Embed Size (px)
Citation preview
9/12/18
1
Clinical Updates for Nurse
Practitioners and Physician
Assistants: 2018
Optimizing COPD Management in Primary Care
Faculty
2
§ Sandra Adams, MD, MSProfessor, Division of Pulmonary Diseases and Critical Care MedicineUT Health San AntonioStaff Physician, The South Texas Veterans Health Care SystemFounder, PresidentWipeDiseases FoundationSan Antonio, TX
§ Fernando Martinez, MD, MSChief, Division of Pulmonary and Critical Care MedicineBruce Webster Professor of MedicineJoan and Sanford I. Weill Department of MedicineWeill Cornell Medical CollegeNew York-Presbyterian Hospital/Weill Cornell Medical CenterNew York, NY
§ Frank Rahaghi, MD, MHS, FCCPDirector of Advanced Lung Disease ClinicDirector, Pulmonary Hypertension ClinicHead of Alpha-1 Foundation Clinical Resource Center Chairman, Dept. of Pulmonary and Critical CareCleveland Clinic FloridaWeston, FL
§ Alanna Kavanaugh, FNP-BC, MSN, CCRNNurse Practitioner Weill Cornell Medical College -Pulmonary, Critical Care Instructor of Practice for Graduate and Undergraduate Program - College of Mount Saint VincentNew York, NY
§ Arunabh Talwar, MD, FCCPDirector, Pulmonary Hypertension and Advanced Lung Disease ProgramNorth Shore University Hospital, Manhasset, NYProfessor of MedicineHofstra North Shore-LIJ School of MedicineHofstra UniversityHempstead, NY
3
§ Dr. Adams has received Contracted Research support from AstraZenecaPharmaceuticals LP, Boehringer Ingelheim Pharmaceuticals, Inc., DaiichiSankyo, GlaxoSmithKline, Novartis Pharmaceuticals, and SunovionPharmaceuticals, Inc.
§ Ms. Kavanaugh has no financial relationships to disclose.§ Dr. Martinez has served as a Consultant for AstraZeneca, Boehringer
Ingelheim, Chiesi, GlaxoSmithKline, and Sunovion and has receivedContracted Research support from AstraZeneca, Boehringer Ingelheim, andGlaxoSmithKline.
§ Dr. Rahaghi has served as a Consultant for Actelion, AstraZeneca, Baxter,Boehringer Ingleheim, Gilead, Reata and United Therapeutics. He has servedon the Speakers’ Bureau for Actelion, Baxter, Boehringer Ingleheim and UnitedTherapeutics and has received Contracted Research support from Actelion,AstraZeneca, Baxter, Bellerophon, Boehringer Ingleheim, Merck, Reata andUnited Therapeutics.
§ Dr. Talwar served on the Speakers’ Bureau for Boehringer Ingelheim. He isalso on the advisory board for Genentech.
3
Disclosures
This educational activity is supported by an educational grant from GlaxoSmithKline.
9/12/18
2
1. Describe “case finding” strategies to identify patients with unrecognized, clinically significant COPD
2. Tailor COPD pharmacotherapy according to current recommended therapeutic guidelines which incorporate unique patient needs and characteristics
3. Discuss strategies to facilitate the appropriate use of inhaled therapies for COPD including proper inhaler technique
4. Recognize appropriate strategies to prevent and manage COPD exacerbations and provide transitions of care post hospitalization
Learning Objectives
4
PRE-TEST QUESTIONS
5
How often do you use COPD Case Finding strategies to identify patients at high likelihood of suffering from COPD that should be treated?
1. Never2. Rarely3. Sometimes4. Often 5. Always
Pre-test ARS Question 1
6
9/12/18
3
How confident are you in your ability to select appropriate inhaled therapies for patients with COPD, based on disease severity and patient characteristics?
1. Not at all confident2. Slightly confident3. Moderately confident4. Pretty much confident5. Very confident
Pre-test ARS Question 2
7
Global Strategy for Diagnosis, Management and Prevention of COPD
§ Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases.
§ Exacerbations and comorbidities contribute to the overall severity in individual patients.
© 2017 Global Initiative for Chronic Obstructive Lung Disease 8
Risk Factors for COPD§ Smoking accounts for 80% of
all COPD diagnosis § 20% are nonsmokers
Other etiologies:§ Second hand smoke§ Environmental exposures
§ Cooking or heating with wood, peat, dung
§ Occupational exposures§ Undertreated asthma§ Genetics – alpha 1 antitrypsin
deficiency 9

9/12/18
4
COPD Symptoms
§ Chronic cough§ usually the first symptom that occurs in COPD§ initially intermittent
§ Chronic expectoration
§ Dyspnea§ Symptom for which patients with COPD seek medical
advice.§ Persistent, daily, progressive over time, exacerbated
by exercise and respiratory infections.
10© 2017 Global Initiative for Chronic Obstructive Lung Disease
Undiagnosed COPD is Associated with Increased Mortality…
Martinez CH, et al. Annals ATS. 2015; 12: 1788-95.
1.0
0.8
0.6
0.4
0.2
0.00 5 10 15 20
Surv
ival
pro
babi
lity
Time (yrs)
Non-OLDUndiagnosed OLDDiagnosed OLD
OLD: obstructive lung disease
11
…and Exacerbation-like Events
Labonte LE et al. AJRCCM 2016; 194: 285-98
Undiagnosed COPD vs. Diagnosed COPD
12
9/12/18
5
COPD is UnderdiagnosedBarriers to Diagnosis of COPD in Primary Care
Haroon, et al. Int J COPD 2015;10(1):1711
Care Providers
Time Limitations
Failure to probe at-risk patients about symptoms
and activity levels and lack of good case-finding
methods
Limited spirometry availability and expertise to
interpret
PatientsUnder-recognized symptoms
leading to delayed presentation
Poor awareness of COPD
Lack of knowledge regarding COPD risk factors and appropriate diagnostic
testing
13
Screening vs. Case Finding§ Many individuals at increased risk for
COPD self restrict activity to minimize symptoms.
§ USPSTF recommendation is based on lack of evidence, not negative evidence.
§ GOLD recommends case-finding in symptomatic patients but does not recommend screening in asymptomatic populations.
§ Future trials are needed to better assess the effects of screening and treatment of at risk individuals in primary care on long-term health outcomes.
Siu, et al. JAMA 2016;315:1372-7 14
Case Finding: A New Approach§ Joint partnership between
NHLBI and COPD Foundation
§ 5-item questionnaire plus Peak Expiratory Flow
§ Designed to identify individuals who are symptomatic or have history of exacerbations
§ In a case control study, CAPTURE exhibited an sensitivity of 95.7% and an specificity of 67.8% for differentiating cases from no-COPD control subjects
Martinez FJ et al, AJRCCM 2017; 195: 748-56 15
9/12/18
6
SYMPTOMS
coughsputumdyspnea
EXPOSURE TO RISK FACTORS
tobacco (10-20 pack/years)occupation
indoor/outdoor pollution
SPIROMETRY
The Global Initiative for Obstructive Lung Disease – 2017 Report. http://goldcopd.org.
COPD Diagnosis Requires Spirometry
16
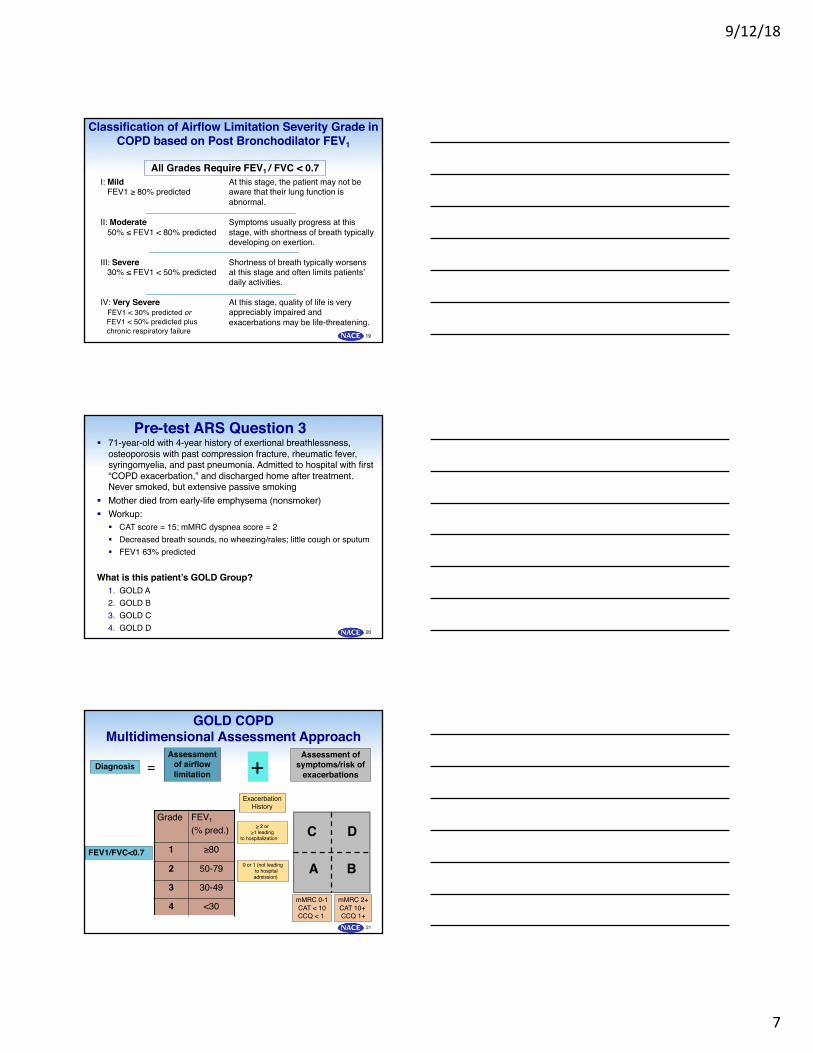
Why is Spirometry Underused?
17
§ Survey of 29 primary case offices§ 2/3 of offices owned a spirometer§ Spirometry performed on 50% of patients with COPD,
asthma, or respiratory symptoms
Main Reasons Cited for Not Performing SpirometryUnsure of impact on care 41%Unfamiliar with test 38%Lack of training 34%Concern about reimbursement 28%Equipment too costly 28%Concern about quality control 28%
Kaminsky DA, et al. Respir Care. 2005;50:1639-1648.
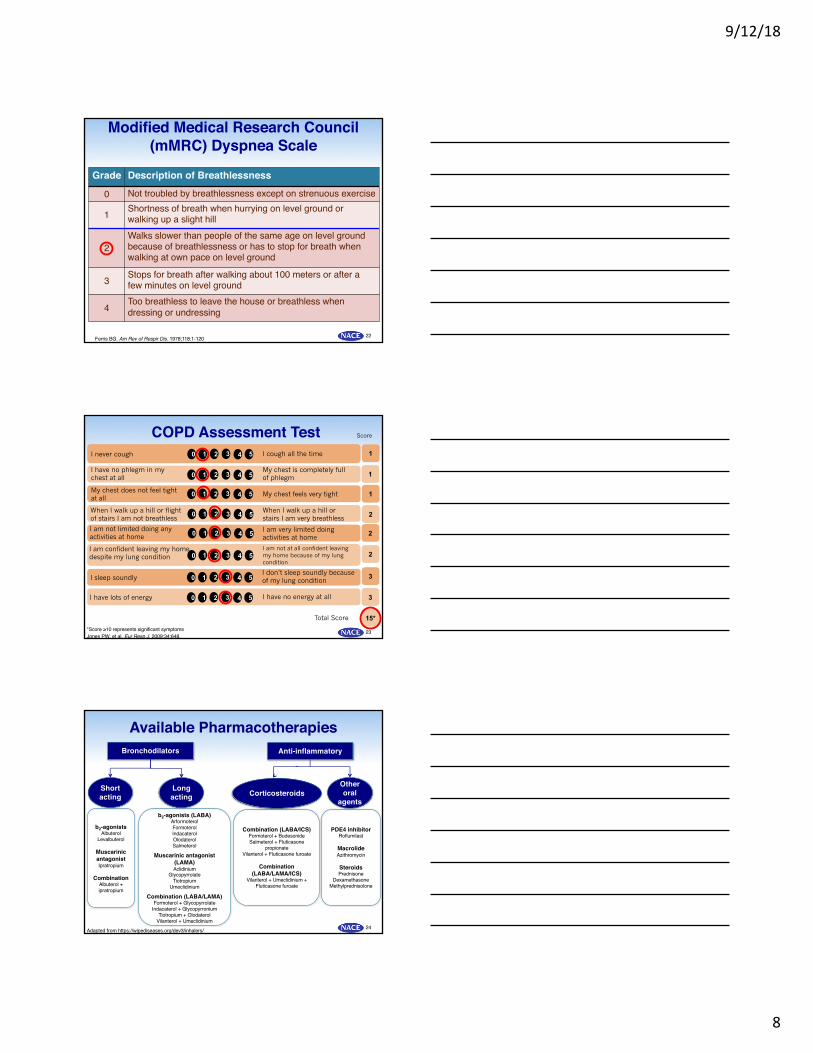
Spirometry: Obstructive Disease
Volu
me,
lite
rs
Time, seconds
5
4
3
2
1
1 2 3 4 5 6
FEV1 = 1.7L
FVC = 3.3L
FEV1/FVC = 0.51
Normal
Obstructive
18
9/12/18
7
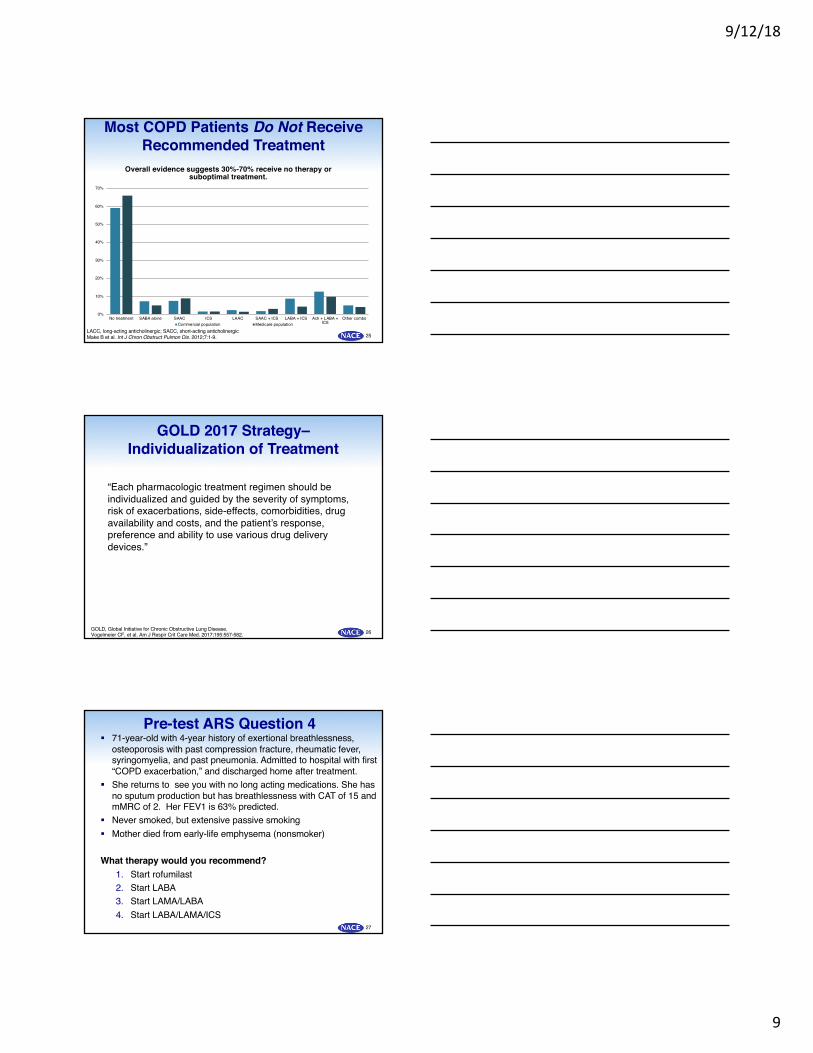
I: MildFEV1 ≥ 80% predicted
II: Moderate50% ≤ FEV1 < 80% predicted
III: Severe30% ≤ FEV1 < 50% predicted
IV: Very SevereFEV1 < 30% predicted orFEV1 < 50% predicted pluschronic respiratory failure
At this stage, the patient may not be aware that their lung function is abnormal.
Symptoms usually progress at this stage, with shortness of breath typicallydeveloping on exertion.
Shortness of breath typically worsens at this stage and often limits patients’ daily activities.
At this stage, quality of life is very appreciably impaired and exacerbations may be life-threatening.
Classification of Airflow Limitation Severity Grade in COPD based on Post Bronchodilator FEV1
19
All Grades Require FEV1 / FVC < 0.7
§ 71-year-old with 4-year history of exertional breathlessness, osteoporosis with past compression fracture, rheumatic fever, syringomyelia, and past pneumonia. Admitted to hospital with first “COPD exacerbation,” and discharged home after treatment. Never smoked, but extensive passive smoking
§ Mother died from early-life emphysema (nonsmoker) § Workup:
§ CAT score = 15; mMRC dyspnea score = 2§ Decreased breath sounds, no wheezing/rales; little cough or sputum§ FEV1 63% predicted
What is this patient’s GOLD Group? 1. GOLD A2. GOLD B3. GOLD C4. GOLD D
Pre-test ARS Question 3
20
Diagnosis
C D
A B
mMRC 0-1CAT < 10CCQ < 1
mMRC 2+CAT 10+ CCQ 1+
> 2 or >1 leading
to hospitalization
0 or 1 (not leadingto hospitaladmission)
ExacerbationHistory
Grade FEV1
(% pred.)
1 ≥80
2 50-79
3 30-49
4 <30
FEV1/FVC<0.7
Assessment of airflowlimitation
Assessment ofsymptoms/risk of
exacerbations+=
GOLD COPD Multidimensional Assessment Approach
21
9/12/18
8
Modified Medical Research Council (mMRC) Dyspnea Scale
Grade Description of Breathlessness
0 Not troubled by breathlessness except on strenuous exercise
1 Shortness of breath when hurrying on level ground or walking up a slight hill
2Walks slower than people of the same age on level ground because of breathlessness or has to stop for breath when walking at own pace on level ground
3 Stops for breath after walking about 100 meters or after a few minutes on level ground
4Too breathless to leave the house or breathless when dressing or undressing
Ferris BG. Am Rev of Respir Dis. 1978;118:1-120 22
*Score ≥10 represents significant symptomsJones PW, et al. Eur Resp J. 2009;34:648.
I never cough I cough all the time0 1 2 3 4 5
I have no phlegm in my chest at all
My chest is completely full of phlegm0 1 2 3 4 5
My chest feels very tight0 1 2 3 4 5My chest does not feel tightat all
When I walk up a hill or flight of stairs I am not breathless
When I walk up a hill orstairs I am very breathless
0 1 2 3 4 5
0 1 2 3 4 5I am not limited doing anyactivities at home
I am very limited doing activities at home
I am confident leaving my homedespite my lung condition
I am not at all confident leaving my home because of my lung condition
0 1 2 3 4 5
I sleep soundlyI don’t sleep soundly because of my lung condition0 1 2 3 4 5
I have lots of energy I have no energy at all0 1 2 3 4 5
Score
1
1
1
2
2
2
3
3
Total Score 15*
COPD Assessment Test
23
Adapted from https://wipediseases.org/dev3/inhalers/
Available Pharmacotherapies Bronchodilators Anti-inflammatory
Short acting
Longacting Corticosteroids
Other oral
agents
b2-agonistsAlbuterol
Levalbuterol
Muscarinic antagonistIpratropium
CombinationAlbuterol + ipratropium
b2-agonists (LABA)ArformoterolFormoterolIndacaterolOlodaterolSalmeterol
Muscarinic antagonist (LAMA)Aclidinium
GlycopyrrolateTiotropium
Umeclidinium
Combination (LABA/LAMA)Formoterol + Glycopyrrolate
Indacaterol + GlycopyrroniumTiotropium + Olodaterol
Vilanterol + Umeclidinium
Combination (LABA/ICS)Formoterol + BudesonideSalmeterol + Fluticasone
propionateVilanterol + Fluticasone furoate
Combination (LABA/LAMA/ICS)
Vilanterol + Umeclidinium + Fluticasone furoate
PDE4 inhibitorRoflumilast
MacrolideAzithromycin
SteroidsPrednisone
DexamethasoneMethylprednisolone
24
9/12/18
9
Most COPD Patients Do Not Receive Recommended Treatment
0%
10%
20%
30%
40%
50%
60%
70%
No treatment SABA alone SAAC ICS LAAC SAAC + ICS LABA + ICS Ach + LABA +ICS
Other combo
Overall evidence suggests 30%-70% receive no therapy or suboptimal treatment.
Commercial population Medicare populationLACC, long-acting anticholinergic; SACC, short-acting anticholinergic Make B et al. Int J Chron Obstruct Pulmon Dis. 2012;7:1-9. 25
GOLD 2017 Strategy–Individualization of Treatment
“Each pharmacologic treatment regimen should be individualized and guided by the severity of symptoms, risk of exacerbations, side-effects, comorbidities, drug availability and costs, and the patient’s response, preference and ability to use various drug delivery devices.”
GOLD, Global Initiative for Chronic Obstructive Lung Disease.Vogelmeier CF, et al. Am J Respir Crit Care Med. 2017;195:557-582. 26
§ 71-year-old with 4-year history of exertional breathlessness, osteoporosis with past compression fracture, rheumatic fever, syringomyelia, and past pneumonia. Admitted to hospital with first “COPD exacerbation,” and discharged home after treatment.
§ She returns to see you with no long acting medications. She has no sputum production but has breathlessness with CAT of 15 and mMRC of 2. Her FEV1 is 63% predicted.
§ Never smoked, but extensive passive smoking § Mother died from early-life emphysema (nonsmoker)
What therapy would you recommend? 1. Start rofumilast2. Start LABA3. Start LAMA/LABA4. Start LABA/LAMA/ICS
Pre-test ARS Question 4
27

9/12/18
10
Group A Group B
Group C Group D
A bronchodilator
Continue, stop ortry alternative classof bronchodilator
Evaluateeffect
A long-acting bronchodilator (LABA or LAMA)
LAMA + LABA
Persistentsymptoms
LAMA
LAMA + LABA LABA + ICS
LAMA + LABA
Consider roflumilast if FEV1 < 50% pred and patient has
chronic bronchitis
FurtherExacerbation(s)
Consider macrolide
LAMA LABA + ICS
LAMA + LABA + ICS
FurtherExacerbation(s)
Persistent symptoms/further
exacerbations
GOLD Therapeutic Recommendations
FurtherExacerbation(s)
The Global Initiative for Obstructive Lung Disease – 2017 Report. http://goldcopd.org.28
Risk Factors Associated With CXR-Confirmed Pneumonia in Patients With COPD
Treated With ICS1,2
1. Crim C et al. Ann Am Thorac Soc. 2015;12:27-34. 2. Dransfield MT et al. Lancet Respir Med. 2013;1:210-223.
§ Older age (≥ 65 years old)§ Low body mass index (BMI < 25 kg/m2)
§ Very severe COPD (FEV1 < 30% predicted)§ Prior pneumonia
29
Group D
LAMA + LABA
Consider roflumilast if FEV1 < 50% pred and
patient has chronic bronchitis
FurtherExacerbation(s)
Consider macrolide
LAMA LABA + ICS
LAMA + LABA + ICS
FurtherExacerbation(s)
Persistent symptoms/further
exacerbations
GOLD Therapeutic Recommendations
The Global Initiative for Obstructive Lung Disease – 2017 Report. http://goldcopd.org.30
9/12/18
11
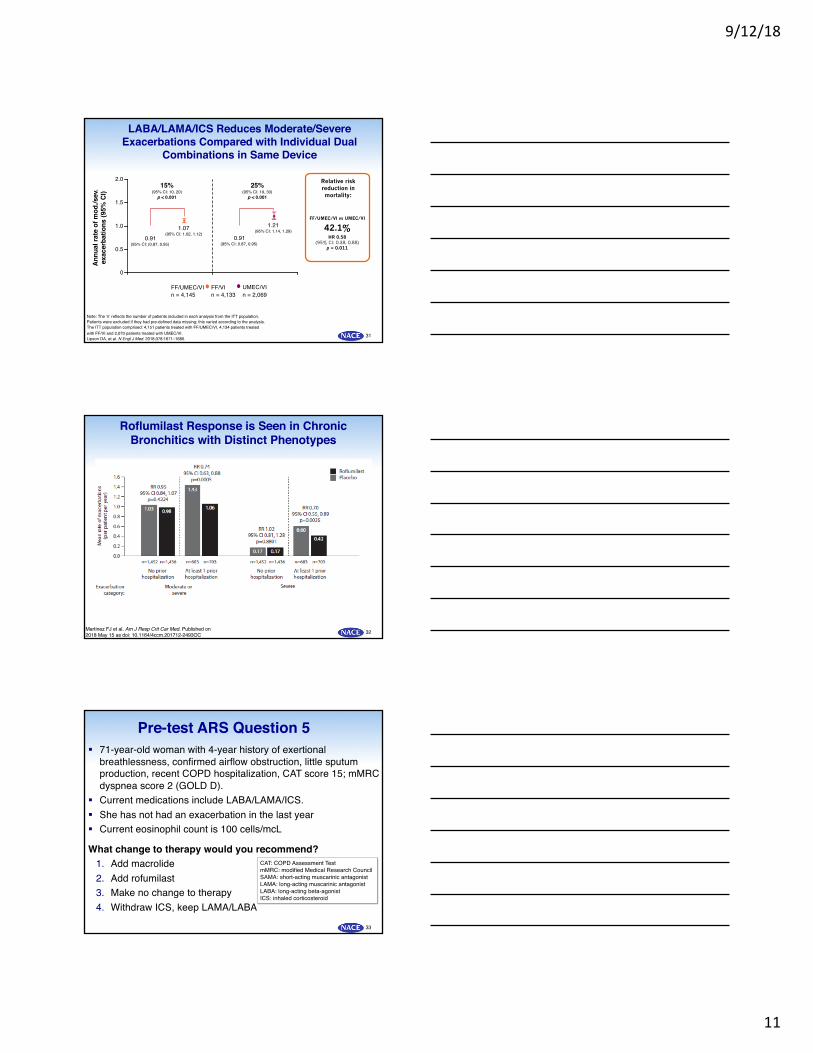
Note: The ‘n’ reflects the number of patients included in each analysis from the ITT population. Patients were excluded if they had pre-defined data missing; this varied according to the analysis. The ITT population comprised: 4,151 patients treated with FF/UMEC/VI, 4,134 patients treated with FF/VI and 2,070 patients treated with UMEC/VI.Lipson DA, et al. N Engl J Med. 2018;378:1671–1680.
LABA/LAMA/ICS Reduces Moderate/Severe Exacerbations Compared with Individual Dual
Combinations in Same Device
0
0.5
1.0
1.5
2.0
Annu
al ra
te o
f mod
./sev
. ex
acer
batio
ns (9
5% C
I)
FF/UMEC/VI FF/VIn = 4,145 n = 4,133
UMEC/VIn = 2,069
25%(95% CI: 19, 30)p < 0.001
1.21(95% CI: 1.14, 1.29)
0.91(95% CI: 0.87, 0.95)
15%(95% CI: 10, 20)p < 0.001
1.07(95% CI: 1.02, 1.12)
0.91(95% CI: (0.87, 0.95)
Relative risk reduction in mortality:
FF/UMEC/VI vs UMEC/VI
42.1%HR 0.58
(95% CI: 0.38, 0.88)p = 0.011
31
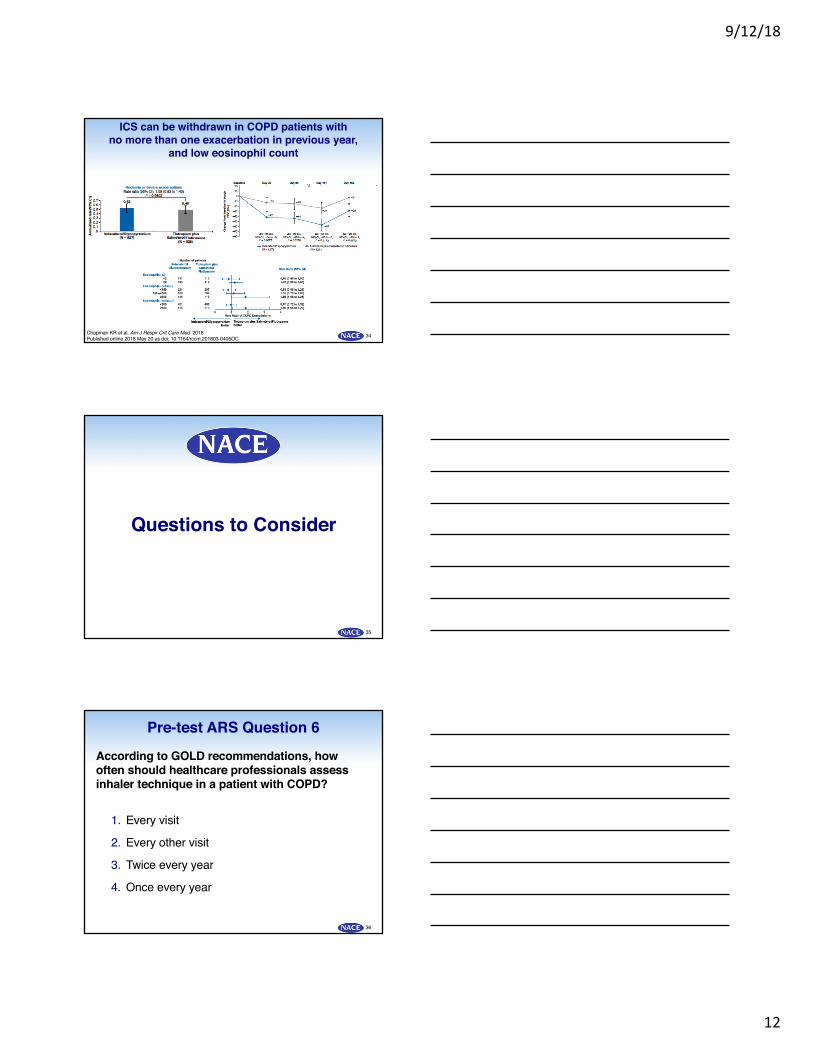
Roflumilast Response is Seen in Chronic Bronchitics with Distinct Phenotypes
Martinez FJ et al. Am J Resp Crit Car Med. Published on 2018 May 15 as doi: 10.1164/4ccm.201712-2493OC 32
§ 71-year-old woman with 4-year history of exertional breathlessness, confirmed airflow obstruction, little sputum production, recent COPD hospitalization, CAT score 15; mMRCdyspnea score 2 (GOLD D).
§ Current medications include LABA/LAMA/ICS.§ She has not had an exacerbation in the last year§ Current eosinophil count is 100 cells/mcL
What change to therapy would you recommend? 1. Add macrolide2. Add rofumilast3. Make no change to therapy 4. Withdraw ICS, keep LAMA/LABA
Pre-test ARS Question 5
CAT: COPD Assessment TestmMRC: modified Medical Research CouncilSAMA: short-acting muscarinic antagonistLAMA: long-acting muscarinic antagonistLABA: long-acting beta-agonistICS: inhaled corticosteroid
33
9/12/18
12
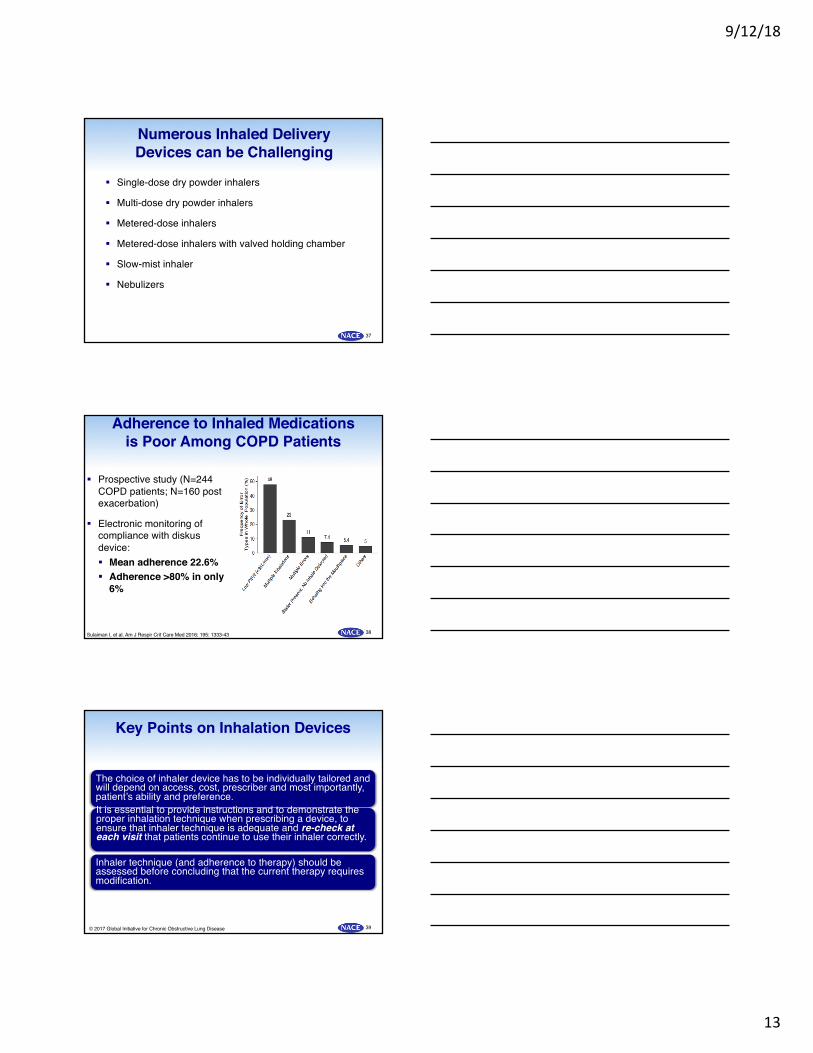
ICS can be withdrawn in COPD patients with no more than one exacerbation in previous year,
and low eosinophil count
Chapman KR et al. Am J Respir Crit Care Med 2018Published online 2018 May 20 as doi: 10.1164/rccm.201803-0405OC 34
Questions to Consider
35
Pre-test ARS Question 6
According to GOLD recommendations, how often should healthcare professionals assess inhaler technique in a patient with COPD?
1. Every visit
2. Every other visit
3. Twice every year
4. Once every year
36
9/12/18
13
Numerous Inhaled Delivery Devices can be Challenging
§ Single-dose dry powder inhalers
§ Multi-dose dry powder inhalers
§ Metered-dose inhalers
§ Metered-dose inhalers with valved holding chamber
§ Slow-mist inhaler
§ Nebulizers
37
Adherence to Inhaled Medications is Poor Among COPD Patients
§ Prospective study (N=244 COPD patients; N=160 post exacerbation)
§ Electronic monitoring of compliance with diskus device:§ Mean adherence 22.6%§ Adherence >80% in only
6%
Sulaiman I, et al. Am J Respir Crit Care Med 2016; 195: 1333-43 38
Key Points on Inhalation Devices
© 2017 Global Initiative for Chronic Obstructive Lung Disease
The choice of inhaler device has to be individually tailored and will depend on access, cost, prescriber and most importantly, patient’s ability and preference.It is essential to provide instructions and to demonstrate the proper inhalation technique when prescribing a device, to ensure that inhaler technique is adequate and re-check at each visit that patients continue to use their inhaler correctly.
Inhaler technique (and adherence to therapy) should be assessed before concluding that the current therapy requires modification.
39
9/12/18
14
Non-pharmacological Therapy of Stable COPD
Patient Essential Recommended Local guidelines
A Smoking cessation Physical activity
Flu and pneumococcal vaccination
B, C, D Smoking cessationPulmonaryrehabilitation
Physical activity
Flu and pneumococcal vaccination
www.goldcopd.org 40
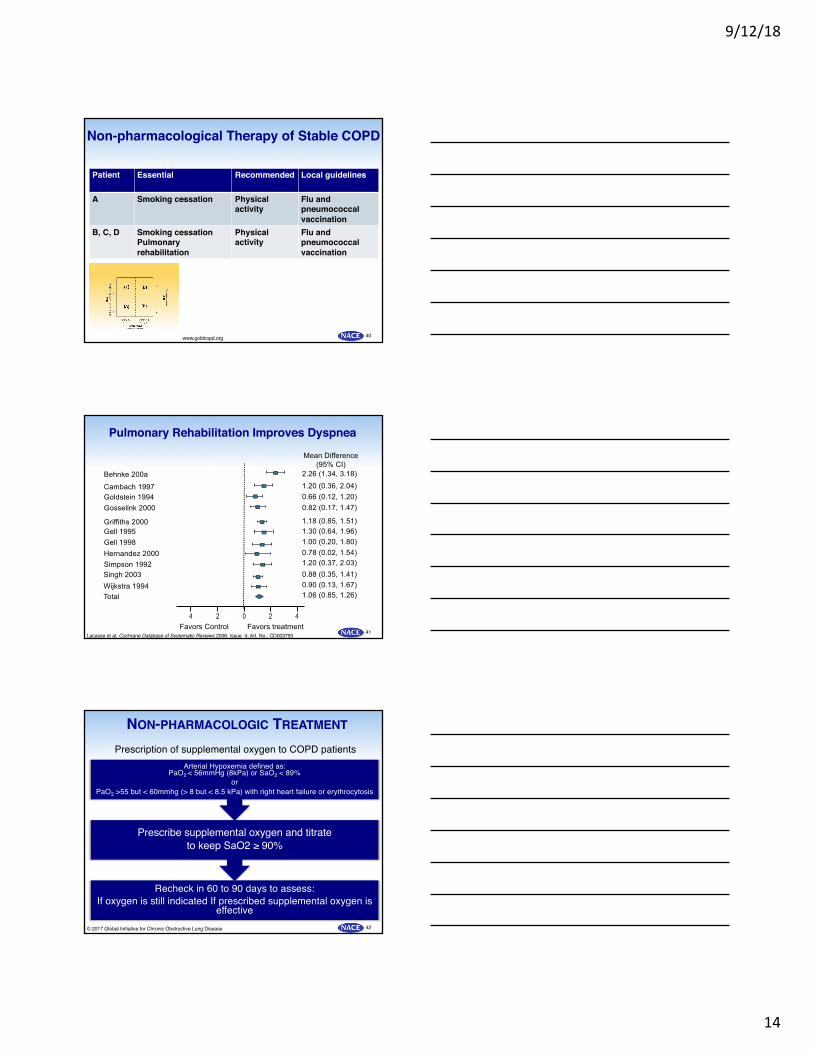
Pulmonary Rehabilitation Improves Dyspnea
Lacasse et al, Cochrane Database of Systematic Reviews 2006; Issue 4; Art. No.: CD003793
4 2 2 4
Behnke 200aCambach 1997
Favors Control Favors treatment
Goldstein 1994
Mean Difference(95% CI)
2.26 (1.34, 3.18)1.20 (0.36, 2.04)0.66 (0.12, 1.20)
0
Gosselink 2000
Griffiths 2000Gell 1995
0.82 (0.17, 1.47)
1.18 (0.85, 1.51)1.30 (0.64, 1.96)
Gell 1998Hernandez 2000Simpson 1992
1.00 (0.20, 1.80)0.78 (0.02, 1.54)1.20 (0.37, 2.03)
Singh 2003Wijkstra 1994Total
0.88 (0.35, 1.41)0.90 (0.13, 1.67)1.06 (0.85, 1.26)
41
NON-PHARMACOLOGIC TREATMENT
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Recheck in 60 to 90 days to assess: If oxygen is still indicated If prescribed supplemental oxygen is
effective
Prescribe supplemental oxygen and titrate to keep SaO2 ≥ 90%
Arterial Hypoxemia defined as:PaO2 < 56mmHg (8kPa) or SaO2 < 89%
or PaO2 >55 but < 60mmhg (> 8 but < 8.5 kPa) with right heart failure or erythrocytosis
Prescription of supplemental oxygen to COPD patients
42
9/12/18
15
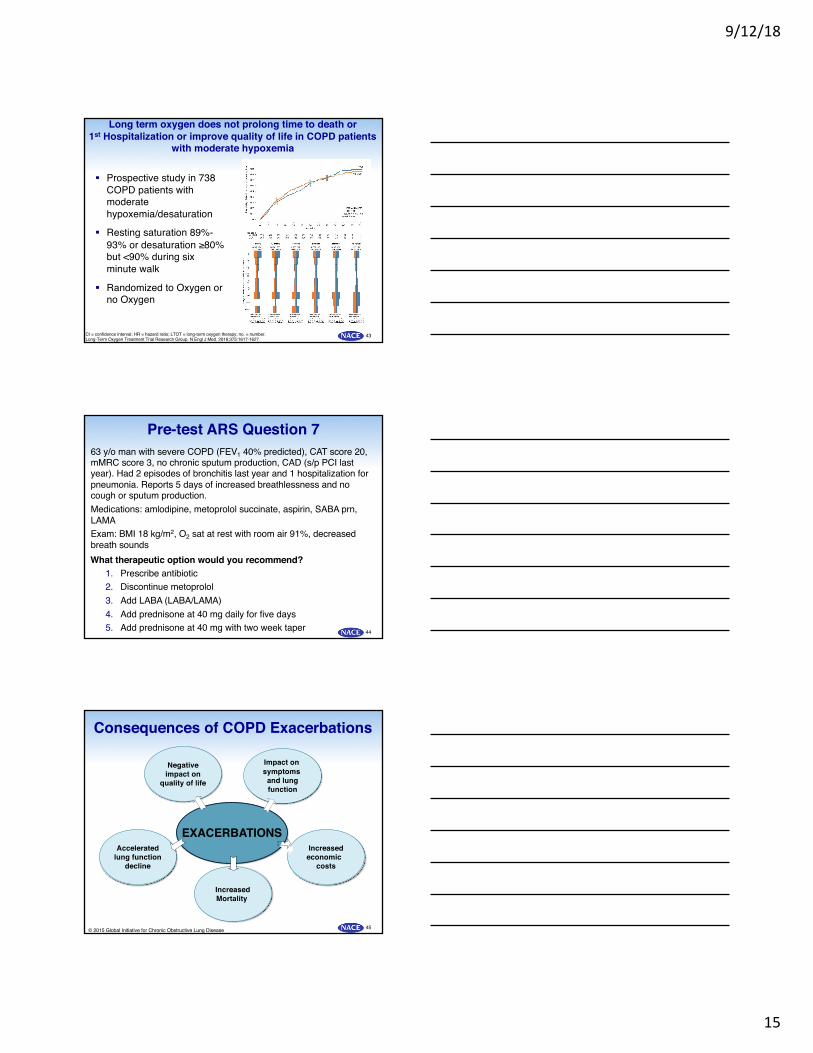
Long term oxygen does not prolong time to death or 1st Hospitalization or improve quality of life in COPD patients
with moderate hypoxemia
§ Prospective study in 738 COPD patients with moderate hypoxemia/desaturation
§ Resting saturation 89%-93% or desaturation ≥80% but <90% during six minute walk
§ Randomized to Oxygen or no Oxygen
CI = confidence interval; HR = hazard ratio; LTOT = long-term oxygen therapy; no. = number. Long-Term Oxygen Treatment Trial Research Group. N Engl J Med. 2016;375:1617-1627.
43
What therapeutic option would you recommend?1. Prescribe antibiotic2. Discontinue metoprolol3. Add LABA (LABA/LAMA) 4. Add prednisone at 40 mg daily for five days5. Add prednisone at 40 mg with two week taper
Pre-test ARS Question 763 y/o man with severe COPD (FEV1 40% predicted), CAT score 20, mMRC score 3, no chronic sputum production, CAD (s/p PCI last year). Had 2 episodes of bronchitis last year and 1 hospitalization for pneumonia. Reports 5 days of increased breathlessness and no cough or sputum production.Medications: amlodipine, metoprolol succinate, aspirin, SABA prn, LAMA Exam: BMI 18 kg/m2, O2 sat at rest with room air 91%, decreased breath sounds
44
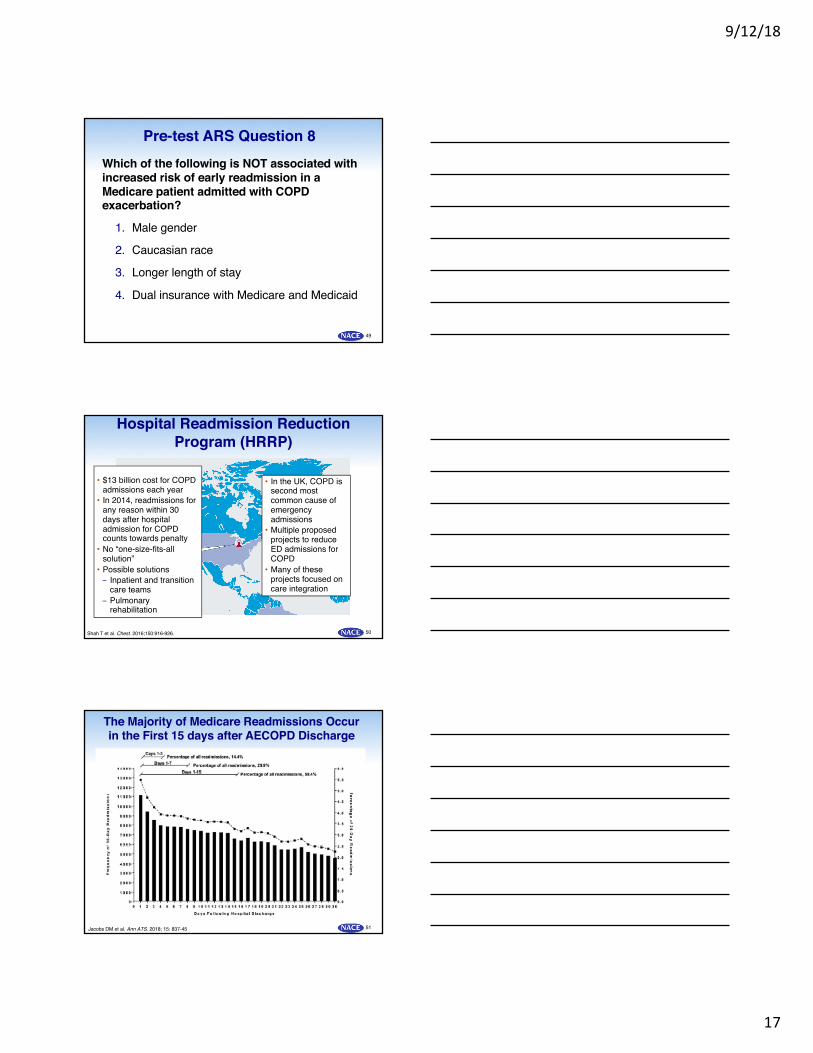
Impact on symptoms
and lungfunction
Negativeimpact on
quality of life
Consequences of COPD Exacerbations
Increasedeconomic
costs
Acceleratedlung function
decline
IncreasedMortality
EXACERBATIONS
© 2015 Global Initiative for Chronic Obstructive Lung Disease 45
9/12/18
16
Management of Exacerbations
© 2017 Global Initiative for Chronic Obstructive Lung Disease
§ OVERALL KEY POINTS:
§ An exacerbation of COPD is defined as an acute worsening of respiratory symptoms that results in additional therapy.
§ Exacerbations of COPD can be precipitated by several factors. The most common causes are respiratory tract infections.
§ The goal for treatment of COPD exacerbations is to minimize the negative impact of the current exacerbation and to prevent subsequent events.
§ Short-acting inhaled beta2-agonists, with or without short-acting anticholinergics, are recommended as the initial bronchodilators to treat an acute exacerbation.
46
Antibiotics should be given to patients:
§ With three cardinal symptoms: § increased dyspnea, § increased sputum volume, and § increased sputum purulence
§ Who require mechanical ventilation
Global Strategy for Diagnosis, Management,and Prevention of COPD:
Manage Exacerbations: Treatment Options
© 2017 Global Initiative for Chronic Obstructive Lung Disease 47
GOLD recommendation
§ A dose of 40 mg prednisone per day for 5 days is recommended (Evidence B), although there are insufficient data to provide firm conclusions concerning the optimal duration of corticosteroid therapy of acute exacerbations of COPD most studies showed no benefit from more than 5 days of therapy.
© 2017 Global Initiative for Chronic Obstructive Lung Disease, p. 103. 48
9/12/18
17
Which of the following is NOT associated with increased risk of early readmission in a Medicare patient admitted with COPD exacerbation?
1. Male gender
2. Caucasian race
3. Longer length of stay
4. Dual insurance with Medicare and Medicaid
Pre-test ARS Question 8
49
Hospital Readmission Reduction Program (HRRP)
• $13 billion cost for COPD admissions each year• In 2014, readmissions for
any reason within 30 days after hospital admission for COPD counts towards penalty• No “one-size-fits-all
solution” • Possible solutions
– Inpatient and transition care teams
– Pulmonary rehabilitation
• In the UK, COPD is second most common cause of emergency admissions• Multiple proposed
projects to reduce ED admissions for COPD• Many of these
projects focused on care integration
Shah T et al. Chest. 2016;150:916-926. 50
The Majority of Medicare Readmissions Occur in the First 15 days after AECOPD Discharge
Jacobs DM et al. Ann ATS. 2018; 15: 837-45 51

9/12/18
18
Numerous Factors are Associated with Medicare Readmission
Shah T, et al. Chest 2015; 147: 1219-26
Characteristic OR (95% CI)Age > 80 years 0.97 (0.96-0.99)
Female gender 0.89 (0.88-0.90)
Black race 1.06 (1.04-1.08)
Charlson 2 1.43 (1.41-1.46)
Dually eligible for Medicare and Medicaid 1.22 (1.20-1.24)
Longer length of stay 1.03 (1.03-1.03)
ICU use 1.03 (1.02-1.05)
Discharge to SNF 1.42 (1.40-1.45)
Discharge home with home care 1.36 (1.34-1.38)
52
53
POST-TEST QUESTIONS
53
After completing this activity, how often do you intend to use COPD Case Finding strategies to identify patients at high likelihood of suffering from COPD that should be treated?
1. Never2. Rarely3. Sometimes4. Often 5. Always
Post-test ARS Question 1
54
9/12/18
19
After completing this activity, how confident are you now in your ability to select appropriate inhaled therapies for patients with COPD, based on disease severity and patient characteristics?
1. Not at all confident2. Slightly confident3. Moderately confident4. Pretty much confident5. Very confident
Post-test ARS Question 2
55
§ 71-year-old with 4-year history of exertional breathlessness, osteoporosis with past compression fracture, rheumatic fever, syringomyelia, and past pneumonia. Admitted to hospital with first “COPD exacerbation,” and discharged home after treatment. Never smoked, but extensive passive smoking
§ Mother died from early-life emphysema (nonsmoker) § Workup:
§ CAT score = 15; mMRC dyspnea score = 2§ Decreased breath sounds, no wheezing/rales; little cough or sputum§ FEV1 63% predicted
What is this patient’s GOLD Group? 1. GOLD A2. GOLD B3. GOLD C4. GOLD D
Post-test ARS Question 3
56
§ 71-year-old with 4-year history of exertional breathlessness, osteoporosis with past compression fracture, rheumatic fever, syringomyelia, and past pneumonia. Admitted to hospital with first “COPD exacerbation,” and discharged home after treatment.
§ She returns to see you with no long acting medications. She has no sputum production but has breathlessness with CAT of 15 and mMRC of 2. Her FEV1 is 63% predicted.
§ Never smoked, but extensive passive smoking § Mother died from early-life emphysema (nonsmoker)
What therapy would you recommend? 1. Start rofumilast2. Start LABA3. Start LAMA/LABA4. Start LABA/LAMA/ICS
Post-test ARS Question 4
57
9/12/18
20
Post-test ARS Question 5§ 71-year-old woman with 4-year history of exertional
breathlessness, confirmed airflow obstruction, little sputum production, recent COPD hospitalization, CAT score 15; mMRCdyspnea score 2 (GOLD D)
§ Current medications include LABA/LAMA/ICS§ She has not had an exacerbation in the last year§ Current eosinophil count is 100 cells/mcL
What change to therapy would you recommend? 1. Add macrolide2. Add rofumilast3. Make no change to therapy 4. Withdraw ICS, keep LAMA/LABA
CAT: COPD Assessment TestmMRC: modified Medical Research CouncilSAMA: short-acting muscarinic antagonistLAMA: long-acting muscarinic antagonistLABA: long-acting beta-agonistICS: inhaled corticosteroid
58
Post-test ARS Question 6
59
According to GOLD recommendations, how often should healthcare professionals assess inhaler technique in a patient with COPD?
1. Every visit
2. Every other visit
3. Twice every year
4. Once every year
Post-test ARS Question 7
60
63 y/o man with severe COPD (FEV1 40% predicted), CAT score 20, mMRC score 3, no chronic sputum production, CAD (s/p PCI last year). Had 2 episodes of bronchitis last year and 1 hospitalization for pneumonia. Reports 5 days of increased breathlessness and no cough or sputum production.Medications: amlodipine, metoprolol succinate, aspirin, SABA prn, LAMA Exam: BMI 18 kg/m2, O2 sat at rest with room air 91%, decreased breath soundsWhat therapeutic option would you recommend?
1. Prescribe antibiotic2. Discontinue metoprolol3. Add LABA (LABA/LAMA) 4. Add prednisone at 40 mg daily for five days5. Add prednisone at 40 mg with two week taper
9/12/18
21
Which of the following is NOT associated with increased risk of early readmission in a Medicare patient admitted with COPD exacerbation?
1. Male gender
2. Caucasian race
3. Longer length of stay
4. Dual insurance with Medicare and Medicaid
Post-test ARS Question 8
61
Approximately how many patients with COPD do you see on a weekly basis, in any clinical setting?
1. None
2. 1-5
3. 6-10
4. 11-15
5. 16-20
6. 21-25
7. > 25
62
Post-test ARS Question 9





























