Embed Size (px)
Citation preview

Optimizing Empirical Antimicrobial Therapy for Infection due to Gram‐Negative Pathogensin the Intensive Care Unit: Utility of a Combination Antibiogram • Author(s): Jennifer Christoff, MD; Jocelyn Tolentino, MPH; Emily Mawdsley, MD;Scott Matushek, MS; David Pitrak, MD; Stephen G. Weber, MD, MSSource: Infection Control and Hospital Epidemiology, Vol. 31, No. 3 (March 2010), pp. 256-261Published by: The University of Chicago Press on behalf of The Society for Healthcare Epidemiologyof AmericaStable URL: http://www.jstor.org/stable/10.1086/650446 .
Accessed: 18/05/2014 00:32
Your use of the JSTOR archive indicates your acceptance of the Terms & Conditions of Use, available at .http://www.jstor.org/page/info/about/policies/terms.jsp
.JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
.
The University of Chicago Press and The Society for Healthcare Epidemiology of America are collaboratingwith JSTOR to digitize, preserve and extend access to Infection Control and Hospital Epidemiology.
http://www.jstor.org
This content downloaded from 195.78.108.162 on Sun, 18 May 2014 00:32:38 AMAll use subject to JSTOR Terms and Conditions

infection control and hospital epidemiology march 2010, vol. 31, no. 3
o r i g i n a l a r t i c l e
Optimizing Empirical Antimicrobial Therapy for Infectiondue to Gram-Negative Pathogens in the Intensive Care Unit:
Utility of a Combination Antibiogram
Jennifer Christoff, MD; Jocelyn Tolentino, MPH; Emily Mawdsley, MD; Scott Matushek, MS;David Pitrak, MD; Stephen G. Weber, MD, MS
objective. To determine whether the use of dual antimicrobial therapy based on the results of a combination antibiotic susceptibilityreport (antibiogram) increases the likelihood of selecting adequate empirical coverage in critically ill patients with infection due to potentiallyresistant gram-negative pathogens.
design. Retrospective data analysis.
setting. Urban academic medical center.
methods. An analysis of culture results and susceptibility data from intensive care unit patients determined by the clinical microbiologylaboratory was performed. The proportion of 5 common gram-negative pathogens susceptible to monotherapy with 1 of 3 antipseudomonalantibiotics (piperacillin-tazobactam, ceftazidime, or imipenem) was compared with the proportion susceptible to each of these 3 “backbone”agents plus 1 of 4 additional antimicrobial agents used in combination.
results. More than 5,000 clinical isolates were examined. When all isolates recovered during the entire study period were included,the addition of any of the second antibiotics studied to each of the 3 backbone agents significantly increased the likelihood of coveringthe causative pathogen ( for each). The benefit of combination therapy was variable when results for each of the 5 organisms wereP ! .01examined individually. When temporal trends in susceptibility were examined, the decrease in the proportion of organisms susceptible tomonotherapy was statistically significant for both imipenem and ceftazidime ( ).P ! .01
conclusions. Reporting antibiotic susceptibility data in the form of a combination antibiogram may be useful to clinicians who areconsidering empirical antimicrobial therapy in the intensive care unit.
Infect Control Hosp Epidemiol 2010; 31:256-261
From the Section of Infectious Diseases (J.C., J.T., E.M., D.P., S.G.W.), Infection Control Program (J.T., S.G.W.), and Clinical Microbiology Laboratory(S.M.), University of Chicago Medical Center, Chicago, Illinois.
Received May 26, 2009; accepted August 24, 2009; electronically published January 7, 2010.� 2009 by The Society for Healthcare Epidemiology of America. All rights reserved. 0899-823X/2010/3103-0005$15.00. DOI: 10.1086/650446
Infection caused by gram-negative bacteria is associated withsignificant morbidity and mortality among patients in theintensive care unit (ICU).1,2 The prevalence of resistance tocommonly prescribed antimicrobial agents has increased con-siderably in these pathogens during the past 2 decades,3,4 withimportant consequences for the critically ill. In this vulnerablegroup, delayed or inadequate antimicrobial therapy (ie, ther-apy to which the causative pathogen is not susceptible) isassociated with worsened clinical outcomes.5-10
Because of the high prevalence of antimicrobial resistanceamong gram-negative pathogens infecting critically ill pa-tients3,11-13 and the potential clinical consequences of inade-quate coverage,5-10 it may be beneficial to supplement em-pirical coverage—that is, to use a single broad-spectrum an-timicrobial agent with the addition of a second antibiotic,such as an aminoglycoside or fluoroquinolone.14-17 In additionto increasing the likelihood that the spectrum of activity of
the combined empirical regimen is adequate to treat highlyresistant gram-negative pathogens, such combination therapyhas been advocated to prevent the emergence of antimicrobialresistance.18
Combination antimicrobial therapy first emerged as themost common treatment approach for serious infection withPseudomonas aeruginosa after it was shown that the coad-ministration of b-lactam and aminoglycoside agents was as-sociated with decreased mortality in animal models.19,20 How-ever, it has since been shown that monotherapy with newerantipseudomonal agents, such as imipenem, ceftazidime, andsome fluoroquinolones, may be equally effective against P.aeruginosa and other gram-negative pathogens.21-24 Moreover,because of the potential toxicity associated with the additionalantimicrobial agents used in combination therapy, the routineuse of this strategy remains controversial.25-29
In most ICUs, the decision whether to use combination
This content downloaded from 195.78.108.162 on Sun, 18 May 2014 00:32:38 AMAll use subject to JSTOR Terms and Conditions
utility of a combination antibiogram 257
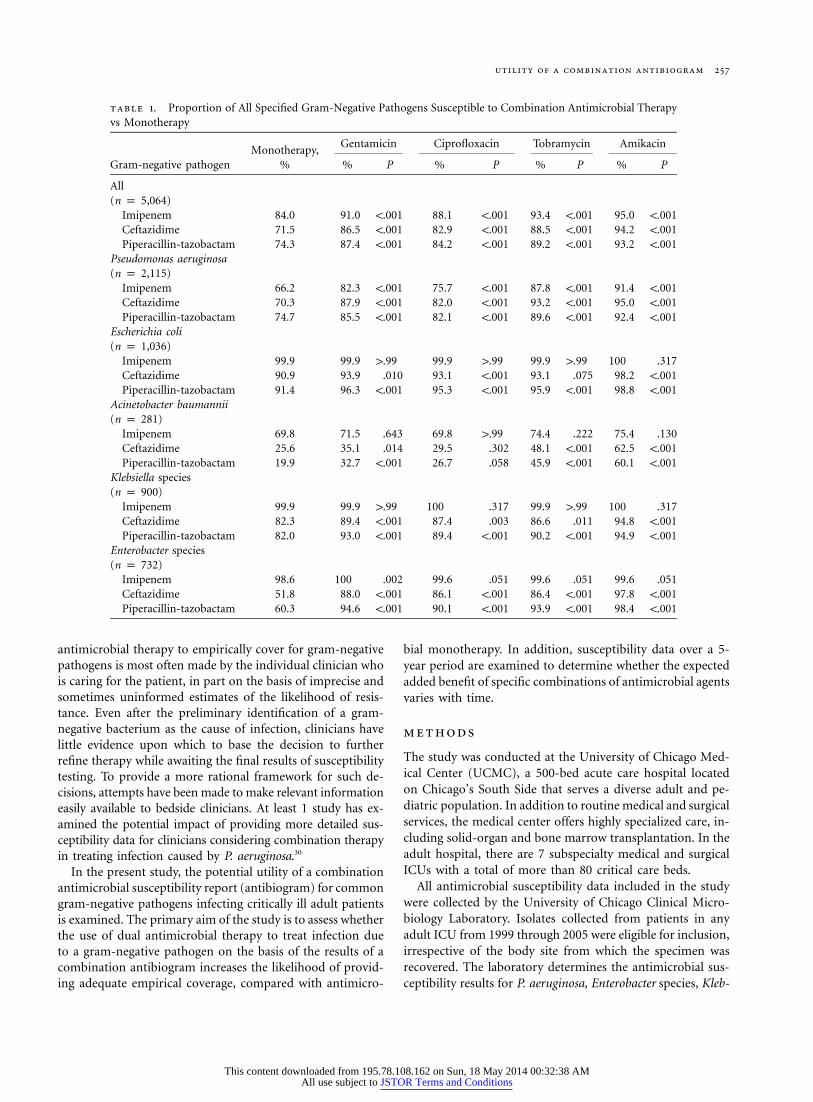
table 1. Proportion of All Specified Gram-Negative Pathogens Susceptible to Combination Antimicrobial Therapyvs Monotherapy
Gram-negative pathogenMonotherapy,
%
Gentamicin Ciprofloxacin Tobramycin Amikacin
% P % P % P % P
All(n p 5,064)
Imipenem 84.0 91.0 !.001 88.1 !.001 93.4 !.001 95.0 !.001Ceftazidime 71.5 86.5 !.001 82.9 !.001 88.5 !.001 94.2 !.001Piperacillin-tazobactam 74.3 87.4 !.001 84.2 !.001 89.2 !.001 93.2 !.001
Pseudomonas aeruginosa(n p 2,115)
Imipenem 66.2 82.3 !.001 75.7 !.001 87.8 !.001 91.4 !.001Ceftazidime 70.3 87.9 !.001 82.0 !.001 93.2 !.001 95.0 !.001Piperacillin-tazobactam 74.7 85.5 !.001 82.1 !.001 89.6 !.001 92.4 !.001
Escherichia coli(n p 1,036)
Imipenem 99.9 99.9 1.99 99.9 1.99 99.9 1.99 100 .317Ceftazidime 90.9 93.9 .010 93.1 !.001 93.1 .075 98.2 !.001Piperacillin-tazobactam 91.4 96.3 !.001 95.3 !.001 95.9 !.001 98.8 !.001
Acinetobacter baumannii(n p 281)
Imipenem 69.8 71.5 .643 69.8 1.99 74.4 .222 75.4 .130Ceftazidime 25.6 35.1 .014 29.5 .302 48.1 !.001 62.5 !.001Piperacillin-tazobactam 19.9 32.7 !.001 26.7 .058 45.9 !.001 60.1 !.001
Klebsiella species(n p 900)
Imipenem 99.9 99.9 1.99 100 .317 99.9 1.99 100 .317Ceftazidime 82.3 89.4 !.001 87.4 .003 86.6 .011 94.8 !.001Piperacillin-tazobactam 82.0 93.0 !.001 89.4 !.001 90.2 !.001 94.9 !.001
Enterobacter species(n p 732)
Imipenem 98.6 100 .002 99.6 .051 99.6 .051 99.6 .051Ceftazidime 51.8 88.0 !.001 86.1 !.001 86.4 !.001 97.8 !.001Piperacillin-tazobactam 60.3 94.6 !.001 90.1 !.001 93.9 !.001 98.4 !.001
antimicrobial therapy to empirically cover for gram-negativepathogens is most often made by the individual clinician whois caring for the patient, in part on the basis of imprecise andsometimes uninformed estimates of the likelihood of resis-tance. Even after the preliminary identification of a gram-negative bacterium as the cause of infection, clinicians havelittle evidence upon which to base the decision to furtherrefine therapy while awaiting the final results of susceptibilitytesting. To provide a more rational framework for such de-cisions, attempts have been made to make relevant informationeasily available to bedside clinicians. At least 1 study has ex-amined the potential impact of providing more detailed sus-ceptibility data for clinicians considering combination therapyin treating infection caused by P. aeruginosa.30
In the present study, the potential utility of a combinationantimicrobial susceptibility report (antibiogram) for commongram-negative pathogens infecting critically ill adult patientsis examined. The primary aim of the study is to assess whetherthe use of dual antimicrobial therapy to treat infection dueto a gram-negative pathogen on the basis of the results of acombination antibiogram increases the likelihood of provid-ing adequate empirical coverage, compared with antimicro-
bial monotherapy. In addition, susceptibility data over a 5-year period are examined to determine whether the expectedadded benefit of specific combinations of antimicrobial agentsvaries with time.
methods
The study was conducted at the University of Chicago Med-ical Center (UCMC), a 500-bed acute care hospital locatedon Chicago’s South Side that serves a diverse adult and pe-diatric population. In addition to routine medical and surgicalservices, the medical center offers highly specialized care, in-cluding solid-organ and bone marrow transplantation. In theadult hospital, there are 7 subspecialty medical and surgicalICUs with a total of more than 80 critical care beds.
All antimicrobial susceptibility data included in the studywere collected by the University of Chicago Clinical Micro-biology Laboratory. Isolates collected from patients in anyadult ICU from 1999 through 2005 were eligible for inclusion,irrespective of the body site from which the specimen wasrecovered. The laboratory determines the antimicrobial sus-ceptibility results for P. aeruginosa, Enterobacter species, Kleb-
This content downloaded from 195.78.108.162 on Sun, 18 May 2014 00:32:38 AMAll use subject to JSTOR Terms and Conditions

258 infection control and hospital epidemiology march 2010, vol. 31, no. 3
siella species, and Escherichia coli by the VITEK 2 automatedsystem (bioMerieux), and Acinetobacter baumannii suscep-tibility profiles are performed by double disk diffusion inaccordance with current accepted standards of the Clinicaland Laboratory Standards Institute.
For the study, antimicrobial susceptibility data were com-piled for the 5 gram-negative pathogens most commonly iso-lated from adult ICU patients at the study institution: P.aeruginosa, Enterobacter species, Klebsiella species, A. bau-mannii, and E. coli. For each organism type, the proportionof individual isolates that were susceptible to the antimicro-bial agents commonly used for empirical coverage of gram-negative pathogens at UCMC was determined. These “back-bone agents”—piperacillin-tazobactam, ceftazidime, and imi-penem—were assessed both as empirical monotherapy andas part of combination antimicrobial treatment. Next, theproportion of individual isolates susceptible to combinationtherapy with each of the backbone agents plus 1 of 4 agentscommonly added to extend the breadth of coverage was ex-amined. In determining the utility of adding amikacin, gen-tamicin, tobramycin, or ciprofloxacin to backbone coverage,a bacterial isolate was designated as susceptible to the com-bination regimen if the organism’s susceptibility profile dem-onstrated it to be adequately treated by either the backboneagent or the second antimicrobial drug.
Isolates were excluded if susceptibility data were not avail-able for any of the following reasons: (1) the patient diedbefore testing was completed; (2) the isolate with a positiveculture result was preceded by an identical isolate within theprevious 72 hours, and in accordance with laboratory policy,susceptibility testing was not performed; and (3) susceptibilityreports were not routinely determined for isolates of A. bau-mannii until the year 2001. Isolates were also excluded thatdid not have susceptibilities reported for both antimicrobialagents that were being compared. Because of this, a range ofisolates is reported as being tested for each antibiotic pairing.
For each of the 5 pathogens studied, the proportion ofindividual isolates susceptible to either antimicrobial com-ponent of combination therapy was compared with the pro-portion susceptible to monotherapy with each backboneagent. Significance was examined using the x2 or Fisher exacttest. In all analyses, a P value threshold of .05 was consideredto be statistically significant.
In addition to an examination of the overall benefit ofcombination coverage versus monotherapy for all isolatesover the entire study period, a number of subanalyses wereperformed. The x2 test for trend was used to determine tem-poral trends in susceptibility patterns. The proportion of iso-lates susceptible to monotherapy versus combination therapywas examined for each year of the study individually. In ad-dition, to obtain a more precise estimate of the potentialadvantage of combination therapy for clinically importantbacterial isolates (rather than for colonizing strains), suscep-tibility to monotherapy versus double coverage was examinedfor bloodstream isolates alone.
The study was approved by the institutional review boardof UCMC. Statistical analyses were conducted using the SASstatistical package, version 8.2 (SAS).
results
A total of 8,604 gram-negative organisms were collected fromadult ICU patients from 1999 through 2005. Among the 5common pathogens eligible for inclusion, from 5,069 to 5,090total specimens were analyzed, depending on the pathogen.
All Gram-Negative Pathogens
When all gram-negative isolates recovered from any body sitewere considered together for the entire study period, the ad-dition of any second antibiotic to each of the 3 backboneagents significantly increased the likelihood of adequatelycovering the causative pathogen ( for each compari-P ! .01son) (Table 1). With monotherapy, 71.5% (ceftazidime) to84.0% (imipenem) of all gram-negative pathogens were cov-ered, increasing to 82.9% (ceftazidime plus ciprofloxacin) to95.0% (imipenem plus amikacin) with combination therapy.When analysis was limited to bloodstream isolates, combi-nation therapy again significantly extended the breadth ofcoverage, compared with monotherapy ( for each com-P ! .01parison), except for the addition of ciprofloxacin to imipenem( ) (Table 2).P p .056
P. aeruginosa
P. aeruginosa accounted for 2,115 (42%) of the gram-negativeorganisms analyzed during the study period. When consid-ered independently of other pathogens, the proportion of allP. aeruginosa isolates that were adequately covered signifi-cantly increased with the addition of any second agent toimipenem, piperacillin-tazobactam, or ceftazidime (P ! .01for all comparisons) (Table 1). In contrast to this benefit, inthe case of bloodstream infection with P. aeruginosa, the ad-dition of ciprofloxacin to piperacillin-tazobactam (73.7% to78.2%; ) or ceftazidime (76.9% to 85.1%; )P p .39 P p .09did not significantly add to the breadth of coverage (data notshown).
Enterobacteriaceae
When imipenem was used to cover Enterobacter species(98.6% isolates susceptible), Klebsiella species (99.9% sus-ceptible), or E. coli (99.9% susceptible), the addition of asecond agent generally did not increase the number of isolatesthat were adequately covered. In contrast, when ceftazidimeor piperacillin-tazobactam was used to treat any of the Enter-obacteriaceae, adding a second agent in combination nearlyalways resulted in a significant increase in coverage (P ! .01for each).
A. baumannii
In treating A. baumannii, monotherapy with imipenem(69.8%) covered a greater number of isolates than the com-
This content downloaded from 195.78.108.162 on Sun, 18 May 2014 00:32:38 AMAll use subject to JSTOR Terms and Conditions
utility of a combination antibiogram 259
table 2. Percentage of All Gram-Negative Pathogens Isolated from Blood Cultures Susceptible to CombinationAntimicrobial Therapy vs Monotherapy
TherapyMonotherapy,
%
Gentamicin Ciprofloxacin Tobramycin Amikacin
% P % P % P % P
Imipenem 88.8 93.4 .007 92.1 .056 94.2 .001 95.8 !.001Ceftazidime 69.2 84.4 !.001 81.3 !.001 84.6 !.001 92.6 !.001Piperacillin-tazobactam 68.8 85.6 !.001 81.4 !.001 85.4 !.001 91.6 !.001
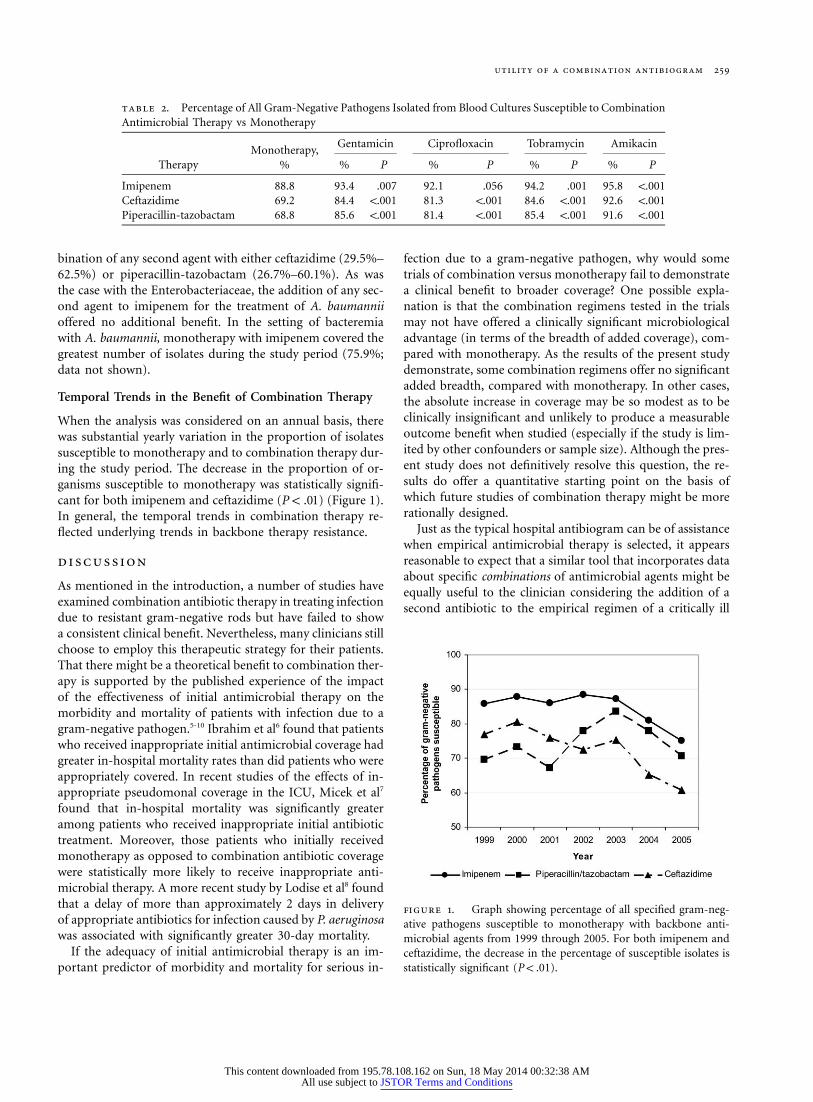
figure 1. Graph showing percentage of all specified gram-neg-ative pathogens susceptible to monotherapy with backbone anti-microbial agents from 1999 through 2005. For both imipenem andceftazidime, the decrease in the percentage of susceptible isolates isstatistically significant ( ).P ! .01
bination of any second agent with either ceftazidime (29.5%–62.5%) or piperacillin-tazobactam (26.7%–60.1%). As wasthe case with the Enterobacteriaceae, the addition of any sec-ond agent to imipenem for the treatment of A. baumanniioffered no additional benefit. In the setting of bacteremiawith A. baumannii, monotherapy with imipenem covered thegreatest number of isolates during the study period (75.9%;data not shown).
Temporal Trends in the Benefit of Combination Therapy
When the analysis was considered on an annual basis, therewas substantial yearly variation in the proportion of isolatessusceptible to monotherapy and to combination therapy dur-ing the study period. The decrease in the proportion of or-ganisms susceptible to monotherapy was statistically signifi-cant for both imipenem and ceftazidime ( ) (Figure 1).P ! .01In general, the temporal trends in combination therapy re-flected underlying trends in backbone therapy resistance.
discussion
As mentioned in the introduction, a number of studies haveexamined combination antibiotic therapy in treating infectiondue to resistant gram-negative rods but have failed to showa consistent clinical benefit. Nevertheless, many clinicians stillchoose to employ this therapeutic strategy for their patients.That there might be a theoretical benefit to combination ther-apy is supported by the published experience of the impactof the effectiveness of initial antimicrobial therapy on themorbidity and mortality of patients with infection due to agram-negative pathogen.5-10 Ibrahim et al6 found that patientswho received inappropriate initial antimicrobial coverage hadgreater in-hospital mortality rates than did patients who wereappropriately covered. In recent studies of the effects of in-appropriate pseudomonal coverage in the ICU, Micek et al7
found that in-hospital mortality was significantly greateramong patients who received inappropriate initial antibiotictreatment. Moreover, those patients who initially receivedmonotherapy as opposed to combination antibiotic coveragewere statistically more likely to receive inappropriate anti-microbial therapy. A more recent study by Lodise et al8 foundthat a delay of more than approximately 2 days in deliveryof appropriate antibiotics for infection caused by P. aeruginosawas associated with significantly greater 30-day mortality.
If the adequacy of initial antimicrobial therapy is an im-portant predictor of morbidity and mortality for serious in-
fection due to a gram-negative pathogen, why would sometrials of combination versus monotherapy fail to demonstratea clinical benefit to broader coverage? One possible expla-nation is that the combination regimens tested in the trialsmay not have offered a clinically significant microbiologicaladvantage (in terms of the breadth of added coverage), com-pared with monotherapy. As the results of the present studydemonstrate, some combination regimens offer no significantadded breadth, compared with monotherapy. In other cases,the absolute increase in coverage may be so modest as to beclinically insignificant and unlikely to produce a measurableoutcome benefit when studied (especially if the study is lim-ited by other confounders or sample size). Although the pres-ent study does not definitively resolve this question, the re-sults do offer a quantitative starting point on the basis ofwhich future studies of combination therapy might be morerationally designed.
Just as the typical hospital antibiogram can be of assistancewhen empirical antimicrobial therapy is selected, it appearsreasonable to expect that a similar tool that incorporates dataabout specific combinations of antimicrobial agents might beequally useful to the clinician considering the addition of asecond antibiotic to the empirical regimen of a critically ill
This content downloaded from 195.78.108.162 on Sun, 18 May 2014 00:32:38 AMAll use subject to JSTOR Terms and Conditions

260 infection control and hospital epidemiology march 2010, vol. 31, no. 3
patient. Mizuta et al30 recently examined the possibility ofchanging the manner in which bacterial susceptibility dataare reported in the form of a combination antibiogram. Thestudy was somewhat limited in that only P. aeruginosa infec-tions at a single institution for a 1-year period were examined.The authors found that clinicians’ antibiotic choices for com-bination therapy that were made on the basis of the conven-tional antibiogram would not have differed had they beenpresented with data that took into account the susceptibilitiesof common antipseudomonal b-lactam and aminoglycosidecombinations.30 Others have also suggested a combinationantibiogram as a potential strategy in choosing an appropriateempirical antibiotic regimen when a resistant gram-negativepathogen is suspected.31,32
In the present study, the approach proposed and discussedby Mizuta et al30 was applied to a greater range of pathogensand for a lengthier period of analysis. The 5 most commonlyisolated gram-negative organisms identified in the adult ICUsduring a 5-year period were examined. When considering allgram-negative pathogens together, combination antimicro-bial therapy significantly increased the likelihood that theorganism that was causing infection was adequately covered.The significant increase in coverage was maintained for allgram-negative pathogens and for P. aeruginosa alone for theentire 5 years of study. When treating P. aeruginosa at all bodysites, the addition of any second agent in combination againsignificantly increased the proportion of isolates covered.When treating A. baumannii, E. coli, Klebsiella species, orEnterobacter species, a second agent generally extended thespectrum of activity compared with monotherapy with cef-tazidime or piperacillin-tazobactam but not compared withimipenem.
In most of the drug-organism combinations examined inthis study, the absolute differences in the proportion of iso-lates covered are relatively modest. This finding is a functionof the resistance profiles of the individual organisms that areprevalent at the study center and are likely to be considerablydifferent at other institutions. Regardless of the magnitudeof the difference in the proportion of isolates covered at anyone hospital or the distribution of these organisms duringany given year, awareness on the part of prescribing cliniciansof the potential quantitative benefit of combination therapycould be valuable. The aim of the combination antibiogramis ultimately to permit the clinician to make a more informeddecision in the selection of empirical antimicrobial therapy,appropriately weighing the risks and benefits of combinationantimicrobial treatment.
On the basis of the results of the present study, reportingantibiotic susceptibility data in the form of a combinationantibiogram appears to be beneficial to clinicians who areconsidering empirical antimicrobial therapy for critically illpatients. Although ultimately such decisions must be madeon a case-by-case basis, a combination antibiogram couldhelp to ensure that the most rational choice is made. Furtherstudies are needed to determine whether there is an effect onphysicians’ decision making with the use of a combination
antibiogram, and ultimately to determine whether there is animpact on clinical outcomes, including mortality. However,even in the absence of such information, the ease with whichthese data can be compiled and the growing problem of an-timicrobial resistance make this a high priority.
acknowledgments
Potential conflicts of interest. D. P. reports that he has received grant supportfrom Abbott, Bristol-Myers Squib, Glaxo Smith Kline, Gilead, and Enzon.S. G. W. reports that he has received research support and honoraria fromMerck and honoraria from Pfizer. All other authors report no conflicts ofinterest relevant to this article.
Address reprint requests to Jennifer Christoff, MD, University of ChicagoMedical Center, 5841 S Maryland Ave (MC 5065), Chicago, IL 60637([email protected]).
references
1. Sligl W, Taylor G, Brindley PG. Five years of nosocomial gram-negativebacteremia in a general intensive care unit: epidemiology, antimicrobialsusceptibility patterns, and outcomes. Int J Infect Dis 2006;10:320–325.
2. Gardiner DF, Scholand SJ, Babinchak T. Mortality and gram-negativerod bacteraemia in the intensive care unit. J Hosp Infect 2006;62:453–457.
3. Fridkin SK. Increasing prevalence of antimicrobial resistance in intensivecare units. Crit Care Med 2001;29:N64–N68.
4. Flournoy DJ, Reinert RL, Bell-Dixon C, Gentry CA. Increasing anti-microbial resistance in gram-negative bacilli isolated from patients inintensive care units. Am J Infect Control 2000;28:244–250.
5. Kollef MH, Sherman G, Ward S, Fraser VJ. Inadequate antimicrobialtreatment of infections: a risk factor for hospital mortality among crit-ically ill patients. Chest 1999;115:462–474.
6. Ibrahim EH, Sherman G, Ward S, Fraser VJ, Kollef MH. The influenceof inadequate antimicrobial treatment of bloodstream infections on pa-tient outcomes in the ICU setting. Chest 2000;118:146–155.
7. Micek ST, Lloyd AE, Ritchie DJ, Reichley RM, Fraser VJ, Kollef MH.Pseudomonas aeruginosa bloodstream infection: importance of appro-priate initial antimicrobial treatment. Antimicrob Agents Chemother 2005;49:1306–1311.
8. Lodise TP Jr, Patel N, Kwa A, et al. Predictors of 30-day mortality amongpatients with Pseudomonas aeruginosa bloodstream infections: impact ofdelayed appropriate antibiotic selection. Antimicrob Agents Chemother2007;51:3510–3515.
9. Fraser A, Paul M, Almanasreh N, et al; TREAT Study Group. Benefit ofappropriate empirical antibiotic treatment: thirty-day mortality and du-ration of hospital stay. Am J Med 2006;119:970–976.
10. Kang C, Kim A, Kim H, et al. Pseudomonas aeruginosa bacteremia: riskfactors for mortality and influence of delayed receipt of effective anti-microbial therapy on clinical outcome. Clin Infect Dis 2003;37:745–751.
11. National nosocomial infections surveillance (NNIS) systems report, datasummary from January 1992–June 2001. Am J Infect Control 2001;29:404–421.
12. Jones RN. Global epidemiology of antimicrobial resistance among com-munity-acquired and nosocomial pathogens: a five-year summary fromthe SENTRY antimicrobial surveillance program (1997–2001). SeminRespir Crit Care Med 2003;24:121–134.
13. Wroblewska MM, Rudnicka J, Marchel H, Luczak M. Multidrug-resistantbacteria isolated from patients hospitalised in intensive care units. Int JAntimicrob Agents 2006;27:285–289.
14. Kollef MH. Inadequate antimicrobial treatment: an important determi-nant of outcome for hospitalized patients. Clin Infect Dis 2000;31:S131–S138.
15. Clark NM, Patterson J, Lynch JP 3rd. Antimicrobial resistance among
This content downloaded from 195.78.108.162 on Sun, 18 May 2014 00:32:38 AMAll use subject to JSTOR Terms and Conditions

utility of a combination antibiogram 261
gram-negative organisms in the intensive care unit. Curr Opin Crit Care2003;9:413–423.
16. Harbarth S, Nobre V, Pittet D. Does antibiotic selection impact patientoutcome? Clin Infect Dis 2007;44:87–93.
17. Allan JD, Moellering RC Jr. Antimicrobial combinations in the therapyof infections due to gram-negative bacilli. Am J Med 1985;78:65–76.
18. Mouton JW. Combination therapy as a tool to prevent emergence ofbacterial resistance. Infection 1999;27:S24–S28.
19. Scott RE, Robson HG. Synergistic activity of carbenicillin and gentamicinin experimental Pseudomonas bacteremia in neutropenic rats. AntimicrobAgents Chemother 1976;10:646–651.
20. Khakoo RA, Kluge RM. Effectiveness of gentamicin and carbenicillin ina rat model against infections with Pseudomonas aeruginosa resistant togentamicin or gentamicin and carbenicillin. J Antimicrob Chemother 1979;5:53–59.
21. Wade JC, Standiford HC, Drusano GL, et al. Potential of imipenem assingle-agent empiric antibiotic therapy of febrile neutropenic patientswith cancer. Am J Med 1985;78:62–72.
22. Eron LJ, Harvey L, Hixon DL, Poretz DM. Ciprofloxacin therapy ofinfections caused by Pseudomonas aeruginosa and other resistant bacteria.Antimicrob Agents Chemother 1985;28:308–310.
23. Verhagen C, de Pauw BE, Donnelly JP, Williams KJ, de Witte T, JanssenTH. Ceftazidime alone for treating Pseudomonas aeruginosa septicaemiain neutropenic patients. J Infect 1986;13:125–131.
24. Liang R, Yung R, Chiu E, et al. Ceftazidime versus imipenem-cislatin asinitial monotherapy for febrile neutropenic patients. Antimicrob AgentsChemother 1990;34:1336–1341.
25. Chow JW, Yu VL. Combination antibiotic therapy versus monotherapyfor gram-negative bacteraemia: a commentary. Int J Antimicrob Agents1999;11:7–12.
26. Safdar N, Handelsman J, Maki DG. Does combination antimicrobialtherapy reduce mortality in gram-negative bacteraemia? A meta-analysis.Lancet Infect Dis 2004;4:519–527.
27. Paul M, Soares-Weiser K, Leibovici L. b-lactam monotherapy versus b-lactam–aminoglycoside combination therapy for fever with neutropenia:systematic review and meta-analysis. BMJ 2003;326:1111.
28. Paul M, Benuri-Silbiger I, Soares-Weiser K, Leibovici L. b-lactam mono-therapy versus b-lactam–aminoglycoside combination therapy for sepsisin immunocompetent patients: systemic review and meta-analysis ofrandomized trials. BMJ 2004;328:668.
29. Leibovici L, Paul M, Poznanski O, et al. Monotherapy versus b-lactam–aminoglycoside combination treatment for gram-negative bacteremia: aprospective, observational study. Antimicrob Agents Chemother 1997;41:1127–1133.
30. Mizuta M, Linkin DR, Nachamkin I, et al. Identification of optimalcombinations for empirical dual antimicrobial therapy of Pseudomonasaeruginosa infection: potential role of a combination antibiogram. InfectControl Hosp Epidemiol 2006;27:413–415.
31. Apisarnthanarak A, Mundy LM. Role of combination antibiogram inempirical treatment of infection due to multidrug-resistant Acinetobacterbaumannii. Infect Control Hosp Epidemiol 2008;29:678–679.
32. Paterson DL. Impact of antibiotic resistance in gram-negative bacilli onempirical and definitive antibiotic therapy. Clin Infect Dis 2008;47:S14–S20.
This content downloaded from 195.78.108.162 on Sun, 18 May 2014 00:32:38 AMAll use subject to JSTOR Terms and Conditions