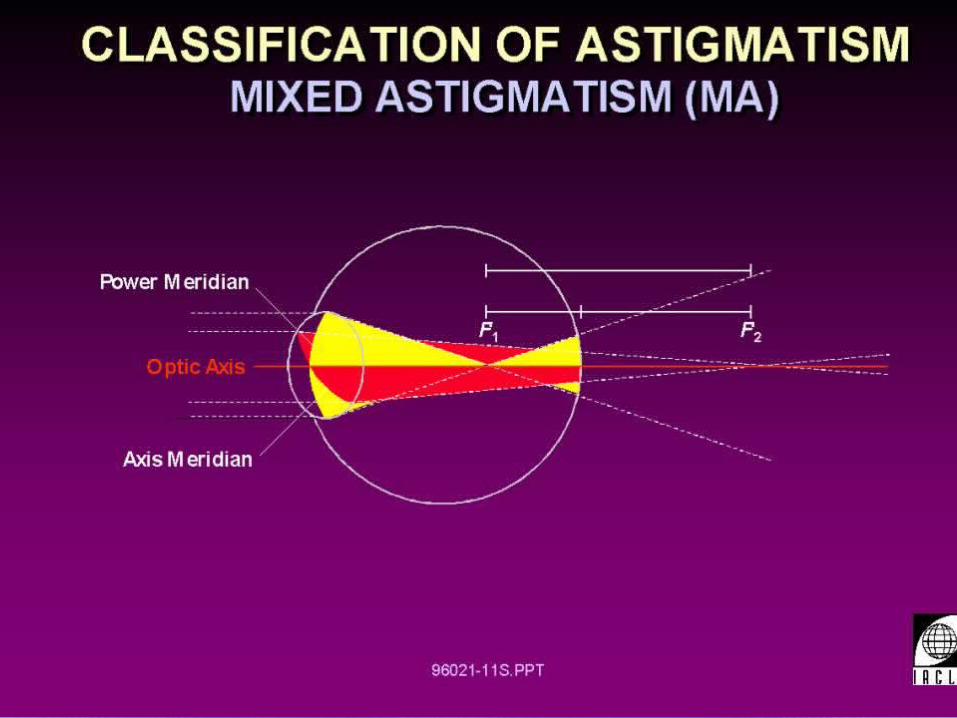
Astigmatism
• Astigmatism : the refractive status that parallel lights can’t focus through refractive system on static refraction because refractive power of individual meridian is different
• Regulation – Irregular astigmatism
– Regular astigmatism
• Regular astigmatism– astigmatism with rule
• strong refractive-power meridian : 90 °±20 °
– astigmatism against rule
• strong refractive-power meridian : 180°±20 °
– oblique astigmatism
• axis: 45°or 135°±20 °
Astigmatism
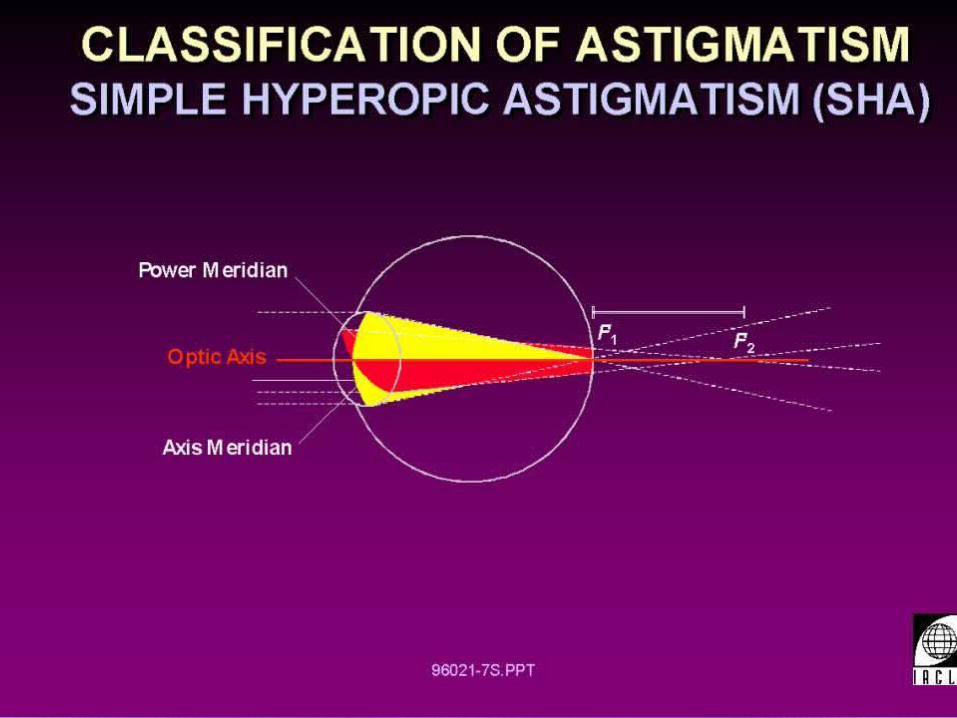
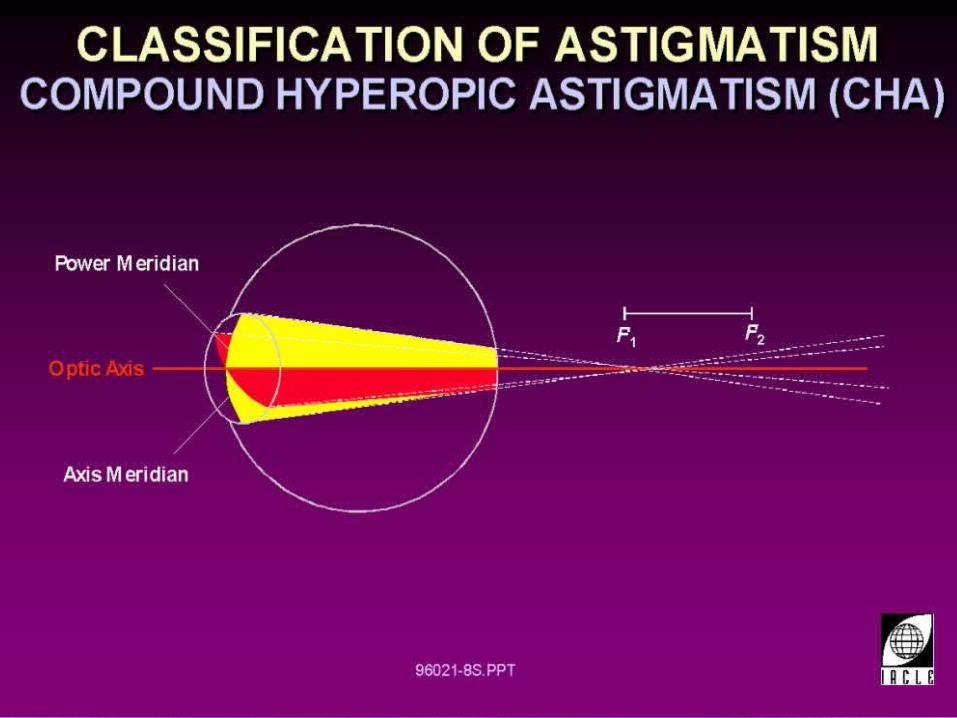
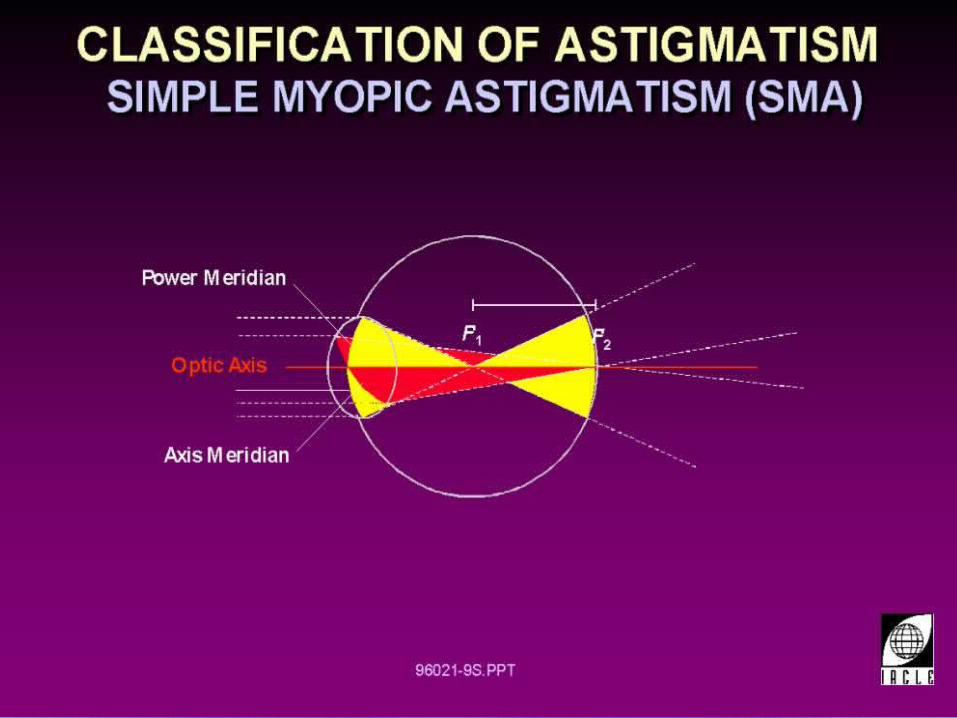
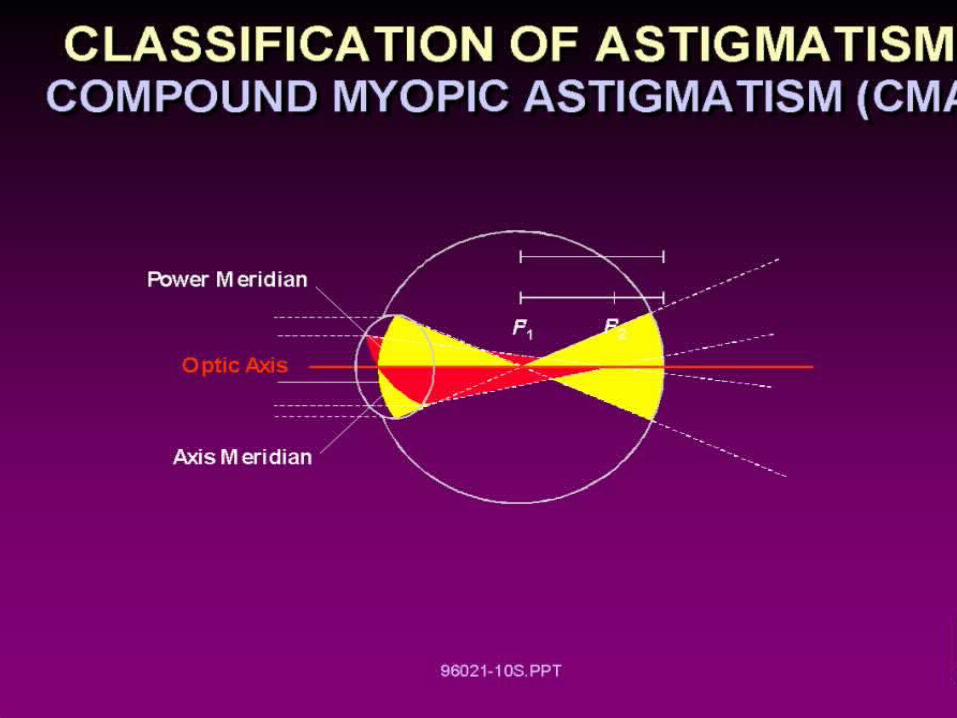
• Classification on refraction
– Simple hyperopic astigmatism ( SHA)
– Compound hyperopic astigmatism ( CHA)
– Simple myopic astigmatism ( SMA)
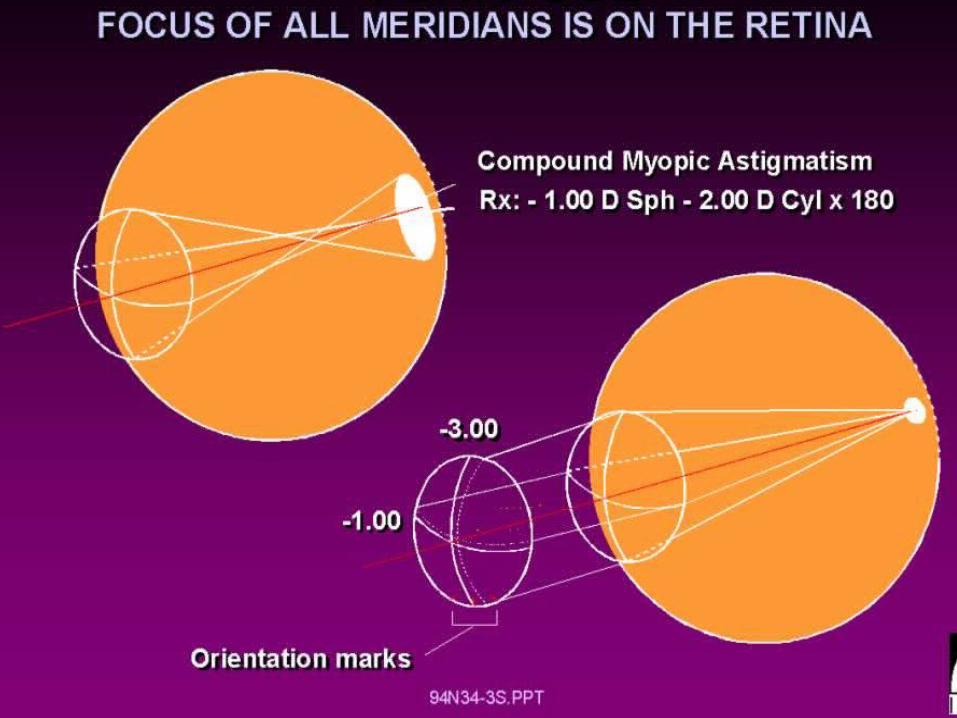
– Compound myopic astigmatism ( CMA)
– Mixed astigmatism ( MA)
Astigmatism
Astigmatism
• Clinical manifestation
– diminution of vision
– asthenopia
• correction
– Preventing overcorrection
Anisometropia• Anisometropia : the refractive status that refraction of
both eye is different
• Clinical presentation– Eruption of binocular single vision
Fusion limitation• the difference of imagination on both retina —— 25 %• the difference of diopter on both eyes ——3.0D
– Asthenopia
– alternative fixation
– amblyopia
Presbyopia
• Presbyopia : the decrease of physiological accommodation with aging
• cause
– Crystal sclerosis , decreased elasticity
– Decreased Ciliaris contraction
– late : enlargement of lens
Presbyopia
• Clinical presentation
– Difficulty in reading or working in a short distance
– Read in bright light
– asthenopia
– Accommodation delay
• Correction —— convex lens
Extraocular muscles
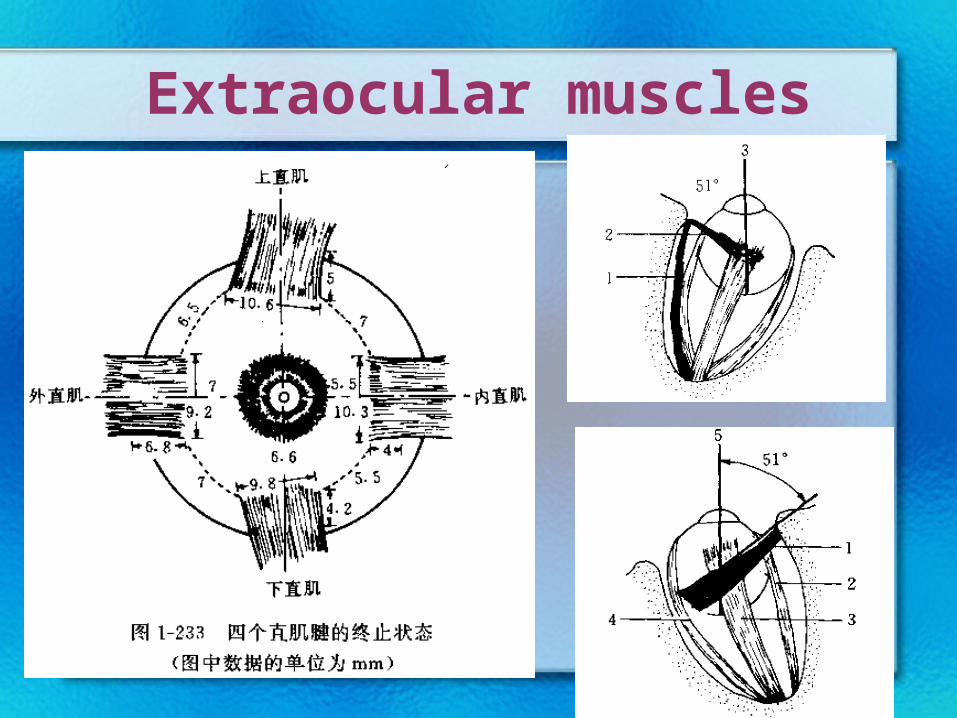
Extraocular muscles
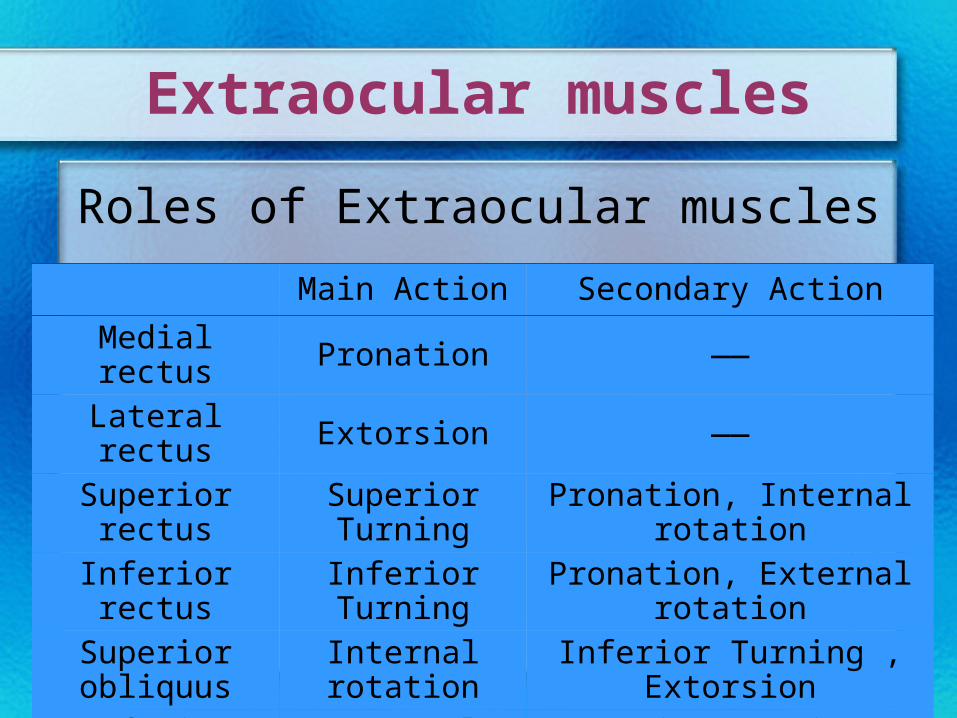
Extraocular muscles
Main Action Secondary Action
Medial rectus Pronation ——
Lateral rectus Extorsion ——
Superior rectus Superior Turning Pronation, Internal rotation
Inferior rectus Inferior Turning Pronation, External rotation
Superior obliquus Internal rotation Inferior Turning , Extorsion
Inferior obliquus External rotation Superior Turning , Extorsion
Roles of Extraocular muscles
Extraocular muscles
• Synergist : the same eye
• antagonist : the same eye
• Yoke muscles : double eyes
Strabismus
• Strabism: both eyes can’t be fixed on the target simultaneously and the optic axes are divergent. one eye is fixing on the target and the other eye is deviating from it.
• Classification
– Comitant strabismus
– Non-concomitant strabismus
– Special strabismus
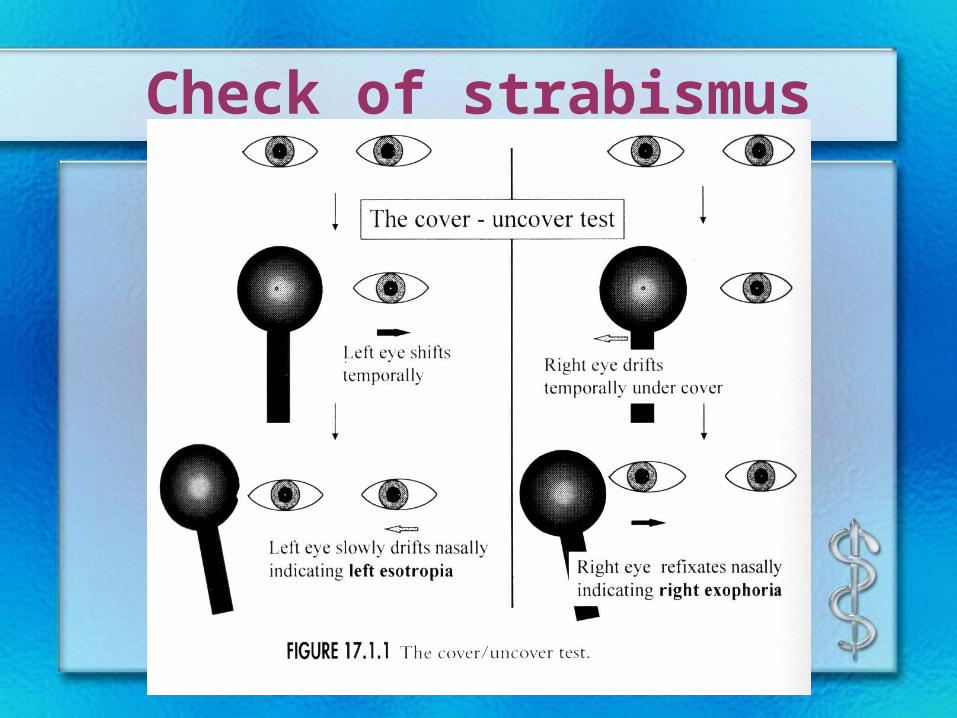
Check of strabismus
• History
• Sight and refraction
mydriasis and refraction
• Divergence of eye /compensatory head position
• ocular movement
• Quantu determination
– Corneal light reflection test
– triangular prism and cover test
– Arc perimetry
– triangular prism and Maddox
– synoptophore
Check of strabismus
Comitant strabismus• Direction
– Concomitant esotropia
– Concomitant exotropia
• Period– Heterophoria
– Heterotropia• Constancy strabismus
• Alternating strabismus
• intermittent strabismus
• accommodation– Accommodation esotropia
– Part Accommodation esotropia
– Non-accommodation esotropia
• Secondary – Paralysis compensation
– Postoperation
– perception
Comitant strabismus
• Therapeutics
– Correction of refractive errors
– Amblyopia discipline
– Position discipline
– operation
Non-concomitant strabismus
• Etiological factor– congenital– aquired : trauma,inflammation, vascular disease,
tumor, Metabolic disease– Physical eyeball motor disturbance
Non-concomitant strabismus
• clinical situation
– Diplopia and Vertigo
– Compensatory head position
– Divergence of eye position
– Limitation of motion
– 2nd angle of strabismus >1st angle of strabismus
Non-concomitant strabismus
• Therapeutics
– etiological factor
– Drug
– triangular prism
– operation
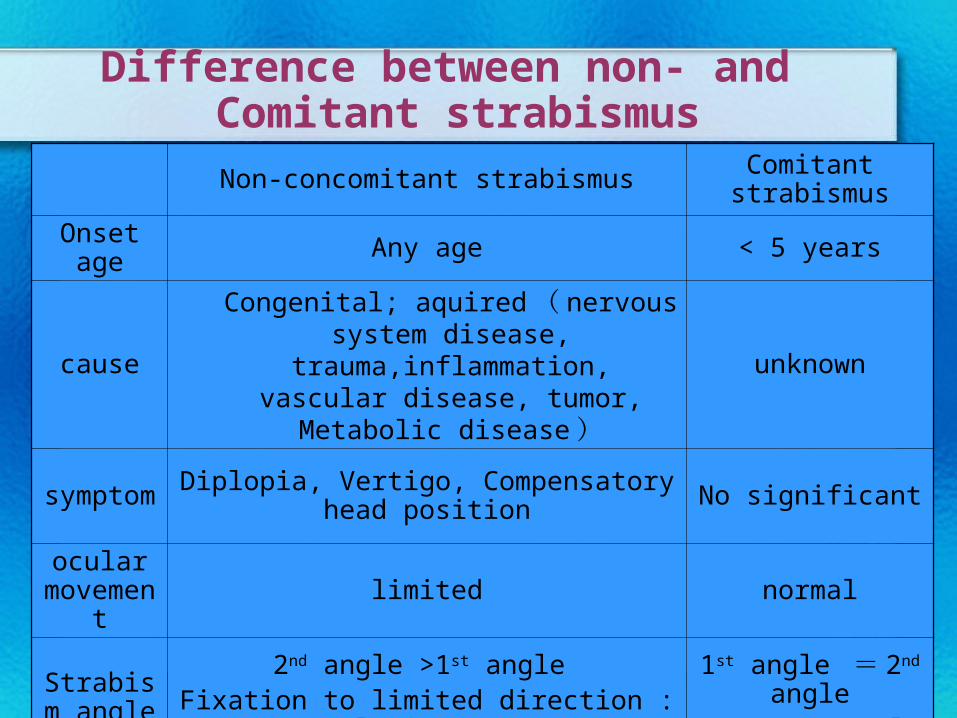
Difference between non- and Comitant strabismus
Non-concomitant strabismus Comitant strabismus
Onset age Any age < 5 years
causeCongenital; aquired ( nervous system disease, trauma,inflammation, vascular disease, tumor, Metabolic disease )
unknown
symptom Diplopia, Vertigo, Compensatory head position No significant
ocular movement limited normal
Strabism angle
2nd angle >1st angle Fixation to limited direction : angle increase
1st angle = 2nd angleConstant angle
Amblyopia
Amblyopia• Amblyopia
the visual development dysfunction of single/ double eye(s) because of insufficiency of visual stimulation into eye(s)—— form deprivation , and (or) difference between double eyes vision import which causes competition inhibition on the key period of visual development .
• BCVA ≤0.8
Amblyopia• Classification and causes
– strabismic amblyopia
– Anisometropic amblyopia
– ametropic amblyopia
– form deprivation amblyopia
– Other causes
• Degree
– slight
• BCVA: 0.6 ~ 0.8
– middle
• BCVA: 0.2 ~ 0.5
– severe
• BCVA: ≤0.1
Amblyopia• Clinical situation
– Poor vision
– Crowding phenomenon
– Abnormal fixation
– PVEP abnormality
– Disfunction of binocular single vision
– Elimination of other visual disfunction
Amblyopia
• Therapeutics
– correction of refractive errors
– amblyopia exercise