Embed Size (px)
Citation preview

Optimizing Nursing Management of Patients Receiving Novel
Therapies for Advanced NSCLC
Beth Eaby-Sandy, MSN, CRNP, OCN®
Nurse Practitioner
Abramson Cancer Center of the University of Pennsylvania

Disclosure of Conflicts of Interest
Beth Eaby-Sandy, MSN, CRNP, OCN® discloses she was a member of the advisory board of Boehringer Ingelheim and a member of the speakers’ bureau of Genentech in the last 12 months. She is currently a member of the speakers’ bureau of Lilly.
NSCLC: Scope of the ProblemEstimated New Cancer Cases in 2013
• Prostate: 238,590 (28%)• Lung/Bronchus: 118,080 (14%)• Colon/Rectum: 73,680 (9%)
• Breast: 226,870 (29%)• Lung/Bronchus: 110,110 (14%)• Colon/Rectum: 69,140 (9%)
ACS, 2013.
PERSPECTIVELung/Bronchus Deaths = 159,480Breast, Prostate, Colon/Rectum, and Pancreatic Deaths = 158,630
NSCLC: Scope of the ProblemEstimated New Cancer Cases in 2013
• Prostate: 238,590 (28%)• Lung/Bronchus: 118,080 (14%)• Colon/Rectum: 73,680 (9%)
• Breast: 226,870 (29%)• Lung/Bronchus: 110,110 (14%)• Colon/Rectum: 69,140 (9%)
ACS, 2013.

Lung Cancer Stages and Survival
0
20
40
60
2003-2009, All Races, Both Sexes
Stage Distribution (%) 5-Year Relative Survival (%)
Stage
Pe
rce
nt
SEER Data, 2003-2009.
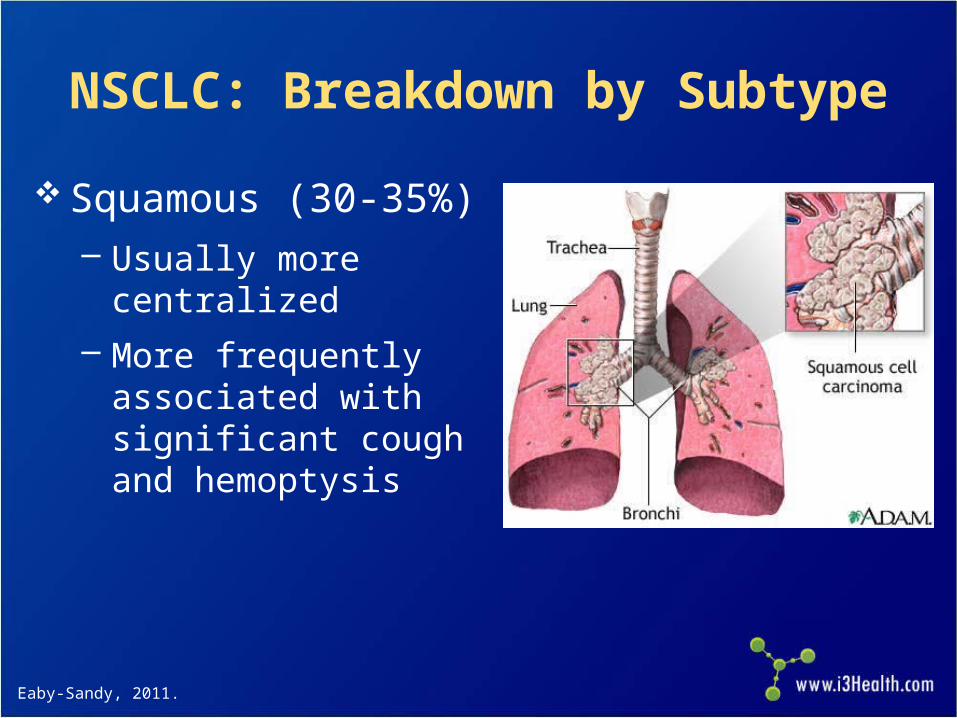
NSCLC: Breakdown by Subtype
Squamous (30-35%)– Usually more
centralized
– More frequently associated with significant cough and hemoptysis
Eaby-Sandy, 2011.

NSCLC: Breakdown by Subtype
Nonsquamous (65%)– Adenocarcinoma (40%)
• Most common type of NSCLC
• Most common type innonsmokers
– Large cell carcinoma (15%)
– Mixed or NOS (10%)
NOS = not otherwise specified.Eaby-Sandy, 2011.

NSCLC: Why Does Histology Matter?
In past, all NSCLC patients treated the same Data have shown that the use of certain
agents in certain histologies results in improved survival and response rates
Histology may predict the presence of biomarkers
Safety parameters of certain treatments depend on histology
NCCN, 2013.

NSCLC: Breakdown of BiomarkersUnknown
KRAS
EGFR
ALK
RET
MET
PI3K
BRAF
HER2
PDGFR
VEGFR
FGFR1
AKT1
MEK1
ROS1
5%
25%
15%
33%
5%
3% 3% 3%
2%
1%
Hirsch, 2012.

NCCN, 2013; Langer et al, 2010.
EGFR • Transmembrane receptor• Detectable in about 80-85% of patients• Level of expression varies widely• Mutations in this domain (10-15% of pts) result in activation of the tyrosine
kinase domain with significantly better response to erlotinib or gefitinib • Mutations: highest incidence in never smokers, adenocarcinoma, women,
and patients with Asian ethnicity
KRAS • 25% of North American population• Associated with smoking and resistance to tyrosine kinase inhibitors• KRAS mutations associated with shorter survival • Therapy with drugs other than erlotinib should be considered first
EML4-ALK • Incidence of EML4-ALK translocation: 2-7%• Estimated prevalence of EML4-ALK in lung cancer: 6,000 pts/yr US; up to
40,000 pts/yr globally• Most EML4-ALK fusion events observed in lung adenocarcinoma specimens
vs squamous or small cell histologies• EML4-ALK rarely coexists with EGFR, HER2, or KRAS mutations, indicating it
is a distinct disease subtype
Molecular Abnormalities in NSCLC With Current Implications
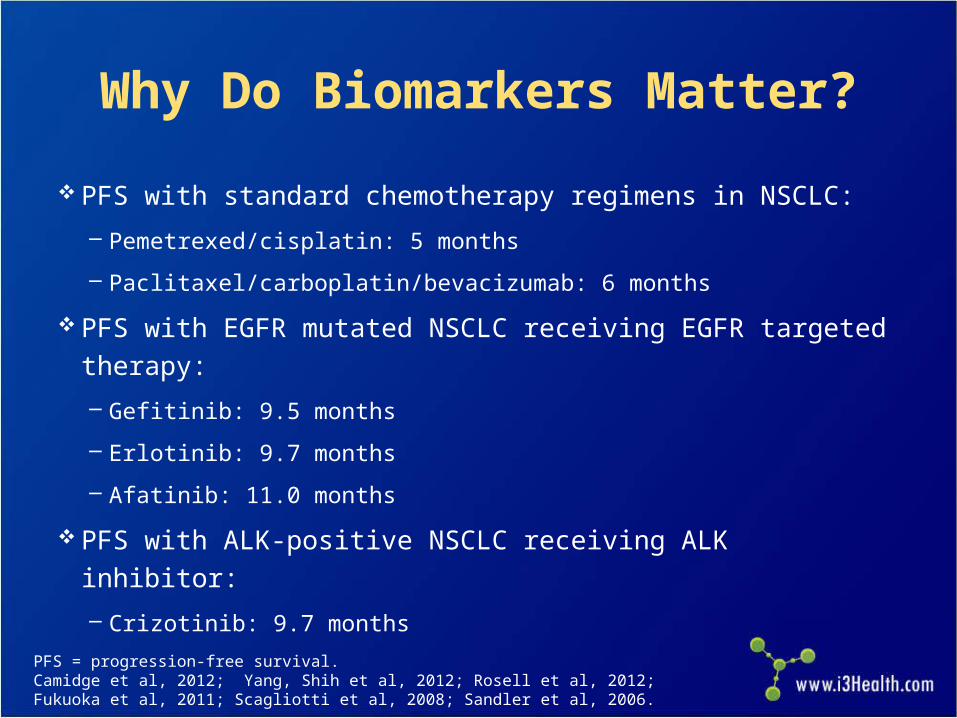
Why Do Biomarkers Matter?
PFS with standard chemotherapy regimens in NSCLC:
– Pemetrexed/cisplatin: 5 months
– Paclitaxel/carboplatin/bevacizumab: 6 months
PFS with EGFR mutated NSCLC receiving EGFR targeted therapy:
– Gefitinib: 9.5 months
– Erlotinib: 9.7 months
– Afatinib: 11.0 months
PFS with ALK-positive NSCLC receiving ALK inhibitor:
– Crizotinib: 9.7 monthsPFS = progression-free survival.Camidge et al, 2012; Yang, Shih et al, 2012; Rosell et al, 2012; Fukuoka et al, 2011; Scagliotti et al, 2008; Sandler et al, 2006.
Patient Factors in Treatment Planning
Patient ECOG PS– PS is a predictor of survival/tolerating chemotherapy
– PS 0/1 patients tolerate chemotherapy best
– PS 2 patients can potentially benefit, even from doublet chemotherapy; however, toxicity must be monitored closely
Comorbidities– Diabetes, heart disease
– Renal disease
ECOG PS = Eastern Cooperative Oncology Group performance status.Rodriguez & Lilenbaum, 2008.

Patient Factors in Treatment Planning
Patient goals for treatment– Quality-of-life issue (eg, hair loss)
– Advanced directives
Demographics Social support
– Involve social worker
– Counseling services
– Nutrition services
Financial issues
Evolving Supportive Care Paradigms
Early palliative care leads to increase in OS in patients with metastatic NSCLC
Increased quality of life, less depressive symptoms Improved understanding of diagnosis
– 1/3 patients at diagnosis thought they had curable disease– Less likely to receive chemotherapy near end of life
OS = overall survival.Temel et al, 2011; Temel et al, 2010.

Case Study: First-Line Treatment
Mrs. JF: History
68-year-old woman, presented 1 month ago with pain in her
lower back
Initial management with NSAIDs somewhat helpful; however,
the pain persisted and an x-ray of the lower spine was ordered
X-ray did not show bone abnormality but revealed a right lung
mass at the right lung base
Further imaging with PET/CT revealed a right lung mass,
mediastinal lymphadenopathy, bone metastases in the lumbar
spine, and liver metastases
– X-rays are often negative
NSAIDs = nonsteroidal antiinflammatory drugs; PET/CT = positron emission tomography/computed tomography.
Mrs. JF: Diagnostic Evaluation
Treating physician referred patient to pulmonologist for a bronchoscopy with biopsy– Mediastinal lymph node was positive for NSCLC,
adenocarcinoma histology
MRI scan of the brain negative for metastatic disease
Baseline labs within normal limits Baseline PS 1 What factors important in treatment planning?
MRI = magnetic resonance imaging.

Mrs. JF: Treatment Considerations
Bronchoscopy yielded core biopsy, able to perform KRAS,
EGFR, ALK, and ROS testing. All were negative.
Patient has a 45-pack-year smoking history, currently
trying to quit
Patient has hypertension (controlled with medication),
hypercholesterolemia, and chronic obstructive pulmonary
disease
No significant weight loss, no hemoptysis
Understands incurable, no advanced directive, would like
to “fight”
Mrs. JF: Treatment Selection
Standard chemotherapy in biomarker-negative patient appropriate therapy
Numerous options available for chemotherapy Platinum based chemotherapy appropriate
given good PS Is hair loss an issue? Does she want to enroll in a clinical trial?
NCCN, 2013.
Mrs. JF: Treatment Selection
Cisplatin versus carboplatin? In US, often use carboplatin in frontline therapy
What drug to pair with carboplatin? Toxicity?– Pemetrexed
– Paclitaxel
– Docetaxel
– nab-paclitaxel
– Gemcitabine
– Vinorelbine
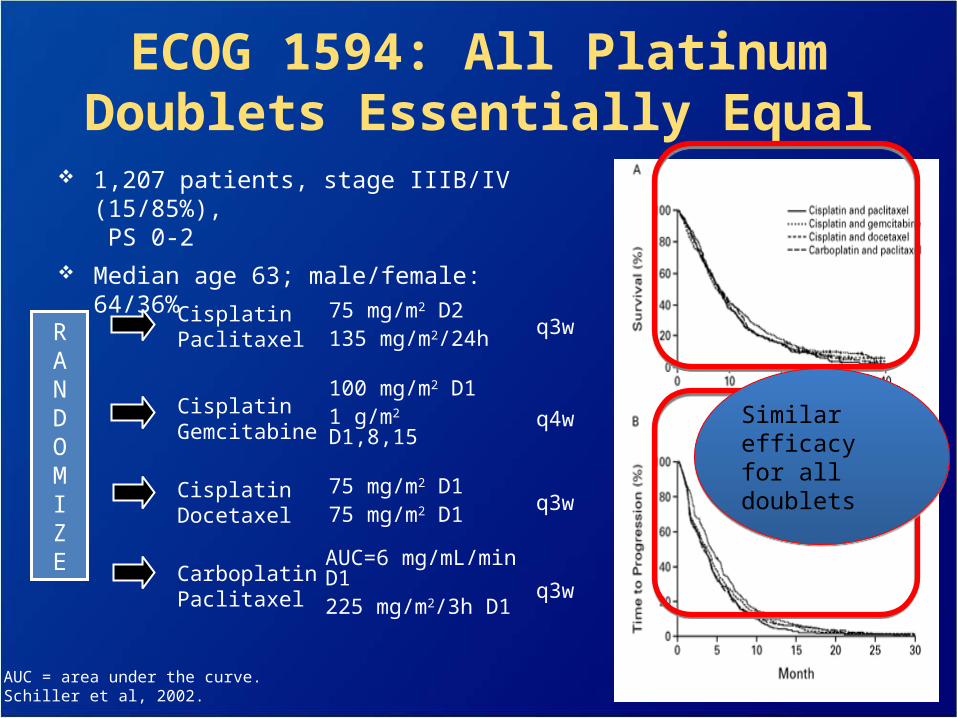
ECOG 1594: All Platinum Doublets Essentially Equal
1,207 patients, stage IIIB/IV (15/85%), PS 0-2
Median age 63; male/female: 64/36%
q3wAUC=6 mg/mL/min D1225 mg/m2/3h D1
CarboplatinPaclitaxel
q3w75 mg/m2 D175 mg/m2 D1
CisplatinDocetaxel
q4w100 mg/m2 D11 g/m2 D1,8,15
CisplatinGemcitabine
q3w75 mg/m2 D2135 mg/m2/24h
CisplatinPaclitaxelR
ANDOMIZE
AUC = area under the curve.Schiller et al, 2002.
Similar efficacy for all doubletsSimilar efficacy for all doublets
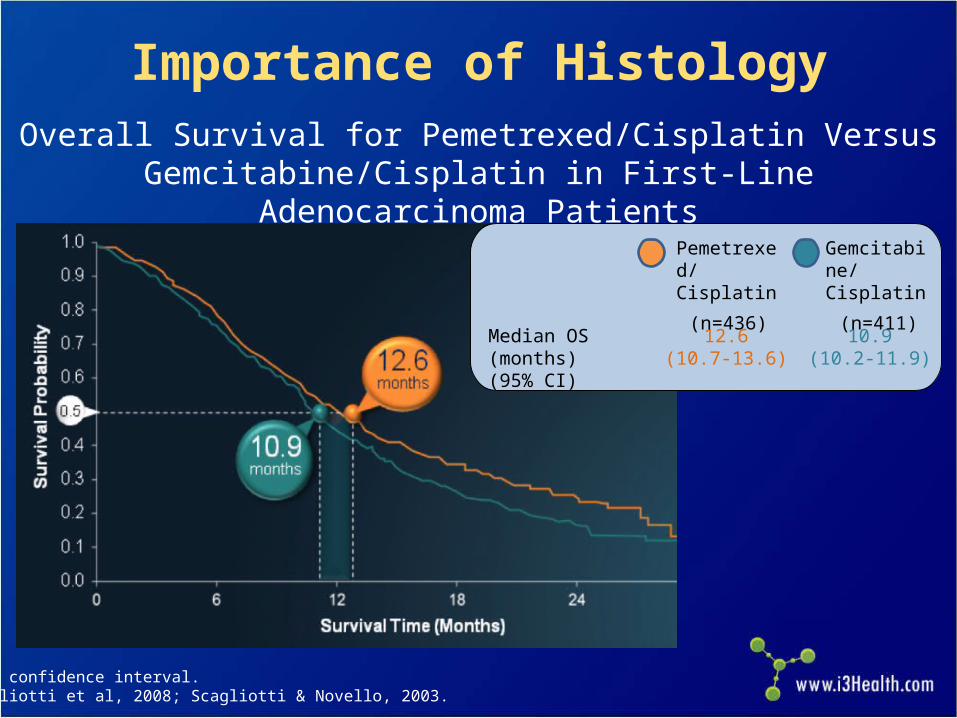
Importance of Histology
Overall Survival for Pemetrexed/Cisplatin VersusGemcitabine/Cisplatin in First-Line Adenocarcinoma Patients
CI = confidence interval.Scagliotti et al, 2008; Scagliotti & Novello, 2003.
Median OS (months)(95% CI)
12.6(10.7-13.6)
10.9(10.2-11.9)
Pemetrexed/Cisplatin
(n=436)
Gemcitabine/Cisplatin
(n=411)
What About Bevacizumab? Targeted therapy that can be added to chemotherapy in metastatic
NSCLC Eligibility criteria and warnings:
– Nonsquamous histology only
– No history hemoptysis (postprocedure ok?)
– No recent history of arterial thrombotic event
– No uncontrolled hypertension
– Nephrotic syndrome (proteinuria ≥3.5gm)
– No surgery within 28 days
– Gastrointestinal perforation
– Non-gastrointestinal fistula formation
– Reversible posterior leukoencephalopathy syndrome
– Infusion reactions
– Ovarian failure
Avastin® prescribing information, 2013.

E4599 Trial: Bevacizumab + PC Versus PC Alone in First-Line Nonsquamous NSCLC
Median OS with Bevacizumab + PC was 12.3 months vs 10.3 months for PC
alone (P=0.013)
PC = paclitaxel + carboplatin.Sandler et al, 2006; Sandler et al, 2011.
1-year survival: 51% vs 44%
2-year survival:23% vs 15%

PointBreak Trial: Can Regimens Be Combined?
Randomized, open-label, phase III superiority study conducted in US Pemetrexed 500 mg/m2; carboplatin AUC 6; bevacizumab 15 mg/kg Paclitaxel 200 mg/m2; carboplatin AUC 6; bevacizumab 15 mg/kg
Induction Phase Maintenance Phase q21d, 4 cycles q21d until PD
Inclusion:− No prior systemic
therapy for lung cancer− PS 0/1− Stage IIIB-IV
nonsquamous NSCLC− Stable treated brain
metastasized
Exclusion:− Peripheral neuropathy
≥grade 1− Uncontrolled pleural
effusions
Pemetrexed+ Carboplatin
+ BevacizumabPemetrexed
+ Bevacizumab
Paclitaxel+ Carboplatin
+ BevacizumabBevacizumab
450 Patients Each
q21d= every 21 days; PD = progressive disease.Patel et al, 2012.
R1:1
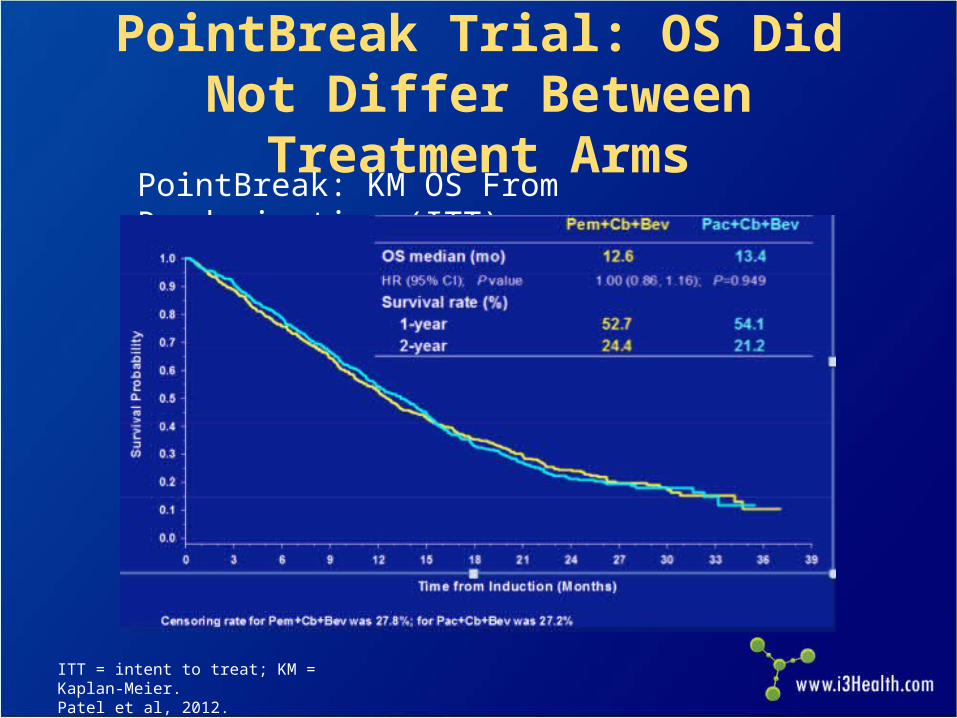
PointBreak Trial: OS Did Not Differ Between Treatment Arms
PointBreak: KM OS From Randomization (ITT)
ITT = intent to treat; KM = Kaplan-Meier.Patel et al, 2012.
Which Regimen to Choose for First-Line Treatment?
Discuss toxicity profiles of different regimens Take histology into account Give patients autonomy to decide
– Do they want treatment?
– If so, which regimen’s toxicity profile is right for them?
– Comorbidities? Diabetes? Coronary artery disease? Renal insufficiency?
Maintenance Therapy
If no disease progression after first-line chemotherapy, continue the chemotherapy and/or targeted agent?
We know that in NSCLC continuing platinum chemotherapy past 4 to 6 cycles does not improve survival, just increases toxicity
However, three drugs have shown improvement in PFS in the maintenance setting
NCCN, 2013.

E4599 Trial: Bevacizumab + PC Versus PC Alone in First-Line Nonsquamous NSCLC
Paclitaxel 200 mg/m2 + carboplatin AUC=6
q3w x 6(no crossover permitted)
(n=444)
Bev 15 mg/kg Solution for IV infusion
q3w + PC x 6(n=434)
Bev 15 mg/kg IVq3w until disease
progression or unacceptable
toxicity
Stratified by• Disease stage• Degree of weight
loss• Prior radiotherapy• Measurable disease
Primaryend point
OS
Secondaryend points
Response rate, PFS, toxicity
q3w = every 3 weeks; IV = intravenously. Sandler et al, 2006.
First-line treatment of patients with stage IIIB and
malignant pleural effusion, stage IV,
or recurrent NSCLC (N=878)
Continued until progression or unacceptable toxicity
Maintenance Pemetrexed
Both studies showed improvement in OS when either switching or continuing on with maintenance pemetrexed after first-line induction platinum-based chemotherapy.
Ciuleanu et al, 2009; Paz-Ares et al, 2012.
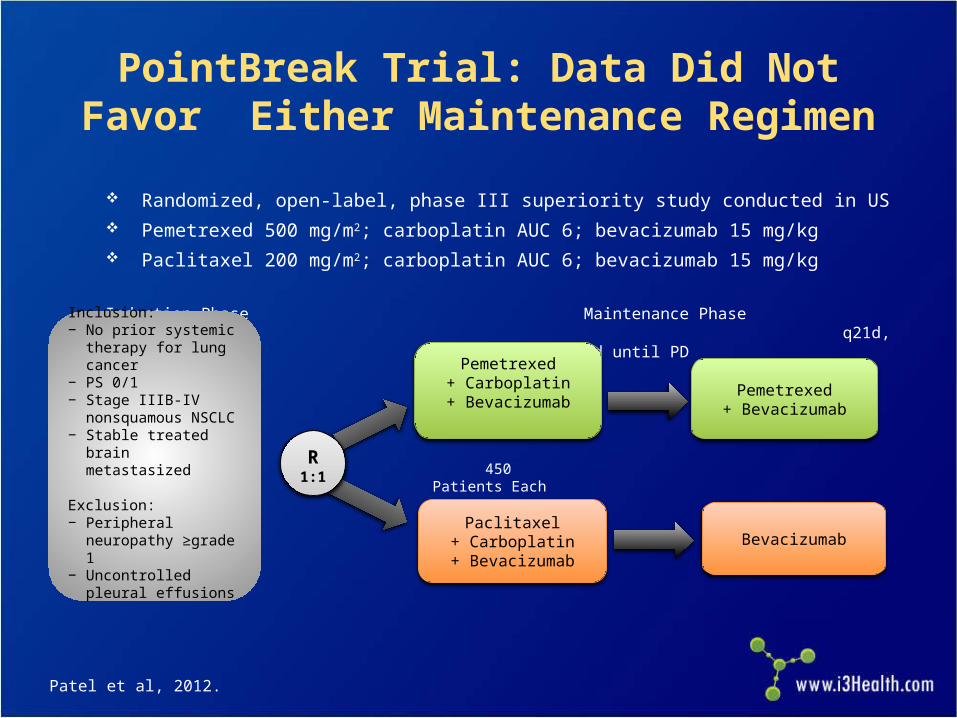
PointBreak Trial: Data Did Not Favor Either Maintenance Regimen
Randomized, open-label, phase III superiority study conducted in US Pemetrexed 500 mg/m2; carboplatin AUC 6; bevacizumab 15 mg/kg Paclitaxel 200 mg/m2; carboplatin AUC 6; bevacizumab 15 mg/kg
Induction Phase Maintenance Phase q21d, 4 cycles q21d until PD
Inclusion:− No prior systemic
therapy for lung cancer− PS 0/1− Stage IIIB-IV
nonsquamous NSCLC− Stable treated brain
metastasized
Exclusion:− Peripheral neuropathy
≥grade 1− Uncontrolled pleural
effusions
Pemetrexed+ Carboplatin
+ BevacizumabPemetrexed
+ Bevacizumab
Paclitaxel+ Carboplatin
+ BevacizumabBevacizumab
450 Patients Each
Patel et al, 2012.
R1:1

SATURN Trial: Erlotinib Maintenance
IHC = immunohistochemistry.Cappuzzo et al, 2010.
PD
PD
Mandatory tumor sampling
4 cycles of first-line
platinum-based doublet
Chemotherapy-naive, advanced NSCLC
N=1,949
Non-PDn=889
Erlotinib150 mg/d
n=438
Placebon=451
SATURN included patients with the following tumor types:– Squamous cell carcinoma– Nonsquamous cell carcinoma (adenocarcinoma, large cell, other)
Coprimary end points:– PFS in all patients– PFS in patients with EGFR IHC-positive tumors
Secondary end points:– OS in all patients and those with EGFR IHC-positive tumors– OS and PFS in EGFR IHC-negative tumors– Safety
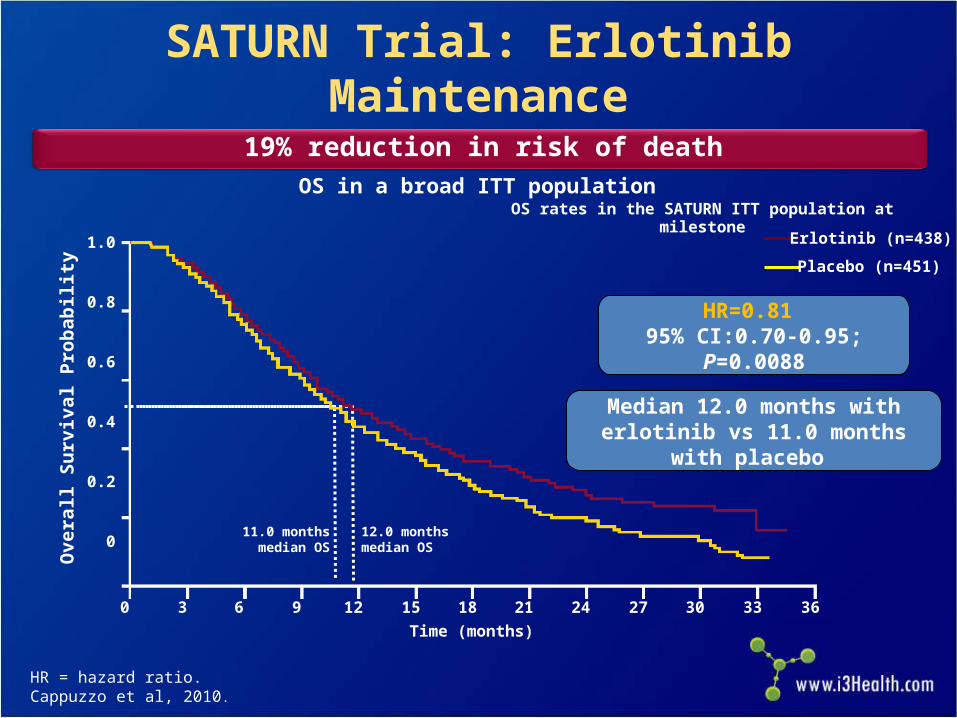
SATURN Trial: Erlotinib Maintenance
0 3 6 9 12 15 18 21 24 27 30 33 36
12.0 monthsmedian OS
11.0 monthsmedian OS
OS rates in the SATURN ITT population at milestone
19% reduction in risk of death
HR = hazard ratio.Cappuzzo et al, 2010.
Time (months)
Ove
rall
Su
rviv
al P
rob
abil
ity
1.0
0.8
0.6
0.4
0.2
0
Erlotinib (n=438)
Placebo (n=451)
OS in a broad ITT population
HR=0.81 95% CI:0.70-0.95; P=0.0088
Median 12.0 months with erlotinib vs 11.0 months with placebo
Maintenance Treatment Conclusions
Again, there are options, just like first-line chemotherapy choice
Do patients want a break or wish to continue? Toxicity profile
– Pemetrexed is chemotherapy: potential for lowering of blood counts, requires vitamin supplementation
– Bevacizumab and erlotinib are targeted agents, with the potential for hypertension/cardiac toxicity, rash
Cost? Should this be an issue? Insurance coverage/denials?

Case Study: Biomarker-Positive Patient

Ms. LT: History
47-year-old woman who had a cough for 2 months. Antibiotics and antihistamines did not improve her symptoms.
Chest x-ray revealed multiple small masses in bilateral lungs and pleural effusion, confirmed by CT; PET/CT revealed no other disease outside of chest
MRI scan of brain negative for metastatic disease
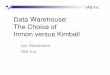
Ms. LT: Diagnostic Evaluation
Pleural fluid positive for adenocarcinoma histology; however, not enough for molecular analysis
Bronchoscopy/endobronchial ultrasound performed; able to biopsy mediastinal lymph node to get more tissue
Molecular testing revealed an exon 19 deletion EGFR mutation
Patient is a never smoker with no significant medical history or comorbidities

EGFR-Positive NSCLC: CT Chest Scan at Diagnosis
Image courtesy of Beth Eaby-Sandy, MSN, CRNP, OCN®

Ms. LT: Treatment Considerations
Chemotherapy versus targeted therapy in first-line treatment?
How long did it take to receive the molecular testing results?
Toxicity profiles, how do they differ? Current approved EGFR tyrosine kinase
inhibitors: gefitinib (no longer approved in US), erlotinib, and afatinib
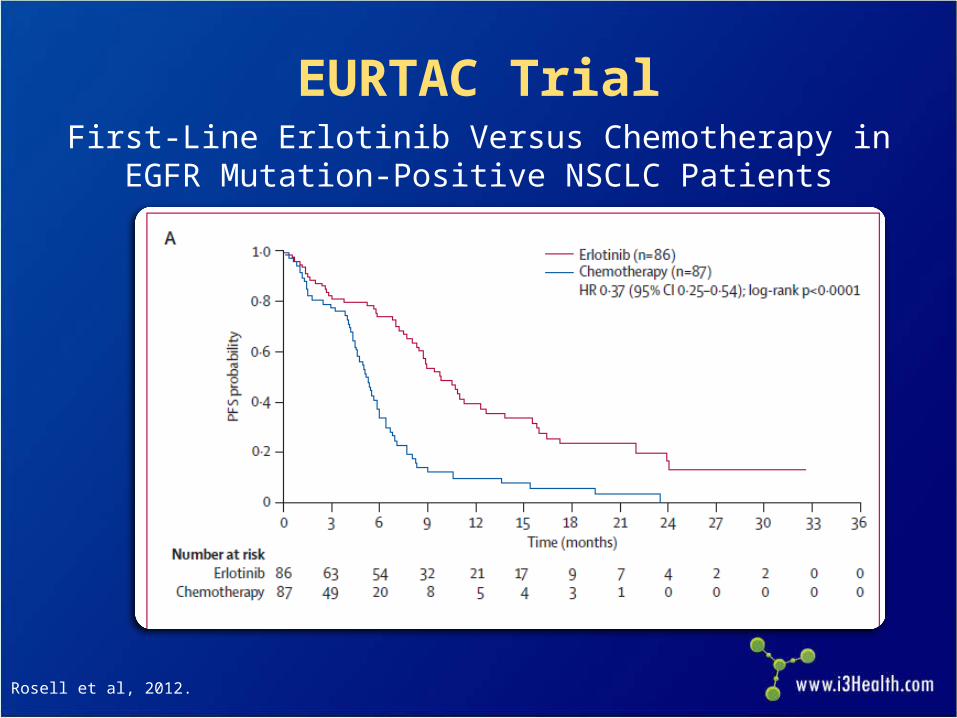
EURTAC TrialFirst-Line Erlotinib Versus Chemotherapy in EGFR
Mutation-Positive NSCLC Patients
Rosell et al, 2012.

Another EGFR Inhibitor
Afatinib– Irreversible pan-EGFR/HER inhibitor
• Approved in July 2013 for first-line treatment of EGFR mutation-positive metastatic NSCLC
– Dose is 40 mg daily, orally
Yang, Shih et al, 2012.
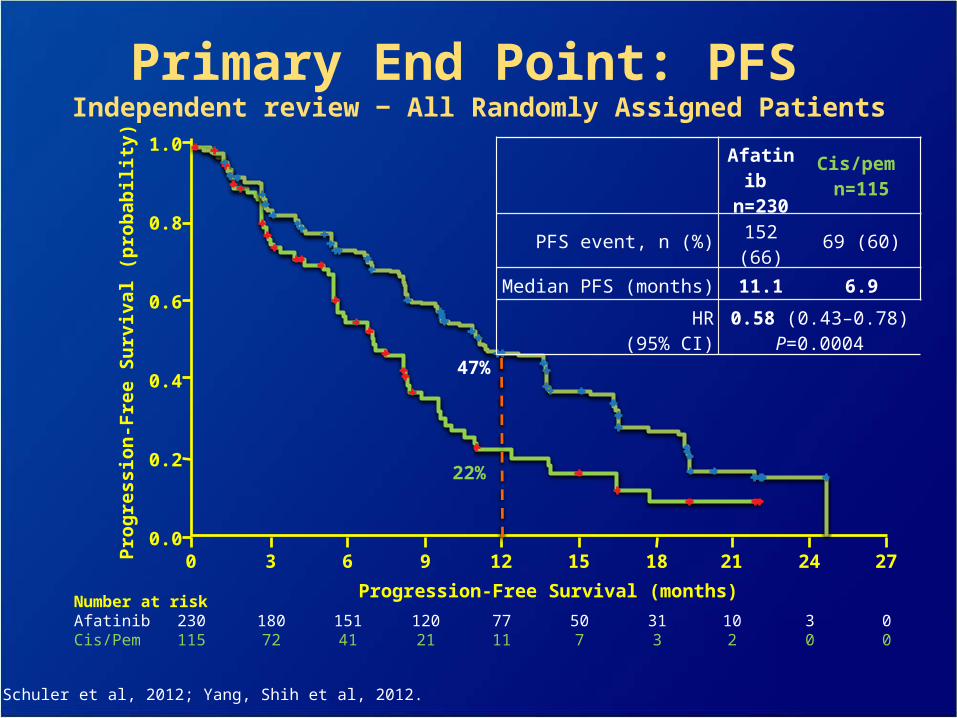
Primary End Point: PFS Independent review ‒ All Randomly Assigned Patients
Pro
gre
ssio
n-F
ree
Su
rviv
al (
pro
bab
ilit
y)1.0
0.8
0.6
0.4
0.2
0.0
Number at riskAfatinib 230 180 151 120 77 50 31 10 3 0Cis/Pem 115 72 41 21 11 7 3 2 0 0
Progression-Free Survival (months)
0 3 6 9 12 15 18 21 24 27
Afatinib
n=230
Cis/pem n=115
PFS event, n (%) 152 (66) 69 (60)
Median PFS (months) 11.1 6.9
HR(95% CI)
0.58 (0.43–0.78)P=0.0004
47%
22%
Yang, Schuler et al, 2012; Yang, Shih et al, 2012.
Ms. LT: Treatment Selection
The patient is treated with erlotinib, first line Dose is 150 mg daily on an empty stomach Most common toxicities in erlotinib arm:
– Papulopustular rash: 80% (grade 3= 13%)
– Diarrhea: 57% (grade 3=5%)
– Fatigue: 57% (grade 3=6%)
– Anorexia 31% (grade 3=0%)
Rosell et al, 2012.
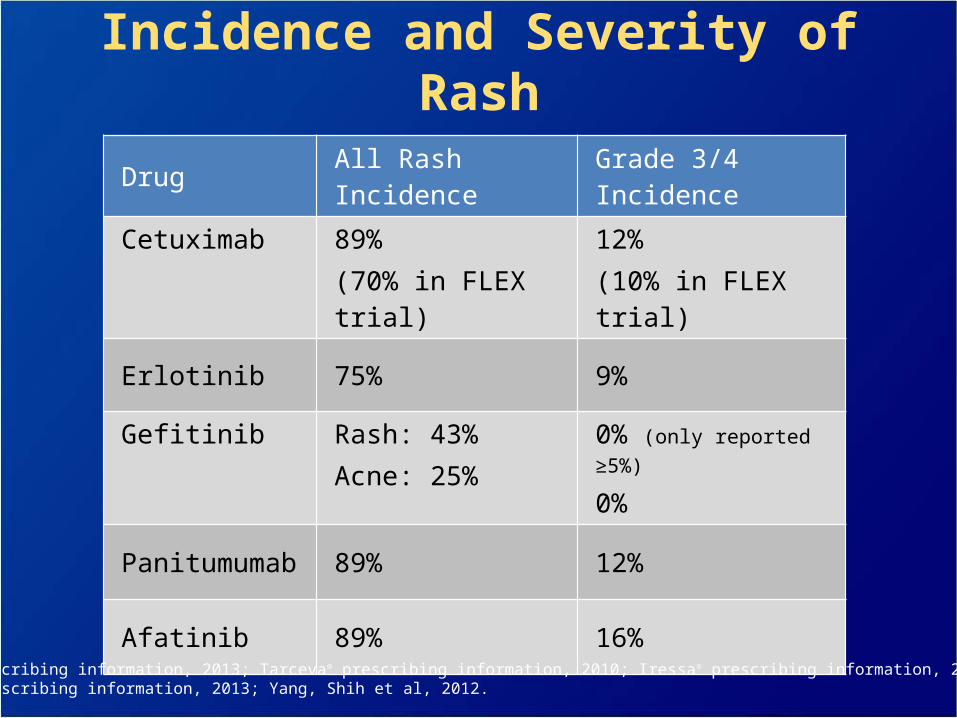
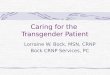
Incidence and Severity of Rash
Drug All Rash Incidence Grade 3/4 Incidence
Cetuximab 89%(70% in FLEX trial)
12%(10% in FLEX trial)
Erlotinib 75% 9%
Gefitinib Rash: 43%Acne: 25%
0% (only reported ≥5%)
0%
Panitumumab 89% 12%
Afatinib 89% 16%
Erbitux® prescribing information, 2013; Tarceva® prescribing information, 2010; Iressa® prescribing information, 2010; Vectibix® prescribing information, 2013; Yang, Shih et al, 2012.
Strategies to Prevent Dermatologic Toxicities: Pre-Emptive
STEPP in metastatic colorectal cancer patients who received panitumumab-containing regimens
95 total patients:– Significant improvement in EGFR rash and quality of
life with pre-emptive doxycycline and topical hydrocortisone cream.
– At 6 weeks, grade ≥2 skin toxicities were reduced by more than 50% in the pre-emptive arm
STEPP = Skin Toxicity Evaluation Protocol With Panitumumab.Lacouture et al, 2010.
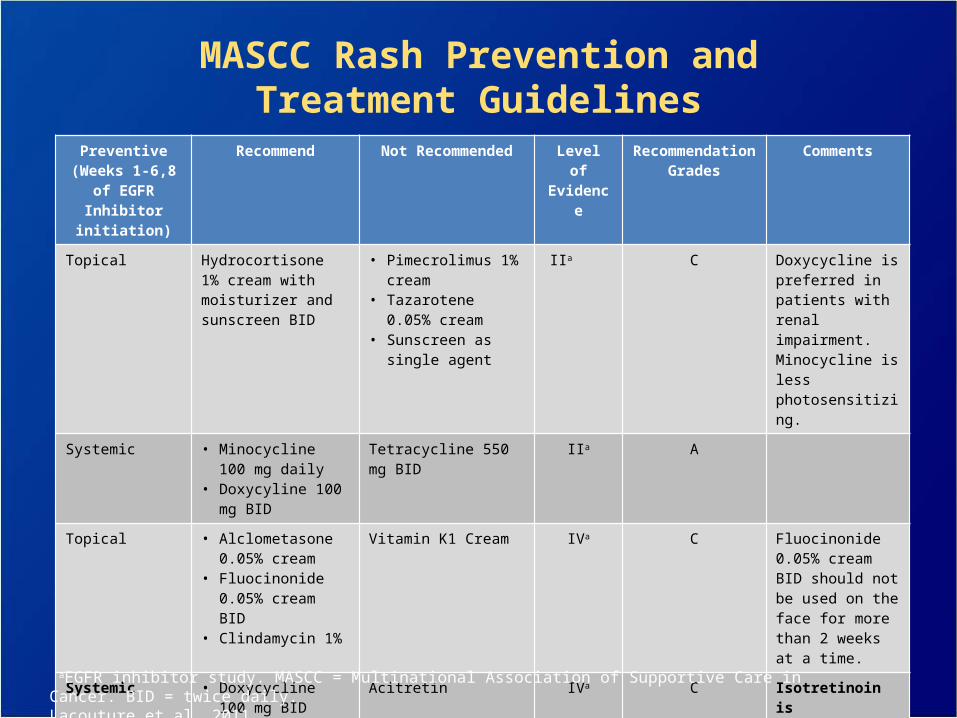
MASCC Rash Prevention andTreatment Guidelines
Preventive(Weeks 1-6,8 of EGFR Inhibitor
initiation)
Recommend Not Recommended Level of Evidence
Recommendation Grades
Comments
Topical Hydrocortisone 1% cream with moisturizer and sunscreen BID
• Pimecrolimus 1% cream
• Tazarotene 0.05% cream
• Sunscreen as single agent
IIa C Doxycycline is preferred in patients with renal impairment. Minocycline is less photosensitizing.
Systemic • Minocycline 100 mg daily
• Doxycyline 100 mg BID
Tetracycline 550 mg BID
IIa A
Topical • Alclometasone 0.05% cream
• Fluocinonide 0.05% cream BID
• Clindamycin 1%
Vitamin K1 Cream IVa C Fluocinonide 0.05% cream BID should not be used on the face for more than 2 weeks at a time.
Systemic • Doxycycline 100 mg BID
• Minocycline 100 mg daily
• Isotretinoin at low doses (20-30 mg/d)
Acitretin IVa C Isotretinoin is photosensitizing and can cause xerosis. Monitor lipids and liver enzymes with retinoids.
aEGFR inhibitor study. MASCC = Multinational Association of Supportive Care in Cancer. BID = twice daily.Lacouture et al, 2011.

Mild Rash
Image courtesy of Beth Eaby-Sandy, MSN, CRNP, OCN®
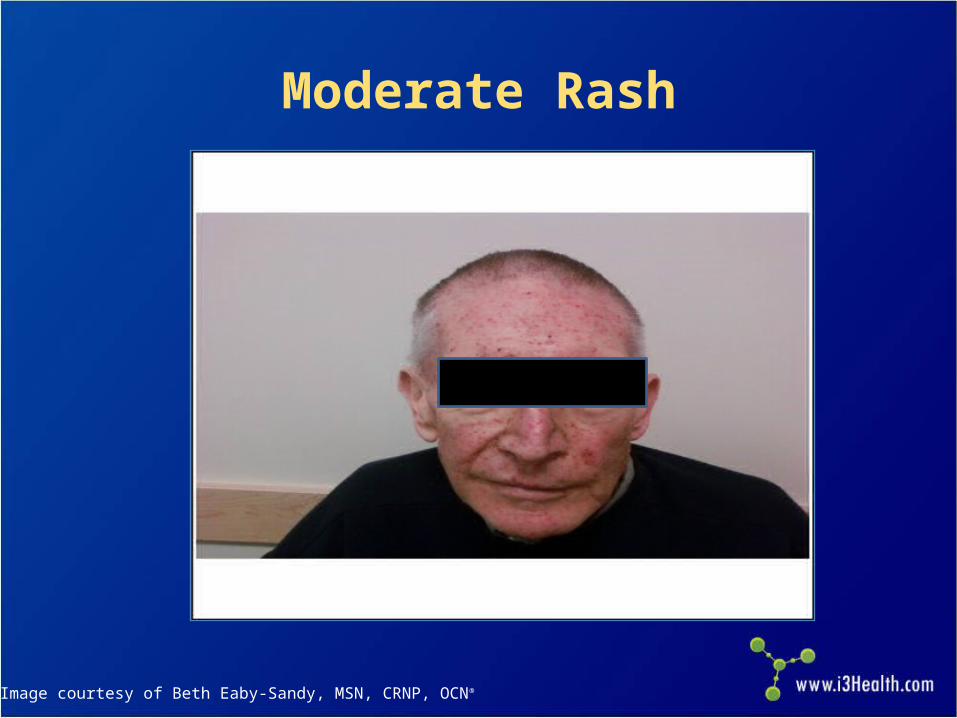
Moderate Rash
Image courtesy of Beth Eaby-Sandy, MSN, CRNP, OCN®

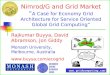
Severe Rash
Image courtesy of Beth Eaby-Sandy, MSN, CRNP, OCN®

Other Cutaneous Toxicities
Alopecia/scalp rash Paronychia Hypertrichosis Fissures
Images courtesy of Beth Eaby-Sandy, MSN, CRNP, OCN®
Case Study: Older Adult With NSCLC

Mr. PD: History
Patient is an 80-year-old fit man who developed increased shortness of breath and cough during the past 6 months, though hemoptysis is what led him to the emergency department
CT scan of the chest reveals a large, central lung mass as well as adrenal metastases
He is a lifelong cigarette smoker, 1 pack per day CT-guided needle biopsy reveals squamous cell
NSCLC

Mr. PD: Diagnostic Evaluation
Brain MRI scan shows a single brain metastasis 1.5 cm, for which he undergoes stereotactic brain radiation
Patient presents to oncology office to decide about treatment options for his cancer
Patient has a supportive wife and daughter; he still plays golf once a week and bridge with his friends on Wednesday nights
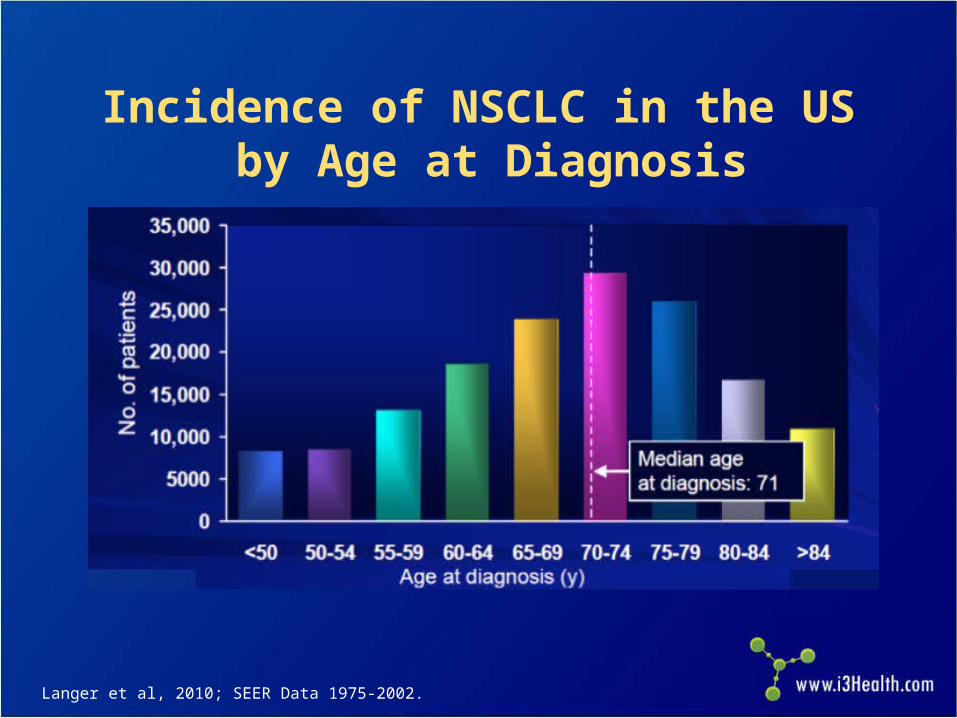
Incidence of NSCLC in the US by Age at Diagnosis
Langer et al, 2010; SEER Data 1975-2002.
Mr. PD: Treatment Considerations
Chemotherapy has survival advantage over best supportive care for the fit elderly
Patient would like to maintain ability to play golf and bridge and spend time with grandchildren
Chemotherapy with platinum-based doublet is an option for him
What can we give him that can maintain quality of life and yet give him chance for increased survival? Family wants him to pursue treatment.
NCCN, 2013.
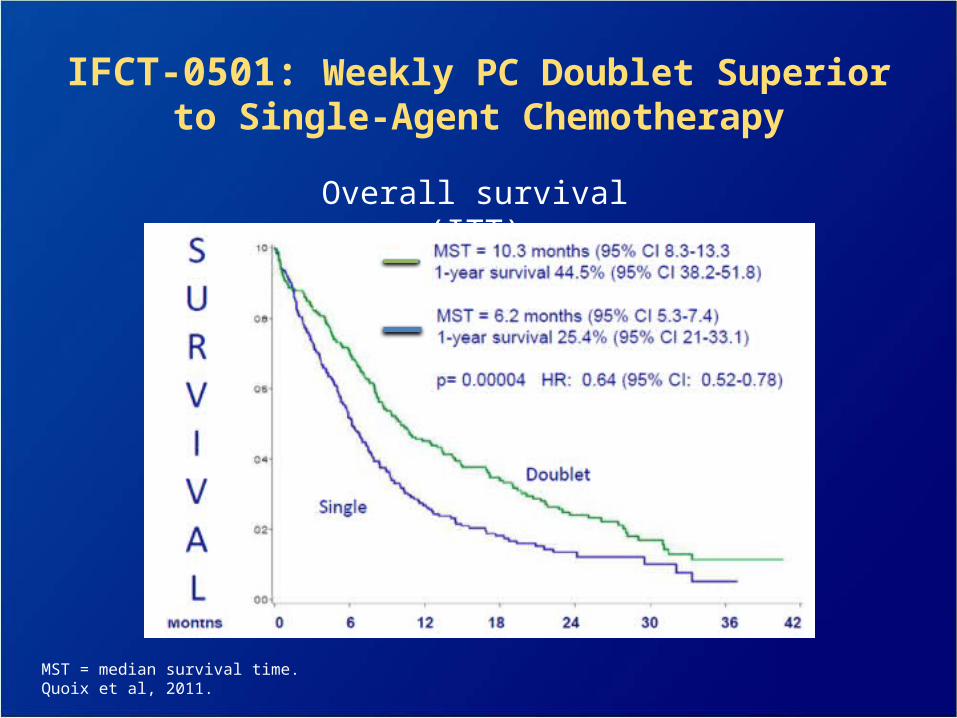
IFCT-0501: Weekly PC Doublet Superior to Single-Agent Chemotherapy
Overall survival (ITT)
MST = median survival time.Quoix et al, 2011.
Which Treatment Regimen to Use?
Toxicity was similar in both arms Weekly paclitaxel/carboplatin a reasonable
treatment option for elderly patients based on 2011 trial data
More recent study examined weeklynab-paclitaxel/carboplatin versus paclitaxel/carboplatin every 3 weeks
Quoix et al, 2011.
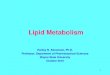
0.75
Pro
bab
ilit
y o
f S
urv
ival
0.50
0.00
30
95% Cl:0.388-0.875HR=0.583
10.4 months
19.9 months
P=0.009
96 15 18 21 2412
0.25
1.00 nab-PC (n=74)
sb-PC (n=82)
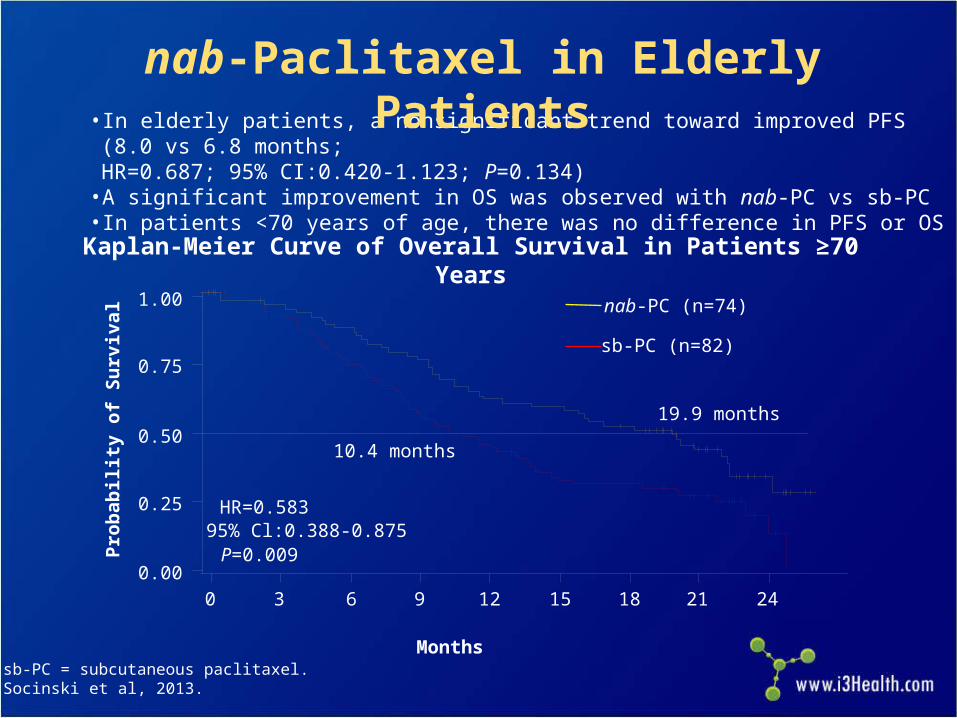
Kaplan-Meier Curve of Overall Survival in Patients ≥70 Years
• In elderly patients, a nonsignificant trend toward improved PFS (8.0 vs 6.8 months; HR=0.687; 95% CI:0.420-1.123; P=0.134)
• A significant improvement in OS was observed with nab-PC vs sb-PC• In patients <70 years of age, there was no difference in PFS or OS
nab-Paclitaxel in Elderly Patients
sb-PC = subcutaneous paclitaxel.Socinski et al, 2013.
Months
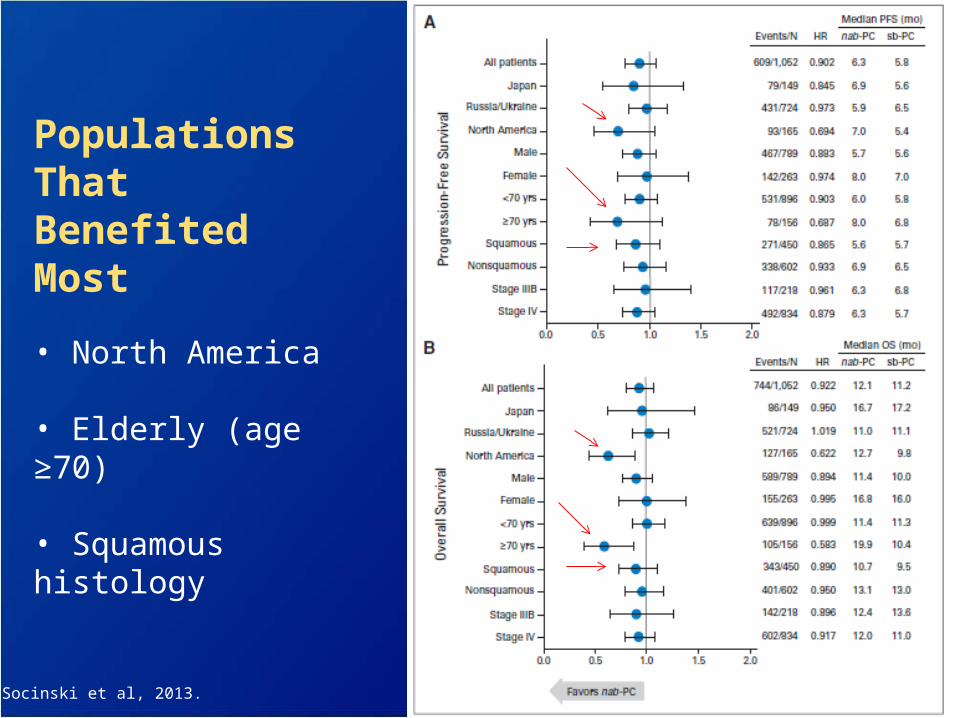
Populations That Benefited Most
• North America
• Elderly (age ≥70)
• Squamous histology
Socinski et al, 2013.

nab-PC sb-PC
Series1
0
1
2
3
4
5
6
1.86
4.99
C2BL
FA
CT
Su
bs
co
re:
Me
an
Ba
se
lin
e S
co
re o
r M
ea
n
Ch
an
ge
Fro
m B
as
eli
ne
C3 C4 C5 C6 C7 C8 Final
Peripheral Neuropathy
Series1
0
0.5
1
1.5
2
2.5
0.70
2.19
C2BL C3 C4 C5 C6 C7 C8 Final
Pain in Hands/Feet
FA
CT
Su
bs
co
re:
Me
an
Ba
se
lin
e S
co
re o
r M
ea
n
Ch
an
ge
fro
m B
as
eli
ne
FACT-Taxane Results in Patients ≥70 Years
Socinski et al, 2013.
Neuropathy in Elderly Patients in nab-Paclitaxel Study

Management of CIPN
Complicating comorbidities, are they under control?
Assessment: FACT-Taxane? DTRs? Vibration testing?
Neurological consult for electromyography?
Several studies evaluating agents such as nortriptyline,
amitriptyline, gabapentin, and lamotrigine have not
shown a benefit, though these agents are often used in
clinical practice
Duloxetine is the only agent shown to diminish CIPN in a
phase III trial
DTRs = deep tendon reflexes; CIPN = chemotherapy-induced peripheral neuropathy.Eaby-Sandy, 2013.
Patient Education Challenges
Explaining targeted therapy versus chemotherapy
Adherence to oral therapies– Cost, Medicare “donut hole”
– Over-adherence vs under-adherence
– Increased clinic visits
– Phone call support
– Logging, pillboxes
– Education on side-effect managementNeuss et al, 2013.

Key Takeaways
Treatment strategies for advanced NSCLC continue to evolve: maintenance, more aggressive treatment for elderly patients
Toxicity profiles can vary significantly depending on selected agent(s)
Oncology nurses play an important role in monitoring for and managing toxicities, as well as providing patient education
References
Alimta® (pemetrexed) prescribing information (2012). Eli Lilly and Company.
American Cancer Society (2013). American Cancer Society: Cancer facts & figures 2013. Atlanta.
Avastin® (bevacizumab) prescribing information (2013). Genentech USA, Inc.
Camidge DR, Bang YJ, Kwak EL, et al (2012). Activity and safety of crizotinib in patients with ALK-positive non-small-cell lung cancer: updated results from a phase 1 study. Lancet Oncol, 13(10):1011-1019.
Cappuzzo F, Ciuleanu T, Stelmakh L, et al (2010). Erlotinib as maintenance treatment in advanced non-small-cell lung cancer: a multicenter, randomized, placebo-controlled phase 3 study. Lancet, 11(6):521-529.
Capuzzo F, Marchetti A, Skokan M, et al (2009). Increased MET gene copy number negatively affects survival of surgically resected non-small-cell lung cancer patients. J Clin Oncol, 27(10):1667-1674.
Ciuleanu T, Brodowicz T, Zielinski C, et al (2009). Maintenance pemetrexed plus best supportive care versus placebo plus best supportive care for non-small-cell lung cancer: a randomised, double-blind, phase 3 study. Lancet, 374(9699):1432-1440.
Eaby-Sandy B (2011). Cancer Nursing: Principals and Practice. Jones and Bartlett Publishers. Sudbury, Massachusetts.
Eaby-Sandy B, Ko A, Renschler et al (2013). Efficacy and toxicity profile of nab-paclitaxel in patients with advanced non-small cell lung cancer (NSCLC): nursing implications and management strategies. Poster presented at Oncology Nursing Society 38th Congress in Washington, DC.
Erbitux® (cetuximab) prescribing information (2013). New York, NY: ImClone Systems, Inc and Princeton, NJ: Bristol-Myers Squibb Co.
Fukuoka M, Wu YL, Thongprasert S, et al (2011). Biomarker analyses and final overall survival results from a phase III, randomized, open-label, first-line study of gefitinib versus carboplatin/paclitaxel in clinically selected patients with advanced non-small-cell lung cancer in Asia (IPASS). J Clin Oncol, 29(21):2866-2874.
References
Hirsch FR (2012). Recent advances in biomarker research in lung cancer with special reference to new targeted therapies. Presented at: 13th International Lung Cancer Congress; July 19-22, 2012; Huntington Beach, CA.
Iressa® (gefitinib) prescribing information (2010). Wilmington, DE: AstraZeneca Pharmaceuticals LP.
Lacouture ME, Anadkat MJ, Bensadoun RJ, et al (2011). Clinical practice guidelines for the prevention and treatment of EGFR inhibitor-associated dermatologic toxicities. Support Care Cancer, 19(8):1079-1095.
Lacouture ME, Mitchell EP, Piperdi B, et al (2010). Skin toxicity evaluation protocol with panitumumab (STEPP), a phase II, open-label, randomized trial evaluating the impact of a pre-Emptive Skin treatment regimen on skin toxicities and quality of life in patients with metastatic colorectal cancer. J Clin Oncol, 28(8):1351-1357.
Langer CJ, Besse B, Gualberto A, et al (2010). The evolving role of histology in the management of advanced non-small cell lung cancer. J Clin Oncol, 28(36):5311-5320.
National Comprehensive Cancer Network (NCCN) (2013). Clinical practice guidelines in oncology. Non-small cell lung cancer. V.2.2013. Available at http://www.nccn.org.
Neuss MN, Polovich M, McNiff K, et al (2013). 2013 updated American Society of Clinical Oncology/Oncology Nursing Society chemotherapy administration safety standards including standards for the safe administration and management of oral chemotherapy. J Oncol Practice, 9(Suppl):5S-13S.
Paz-Ares L, de Marinis F, Dediu M, et al (2012). Maintenance therapy with pemetrexed plus best supportive care versus placebo plus best supportive care after induction therapy with pemetrexed plus cisplatin for advanced non-squamous non-small-cell lung cancer (PARAMOUNT): a double-blind, phase 3, randomised controlled trial. Lancet Oncol, 13(3):247-255.
References
Quoix E, Zalcman G, Oster JP, et al (2011). Carboplatin and weekly paclitaxel doublet chemotherapy compared
with monotherapy in elderly patients with advanced non-small-cell lung cancer: IFCT-0501 randomised, phase 3
trial. Lancet, 378(9796):1079-1088.
Rodriguez E, Lilenbaum RC (2008). New treatment strategies in patients with advanced non-small-cell lung cancer
and performance status 2. Clin Lung Cancer, 9(6):326-330.
Rosell R, Carcereny E, Gervais R, et al (2012). Erlotinib versus standard chemotherapy as first-line treatment for
European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre,
open-label, randomised phase 3 trial. Lancet Oncology, 13(3):239-246.
Sandler A, Graham C, Baggstrom M, et al (2011). An open-label, multicenter, three-stage, phase II study of s-1 in
combination with cisplatin as first-line therapy for patients with advanced non-small cell lung cancer. J Thoracic
Oncol, 6(8):1400-1406.
Sandler A, Gray R, Perry MC, et al (2006). Paclitaxel-carboplatin alone or with bevacizumab for non-small-cell
lung cancer. N Engl J Med, 355(24):2542-2550.
Patel JD, Socinski MA, Garon EB, et al (2012). A randomized, open-label, phase III, Label, Phase III, superiority
study of pemetrexed (Pem) + carboplatin (Cb) + bevacizumab (Bev) followed by maintenance Pem + Bev versus
paclitaxel (Pac) Cb + Bev followed by maintenance Bev in patients with sage IIIB or IV non-squamous non-cmall
cell lung cancer (NS-NSCLC). Available at:
http://www.thoracicsymposium.org/MeetingProgram/documents/PLPatel.pdf.
Scagliotti GV, Novello S (2003). Pemetrexed and its emerging role in the treatment of thoracic malignancies.
Expert Opin Investig Drugs, 12(5):853-863.

References
Scagliotti GV, Parikh P, von Pawel J, et al (2008). Phase III study comparing cisplatin plus gemcitabine with cisplatin plus pemetrexed in chemotherapy-naive patients with advanced-stage nonsmall-cell lung cancer . J Clin Oncol, 20;26(21):3543-3551.
Schiller JH, Harrington D, Belani CP, et al (2002). Comparison of four chemotherapy regimens for advanced non-small-cell lung cancer. N Engl J Med, 346(2):92-98.
Socinski MA, Langer CJ, Okamoto I, et al (2013). Safety and efficacy of weekly nab®-paclitaxel in combination with carboplatin as first-line therapy in elderly patients with advanced non-smallvcell lung cancer. Ann Oncol, 24(2):314-321.
Tarceva® (erlotinib) [prescribing information] (2010). Melville, NY: OSI Pharmaceuticals, Inc.
Temel JS, Greer JA, Admane S, et al (2011). Longitudinal perceptions of prognosis and goals of therapy in patients with metastatic non-small-cell lung cancer: results of a randomized study of early palliative care. J Clin Oncol. 29(17):2319-2326.
Temel JS, Greer JA, Muzikansky A, et al (2010). Early palliative care for patients with metastatic non-small cell lung cancer. N Engl J Med, 363(8):733-742.
Vectibix® (panitumumab) prescribing information] (2013). Thousand Oaks, CA: Amgen, Inc.
Yang JC, Schuler MH, Yamamoto N, et al (2012). LUX-Lung 3: A randomized, open-label, phase III study of afatinib versus pemetrexed and cisplatin as first-line treatment for patients with advanced adenocarcinoma of the lung harboring EGFR-activating mutations. J Clin Oncol, 30(18 Suppl). Abstract LBA7500.
Yang JC, Shih JY, Su WC, et al (2012). Afatinib for patients with lung adenocarcinoma and epidermal growth factor receptor mutations (LUX-Lung 2): a phase 2 trial. Lancet Oncol, 13(5):539-548.