Embed Size (px)
Citation preview

Research ArticleOptimization of Esophageal Ultrasound under Artificial FishSwarm Algorithm and Its Adoption in Treatment of VentricularSeptal Defect
Zhi Li 1 Guihe Chen 1 and Feng Wang 2
1Department of Cardiothoracic Surgery e First Peoplersquos Hospital of Huaihua Huaihua 418000 Hunan China2Department of Ultrasound e First Peoplersquos Hospital of Huaihua Huaihua 418000 Hunan China
Correspondence should be addressed to Zhi Li 15110473063stumailsduteducn
Received 9 September 2021 Revised 31 October 2021 Accepted 5 November 2021 Published 24 November 2021
Academic Editor M Pallikonda Rajasekaran
Copyright copy 2021 Zhi Li et al is is an open access article distributed under the Creative Commons Attribution License whichpermits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
is work was aimed at exploring the adoption value of the optimized and upgraded esophageal ultrasound in the treatment ofpatients with ventricular septal defect (VSD) by artificial fish swarm algorithm A model was built based on artificial fish swarmalgorithm A random ultrasonic optical signal in the database was decomposed several times and sparsity was optimized tocomplete partial optimization which was then extended to global optimization A total of 100 patients with ventricular septaldefect were divided into control group who underwent cardiopulmonary bypass under the guidance of three-dimensional thoracicultrasound and experimental group of ventricular septal defect occlusion under the guidance of esophageal ultrasound based onartificial fish swarm algorithm e results showed that the number of successful cases in the experimental group was 12 cases ofperimembranous type 10 cases of septal type 7 cases of simple membranous type 13 cases of muscular type 4 cases of subdrytype and 2 cases of ridge type e average length of operation after surgery was 7065 minutes the average length of ventilatorventilation was 1258 minutes and the average length of intensive care unit was 3779 minutes e average length of hospital stayafter surgery was 56 days and the average total length of hospital stay was 82 days which were better than the control group inmany aspects with statistical significance (Plt 005) In short the artificial fish swarm algorithm for esophageal ultrasound-guidedventricular septal defect closure had short operation time and good postoperative effect which was of high application value in theclinical treatment of patients with ventricular septal defect
1 Introduction
According to statistics heart ventricular septal defect issecond only to atrial septal defect in adult congenital heartdisease It refers to the abnormal development of the tissueseparating the left and right ventricles during embryoresulting in defects or holes [1 2] Generally patients withlarge defects will suffer from stunting fatigue shortness ofbreath dyspnea and other clinical symptoms If it is nottreated in time subsequent serious diseases such as heartfailure may result [3 4] Clinically three-dimensionaltransthoracic ultrasound is usually used for pathologicaldiagnosis In the diagnosis of obesity emphysema and otherpatients however this examination method has great lim-itations which will affect the quality of ultrasonic image [5]
In the traditional ultrasonic detection there are manydefects in the optical signal but there are also some re-dundant interference noises Ordinary pulse interferencenoise can be removed by simple filtering algorithm How-ever due to the noise emitted by some scattered grains orspecial materials it is difficult to extract the defect infor-mation by using traditional algorithms thus affecting thesubsequent signal processing [6 7]With the development ofscience and technology transesophageal ultrasound exam-ination gradually goes into the public vision It involves theinsertion of an esophageal probe into the patientrsquos body fromthe esophagus which is attached to the back wall of the heart[8ndash10] In this way it can avoid some interference tissue andintuitively detect the internal structure of the heart which ishelpful for the diagnosis of the disease
HindawiScientific ProgrammingVolume 2021 Article ID 7126251 9 pageshttpsdoiorg10115520217126251
Artificial fish swarm algorithm is a new optimizationalgorithm based on simulated fish swarm behavior proposedby Li et al in 2002 e basic idea is that the most fish in abody of water are at the most nutrient-rich parts of the bodyof water Based on this characteristic foraging behavior offish shoal is imitated so as to realize global optimization[11ndash13] e application of artificial fish swarm algorithm inesophageal ultrasound examination can find the optimaldata in signal decomposition with high efficiency optimizethe operation framework and improve the stability [14 15]Moreover it has good anti-interference ability which playsan important role in improving the image quality ofesophageal ultrasound [16 17]
In this experiment the artificial fish swarm algorithmwas used to establish the esophageal model By comparing aseries of indexes of the two groups of patients the appli-cation value of the esophageal ultrasound-guided blockingtechnique based on artificial fish swarm algorithm in theclinical treatment of VSD was comprehensively evaluatedexpected to provide a more reliable basis for the clinicaltreatment of VSD
2 Materials and Methods
21 Research Objects A total of 100 patients who wereadmitted to hospital from May 2019 to December 2020 andneeded to undergo ventricular septal defect surgery wererandomly divided into control group and experimentalgroup with 50 patients in each groupe patients in controlgroup ranged in age from 18 to 40 years with an average ageof 277 years ree-dimensional transthoracic ultrasound-guided cardiopulmonary bypass was used to establish theoperation e patients in experimental group were with anaverage age of 282 years who underwent VSD occlusionunder the guidance of esophageal ultrasound based on ar-tificial fish swarm algorithm Inclusion criteria are as follows(i) patients with cardiac function grades I-II (ii) patientswith no history of thoracic surgery (iii) patients withoutother organic lesions (iv) patients without esophageal andgastric ulcers one week before surgery (v) patients withcomplete clinical and imaging data Exclusion criteria are asfollows (i) patients with a history of thoracic surgery or withother organ diseases (ii) patients who lacked complianceand did not cooperate with the examination (iii) patientswith incomplete clinical data (iv) patients with pharyngealor esophagus lesionsis experiment had been approved bythe Ethics Committee of hospital All relevant matters of theexperiment had been informed to the patients themselvesand their families and informed consent had been signed
22 ree-Dimensional Transthoracic UltrasoundExamination e patient in the control group was placed inthe left decubitus position and the probe was placed besidethe sternum e probe was rotated every 1ndash3deg in the leftventricular long axis atrial septum ventricular septum twogroups of atrioventricular valves and pulmonary vein sec-tion five apical chambers and parasternal region Multiplesections of the heart with different positions angles sizes
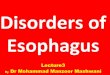
and shapes were obtained on the scanner By continuousrotation in the plane of 0ndash180deg the long and short axialsections of the ventricular septal defect were obtained frommultiple angles so that the location of the ventricular septaldefect was observed from multiple angles (Figure 1)
23 Surgery to Establish Cardiopulmonary Bypass e pa-tients in the control group received intramuscular injectionof 001mgkg atropine and intravenous injection of0125mgkg midazolam 30 minutes before surgery andanesthesia induction was performed with 3 μgkg fentanyl01mgkg vecuronium bromide and 125mgkg ketamineAfter intubation anesthesia machine was connected andintermittent positive pressure ventilation was performede periosteum of the sternumwas cut along themedian linewith an electric knife from the sternumnotch down to about5 cm below the xiphoid process en the pericardium wascut lengthwise midline between the reflexed part of the aortaand the diaphragm and one incision was made on both sidesof the lower incision e pericardial margin was suturedtogether with the soft tissue outside the sternum on bothsides and the sternum was fixed separately to expose theheart Inspections were made on each atrium ventricle andvein for size tension tremor and any local aberrationsPatients were given a routine half-dose of heparin andheparinized to initiate cardiopulmonary bypass First a venacava cuff was applied and two concentric purse-bag sutureswere made with No7 silk thread at the end of the ascendingaorta with heparin injected A small incision was made witha small round knife in the middle of the purse At the sametime when the round knife was put away an artery intu-bation was inserted into the incision of the ascending aortaand the artificial heart-lung machine was connected en apurse line was sewed into the right atrium and the rightchamber After incision the catheter was inserted into thesuperior and inferior vena cava and then connected with theartificial heart-lung machine A pad suture was made at theroot of the ascending aorta After draining of the gas fromthe needle with the cold cardioplegia the catheter wasinserted into the ascending aorta through the middle of thesuture line and the perfusion device was connected A longsuture line was made at the root of the right superiorpulmonary vein where it connected to the left atrium Aftersmall incision the drainage tube was inserted into the leftatrium and connected to the artificial heart-lung machineAfter it was confirmed that all the tubes were correct ex-tracorporeal circulation was performed and the superiorand inferior vena cava and ascending aorta were blocked afew minutes later 10mgkg of cold cardioplegia was infusedinto the aortic root perfusion tube e surface of the heartwas cooled with ice saline at 4degC At that point the heartstopped rapidly and cardiopulmonary bypass was initiatedAfter the operation the aorta was opened and the upper andlower lumen occlusion belts were opened for parallel cir-culation until the heart automatically rebounded en themachine was stopped heparin was neutralized potassiumwas supplemented to replenish blood volume and extu-bation was done after the condition was stable
2 Scientific Programming
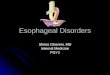
24 Ultrasonography of the Esophagus Patients in the ex-perimental group were supine and treated with generalanesthesia through nasal endotracheal intubation and theanesthesia drugs were the same as extracorporeal circulatione esophagus ultrasonic probe was placed into theesophagus and the left ventricular long axis atrial septumventricular septum two groups of atrioventricular valvesand the section of pulmonary vein namely the fourchambers of the heart apex were observed in the central partof the esophagus In this way the size and location of theventricular septal defect the length of connective tissuebetween the defect and the atrium and ventricle and theregurgitation of the right valve were determined Rotation ofthe probe to 30ndash45deg revealed a short axial section of the aorticroot and the passage of the left ventricular pump to theartery so that the length of the defect from the aortic valvewas assessed which was used to confirm its operationalstatus and valve orifice regurgitation Probe at 60ndash75deg canshow the right ventricular pump flow to the artery and thejunction between the right ventricle and the pulmonaryartery so as to determine the location and size of the defectthe availability of the right ventricular pump flow to theartery and the presence of pulmonary valve stenosis eprobe at 120deg can show the passage of the left ventricularpump to the artery and the junction between the left ven-tricle and the pulmonary artery erefore the length of thedefect site from the aortic valve and the obstruction of theleft ventricular pump blood flow channel to the artery weredetermined to assess the aortic valve regurgitate as pre-sented in Figure 2
25 Ventricular Septal Defect Closure In the experimentalgroup a small incision of about 3-4 cm was made at the lowersternum and xiphoid process in the supine position to separatethe xiphoid process e sternum was cut along the midlinewith an electric knife and the heart sac was cut and suspendedto expose the exterior of the right ventricle e free wall of theright ventricle was suspended on both sides to make twopurses and the right ventricle purses were cut open and loadedinto the guidance wire Patients were given a routine half-
amount of heparin heparinization Under the guidance ofesophageal ultrasound the proximal end of the guide wirepassed through the ventricular septal defect and entered thechannel through which the right ventricular pump blood flewto the artery en the puncture needle was removed andinserted into the dilating vessel sheath along the guide wireeguide wire was withdrawn and the conveying device and theheparinized occluder were placed into the dilated vessel sheathone by one e blocker released the disk in turn in the leftchamber of the defect and then retracted slightly which thenreleased the right ventricle disc in the right ventricle repeatedfor several times Esophageal ultrasound was used to examinewhether there was residual shunt at the interventricular septumand whether there was valve regurgitatione plugging devicewas adjusted to the appropriate position and the conveyingdevice was released after being fixed e purse was tied in aknot heparin was neutralized and the chest was stopped layerby layer and closed
26 Artificial Fish Swarm Algorithm
261 Construction of Artificial Fish Swarm AlgorithmModelIn the decomposition process of optical signals one of themost difficult steps is the calculation of the quantity productduring each decomposition It has large computation highredundancy index and low optimization efficiency econtent of artificial fish swarm algorithm is conductingsingle or partial optimization first so as to realize overalloptimization It can optimize the maximum value andminimum value in a certain part of the operation efficientlymaking the whole operation stable so as to effectivelyovercome the problem of excessive calculation e con-struction process of artificial fish swarm algorithm model isas follows
First it is supposed that M m1 m2 mλ1113864 1113865 is theatomic and molecular database for ultrasonic optical signalprocessing where mλ is the atom with the property λ Afternormalization of it mλ 1 A signal t to be decomposed isselected from the database M m1 m2 mλ1113864 1113865 which isoptimized as follows
(a) (b)
Figure 1 Image of apical four-chamber (a) and left ventricular short-axis view (b)
Scientific Programming 3
f(t) min m minus 1113944n
p1rimi
(1)
In equation (1) mi is the p-th basic signal and ri is itscorrelation decomposition coefficient In the decompositionprocess the biggest difficulty is the need to use several innerproduct operations which requires a large amount of cal-culation and a high redundancy index erefore the arti-ficial fish swarm algorithm is selected to realize theconstruction of the model and the improvement of workefficiency
It is assumed that the length of the signal t to bedecomposed is A a data corresponding to t is selected fromthe database to meet the following requirements
t mλp1113960 111396111138681113868111386811138681113868
11138681113868111386811138681113868 sup t mλ1113858 11138591113868111386811138681113868
1113868111386811138681113868 (2)
O1t is the difference between the actual observation valueand the fitted value after the original optical signal and theoptimized data are paired To implement signal decompo-sition the equation is as follows
fprime(t) t mλ1113858 1113859mλ + Oprimet (3)
s decompositions are performed on the difference be-tween the actual observation value and the fitted valueWhen the requirements of equation (4) are met equation (5)is meaningful
Ost mλ1113858 1113859
11138681113868111386811138681113868111386811138681113868 sup O
st mλp1113960 1113961
11138681113868111386811138681113868
11138681113868111386811138681113868 (4)
Ost O
st mλp1113960 1113961mλ + O
s+1t (5)
In equation (5) the difference O1t between the actualobservation value and the fitted value after c-th decompo-sitions is expressed as follows
fPrime(t) 1113944c
s1O
st mλp1113960 1113961mλ + O
ct (6)
When c increases Oct will be in a decreasing state untilit decreases to 0 en the improvement of the existingstructure of the ultrasonic optical signal is completed whichis expressed as follows
F(t) 1113944
c
s1O
st mλp1113960 1113961mλ (7)
e properties of ultrasonic optical signals are similar toGaussian functions When the signals are decomposed mλneeds to meet the requirements of normal distributionwhich is expressed as follows
mλ 1θ
radic eminus π(ϑminus ϕθ)2 cos(ϕx + η) (8)
Based on the theoretical concept of normal distributionan artificial fish swarm algorithm model is built to find theoptimal data When λ θ ϑ ϕ η1113864 1113865 is taken as a time-fre-quency distribution parameter the set range of all valuescontained in a specific requirement is expressed as follows
θ isin (1 A]
ϑ isin [0 A]
ϕ isin [0 2π)
η isin [02π]
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(9)
Based on the abovementioned time-frequency distri-bution parameters an artificial fish swarm algorithm modelis built which is expressed as follows
Oct mλ1113858 1113859
11138681113868111386811138681113868111386811138681113868
mλ 1θ
radic eminus π(ϑminus ϕθ)2 cos(ϕx + η)
(10)
e application of artificial fish swarm algorithm modelcan solve the disadvantages of large amount of calculationand high redundancy index caused by inner product op-eration and effectively improve the efficiency of ultrasonicoptical signal processing
(a) (b)
Figure 2 Apical four-chamber view (a) and short-axis view of aortic root (b)
4 Scientific Programming
262 Decomposition of Ultrasonic Optical Signal After theartificial fish swarm algorithm model is constructed it isused to realize overall optimization and effectively completethe decomposition and processing of ultrasonic opticalsignals A single factor in an artificial fish swarm is describedby a set of vectors E e1 e2 en1113864 1113865 where ei is set as thevector to be optimized and the food content of the fishswarm currently prescribed is expressed as follows
G f ei( 1113857 (11)
G is the ideal function to be achieved by the fish swarmand the distance hi between a single factor of the fish swarmand a single factor is expressed as follows
h ei ek( 1113857
1113944
n
i1ei minus ek( 1113857
2
11139741113972
(12)
e sight range of a fish swarmrsquos single factor and ad-jacent factors is expressed as follows
Adjoin ek|0lt hi kle view1113864 1113865 l 1 2 n (13)
In equation (13) l is the total amount of individualfactors in the fish swarm and the individual factors in thefish swarm in a transition state are expressed as follows
eq 1113936
ni1 ei(l)
l l 1 2 n (14)
e position and length of the transfer of a single factorin the fish swarm are expressed as follows
ei+1 ei + step middotek(l) minus ei(l)
ek(l) minus ei(l)
l 1 2 n (15)
To ensure the stability of the calculation process a singlefactor must be handled within a transferable range and mustnot exceed the corresponding range If there is a mistake inone operation it is necessary to perform the overall oper-ation again until the optimal solution is searched
27 Statistical Analysis SPSS 240 was employed for datastatistics and analysis Meanplusmn standard deviation (xplusmn s) washow measurement data were expressed and percentage ()was how count data were expressed e t-test was usedwhen the experimental data conformed to normal distri-bution χ2 test was used for univariate analysis of relatedfactors and logistic regression analysis was used for mul-tivariate analysis Plt 005 was considered statisticallysignificant
3 Results
31 Comparison of General Clinical Data of the TwoGroups ofPatients Figure 3 below shows the comparison of generalclinical data between two groups of patients ere were nosubstantial differences in age sex ratio height and weightbetween the control group and the experimental group(Pgt 005)
32 Comparison of the Number of Successful Operations be-tween the Two Groups Figure 4 shows that after three-di-mensional transthoracic ultrasound-guided cardiopulmonarybypass was established in control group there were 12 cases ofperimembrane type of ventricular septal defect of which 10cases were successful 10 cases of septal valve type of which 8cases were successful 8 cases of simple membranous type ofwhich 6 cases were successful 15 cases of muscular type ofwhich 12 cases were successful 2 cases of substem type ofwhich 1 case was successful 3 cases of crest type of which 3cases were successful In the experimental group there were 13cases 11 cases 7 cases 13 cases 4 cases and 2 cases of ven-tricular septal defect occlusion under the guidance of esoph-ageal ultrasound based on artificial fish swarm algorithm enumber of successful cases were 12 10 7 13 4 and 2 re-spectively e number of successful cases of ventricular septaldefect closure guided by esophageal ultrasound based on ar-tificial fish swarm algorithm was greatly higher than that in thecontrol group and the difference was considerable (Plt 005)
33 Comparison of Preoperative and Postoperative LeftVentricular Status between the Two Groups Figure 5 showsthat the left ventricular size and the left ventricular end-dia-stolic volume were reduced to some extent between the controlgroup and the experimental group at three days one monthand three months after surgery but the differences were notconsiderable compared with those before surgery (Pgt 005)
34 Comparison of Cardiac Function between the TwoGroupsof Patients before and after Surgery In Figure 6 there was noconsiderable difference in left ventricular ejection fractionand left ventricular short-axis shorting rate in the fourpostoperative reexaminations between the control groupand the experimental group (Pgt 005)
35 Comparison of the Number of Cases of PostoperativePericardial Effusion andArrhythmia between theTwoGroupsFigure 7 shows that in the control group postoperativepericardial effusion occurred in 15 cases incomplete right
Age Male Female Height Weight
Control groupExperimental group
020406080
100120140160180200
Num
eric
al
Figure 3 Comparison of general clinical data of the two groups ofpatients
Scientific Programming 5
bundle branch block in 31 cases complete right bundlebranch block in 4 cases left anterior branch block in 1 caseand IIIdeg atrioventricular block in 1 case e number ofthese complications in the test group was 6 20 1 0 and 0respectively e number of cases of pericardial effusionand arrhythmia in experimental group was greatly inferiorto that in control group with statistical significance(Plt 005)
36 Comparison of Duration of Operation Duration ofVentilator Ventilation and Duration of Intensive Care Unitbetween the Two Groups Figure 8 shows that in thecontrol group the average duration of operation was15788 minutes the average duration of ventilator ven-tilation was 4607 minutes and the average duration ofintensive care unit was 11876 minutes In the
experimental group the mean operative duration was7065 minutes the mean ventilator duration was 1258minutes and the mean ICU duration was 3779 minutese durations of operation ventilator ventilation andintensive care unit in experimental group were greatlyshorter than those in control group with statisticalsignificance (Plt 005)
37 Comparison of Hospitalization Days between the TwoGroups Figure 9 shows that the average length of hospitalstay in the control group was 75 days and the average totallength of hospital stay was 138 days e mean length ofhospital stay in the experimental group was 56 days and themean total length of hospital stay was 82 days e length ofhospital stay in experimental group was greatly inferior tothat in control group (Plt 005)
A B C D E FType of ventricular septal defect
Control groupExperimental group
02468
10121416
Num
ber o
f cas
es
(a)
Control groupExperimental group
A B C D E FType of ventricular septal defect
0
2
4
6
8
10
12
14
Num
ber o
f cas
es
(b)
Figure 4 Comparison of the number of successful operations between the two groups (a) the number of cases of ventricular septal defecttypes in the two groups (b) the number of successful operations (A) perimembrane type (B) septal type (C) simple membrane type(D) muscle type (E) subdry type (F) ridge type lowastindicates that the number of successful operations in the experimental group was greatlydifferent from the control group (Plt 005)
A B C DTime
Control groupExperimental group
32325
33335
34345
35355
36365
Left
vent
ricul
ar si
ze (m
m)
30
31
32
33
34
35
36
Left
vent
ricul
ar si
ze (m
m)
(a)
Control groupExperimental group
A B C DTime
40
42
44
46
48
50
52
41
43
45
47
49
51
53Le
ft ve
ntric
ular
end
dias
tolic
volu
me (
mL)
(b)
Figure 5 Comparison of left ventricular state before and after surgery between the two groups (a) e comparison of the left ventricularsize before and after surgery (b) the comparison of the left ventricular end-diastolic volume before and after surgery (A) before surgery(B) three days after surgery (C) one month after surgery and (D) three months after surgery
6 Scientific Programming
38 Ultrasonic Images of Esophagus before and after the Ap-plication of Artificial Fish SwarmAlgorithm A patient male22 years old had shortness of breath and dyspnea for morethan half a year During routine esophageal ultrasoundexamination due to the equipment level and other reasonsultrasound image contrast was insufficient ere were re-dundant interference noise and poor spatial resolutionwhich brought some difficulties for the observation of theheart environment e artificial fish swarm algorithm wasapplied in esophageal ultrasound to improve the decom-position speed of optical signals and the searching signalresults were more accurate and the imaging was clearer asillustrated in Figure 10
4 Discussion
An artificial fish swarm algorithm was selected in this ex-periment Its essence was simulating the foraging clusteringand tail-chasing behaviors of fish swarm by constructing anartificial fish model so as to achieve overall optimization[18] In this experiment an atom was randomly selectedfrom the database and optimized by maxima and minimanormalization multiple decomposition etc to complete theoptimization of single factor en the artificial fish swarmalgorithm model was built and then the objective of globaloptimization was approached gradually through opticalsignal decomposition and processing in the designatedrange e artificial fish swarm algorithm was applied to a
A
B
C
D
E
Com
plic
atio
n
Control groupExperimental group
10 20 30 40 50 600Number of cases
Figure 7 Comparison of the number of cases of postoperativepericardial effusion and arrhythmia between the two groups (A)pericardial effusion (B) incomplete right bundle branch block (C)complete right bundle branch block (D) left anterior branch block(E) IIIdeg atrioventricular block lowastindicated that the number of pa-tients with pericardial effusion and incomplete right bundle branchblock in the experimental group was greatly different from that inthe control group (Plt 005)
A B C D ETim
e
Left ventricular ejection fraction ()60626466687072747678
Control groupExperimental group
(a)
31
33
35
37
39
41
43
45
A B C D E
Tim
e
Left ventricular minor axis decurtation ()
Control groupExperimental group
(b)
Figure 6 Comparison of cardiac function between the two groups of patients before and after surgery (a) Comparison of the left ventricularejection fraction before and after surgery (b) comparison of the left ventricular short-axis shortening rate before and after surgery(A) before surgery (B) first review after surgery (C) second review after surgery (D) third review after surgery and (E) fourth review aftersurgery
Operation timeDuration of mechanical ventilationDuration of intensive care unit
0200400600800
100012001400160018002000
Tim
e (m
in)
Experimentalgroup
Control group
Figure 8 Comparison of the durations of operation ventilatorventilation and intensive care unit between the two groupslowastindicated that there were substantial differences in the durationsof operation ventilator ventilation and intensive care unit in theexperimental group compared with the control group (Plt 005)
Scientific Programming 7
collection of 100 patients with ventricular septal defectsrequiring surgical treatment e patients in control groupwere treated with three-dimensional transthoracic ultra-sound-guided cardiopulmonary bypass and those in ex-perimental group were treated with artificial fish-basedultrasound-guided ventricular septal defect closure eresults showed that the number of successful cases in theexperimental group was greatly higher than that in thecontrol group (Plt 005) e number of cases with peri-cardial effusion and arrhythmia after operation was inferiorto that of control group and the difference was notable(Plt 005) Moreover the durations of operation ventilatorventilation and intensive care unit were greatly shorter thanthose of the control group (Plt 005) e length of hospi-talization was greatly inferior to that of the control group(Plt 005) In 2021 Yang et al [19] pointed out that theocclusion of ventricular septal defect under the guidance ofesophageal ultrasound had a high safety and feasibilitybecause of shorter operation time and less intraoperativebleeding compared with traditional repair In this study the
reliability of this statement was verified e ventricularseptal defect occlusion under the guidance of esophagealultrasound based on artificial fish swarm was performed Ithad short operation time short hospitalization days andgood prognosis and was acceptable to patientsrsquo familymembers which was of great significance in the treatment ofventricular septal defect
5 Conclusion
In this study the artificial fish swarm algorithm was used tooptimize the traditional esophageal ultrasound and 100patients requiring surgical treatment of ventricular septaldefects were collected as the research subjects e resultsshowed that the experimental group was better than thecontrol group in terms of the number of successful oper-ations the number of cases with pericardial effusion andarrhythmia after operation the duration of operation theduration of ventilator ventilation the duration of intensivecare unit and the length of hospital stay (Plt 005) However
Postoperativehospitalization
Totalhospitalization
Control groupExperimental group
02468
10121416
Tim
e (da
y)
Figure 9 Comparison of hospitalization days between the two groups lowastindicated that the average length of postoperative hospital stayand the average total length of postoperative hospital stay in the experimental group were greatly different from those of control group(Plt 005)
(a) (b)
Figure 10 Original ultrasonic image of esophagus (a) and ultrasonic image of esophagus after the application of artificial fish swarmalgorithm (b)
8 Scientific Programming
the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9

Artificial fish swarm algorithm is a new optimizationalgorithm based on simulated fish swarm behavior proposedby Li et al in 2002 e basic idea is that the most fish in abody of water are at the most nutrient-rich parts of the bodyof water Based on this characteristic foraging behavior offish shoal is imitated so as to realize global optimization[11ndash13] e application of artificial fish swarm algorithm inesophageal ultrasound examination can find the optimaldata in signal decomposition with high efficiency optimizethe operation framework and improve the stability [14 15]Moreover it has good anti-interference ability which playsan important role in improving the image quality ofesophageal ultrasound [16 17]
In this experiment the artificial fish swarm algorithmwas used to establish the esophageal model By comparing aseries of indexes of the two groups of patients the appli-cation value of the esophageal ultrasound-guided blockingtechnique based on artificial fish swarm algorithm in theclinical treatment of VSD was comprehensively evaluatedexpected to provide a more reliable basis for the clinicaltreatment of VSD
2 Materials and Methods
21 Research Objects A total of 100 patients who wereadmitted to hospital from May 2019 to December 2020 andneeded to undergo ventricular septal defect surgery wererandomly divided into control group and experimentalgroup with 50 patients in each groupe patients in controlgroup ranged in age from 18 to 40 years with an average ageof 277 years ree-dimensional transthoracic ultrasound-guided cardiopulmonary bypass was used to establish theoperation e patients in experimental group were with anaverage age of 282 years who underwent VSD occlusionunder the guidance of esophageal ultrasound based on ar-tificial fish swarm algorithm Inclusion criteria are as follows(i) patients with cardiac function grades I-II (ii) patientswith no history of thoracic surgery (iii) patients withoutother organic lesions (iv) patients without esophageal andgastric ulcers one week before surgery (v) patients withcomplete clinical and imaging data Exclusion criteria are asfollows (i) patients with a history of thoracic surgery or withother organ diseases (ii) patients who lacked complianceand did not cooperate with the examination (iii) patientswith incomplete clinical data (iv) patients with pharyngealor esophagus lesionsis experiment had been approved bythe Ethics Committee of hospital All relevant matters of theexperiment had been informed to the patients themselvesand their families and informed consent had been signed
22 ree-Dimensional Transthoracic UltrasoundExamination e patient in the control group was placed inthe left decubitus position and the probe was placed besidethe sternum e probe was rotated every 1ndash3deg in the leftventricular long axis atrial septum ventricular septum twogroups of atrioventricular valves and pulmonary vein sec-tion five apical chambers and parasternal region Multiplesections of the heart with different positions angles sizes
and shapes were obtained on the scanner By continuousrotation in the plane of 0ndash180deg the long and short axialsections of the ventricular septal defect were obtained frommultiple angles so that the location of the ventricular septaldefect was observed from multiple angles (Figure 1)
23 Surgery to Establish Cardiopulmonary Bypass e pa-tients in the control group received intramuscular injectionof 001mgkg atropine and intravenous injection of0125mgkg midazolam 30 minutes before surgery andanesthesia induction was performed with 3 μgkg fentanyl01mgkg vecuronium bromide and 125mgkg ketamineAfter intubation anesthesia machine was connected andintermittent positive pressure ventilation was performede periosteum of the sternumwas cut along themedian linewith an electric knife from the sternumnotch down to about5 cm below the xiphoid process en the pericardium wascut lengthwise midline between the reflexed part of the aortaand the diaphragm and one incision was made on both sidesof the lower incision e pericardial margin was suturedtogether with the soft tissue outside the sternum on bothsides and the sternum was fixed separately to expose theheart Inspections were made on each atrium ventricle andvein for size tension tremor and any local aberrationsPatients were given a routine half-dose of heparin andheparinized to initiate cardiopulmonary bypass First a venacava cuff was applied and two concentric purse-bag sutureswere made with No7 silk thread at the end of the ascendingaorta with heparin injected A small incision was made witha small round knife in the middle of the purse At the sametime when the round knife was put away an artery intu-bation was inserted into the incision of the ascending aortaand the artificial heart-lung machine was connected en apurse line was sewed into the right atrium and the rightchamber After incision the catheter was inserted into thesuperior and inferior vena cava and then connected with theartificial heart-lung machine A pad suture was made at theroot of the ascending aorta After draining of the gas fromthe needle with the cold cardioplegia the catheter wasinserted into the ascending aorta through the middle of thesuture line and the perfusion device was connected A longsuture line was made at the root of the right superiorpulmonary vein where it connected to the left atrium Aftersmall incision the drainage tube was inserted into the leftatrium and connected to the artificial heart-lung machineAfter it was confirmed that all the tubes were correct ex-tracorporeal circulation was performed and the superiorand inferior vena cava and ascending aorta were blocked afew minutes later 10mgkg of cold cardioplegia was infusedinto the aortic root perfusion tube e surface of the heartwas cooled with ice saline at 4degC At that point the heartstopped rapidly and cardiopulmonary bypass was initiatedAfter the operation the aorta was opened and the upper andlower lumen occlusion belts were opened for parallel cir-culation until the heart automatically rebounded en themachine was stopped heparin was neutralized potassiumwas supplemented to replenish blood volume and extu-bation was done after the condition was stable
2 Scientific Programming
24 Ultrasonography of the Esophagus Patients in the ex-perimental group were supine and treated with generalanesthesia through nasal endotracheal intubation and theanesthesia drugs were the same as extracorporeal circulatione esophagus ultrasonic probe was placed into theesophagus and the left ventricular long axis atrial septumventricular septum two groups of atrioventricular valvesand the section of pulmonary vein namely the fourchambers of the heart apex were observed in the central partof the esophagus In this way the size and location of theventricular septal defect the length of connective tissuebetween the defect and the atrium and ventricle and theregurgitation of the right valve were determined Rotation ofthe probe to 30ndash45deg revealed a short axial section of the aorticroot and the passage of the left ventricular pump to theartery so that the length of the defect from the aortic valvewas assessed which was used to confirm its operationalstatus and valve orifice regurgitation Probe at 60ndash75deg canshow the right ventricular pump flow to the artery and thejunction between the right ventricle and the pulmonaryartery so as to determine the location and size of the defectthe availability of the right ventricular pump flow to theartery and the presence of pulmonary valve stenosis eprobe at 120deg can show the passage of the left ventricularpump to the artery and the junction between the left ven-tricle and the pulmonary artery erefore the length of thedefect site from the aortic valve and the obstruction of theleft ventricular pump blood flow channel to the artery weredetermined to assess the aortic valve regurgitate as pre-sented in Figure 2
25 Ventricular Septal Defect Closure In the experimentalgroup a small incision of about 3-4 cm was made at the lowersternum and xiphoid process in the supine position to separatethe xiphoid process e sternum was cut along the midlinewith an electric knife and the heart sac was cut and suspendedto expose the exterior of the right ventricle e free wall of theright ventricle was suspended on both sides to make twopurses and the right ventricle purses were cut open and loadedinto the guidance wire Patients were given a routine half-
amount of heparin heparinization Under the guidance ofesophageal ultrasound the proximal end of the guide wirepassed through the ventricular septal defect and entered thechannel through which the right ventricular pump blood flewto the artery en the puncture needle was removed andinserted into the dilating vessel sheath along the guide wireeguide wire was withdrawn and the conveying device and theheparinized occluder were placed into the dilated vessel sheathone by one e blocker released the disk in turn in the leftchamber of the defect and then retracted slightly which thenreleased the right ventricle disc in the right ventricle repeatedfor several times Esophageal ultrasound was used to examinewhether there was residual shunt at the interventricular septumand whether there was valve regurgitatione plugging devicewas adjusted to the appropriate position and the conveyingdevice was released after being fixed e purse was tied in aknot heparin was neutralized and the chest was stopped layerby layer and closed
26 Artificial Fish Swarm Algorithm
261 Construction of Artificial Fish Swarm AlgorithmModelIn the decomposition process of optical signals one of themost difficult steps is the calculation of the quantity productduring each decomposition It has large computation highredundancy index and low optimization efficiency econtent of artificial fish swarm algorithm is conductingsingle or partial optimization first so as to realize overalloptimization It can optimize the maximum value andminimum value in a certain part of the operation efficientlymaking the whole operation stable so as to effectivelyovercome the problem of excessive calculation e con-struction process of artificial fish swarm algorithm model isas follows
First it is supposed that M m1 m2 mλ1113864 1113865 is theatomic and molecular database for ultrasonic optical signalprocessing where mλ is the atom with the property λ Afternormalization of it mλ 1 A signal t to be decomposed isselected from the database M m1 m2 mλ1113864 1113865 which isoptimized as follows
(a) (b)
Figure 1 Image of apical four-chamber (a) and left ventricular short-axis view (b)
Scientific Programming 3
f(t) min m minus 1113944n
p1rimi
(1)
In equation (1) mi is the p-th basic signal and ri is itscorrelation decomposition coefficient In the decompositionprocess the biggest difficulty is the need to use several innerproduct operations which requires a large amount of cal-culation and a high redundancy index erefore the arti-ficial fish swarm algorithm is selected to realize theconstruction of the model and the improvement of workefficiency
It is assumed that the length of the signal t to bedecomposed is A a data corresponding to t is selected fromthe database to meet the following requirements
t mλp1113960 111396111138681113868111386811138681113868
11138681113868111386811138681113868 sup t mλ1113858 11138591113868111386811138681113868
1113868111386811138681113868 (2)
O1t is the difference between the actual observation valueand the fitted value after the original optical signal and theoptimized data are paired To implement signal decompo-sition the equation is as follows
fprime(t) t mλ1113858 1113859mλ + Oprimet (3)
s decompositions are performed on the difference be-tween the actual observation value and the fitted valueWhen the requirements of equation (4) are met equation (5)is meaningful
Ost mλ1113858 1113859
11138681113868111386811138681113868111386811138681113868 sup O
st mλp1113960 1113961
11138681113868111386811138681113868
11138681113868111386811138681113868 (4)
Ost O
st mλp1113960 1113961mλ + O
s+1t (5)
In equation (5) the difference O1t between the actualobservation value and the fitted value after c-th decompo-sitions is expressed as follows
fPrime(t) 1113944c
s1O
st mλp1113960 1113961mλ + O
ct (6)
When c increases Oct will be in a decreasing state untilit decreases to 0 en the improvement of the existingstructure of the ultrasonic optical signal is completed whichis expressed as follows
F(t) 1113944
c
s1O
st mλp1113960 1113961mλ (7)
e properties of ultrasonic optical signals are similar toGaussian functions When the signals are decomposed mλneeds to meet the requirements of normal distributionwhich is expressed as follows
mλ 1θ
radic eminus π(ϑminus ϕθ)2 cos(ϕx + η) (8)
Based on the theoretical concept of normal distributionan artificial fish swarm algorithm model is built to find theoptimal data When λ θ ϑ ϕ η1113864 1113865 is taken as a time-fre-quency distribution parameter the set range of all valuescontained in a specific requirement is expressed as follows
θ isin (1 A]
ϑ isin [0 A]
ϕ isin [0 2π)
η isin [02π]
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(9)
Based on the abovementioned time-frequency distri-bution parameters an artificial fish swarm algorithm modelis built which is expressed as follows
Oct mλ1113858 1113859
11138681113868111386811138681113868111386811138681113868
mλ 1θ
radic eminus π(ϑminus ϕθ)2 cos(ϕx + η)
(10)
e application of artificial fish swarm algorithm modelcan solve the disadvantages of large amount of calculationand high redundancy index caused by inner product op-eration and effectively improve the efficiency of ultrasonicoptical signal processing
(a) (b)
Figure 2 Apical four-chamber view (a) and short-axis view of aortic root (b)
4 Scientific Programming
262 Decomposition of Ultrasonic Optical Signal After theartificial fish swarm algorithm model is constructed it isused to realize overall optimization and effectively completethe decomposition and processing of ultrasonic opticalsignals A single factor in an artificial fish swarm is describedby a set of vectors E e1 e2 en1113864 1113865 where ei is set as thevector to be optimized and the food content of the fishswarm currently prescribed is expressed as follows
G f ei( 1113857 (11)
G is the ideal function to be achieved by the fish swarmand the distance hi between a single factor of the fish swarmand a single factor is expressed as follows
h ei ek( 1113857
1113944
n
i1ei minus ek( 1113857
2
11139741113972
(12)
e sight range of a fish swarmrsquos single factor and ad-jacent factors is expressed as follows
Adjoin ek|0lt hi kle view1113864 1113865 l 1 2 n (13)
In equation (13) l is the total amount of individualfactors in the fish swarm and the individual factors in thefish swarm in a transition state are expressed as follows
eq 1113936
ni1 ei(l)
l l 1 2 n (14)
e position and length of the transfer of a single factorin the fish swarm are expressed as follows
ei+1 ei + step middotek(l) minus ei(l)
ek(l) minus ei(l)
l 1 2 n (15)
To ensure the stability of the calculation process a singlefactor must be handled within a transferable range and mustnot exceed the corresponding range If there is a mistake inone operation it is necessary to perform the overall oper-ation again until the optimal solution is searched
27 Statistical Analysis SPSS 240 was employed for datastatistics and analysis Meanplusmn standard deviation (xplusmn s) washow measurement data were expressed and percentage ()was how count data were expressed e t-test was usedwhen the experimental data conformed to normal distri-bution χ2 test was used for univariate analysis of relatedfactors and logistic regression analysis was used for mul-tivariate analysis Plt 005 was considered statisticallysignificant
3 Results
31 Comparison of General Clinical Data of the TwoGroups ofPatients Figure 3 below shows the comparison of generalclinical data between two groups of patients ere were nosubstantial differences in age sex ratio height and weightbetween the control group and the experimental group(Pgt 005)
32 Comparison of the Number of Successful Operations be-tween the Two Groups Figure 4 shows that after three-di-mensional transthoracic ultrasound-guided cardiopulmonarybypass was established in control group there were 12 cases ofperimembrane type of ventricular septal defect of which 10cases were successful 10 cases of septal valve type of which 8cases were successful 8 cases of simple membranous type ofwhich 6 cases were successful 15 cases of muscular type ofwhich 12 cases were successful 2 cases of substem type ofwhich 1 case was successful 3 cases of crest type of which 3cases were successful In the experimental group there were 13cases 11 cases 7 cases 13 cases 4 cases and 2 cases of ven-tricular septal defect occlusion under the guidance of esoph-ageal ultrasound based on artificial fish swarm algorithm enumber of successful cases were 12 10 7 13 4 and 2 re-spectively e number of successful cases of ventricular septaldefect closure guided by esophageal ultrasound based on ar-tificial fish swarm algorithm was greatly higher than that in thecontrol group and the difference was considerable (Plt 005)
33 Comparison of Preoperative and Postoperative LeftVentricular Status between the Two Groups Figure 5 showsthat the left ventricular size and the left ventricular end-dia-stolic volume were reduced to some extent between the controlgroup and the experimental group at three days one monthand three months after surgery but the differences were notconsiderable compared with those before surgery (Pgt 005)
34 Comparison of Cardiac Function between the TwoGroupsof Patients before and after Surgery In Figure 6 there was noconsiderable difference in left ventricular ejection fractionand left ventricular short-axis shorting rate in the fourpostoperative reexaminations between the control groupand the experimental group (Pgt 005)
35 Comparison of the Number of Cases of PostoperativePericardial Effusion andArrhythmia between theTwoGroupsFigure 7 shows that in the control group postoperativepericardial effusion occurred in 15 cases incomplete right
Age Male Female Height Weight
Control groupExperimental group
020406080
100120140160180200
Num
eric
al
Figure 3 Comparison of general clinical data of the two groups ofpatients
Scientific Programming 5
bundle branch block in 31 cases complete right bundlebranch block in 4 cases left anterior branch block in 1 caseand IIIdeg atrioventricular block in 1 case e number ofthese complications in the test group was 6 20 1 0 and 0respectively e number of cases of pericardial effusionand arrhythmia in experimental group was greatly inferiorto that in control group with statistical significance(Plt 005)
36 Comparison of Duration of Operation Duration ofVentilator Ventilation and Duration of Intensive Care Unitbetween the Two Groups Figure 8 shows that in thecontrol group the average duration of operation was15788 minutes the average duration of ventilator ven-tilation was 4607 minutes and the average duration ofintensive care unit was 11876 minutes In the
experimental group the mean operative duration was7065 minutes the mean ventilator duration was 1258minutes and the mean ICU duration was 3779 minutese durations of operation ventilator ventilation andintensive care unit in experimental group were greatlyshorter than those in control group with statisticalsignificance (Plt 005)
37 Comparison of Hospitalization Days between the TwoGroups Figure 9 shows that the average length of hospitalstay in the control group was 75 days and the average totallength of hospital stay was 138 days e mean length ofhospital stay in the experimental group was 56 days and themean total length of hospital stay was 82 days e length ofhospital stay in experimental group was greatly inferior tothat in control group (Plt 005)
A B C D E FType of ventricular septal defect
Control groupExperimental group
02468
10121416
Num
ber o
f cas
es
(a)
Control groupExperimental group
A B C D E FType of ventricular septal defect
0
2
4
6
8
10
12
14
Num
ber o
f cas
es
(b)
Figure 4 Comparison of the number of successful operations between the two groups (a) the number of cases of ventricular septal defecttypes in the two groups (b) the number of successful operations (A) perimembrane type (B) septal type (C) simple membrane type(D) muscle type (E) subdry type (F) ridge type lowastindicates that the number of successful operations in the experimental group was greatlydifferent from the control group (Plt 005)
A B C DTime
Control groupExperimental group
32325
33335
34345
35355
36365
Left
vent
ricul
ar si
ze (m
m)
30
31
32
33
34
35
36
Left
vent
ricul
ar si
ze (m
m)
(a)
Control groupExperimental group
A B C DTime
40
42
44
46
48
50
52
41
43
45
47
49
51
53Le
ft ve
ntric
ular
end
dias
tolic
volu
me (
mL)
(b)
Figure 5 Comparison of left ventricular state before and after surgery between the two groups (a) e comparison of the left ventricularsize before and after surgery (b) the comparison of the left ventricular end-diastolic volume before and after surgery (A) before surgery(B) three days after surgery (C) one month after surgery and (D) three months after surgery
6 Scientific Programming
38 Ultrasonic Images of Esophagus before and after the Ap-plication of Artificial Fish SwarmAlgorithm A patient male22 years old had shortness of breath and dyspnea for morethan half a year During routine esophageal ultrasoundexamination due to the equipment level and other reasonsultrasound image contrast was insufficient ere were re-dundant interference noise and poor spatial resolutionwhich brought some difficulties for the observation of theheart environment e artificial fish swarm algorithm wasapplied in esophageal ultrasound to improve the decom-position speed of optical signals and the searching signalresults were more accurate and the imaging was clearer asillustrated in Figure 10
4 Discussion
An artificial fish swarm algorithm was selected in this ex-periment Its essence was simulating the foraging clusteringand tail-chasing behaviors of fish swarm by constructing anartificial fish model so as to achieve overall optimization[18] In this experiment an atom was randomly selectedfrom the database and optimized by maxima and minimanormalization multiple decomposition etc to complete theoptimization of single factor en the artificial fish swarmalgorithm model was built and then the objective of globaloptimization was approached gradually through opticalsignal decomposition and processing in the designatedrange e artificial fish swarm algorithm was applied to a
A
B
C
D
E
Com
plic
atio
n
Control groupExperimental group
10 20 30 40 50 600Number of cases
Figure 7 Comparison of the number of cases of postoperativepericardial effusion and arrhythmia between the two groups (A)pericardial effusion (B) incomplete right bundle branch block (C)complete right bundle branch block (D) left anterior branch block(E) IIIdeg atrioventricular block lowastindicated that the number of pa-tients with pericardial effusion and incomplete right bundle branchblock in the experimental group was greatly different from that inthe control group (Plt 005)
A B C D ETim
e
Left ventricular ejection fraction ()60626466687072747678
Control groupExperimental group
(a)
31
33
35
37
39
41
43
45
A B C D E
Tim
e
Left ventricular minor axis decurtation ()
Control groupExperimental group
(b)
Figure 6 Comparison of cardiac function between the two groups of patients before and after surgery (a) Comparison of the left ventricularejection fraction before and after surgery (b) comparison of the left ventricular short-axis shortening rate before and after surgery(A) before surgery (B) first review after surgery (C) second review after surgery (D) third review after surgery and (E) fourth review aftersurgery
Operation timeDuration of mechanical ventilationDuration of intensive care unit
0200400600800
100012001400160018002000
Tim
e (m
in)
Experimentalgroup
Control group
Figure 8 Comparison of the durations of operation ventilatorventilation and intensive care unit between the two groupslowastindicated that there were substantial differences in the durationsof operation ventilator ventilation and intensive care unit in theexperimental group compared with the control group (Plt 005)
Scientific Programming 7
collection of 100 patients with ventricular septal defectsrequiring surgical treatment e patients in control groupwere treated with three-dimensional transthoracic ultra-sound-guided cardiopulmonary bypass and those in ex-perimental group were treated with artificial fish-basedultrasound-guided ventricular septal defect closure eresults showed that the number of successful cases in theexperimental group was greatly higher than that in thecontrol group (Plt 005) e number of cases with peri-cardial effusion and arrhythmia after operation was inferiorto that of control group and the difference was notable(Plt 005) Moreover the durations of operation ventilatorventilation and intensive care unit were greatly shorter thanthose of the control group (Plt 005) e length of hospi-talization was greatly inferior to that of the control group(Plt 005) In 2021 Yang et al [19] pointed out that theocclusion of ventricular septal defect under the guidance ofesophageal ultrasound had a high safety and feasibilitybecause of shorter operation time and less intraoperativebleeding compared with traditional repair In this study the
reliability of this statement was verified e ventricularseptal defect occlusion under the guidance of esophagealultrasound based on artificial fish swarm was performed Ithad short operation time short hospitalization days andgood prognosis and was acceptable to patientsrsquo familymembers which was of great significance in the treatment ofventricular septal defect
5 Conclusion
In this study the artificial fish swarm algorithm was used tooptimize the traditional esophageal ultrasound and 100patients requiring surgical treatment of ventricular septaldefects were collected as the research subjects e resultsshowed that the experimental group was better than thecontrol group in terms of the number of successful oper-ations the number of cases with pericardial effusion andarrhythmia after operation the duration of operation theduration of ventilator ventilation the duration of intensivecare unit and the length of hospital stay (Plt 005) However
Postoperativehospitalization
Totalhospitalization
Control groupExperimental group
02468
10121416
Tim
e (da
y)
Figure 9 Comparison of hospitalization days between the two groups lowastindicated that the average length of postoperative hospital stayand the average total length of postoperative hospital stay in the experimental group were greatly different from those of control group(Plt 005)
(a) (b)
Figure 10 Original ultrasonic image of esophagus (a) and ultrasonic image of esophagus after the application of artificial fish swarmalgorithm (b)
8 Scientific Programming
the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9

24 Ultrasonography of the Esophagus Patients in the ex-perimental group were supine and treated with generalanesthesia through nasal endotracheal intubation and theanesthesia drugs were the same as extracorporeal circulatione esophagus ultrasonic probe was placed into theesophagus and the left ventricular long axis atrial septumventricular septum two groups of atrioventricular valvesand the section of pulmonary vein namely the fourchambers of the heart apex were observed in the central partof the esophagus In this way the size and location of theventricular septal defect the length of connective tissuebetween the defect and the atrium and ventricle and theregurgitation of the right valve were determined Rotation ofthe probe to 30ndash45deg revealed a short axial section of the aorticroot and the passage of the left ventricular pump to theartery so that the length of the defect from the aortic valvewas assessed which was used to confirm its operationalstatus and valve orifice regurgitation Probe at 60ndash75deg canshow the right ventricular pump flow to the artery and thejunction between the right ventricle and the pulmonaryartery so as to determine the location and size of the defectthe availability of the right ventricular pump flow to theartery and the presence of pulmonary valve stenosis eprobe at 120deg can show the passage of the left ventricularpump to the artery and the junction between the left ven-tricle and the pulmonary artery erefore the length of thedefect site from the aortic valve and the obstruction of theleft ventricular pump blood flow channel to the artery weredetermined to assess the aortic valve regurgitate as pre-sented in Figure 2
25 Ventricular Septal Defect Closure In the experimentalgroup a small incision of about 3-4 cm was made at the lowersternum and xiphoid process in the supine position to separatethe xiphoid process e sternum was cut along the midlinewith an electric knife and the heart sac was cut and suspendedto expose the exterior of the right ventricle e free wall of theright ventricle was suspended on both sides to make twopurses and the right ventricle purses were cut open and loadedinto the guidance wire Patients were given a routine half-
amount of heparin heparinization Under the guidance ofesophageal ultrasound the proximal end of the guide wirepassed through the ventricular septal defect and entered thechannel through which the right ventricular pump blood flewto the artery en the puncture needle was removed andinserted into the dilating vessel sheath along the guide wireeguide wire was withdrawn and the conveying device and theheparinized occluder were placed into the dilated vessel sheathone by one e blocker released the disk in turn in the leftchamber of the defect and then retracted slightly which thenreleased the right ventricle disc in the right ventricle repeatedfor several times Esophageal ultrasound was used to examinewhether there was residual shunt at the interventricular septumand whether there was valve regurgitatione plugging devicewas adjusted to the appropriate position and the conveyingdevice was released after being fixed e purse was tied in aknot heparin was neutralized and the chest was stopped layerby layer and closed
26 Artificial Fish Swarm Algorithm
261 Construction of Artificial Fish Swarm AlgorithmModelIn the decomposition process of optical signals one of themost difficult steps is the calculation of the quantity productduring each decomposition It has large computation highredundancy index and low optimization efficiency econtent of artificial fish swarm algorithm is conductingsingle or partial optimization first so as to realize overalloptimization It can optimize the maximum value andminimum value in a certain part of the operation efficientlymaking the whole operation stable so as to effectivelyovercome the problem of excessive calculation e con-struction process of artificial fish swarm algorithm model isas follows
First it is supposed that M m1 m2 mλ1113864 1113865 is theatomic and molecular database for ultrasonic optical signalprocessing where mλ is the atom with the property λ Afternormalization of it mλ 1 A signal t to be decomposed isselected from the database M m1 m2 mλ1113864 1113865 which isoptimized as follows
(a) (b)
Figure 1 Image of apical four-chamber (a) and left ventricular short-axis view (b)
Scientific Programming 3
f(t) min m minus 1113944n
p1rimi
(1)
In equation (1) mi is the p-th basic signal and ri is itscorrelation decomposition coefficient In the decompositionprocess the biggest difficulty is the need to use several innerproduct operations which requires a large amount of cal-culation and a high redundancy index erefore the arti-ficial fish swarm algorithm is selected to realize theconstruction of the model and the improvement of workefficiency
It is assumed that the length of the signal t to bedecomposed is A a data corresponding to t is selected fromthe database to meet the following requirements
t mλp1113960 111396111138681113868111386811138681113868
11138681113868111386811138681113868 sup t mλ1113858 11138591113868111386811138681113868
1113868111386811138681113868 (2)
O1t is the difference between the actual observation valueand the fitted value after the original optical signal and theoptimized data are paired To implement signal decompo-sition the equation is as follows
fprime(t) t mλ1113858 1113859mλ + Oprimet (3)
s decompositions are performed on the difference be-tween the actual observation value and the fitted valueWhen the requirements of equation (4) are met equation (5)is meaningful
Ost mλ1113858 1113859
11138681113868111386811138681113868111386811138681113868 sup O
st mλp1113960 1113961
11138681113868111386811138681113868
11138681113868111386811138681113868 (4)
Ost O
st mλp1113960 1113961mλ + O
s+1t (5)
In equation (5) the difference O1t between the actualobservation value and the fitted value after c-th decompo-sitions is expressed as follows
fPrime(t) 1113944c
s1O
st mλp1113960 1113961mλ + O
ct (6)
When c increases Oct will be in a decreasing state untilit decreases to 0 en the improvement of the existingstructure of the ultrasonic optical signal is completed whichis expressed as follows
F(t) 1113944
c
s1O
st mλp1113960 1113961mλ (7)
e properties of ultrasonic optical signals are similar toGaussian functions When the signals are decomposed mλneeds to meet the requirements of normal distributionwhich is expressed as follows
mλ 1θ
radic eminus π(ϑminus ϕθ)2 cos(ϕx + η) (8)
Based on the theoretical concept of normal distributionan artificial fish swarm algorithm model is built to find theoptimal data When λ θ ϑ ϕ η1113864 1113865 is taken as a time-fre-quency distribution parameter the set range of all valuescontained in a specific requirement is expressed as follows
θ isin (1 A]
ϑ isin [0 A]
ϕ isin [0 2π)
η isin [02π]
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(9)
Based on the abovementioned time-frequency distri-bution parameters an artificial fish swarm algorithm modelis built which is expressed as follows
Oct mλ1113858 1113859
11138681113868111386811138681113868111386811138681113868
mλ 1θ
radic eminus π(ϑminus ϕθ)2 cos(ϕx + η)
(10)
e application of artificial fish swarm algorithm modelcan solve the disadvantages of large amount of calculationand high redundancy index caused by inner product op-eration and effectively improve the efficiency of ultrasonicoptical signal processing
(a) (b)
Figure 2 Apical four-chamber view (a) and short-axis view of aortic root (b)
4 Scientific Programming
262 Decomposition of Ultrasonic Optical Signal After theartificial fish swarm algorithm model is constructed it isused to realize overall optimization and effectively completethe decomposition and processing of ultrasonic opticalsignals A single factor in an artificial fish swarm is describedby a set of vectors E e1 e2 en1113864 1113865 where ei is set as thevector to be optimized and the food content of the fishswarm currently prescribed is expressed as follows
G f ei( 1113857 (11)
G is the ideal function to be achieved by the fish swarmand the distance hi between a single factor of the fish swarmand a single factor is expressed as follows
h ei ek( 1113857
1113944
n
i1ei minus ek( 1113857
2
11139741113972
(12)
e sight range of a fish swarmrsquos single factor and ad-jacent factors is expressed as follows
Adjoin ek|0lt hi kle view1113864 1113865 l 1 2 n (13)
In equation (13) l is the total amount of individualfactors in the fish swarm and the individual factors in thefish swarm in a transition state are expressed as follows
eq 1113936
ni1 ei(l)
l l 1 2 n (14)
e position and length of the transfer of a single factorin the fish swarm are expressed as follows
ei+1 ei + step middotek(l) minus ei(l)
ek(l) minus ei(l)
l 1 2 n (15)
To ensure the stability of the calculation process a singlefactor must be handled within a transferable range and mustnot exceed the corresponding range If there is a mistake inone operation it is necessary to perform the overall oper-ation again until the optimal solution is searched
27 Statistical Analysis SPSS 240 was employed for datastatistics and analysis Meanplusmn standard deviation (xplusmn s) washow measurement data were expressed and percentage ()was how count data were expressed e t-test was usedwhen the experimental data conformed to normal distri-bution χ2 test was used for univariate analysis of relatedfactors and logistic regression analysis was used for mul-tivariate analysis Plt 005 was considered statisticallysignificant
3 Results
31 Comparison of General Clinical Data of the TwoGroups ofPatients Figure 3 below shows the comparison of generalclinical data between two groups of patients ere were nosubstantial differences in age sex ratio height and weightbetween the control group and the experimental group(Pgt 005)
32 Comparison of the Number of Successful Operations be-tween the Two Groups Figure 4 shows that after three-di-mensional transthoracic ultrasound-guided cardiopulmonarybypass was established in control group there were 12 cases ofperimembrane type of ventricular septal defect of which 10cases were successful 10 cases of septal valve type of which 8cases were successful 8 cases of simple membranous type ofwhich 6 cases were successful 15 cases of muscular type ofwhich 12 cases were successful 2 cases of substem type ofwhich 1 case was successful 3 cases of crest type of which 3cases were successful In the experimental group there were 13cases 11 cases 7 cases 13 cases 4 cases and 2 cases of ven-tricular septal defect occlusion under the guidance of esoph-ageal ultrasound based on artificial fish swarm algorithm enumber of successful cases were 12 10 7 13 4 and 2 re-spectively e number of successful cases of ventricular septaldefect closure guided by esophageal ultrasound based on ar-tificial fish swarm algorithm was greatly higher than that in thecontrol group and the difference was considerable (Plt 005)
33 Comparison of Preoperative and Postoperative LeftVentricular Status between the Two Groups Figure 5 showsthat the left ventricular size and the left ventricular end-dia-stolic volume were reduced to some extent between the controlgroup and the experimental group at three days one monthand three months after surgery but the differences were notconsiderable compared with those before surgery (Pgt 005)
34 Comparison of Cardiac Function between the TwoGroupsof Patients before and after Surgery In Figure 6 there was noconsiderable difference in left ventricular ejection fractionand left ventricular short-axis shorting rate in the fourpostoperative reexaminations between the control groupand the experimental group (Pgt 005)
35 Comparison of the Number of Cases of PostoperativePericardial Effusion andArrhythmia between theTwoGroupsFigure 7 shows that in the control group postoperativepericardial effusion occurred in 15 cases incomplete right
Age Male Female Height Weight
Control groupExperimental group
020406080
100120140160180200
Num
eric
al
Figure 3 Comparison of general clinical data of the two groups ofpatients
Scientific Programming 5
bundle branch block in 31 cases complete right bundlebranch block in 4 cases left anterior branch block in 1 caseand IIIdeg atrioventricular block in 1 case e number ofthese complications in the test group was 6 20 1 0 and 0respectively e number of cases of pericardial effusionand arrhythmia in experimental group was greatly inferiorto that in control group with statistical significance(Plt 005)
36 Comparison of Duration of Operation Duration ofVentilator Ventilation and Duration of Intensive Care Unitbetween the Two Groups Figure 8 shows that in thecontrol group the average duration of operation was15788 minutes the average duration of ventilator ven-tilation was 4607 minutes and the average duration ofintensive care unit was 11876 minutes In the
experimental group the mean operative duration was7065 minutes the mean ventilator duration was 1258minutes and the mean ICU duration was 3779 minutese durations of operation ventilator ventilation andintensive care unit in experimental group were greatlyshorter than those in control group with statisticalsignificance (Plt 005)
37 Comparison of Hospitalization Days between the TwoGroups Figure 9 shows that the average length of hospitalstay in the control group was 75 days and the average totallength of hospital stay was 138 days e mean length ofhospital stay in the experimental group was 56 days and themean total length of hospital stay was 82 days e length ofhospital stay in experimental group was greatly inferior tothat in control group (Plt 005)
A B C D E FType of ventricular septal defect
Control groupExperimental group
02468
10121416
Num
ber o
f cas
es
(a)
Control groupExperimental group
A B C D E FType of ventricular septal defect
0
2
4
6
8
10
12
14
Num
ber o
f cas
es
(b)
Figure 4 Comparison of the number of successful operations between the two groups (a) the number of cases of ventricular septal defecttypes in the two groups (b) the number of successful operations (A) perimembrane type (B) septal type (C) simple membrane type(D) muscle type (E) subdry type (F) ridge type lowastindicates that the number of successful operations in the experimental group was greatlydifferent from the control group (Plt 005)
A B C DTime
Control groupExperimental group
32325
33335
34345
35355
36365
Left
vent
ricul
ar si
ze (m
m)
30
31
32
33
34
35
36
Left
vent
ricul
ar si
ze (m
m)
(a)
Control groupExperimental group
A B C DTime
40
42
44
46
48
50
52
41
43
45
47
49
51
53Le
ft ve
ntric
ular
end
dias
tolic
volu
me (
mL)
(b)
Figure 5 Comparison of left ventricular state before and after surgery between the two groups (a) e comparison of the left ventricularsize before and after surgery (b) the comparison of the left ventricular end-diastolic volume before and after surgery (A) before surgery(B) three days after surgery (C) one month after surgery and (D) three months after surgery
6 Scientific Programming
38 Ultrasonic Images of Esophagus before and after the Ap-plication of Artificial Fish SwarmAlgorithm A patient male22 years old had shortness of breath and dyspnea for morethan half a year During routine esophageal ultrasoundexamination due to the equipment level and other reasonsultrasound image contrast was insufficient ere were re-dundant interference noise and poor spatial resolutionwhich brought some difficulties for the observation of theheart environment e artificial fish swarm algorithm wasapplied in esophageal ultrasound to improve the decom-position speed of optical signals and the searching signalresults were more accurate and the imaging was clearer asillustrated in Figure 10
4 Discussion
An artificial fish swarm algorithm was selected in this ex-periment Its essence was simulating the foraging clusteringand tail-chasing behaviors of fish swarm by constructing anartificial fish model so as to achieve overall optimization[18] In this experiment an atom was randomly selectedfrom the database and optimized by maxima and minimanormalization multiple decomposition etc to complete theoptimization of single factor en the artificial fish swarmalgorithm model was built and then the objective of globaloptimization was approached gradually through opticalsignal decomposition and processing in the designatedrange e artificial fish swarm algorithm was applied to a
A
B
C
D
E
Com
plic
atio
n
Control groupExperimental group
10 20 30 40 50 600Number of cases
Figure 7 Comparison of the number of cases of postoperativepericardial effusion and arrhythmia between the two groups (A)pericardial effusion (B) incomplete right bundle branch block (C)complete right bundle branch block (D) left anterior branch block(E) IIIdeg atrioventricular block lowastindicated that the number of pa-tients with pericardial effusion and incomplete right bundle branchblock in the experimental group was greatly different from that inthe control group (Plt 005)
A B C D ETim
e
Left ventricular ejection fraction ()60626466687072747678
Control groupExperimental group
(a)
31
33
35
37
39
41
43
45
A B C D E
Tim
e
Left ventricular minor axis decurtation ()
Control groupExperimental group
(b)
Figure 6 Comparison of cardiac function between the two groups of patients before and after surgery (a) Comparison of the left ventricularejection fraction before and after surgery (b) comparison of the left ventricular short-axis shortening rate before and after surgery(A) before surgery (B) first review after surgery (C) second review after surgery (D) third review after surgery and (E) fourth review aftersurgery
Operation timeDuration of mechanical ventilationDuration of intensive care unit
0200400600800
100012001400160018002000
Tim
e (m
in)
Experimentalgroup
Control group
Figure 8 Comparison of the durations of operation ventilatorventilation and intensive care unit between the two groupslowastindicated that there were substantial differences in the durationsof operation ventilator ventilation and intensive care unit in theexperimental group compared with the control group (Plt 005)
Scientific Programming 7
collection of 100 patients with ventricular septal defectsrequiring surgical treatment e patients in control groupwere treated with three-dimensional transthoracic ultra-sound-guided cardiopulmonary bypass and those in ex-perimental group were treated with artificial fish-basedultrasound-guided ventricular septal defect closure eresults showed that the number of successful cases in theexperimental group was greatly higher than that in thecontrol group (Plt 005) e number of cases with peri-cardial effusion and arrhythmia after operation was inferiorto that of control group and the difference was notable(Plt 005) Moreover the durations of operation ventilatorventilation and intensive care unit were greatly shorter thanthose of the control group (Plt 005) e length of hospi-talization was greatly inferior to that of the control group(Plt 005) In 2021 Yang et al [19] pointed out that theocclusion of ventricular septal defect under the guidance ofesophageal ultrasound had a high safety and feasibilitybecause of shorter operation time and less intraoperativebleeding compared with traditional repair In this study the
reliability of this statement was verified e ventricularseptal defect occlusion under the guidance of esophagealultrasound based on artificial fish swarm was performed Ithad short operation time short hospitalization days andgood prognosis and was acceptable to patientsrsquo familymembers which was of great significance in the treatment ofventricular septal defect
5 Conclusion
In this study the artificial fish swarm algorithm was used tooptimize the traditional esophageal ultrasound and 100patients requiring surgical treatment of ventricular septaldefects were collected as the research subjects e resultsshowed that the experimental group was better than thecontrol group in terms of the number of successful oper-ations the number of cases with pericardial effusion andarrhythmia after operation the duration of operation theduration of ventilator ventilation the duration of intensivecare unit and the length of hospital stay (Plt 005) However
Postoperativehospitalization
Totalhospitalization
Control groupExperimental group
02468
10121416
Tim
e (da
y)
Figure 9 Comparison of hospitalization days between the two groups lowastindicated that the average length of postoperative hospital stayand the average total length of postoperative hospital stay in the experimental group were greatly different from those of control group(Plt 005)
(a) (b)
Figure 10 Original ultrasonic image of esophagus (a) and ultrasonic image of esophagus after the application of artificial fish swarmalgorithm (b)
8 Scientific Programming
the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9

f(t) min m minus 1113944n
p1rimi
(1)
In equation (1) mi is the p-th basic signal and ri is itscorrelation decomposition coefficient In the decompositionprocess the biggest difficulty is the need to use several innerproduct operations which requires a large amount of cal-culation and a high redundancy index erefore the arti-ficial fish swarm algorithm is selected to realize theconstruction of the model and the improvement of workefficiency
It is assumed that the length of the signal t to bedecomposed is A a data corresponding to t is selected fromthe database to meet the following requirements
t mλp1113960 111396111138681113868111386811138681113868
11138681113868111386811138681113868 sup t mλ1113858 11138591113868111386811138681113868
1113868111386811138681113868 (2)
O1t is the difference between the actual observation valueand the fitted value after the original optical signal and theoptimized data are paired To implement signal decompo-sition the equation is as follows
fprime(t) t mλ1113858 1113859mλ + Oprimet (3)
s decompositions are performed on the difference be-tween the actual observation value and the fitted valueWhen the requirements of equation (4) are met equation (5)is meaningful
Ost mλ1113858 1113859
11138681113868111386811138681113868111386811138681113868 sup O
st mλp1113960 1113961
11138681113868111386811138681113868
11138681113868111386811138681113868 (4)
Ost O
st mλp1113960 1113961mλ + O
s+1t (5)
In equation (5) the difference O1t between the actualobservation value and the fitted value after c-th decompo-sitions is expressed as follows
fPrime(t) 1113944c
s1O
st mλp1113960 1113961mλ + O
ct (6)
When c increases Oct will be in a decreasing state untilit decreases to 0 en the improvement of the existingstructure of the ultrasonic optical signal is completed whichis expressed as follows
F(t) 1113944
c
s1O
st mλp1113960 1113961mλ (7)
e properties of ultrasonic optical signals are similar toGaussian functions When the signals are decomposed mλneeds to meet the requirements of normal distributionwhich is expressed as follows
mλ 1θ
radic eminus π(ϑminus ϕθ)2 cos(ϕx + η) (8)
Based on the theoretical concept of normal distributionan artificial fish swarm algorithm model is built to find theoptimal data When λ θ ϑ ϕ η1113864 1113865 is taken as a time-fre-quency distribution parameter the set range of all valuescontained in a specific requirement is expressed as follows
θ isin (1 A]
ϑ isin [0 A]
ϕ isin [0 2π)
η isin [02π]
⎧⎪⎪⎪⎪⎪⎨
⎪⎪⎪⎪⎪⎩
(9)
Based on the abovementioned time-frequency distri-bution parameters an artificial fish swarm algorithm modelis built which is expressed as follows
Oct mλ1113858 1113859
11138681113868111386811138681113868111386811138681113868
mλ 1θ
radic eminus π(ϑminus ϕθ)2 cos(ϕx + η)
(10)
e application of artificial fish swarm algorithm modelcan solve the disadvantages of large amount of calculationand high redundancy index caused by inner product op-eration and effectively improve the efficiency of ultrasonicoptical signal processing
(a) (b)
Figure 2 Apical four-chamber view (a) and short-axis view of aortic root (b)
4 Scientific Programming
262 Decomposition of Ultrasonic Optical Signal After theartificial fish swarm algorithm model is constructed it isused to realize overall optimization and effectively completethe decomposition and processing of ultrasonic opticalsignals A single factor in an artificial fish swarm is describedby a set of vectors E e1 e2 en1113864 1113865 where ei is set as thevector to be optimized and the food content of the fishswarm currently prescribed is expressed as follows
G f ei( 1113857 (11)
G is the ideal function to be achieved by the fish swarmand the distance hi between a single factor of the fish swarmand a single factor is expressed as follows
h ei ek( 1113857
1113944
n
i1ei minus ek( 1113857
2
11139741113972
(12)
e sight range of a fish swarmrsquos single factor and ad-jacent factors is expressed as follows
Adjoin ek|0lt hi kle view1113864 1113865 l 1 2 n (13)
In equation (13) l is the total amount of individualfactors in the fish swarm and the individual factors in thefish swarm in a transition state are expressed as follows
eq 1113936
ni1 ei(l)
l l 1 2 n (14)
e position and length of the transfer of a single factorin the fish swarm are expressed as follows
ei+1 ei + step middotek(l) minus ei(l)
ek(l) minus ei(l)
l 1 2 n (15)
To ensure the stability of the calculation process a singlefactor must be handled within a transferable range and mustnot exceed the corresponding range If there is a mistake inone operation it is necessary to perform the overall oper-ation again until the optimal solution is searched
27 Statistical Analysis SPSS 240 was employed for datastatistics and analysis Meanplusmn standard deviation (xplusmn s) washow measurement data were expressed and percentage ()was how count data were expressed e t-test was usedwhen the experimental data conformed to normal distri-bution χ2 test was used for univariate analysis of relatedfactors and logistic regression analysis was used for mul-tivariate analysis Plt 005 was considered statisticallysignificant
3 Results
31 Comparison of General Clinical Data of the TwoGroups ofPatients Figure 3 below shows the comparison of generalclinical data between two groups of patients ere were nosubstantial differences in age sex ratio height and weightbetween the control group and the experimental group(Pgt 005)
32 Comparison of the Number of Successful Operations be-tween the Two Groups Figure 4 shows that after three-di-mensional transthoracic ultrasound-guided cardiopulmonarybypass was established in control group there were 12 cases ofperimembrane type of ventricular septal defect of which 10cases were successful 10 cases of septal valve type of which 8cases were successful 8 cases of simple membranous type ofwhich 6 cases were successful 15 cases of muscular type ofwhich 12 cases were successful 2 cases of substem type ofwhich 1 case was successful 3 cases of crest type of which 3cases were successful In the experimental group there were 13cases 11 cases 7 cases 13 cases 4 cases and 2 cases of ven-tricular septal defect occlusion under the guidance of esoph-ageal ultrasound based on artificial fish swarm algorithm enumber of successful cases were 12 10 7 13 4 and 2 re-spectively e number of successful cases of ventricular septaldefect closure guided by esophageal ultrasound based on ar-tificial fish swarm algorithm was greatly higher than that in thecontrol group and the difference was considerable (Plt 005)
33 Comparison of Preoperative and Postoperative LeftVentricular Status between the Two Groups Figure 5 showsthat the left ventricular size and the left ventricular end-dia-stolic volume were reduced to some extent between the controlgroup and the experimental group at three days one monthand three months after surgery but the differences were notconsiderable compared with those before surgery (Pgt 005)
34 Comparison of Cardiac Function between the TwoGroupsof Patients before and after Surgery In Figure 6 there was noconsiderable difference in left ventricular ejection fractionand left ventricular short-axis shorting rate in the fourpostoperative reexaminations between the control groupand the experimental group (Pgt 005)
35 Comparison of the Number of Cases of PostoperativePericardial Effusion andArrhythmia between theTwoGroupsFigure 7 shows that in the control group postoperativepericardial effusion occurred in 15 cases incomplete right
Age Male Female Height Weight
Control groupExperimental group
020406080
100120140160180200
Num
eric
al
Figure 3 Comparison of general clinical data of the two groups ofpatients
Scientific Programming 5
bundle branch block in 31 cases complete right bundlebranch block in 4 cases left anterior branch block in 1 caseand IIIdeg atrioventricular block in 1 case e number ofthese complications in the test group was 6 20 1 0 and 0respectively e number of cases of pericardial effusionand arrhythmia in experimental group was greatly inferiorto that in control group with statistical significance(Plt 005)
36 Comparison of Duration of Operation Duration ofVentilator Ventilation and Duration of Intensive Care Unitbetween the Two Groups Figure 8 shows that in thecontrol group the average duration of operation was15788 minutes the average duration of ventilator ven-tilation was 4607 minutes and the average duration ofintensive care unit was 11876 minutes In the
experimental group the mean operative duration was7065 minutes the mean ventilator duration was 1258minutes and the mean ICU duration was 3779 minutese durations of operation ventilator ventilation andintensive care unit in experimental group were greatlyshorter than those in control group with statisticalsignificance (Plt 005)
37 Comparison of Hospitalization Days between the TwoGroups Figure 9 shows that the average length of hospitalstay in the control group was 75 days and the average totallength of hospital stay was 138 days e mean length ofhospital stay in the experimental group was 56 days and themean total length of hospital stay was 82 days e length ofhospital stay in experimental group was greatly inferior tothat in control group (Plt 005)
A B C D E FType of ventricular septal defect
Control groupExperimental group
02468
10121416
Num
ber o
f cas
es
(a)
Control groupExperimental group
A B C D E FType of ventricular septal defect
0
2
4
6
8
10
12
14
Num
ber o
f cas
es
(b)
Figure 4 Comparison of the number of successful operations between the two groups (a) the number of cases of ventricular septal defecttypes in the two groups (b) the number of successful operations (A) perimembrane type (B) septal type (C) simple membrane type(D) muscle type (E) subdry type (F) ridge type lowastindicates that the number of successful operations in the experimental group was greatlydifferent from the control group (Plt 005)
A B C DTime
Control groupExperimental group
32325
33335
34345
35355
36365
Left
vent
ricul
ar si
ze (m
m)
30
31
32
33
34
35
36
Left
vent
ricul
ar si
ze (m
m)
(a)
Control groupExperimental group
A B C DTime
40
42
44
46
48
50
52
41
43
45
47
49
51
53Le
ft ve
ntric
ular
end
dias
tolic
volu
me (
mL)
(b)
Figure 5 Comparison of left ventricular state before and after surgery between the two groups (a) e comparison of the left ventricularsize before and after surgery (b) the comparison of the left ventricular end-diastolic volume before and after surgery (A) before surgery(B) three days after surgery (C) one month after surgery and (D) three months after surgery
6 Scientific Programming
38 Ultrasonic Images of Esophagus before and after the Ap-plication of Artificial Fish SwarmAlgorithm A patient male22 years old had shortness of breath and dyspnea for morethan half a year During routine esophageal ultrasoundexamination due to the equipment level and other reasonsultrasound image contrast was insufficient ere were re-dundant interference noise and poor spatial resolutionwhich brought some difficulties for the observation of theheart environment e artificial fish swarm algorithm wasapplied in esophageal ultrasound to improve the decom-position speed of optical signals and the searching signalresults were more accurate and the imaging was clearer asillustrated in Figure 10
4 Discussion
An artificial fish swarm algorithm was selected in this ex-periment Its essence was simulating the foraging clusteringand tail-chasing behaviors of fish swarm by constructing anartificial fish model so as to achieve overall optimization[18] In this experiment an atom was randomly selectedfrom the database and optimized by maxima and minimanormalization multiple decomposition etc to complete theoptimization of single factor en the artificial fish swarmalgorithm model was built and then the objective of globaloptimization was approached gradually through opticalsignal decomposition and processing in the designatedrange e artificial fish swarm algorithm was applied to a
A
B
C
D
E
Com
plic
atio
n
Control groupExperimental group
10 20 30 40 50 600Number of cases
Figure 7 Comparison of the number of cases of postoperativepericardial effusion and arrhythmia between the two groups (A)pericardial effusion (B) incomplete right bundle branch block (C)complete right bundle branch block (D) left anterior branch block(E) IIIdeg atrioventricular block lowastindicated that the number of pa-tients with pericardial effusion and incomplete right bundle branchblock in the experimental group was greatly different from that inthe control group (Plt 005)
A B C D ETim
e
Left ventricular ejection fraction ()60626466687072747678
Control groupExperimental group
(a)
31
33
35
37
39
41
43
45
A B C D E
Tim
e
Left ventricular minor axis decurtation ()
Control groupExperimental group
(b)
Figure 6 Comparison of cardiac function between the two groups of patients before and after surgery (a) Comparison of the left ventricularejection fraction before and after surgery (b) comparison of the left ventricular short-axis shortening rate before and after surgery(A) before surgery (B) first review after surgery (C) second review after surgery (D) third review after surgery and (E) fourth review aftersurgery
Operation timeDuration of mechanical ventilationDuration of intensive care unit
0200400600800
100012001400160018002000
Tim
e (m
in)
Experimentalgroup
Control group
Figure 8 Comparison of the durations of operation ventilatorventilation and intensive care unit between the two groupslowastindicated that there were substantial differences in the durationsof operation ventilator ventilation and intensive care unit in theexperimental group compared with the control group (Plt 005)
Scientific Programming 7
collection of 100 patients with ventricular septal defectsrequiring surgical treatment e patients in control groupwere treated with three-dimensional transthoracic ultra-sound-guided cardiopulmonary bypass and those in ex-perimental group were treated with artificial fish-basedultrasound-guided ventricular septal defect closure eresults showed that the number of successful cases in theexperimental group was greatly higher than that in thecontrol group (Plt 005) e number of cases with peri-cardial effusion and arrhythmia after operation was inferiorto that of control group and the difference was notable(Plt 005) Moreover the durations of operation ventilatorventilation and intensive care unit were greatly shorter thanthose of the control group (Plt 005) e length of hospi-talization was greatly inferior to that of the control group(Plt 005) In 2021 Yang et al [19] pointed out that theocclusion of ventricular septal defect under the guidance ofesophageal ultrasound had a high safety and feasibilitybecause of shorter operation time and less intraoperativebleeding compared with traditional repair In this study the
reliability of this statement was verified e ventricularseptal defect occlusion under the guidance of esophagealultrasound based on artificial fish swarm was performed Ithad short operation time short hospitalization days andgood prognosis and was acceptable to patientsrsquo familymembers which was of great significance in the treatment ofventricular septal defect
5 Conclusion
In this study the artificial fish swarm algorithm was used tooptimize the traditional esophageal ultrasound and 100patients requiring surgical treatment of ventricular septaldefects were collected as the research subjects e resultsshowed that the experimental group was better than thecontrol group in terms of the number of successful oper-ations the number of cases with pericardial effusion andarrhythmia after operation the duration of operation theduration of ventilator ventilation the duration of intensivecare unit and the length of hospital stay (Plt 005) However
Postoperativehospitalization
Totalhospitalization
Control groupExperimental group
02468
10121416
Tim
e (da
y)
Figure 9 Comparison of hospitalization days between the two groups lowastindicated that the average length of postoperative hospital stayand the average total length of postoperative hospital stay in the experimental group were greatly different from those of control group(Plt 005)
(a) (b)
Figure 10 Original ultrasonic image of esophagus (a) and ultrasonic image of esophagus after the application of artificial fish swarmalgorithm (b)
8 Scientific Programming
the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9

262 Decomposition of Ultrasonic Optical Signal After theartificial fish swarm algorithm model is constructed it isused to realize overall optimization and effectively completethe decomposition and processing of ultrasonic opticalsignals A single factor in an artificial fish swarm is describedby a set of vectors E e1 e2 en1113864 1113865 where ei is set as thevector to be optimized and the food content of the fishswarm currently prescribed is expressed as follows
G f ei( 1113857 (11)
G is the ideal function to be achieved by the fish swarmand the distance hi between a single factor of the fish swarmand a single factor is expressed as follows
h ei ek( 1113857
1113944
n
i1ei minus ek( 1113857
2
11139741113972
(12)
e sight range of a fish swarmrsquos single factor and ad-jacent factors is expressed as follows
Adjoin ek|0lt hi kle view1113864 1113865 l 1 2 n (13)
In equation (13) l is the total amount of individualfactors in the fish swarm and the individual factors in thefish swarm in a transition state are expressed as follows
eq 1113936
ni1 ei(l)
l l 1 2 n (14)
e position and length of the transfer of a single factorin the fish swarm are expressed as follows
ei+1 ei + step middotek(l) minus ei(l)
ek(l) minus ei(l)
l 1 2 n (15)
To ensure the stability of the calculation process a singlefactor must be handled within a transferable range and mustnot exceed the corresponding range If there is a mistake inone operation it is necessary to perform the overall oper-ation again until the optimal solution is searched
27 Statistical Analysis SPSS 240 was employed for datastatistics and analysis Meanplusmn standard deviation (xplusmn s) washow measurement data were expressed and percentage ()was how count data were expressed e t-test was usedwhen the experimental data conformed to normal distri-bution χ2 test was used for univariate analysis of relatedfactors and logistic regression analysis was used for mul-tivariate analysis Plt 005 was considered statisticallysignificant
3 Results
31 Comparison of General Clinical Data of the TwoGroups ofPatients Figure 3 below shows the comparison of generalclinical data between two groups of patients ere were nosubstantial differences in age sex ratio height and weightbetween the control group and the experimental group(Pgt 005)
32 Comparison of the Number of Successful Operations be-tween the Two Groups Figure 4 shows that after three-di-mensional transthoracic ultrasound-guided cardiopulmonarybypass was established in control group there were 12 cases ofperimembrane type of ventricular septal defect of which 10cases were successful 10 cases of septal valve type of which 8cases were successful 8 cases of simple membranous type ofwhich 6 cases were successful 15 cases of muscular type ofwhich 12 cases were successful 2 cases of substem type ofwhich 1 case was successful 3 cases of crest type of which 3cases were successful In the experimental group there were 13cases 11 cases 7 cases 13 cases 4 cases and 2 cases of ven-tricular septal defect occlusion under the guidance of esoph-ageal ultrasound based on artificial fish swarm algorithm enumber of successful cases were 12 10 7 13 4 and 2 re-spectively e number of successful cases of ventricular septaldefect closure guided by esophageal ultrasound based on ar-tificial fish swarm algorithm was greatly higher than that in thecontrol group and the difference was considerable (Plt 005)
33 Comparison of Preoperative and Postoperative LeftVentricular Status between the Two Groups Figure 5 showsthat the left ventricular size and the left ventricular end-dia-stolic volume were reduced to some extent between the controlgroup and the experimental group at three days one monthand three months after surgery but the differences were notconsiderable compared with those before surgery (Pgt 005)
34 Comparison of Cardiac Function between the TwoGroupsof Patients before and after Surgery In Figure 6 there was noconsiderable difference in left ventricular ejection fractionand left ventricular short-axis shorting rate in the fourpostoperative reexaminations between the control groupand the experimental group (Pgt 005)
35 Comparison of the Number of Cases of PostoperativePericardial Effusion andArrhythmia between theTwoGroupsFigure 7 shows that in the control group postoperativepericardial effusion occurred in 15 cases incomplete right
Age Male Female Height Weight
Control groupExperimental group
020406080
100120140160180200
Num
eric
al
Figure 3 Comparison of general clinical data of the two groups ofpatients
Scientific Programming 5
bundle branch block in 31 cases complete right bundlebranch block in 4 cases left anterior branch block in 1 caseand IIIdeg atrioventricular block in 1 case e number ofthese complications in the test group was 6 20 1 0 and 0respectively e number of cases of pericardial effusionand arrhythmia in experimental group was greatly inferiorto that in control group with statistical significance(Plt 005)
36 Comparison of Duration of Operation Duration ofVentilator Ventilation and Duration of Intensive Care Unitbetween the Two Groups Figure 8 shows that in thecontrol group the average duration of operation was15788 minutes the average duration of ventilator ven-tilation was 4607 minutes and the average duration ofintensive care unit was 11876 minutes In the
experimental group the mean operative duration was7065 minutes the mean ventilator duration was 1258minutes and the mean ICU duration was 3779 minutese durations of operation ventilator ventilation andintensive care unit in experimental group were greatlyshorter than those in control group with statisticalsignificance (Plt 005)
37 Comparison of Hospitalization Days between the TwoGroups Figure 9 shows that the average length of hospitalstay in the control group was 75 days and the average totallength of hospital stay was 138 days e mean length ofhospital stay in the experimental group was 56 days and themean total length of hospital stay was 82 days e length ofhospital stay in experimental group was greatly inferior tothat in control group (Plt 005)
A B C D E FType of ventricular septal defect
Control groupExperimental group
02468
10121416
Num
ber o
f cas
es
(a)
Control groupExperimental group
A B C D E FType of ventricular septal defect
0
2
4
6
8
10
12
14
Num
ber o
f cas
es
(b)
Figure 4 Comparison of the number of successful operations between the two groups (a) the number of cases of ventricular septal defecttypes in the two groups (b) the number of successful operations (A) perimembrane type (B) septal type (C) simple membrane type(D) muscle type (E) subdry type (F) ridge type lowastindicates that the number of successful operations in the experimental group was greatlydifferent from the control group (Plt 005)
A B C DTime
Control groupExperimental group
32325
33335
34345
35355
36365
Left
vent
ricul
ar si
ze (m
m)
30
31
32
33
34
35
36
Left
vent
ricul
ar si
ze (m
m)
(a)
Control groupExperimental group
A B C DTime
40
42
44
46
48
50
52
41
43
45
47
49
51
53Le
ft ve
ntric
ular
end
dias
tolic
volu
me (
mL)
(b)
Figure 5 Comparison of left ventricular state before and after surgery between the two groups (a) e comparison of the left ventricularsize before and after surgery (b) the comparison of the left ventricular end-diastolic volume before and after surgery (A) before surgery(B) three days after surgery (C) one month after surgery and (D) three months after surgery
6 Scientific Programming
38 Ultrasonic Images of Esophagus before and after the Ap-plication of Artificial Fish SwarmAlgorithm A patient male22 years old had shortness of breath and dyspnea for morethan half a year During routine esophageal ultrasoundexamination due to the equipment level and other reasonsultrasound image contrast was insufficient ere were re-dundant interference noise and poor spatial resolutionwhich brought some difficulties for the observation of theheart environment e artificial fish swarm algorithm wasapplied in esophageal ultrasound to improve the decom-position speed of optical signals and the searching signalresults were more accurate and the imaging was clearer asillustrated in Figure 10
4 Discussion
An artificial fish swarm algorithm was selected in this ex-periment Its essence was simulating the foraging clusteringand tail-chasing behaviors of fish swarm by constructing anartificial fish model so as to achieve overall optimization[18] In this experiment an atom was randomly selectedfrom the database and optimized by maxima and minimanormalization multiple decomposition etc to complete theoptimization of single factor en the artificial fish swarmalgorithm model was built and then the objective of globaloptimization was approached gradually through opticalsignal decomposition and processing in the designatedrange e artificial fish swarm algorithm was applied to a
A
B
C
D
E
Com
plic
atio
n
Control groupExperimental group
10 20 30 40 50 600Number of cases
Figure 7 Comparison of the number of cases of postoperativepericardial effusion and arrhythmia between the two groups (A)pericardial effusion (B) incomplete right bundle branch block (C)complete right bundle branch block (D) left anterior branch block(E) IIIdeg atrioventricular block lowastindicated that the number of pa-tients with pericardial effusion and incomplete right bundle branchblock in the experimental group was greatly different from that inthe control group (Plt 005)
A B C D ETim
e
Left ventricular ejection fraction ()60626466687072747678
Control groupExperimental group
(a)
31
33
35
37
39
41
43
45
A B C D E
Tim
e
Left ventricular minor axis decurtation ()
Control groupExperimental group
(b)
Figure 6 Comparison of cardiac function between the two groups of patients before and after surgery (a) Comparison of the left ventricularejection fraction before and after surgery (b) comparison of the left ventricular short-axis shortening rate before and after surgery(A) before surgery (B) first review after surgery (C) second review after surgery (D) third review after surgery and (E) fourth review aftersurgery
Operation timeDuration of mechanical ventilationDuration of intensive care unit
0200400600800
100012001400160018002000
Tim
e (m
in)
Experimentalgroup
Control group
Figure 8 Comparison of the durations of operation ventilatorventilation and intensive care unit between the two groupslowastindicated that there were substantial differences in the durationsof operation ventilator ventilation and intensive care unit in theexperimental group compared with the control group (Plt 005)
Scientific Programming 7
collection of 100 patients with ventricular septal defectsrequiring surgical treatment e patients in control groupwere treated with three-dimensional transthoracic ultra-sound-guided cardiopulmonary bypass and those in ex-perimental group were treated with artificial fish-basedultrasound-guided ventricular septal defect closure eresults showed that the number of successful cases in theexperimental group was greatly higher than that in thecontrol group (Plt 005) e number of cases with peri-cardial effusion and arrhythmia after operation was inferiorto that of control group and the difference was notable(Plt 005) Moreover the durations of operation ventilatorventilation and intensive care unit were greatly shorter thanthose of the control group (Plt 005) e length of hospi-talization was greatly inferior to that of the control group(Plt 005) In 2021 Yang et al [19] pointed out that theocclusion of ventricular septal defect under the guidance ofesophageal ultrasound had a high safety and feasibilitybecause of shorter operation time and less intraoperativebleeding compared with traditional repair In this study the
reliability of this statement was verified e ventricularseptal defect occlusion under the guidance of esophagealultrasound based on artificial fish swarm was performed Ithad short operation time short hospitalization days andgood prognosis and was acceptable to patientsrsquo familymembers which was of great significance in the treatment ofventricular septal defect
5 Conclusion
In this study the artificial fish swarm algorithm was used tooptimize the traditional esophageal ultrasound and 100patients requiring surgical treatment of ventricular septaldefects were collected as the research subjects e resultsshowed that the experimental group was better than thecontrol group in terms of the number of successful oper-ations the number of cases with pericardial effusion andarrhythmia after operation the duration of operation theduration of ventilator ventilation the duration of intensivecare unit and the length of hospital stay (Plt 005) However
Postoperativehospitalization
Totalhospitalization
Control groupExperimental group
02468
10121416
Tim
e (da
y)
Figure 9 Comparison of hospitalization days between the two groups lowastindicated that the average length of postoperative hospital stayand the average total length of postoperative hospital stay in the experimental group were greatly different from those of control group(Plt 005)
(a) (b)
Figure 10 Original ultrasonic image of esophagus (a) and ultrasonic image of esophagus after the application of artificial fish swarmalgorithm (b)
8 Scientific Programming
the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9

bundle branch block in 31 cases complete right bundlebranch block in 4 cases left anterior branch block in 1 caseand IIIdeg atrioventricular block in 1 case e number ofthese complications in the test group was 6 20 1 0 and 0respectively e number of cases of pericardial effusionand arrhythmia in experimental group was greatly inferiorto that in control group with statistical significance(Plt 005)
36 Comparison of Duration of Operation Duration ofVentilator Ventilation and Duration of Intensive Care Unitbetween the Two Groups Figure 8 shows that in thecontrol group the average duration of operation was15788 minutes the average duration of ventilator ven-tilation was 4607 minutes and the average duration ofintensive care unit was 11876 minutes In the
experimental group the mean operative duration was7065 minutes the mean ventilator duration was 1258minutes and the mean ICU duration was 3779 minutese durations of operation ventilator ventilation andintensive care unit in experimental group were greatlyshorter than those in control group with statisticalsignificance (Plt 005)
37 Comparison of Hospitalization Days between the TwoGroups Figure 9 shows that the average length of hospitalstay in the control group was 75 days and the average totallength of hospital stay was 138 days e mean length ofhospital stay in the experimental group was 56 days and themean total length of hospital stay was 82 days e length ofhospital stay in experimental group was greatly inferior tothat in control group (Plt 005)
A B C D E FType of ventricular septal defect
Control groupExperimental group
02468
10121416
Num
ber o
f cas
es
(a)
Control groupExperimental group
A B C D E FType of ventricular septal defect
0
2
4
6
8
10
12
14
Num
ber o
f cas
es
(b)
Figure 4 Comparison of the number of successful operations between the two groups (a) the number of cases of ventricular septal defecttypes in the two groups (b) the number of successful operations (A) perimembrane type (B) septal type (C) simple membrane type(D) muscle type (E) subdry type (F) ridge type lowastindicates that the number of successful operations in the experimental group was greatlydifferent from the control group (Plt 005)
A B C DTime
Control groupExperimental group
32325
33335
34345
35355
36365
Left
vent
ricul
ar si
ze (m
m)
30
31
32
33
34
35
36
Left
vent
ricul
ar si
ze (m
m)
(a)
Control groupExperimental group
A B C DTime
40
42
44
46
48
50
52
41
43
45
47
49
51
53Le
ft ve
ntric
ular
end
dias
tolic
volu
me (
mL)
(b)
Figure 5 Comparison of left ventricular state before and after surgery between the two groups (a) e comparison of the left ventricularsize before and after surgery (b) the comparison of the left ventricular end-diastolic volume before and after surgery (A) before surgery(B) three days after surgery (C) one month after surgery and (D) three months after surgery
6 Scientific Programming
38 Ultrasonic Images of Esophagus before and after the Ap-plication of Artificial Fish SwarmAlgorithm A patient male22 years old had shortness of breath and dyspnea for morethan half a year During routine esophageal ultrasoundexamination due to the equipment level and other reasonsultrasound image contrast was insufficient ere were re-dundant interference noise and poor spatial resolutionwhich brought some difficulties for the observation of theheart environment e artificial fish swarm algorithm wasapplied in esophageal ultrasound to improve the decom-position speed of optical signals and the searching signalresults were more accurate and the imaging was clearer asillustrated in Figure 10
4 Discussion
An artificial fish swarm algorithm was selected in this ex-periment Its essence was simulating the foraging clusteringand tail-chasing behaviors of fish swarm by constructing anartificial fish model so as to achieve overall optimization[18] In this experiment an atom was randomly selectedfrom the database and optimized by maxima and minimanormalization multiple decomposition etc to complete theoptimization of single factor en the artificial fish swarmalgorithm model was built and then the objective of globaloptimization was approached gradually through opticalsignal decomposition and processing in the designatedrange e artificial fish swarm algorithm was applied to a
A
B
C
D
E
Com
plic
atio
n
Control groupExperimental group
10 20 30 40 50 600Number of cases
Figure 7 Comparison of the number of cases of postoperativepericardial effusion and arrhythmia between the two groups (A)pericardial effusion (B) incomplete right bundle branch block (C)complete right bundle branch block (D) left anterior branch block(E) IIIdeg atrioventricular block lowastindicated that the number of pa-tients with pericardial effusion and incomplete right bundle branchblock in the experimental group was greatly different from that inthe control group (Plt 005)
A B C D ETim
e
Left ventricular ejection fraction ()60626466687072747678
Control groupExperimental group
(a)
31
33
35
37
39
41
43
45
A B C D E
Tim
e
Left ventricular minor axis decurtation ()
Control groupExperimental group
(b)
Figure 6 Comparison of cardiac function between the two groups of patients before and after surgery (a) Comparison of the left ventricularejection fraction before and after surgery (b) comparison of the left ventricular short-axis shortening rate before and after surgery(A) before surgery (B) first review after surgery (C) second review after surgery (D) third review after surgery and (E) fourth review aftersurgery
Operation timeDuration of mechanical ventilationDuration of intensive care unit
0200400600800
100012001400160018002000
Tim
e (m
in)
Experimentalgroup
Control group
Figure 8 Comparison of the durations of operation ventilatorventilation and intensive care unit between the two groupslowastindicated that there were substantial differences in the durationsof operation ventilator ventilation and intensive care unit in theexperimental group compared with the control group (Plt 005)
Scientific Programming 7
collection of 100 patients with ventricular septal defectsrequiring surgical treatment e patients in control groupwere treated with three-dimensional transthoracic ultra-sound-guided cardiopulmonary bypass and those in ex-perimental group were treated with artificial fish-basedultrasound-guided ventricular septal defect closure eresults showed that the number of successful cases in theexperimental group was greatly higher than that in thecontrol group (Plt 005) e number of cases with peri-cardial effusion and arrhythmia after operation was inferiorto that of control group and the difference was notable(Plt 005) Moreover the durations of operation ventilatorventilation and intensive care unit were greatly shorter thanthose of the control group (Plt 005) e length of hospi-talization was greatly inferior to that of the control group(Plt 005) In 2021 Yang et al [19] pointed out that theocclusion of ventricular septal defect under the guidance ofesophageal ultrasound had a high safety and feasibilitybecause of shorter operation time and less intraoperativebleeding compared with traditional repair In this study the
reliability of this statement was verified e ventricularseptal defect occlusion under the guidance of esophagealultrasound based on artificial fish swarm was performed Ithad short operation time short hospitalization days andgood prognosis and was acceptable to patientsrsquo familymembers which was of great significance in the treatment ofventricular septal defect
5 Conclusion
In this study the artificial fish swarm algorithm was used tooptimize the traditional esophageal ultrasound and 100patients requiring surgical treatment of ventricular septaldefects were collected as the research subjects e resultsshowed that the experimental group was better than thecontrol group in terms of the number of successful oper-ations the number of cases with pericardial effusion andarrhythmia after operation the duration of operation theduration of ventilator ventilation the duration of intensivecare unit and the length of hospital stay (Plt 005) However
Postoperativehospitalization
Totalhospitalization
Control groupExperimental group
02468
10121416
Tim
e (da
y)
Figure 9 Comparison of hospitalization days between the two groups lowastindicated that the average length of postoperative hospital stayand the average total length of postoperative hospital stay in the experimental group were greatly different from those of control group(Plt 005)
(a) (b)
Figure 10 Original ultrasonic image of esophagus (a) and ultrasonic image of esophagus after the application of artificial fish swarmalgorithm (b)
8 Scientific Programming
the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9

38 Ultrasonic Images of Esophagus before and after the Ap-plication of Artificial Fish SwarmAlgorithm A patient male22 years old had shortness of breath and dyspnea for morethan half a year During routine esophageal ultrasoundexamination due to the equipment level and other reasonsultrasound image contrast was insufficient ere were re-dundant interference noise and poor spatial resolutionwhich brought some difficulties for the observation of theheart environment e artificial fish swarm algorithm wasapplied in esophageal ultrasound to improve the decom-position speed of optical signals and the searching signalresults were more accurate and the imaging was clearer asillustrated in Figure 10
4 Discussion
An artificial fish swarm algorithm was selected in this ex-periment Its essence was simulating the foraging clusteringand tail-chasing behaviors of fish swarm by constructing anartificial fish model so as to achieve overall optimization[18] In this experiment an atom was randomly selectedfrom the database and optimized by maxima and minimanormalization multiple decomposition etc to complete theoptimization of single factor en the artificial fish swarmalgorithm model was built and then the objective of globaloptimization was approached gradually through opticalsignal decomposition and processing in the designatedrange e artificial fish swarm algorithm was applied to a
A
B
C
D
E
Com
plic
atio
n
Control groupExperimental group
10 20 30 40 50 600Number of cases
Figure 7 Comparison of the number of cases of postoperativepericardial effusion and arrhythmia between the two groups (A)pericardial effusion (B) incomplete right bundle branch block (C)complete right bundle branch block (D) left anterior branch block(E) IIIdeg atrioventricular block lowastindicated that the number of pa-tients with pericardial effusion and incomplete right bundle branchblock in the experimental group was greatly different from that inthe control group (Plt 005)
A B C D ETim
e
Left ventricular ejection fraction ()60626466687072747678
Control groupExperimental group
(a)
31
33
35
37
39
41
43
45
A B C D E
Tim
e
Left ventricular minor axis decurtation ()
Control groupExperimental group
(b)
Figure 6 Comparison of cardiac function between the two groups of patients before and after surgery (a) Comparison of the left ventricularejection fraction before and after surgery (b) comparison of the left ventricular short-axis shortening rate before and after surgery(A) before surgery (B) first review after surgery (C) second review after surgery (D) third review after surgery and (E) fourth review aftersurgery
Operation timeDuration of mechanical ventilationDuration of intensive care unit
0200400600800
100012001400160018002000
Tim
e (m
in)
Experimentalgroup
Control group
Figure 8 Comparison of the durations of operation ventilatorventilation and intensive care unit between the two groupslowastindicated that there were substantial differences in the durationsof operation ventilator ventilation and intensive care unit in theexperimental group compared with the control group (Plt 005)
Scientific Programming 7
collection of 100 patients with ventricular septal defectsrequiring surgical treatment e patients in control groupwere treated with three-dimensional transthoracic ultra-sound-guided cardiopulmonary bypass and those in ex-perimental group were treated with artificial fish-basedultrasound-guided ventricular septal defect closure eresults showed that the number of successful cases in theexperimental group was greatly higher than that in thecontrol group (Plt 005) e number of cases with peri-cardial effusion and arrhythmia after operation was inferiorto that of control group and the difference was notable(Plt 005) Moreover the durations of operation ventilatorventilation and intensive care unit were greatly shorter thanthose of the control group (Plt 005) e length of hospi-talization was greatly inferior to that of the control group(Plt 005) In 2021 Yang et al [19] pointed out that theocclusion of ventricular septal defect under the guidance ofesophageal ultrasound had a high safety and feasibilitybecause of shorter operation time and less intraoperativebleeding compared with traditional repair In this study the
reliability of this statement was verified e ventricularseptal defect occlusion under the guidance of esophagealultrasound based on artificial fish swarm was performed Ithad short operation time short hospitalization days andgood prognosis and was acceptable to patientsrsquo familymembers which was of great significance in the treatment ofventricular septal defect
5 Conclusion
In this study the artificial fish swarm algorithm was used tooptimize the traditional esophageal ultrasound and 100patients requiring surgical treatment of ventricular septaldefects were collected as the research subjects e resultsshowed that the experimental group was better than thecontrol group in terms of the number of successful oper-ations the number of cases with pericardial effusion andarrhythmia after operation the duration of operation theduration of ventilator ventilation the duration of intensivecare unit and the length of hospital stay (Plt 005) However
Postoperativehospitalization
Totalhospitalization
Control groupExperimental group
02468
10121416
Tim
e (da
y)
Figure 9 Comparison of hospitalization days between the two groups lowastindicated that the average length of postoperative hospital stayand the average total length of postoperative hospital stay in the experimental group were greatly different from those of control group(Plt 005)
(a) (b)
Figure 10 Original ultrasonic image of esophagus (a) and ultrasonic image of esophagus after the application of artificial fish swarmalgorithm (b)
8 Scientific Programming
the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9

collection of 100 patients with ventricular septal defectsrequiring surgical treatment e patients in control groupwere treated with three-dimensional transthoracic ultra-sound-guided cardiopulmonary bypass and those in ex-perimental group were treated with artificial fish-basedultrasound-guided ventricular septal defect closure eresults showed that the number of successful cases in theexperimental group was greatly higher than that in thecontrol group (Plt 005) e number of cases with peri-cardial effusion and arrhythmia after operation was inferiorto that of control group and the difference was notable(Plt 005) Moreover the durations of operation ventilatorventilation and intensive care unit were greatly shorter thanthose of the control group (Plt 005) e length of hospi-talization was greatly inferior to that of the control group(Plt 005) In 2021 Yang et al [19] pointed out that theocclusion of ventricular septal defect under the guidance ofesophageal ultrasound had a high safety and feasibilitybecause of shorter operation time and less intraoperativebleeding compared with traditional repair In this study the
reliability of this statement was verified e ventricularseptal defect occlusion under the guidance of esophagealultrasound based on artificial fish swarm was performed Ithad short operation time short hospitalization days andgood prognosis and was acceptable to patientsrsquo familymembers which was of great significance in the treatment ofventricular septal defect
5 Conclusion
In this study the artificial fish swarm algorithm was used tooptimize the traditional esophageal ultrasound and 100patients requiring surgical treatment of ventricular septaldefects were collected as the research subjects e resultsshowed that the experimental group was better than thecontrol group in terms of the number of successful oper-ations the number of cases with pericardial effusion andarrhythmia after operation the duration of operation theduration of ventilator ventilation the duration of intensivecare unit and the length of hospital stay (Plt 005) However
Postoperativehospitalization
Totalhospitalization
Control groupExperimental group
02468
10121416
Tim
e (da
y)
Figure 9 Comparison of hospitalization days between the two groups lowastindicated that the average length of postoperative hospital stayand the average total length of postoperative hospital stay in the experimental group were greatly different from those of control group(Plt 005)
(a) (b)
Figure 10 Original ultrasonic image of esophagus (a) and ultrasonic image of esophagus after the application of artificial fish swarmalgorithm (b)
8 Scientific Programming
the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9

the sample size collected in this experiment was small thelength of hospitalization of patients was short and theobservation had certain limitations and one-sidedness It isexpected that further research in this direction will provide amore reliable basis for the clinical treatment of ventricularseptal defect
Data Availability
e data used to support the findings of this study areavailable from the corresponding author upon request
Conflicts of Interest
e authors declare no conflicts of interest
References
[1] B H Morray ldquoVentricular septal defect closure devicestechniques and outcomesrdquo Interventional Cardiology Clinicsvol 8 no 1 pp 1ndash10 2019
[2] L Lopez L Houyel S D Colan et al ldquoClassification ofventricular septal defects for the eleventh iteration of theinternational classification of diseases-striving for consensusa report from the international society for nomenclature ofpaediatric and congenital heart diseaserdquo e Annals of o-racic Surgery vol 106 no 5 pp 1578ndash1589 2018
[3] S Omar G L Morgan H B Panchal et al ldquoManagement ofpost-myocardial infarction ventricular septal defects a criticalassessmentrdquo Journal of Interventional Cardiology vol 31no 6 pp 939ndash948 2018
[4] Y-S Cho S E Park S-K Hong N-Y Jeong and E-Y Choildquoe natural history of fetal diagnosed isolated ventricularseptal defectrdquo Prenatal Diagnosis vol 37 no 9 pp 889ndash8932017
[5] L P Badano P Aruta K Nguyen et al ldquoPrincipali appli-cazioni dellrsquoecocardiografia tridimensionale nellrsquoattuale pra-tica clinica [Current clinical applications of three-dimensionalechocardiography]rdquo Glomale Italiano di Caradiologia vol 20no 12 pp 722ndash735 2019
[6] X Bai M Hu T Gang and Q Rong ldquoA submerged opticalfiber ultrasonic sensor using matched fiber bragg gratingsrdquoSensors vol 18 no 6 Article ID 1942 2018
[7] W Y Choi S W Kwon Y H Kim K C Kang andK K Park ldquoSingle-shot near-field volumetric imaging systemfor optical ultrasound and photoacoustics using capacitivemicromachined ultrasonic transducer without transmissionmoderdquo IEEE Transactions on Ultrasonics Ferroelectrics andFrequency Control vol 67 no 6 pp 1151ndash1158 2020
[8] A B Freitas-Ferraz M Bernier R Vaillancourt et al ldquoSafetyof transesophageal echocardiography to guide structuralcardiac interventionsrdquo Journal of the American College ofCardiology vol 75 no 25 pp 3164ndash3173 2020
[9] T C Wray K Schmid D Braude et al ldquoSafety of trans-esophageal echocardiography performed by intensivists andemergency physicians in critically ill patients with coagul-opathy and thrombocytopenia a single-center experiencerdquoJournal of Intensive Care Medicine vol 36 no 1 pp 123ndash1302021
[10] X Lei X Yang and FWu ldquoArtificial fish swarm optimizationbased method to identify essential proteinsrdquo IEEEACMTransactions on Computational Biology and Bioinformaticsvol 17 no 2 p 1 2019
[11] S Xie Z Yu and Z Lv ldquoMulti-disease prediction based ondeep learning a surveyrdquo Computer Modeling in Engineeringand Sciences vol 128 no 2 pp 489ndash522 2021
[12] M Mostefa-Kara L Houyel and D Bonnet ldquoAnatomy of theventricular septal defect in congenital heart defects a randomassociationrdquo Orphanet Journal of Rare Diseases vol 13 no 1p 118 2018
[13] U Radhakrishna S Albayrak R Zafra et al ldquoPlacentalepigenetics for evaluation of fetal congenital heart defectsventricular Septal Defect (VSD)rdquo PLoS One vol 14 no 3Article ID e0200229 2019
[14] T Buck L Bosche and B Plicht ldquoEchtzeit-3-D-Echo-kardiographie zur Schweregradbeurteilung von Herzklap-penvitienrdquo Herz vol 42 no 3 pp 241ndash254 2017
[15] S Montis D Sirigu A Marini et al ldquoLrsquoipnosi nellrsquoeco-cardiografia transesofagea Lrsquoesperienza di un Centro diCardiologia Pediatrica e delle Cardiopatie Congenite [Hyp-nosis in transesophageal echocardiography e experience ina Pediatric Cardiology and Congenital Heart Disease Unit]rdquoGlomale Italiano di Caradiologia vol 20 no 11 pp 651ndash6572019
[16] T Gluck M Kravchik S Chocron Y Elovici and A ShabtaildquoSpoofing attack on ultrasonic distance sensors using acontinuous signalrdquo Sensors vol 20 no 21 Article ID 61572020
[17] Z Kou F Yang JWu and T Li ldquoApplication of ICEEMDANenergy entropy and AFSA-SVM for fault diagnosis of hoistsheave bearingrdquo Entropy vol 22 no 12 Article ID 1347 2020
[18] S Schubert M Kelm N R Koneti and F Berger ldquoFirstEuropean experience of percutaneous closure of ventricularseptal defects using a new CE-marked VSD occluderrdquoEuroIntervention vol 15 no 3 pp e242ndashe243 2019
[19] H Yang J Mu Y Zhao Z Chen H Song and J Liu ldquoTrans-esophageal echocardiography guided closure of ventricularseptal defect with 2 occluders from different incisions si-multaneouslyrdquo Medicine (Baltimore) vol 100 no 19 ArticleID e23854 2021
Scientific Programming 9