Embed Size (px)
Citation preview

3/26/17
1
Understanding elements or characterizing the patient episode of
careJohn Wallace PT OCS
OPTA April 2017
What we will be covering
• Changes in macro healthcare environment• New PT and OT evaluation codes and
reevaluation codes for 2017 and why they are so important
• Characterizing the episode of care• Demonstrating medical necessity• Billable Assessment codes
Healthcare complexities driving changes in payment and payer policies
The healthcare systems affecting physical therapy services have been evolving for some time
– 2007 Medicare, Medicaid, and SCHIPExtension Act of 2007: brought the therapy cap to hospitals and mandated CMS change payment for therapy services to an alternative to the Part B Physician Fee Schedule
– CMS Manual changes requiring to include measureable outcomes in documentation: FOTO, OPTIMAL, etc.
Healthcare complexities driving changes in payment and payer policies
– Value-based payment initiatives: PQRS and Functional Limitation Reporting.
– Affordable Care Act (Obamacare): • Bundling, • MACRA/Mips, • ACOs, • Exponential growth Medicaid and Medicare risk
sharing • Tremendous growth of utilization management for
outpatient therapy claims (OrthoNet, OPTUM, Landmark, etc.)
Why new evaluation and reeval codes
• Current law requires that for the Therapy Cap be abolished and that Medicare payment must be changed from fee for service to an alternative payment system. We have been seeing movement in this direction through FLR and MACRA/Mips
• This has opened the door to treatment based on intervention strategies based on patient severity and complexity of clinical decision making, evidences by new eval codes– Could lead to new intervention codes or even
episodic payment alternatives.
2017 Evaluation Codes for PT
• 3 new levels of evaluation codesLevel chosen is dependent on: • Complexity of clinical decision making
and • Severity of the patient’s condition
Together, these 2 elements determine the level of service: low, moderate or high complexity.
3/26/17
2
2017 Evaluation Codes for PT
• Evaluation– 97161 Low Complexity Evaluation– 97162 Moderate Complexity Evaluation– 97163 High Complexity Evaluation
• Re-evaluation– 97164 A single code
CMS RVU Decision for 2017
• Work values for the PT and OT Evaluation codes will be unchanged from the values for 97001 and 97003.
• The work values for the reeval codes 97002 and 97004 are up marginally.
• CMS wants to allow a year of data collection and for providers to get training and learn to use the codes accurately.
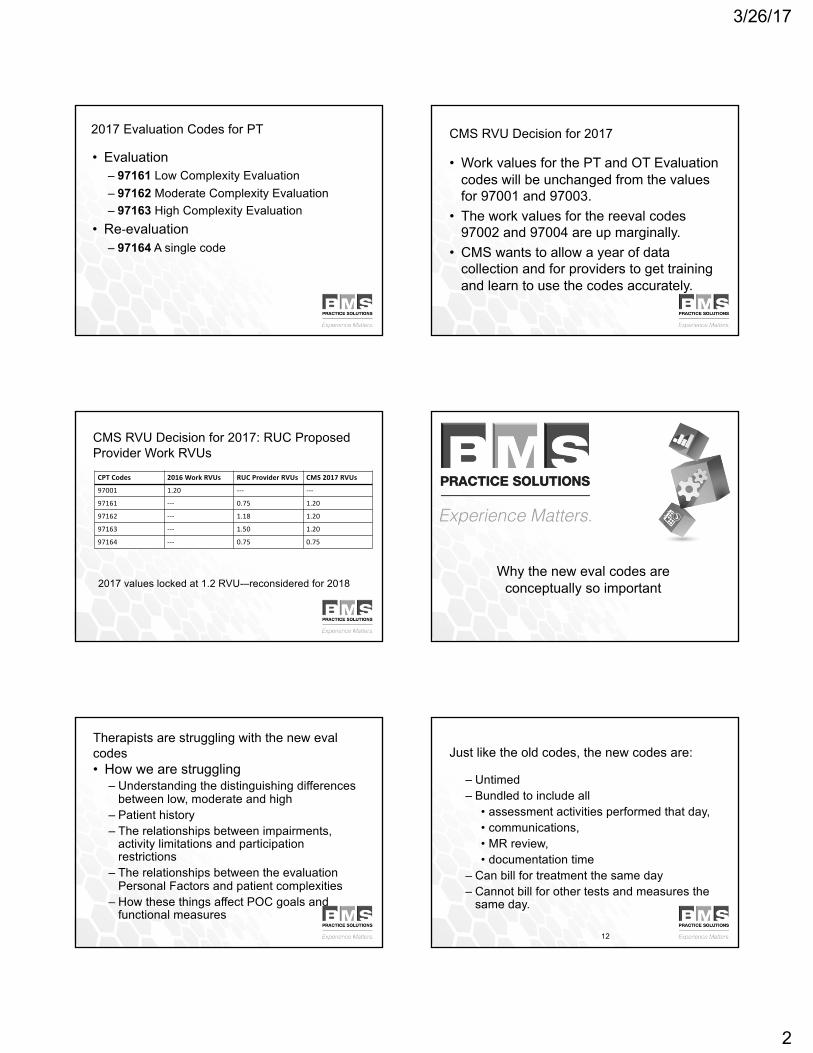
CMS RVU Decision for 2017: RUC Proposed Provider Work RVUs
2017 values locked at 1.2 RVU-–reconsidered for 2018
CPTCodes 2016WorkRVUs RUCProviderRVUs CMS 2017RVUs
97001 1.20 --- ---
97161 --- 0.75 1.20
97162 --- 1.18 1.20
97163 --- 1.50 1.20
97164 --- 0.75 0.75
Why the new eval codes are conceptually so important
Therapists are struggling with the new evalcodes• How we are struggling
– Understanding the distinguishing differences between low, moderate and high
– Patient history– The relationships between impairments,
activity limitations and participation restrictions
– The relationships between the evaluation Personal Factors and patient complexities
– How these things affect POC goals and functional measures
12
Just like the old codes, the new codes are:
– Untimed– Bundled to include all
• assessment activities performed that day, • communications, • MR review, • documentation time
– Can bill for treatment the same day– Cannot bill for other tests and measures the
same day.
3/26/17
3
PT Evaluation Codes Include
• Patient history• Examination with development of a plan of
care (POC)• Includes coordination, consultation, and
collaboration of care with physicians and other healthcare professionals or agencies
PT Evaluation minimum required elements
Each of the following components from the code descriptors must be documented:• History• Examination• Clinical decision making• Development of POC
PT Examination Definitions
• Body regions and body systems are defined as follows:– Body region: head, neck, back, lower
extremities, upper extremities, and trunk– Body systems: musculoskeletal,
neuromuscular, cardiovascular, and integumentary
– Review of body systems include see following slides:
PT Examination Definitions
Review of body systems include :– Musculoskeletal: assessment of gross anatomy,
gross ROM, gross strength, height and weight– Neuromuscular: general assessment of gross
coordinated movement (e.g. balance, gait, locomotion, transfers, and transitions) and motor function (motor control and motor learning)
– Cardiovascular/Pulmonary: assessment of heart rate, resp. rate, blood pressure, and edemacontinued
PT Examination Definitions
Review of body systems include : cont’d.– Integumentary: the assessment of pliability
(texture), presence of scar formation, skin color, and skin integrity
– A review of the body system also includes the assessment of the ability to make needs known, consciousness, orientation (PP&T), expected emotional/behavioral responses, and ability to learn.
PT Examination Definitions
Review of body systems include: cont’d.– Body structures: the structural or anatomical
parts of the body, such as organs, limbs, and their components, classified according to systems. [Impairments]
– Personal factors: Factors that include age, coping styles, social background, education, profession, past and current experiences overall behavior pattern, character, and other factors that influence how disability is experienced by the individual. [Complexities]

3/26/17
4
PT Examination Definitions
• Complexities: secondary diagnoses and other complicating factors that may influence treatment e.g. may influence the type, frequency, intensity, &/or duration of treatment.
Represented by:• diagnoses as comorbidities • patient factors such as age, severity, acuity, multiple
conditions, and motivation, or by social circumstances such as the support of significant other or the availability of transportation to therapy
Elements of a PT Evaluation (from the Guide)
• Examination (includes history, systems review, and tests and measures)
• Evaluation (the thought process leading to identifying impairments, functional limitations, disabilities, and needs for prevention)
• Diagnosis (impact of the condition on function)• Prognosis (professional judgment regarding
the predicted functional outcome and the estimated duration of services required)
• Plan of Care (the culmination of an evaluation)
PT Eval Codes: 4 components of severity and complexity
1. Patient history: medical and functional, including relevant complexities
2. Examination: impairments including standardized tests and measures
3. Clinical presentation of the patient: stable, changing, or unstable
4. Clinical decision making: use of standardized patient assessment instrument and/or measurable assessment of function
Patient History
• Comorbidities, medical hx & meds that impact function or otherwise impact POC
• Prior functional level and context of current functional abilities
• Past treatment, if appropriate, and other factors that may impact ability to reach goals
• Social history, living environment, work status, cultural factors
CLINICAL PRESENTATION
Is the patient• Stable and uncomplicated, or• Evolving clinically with predictable
changing clinical characteristics, or• Evolving clinical presentation with
unstable or worsening and unpredictable characteristics
The next step…
• Thinking like a reviewer...• How ICF can connect the dots between
impairments, personal factors, and complexities in characterizing complexity of clinical decision making
3/26/17
5
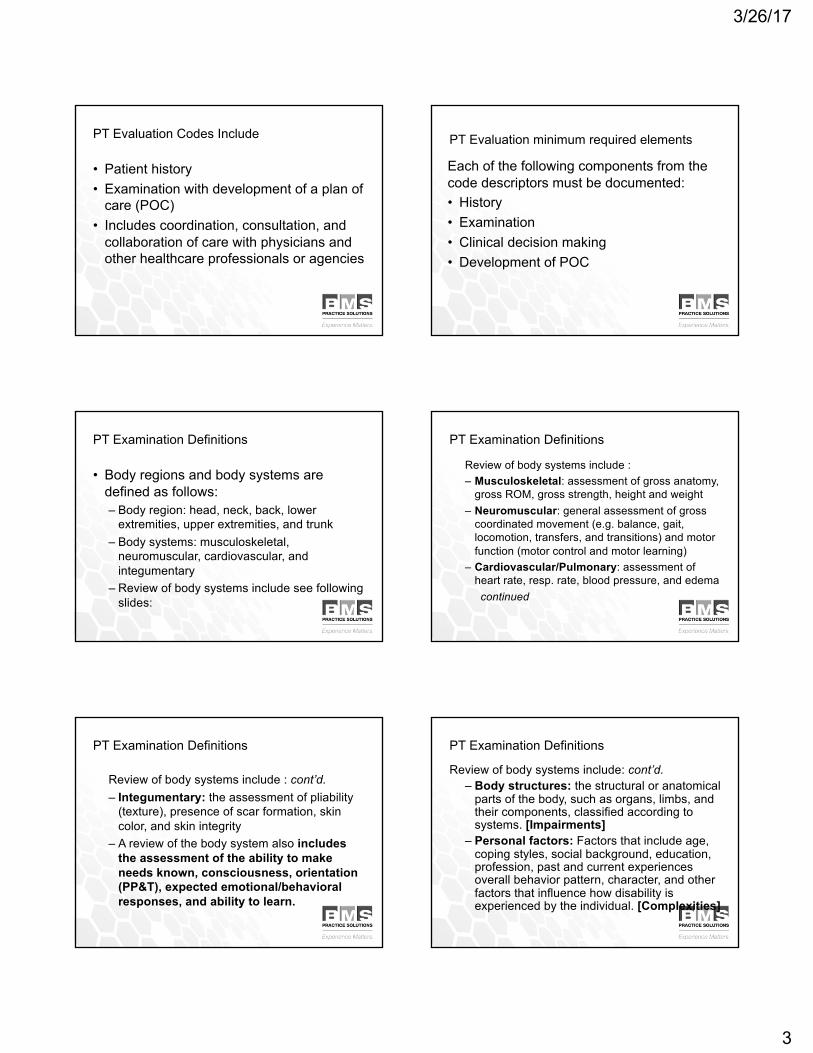
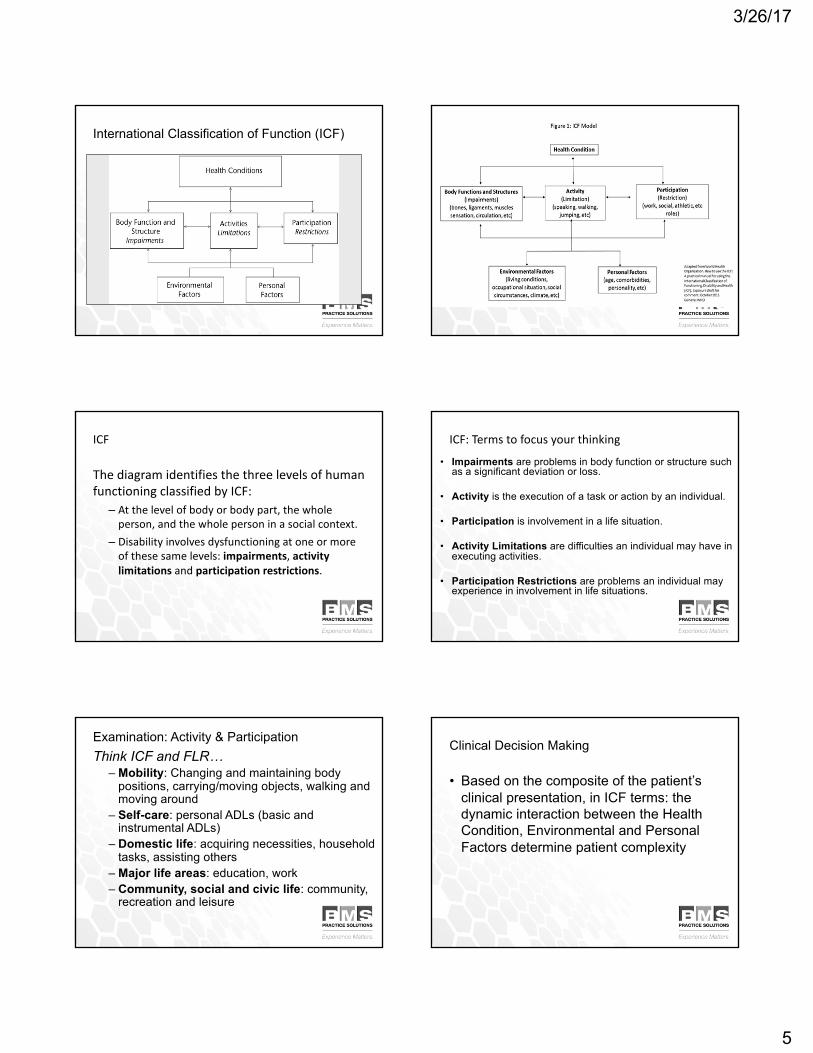
International Classification of Function (ICF)
ICF
ThediagramidentifiesthethreelevelsofhumanfunctioningclassifiedbyICF:
– Atthelevelofbodyorbodypart,thewholeperson,andthewholepersoninasocialcontext.
– Disabilityinvolvesdysfunctioningatoneormoreofthesesamelevels:impairments,activitylimitations andparticipationrestrictions.
ICF:Termstofocusyourthinking
• Impairments are problems in body function or structure such as a significant deviation or loss.
• Activity is the execution of a task or action by an individual.
• Participation is involvement in a life situation.
• Activity Limitations are difficulties an individual may have in executing activities.
• Participation Restrictions are problems an individual may experience in involvement in life situations.
Examination: Activity & ParticipationThink ICF and FLR…
– Mobility: Changing and maintaining body positions, carrying/moving objects, walking and moving around
– Self-care: personal ADLs (basic and instrumental ADLs)
– Domestic life: acquiring necessities, household tasks, assisting others
– Major life areas: education, work– Community, social and civic life: community,
recreation and leisure
Clinical Decision Making
• Based on the composite of the patient’s clinical presentation, in ICF terms: the dynamic interaction between the Health Condition, Environmental and Personal Factors determine patient complexity
3/26/17
6
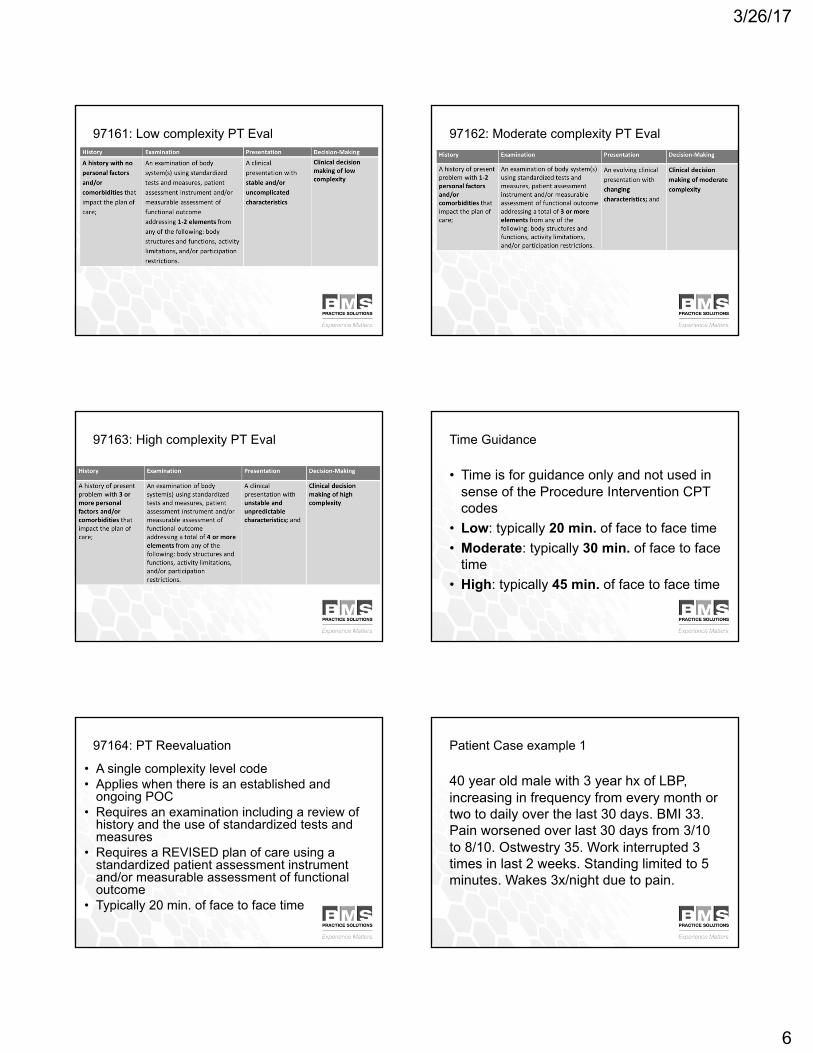
97161: Low complexity PT Eval 97162: Moderate complexity PT Eval
97163: High complexity PT Eval Time Guidance
• Time is for guidance only and not used in sense of the Procedure Intervention CPT codes
• Low: typically 20 min. of face to face time• Moderate: typically 30 min. of face to face
time• High: typically 45 min. of face to face time
97164: PT Reevaluation
• A single complexity level code• Applies when there is an established and
ongoing POC• Requires an examination including a review of
history and the use of standardized tests and measures
• Requires a REVISED plan of care using a standardized patient assessment instrument and/or measurable assessment of functional outcome
• Typically 20 min. of face to face time
Patient Case example 1
40 year old male with 3 year hx of LBP, increasing in frequency from every month or two to daily over the last 30 days. BMI 33. Pain worsened over last 30 days from 3/10 to 8/10. Ostwestry 35. Work interrupted 3 times in last 2 weeks. Standing limited to 5 minutes. Wakes 3x/night due to pain.

3/26/17
7
Patient Case example 1
1. History: +BMI for overweight, pain frequency/intensity increasing
2. Examination: Work interuption, standing time, sleep interrupted, trunk exam
3. Presentation: Evolving clinical presentation4. Time: 35 min face-to-face time5. Clinical decision making: Moderate97612
Patient case example 2
• 67 y/o male with 6 month history of neck pain with pain and stiffness of rt. Shoulder. Pain decreasing over last month but stiffness increasing. + MRI C5-C6 Disc, Poorly controlled DM, BMI 35, hx of COPD. Limited self care, can’t carry objects with rt arm, can’t do yard work or vacuum. Neck Pain and Disability Index 25/50 (border line severe). DASH 69.2
Patient case example 2
1. History: + MRI, BMI, COPD, DM,2. Examination: Home ADLs affected, carry
objects impacted, NPDI, DASH, Neck, UE3. Presentation: unstable clinical
consideration/worsening symptoms4. Time: 50 min. f-t-f time5. Clinical decision making: High97163
What payers want to know
Healthcare stakeholders want to know 4 things:1. What did you do?2. Why did you do it?3. How is it helping and how do you know?4. How much more or longer do you need to
do it?These must be specific to each patient
Documentation systems can help you or hurt you…• Can help
– Force required elements, document types and track and sort
• Cannot help – Provide patient specific insights and analysis– Demonstrate skilled care without proper input– Forecast outcomes and identify clinical exceptions– Explain outlier resultsOnly therapists can make and document these judgments
The essential problems
• The notes are legible• Without purposeful activity, therapists can write
nearly identical notes for a patent or multiple patients via the use of pick lists and templates
• Therapist over rely on the EMR to make the case for skilled care by relying on volumes of impairment data and the completion of required document types rather than considering the elements of skilled care specific to the patient.

3/26/17
8
The essential problems
• Therapists are be obsessed with templates and “pre-loaded” pages that can apply to all patients with a particular diagnosis or problem to decrease time required to create the medical record
• The combination of non-patient specific aids can create notes that do not adequately support skilled care based on individual patient needs
Understanding the basics of establishing Medical Necessity
You can’t outsource this to software developers
Establishing Medical Necessity and Skilled care
• Medicare has strict but well defined definitions of Medical necessity:– Reasonable and Necessary– Skilled care
• Rehabilitative care• Maintenance care
• These must be addressed individually for each patient
Requirements for care
• Patient must be under the care of a physician (an order is not required)
• A Plan of Care (POC) must be established by the therapist
• POC must be signed by the Physician within first 30 days
• POC must be recertified after 90 days, or sooner if POC duration was written for <90 days
Reasonable and Necessary
• The services shall be considered under accepted standards of medical practice to be a specific and effective treatment for the patient’s condition. As evidenced by– Medicare Manuals 100-03 and 100-04– Contractors LCDs and CMS LCDs– Guidelines and literature of rehab professions:
APTA.org and PTNow.org
Reasonable and Necessary
• The services shall be of such a level of complexity and sophistication or the condition of the patient shall be such that the services required can be safely and effectively performed only by a therapist, or in the case of physical therapy and occupational therapy, by and under the supervision of a therapist.

3/26/17
9
Reasonably and Necessary
• Services that do not require the performance or supervision of a therapist are not skilled and are not considered reasonable or necessary therapy services, even if they are performed or supervised by a qualified professional.
Reasonably and Necessary
• While a beneficiary’s particular medical condition is a valid factor in deciding if skilled therapy services are needed, a beneficiary’s diagnosis or prognosis cannot be the sole factor in deciding that a service is or is not skilled. The key issue is whether the skills of a therapist are needed to treat the illness or injury, or whether the services can be carried out by nonskilled personnel.
Rehabilitative Therapy
• Services designed to address recovery or improvement in function or restoration to a previous level of health and well-being.
• Evaluation, re- evaluation and assessment documented in the Progress Report should describe objective measurements which, when compared, show improvements in function, decrease in severity or rationalization for an optimistic outlook to justify continued treatment.
Rehabilitative Therapy
• Rehabilitative therapy requires the skills of a therapist to safely and effectively furnish a recognized therapy service whose goal is improvement of an impairment or functional limitation.
• Services that can be safely and effectively furnished by nonskilled personnel or by PTA without supervision are not rehabilitative therapy
Maintenance Programs
• Skilled therapy services that do not meet the criteria for rehabilitative therapy may be covered in certain circumstances as maintenance therapy under a maintenance program.
• The goals of a maintenance program would be, for example, to maintain functional status or to prevent or slow further deterioration in function.
Maintenance Programs
Skilled therapy services related to a reasonable and necessary maintenanceprogram are covered in the following circumstances:• Establish or design a program to maintain the
current condition or to prevent or slow further decline
• Also covers periodic reevaluations or reassessments

3/26/17
10
Maintenance Programs
• Skilled therapy services are covered when an individualized assessment of the patient’s clinical condition demonstrates that the specialized judgment, knowledge, and skills of a qualified therapist are necessary for the performance of safe and effective services in a maintenance program.
Maintenance Programs
• Such skilled care is necessary for the performance of a safe and effective maintenance program only when (a): – the therapy procedures are required to
maintain the patient’s current function or – to prevent or slow further deterioration– and are of such complexity and sophistication
that the skills of a qualified therapist are required to furnish the therapy procedure;
Maintenance Programs
• Such skilled care is necessary for the performance of a safe and effective maintenance program only when (b):– the particular patient’s special medical
complications require the skills of a qualified therapist to furnish a therapy service required to maintain the patient’s current function or
– to prevent or slow further deterioration, even if the skills of a therapist are not ordinarily needed to perform such therapy procedures.
Maintenance Programs
• The deciding factors are always whether the services are – considered reasonable, effective treatments
for the patient’s condition and require the skills of a therapist, or
– whether they can be safely and effectively carried out by nonskilled personnel or caregivers.
Maintenance Programs
• Objective measures and tests in the form of valid and reliable functional tests and patient surveys are essential to making the case for the effectiveness of skilled care in the provision of maintenance programs.– This has been an essential element of
Medicare’s documentation requirements since 2007 but most therapists did not comply
– The result: increased RAC activity and the FLR program
Medicare Documentation Requirements• Evaluations
– Results of one of the following four measurement instruments are recommended but not required:• OPTIMAL (APTA tool available on APTA
web site to members who can also request permission to use for free)
• Patient Inquiry by FOTO• Activity Measure—Post Acute Care
(AM-PAC)

3/26/17
11
Medicare Documentation Requirements
– If one of the measurement tools on previous slide is not used, the following documentation is required to indicate objective, measurable patient physical function including:1. Functional assessment individual item and
summary scores from commercially available therapy instruments including comparisons from sequential use over the episode of care
Medicare Documentation Requirements
2. Functional assessment scores from tests and measures validated in the professional literature including comparisons to prior assessments
3. Other measurable progress towards identifiable goals for function during the episode of care and at the conclusion of therapy.
Required documents in the Medicare program
• Evaluation and POC • Certification and re-certification (if
indicated)• Progress Reports and D/C Progress
Reports – may be included in Treatment Notes if required elements are included
• Treatment Notes for each treatment day• Optional Therapy Cap Justification
Statement
Elements of critical decision making
The therapist needs to consider the following factors:
– The effect of treatment on the patient’s primary condition
– The patient’s complexities: comorbidities in the form of other current (non-PT) conditions, preexisting conditions, and social situation
– The status of the patient’s comorbidities and primary condition on ability to function
Elements of critical decision making for maintenance therapy
– The probability that changes in function will result in increased impairments, more activity/participation restrictions restrictions if therapy is stopped
– The ability of the patient with the help of unskilled assistance, to manage a program to maintain function.
– Whether the skills of a therapist are necessary for the patient to carry out the program.
Elements of critical decision making
Documenting clinical reasoning is evidenced through consideration of1. Analysis of scores of functional assessment2. Objective data on impairments like pain,
strength, ROM, balance etc.3. Impact of comorbidities and
social/environmental factors on the patient’s function and ability to participate

3/26/17
12
Documentation strategy
Capturing clinical insight and analysis:• The difficulties:
– What to write– How to say it– Preserving the patient-specific nature– Helping the reviewer draw the same clinical
conclusions based on what you report about your assessment and clinical reasoning
PatellofemoralPainExample
• Pick the right measure: one that’s valid in your patient population….– LEFS– Initial visit score: 52/80– After 3 weeks (7 visits): 72/80
See PTNOW.org for suggestions of measures valid in your patient population
ICF: Terms to focus your thinking
Your primary objectives in documentation:• Identify patient specific impairments• Link these impairments to patient specific
problems in the evaluation process• Demonstrate the effect on function by
identifying Activity Limitations and Participation Restrictions
• Measure these with OTMs and demonstrate progress or maintenance of function

3/26/17
13
Evaluation: Essential questions
• Reason for the referral?• Has there been a change in activity level
or medical condition (especially if condition is chronic)?
• Identified the impairments and resulting activity limitations and participation restrictions?
• Is baseline functional status objectively measured?
Evaluation: Essential questions
• Changes in the patient’s condition– Is is getting better or worse?– Given the primary pathology/impairments, is
the presentation: • Stable and uncomplicated?• Evolving and changing in an expected and
predicable manners?• Unstable and evolving in unexpected and
unpredictable ways?
Documentation Information to Meet Medicare Requirements
• Evaluation, Re-evaluation, and Plan of Care– Evaluation or Eval including the POC should
document the necessity for a course of therapy through objective findings and subjective patient self-reporting.
– Can be done only by a therapist– May include objective measurements or
observations made by assistants within their scope of practice but clinical assessment and judgment is the responsibility of the therapist.
– Should include a list of conditions and complexities, and, when not obvious, describe their impact on the prognosis and plan for treatment.
Documentation Information to Meet Medicare Requirements• Evaluation continued
– Include the body part and all conditions and complexities that may impact treatment
– Complexities may include:• Comorbidities• Premorbid functional levels• Date of onset• Current functional levels• Functional Limitation G-codes and
modifiers required
Diagnosis
Represents a label that identifies the impact of a condition and complexities on the patients ability to function • At the movement system level• At the whole person levelThese affect activities and participation and quality of life and should lead naturally to patient problems
Documentation Information to Meet Medicare RequirementsPlan of Care should contain:
– Summary of patient problems, prior level of function, and pertinent medical history
– Diagnosis(s) that require physical therapy– Therapeutic interventions to be used– Frequency of treatment (“tapering” is allowed)– Duration of treatment in weeks– Long term treatment goals (these must be specific
and measurable)– Functional Limitation G-codes and modifiers required– Must be signed and dated by therapist and
physician

3/26/17
14
Required elements: POC
• Patient specific problem list: Activity focused, not impairment focused
• Goals that are functional, measureable, and indicate predicted levels of improvement
• Interventions to achieve the goals• Duration and frequency (not hyphenated)• Anticipated discharge plan
POCRecord clinical reasoning to connect the dots from/to:
– Impairments identified in the evaluation – interventions that address the impairments– Activity limitations/Participation Restrictions
caused by the impairments ( = decreased function)
– Measure the current level of function– Design goals that address the activity
limitations/participation restrictions that can be measured with OTMs
POC Goals• Goals are not impairment based• They are measureable by re-evaluation or
assessment use of OTMs• Related to activity limitations and
participation restrictions identified• Include anticipated timeframes for
achievement• State in functional terms specific to the
patient
POC Goals
• Relatedtotheoutcomeoftheepisodenotthecertificationperiod
• Patientfocused• Identifytheskilledactivitiesorinterventionsneededtoachievethegoals
• Eachgoalshouldbetiedtoaspecificproblem• Eachgoalshouldhavemeasureablefunction• Howwillitimprovequalityoflife
Goal examples
• Improve ROM to WNL and strength to 4/5 in 2 weeks
• Improved balance so patient can do ADLs independently in 2 weeks
• UE functional improvement as evidence by change in Dash Score from 50 to 35 in 2 weeks
• Improve standing balance with TUG changing from 20 sec to 12 sec in 2 weeks
Prognosis
• The prognosis is the determination of the predicted optimal level of improvement in function reflected in the goals and
• the amount of time needed to reach that level, and
• may include a prediction of levels of improvement that may be reached at various intervals during the course of therapy. Guide to Physical Therapist Practice

3/26/17
15
Prognosis
• prognosis conveys the physical therapist’s professional judgment for– the patient’s/client’s predicted functional
outcome and – the required duration of services to obtain
this functional outcome.
Prognosis
• It is important to differentiate between the patient’s/client’s medical prognosis and his/her rehabilitation prognosis.
• It is important to consider the prognosis for the entire episode of care and not just one specific timeframe
• Document your clinical reasoning reflecting these points
Treatment Notes
• Need to demonstrate only a therapist could perform or supervise (if a PTA was used) the interventions/treatment
• Must reflect skilled knowledge of movement and function
• Needs to be more than a list of interventions, tasks or exercises
Treatment Notes
• Intervention “dosage” must be included– The techniques, the reps, the time, the way
you measure the intervention– Reviewers should be able to get a real sense
of what you did and how much time it took to deliver the treatment
– This includes assessment and management activities
– Showing progression is essential to demonstrating skilled care
Treatment Notes
Flow Sheets: • Provider of care must be clearly identified,• Provider must demonstrate skilled care was
delivered: • NEVERUSECHECKMARKSwithoutdosinginfo!• Recordexercise/activitydosing• Dropexercisesoffwhenskilledcarenolongernecessaryandreplacewithmorecomplex/higherlevelactivities—avoidrepetitiveexercisesthatare“unskilled”
Treatment Notes
• While it is important to include the interventions provided in a way that allows a reviewer to tie to the CPT codes billed, this does not demonstrate skilled care
• Evidence skilled care by documenting what you observe before, during and after an intervention and the patient’s specific response to the intervention.

3/26/17
16
Treatment Notes
• Must document progression of care– Changes in intervention dosage to reflect
progress or challenges in reaching treatment goals
– Response to treatment that reflects ongoing resolution of impairments resulting in progress toward POC goals and resolution of patient problems
– In maintenance treatment, demonstrate that treatment is maintaining functional status
– If noted in detail, may obviate need for Progress Reports
Treatment Notes
• Providers are required to support the reporting of timed procedure and modality codes in their clinical documentation.– Medicare requires that the total time attributable
to timed codes be recorded each visit– Medicare does not require time to be attributed to
each CPT code– Some payers do– In all cases, times attributed should include all
assessment and management time
Progress Reports
• Should provide an update on the patient’s status as it relates to the POC.
• Include detailed information on the patient’s current status as compared to previous treatment notes and reference any reevaluation, reexamination, or or previous progress reports
Medicare Documentation RequirementsProgress Report:• Is a periodic summary of patient progress• Information must be provided every 10 visits• Absences due to illness or holidays do not affect
the requirement for Progress Reports.• If delayed it must be completed within 7 days or
the end of the reporting period and should explain the reason for the delay.
• Functional Limitation G-codes and modifiers required
Medicare Documentation RequirementsProgress Report• Discharge Progress report required for each
episode– Covers the last reporting period up to the
discharge date– Functional Limitation G-codes and modifiers
required– If discharge is unanticipated, the therapist may
base judgment on the Treatment Notes and other available documentation or verbal reports.
– Does not have to be “certified” or signed by the physician.
Medicare Documentation RequirementsContents of Progress Report
• Assessment of improvement, extent of progress (or lack thereof) toward each goal
• Reference to any re-evaluation data• Plans for continuing treatment• Changes to goals (would trigger new POC) and
Functional Limitation G-codes and modifiers required
• discharge plans• Re-evaluation should not be required before
every Progress Note but may be appropriate when assessment indicates changes not anticipated in the current POC

3/26/17
17
Medicare Documentation RequirementsProgress Report
– The report must justify necessity of services. Justification must include objective evidence or a clinically supportable statement of expectation that:
• The patient’s condition has the potential to improve or is improving with therapy
• Maximum improvement is not yet attained• There is an expectation that anticipated improvement
is attainable in a reasonable period of time– Must contain objective evidence of standardized
patient assessment instruments, outcome measurement tools or measurable assessments of functional outcomes.
Discharge Progress Report
• Discharge report documents the extent of the patient’s achievement of the predicted goals and expected outcomes for the episode of care.
• It should also summarize the patient’s progress since the last Progress Report
• It can only be documented by a therapist– Measurement completed by PTAs within their
scope are permitted
Discharge Progress Report
• The report should include:– attainment of goals and goals that have not been
attained substantiated by functional OTMs– recommendations and instructions that were
provided to the to the patient/client, such as home program, equipment provided, and
– Any patient or caregiver training, instruction, counsel and advice.
– a patient/client is discharged to another healthcare provider evidence of coordination of care should also be included.
Discharge Progress Report
• A discharge summary should comment if the patient stops coming to therapy against recommendation of the therapist.
• If the patient is discharged prior to achievement of forecasted goals and outcomes, document the status of the patient and the reason for discontinuation.
Correcting and clarifying the record
• Most EMRs have “addendum” functionality• Often underused to clarify the medical
record– Bad habit from the paper record days
• Use to – Correct documentation mistakes– Clarify previous notations in the record– Additional justification in the record of
therapist decisions regarding treatment, discharge, etc.
Correcting and clarifying the record
Addendums• Dated chronologically in real time • They refer to a previous therapy visit or
date of an interaction or observation about the patient
• Can be used to fine-tune the record if, on review, the therapist believes that documentation of clinical decision making is not clear.

3/26/17
18
Proper use of Assessment CPT Codes
Evaluation and Assessment
– Definitions:Assessment is separate from evaluation/re-evaluation• Evaluation is a separately billable service• Assessment is a component of each billable
intervention/treatment and not separately billable
• Both are Provided only by clinicians (therapists)
• There are billable assessment interventions that can be separately billable.
Evaluation and Assessment Rules
• Only one evaluative code CAN be used per a day, per discipline
• Billable assessment codes and evaluative codes CANNOT be used on the same day
• Multiple billable assessment codes CANusually be billed the same day
• You CAN charge for evaluation + treatment or billable assessments + treatment the same day
Therapeutic Procedures97750 Physical performance test or
measurement (e.g., musculoskeletal, functional capacity) with written report,
each 15 minutes• Use for testing required for FLR• Assessment tests separate and distinct from evaluative
procedures and ROM /MMT activities• Examples: isokinetic/isometric tests, Berg Balance Test,
Tinetti’s Test, Semms-Weinstein test, Volumetric testing, Denver Dev Screening, Outcomes Tests and Measures: Oswestry, Lysholm Knee Score
• Require separate report• Do not bill same day as eval or re-eval
Manual Muscle Testing Codes95831 Muscle testing, manual, with report;
extremity (excluding hand) or trunk95832 hand, with or w/o comparison 95833 total evaluation body, excl. hands95834 total evaluation of body, incl. hands• Must report on each code in its entirety: extremity
means each muscle of functional group in that extremity
• Can bill multiple codes for left and right extremities• Need to report in the medical record
ROM Testing Codes
95851 ROM measurements and reports; each extremity (excl. hands) or eachtrunk section (spine)
95852 hand, with or w/o comparison• Must report on each code in its entirety:
extremity means each muscle of functional group in that extremity and for multiple spinal regions
• Can bill multiple codes for left and right extremities
• Need to report in the medical record
3/26/17
19
MMT and ROM codes
• Do not bill same day as evaluative procedures
• Can use only ROM or MMT• Can bill with treatment• Can bill with one or the other with 97750• Require detailed reporting within a daily
note or as a separate report
For more information...
• John Wallace, PT, OCS 800 [email protected]
110