Embed Size (px)
Citation preview

OPTIMIZING FUNCTIONAL OUTCOMES IN SCHIZOPHRENIA: MANAGING NEGATIVE SYMPTOMS, COGNITIVE IMPAIRMENT, AND ADVERSE EFFECTS

Learning Objectives
• Implement evidence-based strategies to address the negative symptoms of schizophrenia
• Examine evidence-based strategies to address the cognitive symptoms of schizophrenia
• Apply pre-emptive and monitoring strategies to mitigate the impact of adverse effects
• Evaluate the status of plasma monitoring and long-acting injectables (LAIs) with treatment adherence

Patients can't achieve functional outcomes without relief of negative symptoms.
• Difficulty forming a therapeutic alliance
• Impaired occupational functioning• Impaired social functioning• Impairment in relationships
• Reduced quality of life
Velligan DI et al. J Clin Psychiatry 2009;70(suppl 4):1-46;Milev P et al. Am J Psychiatry 2005;162:495-506.
Reduced speech
Limited eye contact
Reduced interest
Poor grooming
Reduced emotional responsiveness
Reduced social drive

Treatments of Negative Symptoms in Schizophrenia:Meta-Analysis
Fusar-Poli P et al. Schizophr Bull 2015;41(4):892-9.
statistical significance
clinical significance

substantia nigra
striatum
VTA
nucleus accumbens
DLPFC
VMPFChypothalamus
pituitary
thalamus
Why aren't negative symptoms sufficiently improved with dopamine 2 antagonists?
mesolimbic
Stahl SM. Stahl's Essential Psychopharmacology. 4th ed; 2013.

substantia nigra
striatum
VTA
nucleus accumbens
DLPFC
VMPFChypothalamus
pituitary
thalamus
Why aren't negative symptoms sufficiently improved with dopamine 2 antagonists? (cont.)
mesolimbic
reward circuitsmesocortical
Stahl SM. Stahl's Essential Psychopharmacology. 4th ed; 2013.

In the striatum
VMAT2
D2/3autoreceptorDA
DAT
D1 D2 D3 D4 D5
In the prefrontal cortex
D1 D1 D1 D1 D1
VMAT2
DA
Overview of the Dopamine Synapse
Stahl SM. CNS Spectrums 2017;22:305-11.

Functional Output of Cortical Dopamine and Cognition
Cog
nitiv
e pe
rfor
man
ce
Dopamine levels (PFC)
Blocking D1 Blocking D3
Stahl SM. CNS Spectrums 2017;22:305-11.

Dopamine Receptor Affinities
K (n
M) f
or d
opam
ine
Dopamine receptorD1 D2 D3 D4 D5
1
10
100
1,000
10,000
Stahl SM. CNS Spectrums 2017;22:305-11.

Regulation of Dopamine Levels at the Synapse
D1D2 D3 D4 D5 D1
D2 D3 D4 D5
VMAT2 VMAT2
D2auto-receptor
D3auto-receptor
Stahl SM. CNS Spectrums 2017;22:305-11.

Receptor affinities dictate neuronal response totonic and phasic firing.
VMAT2 VMAT2
- Slow, irregular- Sets background DA level
- Rapid, synchronous burst- Spike in extracellular DA
Tonic firing Phasic firing
Stahl SM. CNS Spectrums 2017;22:305-11.

1 order of magnitude higher
affinity than for D2
2 orders of magnitude higher
affinity than for D2
3 orders of magnitude higher
affinity than for D2
3 orders of magnitude lower affinity than for
D2
2 orders of magnitude lower affinity than for
D2
1 order of magnitude lower affinity than for
D2
Blonanserinbinding affinity
for D3 (0.49nM)
Brexpiprazolebinding affinity for D3 (1.1nM)
Asenapinebinding affinity for D3 (1.8nM)
Paliperidonebinding affinity for D3 (2.6nM)Aripiprazole
binding affinity for D3 (4.6nM)Risperidone
binding affinity for D3 (7.3nM)Ziprasidone
binding affinity for D3 (7.3nM)
Iloperidonebinding affinity
for D3 (10.5nM)
Lurasidonebinding affinity
for D3 (15.7nM)
Olanzapinebinding affinity
for D3 (38.1nM)
Clozapinebinding affinity for D3 (310nM)Quetiapine
binding affinity for D3 (394nM)
Drugbinding
affinity for D2 (Ki)
D3
Cariprazinebinding affinity
for D3 (0.09nM)

Conclusions
• Most antipsychotics have about the same affinity for D3 receptors as they have for D2 receptors
• Cariprazine has somewhat higher affinity for D3 receptors than for D2 receptors
• Lurasidone, brexpiprazole, and iloperidone have lower affinity for D3 receptors than for D2 receptors

So what?
• It’s not about an antipsychotic’s relative affinities for D1 and D3 receptors compared to D2 receptors
• At antipsychotic doses, and in the presence of dopamine…it’s about an antipsychotic’s relative affinity for dopamine receptors compared to Dopamine’s affinity for those receptors
• The one with the highest affinity “wins”

Cariprazinebinding
affinity for D2(0.49nM)
Blonanserinbinding
affinity for D2(0.14nM)
Brexpiprazolebinding affinity
for D2(0.3nM)
Asenapinebinding
affinity for D2(1.7nM)
Paliperidonebinding
affinity for D2(1.4nM)
Aripiprazolebinding
affinity for D2(2.3nM)
Risperidonebinding
affinity for D2(3.7nM)
Ziprasidonebinding
affinity for D2(4.75nM)
Iloperidonebinding
affinity for D2(8.3nM)
Lurasidonebinding
affinity for D2(0.66nM)
Olanzapinebinding
affinity for D2(30.8nM)
Clozapinebinding
affinity for D2(147nM)
Quetiapinebinding
affinity for D2(437nM)
DABinding
affinity for D2 (Ki
=540nm)
1 order of magnitude
higher affinity than DA
2 orders of magnitude
higher affinity than DA
3 orders of magnitude
higher affinity than DA
3 orders of magnitude
lower affinity than DA
2 orders of magnitude
lower affinity than DA
1 order of magnitude
lower affinity than DA

Conclusions
• Every antipsychotic has the same or higher affinity for D2 receptors as dopamine has for D2 receptors
• Not surprising, because if they didn’t they wouldn’t be antipsychotics
• However…

Dopamine can displace antipsychotics from D2.
Basal dopamine levels
Dopamine overflow was stimulated by amphetamine injection (0.2 mg/kg) in schizophrenia patients
PET scan in patients with schizophrenia before and after amphetamine stimulation
Elevated dopamine levels
[11C]-raclopride
bound to D2100%
0%
[11C]-racloprideDopamine
Breier A et al. PNAS 1997;94:2569-74.

Antagonist/Partial Agonist Effects at D2 Dopamine Receptors
Dysregulation of D2-mediatedsignaling in the motor striatumcan result in EPS
This mitigates the effects ofoveractive mesolimbic dopamine,reducing positive symptoms
D2 antagonists block and inhibit activity of postsynaptic D2 receptors
Prefrontal cortex
Nucleusaccumbens
Ventraltegmentalarea
Mesolimbic dopaminepathway
Therapeuticeffects
GABA neuron
D2
D2
HyperactiveDA inputs from VTA
Motor striatum Side
effects
Stahl SM. CNS Spectrums 2017;22:375-84.

Cariprazinebinding
affinity for D3(0.09nM)
Blonanserinbinding
affinity for D3(0.49nM)
Brexpiprazolebinding affinity
for D3(1.1nM)
Asenapinebinding affinity
for D3(1.8nM)
Paliperidonebinding
affinity for D3(2.6nM)
Aripiprazolebinding
affinity for D3(4.6nM)
Risperidonebinding
affinity for D3(7.3nM)
Ziprasidonebinding
affinity for D3(7.3nM)
Iloperidonebinding
affinity for D3(10.5nM)
Lurasidonebinding
affinity for D3(15.7nM)
Olanzapinebinding affinity
for D3(38.1nM)
Clozapinebinding affinity
for D3(310nM)
Quetiapinebinding
affinity for D3(394nM)
DABinding
affinity for D3 (Ki
=60nm)
1 order of magnitude
higher affinity than DA
2 orders of magnitude
higher affinity than DA
3 orders of magnitude
higher affinity than DA
3 orders of magnitude
lower affinity than DA
2 orders of magnitude
lower affinity than DA
1 order of magnitude
lower affinity than DA

Conclusions
• Almost all antipsychotics have about the same affinity for D3 receptors as dopamine, resulting in little net D3 blockade in the presence of dopamine and at antipsychotic doses
• However, two antipsychotics have even higher affinity for D3 receptors than dopamine does, and do result in net blockade of D3 receptors
• cariprazine > blonanserin

Who cares if you block D3 receptors?
• Increased dopamine delivery to prefrontal cortex and possibly limbic striatum
• Disinhibition of D3 autoreceptors, especially in the VTA/SN
• Enhancement of mood, cognition, negative symptoms, apathy, anhedonia?

Antagonist/Partial Agonist Effects at D3 Dopamine Receptors
Prefrontal cortex
Nucleusaccumbens
Ventraltegmentalarea
Gluneuron
D1D1
D3
This results in an increase in DArelease in the PFC
D3 antagonists/partial agonists block and inhibit the activity of somatodendritic D3 receptors
Increased DA release in the PFC re-regulates aberrant cortical activity and could theoretically improve negative symptoms and cognitive impairment
Stahl SM. CNS Spectrums 2017;22:375-84.

Summary: Antipsychotic Binding at Dopamine Receptors
brexpiprazolepaliperidonearipiprazolerisperidone
ziprasidoneiloperidonelurasidonequetiapine
asenapineolanzapineclozapine
cariprazineblonanserin
D2
D1 D2 D3
predominately D2
D2D1
D1 D2 D3
Plus D1
D2D3
D1 D2 D3
Plus D3
Stahl SM. CNS Spectrums 2017;22:375-84.

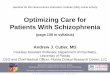
D3 (Cariprazine) vs. D2 (Risperidone)for Negative Symptoms
Nemeth G et al. Lancet 2017;389:1103-13.Week0 5 10 15 20 25 30
0-1-2-3-4-5-6-7-8-9
-10
Leas
t squ
ares
mea
n ch
ange
from
ba
selin
e in
PAN
SS-F
SNS
*p=0.0079 **p=0.0011 ***p=0.0016 ****p=0.0022
p=0.0092 for the overall treatment effect of
cariprazine versus
risperidone
* ** *** ****cariprazine (n=230)risperidone (n=231)

D3 (Cariprazine) vs. D2 (Risperidone)for Negative Symptoms (cont.)
Nemeth G et al. Lancet 2017;389:1103-13.Week0 5 10 15 20 25 30
16
128
4
0
Leas
t squ
ares
mea
n ch
ange
from
ba
selin
e in
PSP
tota
l sco
re *p=0·0053. **p=0·0046. ***p=0.0004† p<0.0001‡ p<0.0001
PSP: Personal and
socialperformance
*
†‡cariprazine (n=230)
risperidone (n=231)
*****

Treatment of Negative Symptoms:Other Strategies
• Exercise - Meta-analyses show moderate effect of aerobic exercise and yoga
• Music therapy - Meta-analysis show large significant effect compared to treatment as usual (TAU)
• Cognitive behavioral therapy - Recent meta-analysis of 30 studies did not find beneficial effect
• Cognitive remediation therapy (CRT)• High frequency repetitive transcranial magnetic
stimulation (HF-rTMS)
Veerman SRT et al. Drugs 2017;77:14723-59. Cella M et al. Clin Psych Rev 2017;52:43-51.

CRT Effectiveness
• Current evidence suggests that CRT is associated with both neurobiological and cognitive improvement in patients with schizophrenia
• Studies indicate that CRT affects several brain regions and circuits, including prefrontal, parietal, and limbic areas, both in terms of activity and structure
• Changes to prefrontal areas are the most reported finding, fitting to previous evidence of dysfunction in this region
Thorsen et al. Frontiers in Psychiatry 2014;5(103):1-9.

Neuroimaging and CRT
• CRT group exhibited significantly greater improvements than the TAU group in verbal fluency (p=0.012)
• CRT group demonstrated significantly greater improvements than the TAU group in global cognitive scores (p=0.049)
• CRT group also exhibited significantly greater hippocampal volume than in the TAU group (p <0.001)
• Changes in verbal fluency scores and right hippocampal volumes were positively correlated
• Results suggest that CRT induces cognitive improvement through hippocampal plasticity
Morimoto et al., BMC Psychiatry 2018;18(83):1-8.

Transcranial Magnetic Stimulation for Treatment of Schizophrenia
• Recent pilot study: bilateral high frequency repetitive transcranial magnetic stimulation (HF-rTMS) on cognitive function in patients with early-phase psychosis
• Over 2 weeks, 21 subjects underwent ten sessions of HF, bilateral, sequential rTMS over the dorsolateral prefrontal cortex (DLPFC) or sham
• Participants completed a cognitive assessment and MRI prior to and after completion of the study • Those who received rTMS displayed improvement on a standardized cognitive battery test both
immediately following the course of study treatment and at follow-up two weeks later• MRI results indicated that left frontal cortical thickness at baseline was correlated with treatment
response • Study treatment was safe and well tolerated • rTMS may be an effective treatment of cognitive dysfunction in the early phase of psychosis
Francis et al. Brain Imaging Behavior 2018; doi.org/10.1007/s11682-018-9902-4.

Transcranial Magnetic Stimulation for Treatment of Cognitive Impairment in Schizophrenia
Cognitive assessment at
baseline
MRI at baseline
2 weeks; ten sessions HF, bilateral sequential rTMS
over DLPFC or sham
Cognitive assessment
at end of study MRI at
end of study
Pilot study: 21 participants
Results: • rTMS improved scores on standardized cognitive battery test both immediately after study
treatment and at follow-up two weeks after • MRI results indicated that left frontal cortical thickness at baseline was correlated with
treatment response
Francis et al. Brain Imaging Behavior 2018; doi.org/10.1007/s11682-018-9902-4.

MANAGING ADVERSE EFFECTS

Monitoring Challenging Adverse Effects
• Antipsychotic (AP)-related weight gain
• Extrapyramidal Symptoms (EPS)
• Akathisia

Weight Gain & Antipsychotics
• Most antipsychotics• Younger and AP naive patients are
more sensitive
• Tip: don’t just look at mean change in weight; also look at proportion of patients in each group who gained or lost ≥ 7% of baseline body weight
• Tip: must compare to placebo
• Mechanisms: H1 or 5HT2C blockade

Weight Gain Management: Let’s Prescribe Metformin More Often
• Metformin reduces weight, BMI, fasting glucose, fasting insulin, triglycerides, and total cholesterol
• Of treatments for antipsychotic-induced weight gain/metabolic abnormalities, metformin was the most effective
• Average weight loss: 6.5 lbs• Hypoglycemia is rare with metformin, and the risk of lactic acidosis
is extremely low until eGFR is < 30 mL/min• Reevaluate metformin if eGFR < 45 mL/min, and stop if < 30 mL/min
Zheng et al., 2015 (PMID: 26280837). Maayan et al., 2010 (PMID: 20336059); Kirpichnikov et al., 2002 (PMID: 12093242); Lipska KJ Diabetes Care 2011; 34: 1431-37 (PMID 21617112).

Metformin: for Whom
• Metformin works whether or not there is increased blood sugar or hemoglobin A1C
• Who is most likely to respond? 1. Younger patients 2. Recently started on the antipsychotic3. Before weight gain (to prevent it)4. Early on if weight gain occurs
Standard titration: 500 mg qam the first week. Increase by 500 mg/wk if tolerated to 1000 mg BID. Use extended release formulation if GI adverse effects.
Jarskog et al., 2013 (PMID: 23846733);Hasnain and Viewing, 2013 (PMID: 23659558).

Combination of Metformin and Lifestyle Intervention
• Recent meta-analysis of six RCTs: metformin, placebo, or metformin and lifestyle combination (MLC)
• MLC group had significant reduction in weight and body mass index
• Less frequent weight gain of ≥ 7% in the MLC group over placebo
• No other group differences in total adverse drug reactions, total psychopathology, and all-cause discontinuation
• Combining metformin and lifestyle intervention significantly reduces AP-related weight gain
Zheng et al. Pharmacopsychiatry 2018;Epub ahead of print.

Weight Gain Management: Topiramate
• Eight RCTs for weight gain on second-generation antipsychotics
• Mean decrease in weight: 6.2 lbs
• Which (again) means—many of the patients lost more than that
Mahmood et al., 2013 (PMID: 23277264).

Weight Gain Management: Topiramate Considerations
BUT:
• Cognitive dulling
• Risk of renal stones
• Drug interactions
Ellinger et al., 2010 (PMID: 20233913).

What are extrapyramidal signs (EPS) and extrapyramidal side effects (EPSE)?
• Movement disorders that occur with antipsychotics
• Thought to involve structures outside of the pyramidal tract
• Occur in acute and late (tardive) forms
• Reason for the older term "neuroleptic" to describe antipsychotics

Extrapyramidal Side Effects• Acute extrapyramidal side effects
• Dystonia• Disturbance in muscle tone leading to prolonged contractions of muscle
groups• Occurs within 24–48 hours of antipsychotic initiation• Only acute EPS that is less common in the elderly
• Parkinsonism• Classic triad of bradykinesia, rigidity, and tremor• Occurs within days of starting treatment or dose increase in 1/4 to 1/3
of patients• Can occur in up to 75% of older patients

Pathophysiology and Treatment• Pathophysiology
• Due to D2 blockade in the dorsal striatum
• Treatment• Reduction in dose• Anticholinergics and other antiparkinsonians (e.g., amantadine) until
plasma antipsychotic levels have been reduced below the threshold for motor adverse effects
• Chronic anticholinergic treatment should be avoided due to adverse cognitive effects and increased ileus risk

Akathisia: Subjective Symptoms
• Often extraordinarily difficult for the patient to describe, to some extent, because there are few subjective states to which it can be compared
• Patients often use terms such as "anxiety" or "itching," although these do not really capture the essence of the condition
• Since many clinicians have never experienced it, there is often a lack of common ground in communicating the problem

Hypothesized Mechanism of Akathisia:the Role of the Nucleus Accumbens
Cg1: cingulate gyrus, 1. OFC: orbitofrontal cortex. IL: infralimbic cortex. NAcbC: nucleus accumbens core. NAcbS: nucleus accumbens shell.
VTA: ventral tegmental area. LC: locus coeruleus.Stahl et al. CNS Spectrums 2011: www.neiglobal.com.

Akathisia: Rates in FDA Registrational TrialsAgent Incident Rates of Akathisia for SchizophreniaAripiprazole 10-13% monotherapy; 19-25% with lithium, divalproex, or
antidepressantsAsenapine 4-11%Brexpiprazole 4-7% (dosed 1-4 mg/day)Cariprazine 9-14%Clozapine 3%Iloperidone 1-2%Lurasidone 6-22%Olanzapine 3%Paliperidone 6-9%Quetiapine 1-4%Risperidone 5-9%Ziprasidone 8-10%
BP: bipolar depression. MDD: major depressive disorder. SZ: schizophrenia.Goldberg, Ernst. Managing the Side Effects of Psychotropic Medications. 2012.

Treatment Strategies for Akathisia
• Dosage reduction
• Change to lower-risk agents if feasible
• Withdrawal akathisia can occur; allow at least 6 weeks before judging effectiveness of dose reduction/medication switch
• Adjunctive medications
Goldberg, Ernst. Managing the Side Effects of Psychotropic Medications. 2012.

Adjunctive Treatment Strategies for Akathisia
• Centrally-acting beta blockers• Propranolol: nonselective, lipophilic. Dose: 30-90 mg/day: start at 10
mg BID, increase by 10 mg BID increments as tolerated • Betaxolol: beta1, selective, lipophilic 10-20 mg/day
• Mirtazapine: 5HT2A antagonist property helps mitigate akathisia • 15 mg/day is the most common mirtazapine dose studied; unclear if
higher doses are more effective. Avoid if h/o mania
• Clonazepam• Anticholinergics (e.g., benztropine): appear less effective than other agents,
and carry the anticholinergic burden. Generally avoided
Rathbone and Soares-Weiser, 2006 (PMID: 17054182); Laoutidis and Luckhaus, 2014 (PMID: 24286228); Poyurovsky et al., 2006 (PMID: 16497273).

Reverberations From Side Effects
• Weiden PJ, Buckley PF. J Clin Psychiatry 2007;68(suppl 6):14-23.
Side effectappears
Subjective distress
Objective severity
Adherence impact
Safety and risk
How patient and clinician responses may differ

Considering the Side Effect Profile When Choosing a Treatment
• Important because side effects may:• Contribute to treatment nonadherence• Limit return to maximal levels of social functioning• Potentially contribute to long-term morbidity
• Atypical antipsychotics are better tolerated than typical antipsychotics (mainly due to decreased EPS)
• Differences in drug-specific adverse effect profiles, including metabolic effects, may impact treatment adherence and long-term outcomes
Velligan DI et al. J Clin Psychiatry 2009;70(suppl 4):1-46; Tandon R. Psychiatr Q 2002;73(4):297-311.

NONADHERENCE AND PLASMA LEVELS

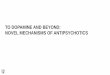
Rates of RelapseWith Continued vs. Discontinued Treatment
Chen EYH et al. BMJ 2010;310:c4024. Farooq et al. Br J Psychiatry 2011;199:467-72.
178 asymptomatic patients treated for ≥1 year with AP and randomized to quetiapine 400 mg/day (n=89) or placebo (n=89).1
50% of patients become nonadherent within 1 year of hospital discharge2
quetiapine vs. placebo: p<0.001

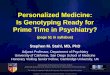
We Are Not Good at Estimating Adherence:Clinician Assessment vs. Plasma Levels
Among 105 patients admitted to a US psychiatric hospital previously on antipsychotics:
Antipsychotic: risperidone, olanzapine, quetiapine, paliperidone, aripiprazoleLopez LV et al. J Clin Psychopharmacology 2017;37:310-14.
Therapeutic plasma levels
34%
Sub-therapeutic plasma levels
66%
67%52%
Staff correctly identified:Staff correctly identified:

Many treatment-resistant patients have subtherapeutic plasma levels.
Study 1: Antipsychotic plasma levels were measured in 36 outpatients identified as having treatment-resistant schizophrenia by their treating clinicians in the UK. 44% of patients showed subtherapeutic levels, 43% of which were undetectable. 56% of patients had levels in the therapeutic range.
Study 2: Antipsychotic plasma levels were measured in 99 outpatients identified as having treatment-resistant schizophrenia by their treating clinicians in the UK. 35% of patients showed subtherapeutic levels, 34% of which were undetectable. 65% of patients had levels in the therapeutic range.
McCutcheon R., et al. Journal of Psychopharmacology 2015; 29(8) 892–897; McCutcheon R, et al. Antipsychotic plasma levels in the assessment of poor treatment response in schizophrenia. Acta Psychiatr Scand 2018; 137(1): 39-46.

Which antipsychotics are recommended for plasma level monitoring?
Usual Doses to Achieve 60–80% D2 Receptor OccupancyUsual dose range (mg/d)* Rec plasma levels (ng/mL)1
Aripiprazole 15–30 150–500Clozapine 300–450 350–700Fluphenazine 0.5–10 0.8–2.0Haloperidol 1–40 3–20Olanzapine 10–20 20–80Paliperidone 3–6 20–60Perphenazine 2–8 20–60Risperidone 2–8 20–60Ziprasidone 40–200 50–200
*In schizophreniaHiemki C et al. Pharmacopsychiatry 2011;44(6):195-235;
Potkin SG et al. CNS Spectrums 2014;19(2):176-81.

Dosing/Plasma Levels for Newer Antipsychotics
Usual Doses to Achieve 60–80% D2 Receptor OccupancyUsual dose range (mg/d)* Rec plasma levels (ng/mL)1
Asenapine 10–20 2–5Brexpiprazole 2–4 ?Cariprazine 1.5–6 ?Iloperidone 12–24 5–10Lurasidone 40–160 >702
Quetiapine 400–800 Not reliable or used
*In schizophreniaHiemki C et al. Pharmacopsychiatry 2011;44(6):195-235;
Potkin SG et al. CNS Spectrums 2014;19(2):176-81.

Obtaining Plasma Levels
• 12-hour trough• For patients on twice/day dosing, make sure they
hold the morning dose until the AM trough is obtained
• Levels may fluctuate up to 30% in adherent patients
• Greater fluctuations likely reflect nonadherence or kinetic issues

Technology-Based Services
• Text reminders• Two studies found that 3–4 texts/day (about adherence,
socialization, and hallucinations) significantly improved adherence in patients living independently for up to 6 months
• Phone calls• Weekly calls led to significantly higher adherence
• Electronic pill counters• Adherence rate of 67% at 6 weeks
• Tracking devices?
Haddad et al. Patient Related Outcome Measures. 2014; 5(43): 43-62.

Summary• D3 antagonism is a potential mechanism for reducing negative
symptoms• Other pharmacological mechanisms are being investigated, but so
far nothing shows robust efficacy• Established psychosocial methods may effectively treat cognitive
symptoms of schizophrenia• Nonpharmacological methods are on the horizon (e.g., TMS) for
treating cognitive symptoms of schizophrenia• There are many medications available to effectively manage
adverse effects associated with antipsychotics• Adherence can be optimized with careful monitoring