Embed Size (px)
Citation preview
Optimize Your Practice
Philip Clark, MBA, CMPE
Business Manager, Duke Metabolic and Weight Loss Surgery
Billing and Coding, the Role of Fellows and Physician
Extenders, Band Adjustments and Diversifying
Strategies to Increase Revenue
Managing the Revenue Cycle
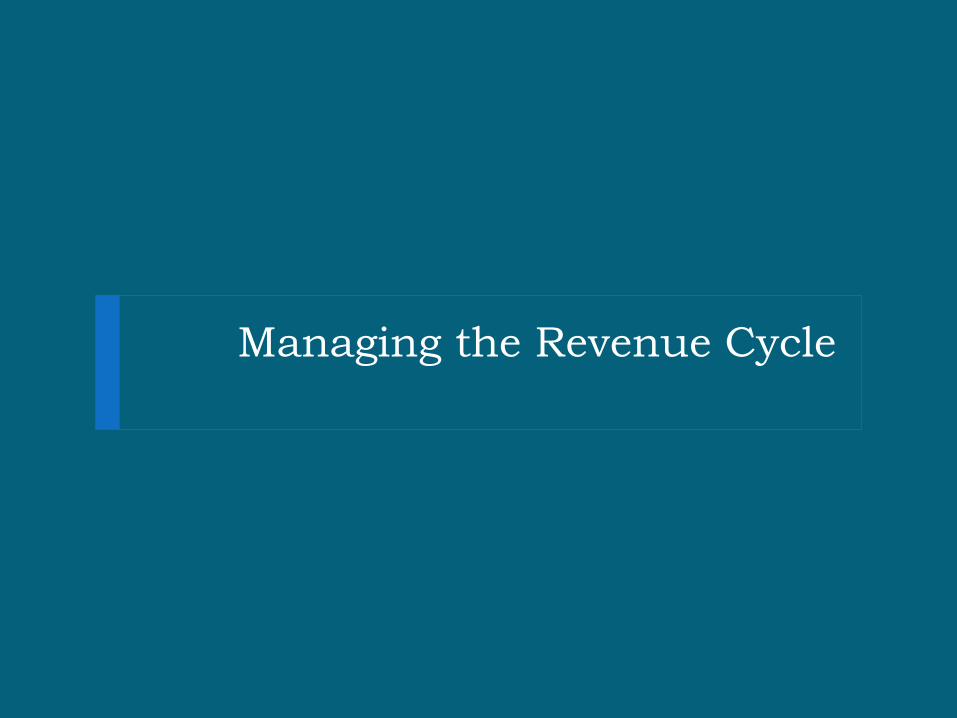
Billing and Coding: Revenue Cycle
New Patient Visit
Evaluation
Surgery
Payment
Accounts Receivable
Referral
Pre-
Authorization
Pre-
Determination
Pre-Verification
Op. Notes
Coding
Appeals
Patient Balance
Physician Involvement
=
= +
Pre-Operative Revenue Cycle
If you waited until you received the denial notification to deal with the insurance company, you left it to late!
Front End Management is Key to Successful Revenue Cycle – Optimize all processes prior to the bill being sent
Determine Bariatric Benefits (prior to delivering any services)
[Optimize – Convert to Self Pay]
Match Medical Evaluation Phase to Fit the Insurance Benefits
[Optimize – Personalize the evaluation process to the patients insurance benefit]
Get the right surgical authorization
[Optimize – add all potential procedures to the authorization]
Documentation in Pre-Evaluation Phase and in the OR
[Optimize – make sure that medical decision making and assessments match the actions of the encounters, template where appropriate]

Accounts Receivable
Denial Reason Write Off Billing Correction /
Documentation (Billing)
Appeal
(Physician)
Authorization required X
Services not Covered X
Coverage Terminated X
Medical Records X
More Documentation / Info X X
Medical Necessity X X
Missing / Invalid CPT X X
Coordination of Benefits X
Untimely Filing X
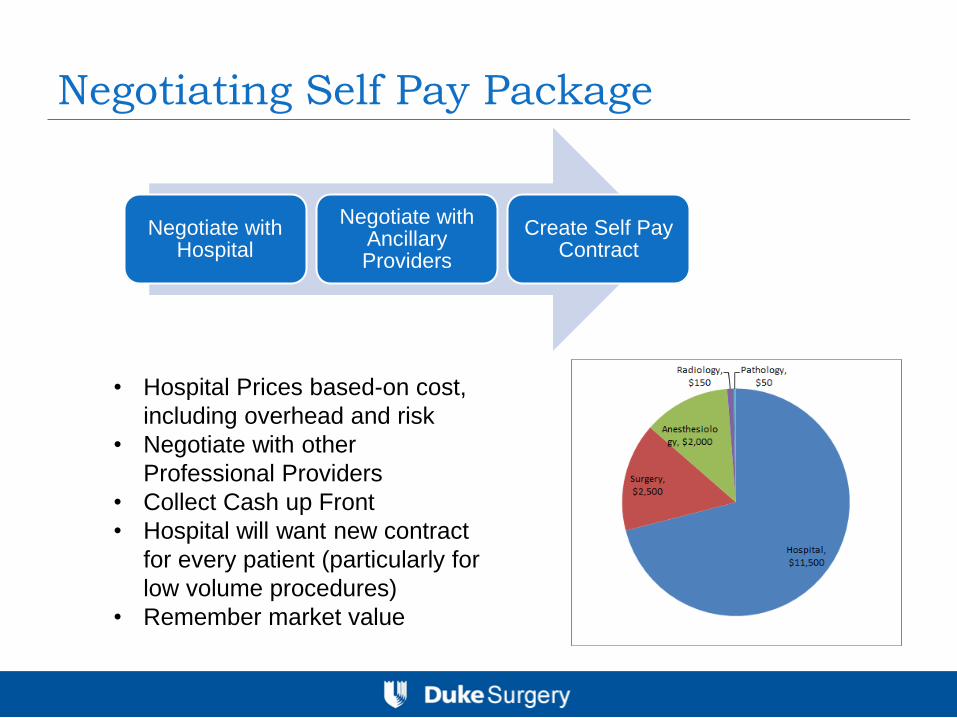
Negotiating Self Pay Package
Negotiate with Hospital
Negotiate with Ancillary Providers
Create Self Pay Contract
• Hospital Prices based-on cost,
including overhead and risk
• Negotiate with other
Professional Providers
• Collect Cash up Front
• Hospital will want new contract
for every patient (particularly for
low volume procedures)
• Remember market value
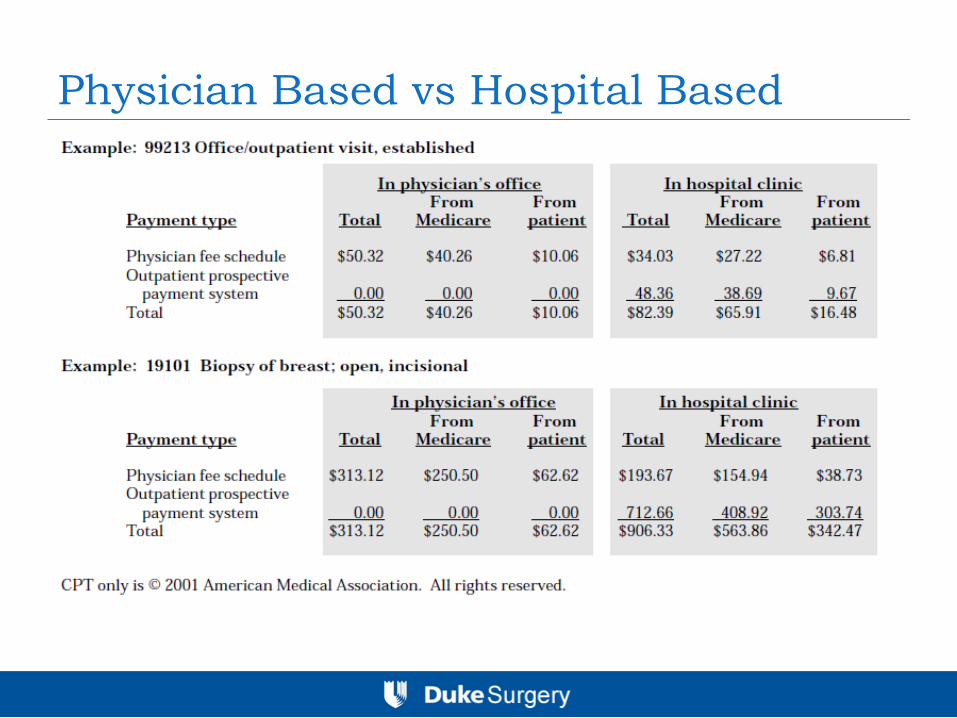
Physician Based vs Hospital Based
Billing and Coding
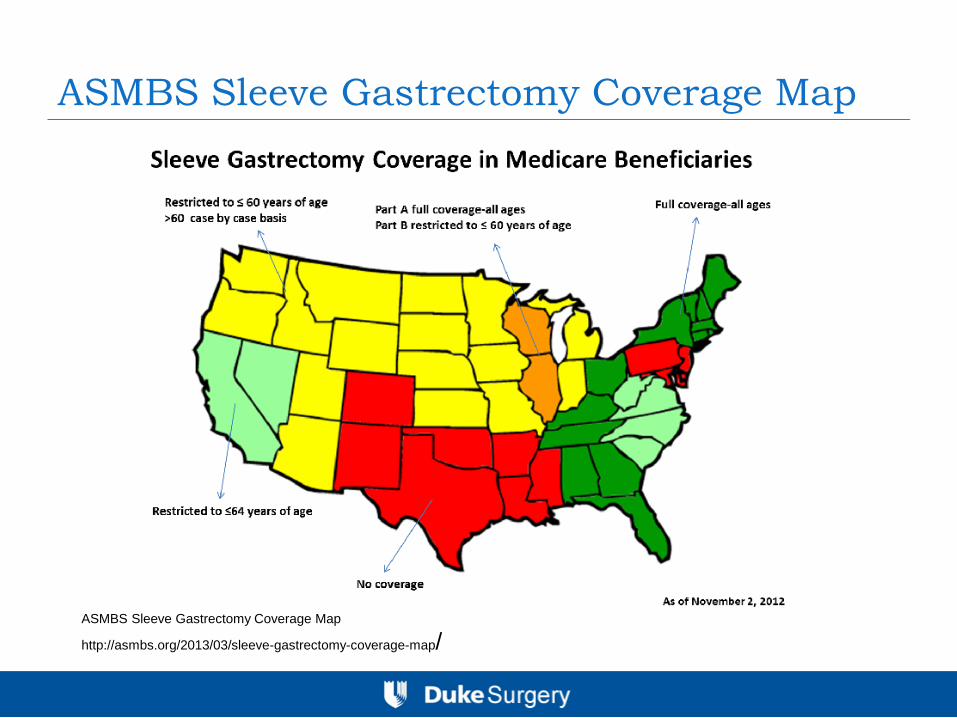
ASMBS Sleeve Gastrectomy Coverage Map
ASMBS Sleeve Gastrectomy Coverage Map
http://asmbs.org/2013/03/sleeve-gastrectomy-coverage-map/

Why E&M Coding Matters
Recovery Audit Program [RAC]
CMS: Medicare Fee-for-Service Recovery Audit Program Myths – December 17, 2012
http://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Recovery-Audit-Program/Downloads/RAC-Program-Myths-12-18-12.pdf
E&M Coding
Estimate E&M Coding: 14% - 20% of Total Surgeon
Income
Documentation should include:
Reason for encounter and relevant history, physical
exam findings and prior diagnostic tests
Assessment, clinical impression and diagnosis
Medical plan of care
Date and legible identity of observer
If you do not understand E&M Coding, get educated.
Pre Surgical Evaluations
Pre-Operative Visits
E&M visits conducted for pre-operative clearance
are part of the global period of the surgery, even if
they occur 2 – 7 days before the surgery.
E&M visits prior to the surgery are only payable if
directly for the decision for surgery
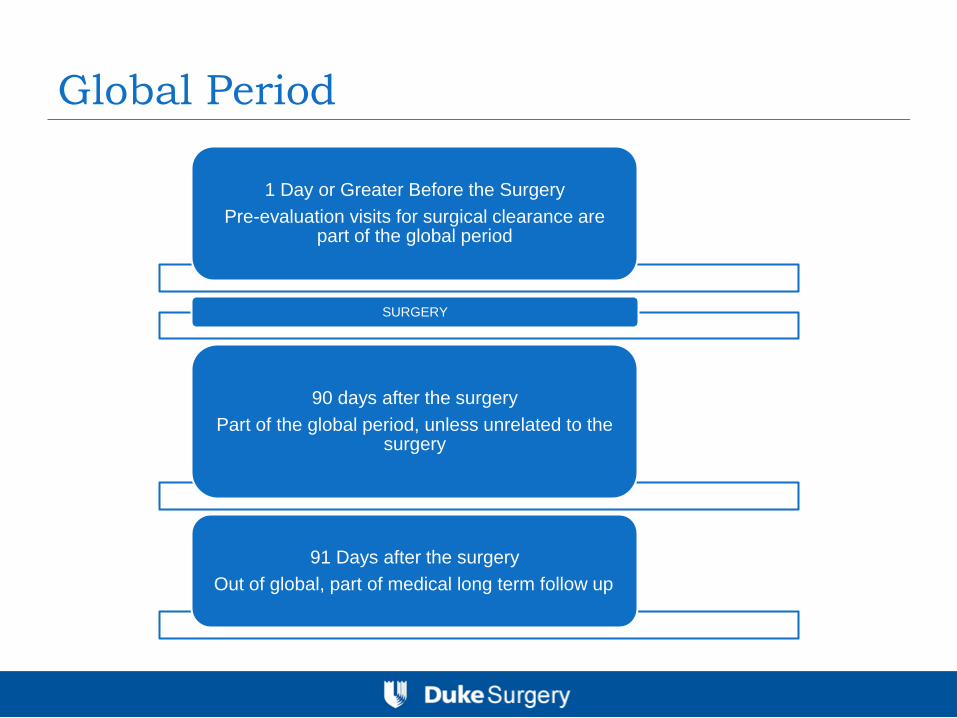
Global Period
1 Day or Greater Before the Surgery
Pre-evaluation visits for surgical clearance are part of the global period
SURGERY
90 days after the surgery
Part of the global period, unless unrelated to the surgery
91 Days after the surgery
Out of global, part of medical long term follow up
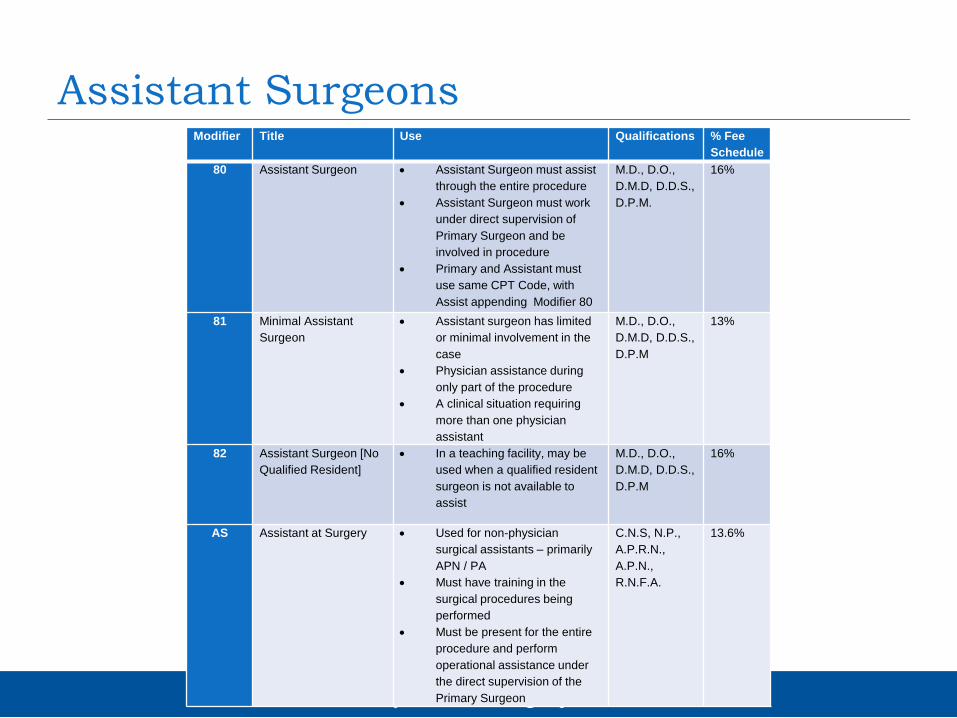
Assistant Surgeons Modifier Title Use Qualifications % Fee
Schedule
80 Assistant Surgeon Assistant Surgeon must assist
through the entire procedure
Assistant Surgeon must work
under direct supervision of
Primary Surgeon and be
involved in procedure
Primary and Assistant must
use same CPT Code, with
Assist appending Modifier 80
M.D., D.O.,
D.M.D, D.D.S.,
D.P.M.
16%
81 Minimal Assistant
Surgeon
Assistant surgeon has limited
or minimal involvement in the
case
Physician assistance during
only part of the procedure
A clinical situation requiring
more than one physician
assistant
M.D., D.O.,
D.M.D, D.D.S.,
D.P.M
13%
82 Assistant Surgeon [No
Qualified Resident]
In a teaching facility, may be
used when a qualified resident
surgeon is not available to
assist
M.D., D.O.,
D.M.D, D.D.S.,
D.P.M
16%
AS Assistant at Surgery Used for non-physician
surgical assistants – primarily
APN / PA
Must have training in the
surgical procedures being
performed
Must be present for the entire
procedure and perform
operational assistance under
the direct supervision of the
Primary Surgeon
C.N.S, N.P.,
A.P.R.N.,
A.P.N.,
R.N.F.A.
13.6%

Deploying Fellows and Physician
Extenders
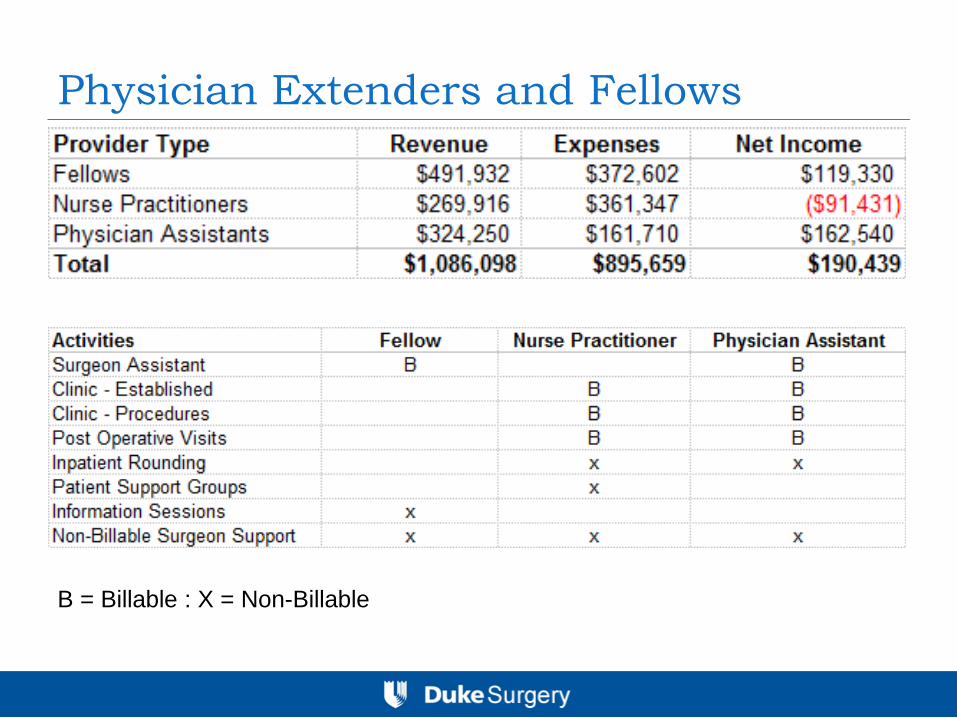
Physician Extenders and Fellows
B = Billable : X = Non-Billable
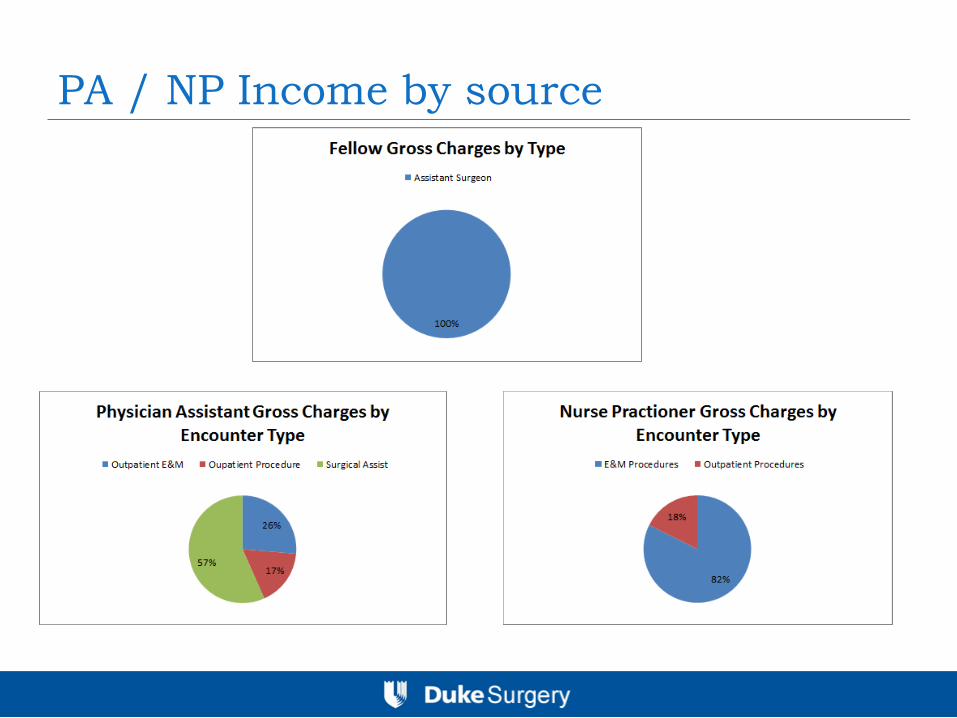
PA / NP Income by source
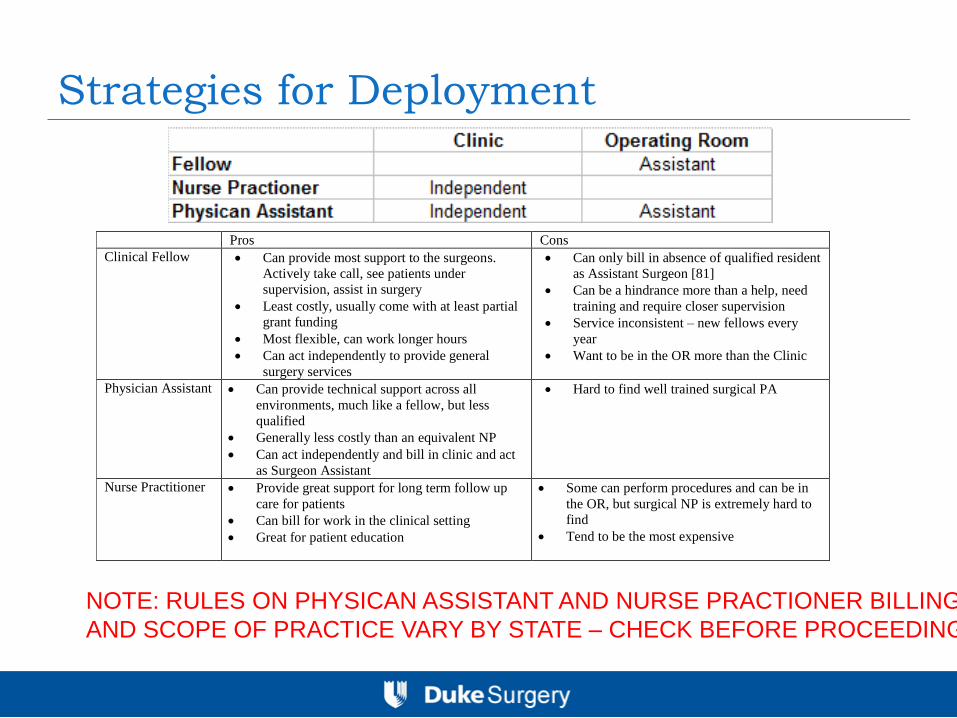
Strategies for Deployment
Pros Cons
Clinical Fellow Can provide most support to the surgeons.
Actively take call, see patients under
supervision, assist in surgery
Least costly, usually come with at least partial
grant funding
Most flexible, can work longer hours
Can act independently to provide general
surgery services
Can only bill in absence of qualified resident
as Assistant Surgeon [81]
Can be a hindrance more than a help, need
training and require closer supervision
Service inconsistent – new fellows every
year
Want to be in the OR more than the Clinic
Physician Assistant Can provide technical support across all
environments, much like a fellow, but less
qualified
Generally less costly than an equivalent NP
Can act independently and bill in clinic and act
as Surgeon Assistant
Hard to find well trained surgical PA
Nurse Practitioner Provide great support for long term follow up
care for patients
Can bill for work in the clinical setting
Great for patient education
Some can perform procedures and can be in
the OR, but surgical NP is extremely hard to
find
Tend to be the most expensive
NOTE: RULES ON PHYSICAN ASSISTANT AND NURSE PRACTIONER BILLING
AND SCOPE OF PRACTICE VARY BY STATE – CHECK BEFORE PROCEEDING
Recommendation on Extender Type
Depends on program and needs:
Academic program > Hire a fellow
Non-Academic Program - Technical Assistance in the OR
> Hire a PA
Clinic support> Hire an NP
OR and Clinic Support> Hire an PA
Incentive Plans for Fellows and Physician
Extenders
Fellow and extenders are assisting in the care of the
patients that you have recruited, and should be
incentivized.
Flat Rate Incentive based on individualized targets
($3,000 - $5,000)
Percent of Net Collections (5%) with a cap
When to Recruit a Physician Extender:
Financial Modeling Considerations
The recruitment decision is a decision based around
opportunity cost:
Opportunity cost is the cost of any activity measured in terms of the value of the next
best alternative forgone (that is not chosen). It is the sacrifice related to the second best
choice available to someone, or group, who has picked among several mutually exclusive
choices
Choice A: Physician Performs the Services and Collects the Income
Choice B: Recruit an Extender to Perform the Services and Collect the Revenue, while
Physician Does some Other Activity
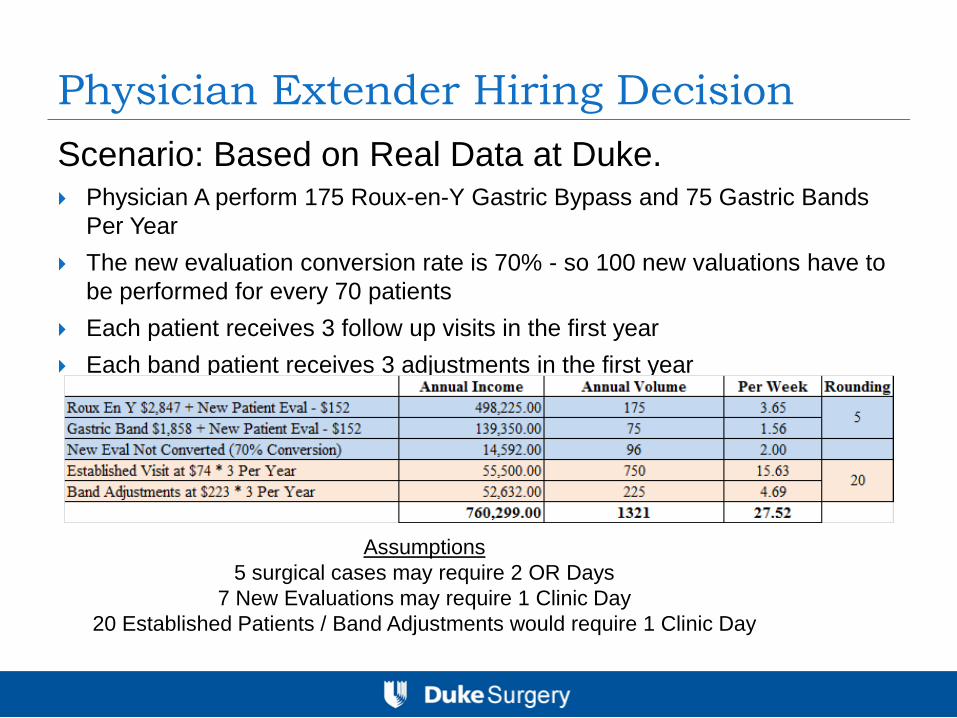
Physician Extender Hiring Decision
Scenario: Based on Real Data at Duke. Physician A perform 175 Roux-en-Y Gastric Bypass and 75 Gastric Bands
Per Year
The new evaluation conversion rate is 70% - so 100 new valuations have to
be performed for every 70 patients
Each patient receives 3 follow up visits in the first year
Each band patient receives 3 adjustments in the first year
Assumptions
5 surgical cases may require 2 OR Days
7 New Evaluations may require 1 Clinic Day
20 Established Patients / Band Adjustments would require 1 Clinic Day
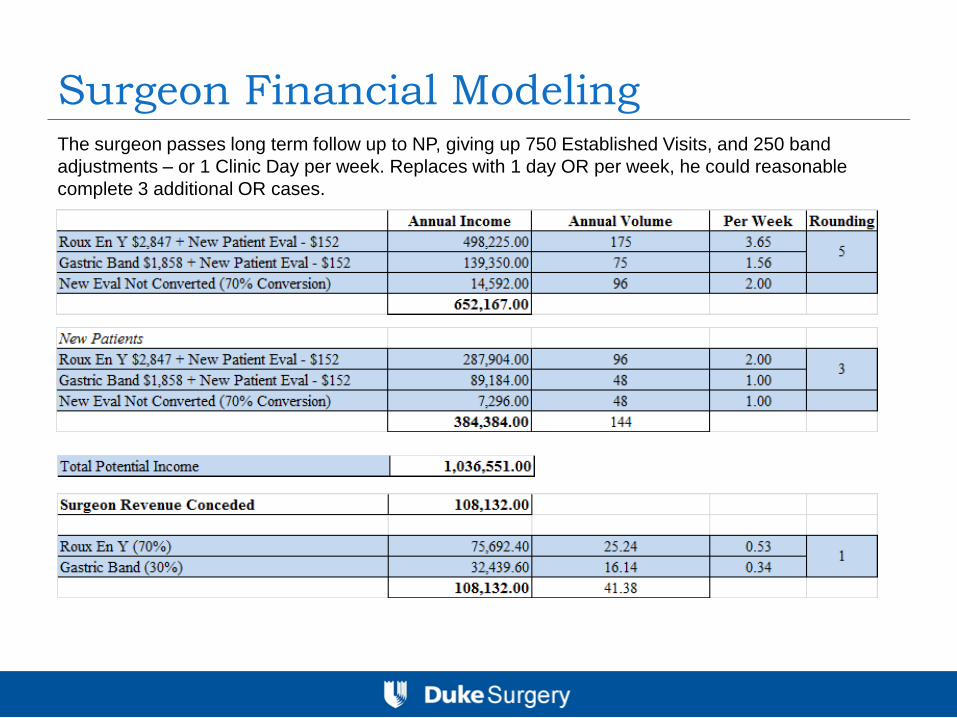
Surgeon Financial Modeling The surgeon passes long term follow up to NP, giving up 750 Established Visits, and 250 band
adjustments – or 1 Clinic Day per week. Replaces with 1 day OR per week, he could reasonable
complete 3 additional OR cases.
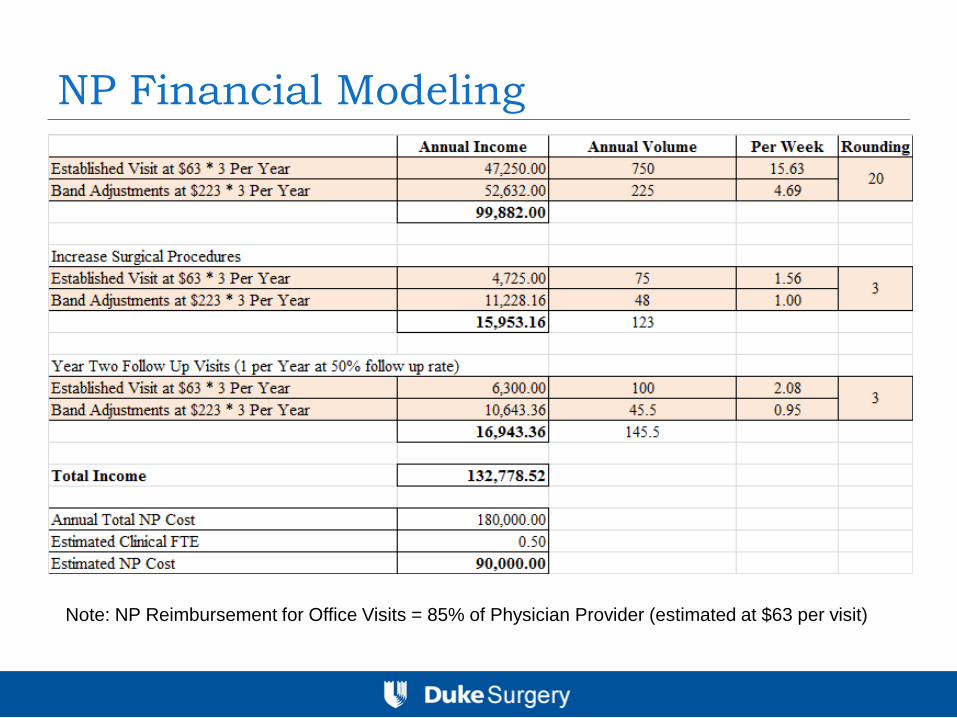
NP Financial Modeling
Note: NP Reimbursement for Office Visits = 85% of Physician Provider (estimated at $63 per visit)
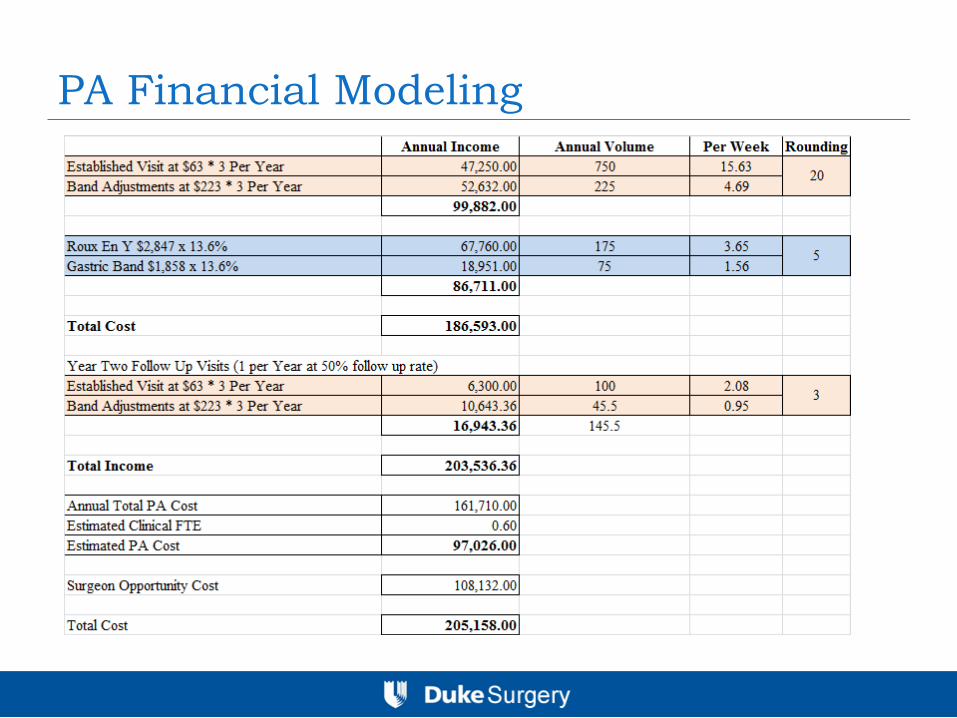
PA Financial Modeling

Diversifying Strategies to
Increase Revenue
Diagnostic EGDs: Refer or Manage
Refer:
Can create goodwill with GI (although not a critical referrer of patients).
Endo Suite scheduling not always convenient
Need credentialing to perform Endo in the suite, high risk patients may need to be completed in the OR
Manage:
Additional source for professional fee income, if performed in the hospital setting
$400 - $600 per patient for about 20-45 minutes time
Can be billed in the pre-operative phase if diagnosis supports (commonly GERD)
Ancillary Services in the Provider Setting
Vitamin and Supplement Sales
Pros: Can provide good nutritional support to patients, especially for those on malabsorptive diet.
Income for practice, usually 50% mark up, or potential $15 – 20 per patient per month. $100 patient = $2,000.
Cons: Can be difficult to administer in a large system – make sure you get on consignment
Transnasal Endoscopy
Pros: Provides in office diagnostics for some bariatric complications, GERD, and Hernia [ disposable sheaths]
Income for the practice can be reasonable, estimated at $260 per case, need to perform about 100 cases for break even on equipment and supplies
Cons: Not well tolerated by patients, difficult to find suitable patients
Intra-Operative Services
Intra-Operative EGD billing
Usually considered part of the operative procedure, if
used to “check” anastomosis
Can be used for diagnostic if unrelated to primary
procedure, common diagnosis “esophagitis”
Medical Necessity must be documented
Liver Biopsy
Must document the reason for taking a liver biopsy
Can be used for “fatty liver”
Post Bariatric Concierge Services
Exercise Physiology
Usually will involve employing the services of a exercise trainer with some medical background to develop individualized training regimens
Nutritional Consulting
Requires nutritional counseling on an ongoing bases from a dietician
Focus Groups
Provide long term support groups for the well being of the patients
PROs: Great for long term patient satisfaction and can improve outcomes
CONS: Hard to sell in a down economy, difficult for surgeons to make money – need to pay the ancillary providers.
Hospital Revenue On Call Compensation
Hospital Requirement (Bariatric Service)
Per Call Day Rate
Reimbursement Per Case for Uninsured/Underinsured
Medical Director Stipend
Reimbursement for administrative duties related to managing the program and participating in hospital required functions. Usually reimbursable at fixed annual rate [$25,000 - $50,000]
Service Line Co-Management
Reimbursement for managing the entire service line (surgical and related specialties) and includes much more involvement in business decisions related to the program. Contracts can be flat rate, and/or incentivized for improvements in efficiency, quality and financial metrics.
Non Surgical Physician Providers Endocrinology Base Sal. $180,000 [Partner]
PROS: Congruence with surgical practice for diabetic patients, can attract more diabetics, and generate more patients
CONS: Thrive of inpatient hospital setting, may not be ideal in ASc, low income specialty, income primarily derived from long term treatment – remission of diabetes could be a conflict
Psychiatry Base Sal. $200,000 [Buy – Hospital]
PROS: Absolute requirement for clearance of patients, may be option to employ
CONs: Can cause throughput issues if they become overwhelmed with patients, visits take much longer. Not all insurers reimburse the evaluation (Medicaid)
Bariatrician Base Sal. $150,000 [Buy – Practice]
PROs: Can provide higher level of post op care than a non-physician provider (NP/PA). Can develop an ancillary medical weight loss business for low BMI patients, and assist recruiting higher BMI patients
CONs: Bariatrician could compete for same obese patient population
Financial Outlook for Bariatric
Surgery
Tiered-Hospital Networks
Movement by the insurance companies to sensitize employees to the real cost of health – use tiered networks to drive down cost and increase quality Tiered Networks for Hospital and Physician Health Care – EBRI Issue Brief #260
Blue Select is a new “tiered benefit” health plan that can save employers as much as 10 percent* compared to traditional PPO plans. BCBSNC used its provider relationships, claims data and expertise to organize in-network hospitals and selected specialists (general surgery, OB/GYN, cardiology, orthopedics and gastroenterology) into two tiers based on quality, cost efficiency and accessibility. This product includes the following benefit levels:
Tier 1 represents the hospitals and selected specialists that receive BCBSNC’s top rating for clinical quality outcomes, cost efficiency or accessibility. Consumers pay less out-of-pocket costs when visiting a tier 1 provider compared to a tier 2 provider.
Tier 2 represents the remaining network hospitals and specialists that reach BCBSNC’s high standards for clinical quality outcomes and/or cost efficiency. Customers pay more to visit these providers
New BCBSNC Products Offer Cost Savings for Individuals and Employers
http://mediacenter.bcbsnc.com/pr/bluecross/new-bcbsnc-products-offer-cost-241718.aspx
Narrow Networks
Limited coverage products that will likely match the
EHB and offer limited benefits to employees and
employer groups.
Insurance Industry is preparing to enter the Health
Insurance Exchange in 2014, and they bring 150
million Americans with them
2010 – Narrow, Tiered Products accounted for 16% Market
2011 – Narrow, Tiered Products accounted for 20% Market
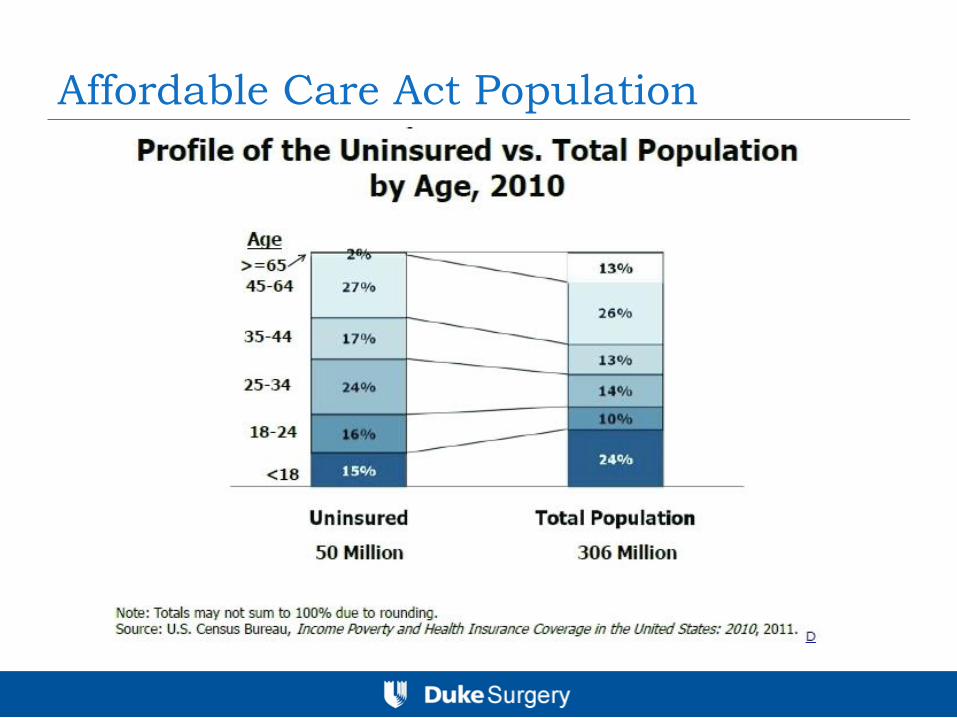
Affordable Care Act Population
Health Care Reform: EHB
Each State is required to have a Essential Health Benefits
(EHB) Plan that will form the basis of insurance plans in the
Health Insurance Exchanges (HIE)
The EHB is a federal or state-mandated minimum scope of
coverage that all health insurers in that market must
include in their plans. States can choose Federal EHB or to
opt for a state EHB, which must be based on the coverage
offered plan’s currently offered by the 3 largest small group
plan’s in the state.
Uninsured patients will receive tax credits to buy affordable
insurance from the exchange
Outlook Summary
The outlook depends on whether Bariatric Surgery is
included in State EHB Plans as this will set the bench
mark for commercial insurance narrow tiered plans.
Yes = 50 million more Americans will qualify for
surgery
No = more insurance products on the private market
with narrow tiers, which will exclude bariatric surgery
and therefore there will be less patients