Embed Size (px)
Citation preview

854 IEEE JOURNAL OF SELECTED TOPICS IN QUANTUM ELECTRONICS, VOL. 16, NO. 4, JULY/AUGUST 2010
Optical Spectroscopy to Guide PhotodynamicTherapy of Head and Neck Tumors
Dominic J. Robinson, M. Baris Karakullukcu, Bastiaan Kruijt, Stephen Chad Kanick, Robert P. L. van Veen,Arjen Amelink, Henricus J. C. M. Sterenborg, Max J. H. Witjes, and I. Bing Tan
(Invited Paper)
Abstract—In contrast to other interstitial applications of pho-todynamic therapy (PDT), optical guidance or monitoring in thehead and neck is at a very early stage of development. The presentpaper reviews the use of optical approaches, in particular opticalspectroscopy, that have been used or have the potential to guidethe application of PDT. When considering the usefulness of thesemethods, it is important to consider the volume over which thesemeasurements are acquired, the influence of differences in andchanges to the background optical properties, the implications forthese effects on the measured parameters and the difficulty of in-corporating these types of measurements in clinical practice inhead and neck PDT. To illustrate these considerations, we presentan application of a recently developed technique, which we termfluorescence differential path length spectroscopy for monitoringmeta-tetra(hydroxyphenyl)-chlorin or Foscan-PDT of interstitialhead and neck cancer.
Index Terms—Biomedical applications of optical radiation,blood, cancer, fluorescence spectroscopy, tumors.
I. INTRODUCTION
PHOTODYNAMIC therapy (PDT) is now established as atreatment modality for a range of solid tumors [1]–[3]. It
is based on the use of a photosensitizer that is administeredsystemically. Excitation of a photosensitizer with light of an ap-propriate wavelength results in the transfer of energy to molec-ular oxygen, which leads to the formation of reactive oxygenspecies. These species lead to the destruction of the target tissue,and surrounding normal tissue, by a range of mechanisms thatinclude direct tumor cell kill, destruction of tumor vasculatureand an immune response against tumor cells [4]–[7].
Manuscript received August 19, 2009; revised October 7, 2009; acceptedOctober 24, 2009. Date of publication March 22, 2010; date of current versionAugust 6, 2010. This work was supported in part by ZonMw: The Nether-lands Organization for Health Research and Development under Grant pTO95100107.
D. J. Robinson, B. Kruijt, S. C. Kanick, R. P. L. van Veen, A. Amelink, andH. J. C. M. Sterenborg are with the Department of Radiation Oncol-ogy, Center for Optical Diagnostics and Therapy, Erasmus Medical Center,Rotterdam 3000 CA, The Netherlands (e-mail: [email protected];[email protected]; [email protected]; [email protected];[email protected]; [email protected]).
M. B. Karakullukcu is with The Netherlands Cancer Institute—Antonivan Leeuwenhoek Hospital, 1066 CX Amsterdam, The Netherlands (e-mail:[email protected]).
M. J. H. Witjes is with the University Medical Center Groningen, Groningen9700 RB, The Netherlands (e-mail: [email protected]).
I. B. Tan is with the Netherlands Cancer Institute—Antoni van LeeuwenhoekHospital, 1066 CX Amsterdam, The Netherlands, and also with the Departmentof Otorhinolaryngology, Academic Medical Centre, Amsterdam 1100 DD, TheNetherlands (e-mail: [email protected]).
Color versions of one or more of the figures in this paper are available onlineat http://ieeexplore.ieee.org.
Digital Object Identifier 10.1109/JSTQE.2009.2035930
PDT has been applied widely in many clinical specialties. Asurvey of the literature on PDT yields relatively few publicationsdealing with head and neck cancer compared to, for example,prostate, esophageal, or lung cancer. The reason for this is likelyto be related to the current lack of regulatory approval for PDTin the United States and the only recent approval of PDT forhead and neck cancer in Europe for a limited number of indi-cations. Notwithstanding these regulatory issues, a number ofresearch groups are investigating the application of PDT in headand neck cancer with significant clinical success. A particularlygood example of efforts to this end is the application of PDTusing the photosensitizer meta-tetra(hydroxyphenyl)chlorin (m-THPC), Temoporfin, or Foscan. Foscan is approved for palliativetreatment of squamous cell carcinoma (SCC) of the head andneck in the European Union [2], [8], [9] and is used for curativeintent in superficial tumors in the oral cavity.
Head and neck SCC is the fifth most common form of cancerworldwide with an incidence of 780 000 new cases a year [10].The number of newly diagnosed head and neck cancer patientsis unfortunately still increasing. Recent data from the Dutchcancer registry have shown a 10% increase from 2400 newcases/year in 2003 to approximately 2650 in 2005 [10], [11].Approximately 40–50% of patients die of recurrent or residualdisease after conventional treatment. In addition, 20% of thesepatients show a second primary tumor of the head and neckregion. Surgery and/or radiotherapy are the cornerstones of firstline therapy [12]. However, in the case of recurrent or residualdisease, there are often very limited options. Surgery is oftennot feasible because of the inoperability of the tumor or eth-ically unacceptable collateral damage. Radiotherapy, possiblycombined with chemotherapy, can only be given to a certainmaximum dose, which usually is reached during the primarytreatment. Reirradiation can be an option in selected cases butis not routinely applied. Conventional treatment strategies haveconsiderable limitations in these cases of recurrent disease.
PDT does not utilize hazardous ionizing radiation and inprincipal does not have a maximal cumulative dose. For thisreason PDT remains a treatment option in the case of recurrenceor residual disease after the initial treatment. It has successfullybeen applied in the primary treatment of superficial SCC and inpalliative treatment of recurrent disease. The major advantageof PDT over conventional surgery or radiotherapy is that thewounds heal with less collateral damage [13], [14].
The therapeutic effect in PDT is mediated by the productionof reactive oxygen species in tissue and depends on the presenceof three components: light, photosensitizer, and oxygen, each in
1077-260X/$26.00 © 2010 IEEE

ROBINSON et al.: OPTICAL SPECTROSCOPY TO GUIDE PHOTODYNAMIC THERAPY OF HEAD AND NECK TUMORS 855
sufficient quantities to ablate tissue in the treatment volume. Ifone is missing, there is no biological effect. Studies have shownthat inter and intrasubject differences in parameters such as tis-sue optical properties and subsequent differences in deliveredfluence (rate), uptake of photosensitizer and tissue response toPDT can lead to wide variations in the dose delivered duringPDT [15]–[17]. Each of these parameters can be different forindividual lesions, patients, and crucially, they are interdepen-dent and change dynamically during, often as a result of ther-apy [16], [18]. There is a growing body of evidence to suggestthat the combined selectively offered by light and photosensi-tizer adds significantly to the complexity of PDT and that thiscan lead to the wide variations in the PDT dose that is deliveredto the target tissue and the surrounding normal tissues. Thesedosimetric uncertainties can easily lead to under treatment ofthe tumor and/or to the over treatment of normal tissue. Thepresent manuscript describes how ranges of optical approaches,in particular optical spectroscopy have been or could be appliedto guide PDT in the treatment of head and neck cancer.
Review: PDT is an optical therapy in which light, normallyred light, is delivered to the treatment site. In head and neckcancer the treatment site (or target volume) can range from asuperficial lesion in the oral cavity, the mucosa of an internallining of a cavity such as the nasopharynx or large solid tumorin, or for example, the tongue base. It is important to recognizethat the delivery of light to these markedly different volumesof tissue is a critical consideration, that is the subject of nu-merous ongoing studies [19]–[21]. For superficial lesions, it isrelatively straightforward to deliver light using surface illumi-nation. However, for intracavity illumination and the treatmentof large tumors, where interstitial illumination is necessary, thedelivery of light, only one of the components that is neces-sary for effective PDT, can be very challenging. While it isnot necessary to use spectroscopy to monitor the distributionof light within tissue, it is critical to many of the associatedfactors that influence PDT. Measuring, modeling, and monitor-ing the distribution of treatment light in tissue has a very longhistory [22] and has led to a deep understanding of the impor-tance of tissue optical properties. Optical spectroscopy can beused to measure tissue optical properties that have been usedby many investigators to inform the choice of PDT treatmentparameters such as the illumination wavelength, the separationof interstitial treatment fibers and the choice of optical treatmentparameters such as fluence and fluence rate. These parametersare dependent on the illumination wavelength, which is nor-mally determined by the photophysical properties of the pho-tosensitizer. The absorption and fluorescence characteristics ofphotosensitizers mean that they can be interrogated using opti-cal spectroscopy. The concentration of photosensitizer is clearlyan important parameter in the efficacy of PDT. Differences inthe uptake of photosensitizer in tumor tissue, between lesionsand/or patients and differences between the uptake in tumor andthe surrounding normal tissue are concepts that are critical toeffective PDT. Both the absorption and fluorescence propertiesof photosensitizer have been investigated for monitoring theirconcentrations. Photosensitizer spectroscopy in this sense canbe limited to the ex-vivo measurement of the concentrations ofdrug in tissue samples or it can be extended to incorporate in
vivo measurements. Monitoring photosensitizer pharmacokinet-ics (both temporal and spatial) is one of the most fundamentalareas of PDT investigation and examples of these types of stud-ies are too numerous to mention. The use of absorption andfluorescence spectroscopy is described in greater detail belowbut it is important to carefully consider the path length of lightin tissue if these types of measurements are to be quantitative.It is also useful to note that absorption techniques are affectedby lower signal to noise ratios and measurement techniques en-counter challenges associated with limited dynamic range whenphotosensitizers with low absorption coefficients are encoun-tered at low concentrations. In contrast, the dynamic range forfluorescence measurements is much larger than for absorptionmeasurements since the fluorescence is measured at a differ-ent wavelength than the excitation light. It is also important tonote that absorption and fluorescence measurements should beinterpreted with care. Fluorescence emission from fluorophoresis influenced by their environment. There exists a complex re-lationship between the concentration of a chromophore and itsabsorption cross-section and fluorescence emission intensity.In vivo fluorescence (and to a lesser degree absorption) canbe altered by many factors that include changes in quantumyield induced by changes in the microenvironment [23], photo-bleaching [24], biological compartmentalization, and alterationin binding and aggregation [25], [26].
In vivo absorption and to a greater degree fluorescence spec-troscopy are often used to monitor pharmacokinetics in preclin-ical models. These techniques are much less often used in theclinical environment. This is unfortunate since this is where theycan potentially have the greatest impact. Measuring photosen-sitizer pharmacokinetics is not the only area in which photo-sensitizer spectroscopy can be utilized in guiding or monitoringPDT. Clearly, PDT is a complex photochemical/biological pro-cess and is influenced by a wide range of parameters. Opticalspectroscopy has been used to investigate the processes thatoccur during PDT. The process of progressive destruction ofthe photosensitizer during PDT, mediated by the generation ofreactive oxygen species was recognized as an important factorin PDT dosimetry over two decades ago. This process termedphotosensitizer photobleaching has since been investigated innumerous preclinical studies for many photosensitizers. Pho-tobleaching was originally thought to be advantageous sincedifferential uptake of photosensitizer in tumor and normal com-bined with photobleaching to enhance selectivity [27]. Sincethese early studies, investigations utilizing photobleaching hasled investigators to a greater understanding of the photochem-istry that is underlying PDT and have been incorporated intodosimetric models for PDT [23], [28]. Over this time period,the understanding of the complexity of the role of tissue vas-culature and the demand (and supply) of oxygen during PDThas increased dramatically. The important role of fluence rateon the photobiology that occurs during PDT and its relationshipto PDT response is becoming increasingly clear [29]. In manycircumstances, the choice of clinical fluence rate is far abovethat that has been shown to be optimal in preclinical models.Again, it is important to highlight two points. First, it is critical tounderstand the mechanisms underlying the processes surround-ing fluorescence photobleaching and how they relate to tissue

856 IEEE JOURNAL OF SELECTED TOPICS IN QUANTUM ELECTRONICS, VOL. 16, NO. 4, JULY/AUGUST 2010
response. These can be different for different photosensitizersand different for different environments. Second, just as forpharmacokinetic measurements it is disappointing that very fewclinical studies have incorporated these types of measurements.
Optical spectroscopy can also be used to study other importanteffects that are related to the PDT process that may be used toguide PDT in Head and Neck cancer. Reflectance spectroscopycan be used to interrogate the tissue before, during, and afterPDT to monitor changes in the concentration of native absorbers.The predominate absorbers in the visible region of the spectrumin tissue are oxy- and deoxhemoglobin. These can and have beenused to determine variations in physiological parameters suchas blood saturation and blood content (volume). These types oftechniques have been used in PDT by a number of investigatorsto monitor the vascular response to PDT [30]–[32]. Dependingon the photosensitizer and its localization, the acute vascular re-sponse can be useful in predicting the overall response to PDT.These approaches are particularly important for predominatelyvascular-based photosensitizer such as Visudyne and Tookad.In this context, it is important to consider blood flow in tissueundergoing PDT. Here, other novel approaches such as laserspeckle imaging [32] and diffuse correlation spectroscopy [33]have been utilized to monitor blood flow. It is also possibleto consider the use of other spectroscopy techniques such asRaman spectroscopy [34] and spectroscopic optical coherencetomography [35] but considering the complexity of these tech-niques they are not yet read for implementation for guiding ormonitoring PDT.
When considering the spectroscopic approaches describedearlier and their utility for guiding PDT in the head and neckit is important to consider: 1) the volume over which thesemeasurements are acquired; 2) the influence of differences inand changes to the background optical properties; 3) the im-plications for these effects on the measured parameters; and 4)the difficulty of incorporating these types of measurements inclinical practice in head and neck PDT.
To illustrate these considerations, we present an application ofa recently developed technique we term fluorescence differentialpath length spectroscopy (FDPS) for monitoring Foscan-PDTin head and neck cancer.
II. MATERIALS AND METHODS
A. Optical Spectroscopy
The noninvasive quantitative optical measurement of chro-mophore concentrations in tissue requires knowledge of the op-tical path length in the tissue. For most fiber-optic measurementgeometries the optical path length depends on the scatteringcoefficient µs and on the absorption coefficient µa . Since bothµs and µa vary significantly in tissue, quantitative measure-ments prove to be difficult in tissue unless specific fiber-opticmeasurement geometries are chosen. For example, the opti-cal pharmacokinetic spectroscopy (OPS) device developed byMourant et al. [36] uses elastic scattering spectra of tissue tocalculate the concentration of chromophores in tissue. This de-vice utilizes a fiber-optic probe that contains a single source anda single detector fiber that are separated by 2 mm. This separa-tion was chosen to minimize the dependence of the path length
of the collected photons on scattering properties of tissue. Forscattering parameters that are typical of tissue, the path lengthvaries by less than 20% for a given background absorption. Adrawback of this method is that the path length is sensitive tothe (background) absorption coefficient of tissue. This meansthat the amount of measured absorption due to the target chro-mophore strongly depends on the local blood content and bloodsaturation. As a consequence, a measurement must be madeprior to injection of the target chromophore and only changes inconcentration can be measured assuming that the backgroundabsorption does not change in time. This makes OPS measure-ments difficult when a background reflectance spectrum cannotbe acquired, and even more difficult to interpret when thereare changes in the background absorption of tissue. Changesin background absorption can occur for a variety of reasons,for example, pressure between the measurement probe and thesurface of the tissue can influence the blood content. Open sur-gical procedures can significantly influence both blood volumeand saturation. Furthermore, changes in background absorptionare a particular problem during PDT since blood volume andsaturation can change as a result of the therapy itself. Anothertechnique that features a known path length is differential pathlength spectroscopy (DPS) [37]. The path length of photons con-tributing to the differential reflectance signal varies only slightlyover a very broad range of both scattering and absorption coeffi-cients. This facilitates quantitative concentration measurementseven for strong variations in either absorption or scattering. Forthis reason, we have now developed a technique based on theprinciples of DPS (subtraction of the diffuse photons to obtaina well-defined measurement volume) but with the enhanced dy-namic range of fluorescence measurements: fluorescence-DPS(FDPS) [38].
B. Patients and Procedure
Patients undergoing PDT for the palliative treatment of SCCof the head and neck gave written informed consent to par-ticipate in the study and the local hospital ethics committeeapproved the study. Ninety-six hours before illumination pa-tients were administered with 0.15 mg/kg intravenous Foscan(Biolitec Pharma, Ireland). On the day of the illumination hollowneedles are inserted percutaneously through the palpable tumormass. Tumor volumes can range from 40 cm3 up to 150 cm3 .Catheters are positioned in rows with an inter catheter distanceof less then <15 mm to aim for full coverage of the excitationlight throughout the tumor volume. After the inner sections ofthe needles are removed, the catheters are guided to the needletip, the needles are withdrawn and the transparent catheters arein position. After all of the catheters are in place, they are filledwith dummy after-loader. Each after-loader consists of a thinflexible wire with lead beads with an inter distance spacing of10 mm that allows for the unique identification of each catheterunder X-ray imaging. In order to confirm proper catheter iden-tification and localization, two orthogonal images are acquired.Based upon this information, the length and insertion depthof each cylindrical diffuser is estimated. During therapy eachlinear diffuser sequentially delivers a fixed incident fluence of30 J·cm−1 at a fluence rate of 100 mW·cm−1 .

ROBINSON et al.: OPTICAL SPECTROSCOPY TO GUIDE PHOTODYNAMIC THERAPY OF HEAD AND NECK TUMORS 857
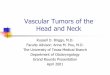
Fig. 1. Schematic overview of the FDPS setup illustrating how notch filters are used to block the treatment radiation so that reflectance and fluorescence spectracan be acquired without interrupting the therapeutic illumination.
C. Fluorescence Differential Path Length Spectroscopy
A single FDPS needle probe was designed for this application.A stainless steel needle contained two 400 µm fibers placed at acore-to-core distance of 440 µm and polished under an angle of35◦ to minimize specular reflection at the probe-tissue interface.Excitation light from a 650 nm diode laser (Diomed, Cambridge,United Kingdom) for fluorescence measurements delivered lightto the FDPS probe. Note, this laser was used in addition to thatused for the PDT illumination. Shutters (Ocean Optics, Duiven,the Netherlands) in the individual light paths allowed control ofthe excitation light. The excitation light is then coupled into a100 µm bifurcated fiber, the other leg is coupled into a whitelight source for DPS measurements. The distal end of the 100µm bifurcated fiber is coupled into a 200 µm fiber of which theother leg is coupled into the first channel of a 650 nm notchfiltered two-channel spectrograph. The distal end of the 200 µmbifurcated fiber is coupled into the light delivery and collection(dc) fiber of the FDPS needle. The collection (c) fiber is coupleddirectly into the second channel of the 650 nm notch filtered two-channel spectrograph. A schematic diagram of the setup and thetransmission of the notch filter is shown in Fig. 1. Immediatelybefore the start of the treatment procedure, the FDPS needlewas inserted into the tumor at a position approximately 2 cmfrom the surface of the skin in the chin side of the patientapproximately at the center of the tumor volume. Before theonset of the therapeutic illumination, sequences of reflectancespectra were acquired to ensure that the FDPS needle tip wasin contact with the tissue. During illumination, FDPS spectrawere acquired with an integration time of between 2 and 5 s atan interval between 2 and 10 s, respectively.
D. Data Analysis
Fluorescence spectra were analyzed as a linear combinationof basis spectra using a singular value decomposition (SVD)algorithm as others and we described previously [39], [40]. The
fluorescence was described by a combination of autofluores-cence and Foscan fluorescence and a third component since thedifferential fluorescence spectra contain a small contributionfrom the therapeutic laser. Based on the residual laser signal be-fore and beyond the blocking region of the 650 nm notch filter,a Gaussian was fitted to describe the laser signal, peak at 648nm width 12.3 nm. For the Foscan component, the first and lastspectra during illumination were subtracted under the assump-tion that any possible Foscan photoproducts have a negligiblecontribution to the measured fluorescence and that the autofluo-rescence signal is constant. Subsequently, the Foscan and lasercomponents were subtracted from the measured fluorescencesignal to yield a component for the autofluorescence. The dif-ferential reflectance signal was fitted using the same model asdescribed previously [40] to obtain values on saturation andblood volume.
III. RESULTS
Fig. 2 shows a preoperative sagittal T1-weighted MR imageof a recurrent SCC at the base of tongue typical of the sizetreated with PDT. The treatment volume was then imaged usinga plane X-ray (C-bow) as shown in Fig. 3. Fig. 4 shows the place-ment of a single therapeutic light source with an FDPS needleplaced immediately adjacent to this light source approximatelyat the center of the illumination catheter near the center of thetumor. Fig. 5 shows the normalized basis spectra of Foscan andthe combination of tissue autofluorescence and a small compo-nent of scattered laser light above 675 nm that were used tofit the FDPS spectrum acquired during illumination. Before thetherapeutic illumination, the blood saturation was 4 ± 1% andthe blood volume was 3 ± 0.2% illustrating the low saturationthat is typical of head and neck tumors. Fig. 6 shows two DPSspectra acquired at the start of and at the end of a single thera-peutic illumination. During the course of the illumination, therewas a small decrease in the blood saturation within the tumor

858 IEEE JOURNAL OF SELECTED TOPICS IN QUANTUM ELECTRONICS, VOL. 16, NO. 4, JULY/AUGUST 2010
Fig. 2. Example of a sagittal T1-weighted MR image of recurrent SCC baseof tongue.
Fig. 3. Intraoperative X-ray: PDT/brachytherapy catheters after loaded withwires containing lead implants (interspacing 10 mm). Opaque buttons demarcatethe surface of the tongue and the skin of the chin.
(to 2 ± 3%) and a significant increase in the blood volume from3% to 10%. Fig. 7 shows the fitted FDPS component attributedto Foscan. During the course of the illumination, there is a re-duction in Foscan fluorescence of approximately 50%. Based ona first estimate of the tissue optical properties within the treat-ment volume (µs ′ = 5 cm−1 and µa = 0.2 cm−1) we estimatethe fluence rate at the tip of the FDPS probe to be between 30and 50 mW cm−2 .
IV. DISCUSSION
This paper illustrates the implementation of a method forquantitative reflectance and quantitative fluorescence spec-troscopy measurements in PDT of head and neck cancer. In con-
Fig. 4. Photodynamic therapy illumination procedure: sequential illuminationusing seven interstitially implanted catheters containing cylindrical diffusingfibers: illumination time 300 s per source, output power 100 mW·cm−1 diffuser.
Fig. 5. Basis spectra for FDPS (Foscan) and tissue autofluorescence.
trast to other interstitial applications of PDT, optical monitoringin the head and neck is at a very early stage of development.Groups working in organs such as the prostate [19], [20], [41],the brain [42], [43] and in the GI tract [44], [45] have mademuch more progress toward in vivo guidance and monitoringusing optical spectroscopy. This is clearly a consequence of thedifferent stages of implementation of PDT in these organs butis also influenced by the limited use of optical monitoring inclinical PDT as a whole. Except for a small number of notableexceptions the use of these types of pharmacokinetic and opticaldosimetric measurements has not been widely adopted. This isparticularly true in interstitial PDT where dosimetric consid-erations are often restricted to that of light. It is important tonote that optical guidance using spectroscopy during interstitialPDT is challenging. The time that can be associated with thesetypes of measurements is a significant barrier to their adoption.For example, the acquisition of reflectance spectra during PDT

ROBINSON et al.: OPTICAL SPECTROSCOPY TO GUIDE PHOTODYNAMIC THERAPY OF HEAD AND NECK TUMORS 859
Fig. 6. Two representative Levenberg–Marquardt fit of the DPS signal ac-quired during PDT indicating blood saturation StO2 and blood volume (ρ).Note the discontinuities in the spectrum at 652 and 450 nm are due to the notchfilter. Error bars represent the standard deviation within a bin width of ten datapoints.
Fig. 7. Absolute fitted FDPS intensity acquired during the illumination ofa single therapeutic source located adjacent (5 mm distance) from the FDPSneedle, where error bars represent the fit inaccuracy on individual spectral fits.
is normally limited by the therapeutic illumination [31], [46].This means that either the acquisition of reflectance spectrais limited to directly pre- and post-PDT or the illuminationis interrupted for the acquisition of reflectance spectra. In thelatter case, this also means an alteration of the intended lighttreatment parameters. In the spectroscopic technique that wehave implemented here, we overcame this problem by placing anotch filter centered at the treatment wavelength. This allows ac-quisition of differential reflectance measurements during PDTwithout interruptions to the illumination. This relatively sim-ple step that facilitates the incorporation of these measurementsinto the clinical environment should not be underestimated sinceinterrupting PDT can have significant effects on the supply of
oxygen to tissue [47]. We have also used an approach to theacquisition of fluorescence spectra that is similar to that used byother investigators for other photosensitizers in other treatmentgeometries [40], [48]. Utilizing fluorescence excitation at thetreatment wavelength means that these measurements can beacquired without interrupting PDT. This can, however, be chal-lenging for photosensitizers that do not have strong fluorescenceemission beyond the therapeutic illumination wavelength.
The data we present show the feasibility of the approach tofiber optic spectroscopy in head and neck cancer. It is possible torecover fluorescence from Foscan 96 h after the administrationof Foscan and to monitor the local reduction of Foscan fluores-cence during PDT. The parameters that are recovered using DPSinclude blood saturation and blood volume. Our measurementsare consistent with data in the literature and confirm the lowoxygenation status of head and neck tumors [49]. Our data alsoshow that PDT induces changes in local blood volume that maybe consistent with vascular response to PDT. Taken as a whole,these data represent clear challenges to our understanding ofthe photochemistry underlying Foscan PDT and its relationshipto local PDT response. It is known that the mechanism(s) un-derlying the deposition of dose during PDT with Foscan arecomplex [50]–[54] but it is clear that in vivo local oxygen satu-rations that are encountered are very low.
Given these encouraging preliminary data it is important tostress that these measurements are acquired very locally andsingle optical probe measurements cannot be considered to berepresentative of larger volumes of tumor tissue. This has ledmany investigators to use diffuse optical techniques such asdiffuse reflectance spectroscopy with either visible/white light[31]–[33], [55]. Clearly, while these approaches could have animportant role in the spectroscopic guidance of PDT in headand neck cancer they do suffer from some disadvantages.
A potential source of error in diffuse reflectance spectroscopyis that the path length and hence the interrogated volume arestrongly wavelength dependent. Tissue optical properties canvary during PDT making the wavelength dependent path lengthalso variable in time. In contrast, DPS is used in this paper todetermine saturation and blood volume where the path lengthis known and insensitive to changes in optical properties. Thiscould make these types of measurements more advantageousfor monitoring PDT locally.
Another important issue is that the interrogated volume indiffuse reflectance spectroscopy is larger than in DPS where itis approximately the fiber diameter used. In large tissue volumemeasurements, there exists wide range of variations in fluencerate, dose deposition, and possibly variations in photosensitizerconcentration over the interrogated volume during illumination.All these variations are averaged out over the interrogated tissuevolume together with potential important local PDT-induced ef-fects. DPS measures over smaller volumes over which obviouslythe variations in fluence rate, deposited dose, and photosensi-tizer concentration are smaller.
One advantage of our approach to optical monitoring us-ing FDPS is that the blood saturation, blood volume, andfluorescence are measured using the same geometry and are,therefore, acquired from similar volumes of tissue. Monitoring

860 IEEE JOURNAL OF SELECTED TOPICS IN QUANTUM ELECTRONICS, VOL. 16, NO. 4, JULY/AUGUST 2010
fluorescence in optically thick or interstitial geometries is com-plicated by the fact that fluorescence is normally collected fromvolumes of tissue that are illuminated with a wide range offluence rates. This can confound the interpretation of signalssuch as fluorescence photobleaching, which may or may not befluence rate dependent depending on the photosensitizer.
Again, it is clear that these types of fluorescence measure-ments are unlikely to be representative of large volumes of tu-mor tissue and there is a clear requirement for multiple measure-ments as has been suggested previously by other authors [56]. Itis probable that it will be most advantageous to consider local-izing the regions over which spectroscopic guidance and opticalmonitoring are performed to a reasonable number of volumeswithin the target tissue. In this way, volumes of tissue could bechosen to monitor the extremes of photosensitizer concentrationand tissue oxygenation within the target tumor volume and invulnerable normal tissue.
An obvious parameter that is missing from our approach butthat has been extensively incorporated using diffuse optical tech-niques is a local measurement of blood flow [57]. Without suchdata, it can be difficult to correctly interpret dynamic changesin blood volume and saturation and their relationship to PDTinduced effects. It is, however, likely that measurement of bloodflow would need to be made over a larger volume to incorporatea measure of the regional blood flow.
Given the feasibility of the type of optical monitoring thatwe propose, it is important to consider the potential for thesetypes of measurements, and how they might be incorporatedinto the wider use of online dosimetry models or be applied tothe modification of the PDT treatment parameters. Quantitativemeasurements of pretreatment Foscan fluorescence intensitiescould offer the possibility of measuring spatial variations inphotosensitizer concentration within individual tumors or be-tween tumors in different patients. In a similar way, quantitativemeasurements of blood saturation and blood volume fractioncould be incorporated into the clinical decision-making process.Quantitative measurements of photosensitizer photobleachingin combination with the local measurements of tissue physiol-ogy may give more detailed insights into the choice of clinicaltreatment parameters such as fluence rate and drug light interval.
In conclusion, while it is clear that optical guidance of PDT inhead and neck cancer is at a very early stage of development, itseems critical that we learn from the experience of other inves-tigators working in other organs and to choose the appropriatemethods for optical monitoring that allow for representativequantitative measurements that can be incorporated into clinicaltreatment regimens.
REFERENCES
[1] B. C. Wilson and M. S. Patterson, “The physics, biophysics and technologyof photodynamic therapy,” Phys. Med. Biol., vol. 53, pp. R61–R109, 2008.
[2] W. Jerjes, T. Upile, C. S. Betz, M. El Maaytah, S. Abbas, A. Wright et al.,“The application of photodynamic therapy in the head and neck,” Dent.Update, vol. 34, pp. 478–484, 486, 2007.
[3] H. Stepp, T. Beck, T. Pongratz, T. Meinel, F. W. Kreth, J. Ch. Tonn, andW. Stummer, “ALA and malignant glioma: Fluorescence-guided resectionand photodynamic treatment,” J. Environ. Pathol. Toxicol. Oncol., vol. 26,pp. 157–164, 2007.
[4] B. W. Henderson, S. M. Waldow, T. S. Mang, W. R. Potter, P. B. Malone,and TJ. Dougherty, “Tumor destruction and kinetics of tumor cell deathin two experimental mouse tumors following photodynamic therapy,”Cancer Res., vol. 45, pp. 572–576, 1985.
[5] B. Krammer, “Vascular effects of photodynamic therapy,” AnticancerRes., vol. 21, pp. 4271–4277, 2001.
[6] M. Korbelik and G. J. Dougherty, “Photodynamic therapy-mediated im-mune response against subcutaneous mouse tumors,” Cancer Res., vol. 59,pp. 1941–1946, 1999.
[7] Y. G. Qiang, C. M. Yow, and Z. Huang, “Combination of photodynamictherapy and immunomodulation: Current status and future trends,” Med.Res. Rev., vol. 28, pp. 632–644, 2008.
[8] K. J. Lorenz and H. Maier, “Photodynamic therapy with meta-tetrahydroxyphenylchlorin (Foscan) in the management of squamous cellcarcinoma of the head and neck: Experience with 35 patients,” Eur. Arch.Otorhinolaryngol., vol. 266, pp. 1937–1944, 2009.
[9] European Medicines Agencies. H-C-318 Foscan European Public Assess-ment Rep. 30-4-2009.
[10] Visser & K van Noord, Feiten en Fabels over kanker in Nederland, Verenig-ing van Nederlandse Kanker Centra. Almelo 2005.
[11] Dutch Cancer Registry: De cijfers van de Nederlandse Kanker registratie:(kankerregistratie.nl).
[12] Richtlijn Mondholte en orofarynxcarcinoom. Nederlandse WerkgroepHoofd Hals Tumoren. 2004. van Zuiden (Alphen a/d Rijn ISBN 90-8523-005-5).
[13] C. Hopper, A. Kubler, H. Lewis, I. B. Tan, and G. Putnam, “mTHPC-mediated photodynamic therapy for early oral squamous cell carcinoma,”Int. J. Cancer, vol. 10, pp. 138–146, 2004.
[14] S. B. Brown, E. A. Brown, and I. Walker, “The present and future roleof photodynamic therapy in cancer treatment,” Lancet Oncol., vol. 5,pp. 497–508, 2004 [Review].
[15] H. J. Nyst, R. L. van Veen, I. B. Tan, R. Peters, S. Spaniol, D. J. Robinson,F. A. Stewart, P. C. Levendag, and H. J. C. M. Sterenborg, “Performanceof a dedicated light delivery and dosimetry device for photodynamic ther-apy of nasopharyngeal carcinoma: Phantom and volunteer experiments,”Lasers Surg. Med., vol. 39, pp. 647–653, 2007.
[16] T. Glanzmann, C. Hadjur, M. Zellweger, P. Grosiean, M. Forrer, J. P.Ballini, P. Monnier, H. Van Den Bergh, C. K. Lim, and G. Wagnieres,“Pharmacokinetics of tetra(m-hydroxyphenyl)chlorin in human plasmaand individualized light dosimetry in photodynamic therapy,” Photochem.Photobiol., vol. 67, pp. 596–602, 1998.
[17] T. C. Zhu, A. Dimofte, J. C. Finlay, D. Stripp, T. Busch, J. Miles,R. Whittington, S. B. Malkowicz, Z. Tochner, E. Glatstein, and S. M. Hahn,“Optical properties of human prostate at 732 nm measured in mediatedphotodynamic therapy,” Photochem. Photobiol., vol. 81, pp. 96–105,2005.
[18] A. Amelink, A. Van Den Heuvel, W. J. de Wolf, D. J. Robinson, and H. J.C. M. Sterenborg, “Monitoring PDT by means of superficial reflectancespectroscopy,” J. Photochem. Photobiol. B: Biol., vol. 79, pp. 243–251,2005.
[19] J. C. Finlay, T. C. Zhu, A. Dimofte, D. Stripp, S. B. Malkowicz, T. M.Busch, and S. M. Hahn, “Interstitial fluorescence spectroscopy in the hu-man prostate during motexafin lutetium-mediated photodynamic therapy,”Photochem. Photobiol., vol. 82, pp. 1270–1278, 2006.
[20] R. A. Weersink, A. Bogaards, M. Gertner, S. R. Davidson, K. Zhang,G. Netchev, J. Trachtenberg, and B. C. Wilson, “Techniques for deliveryand monitoring of TOOKAD (WST09)-mediated photodynamic therapyof the prostate: Clinical experience and practicalities,” J. Photochem.Photobiol. B, vol. 79, pp. 211–222, 2005.
[21] W. J. Cottrell, A. D. Paquette, K. R. Keymel, T. H. Foster, and A. R.Oseroff, “Irradiance-dependent photobleaching and pain in aminolevulinicacid-photodynamic therapy of superficial basal cell carcinomas,” Clin.Cancer Res., vol. 14, pp. 4475–4483, 2008.
[22] W. M. Star, “Light dosimetry in vivo,” Phys. Med. Biol., vol. 42, pp. 763–787, 1997 [A Review].
[23] B. C. Wilson, M. S. Patterson, and L. Lilge, “Implicit and explicit dosime-try in photodynamic therapy: A new paradigm,” Lasers Med. Sci., vol. 12,pp. 182–199, 1997.
[24] D. J. Robinson, H. S. de Bruijn, N. Van Der Veen, M. R. Stringer, S. B.Brown, and W. M. Star, “Fluorescence photobleaching of ALA-inducedprotoporphyrin IX during photodynamic therapy of normal hairless mouseskin: The effect of light dose and irradiance and the resulting biologicaleffect,” Photochem. Photobiol., vol. 67, pp. 140–149, 1998.
[25] K. Woodburn, C. K. Chang, S. Lee, B. Henderson, and D. Kessel, “Biodis-tribution and PDT efficacy of a ketochlorin photosensitizer as a function

ROBINSON et al.: OPTICAL SPECTROSCOPY TO GUIDE PHOTODYNAMIC THERAPY OF HEAD AND NECK TUMORS 861
of the delivery vehicle,” Photochem. Photobiol., vol. 60, pp. 154–159,1994.
[26] B. Aveline, T. Hasan, and R. W. Redmond, “Photophysical and pho-tosensitizing properties of benzoporphyrin derivative monoacid ring A(BPD-MA),” Photochem. Photobiol., vol. 59, pp. 328–335, 1994.
[27] T. S. Mang, T. J. Dougherty, W. R. Potter, D. G. Boyle, S. Somer, andJ. Moan, “Photobleaching of porphyrins used in photodynamic therapyand implications for therapy,” Photochem. Photobiol., vol. 45, pp. 501–506, 1987.
[28] K. K. Wang, S. Mitra, and T. H. Foster, “A comprehensive mathematicalmodel of microscopic dose deposition in photodynamic therapy,” Med.Phys., vol. 34, pp. 282–293, 2007.
[29] B. W. Henderson, T. M. Busch, and J. W. Snyder, “Fluence rate as amodulator of PDT mechanisms,” Lasers Surg. Med., vol. 38, pp. 489–493, 2006 [Review].
[30] H. W. Wang, M. E. Putt, M. J. Emanuele, D. B. Shin, E. Glatstein, A. G.Yodh, and T. M. Busch, “Treatment-induced changes in tumor oxygenationpredict photodynamic therapy outcome,” Cancer Res., vol. 64, pp. 7553–7561, 2004.
[31] B. W. Pogue, K. D. Paulsen, J. A. O’Hara, C. M. Wilmot, and H. M. Swartz,“Estimation of oxygen distribution in RIF-1 tumors by diffusion model-based interpretation of pimonidazole hypoxia and eppendorf measure-ments,” Radiat. Res., vol. 155, pp. 15–25, 2001.
[32] B. Kruijt, H. S. de Bruijn, A. Van Der Ploeg-van den Heuvel, H. J.Sterenborg, and D. J. Robinson, “Laser speckle imaging of dynamicchanges in flow during photodynamic therapy,” Lasers Med. Sci., vol. 21,pp. 208–212, 2006.
[33] G. Yu, T. Durduran, C. Zhou, T. C. Zhu, J. C. Finlay, T. M. Busch, S. B.Malkowicz, S. M. Hahn, and A. G. Yodh, “Real-time in situ monitoringof human prostate photodynamic therapy with diffuse light,” Photochem.Photobiol., vol. 82, pp. 1279–1284, 2006.
[34] A. Nijssen, S. Koljenovic, T. C. B. Schut, P. J. Caspers, and G. J. Puppels,“Towards oncological application of Raman spectroscopy,” J. Biophoton.,vol. 2, pp. 29–36, 2009.
[35] M. Khurana, E. H. Moriyama, A. Mariampillai, and B. C. Wilson, “In-travital high-resolution optical imaging of individual vessel response tophotodynamic treatment,” J. Biomed. Opt., vol. 13, p. 040502.X, 2008.
[36] J. M. Mourant, T. M. Johnson, G. Los, and I. J. Bigio, “Noninvasivemeasurement of chemotherapy drug concentrations in tissue: Prelimi-nary demonstrations of in vivo measurement,” Phys. Med. Biol., vol. 44,pp. 1397–1417, 1999.
[37] A. Amelink and H. J. C. M. Sterenborg, “Measurement of the local opticalproperties of turbid media using differential pathlength spectroscopy,”Appl. Opt., vol. 43, pp. 3048–3054, 2004.
[38] A. Amelink, B. Kruijt, D. J. Robinson, and H. J. Sterenborg, “Quantitativefluorescence spectroscopy in turbid media using fluorescence differentialpath length spectroscopy,” J. Biomed. Opt., vol. 13, p. 054051, 2008.
[39] J. C. Finlay, D. L. Conover, E. L. Hull, and T. H. Foster, “Porphyrinbleaching and PDT-induced spectral changes are irradiance dependent inALA-sensitized normal rat skin in vivo,” Photochem. Photobiol., vol. 73,pp. 54–63, 2001.
[40] B. Kruijt, H. S. de Bruijn, A. Van Der Ploeg-van den Heuvel, R. W. deBruin, H. J. Sterenborg, A. Amelink, and D. J. Robinson, “MonitoringALA-induced PpIX photodynamic therapy in the rat esophagus using flu-orescence and reflectance spectroscopy,” Photochem. Photobiol., vol. 84,pp. 1515–1527, 2008.
[41] T. Svensson, E. Alerstam, M. Einarsdottır, K. Svanberg, and S. Andersson-Engels, “Towards accurate in vivo spectroscopy of the human prostate,”J. Biophoton., vol. 1, pp. 200–203, 2008.
[42] V. X. Yang, P. J. Muller, P. Herman, and B. C. Wilson, “A multispectralfluorescence imaging system: Design and initial clinical tests in intra-operative Photofrin-photodynamic therapy of brain tumors,” Lasers Surg.Med., vol. 32, pp. 224–232, 2003.
[43] H. Stepp, T. Beck, T. Pongratz, T. Meinel, F. W. Kreth, J. Ch. Tonn, andW. Stummer, “ALA and malignant glioma: Fluorescence-guided resectionand photodynamic treatment,” J. Environ. Pathol. Toxicol. Oncol., vol. 26,pp. 157–164, 2007.
[44] R. S. Dacosta, B. C. Wilson, and N. E. Marcon, “Spectroscopy and fluo-rescence in esophageal diseases,” Best Pract. Res. Clin. Gastroenterol.,vol. 20, pp. 41–57, 2006.
[45] R. L. van Veen, D. J. Robinson, P. D. Siersema, and H. J. Sterenborg, “Theimportance of in situ dosimetry during photodynamic therapy of Barrett’sesophagus,” Gastrointest. Endosc., vol. 64, pp. 786–788, 2006.
[46] E. L. Larsen, L. L. Randeberg, O. A. Gederaas, C. J. Arum, A. Hjelde,C. M. Zhao, D. Chen, H. E. Krokan, and L. O. Svaasand, “Monitoring
of hexyl 5-aminolevulinate-induced photodynamic therapy in rat bladdercancer by optical spectroscopy,” J. Biomed. Opt., vol. 13, p. 044031,2008.
[47] H. Tsutsui, A. J. MacRobert, A. Curnow, A. Rogowska, G. Buonaccorsi,H. Kato, and S. G. Bown, “Optimisation of illumination for photodynamictherapy with mTHPC on normal colon and a transplantable tumour in rats,”Lasers Med. Sci., vol. 17, pp. 101–109, 2002.
[48] W. J. Cottrell, A. D. Paquette, K. R. Keymel, T. H. Foster, and A. R.Oseroff, “Irradiance-dependent photobleaching and pain in aminolevulinicacid-photodynamic therapy of superficial basal cell carcinomas,” Clin.Cancer Res., vol. 14, pp. 4475–4483, 2008.
[49] E. Lartigau, A. M. Le Ridant, P. Lambin, P. Weeger, L. Martin, R. Sigal,A. Lusinchi, B. Luboinski, F. Eschwege, and M. Guichard, “Oxygenationof head and neck tumors,” Cancer, vol. 71, pp. 2319–2325, 1993.
[50] J. C. Finlay, S. Mitra, and T. H. Foster, “In vivo m-THPC photobleachingin normal rat skin exhibits unique irradiance-dependent features,” Pho-tochem. Photobiol., vol. 75, pp. 282–288, 2002.
[51] C. Hadjur, N. Lange, J. Rebstein, P. Monnier, H. Van Den Bergh, andG. Wagnieres, “Spectroscopic studies of photobleaching and photoproductformation of meta(tetrahydroxyphenyl)chlorin (m-THPC) used in pho-todynamic therapy. The production of singlet oxygen,” J. Photochem.Photobiol. B, vol. 45, pp. 170–178, 1998.
[52] S. Coutier, S. Mitra, L. N. Bezdetnaya, R. M. Parache, I. Georgakoudi,T. H. Foster, and F. Guillemin, “Effects of fluence rate on cellsurvival and photobleaching in meta-tetra-(hydroxyphenyl)chlorin-photosensitized Colo 26 multicell tumor spheroids,” Photochem. Pho-tobiol., vol. 73, pp. 297–303, 2001.
[53] L. Kunz and A. J. MacRobert, “Intracellular photobleaching of 5,10,15,20-tetrakis(m-hydroxyphenyl) chlorin (Foscan) exhibits a complex depen-dence on oxygen level and fluence rate,” Photochem. Photobiol., vol. 75,pp. 28–35, 2002.
[54] J. S. Dysart, M. S. Patterson, T. J. Farrell, and G. Singh, “Relationshipbetween m-THPC fluorescence photobleaching and cell viability duringin vitro photodynamic treatment of DP16 cells,” Photochem. Photobiol.,vol. 75, pp. 289–295, 2002.
[55] J. H. Woodhams, L. Kunz, S. G. Bown, and A. J. MacRobert, “Correlationof real-time haemoglobin oxygen saturation monitoring during photody-namic therapy with microvascular effects and tissue necrosis in normal ratliver,” Brit. J. Cancer, vol. 91, pp. 788–794, 2004.
[56] B. W. Pogue, B. Chen, X. Zhou, and P. J. Hoopes, “Analysis of samplingvolume and tissue heterogeneity on the in vivo detection of fluorescence,”J. Biomed. Opt., vol. 10, p. 41206, 2005.
[57] U. Sunar, H. Quon, T. Durduran, J. Zhang, J. Du, C. Zhou, G. Yu, R. Choe,A. Kilger, R. Lustig, L. Loevner, S. Nioka, B. Chance, and A. G. Yodh,“Noninvasive diffuse optical measurement of blood flow and blood oxy-genation for monitoring radiation therapy in patients with head and necktumors: A pilot study,” J. Biomed. Opt., vol. 11, p. 064021, 2006.
Dominic J. Robinson received the B.Sc. degree inphysics from the University of Manchester, Manch-ester, U.K., in 1992, the M.Sc. degree in medicalphysics in 1994 and the Ph.D. degree from the Uni-versity of Leeds, Leeds, U.K., in 1998.
In 1998, he joined as a Postdoctoral Fellow atthe Daniel den Hoed Cancer Center, Rotterdam, TheNetherlands. He was appointed Assistant Professorin the Department of Radiation Oncology, Center forOptical Diagnostics and Therapy, Erasmus MedicalCenter, Rotterdam, in 2002, where he is currently
leading a range of projects focused on the translational development of pho-todynamic therapy including investigating the use of optical spectroscopy formonitoring photodynamic therapy (PDT) in preclinical models and in clinicalPDT. His Ph.D. thesis was on the use of in vivo optical monitoring photodynamictherapy using fluorescence spectroscopy. His research interests include photo-physical, photochemical, photobiological mechanisms underlying the efficacyof therapy, development of receptor-targeted photosensitizers conjugates forPDT of cancer and autoimmune diseases, and the use of targeted nanomedicinesfor use in PDT and optical diagnostics.
Dr. Robinson is the Editor of the Journal of Photochemistry and Photobiol-ogy B: Biology.

862 IEEE JOURNAL OF SELECTED TOPICS IN QUANTUM ELECTRONICS, VOL. 16, NO. 4, JULY/AUGUST 2010
M. Baris Karakullukcu received the M.D. degree from Istanbul UniversityMedical Faculty, Istanbul, Turkey, in 1998, and received the otolaryngologyspecialty training from Istanbul University Cerrahpasa Medical Faculty, Istan-bul, during 1999 and 2004.
From 2005 to 2007, he was a Fellow of head and neck surgery and mi-crovascular reconstruction with the Jackson Memorial Hospital, University ofMiami, Miami, FL, where he was engaged in the photodynamic treatment ofhead and neck tumors. He joined the Netherlands Cancer Institute, Antoni vanLeeuwenhoek Hospital, Amsterdam, The Netherlands in 2008, where he is cur-rently engaged in the photodynamic therapy of head and neck tumors as a partof a multicenter team contributing from clinical standpoint.
Bastiaan Kruijt received the B.Sc. degree in applied physics (photonics) fromthe Polytechnic University, Rijswijk, The Netherlands, in 2001. Since 2005, hehas been working toward the Ph.D. degree in monitoring photodynamic therapyfrom the Department of Radiation Oncology, Center for Optical Diagnosticsand Therapy, Erasmus Medical Center, Rotterdam, The Netherlands.
From 2002 to 2005, he was engaged in projects on biophotonics at theErasmus Medical Center and at Lund University, Lund, Sweden. At the endof 2005 he started his doctoral l thesis centered on monitoring photodynamictherapy at the Erasmus Medical Center.
Stephen Chad Kanick received the B.S. degree from West Virginia University,Morgantown, in 2002, and the M.S. and Ph.D. degrees from the University ofPittsburgh, Pittsburgh, PA, in 2004 and 2008, respectively, all in chemical engi-neering.
Since 2008, he has been with the Department of Radiation Oncology, Cen-ter for Optical Diagnostics and Therapy, Erasmus Medical Center, Rotterdam,The Netherlands, where he has been currently engaged in developing noveltechniques to improve the accuracy of quantitative reflectance and fluorescencedevices that are utilized for tissue diagnostics and for monitoring of photody-namic therapy. His Ph.D. thesis was focused on the use of elastic scatteringspectroscopic measurements to quantify the pharmacokinetics of optically ac-tive drugs in tissue in vivo.
Robert P. L. van Veen received the B.Sc. degree in applied physics (photonics)from the Polytechnic University, in Rijswijk, The Netherlands, in 1997, and thePh.D degree for his thesis entitled in vivo optical measurements for diagnosticsand monitoring of treatment from Erasmus Medical Center, Rotterdam, TheNetherlands, in 2006.
After completing the B.Sc. degree, he joined the Department of ClinicalPhysics, Daniel den Hoed Cancer Center, Rotterdam, where he was engagedin optimizing in vivo light dosimetry for photodynamic therapy, in vivo tissueoptical properties using spatially resolved diffuse reflectance spectroscopy, anddifferential path length spectroscopy. He is currently with the Department ofRadiation Oncology, Center for Optical Diagnostics and Therapy, ErasmusMedical Center.
Dr. van Veen was awarded the prestigious VENI research grant in 2008,focusing on the development of the 3-D (pre)treatment light dosimetry planningstrategy for interstitial photodynamic therapy for head and neck cancer.
Arjen Amelink received the M.Sc. degree in experimental physics from theUniversity of Groningen, Groningen, The Netherlands, in 1995, and the PhD.Degree in physics from Utrecht University, Utrecht, The Netherlands, in 2000.
His Ph.D. thesis was on the development of atomic traps using laser coolingtechniques and the study of ultracold collisions of sodium atoms. He subse-quently joined Philips Research, Eindhoven, The Netherlands, where he wasa Research Scientist in the Optical Storage group for one year. Since 2001,he has been with the Department of Radiation Oncology, Center for OpticalDiagnostics and Therapy (CODT), Erasmus Medical Center, Rotterdam, TheNetherlands, first as a Postdoctoral Fellow, and since 2005 as an Assistant Pro-fessor. At the CODT, he has been engaged in the technological developmentof optical spectroscopic techniques for biomedical applications, clinical (onco-logic) applications of optical spectroscopy, and noninvasive quantification oftissue compounds in vivo using quantitative reflectance and fluorescence spec-troscopy.
Dr. Amelink is member of the Optical Society of America.
Henricus J. C. M. Sterenborg received the M.Sc. degree in applied physicsfrom the University of Eindhoven, Eindhoven, The Netherlands, in 1982, andthe Ph.D. degree in skin cancer induction by ultraviolet radiation from the Uni-versity Medical Center, Utrecht, The Netherlands, in 1987.
He was a plasma and laser Physicist and switched to the medical field earlyin his career. He was with the Medical Laser Center, University of Amster-dam, Amsterdam, The Netherlands, for 10 years, where he was engaged in thedevelopment of a range of different clinical applications of light. In 1998, hejoined the Daniel den Hoed Cancer Center, Rotterdam, The Netherlands as anAssociate Professor, where he setup the Center for Optical Diagnostics andTherapy, where he was engaged in photodynamic therapy, optical spectroscopy,and imaging for diagnosis of cancer. Since 2008, he is a Professor of photody-namic therapy with the Department of Radiation Oncology, Center for OpticalDiagnostics and Therapy, Erasmus Medical Center, Rotterdam.
Max J. H. Witjes received the D.D.S. degree in dentistry in 1991, the M.D.degree in medicine in 1997, and the Ph.D. degree in medical science in 1997,all from the University of Groningen, Groningen, The Netherlands.
He is currently with the University Medical Center Groningen, Groningen,The Netherlands. Since 1991, he has been engaged in the research on photo-dynamic therapy (PDT) and optical diagnosis. In the field of photodynamictherapy, he investigated the potential for PDT and fluorescence localization of(pre)malignancies of several sensitizers (photofrin, 5-ALA, aluminum phthalo-cyanines, mTHPC, nile blue). This research has lead to the use of Foscan-basedPDT in clinical practice. He initiated several studies investigating the possibil-ity of optical spectroscopy for the detection of (pre)malignancies of the oralmucosa. He was involved in the first time use of Raman spectroscopy in vivo.He also conducted a large study investigating the use of autofluorescence spec-troscopy for detection of early lesions of the oral cavity.
I. Bing Tan received the M.D. degree in medicine from the University of Lei-den, The Netherlands, in 1980, and the Ph.D. degree in medical science fromRoussy, Villejuif, France, in 1986.
He is currently a Senior Staff Member in the Department of Head and NeckOncology and Surgery, Netherlands Cancer Institute, and with the Departmentof Otorhinolaryngology, Academic Medical Centre, both in Amsterdam, TheNetherlands. He was trained as an otorhinolaryngologist at the Free University,Amsterdam by Prof. (Dr.) G. B. Snow. As a Fellow with the Netherlands Can-cer Foundation, he was trained in head and neck surgical oncology at the FreeUniversity, the Netherlands Cancer Institute, and the Institute Gustave Roussy,Paris, France. He is a recognized authority in the field of photodynamic therapyand has a special interest in voice restoration after total laryngectomy. He isalso involved in a collaboration program between the Universities of Jakartaand Yogyakarta, Indonesia and the Netherlands Cancer Institute, which is spon-sored by the Dutch Cancer Foundation and the European Community and hasresulted in an ASIA/Link grant. Since 2007, he has also been appointed as anextra-ordinary Professor with medical faculty of the Gadjah Mada University,Yogyakarta, Indonesia. He is the author or coauthor of 45 papers, 38 of whichcan be traced back through Pubmed and he has presented numerous papers atinternational head and neck conferences, mainly dealing with photodynamictherapy and rehabilitation after total laryngectomy.









![induced photodynamic therapy of deep-seated tumors 5 8 · induced photodynamic therapy of deep-seated tumors 7KLV (OHFWURQLF6XSSOHPHQWDU\0DWHULDO (6, IRU0DWHULDOV+RUL]RQV ... Cr powder](https://img.pdfslide.us/doc/110x75/5e8490377f1f7557440a829a/induced-photodynamic-therapy-of-deep-seated-tumors-5-8-induced-photodynamic-therapy.jpg)















![Ivyspring International Publisher Thheerraannoossttiiccssand photodynamic therapy for resistant head and neck cancers [18]. Despite great promising, most current nanocarriers for chemo-photodynamic](https://img.pdfslide.us/doc/110x75/5f8d3c198976425d76740fa9/ivyspring-international-publisher-thheerraannoossttiiccss-and-photodynamic-therapy.jpg)