Embed Size (px)
Citation preview
From Coke to Pepsi or a cocktail? Rotating and adding opioids in advanced pediatric pain medicineStefan J. Friedrichsdorf, MD, FAAPAssociate Professor of Pediatrics, University of Minnesota Medical SchoolMedical Director, Department of Pain Medicine, Palliative Care & Integrative Medicine, Children's Hospitals and Clinics of Minnesota, Minneapolis/St. Paul, MN
Simon A. Cohen, BSc MBChB MRCPCH (UK) FRACP FFPMANZCAPaediatric Pain Consultant, Monash Children’s Hospital, MelbourneChief Medical Officer, Very Special Kid’s hospice, Melbourne
[email protected] Twitter: @NoNeedlessPain
Learning Objectives
• Case Example [“hook”]
• Discuss indications for and misconceptions about opioid conversion [“attitude”]
• Review cross-tolerance and rationale for opioid rotation and combining Opioids [“knowledge”]
• Practice examples for opioid conversion [“skill”]
Case Example
• Andrea is a 10-year-old girl in severe acute pain (VAS 8/10) due to metastasized osteosarcoma; weight: 20 kgs
• Andrea has been started on morphine 3 days ago - now the nurse calls you that she is poorly arousable, respiratory rate 9/min, oxygen saturation 82% when eyes closed
• What might be your next questions & steps?
• Over sedation => good analgesia?
• Over sedation => poor analgesia?
Management of Opioid Adverse Effect “Over Sedation”
• Dose reduction
• If good analgesia
• Opioid rotation
• If poor analgesia and/or medium-severe side effects
• Adverse effect targeted therapy
• If mild side effects or opioid rotation not possible
• What arguments might you hear from parents, patients or colleagues/care team NOT to rotate the opioid?
Analgesic Response
• Patients differ in their response to opioid analgesics
• Even in well designed, successful clinical trials, as much as 40% of patients do not respond well to analgesic being studied Argoff CE, Yanni LM. Pharmacogenetics and pain. Prim Care Q 2010;1-8
• Unsurprising, patients may require trials of several opioids to find effective analgesia with acceptable tolerability
μ-Receptor Subtypes• Individuals display variety of
combinations of different mu-receptor subtypes
• Generated through “alternative splicing”, known to enhance protein diversity
• Binding profiles & resulting pharmacologic effects of opioid receptor subtypes vary among μ-opioids
• Contributing to individual variance in therapeutic response & incomplete cross-tolerance
• Review Brennan MJ. The clinical implications of cytochrome p450 interactions with opioids and strategies for pain management. Journal of Pain and Symptom Management. 2012 Dec;44(6 Suppl):S15-22.
dimer of μ receptors. Credit: Kobilka lab
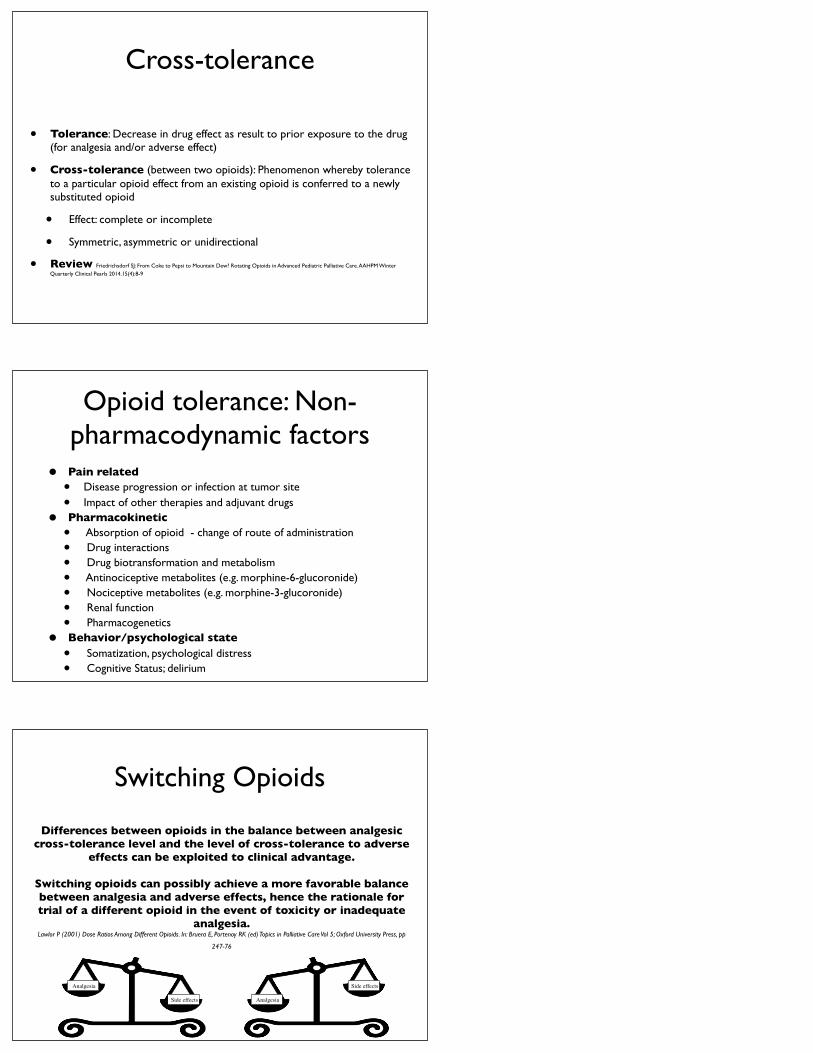
Cross-tolerance
• Tolerance: Decrease in drug effect as result to prior exposure to the drug (for analgesia and/or adverse effect)
• Cross-tolerance (between two opioids): Phenomenon whereby tolerance to a particular opioid effect from an existing opioid is conferred to a newly substituted opioid
• Effect: complete or incomplete
• Symmetric, asymmetric or unidirectional
• Review Friedrichsdorf SJ: From Coke to Pepsi to Mountain Dew? Rotating Opioids in Advanced Pediatric Palliative Care. AAHPM Winter Quarterly Clinical Pearls 2014.15(4):8-9
Opioid tolerance: Non-pharmacodynamic factors
• Pain related • Disease progression or infection at tumor site
• Impact of other therapies and adjuvant drugs
• Pharmacokinetic• Absorption of opioid - change of route of administration
• Drug interactions
• Drug biotransformation and metabolism
• Antinociceptive metabolites (e.g. morphine-6-glucoronide)
• Nociceptive metabolites (e.g. morphine-3-glucoronide)
• Renal function
• Pharmacogenetics
• Behavior/psychological state• Somatization, psychological distress
• Cognitive Status; delirium
Switching Opioids
Differences between opioids in the balance between analgesic cross-tolerance level and the level of cross-tolerance to adverse
effects can be exploited to clinical advantage.
Switching opioids can possibly achieve a more favorable balance between analgesia and adverse effects, hence the rationale for trial of a different opioid in the event of toxicity or inadequate
analgesia.Lawlor P (2001) Dose Ratios Among Different Opioids. In: Bruera E, Portenoy RK (ed) Topics in Palliative Care Vol 5; Oxford University Press, pp
247-76
Analgesia
Side effects Analgesia
Side effects
Adding and Mixing Opioids
Perceived Efficacy of Analgesic Drug Regimens Used for Koalas (Phascolarctos
cinereus) in AustraliaDe Kauwe T, Kimble B, Govendir M
Journal of Zoo and Wildlife Medicine 2014 Jun;45(2):350-6.
‘Analgesic drug combinations were generally thought efficacious‘
7
8
Morphine
63
O
N
HO OH
CH3
Methadone
C CH2 CH
CH3
NCCH3
CH3
CH3CH2
O
CH2CH2N
CH3CH2CN
O
Fentanyl
63
Heroin
N
O OCCH3
CH3
CH3CO
OO
Morphine 6-Glucuronide
O
N
HO O
CH3
COOH
OHOHHO
O
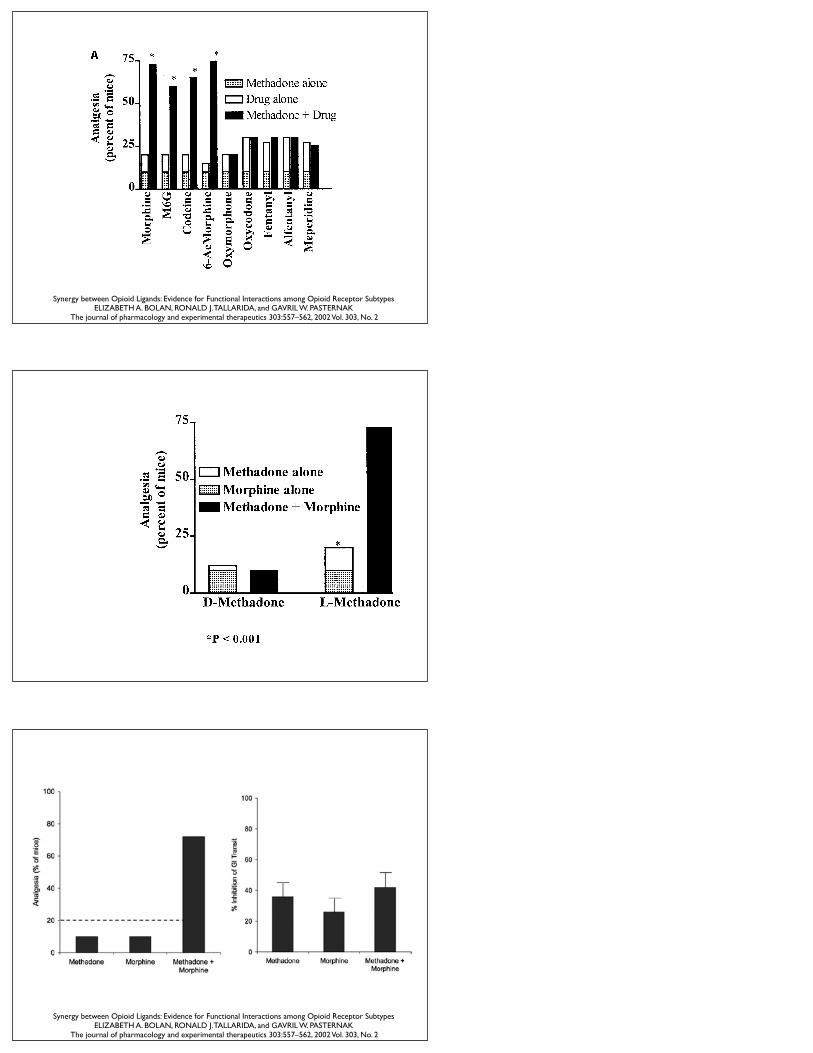
Synergy between Opioid Ligands: Evidence for Functional Interactions among Opioid Receptor Subtypes ELIZABETH A. BOLAN, RONALD J. TALLARIDA, and GAVRIL W. PASTERNAK
The journal of pharmacology and experimental therapeutics 303:557–562, 2002 Vol. 303, No. 2
Synergy between Opioid Ligands: Evidence for Functional Interactions among Opioid Receptor Subtypes ELIZABETH A. BOLAN, RONALD J. TALLARIDA, and GAVRIL W. PASTERNAK
The journal of pharmacology and experimental therapeutics 303:557–562, 2002 Vol. 303, No. 2
Comparison of sustained-release morphine with sustained-releaseoxycodone in advanced cancer patients
British Journal of Cancer (2003) 89, 2027 – 2030
& 2003 Cancer Research UK All rights reserved 0007 – 0920/03 $25.00
www.bjcancer.com
Support Care Cancer (2004) 12:762–766DOI 10.1007/s00520-004-0650-1 O R I G I NA L ART I C L E
Sebastiano MercadantePatrizia VillariPatrizia FerreraAlessandra Casuccio
Addition of a second opioidmay improve opioid response in cancer pain:preliminary data
Analgesic Efficacy and Tolerability of Intravenous MorphineVersus Combined Intravenous Morphine and Oxycodone in a2-Center, Randomized, Double-Blind, Pilot Trial of PatientsWith Moderate to Severe Pain After Total Hip Replacement
Robin Joppich, MD1,*; Patricia Richards, MD, PhD2,*; Robin Kelen, MS, RN2;2 4 4 †
Clinical Therapeutics/Volume 34, Number 8, 2012
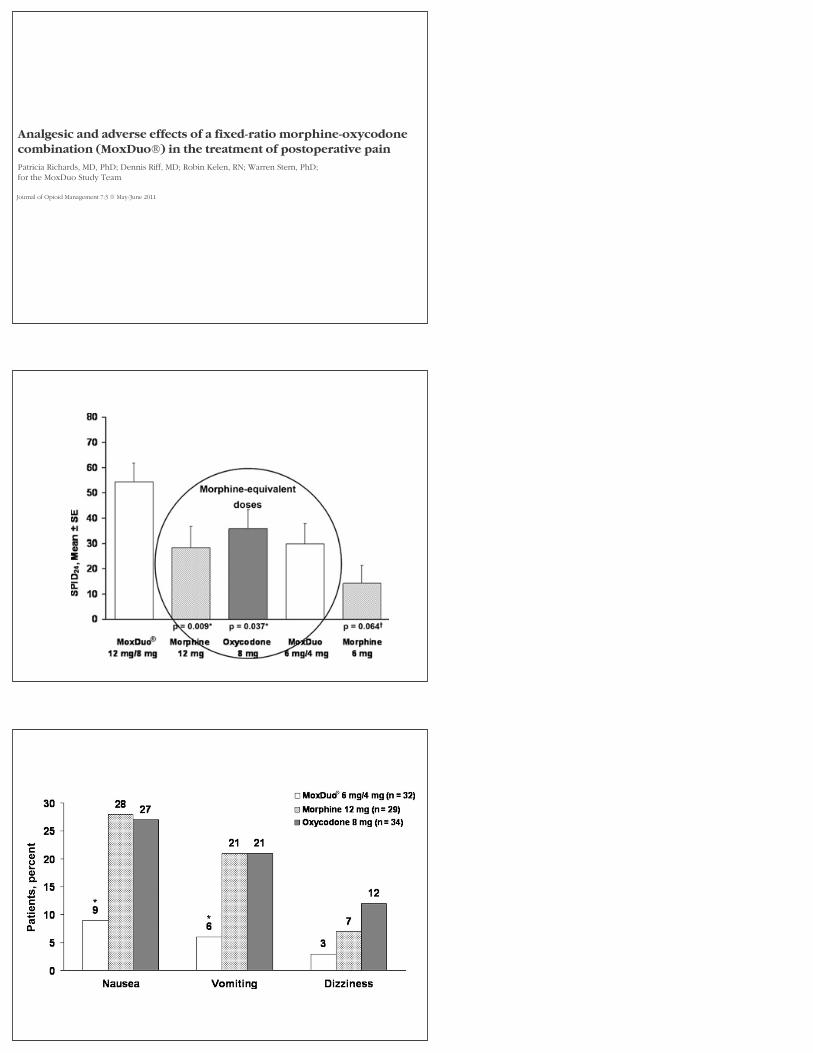
Analgesic and adverse effects of a fixed-ratio morphine-oxycodonecombination (MoxDuo®) in the treatment of postoperative pain
Patricia Richards, MD, PhD; Dennis Riff, MD; Robin Kelen, RN; Warren Stern, PhD; for the MoxDuo Study Team
Journal of Opioid Management 7:3 May/June 2011
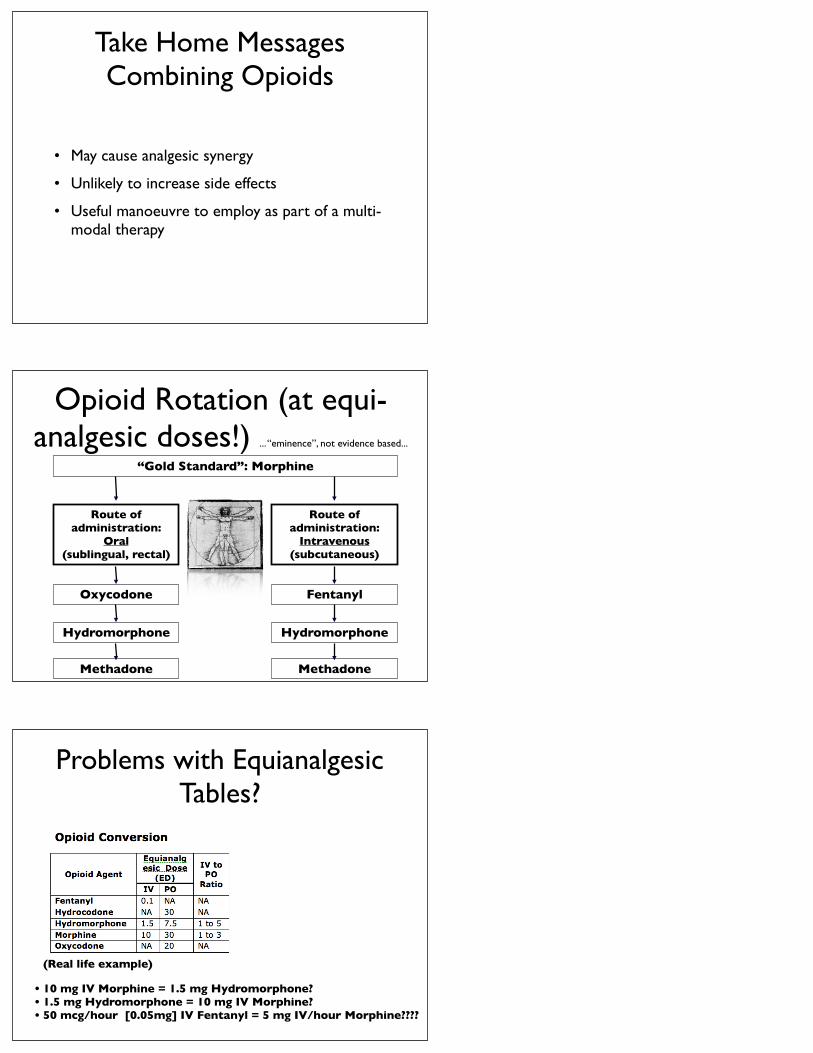
Take Home Messages Combining Opioids
• May cause analgesic synergy
• Unlikely to increase side effects
• Useful manoeuvre to employ as part of a multi-modal therapy
Opioid Rotation (at equi-analgesic doses!) ... “eminence”, not evidence based...
“Gold Standard”: Morphine
Route of administration:
Oral (sublingual, rectal)
Oxycodone
Route of administration:
Intravenous (subcutaneous)
Hydromorphone
Fentanyl
Hydromorphone
MethadoneMethadone
Problems with Equianalgesic Tables?
• 10 mg IV Morphine = 1.5 mg Hydromorphone?• 1.5 mg Hydromorphone = 10 mg IV Morphine?• 50 mcg/hour [0.05mg] IV Fentanyl = 5 mg IV/hour Morphine????
(Real life example)
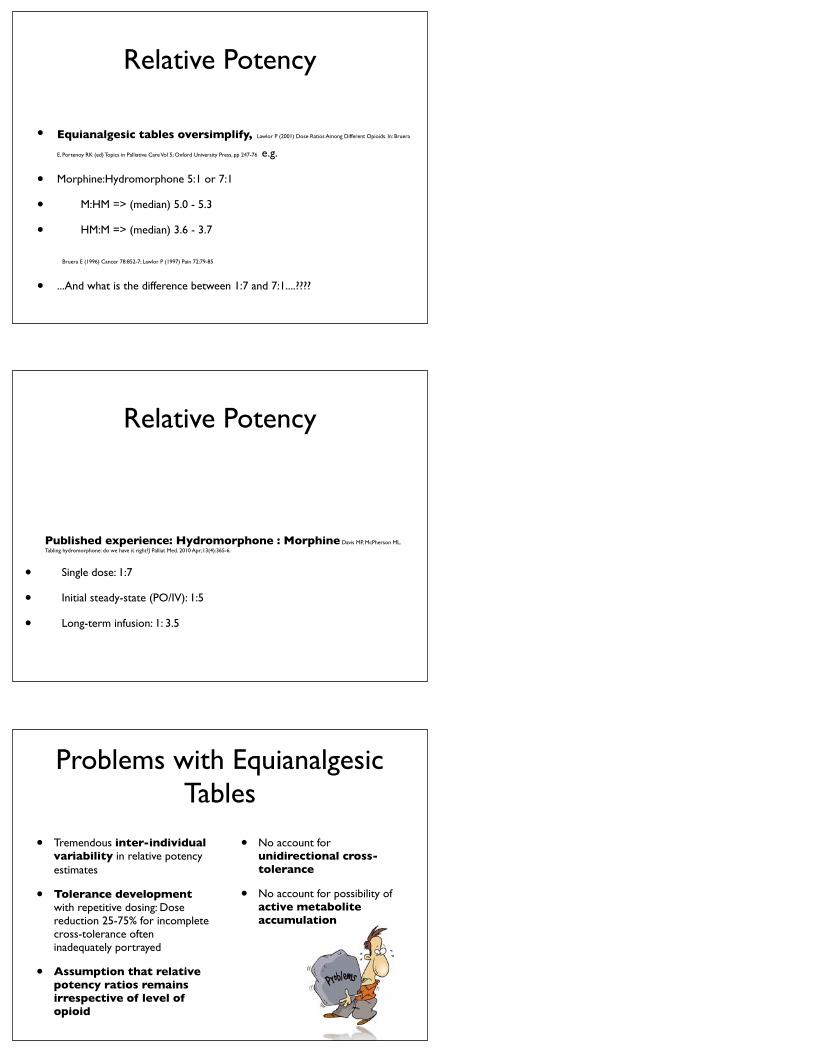
Relative Potency
• Equianalgesic tables oversimplify, Lawlor P (2001) Dose Ratios Among Different Opioids. In: Bruera
E, Portenoy RK (ed) Topics in Palliative Care Vol 5; Oxford University Press, pp 247-76 e.g.
• Morphine:Hydromorphone 5:1 or 7:1
• M:HM => (median) 5.0 - 5.3
• HM:M => (median) 3.6 - 3.7
Bruera E (1996) Cancer 78:852-7; Lawlor P (1997) Pain 72:79-85
• ...And what is the difference between 1:7 and 7:1....????
Relative Potency
Published experience: Hydromorphone : Morphine Davis MP, McPherson ML. Tabling hydromorphone: do we have it right?J Palliat Med. 2010 Apr;13(4):365-6.
• Single dose: 1:7
• Initial steady-state (PO/IV): 1:5
• Long-term infusion: 1: 3.5
Problems with Equianalgesic Tables
• Tremendous inter-individual variability in relative potency estimates
• Tolerance development with repetitive dosing: Dose reduction 25-75% for incomplete cross-tolerance often inadequately portrayed
• Assumption that relative potency ratios remains irrespective of level of opioid
• No account for unidirectional cross-tolerance
• No account for possibility of active metabolite accumulation
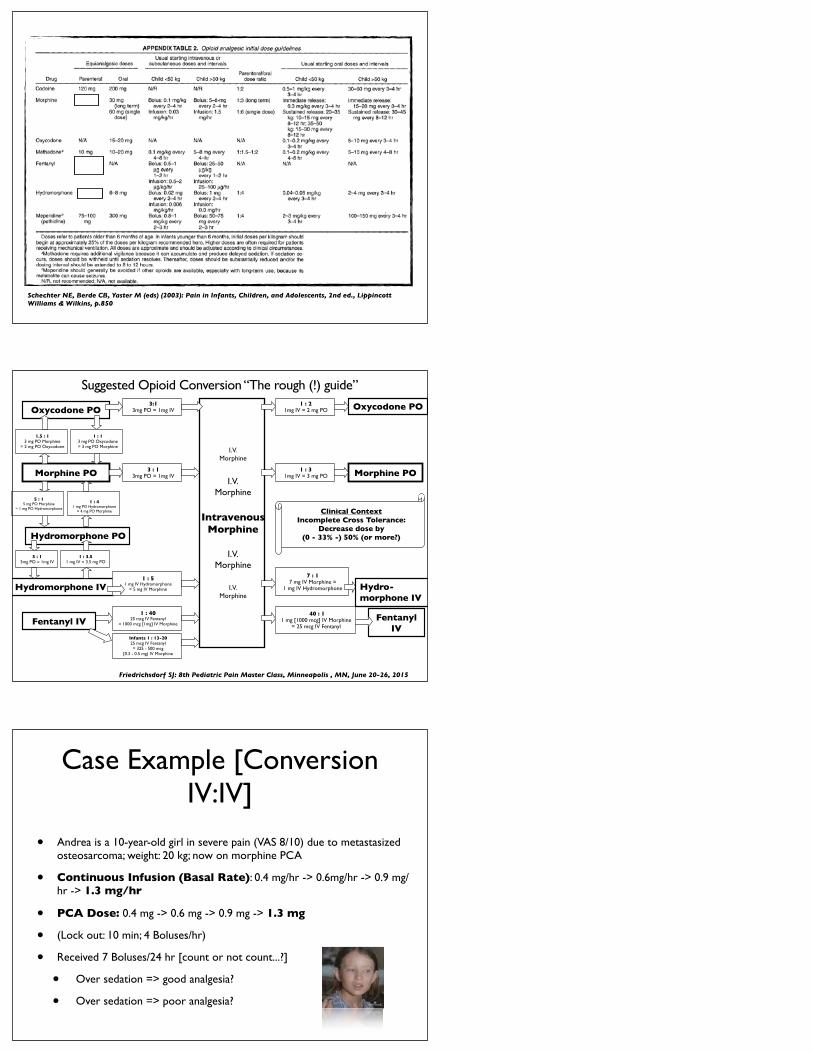
Schechter NE, Berde CB, Yaster M (eds) (2003): Pain in Infants, Children, and Adolescents, 2nd ed., Lippincott Williams & Wilkins, p.850
I.V.Morphine
I.V.Morphine
IntravenousMorphine
I.V.Morphine
I.V.Morphine
Morphine PO
Oxycodone PO
Hydromorphone IV
Hydromorphone PO
Oxycodone PO
Morphine PO
Fentanyl IV
Friedrichsdorf SJ: 8th Pediatric Pain Master Class, Minneapolis , MN, June 20-26, 2015
3:13mg PO = 1mg IV
3 : 13mg PO = 1mg IV
1.5 : 13 mg PO Morphine
= 2 mg PO Oxycodone
5 : 15mg PO = 1mg IV
1 : 3.51 mg IV = 3.5 mg PO
1 : 51 mg IV Hydromorphone
= 5 mg IV Morphine
1 : 4025 mcg IV Fentanyl
= 1000 mcg [1mg] IV Morphine
Infants 1 : 13-2025 mcg IV Fentanyl = 325 - 500 mcg
[0.3 - 0.5 mg) IV Morphine
1 : 21mg IV = 2 mg PO
1 : 31mg IV = 3 mg PO
7 : 17 mg IV Morphine =
1 mg IV Hydromorphone Hydro-morphone IV
Fentanyl IV
40 : 11 mg [1000 mcg] IV Morphine
= 25 mcg IV Fentanyl
Clinical ContextIncomplete Cross Tolerance:
Decrease dose by (0 - 33% -) 50% (or more?)
1 : 13 mg PO Oxycodone= 3 mg PO Morphine
5 : 15 mg PO Morphine
= 1 mg PO Hydromorphone
1 : 41 mg PO Hydromorphone
= 4 mg PO Morphine
Suggested Opioid Conversion “The rough (!) guide”
Case Example [Conversion IV:IV]
• Andrea is a 10-year-old girl in severe pain (VAS 8/10) due to metastasized osteosarcoma; weight: 20 kg; now on morphine PCA
• Continuous Infusion (Basal Rate): 0.4 mg/hr -> 0.6mg/hr -> 0.9 mg/hr -> 1.3 mg/hr
• PCA Dose: 0.4 mg -> 0.6 mg -> 0.9 mg -> 1.3 mg
• (Lock out: 10 min; 4 Boluses/hr)
• Received 7 Boluses/24 hr [count or not count...?]
• Over sedation => good analgesia?
• Over sedation => poor analgesia?

Morphine PCAContinuous Infusion (Basal Rate): 1.3 mg/hr (= 1300 mcg/hr) Fentanyl [M:F = 40:1]
1300 mcg/hrMorphine65 mcg/kg/hr
/ 4032 mcg/hrFentanyl
1.6 mcg/kg/hr 0% Dose reduction
32 mcg PCA Bolus
Lockout 5-10 min, max 4-6/hr
33 % Dose reduction 21 mcg/hr
Fentanyl1 mcg/kg/hr
21 mcg PCA Bolus
Lockout 5-10 min, max 4-6/hr
Case Example [Conversion IV:IV]
...Dose reduction...?
Clinical ContextIncomplete Cross
Tolerance: Decrease dose by
(0 - 33% -) 50% (or more?)
...it depends...
Morphine PCAContinuous Infusion (Basal Rate): 1.3 mg/hr (= 1300 mcg/hr)
Case Example [Conversion IV:IV]
Hydromorphone [M:H = 7:1]
1.3 mg/hrMorphine65 mcg/kg/hr
/ 70.19 mg/hr
Hydromorphone9 mcg/kg/hr
0% Dose reduction0.19 mg
PCA Bolus Lockout 7 min, max 6/hr
50 % Dose reduction 0.1 mg/hr
Hydromorphone4.5 mcg/kg/hr
0.1 mgPCA Bolus
Lockout 7 min, max 6/hr
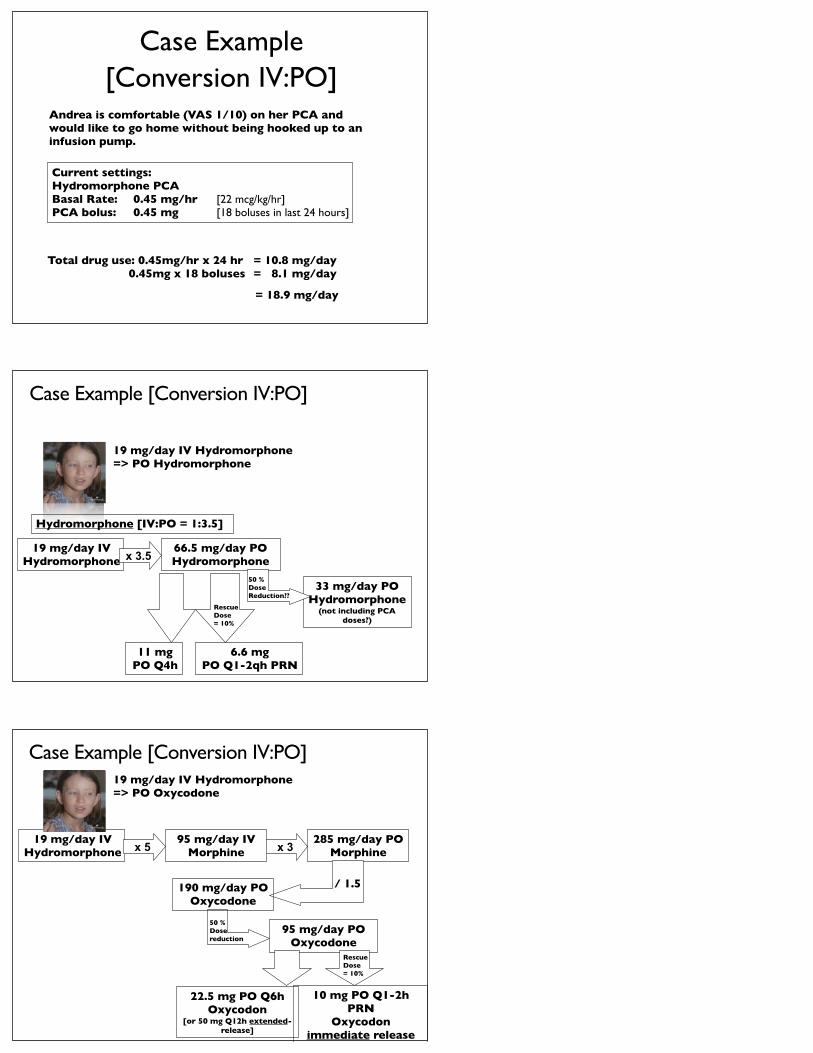
Case Example [Conversion IV:PO]
Andrea is comfortable (VAS 1/10) on her PCA and would like to go home without being hooked up to an infusion pump.
Current settings: Hydromorphone PCA Basal Rate: 0.45 mg/hr [22 mcg/kg/hr]PCA bolus: 0.45 mg [18 boluses in last 24 hours]
Total drug use: 0.45mg/hr x 24 hr = 10.8 mg/day 0.45mg x 18 boluses = 8.1 mg/day
= 18.9 mg/day
Case Example [Conversion IV:PO]
19 mg/day IV Hydromorphone=> PO Hydromorphone
Hydromorphone [IV:PO = 1:3.5]
19 mg/day IVHydromorphone x 3.5
66.5 mg/day POHydromorphone
33 mg/day POHydromorphone
(not including PCA doses?)
11 mgPO Q4h
50 % Dose Reduction??
RescueDose= 10%
6.6 mgPO Q1-2qh PRN
Case Example [Conversion IV:PO] 19 mg/day IV Hydromorphone=> PO Oxycodone
19 mg/day IVHydromorphone x 5
95 mg/day IVMorphine
95 mg/day POOxycodone
50 % Dose reduction
RescueDose= 10%
10 mg PO Q1-2h PRN
Oxycodon immediate release
x 3285 mg/day PO
Morphine
190 mg/day POOxycodone
/ 1.5
22.5 mg PO Q6hOxycodon
[or 50 mg Q12h extended-release]
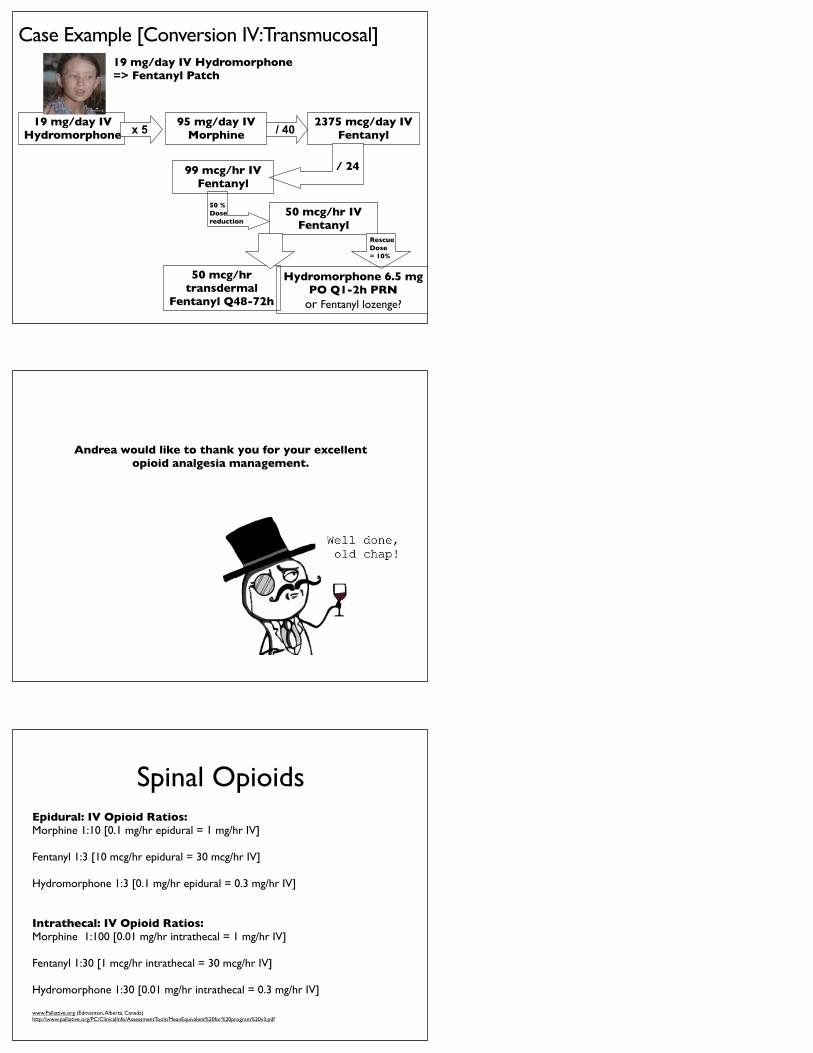
Case Example [Conversion IV:Transmucosal] 19 mg/day IV Hydromorphone=> Fentanyl Patch
19 mg/day IVHydromorphone x 5
95 mg/day IVMorphine
50 mcg/hr IVFentanyl
50 mcg/hrtransdermal
Fentanyl Q48-72h
50 % Dose reduction
RescueDose= 10%
Hydromorphone 6.5 mg PO Q1-2h PRN
or Fentanyl lozenge?
/ 402375 mcg/day IV
Fentanyl
99 mcg/hr IVFentanyl
/ 24
Andrea would like to thank you for your excellentopioid analgesia management.
Spinal OpioidsEpidural: IV Opioid Ratios:Morphine 1:10 [0.1 mg/hr epidural = 1 mg/hr IV]
Fentanyl 1:3 [10 mcg/hr epidural = 30 mcg/hr IV]
Hydromorphone 1:3 [0.1 mg/hr epidural = 0.3 mg/hr IV]
Intrathecal: IV Opioid Ratios:Morphine 1:100 [0.01 mg/hr intrathecal = 1 mg/hr IV]
Fentanyl 1:30 [1 mcg/hr intrathecal = 30 mcg/hr IV]
Hydromorphone 1:30 [0.01 mg/hr intrathecal = 0.3 mg/hr IV]
www.Palliative.org (Edmonton, Alberta, Canada)http://www.palliative.org/PC/ClinicalInfo/AssessmentTools/MeanEquivalent%20for%20program%20v3.pdf
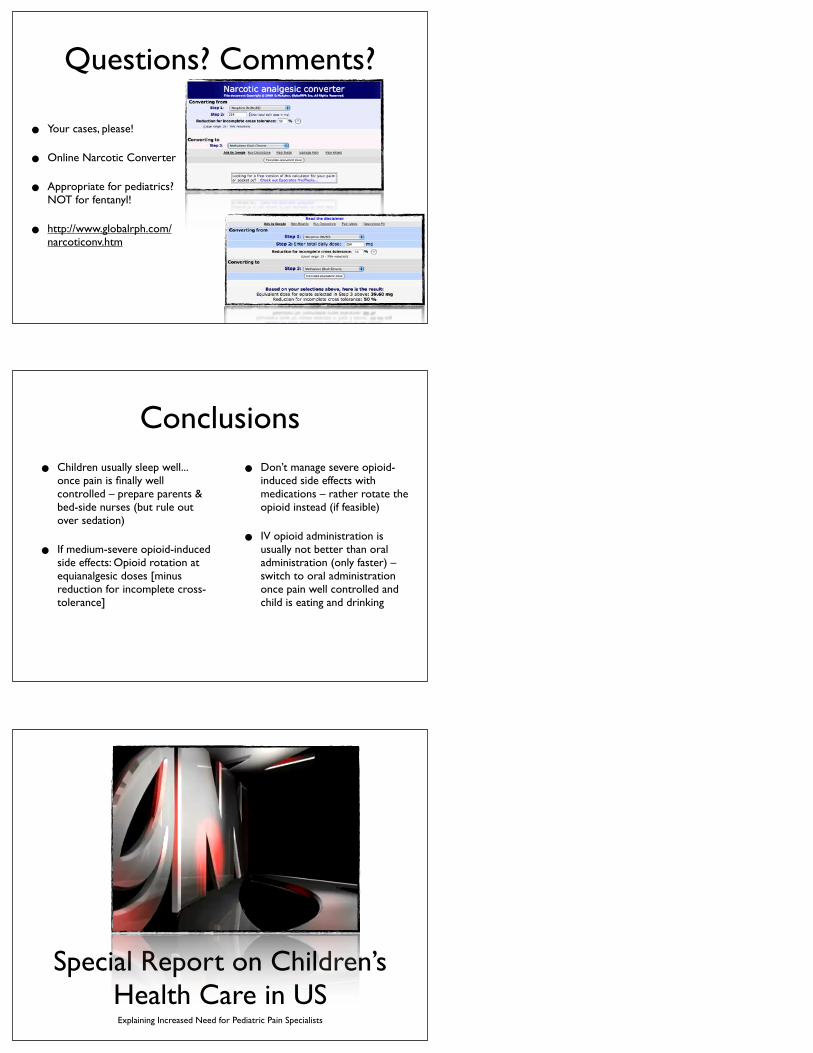
Questions? Comments?
• Your cases, please!
• Online Narcotic Converter
• Appropriate for pediatrics? NOT for fentanyl!
• http://www.globalrph.com/narcoticonv.htm
Conclusions• Children usually sleep well...
once pain is finally well controlled – prepare parents & bed-side nurses (but rule out over sedation)
• If medium-severe opioid-induced side effects: Opioid rotation at equianalgesic doses [minus reduction for incomplete cross-tolerance]
• Don’t manage severe opioid-induced side effects with medications – rather rotate the opioid instead (if feasible)
• IV opioid administration is usually not better than oral administration (only faster) – switch to oral administration once pain well controlled and child is eating and drinking
Special Report on Children’s Health Care in USExplaining Increased Need for Pediatric Pain Specialists
Twitter: @NoNeedlessPain
Stefan J. Friedrichsdorf, MD, FAAP Associate Professor of Pediatrics, University of Minnesota Medical School
Medical Director, Department of Pain Medicine, Palliative Care & Integrative Medicine Children's Hospitals and Clinics of Minnesota
2525 Chicago Ave S | Minneapolis, MN 55404 | USA612.813.6450 phone | 612.813.7199 fax
http://www.childrensmn.org/services/painpalliativeintegrativemed
Further Training: [email protected]
9th Annual Pediatric Pain Master Class • Minneapolis, MN | June 11-17, 2016
Education in Palliative & End-of-life Care [EPEC]: Become an EPEC-Pediatrics Trainer• 8th Conference: Montevideo, Uruguay | Sept 5, 2015 • 9th Conference: Chicago, IL | March 12-13, 2016
Blog: http://NoNeedlessPain.org