Embed Size (px)
Citation preview
1
Sarah J. Payne, MS, PharmD, BCPS
Assistant Professor, UNT System College of Pharmacy
The Opioid Epidemic
Learning Objectives
1. Describe the prescription painkiller epidemic.
2. State the DEA Scheduling Class for hydrocodone as of October 2014.
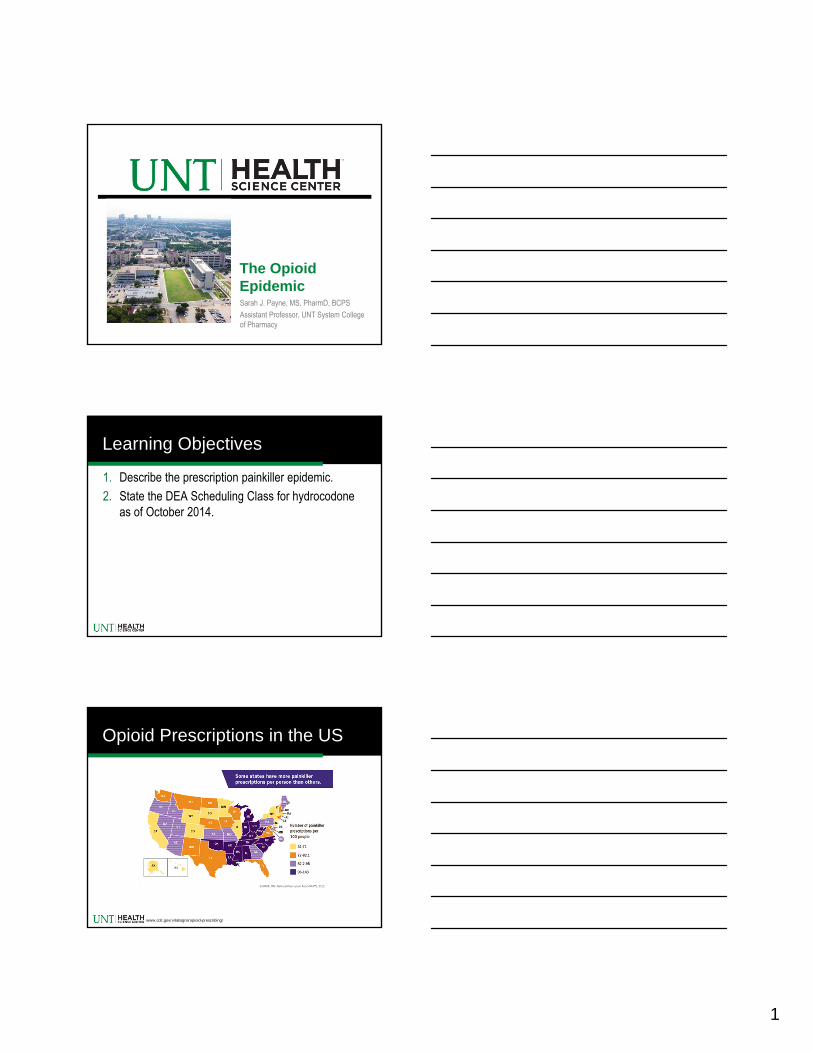
Opioid Prescriptions in the US
www.cdc.gov/vitalsigns/opioid-prescribing/
2
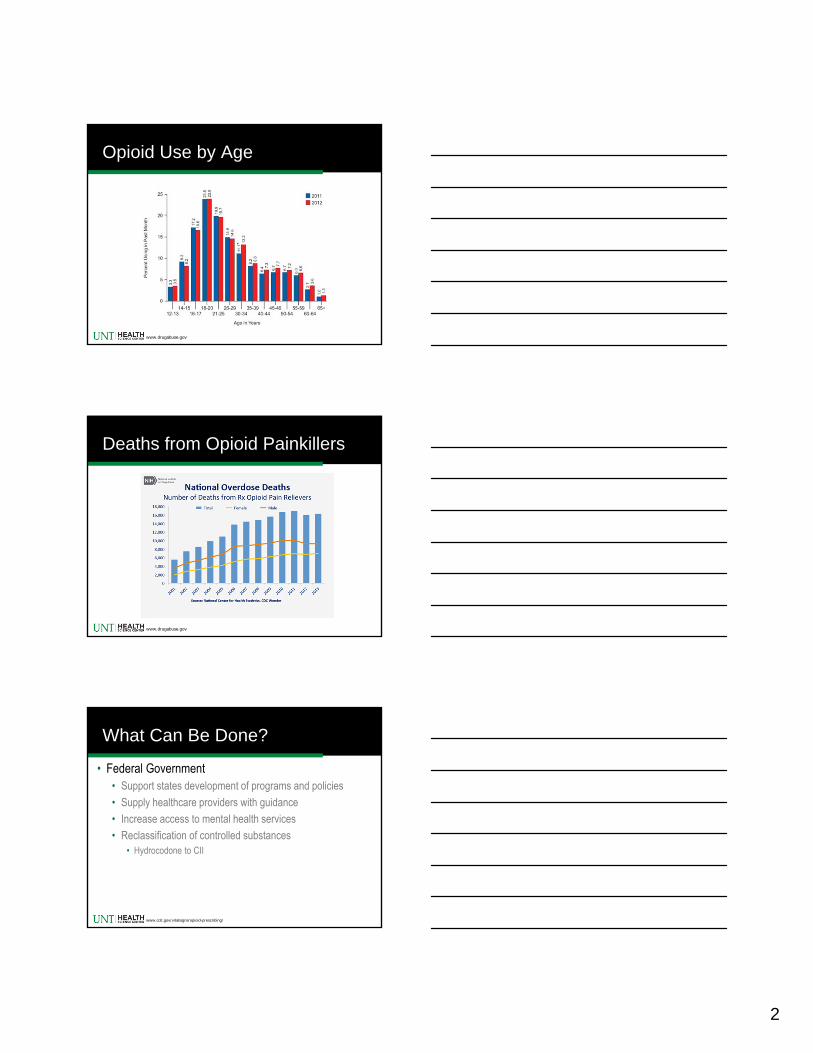
Opioid Use by Age
www.drugabuse.gov
Deaths from Opioid Painkillers
www.drugabuse.gov
What Can Be Done?
• Federal Government• Support states development of programs and policies
• Supply healthcare providers with guidance
• Increase access to mental health services
• Reclassification of controlled substances• Hydrocodone to CII
www.cdc.gov/vitalsigns/opioid-prescribing/
3
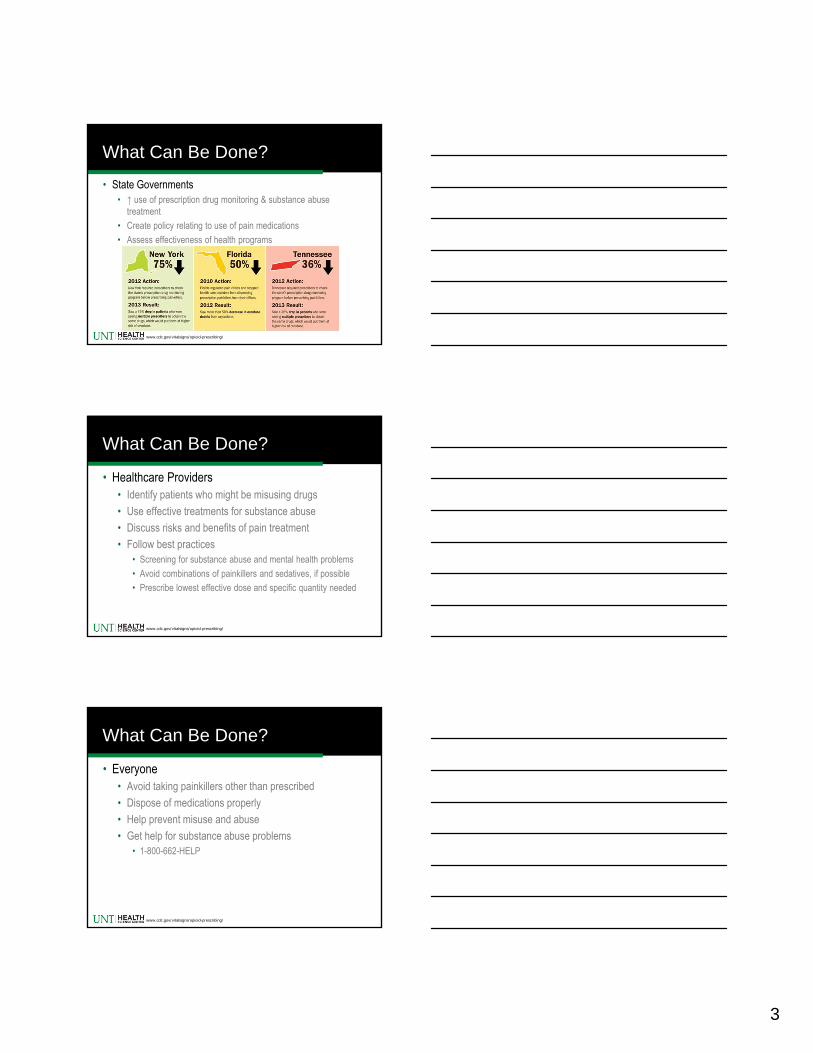
What Can Be Done?
• State Governments• ↑ use of prescription drug monitoring & substance abuse
treatment
• Create policy relating to use of pain medications
• Assess effectiveness of health programs
www.cdc.gov/vitalsigns/opioid-prescribing/
What Can Be Done?
• Healthcare Providers• Identify patients who might be misusing drugs
• Use effective treatments for substance abuse
• Discuss risks and benefits of pain treatment
• Follow best practices• Screening for substance abuse and mental health problems
• Avoid combinations of painkillers and sedatives, if possible
• Prescribe lowest effective dose and specific quantity needed
www.cdc.gov/vitalsigns/opioid-prescribing/
What Can Be Done?
• Everyone• Avoid taking painkillers other than prescribed
• Dispose of medications properly
• Help prevent misuse and abuse
• Get help for substance abuse problems• 1-800-662-HELP
www.cdc.gov/vitalsigns/opioid-prescribing/
4
Jon C. Sivoravong, D.O.Associate Professor and
Vice Chair for Clinical Affairs Department of Family Medicine-UNTHSC
March 2015
Understand acute and chronic pain
Understand abuse, addiction and aberrant behaviors
Describe the frame work for opioid prescription
Able to locate Prescription Access in Texas website
Able to write schedule II prescription
Goals and objectives
No issue more polarizing than management of chronic pain
Spectrum of belief on treatment ranges from those who believe narcotics should never be prescribed who believe narcotics best therapeutic option
1:4 American suffers from chronic pain
Treatment of nonmalignant chronic pain in primary setting
5
No issue more polarizing than management of chronic pain
Spectrum of belief on treatment ranges from those who believe narcotics should never be prescribed who believe narcotics best therapeutic option
1:4 American suffers from chronic pain
Treatment of nonmalignant chronic pain in primary setting
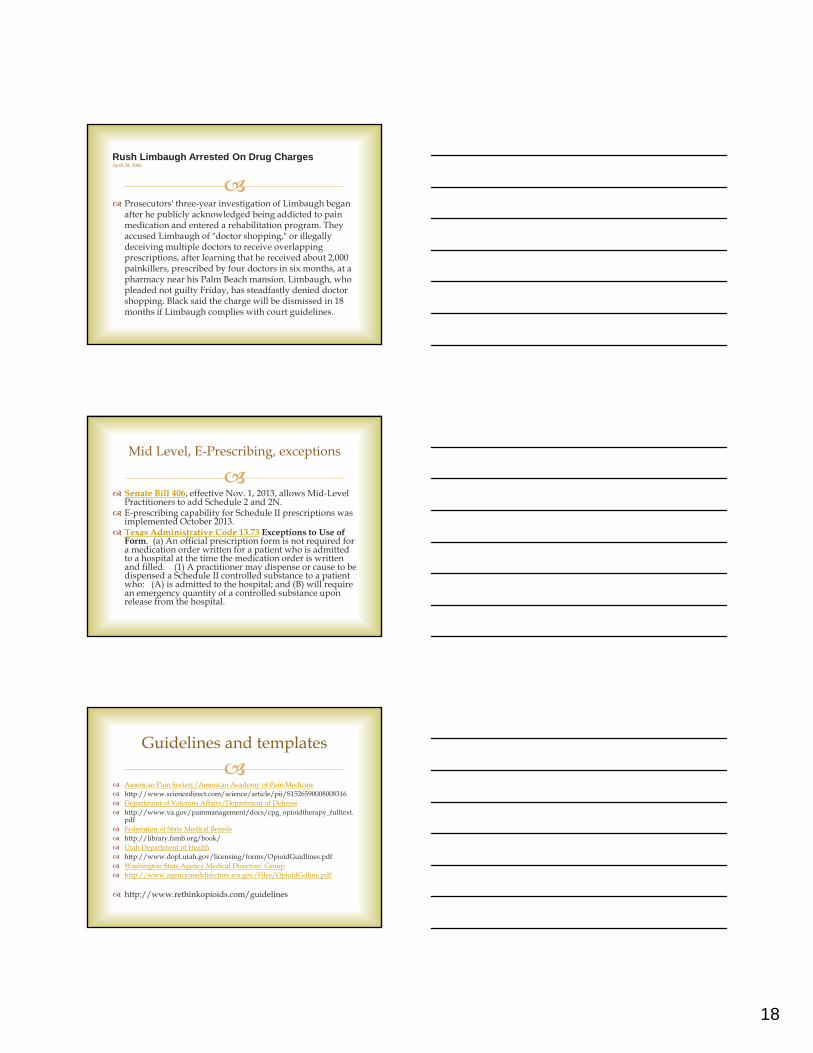
Nociceptive Pain RA, Gout, Osteoarthritis
Neuropathic Pain Diabetic peripheral neuropathy, post herpetic
neuralgia
Sensory Hypersensitivity Fibromyalgia
Three Main types of pain pathophysiology
Nociceptive Pain RA, Gout, Osteoarthritis
Neuropathic Pain Diabetic peripheral neuropathy, post herpetic
neuralgia
Sensory Hypersensitivity Fibromyalgia
Three Main types of pain pathophysiology
6
Nociceptive Pain RA, Gout, Osteoarthritis
Neuropathic Pain Diabetic peripheral neuropathy, post herpetic
neuralgia
Sensory Hypersensitivity Fibromyalgia
Three Main types of pain pathophysiology
Unpleasant sensory and emotional experience
associated with actual or potential tissue damage or described in terms of such damage
does not require nociception, as pain is emotional experience.
Pain:
International Association for the Study of Pain (IASP) - 1994
Unpleasant sensory and emotional experience
associated with actual or potential tissue damage or described in terms of such damage
does not require nociception, as pain is emotional experience.
Pain:
International Association for the Study of Pain (IASP) - 1994
7
Short or appropriate duration (usually <2 wk.)
Specific pathology
Treatment obvious
Useful in getting person to physician
Generally does not interfere with function
Acute pain
Short or appropriate duration (usually <2 wk.)
Specific pathology
Treatment obvious
Useful in getting person to physician
Generally does not interfere with function
Acute pain
Persist longer than 3 or 6 month Persist longer beyond the normal healing process Occurs after acute injury or have no apparent cause May spread beyond the original site Appears to serve no biological purpose Moderate to severe intensity Limits physiologic function and Psychological and emotional
activities Reduce quality of life Refractory to treatment.
JAMA 2003
Chronic pain -70 million sufferer 2003
8
Persist longer than 3 or 6 month Persist longer beyond the normal healing process Occurs after acute injury or have no apparent cause May spread beyond the original site Appears to serve no biological purpose Moderate to severe intensity Limits physiologic function and Psychological and emotional
activities Reduce quality of life Refractory to treatment.
JAMA 2003
Chronic pain -70 million sufferer 2003
Pain is usually undertreated due to multiple cause Decision to give opioids is difficult when patient is not an ideal candidate Prescriptions must be individualized (medical, psychiatric and hsx response) Prescriber may occasionally be misled by patients who divert or misuse Prescribers have obligation to understand the risks, and management of
addictive disease. Prescribers who persistently fail to treat addiction is poor medical practice Prescribers who fail to prescribe opioids when use is indicated is also poor
medical practice Providers traditionally receive little or no education about pain
management or treatment of addition.
American Academy of Pain Medicine 2004
Rights and Responsibilities of prescribers of Opioids
Prescription drug abuse
Most abused
OpioidsCNS depressant
anxiety and sleep disorders
Stimulants ADHD and Narcolepsy
Young people
1 in 5 teenager Most popular drugs Hydrocodone 18% Oxycodone 10% ADHD drugs 10%
National Institute of Drug Abuse. 2005 Partnership for drug free America 2007
9
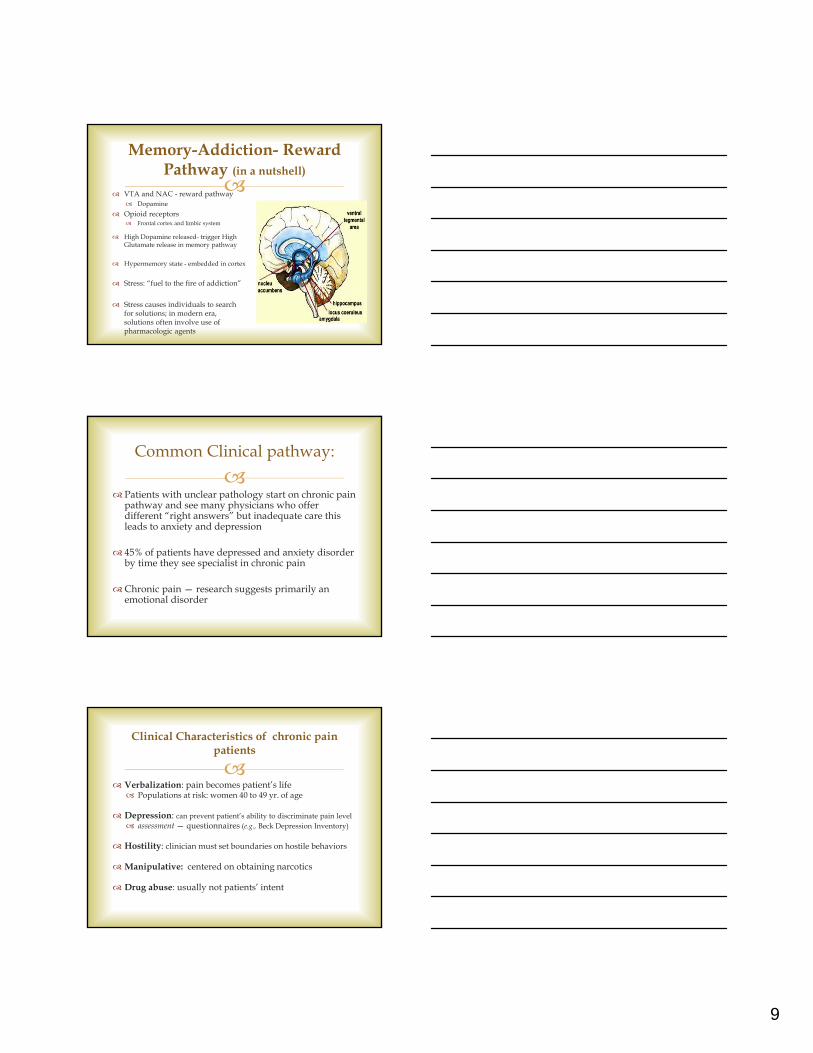
Memory-Addiction- Reward Pathway (in a nutshell)
VTA and NAC - reward pathway Dopamine
Opioid receptors Frontal cortex and limbic system
High Dopamine released- trigger High Glutamate release in memory pathway
Hypermemory state - embedded in cortex
Stress: “fuel to the fire of addiction”
Stress causes individuals to search for solutions; in modern era, solutions often involve use of pharmacologic agents
Patients with unclear pathology start on chronic pain
pathway and see many physicians who offer different “right answers” but inadequate care this leads to anxiety and depression
45% of patients have depressed and anxiety disorder by time they see specialist in chronic pain
Chronic pain — research suggests primarily an emotional disorder
Common Clinical pathway:
Verbalization: pain becomes patient’s life Populations at risk: women 40 to 49 yr. of age
Depression: can prevent patient’s ability to discriminate pain level assessment — questionnaires (e.g., Beck Depression Inventory)
Hostility: clinician must set boundaries on hostile behaviors
Manipulative: centered on obtaining narcotics
Drug abuse: usually not patients’ intent
Clinical Characteristics of chronic pain patients
10
The use of any substance for nontherapeutic purpose
or the use of medication for purposes other than those for which the agent is prescribed.
Drug abuse
The use of any substance for nontherapeutic purpose
or the use of medication for purposes other than those for which the agent is prescribed.
Drug abuse
A primary chronic neurobiological disease
influenced by genetics, psychosocial, and environmental factors.
It is characterize by impaired control over drug use, compulsive drug use, and continued drug use despite harm and because of craving.
Addiction
11
A primary chronic neurobiological disease
influenced by genetics, psychosocial, and environmental factors.
It is characterize by impaired control over drug use, compulsive drug use, and continued drug use despite harm and because of craving.
Addiction
Abuse vs Addiction:
Abuser
Stressors influential in Abusers
Abusers or heavy abusers behave as if addicted when under severe stress
Addiction Behavior uncontrolled
without means of modulation
Substance escalate steadily under normal circumstances in absence of stress
Eventually, substance becomes solution to every form of emotional discomfort
Chronic pain patient vs
Addicted patient
Chronic pain
Medication use not out of control
Medication improve quality of life
Is concerned about physical problem
Follow agreement for opioids
Frequently has leftover
Addicted Out of control Medication diminished
quality of life Increase medication use
despite adverse effects Unaware of or denial about
problem as a result from drug treatment
Does not follow agreement Does not have leftover, loses
prescriptions, always has a story
12
Chronic pain pt.
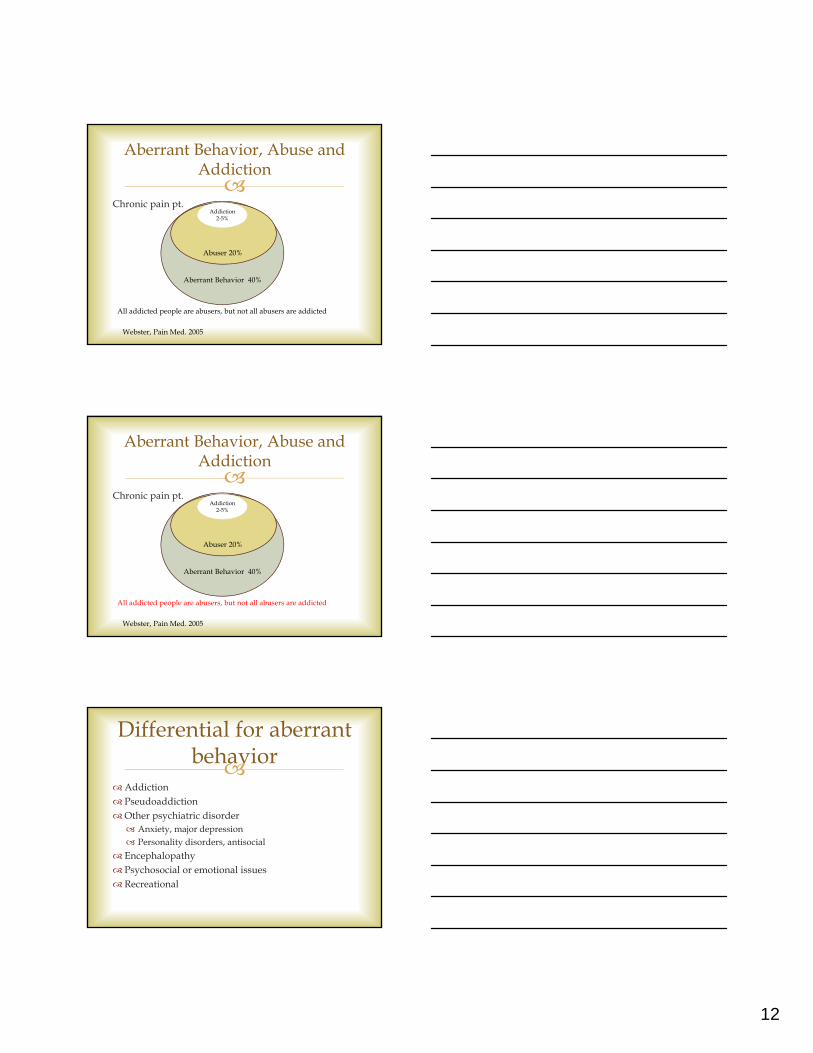
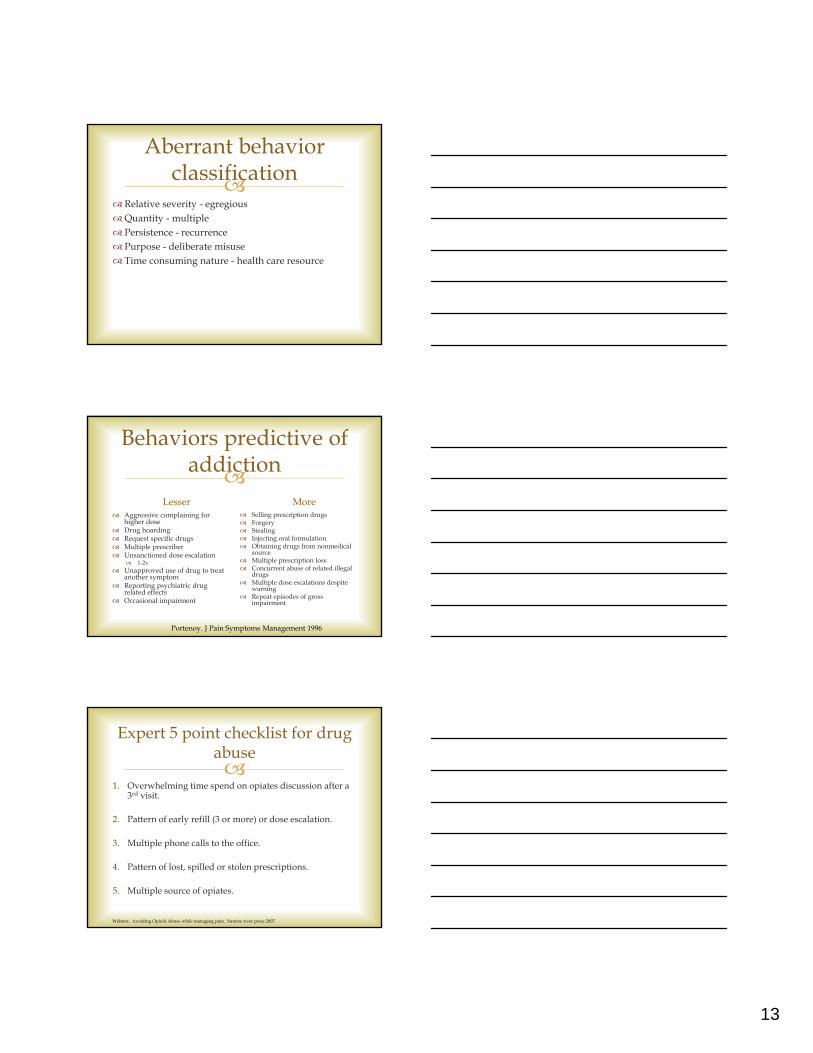
Aberrant Behavior, Abuse and Addiction
Addiction 2-5%
Abuser 20%
Aberrant Behavior 40%
Webster, Pain Med. 2005
All addicted people are abusers, but not all abusers are addicted
Chronic pain pt.
Aberrant Behavior, Abuse and Addiction
Addiction 2-5%
Abuser 20%
Aberrant Behavior 40%
Webster, Pain Med. 2005
All addicted people are abusers, but not all abusers are addicted
Addiction PseudoaddictionOther psychiatric disorder Anxiety, major depression Personality disorders, antisocial
Encephalopathy Psychosocial or emotional issues Recreational
Differential for aberrant behavior
13
Relative severity - egregious Quantity - multiple Persistence - recurrence Purpose - deliberate misuse Time consuming nature - health care resource
Aberrant behavior classification
Behaviors predictive of addiction
Lesser Aggressive complaining for
higher dose Drug hoarding Request specific drugs Multiple prescriber Unsanctioned dose escalation
1-2x Unapproved use of drug to treat
another symptom Reporting psychiatric drug
related effects Occasional impairment
More Selling prescription drugs Forgery Stealing Injecting oral formulation Obtaining drugs from nonmedical
source Multiple prescription loss Concurrent abuse of related illegal
drugs Multiple dose escalations despite
warning Repeat episodes of gross
impairment
Portenoy. J Pain Symptoms Management 1996
1. Overwhelming time spend on opiates discussion after a
3rd visit.
2. Pattern of early refill (3 or more) or dose escalation.
3. Multiple phone calls to the office.
4. Pattern of lost, spilled or stolen prescriptions.
5. Multiple source of opiates.
Expert 5 point checklist for drug abuse
Webster, Avoiding Opioid Abuse while managing pain. Sunrise river press 2007
14
Careful observation and documentation of drug
aberrant behavior should be charted in chronic pain patients like any clinical data such as hemoglobin A1c in diabetic patients and blood pressure reading on hypertensive patients.
Documentations
Narcotic prescription needs to be highly structured policy
Specific guidelines Pain contract, UDS, refills, multidisciplinary team approach
1: Assess Risk - consider non opioids first Assess patient’s risk for aberrant behaviors Assess the patient for psychological disorders Review your state’s prescription monitoring program Conduct a baseline urine drug test
2: Select Agent – Consider the patient’s general condition, medical status, and prior opioid experience After deciding on an agent, consider an abuse-deterrent opioid
3: Dialogue with patient Discuss treatment expectations Review written treatment agreement
4: Monitor Treatment – Regularly assess the “4 A’s” Analgesia: Activity: Adverse effects: Aberrant behavior:
A Framework for Appropriate Opioid prescribing
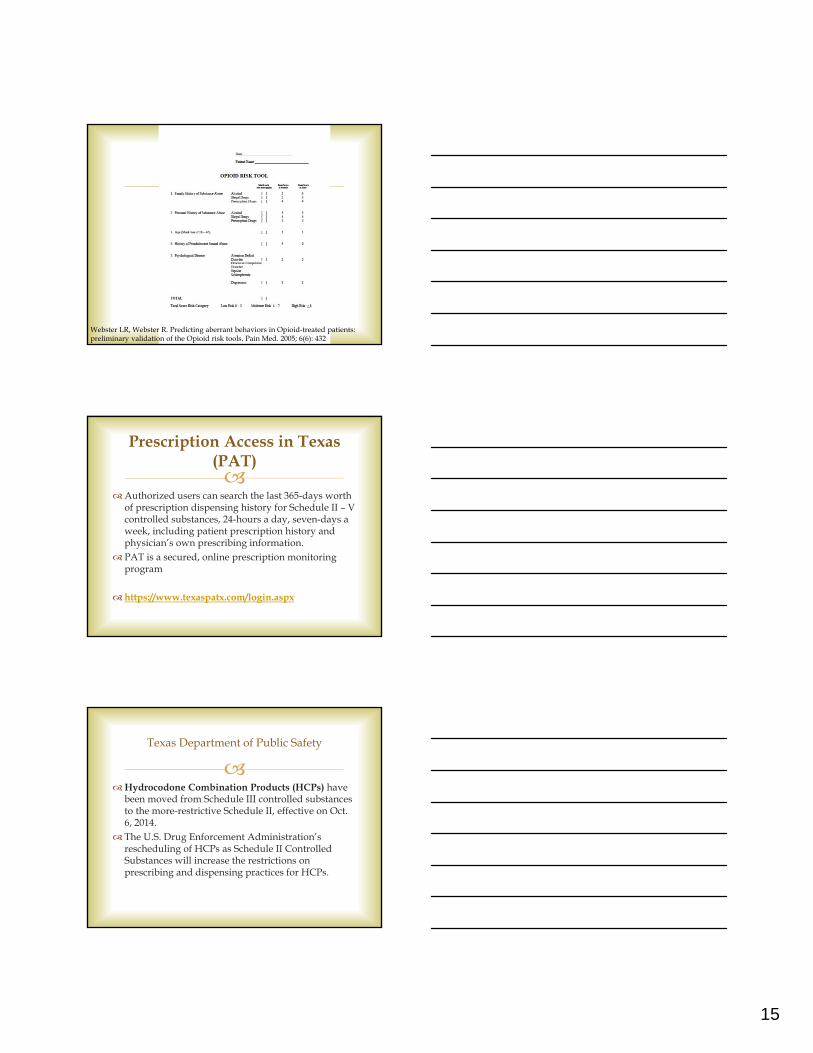
Addiction severity index Self or interview 200 item 1hr
Alcohol use Disorder identification Test Self or interview 10 item 2 minutes
Structure interview DSM-IV interview 30-60 min
CAGE interview 4 item <1 min
Case Adapted to include drugs interview 4 items <1 min
Two item conjoint screening tool interview 2 items <1 min
Screener and Opioid Assessment for Patients with Pain (SOAPP)
Self or interview 24 items 10 min
Prescription Drug use Questionnaire interview 42 items 20 min
RAFFT Self 5 items about 1 min
Drug Abuse Screening Test self 20 items 5 min
Michigan Alcohol Screening Test Self or interview 25 items 15 min
Screening Instrument for Substance Abuse Potential
interview 5 Items about 1 min
Substance abuse Subtle Screening Inventory
self 1 page 15 min
Severity of opiate Dependence Questionnaire
self 21 items about 5 min
Opioid Risk Tool self 5 items 1 min
Risk Tools
15
Webster LR, Webster R. Predicting aberrant behaviors in Opioid-treated patients: preliminary validation of the Opioid risk tools. Pain Med. 2005; 6(6): 432
Authorized users can search the last 365-days worth
of prescription dispensing history for Schedule II – V controlled substances, 24-hours a day, seven-days a week, including patient prescription history and physician’s own prescribing information.
PAT is a secured, online prescription monitoring program
https://www.texaspatx.com/login.aspx
Prescription Access in Texas (PAT)
Hydrocodone Combination Products (HCPs) have
been moved from Schedule III controlled substances to the more-restrictive Schedule II, effective on Oct. 6, 2014.
The U.S. Drug Enforcement Administration’s rescheduling of HCPs as Schedule II Controlled Substances will increase the restrictions on prescribing and dispensing practices for HCPs.
Texas Department of Public Safety
16
(A) the date the prescription is issued
(B) the controlled substance prescribed(C) the quantity of controlled substance prescribed, shown:
(i) numerically, followed by the number written as a word (ii) numerically, if the prescription is electronic;
(D) the intended use - the diagnosis (E) the practitioner's name, address, and DEA number (F) the name, address, and date of birth or age of the person(G) if the prescription is issued to be filled at a later date under
481.074(d-1), the earliest date on which a pharmacy may fill the prescription;
(f) Not more than one prescription may be recorded on an official prescription form, except as provided by rule adopted under §481.0761.
Each official prescription form or electronic prescription used to
prescribe a Schedule II controlled substance must contain:
Dilemmas in treatment of
Chronic nonmalignant pain: Lack appreciation between acute
and chronic
Use extended-release opioids (immediate-release agents may act as trigger)
Emotional pain even in breakthrough pain
Patients must stop “chasing their pain”
Need to minimize effects on dopaminergic pathway
Opioid limits: keep patients below
high-dose level 100-120 mg of morphine
equivalents per 24-hr period * <60 mg recommended if
possible
Rotate long-term opioid use,
agents and lower dose
*Dunn KM, et. Opioid prescriptions for chronic pain and overdose: a cohort study. Ann Intern Med 2010;152(2):85-92.
http://www.rethinkopioids.com/medication-options-of-chronicpain
17
A physiologic state caused by regular use of an
opioid in which increased doses are needed to maintain the same effect.
In patients with “analgesic tolerance,” increased doses of the opioid are needed to maintain pain relief
Tolerance
A physiologic state characterized by abstinence
syndrome (withdrawal) if treatment with an opioid is stopped or decreased abruptly or an opioid antagonist is administered.
It is an expected result of opioid therapy and does not by itself equal addiction
Physical Dependence
A syndrome characterized by symptoms that include
sweating, tremor, vomiting, anxiety, insomnia, and muscle pain. caused by reduction in the opioid dose or opioid antagnonist.
It can be avoided by carefully tapering the opioids dosage and monitoring the patient.
American Academy of pain medicine American pain Society American society of addiction medicine
Abstinence Syndrome
18
Prosecutors' three-year investigation of Limbaugh began
after he publicly acknowledged being addicted to pain medication and entered a rehabilitation program. They accused Limbaugh of "doctor shopping," or illegally deceiving multiple doctors to receive overlapping prescriptions, after learning that he received about 2,000 painkillers, prescribed by four doctors in six months, at a pharmacy near his Palm Beach mansion. Limbaugh, who pleaded not guilty Friday, has steadfastly denied doctor shopping. Black said the charge will be dismissed in 18 months if Limbaugh complies with court guidelines.
Rush Limbaugh Arrested On Drug ChargesApril 28, 2006
Senate Bill 406, effective Nov. 1, 2013, allows Mid-Level
Practitioners to add Schedule 2 and 2N. E-prescribing capability for Schedule II prescriptions was
implemented October 2013. Texas Administrative Code 13.73 Exceptions to Use of
Form. (a) An official prescription form is not required for a medication order written for a patient who is admitted to a hospital at the time the medication order is written and filled. (1) A practitioner may dispense or cause to be dispensed a Schedule II controlled substance to a patient who: (A) is admitted to the hospital; and (B) will require an emergency quantity of a controlled substance upon release from the hospital.
Mid Level, E-Prescribing, exceptions
American Pain Society/American Academy of Pain Medicine http://www.sciencedirect.com/science/article/pii/S1526590008008316 Department of Veterans Affairs/Department of Defense http://www.va.gov/painmanagement/docs/cpg_opioidtherapy_fulltext.
pdf Federation of State Medical Boards http://library.fsmb.org/book/ Utah Department of Health http://www.dopl.utah.gov/licensing/forms/OpioidGuidlines.pdf Washington State Agency Medical Directors’ Group http://www.agencymeddirectors.wa.gov/Files/OpioidGdline.pdf
http://www.rethinkopioids.com/guidelines
Guidelines and templates
19
C H R I S T O P H E R J O R D A N , D O , F A C O I
M A R C H 1 8 , 2 0 1 5
U N T H S C G R A N D R O U N D S
Pain Management in Oncology
Identifying Pain
There are many tools useful for identifying patients with cancer-related pain
Verbal Patient
Literate
Illiterate
Non-verbal Patient
Dementia
ICU patient
Anticipating Pain
Pre-Procedural—pain is expected in many different procedures in Oncology, (bone marrow aspiration and biopsies, radiation, mediport placement and/or access, wound care, line placement, port access, LP, skin biopsies, etc…) as well as other maneuvers, such as transportation
Sufficient time and discussion with patients and family are important to plan analgesics (topical, local, and/or systemic therapy) as well as anxiolytic therapy
20
Pain Assessment
There are many different factors involved in assessment of pain, and each one is helpful to identifying the best possible treatment of pain
-cancer itself
-treatment and/or procedures
-coincidental (arthritis, etc…)
Pathophysiology—nociceptive, neuropathic, visceral, effective, behavioral, cognitive
The Pain Experience
Location, referral pattern, and pain radiation
Intensity—last 24 hrs and current (rest, movement)
Interference with activities**
Timing
Description or quality of pain
Aggrevating and alleviating factors
Current treatment plan (both pharmacologic and non-pharmacologic)
Response to current therapy
The Pain Experience (cont)
Breakthrough pain
Prior pain therapies
Special issues relating to pain—family and patient understanding, meaning and consequences of pain, patient goals, cultural, spiritual and religious beliefs toward pain medications, potential for abuse/misuse

21
Pain Management
First, its necessary to distinguish pain as an oncologic emergency or non-emergency
Then, determination of pain medications is necessary based on patients being narcotic naïve or tolerant.
Then, rating the pain 0-10 on numeric or picture scales, or using non-verbal pain scales, is necessary to establish severity of pain
Pain management (cont)
In patients experiencing pain <7 on 10 point scale, opiates should be a consideration up front, and adjuvant analgesics should be considered cautiously, as some can have adverse effects in both opiate naïve and opiate tolerant patients, though the dosages may differ significantly.
Caution should be used in both so dangerous side effects (respiratory depression, etc…) can be avoided and titration should be rapid.
Pain Management (cont)
Once adequate pain control is achieved with short acting opioids, and the goal of therapy should be the highest level of pain control with the least amount of side effects, if pain is adequately controlled with short acting opioids, whether alone or in combination with other anagesics, then would keep patient on the current dosages
22
Pain Management (cont)
If pain medication levels are adequate to achieve short term pain control, but are not sufficient for the prescribed period of time, then addition of longer acting medications is prudent here
Long-acting medications should be prescribed to take around the clock and not prn and should not be used for the short term control of pain. Dosages should be equivalent to the shorter acting medications for the prescribed time periods of the shorter acting medications, though the length of action of longer acting medications will generally be longer (12-72 hours depending on medications)
Breakthrough pain
Defined as pain that develops between doses of medication, whatever the interval is. Generally, when patients have these levels of pain, they should be on long-acting medications and have short acting combination agents for short term, break through pain control
Example: MS Contin Q12 hours ATC, followed by Norco Q4-6 hours prn breakthrough pain
Breakthrough pain
If breakthrough pain is severe and frequent, short acting pain medication is necessary and rapid titration of these medications are necessary to achieve short term pain control. Once these short acting doses are known, then increasing the dose of long acting medications would be appropriate
23
Other pain management options
If pain is confined to one area, narcotic and non-narcotic topical agents may be appropriate. These are beneficial because of local control with significantly less systemic effects.
Limitations: not for generalized pain. Require compounding pharmacy expertise typically.
Other pain management options (cont)
Injections—often, if pain is located in one area where a nerve block or local pain medications are appropriate, these can achieve very high levels of pain control (ex. Celiac plexus block in patients with pancreatic cancer)
Pain pumps—inserted to deliver continuous pain medication, typically to a specific nerve area to achieve adequate pain control
Other pain management options (cont)
Pain management consultation—practitioners specializing in pain management can assist significantly in the management of pain in patients with cancer and should be considered when unable to adequately control pain with medication prescriptions
Psychiatric consultation—in patients with psychiatric disorders, such as depression, pain can be significantly exacerbated by the underlying condition and prescription of psychiatric medications as adjunct therapies should be considered. Also, patients without underlying conditions can certainly have depression secondary to their cancer diagnosis and this should ALWAYS be a consideration in pain management
24
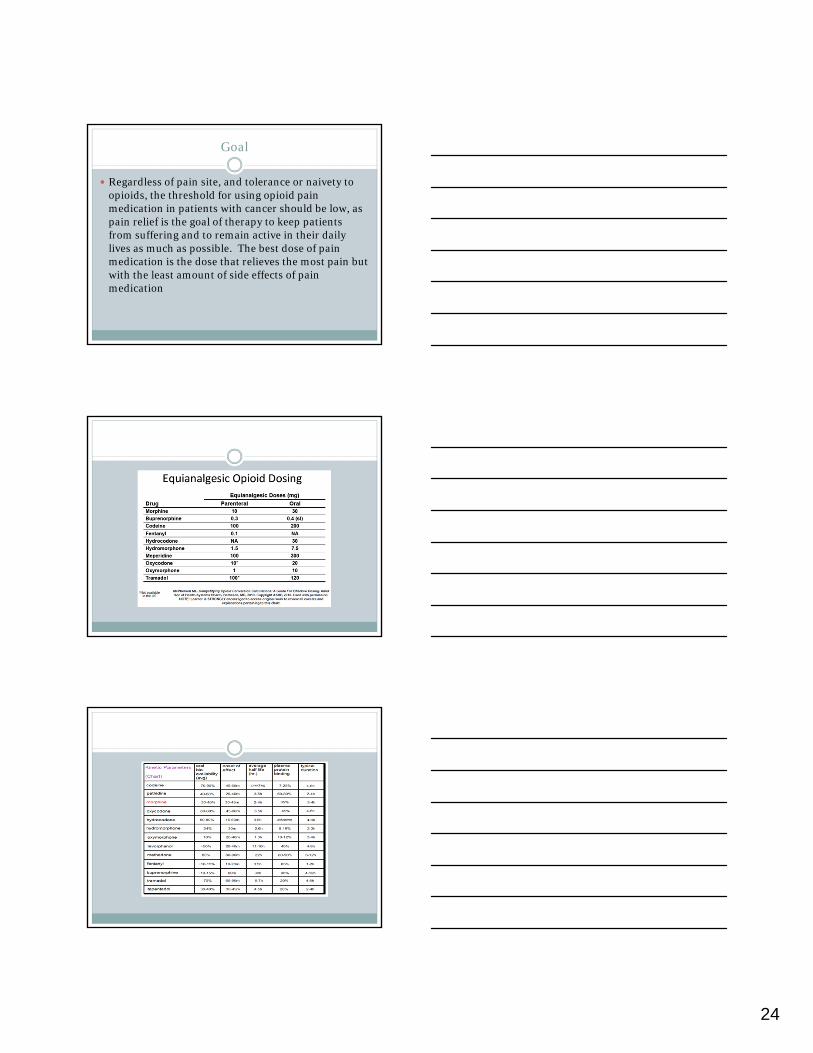
Goal
Regardless of pain site, and tolerance or naivety to opioids, the threshold for using opioid pain medication in patients with cancer should be low, as pain relief is the goal of therapy to keep patients from suffering and to remain active in their daily lives as much as possible. The best dose of pain medication is the dose that relieves the most pain but with the least amount of side effects of pain medication