Embed Size (px)
Citation preview

Optimal Anticoagulation: New Drugs, Indications, and Reversal
Roy E. Smith, M.D., M.S.Department of Medicine
Division of Hematology and Medical OncologyUniversity of Pittsburgh Medical Center
10/21/19 1

Objectives:
• Understand the mechanisms of action and differences of the new oral
anticoagulants
• Know indications for each new oral anticoagulant
• Increase knowledge of use of each new oral anticoagulant in special
circumstances.
• Understand useful reversal strategies for each new oral anticoagulant
10/21/19 2

10/21/19 3

10/21/19 4
Tyranny of Choice – Current Challenges
• DOACs differ in a number ways
• Must consider drug and patient characteristics
• No randomized comparisons of DOACs
• Safety and efficacy similar to warfarin and with reduced risk of spontaneous ICH

10/21/19 5
Differences in DOACS

10/21/19 6
Dabigatran Rivaroxaban Apixaban Edoxaban BetrixabanHip replacement
Knee replacement
Stroke/SE in NVAF
Acute VTE
Extended VTE
CAD/PAD
VTE ppx
Yes yes yes
yes yes
yes yes
yes yes yes yes
yes yes yes
yes
yes

10/21/19 7
Makan et al. PLOS one 2018
Efficacy and Safety of DOACs vs Warfarin

10/21/19 8
Makan et al. PLOS one 2018
Efficacy and Safety of DOACs vs Warfarin in NVAF

10/21/19 9
Makan et al. PLOS one 2018
Efficacy and Safety of DOACs vs Warfarin in VTE

10/21/19 10
VTE ppx for THR or TKR vs Enoxaparin
Rivaroxaban Superior with no difference in bleeding
Edoxaban Not approved for these indication
RE-NOVATE I and II THRDabigatran
Lassen et al. NEJM 2010Eriksson et al. NEJM 2008Kakkar et al. Lancet 2008Eriksson et al. Lancet 2007Eriksson et al. J thromb Haemost 2007
Apixaban Advance 3 THR Superior with no difference in bleeding
Record 1 and 2 THR
Non-inferior
Apixaban Superior with no difference in bleedingAdvance 2 TKR
Rivaroxaban Superior with no difference in bleedingRecord 1 and 2 TKR
TKR Not approved for this IndicationDabigatran

10/21/19 11
Evidence for VTE Risk Reduction after Treatment
Edoxaban Not approved for this indication
Agnelli et al. NEJM 2012Weitz et al NEJM 2017Buller Blood 2009Schulman et al. NEJM 2013
Apixaban AMPLIFY - EXT Superior: vs placebo with similar bleeding
Rivaroxaban EINSTEIN – EXT and CHOICE • Superior: vs placebo with higher bleeding major bleeding
• 10mg and 20mg better than ASA
RE - MEDY and RE - SONATEDabigatran • Non-inferior vs warfarin with similar bleeding
• Superior vs placebo, higher major bleeding

10/21/1912
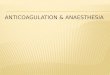
Reduction of Risk of Major Cardiovascular Events in Patients with Chronic CAD or PAD
COMPASS TRIAL
Ischemic stroke 0.51 (0.38, 0.69)Coronary heart disease death 0.73 (0.55, 0.96)Acute limb ischemia 0.55 (0.32, 0.92)Lower extremity amputations 0.45 (0.26, 0.89)
N = 9152 N = 9126
Rivaroxaban 2.5mg + ASA 100mg ASA 100mg alone
Patients with CAD and PAD
Patients with PAD
Acute limb ischemia 0.56 (0.32, 0.99)
Eikelboom et al. NEJM 2017

10/21/19 13
APEX: a multinational pivotal trial of extended VTE prophylaxis in acutely ill
medical patients (N=7513)1,*
Extended-duration Bevyxxa (35 to 42 days) vs enoxaparin (6 to 14 days) + placebo
Cohen et al. NEJUM 2016
Primary Efficacy Endpoint: Asymptomatic proximal DVT + symptomatic DVT
0.76 (95%CI 0.63, 0.92); p=0.006
Principle safety outcome: Major bleeding
1.19 (95% CI 0.67, 2.12); p=0.55

10/21/19 14
Why DOACs are preferred for most patients with VTE
• More convenient • No routine monitoring or dose adjustment • No dietary (and few drug-drug) interactions
• Simplified peri-procedural anticoagulation
• As effective as warfarin and safer

10/21/19 15
• Pro-thrombotic states: e.g. APLS
• Severe renal impairment (CrCl< 30 ml/min)
• Moderate to severe hepatic impairment
• Clinically significant drug interactions
• Extremely high body weight (> 120 kg ?)
• Prohibitive cost
When should a DOAC not be the first choice?

10/21/19 16
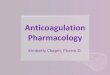
The folly of monitoringSchematic of drug effect: warfarin vs DOACs

10/21/19 17
Measuring DOACs: When

10/21/19 18
Lab Measurement for DOACs
• DOACs can (but do not always) prolong “traditional” clotting times (PTT or PT)
• Thrombin time (TT) is very sensitive to (even low concentrations of) dabigatran –a normal thrombin time excludes dabigatran

10/21/19 19Cuker et al JACC 2014
Measuring DOACs: How

10/21/19 20
Best tests for DOACsDabigatran: dilute thrombin time (calibrated for dabigatran)
Fxa inhibitors: anti-Xa assay (calibrated for a particular DOAC)
• Therapeutic ranges are not established
• “expected” trough: ~ 50 ng/mL
• “expected” peak: 150 –250 ng/mL
• “Safe” trough levels < 30 – 50ng/mL
Samuelson et al. Chest. 2016
Douxfils et al. JTH 2017
Levy et al. JTH 2015

10/21/19 21
FXa Inhibitory Profile of DOACS Does Fully Reflect Their Biologic Spectrum
Siddiqui et al. Clin Appl Thomb Hemost. 2019

10/21/19 22
DOACs and Heparins

10/21/19 23
Macedo et al. Annals of Pharmacotherapy 2018
Influence of of DOACs on Anti-FXa Measurements

10/21/19 24
Initiation of AC in Patients with Liver Disease

10/21/19 25
• Extreme obesity—also referred to as severe, grade III, or morbid obesity• BMI > 40 kg/m2
• 7.7% of the adult US population.
• 20 million extremely obese adults living in the US
• 500 000 extremely obese individuals in the US with AF have an indication or are receiving AC.
• 70 000 extremely obese patients in the US with VTE require AC
DOACs and the Obese Patient

10/21/19 26
PK /PD Studies in Obese Patients
Apixaban: • >120 kg vs 65-85 kg• 31% lower mean [peak]; 144ng/mL vs 207ng/mL• 24% higher Vd; 76 L vs 61 L• 20% decreased AUC• Authors considered differences in to be unimportant
Rivaroxaban• >120 kg vs 70-80 kg• Similar [peak} and AUC• Weight has no effect
Rivaroxaban pooled form Einstein DVT an ODIXa – DVT)• No difference in [peak]• High wt individuals have increase VD
Upreti et al. Br J Clin Pharmacol 2013Kubitza et al. J Clin Pharmacol 2007Meuck et al. Clin Pharmacokinet 2011

10/21/19 27
PK /PD Studies in Obese Patients
• Subgroup Analysis of Available PK data from large clinical trials
• PK/PD data suggests reduced drug exposure, lower [peak] and shorter t/2
• High interpatient patient variability by dose and indication
• Also there is large intra-patient variability for dabigatran

10/21/19 28
The International Society on Thrombosis and Haemostasis (ISTH)
• Subgroup analyses of obese patients from the large phase III DOAC vs warfarin trials suggest that DOACs are efficacious and safe in obese patients
• F <20% of patients in clinical trials had body weight ≥ 100kg
• Few patients with BMI >40 kg/m2 and PK data
• Suggest that DOACs not be used in patients with a BMI > 40 kg/m2 or a weight >120 kg
• If a DOAC is used , peak and trough levels should be measured
Piran et al. Res Pract Thromb Haemost. 2018Martin et al. JTH 2016

10/21/19 29
DOACs and APLS
TRAPS H/O thrombosis (VAM) plus Triple + Rivaroxaban vs warfarin 19% vs 3%
Events
ASTRO- APS H/O thrombosis ≥ 6 months on AC and APS Apixaban vs warfarin
Pengo et al. Blood 2008

10/21/19 30
DOACs and Patients with a History of GI Bleeding• The incidence of major GI bleeding varies among the DOACS
• RE-LY Trial• Dabigatran 150 vs warfarin 1.51 vs 11,02%/year; p<0.001• Dabigatran 110 vs warfarin 1.12 vs 1.02 %/year; p = 0.43
• Rocket-AF• Rivaroxaban vs warfarin 3.61 events /100 pt-yrs vs 2.60 events/pt-yrs
• ARISTOTLE • Apixaban vs warfarin no difference
• ENGAGE-TIMI-AF 48• Edoxaban 60 vs warfarin 1.51% va 1.23%; p = 0.03• Edoxaban 30 vs warfarin 0.82% p < 0.001
Czuprynska et al. BJH. 2017

10/21/19 31
Cancer Associated Venous ThrombosisDOAC vs dalteparin
RVTE %
Death (%)
Hokusai VTE Cancer(edoxaban)
Select-D VTE Cancerrivaroxaban
Pts
E 522
D 524
R 203
D 203
Duration
12 months
6 months
Major Bleeding%
6.9
4.0
6
4
7.9
11.3
4
11
39.5
36.6
25
30
Raskob et al. NEJM 2018Young et al. JCO 2019

10/21/19 32
DOACs to Prevent Cancer Associated Venous ThrombosisRandomized DOAC vs Placebo
AVERT Apixaban 2.5 4.2% vs 10.2% 0.41 (CI 0.26 – 0.65); P<0.001
Cassini Rivaroxaban 10 6.0% vs 8.8% 0.66 (CI 0.40 – 1.09); P<0.1
Major bleeding 3.5% vs 1.8%; p = 0.046
Major bleeding 4.7% vs 3.0%; p = 0.24
• apixaban – less VTE, more bleeding
• rivaroxaban – no change in VTE, more bleeding
Khorana et al. NEJM. 2019Carrier et al. NEJM. 2019

10/21/19 33
Heparin-induced Thrombocytopenia and Thrombosis
• 56 patients treated with DOACs and LAC
• Patients received • upfront DOAC, • after lead in AC• After platelet recovery
• 36 rivaroxaban; 12 apixaban, 11 dabigatran• 0 bleeds, 1 thrombotic event
Warkentin et a;l. Blood 2017

10/21/19 34
Barlow egt al. Pharmacotherapy 2019Cuker et al Blood Advances 2018Ng Thromb Res 2015
American Society of Hematology 2018 Guidelines for HIT
• DOACs (apixaban, dabigatran, rivaroxaban) conditional recommendation
• Stable patients without life or limb threatening VTE
• Patients with HIT characterized by platelet recovery
• Based on small case series and indirect evidence of less bleeding and similar efficacy to warfarin in VTE patients

10/21/19 35
American Society of Hematology HIT Guidelines

DOAC Pharmacokinetics
• Dabigatran• T1/2 CrCl > 50; 12-18 hours• T1/2 CrCl 30-50; 13-23 hours
• Rivaroxaban• T1/2 CrCl > 50; 7-10 hours• T1/2 CrCl 30-50; 9-13 hours
• Apixaban• T1/2 CrCl > 50; 7-10 hours• T1/2 CrCl 30-50; 9-13 hours
• Edoxaban• T1/2 CrCl > 50; 12-18 hours• Dosed reduced CrCl 30-50
Tafur et al et al Heart 2018
10/21/19 36

10/21/19 37
DOACS in Renal Impairment and Dialysis
Moll et al. The Hematologist 2017

10/21/19 38
DOACS in Renal Impairment and Dialysis
Moll et al. The Hematologist 2017Mavrakanas et al. J Am Soc Nephrol. 2017
• Patients on HD received 2.5 mg of apixaban
• AUC increased 2 -5.4 times between day 2 and day 8; p<0.001
• AUC was similar to 5mg dose in patients with preserved renal function
• Cmin and Cmax increased significantly
• Only 4% of drug removed during HD
• No significant data with other DOACs

Perioperative AC Use for Surgery Evaluation (PAUSE) Study
Presumes• A standardized protocol would be both easier and safe
• Obviates the need for heparin bridging and preoperative coagulation testing
• A low rate of major bleeding (1%) and arterial thrombosis (0.5%)
• >90% of patients will have minimal or non-detectable DOAC levels at surgery
Douketis et al ASH 201810/21/19 39

Patient Recruitment
N = 1082rivaroxaban cohort
3,640 patients screened
663 (17.4%) excluded
N = 1257apixaban cohort
N = 668dabigatran cohort
Mean age 72.533% HBR
Perioperative AC Use for Surgery Evaluation (PAUSE) Study
Eligibility• DOACs a sustained time• Creatinine Clearance >30 mL/min (apixaban >25)• Bleeding and thrombotic risk assessment by surgery
• Aim: Establish Safe standardized protocol for the perioperative management of patients with AF who are DOACs
• Design: Multi-center prospective observational cohort
• Patients: N=3300 with AF (1100/DOAC)
10/21/19 40Douketis et al ASH 2018

Perioperative AC Use for Surgery Evaluation (PAUSE) Study
RivaroxabanApixaban
Dabigatran
Bleeding risk LOW HIGH
STOP Id BEFORE STOP 2d BEFORE
LOW HIGH
CrCl ≥ 50<50≥ 50 <50
STOP Id BEFORE STOP 2d BEFORE STOP 4d BEFOREDouketis et al ASH 201810/21/19 41

PAUSE STUDY RESULTS
• Major Bleeding: apixaban 1.35%, dabigatran 0.9%, rivaroxaban 1.85%
• Arterial thromboembolism: apixaban 0.16%, dabigatran 0.6%, rivaroxaban 0.37%
• DOAC < 50ng/ml: apixaban 90.5%, dabigatran 96.8%, rivaroxaban 98.8%
• Standardized approach was safe and effective:• High bleeding risk: hold for 48h before; restart 48h after• Low bleeding risk: hold for 24h before; restart 24h after
• Bridging not needed
10/21/19 42Douketis et al ASH 2018

10/21/19 43
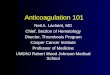
Idarucizumab: specific reversal agent for dabigatran

10/21/19 44
Idarucizumab: specific reversal agent for dabigatran
Glund S et al. AHA 2013
Healthy volunteer study: immediate, dose-dependent reversal of dabigatran anticoagulation

10/21/19 45
Clinical Outcomes
Group A
3 of 51 patients died from bleeding within 30 days
Group BNormal intraoperative hemostasis: 33
Mildly abnormal hemostasis: 2
Moderately abnormal hemostasis: 1
No evidence of prothrombotic or immunologic effect
Pollock et al. NEJM 2015

10/21/19 46
Andexanet: (FXa Decoy)Siegal et al. NEJM 2015
Binds and sequesters the factor Xa inhibitors,
rivaroxaban and apixaban
Binds and inhibits the activity of Tissue
Factor Pathway Inhibitor (TFPI) leading to
increased tissue factor-initiated thrombin
generation

10/21/19 47
Mechanism of Action of Prothrombin Complex Concentrates
Brinkman InTechOpen 2016

Reversal Agent OutcomesReversal Agent ANNEXA-4
Andexxa®Schulman et al. PCCs RE-VERSE AD
Praxbind®UPRATE
PCCs
Oral anticoagulant RivaroxabanApixaban
RivaroxabanApixaban
Dabigatran(Group A)
RivaroxabanApixaban
Study design Prospective, open-labelProspective,
observationalProspective, open-label
Prospective,
observational
Efficacy Population (N) 254 66 301 84
Age in years 77 (mean) 77 (mean) 79 (median) 75 (median)
Intracranial bleeding 67% 55% 33% 70%
Gastrointestinal bleeding 24% 24% 46% 16%
Ineffective hemostasis 18%* 32% 22% 31%
Safety Population (N) 352 66 301 84
Death 14% 14% 14% 32%
Thrombotic event 10% 8% 5% 4%
48*5 patients not included in analysis of hemostatic efficacy for administrative reasons.
NEJM 2019; 380(14): 1326-35.
Thromb Haemost 2018; 118(05): 842-51.
Blood 2017; 130(5): 1706-12.
NEJM 2017; 377(5): 431-41.

Direct Cost ComparisonReversal Agent Regimen Drug Cost per Unit Cost per Treatment*
Andexxa®Low Dose
$2750/100 mg$24,750
High Dose $49,500
Kcentra® 50 units/kg $1.60/unit $6400
FEIBA NF® 50 units/kg $1.70/unit $6800
Reimbursement Program for Andexxa®• New Technology Add-On Payment (NTAP)
reimbursement
*For 80 kg patient with INR > 6Cost Reflective As Of: 6/2019 Source: HC Pharmacy
49

10/21/19 50
Summary
• DOACs have differing biological properties
• In general appear to be similar to warfarin and LMWH in efficacy and less bleeding
• Rivaroxaban + aspirin has benefit for CAD and PAD
• My be ineffective or hazardous among special populations• Renal impairment, dialysis, APLS, Cancer patients
• Bleeding may be effectively reversed with specific antidotes, 4 factor PCCs, or by removal