Embed Size (px)
Citation preview

Opioid Analgesics:Pathways to Addiction.
Chris Evans, PhDNIDA Center for the Study of Opioid
Receptors and Drugs of Abuse (CSORDA),UCLA, California

One side of the story- Pain of all types is undertreated in our society. The pediatric and geriatric populationsare especially at risk for undertreatment. Physicians’ fears of using opioid therapy, and the fears of other healthprofessionals, contribute to this problem.
- Opioid analgesics are generally safe medications when prescribed withappropriate monitoring. There is very little if any evidence of organ damage from the long termtherapeutic use of opioids. With appropriate titration and stable dosing, tolerance develops to most of the side effectsof opioid therapy, including cognitive impairment. Constipation is the most common persistent side effect and should bemanaged prophylactically.
Use of opioid analgesics for the treatment of chronic noncancer pain - A consensusstatement and guidelines from the Canadian Pain Society 1998
John Liebeskind 1935-1997

1) New Nonmedical Prescription Pain Reliever users Outnumbered New Marijuana Users (2002-2004)
2) 2.7% of the population 12 and older in 03 used prescription psychotherapeutic medications
nonmedically in the month prior to surveyed. This included 4.7 million using pain relievers (compares to
166,000 Heroin users).
3) Estimated 415,000 Americans received treatment for pain reliever abuse in the past year.
4) Past year abuse of Vicodin 3.0% among 8th-graders, 7.0 % among 10th-graders, and 9.7% among
12th-graders in 2006, (stable since ‘02). Despite a drop in past year abuse of OxyContin among
12th-graders in ‘06, abuse among 8th-graders nearly doubled since 2002 (1.3% in ‘02 - 2.6 % in ‘06)Data from the 2002, 2003 and 2004 National Surveys on Drug Use and Health
Past Year Nonmedical Use of PainRelievers (% use 12 or Older, 02-04)
Nonmedical New Usersof Psychotheraputics
% US Population5.68-7.003.78-5.672.61-3.75
The Other Side
3 million
2 million
1million
0

MORPHINE, FENTANYL, ETORPHINE, HYDROCODONE, OXYCODONE,CODEINE, BUPRENORPHINE, HEROIN, METHADONE
(RARELY RECEPTOR SPECIFIC - Drugs are dirty)
ACTH, MSH
POMC PROENKEPHALIN PRODYNORPHIN
Prohormone Convertases (PC’s)CPE and PAM
ENDOMORPHINS?MORPHINE?
PROORPHANIN-FQ
δ κ µ ORL-1

NCCH2CH3CH2CH2N
Fentanyl (epidural, Moscow Siege Gas)
O
N-CH3
OH
OH
O
Morphine (surgery)
HO-C-CH3
N-CH2
C (CH3)3
OH
O
CH3O
Buprenorphine (addicts) Methadone (addicts)
CH3
CH3-N-CH3CH3O
Oxy/hydrocodone (pain)
Opioid Receptor selectivityAgonist/Partial AgonistsActivity at other receptors (NMDA)Rate of onset/duration*Route of AdministrationDependency/toleranceActivity at mu opioid receptors
OXY (X=OH)HYDRO (X=H)CODONE
NCH3
O
CH3O
XO
PERCOSETPERCODAN OXYCODONE OXYCONTINVICODIN HYDROCODONE

MuAgonists: analgesia, constipation, reward, nausea,respiratory depression - gender specificAntagonists: aversive*, prevent reward
DeltaAgonists: not-rewarding, weak analgesia,seizure-inducingAntagonists: no obvious effects
KappaAgonists: aversive, hallucinogenic, analgesiaAntagonists: potential antidepressants/relapseORL-1Agonists: Hyperalgesia* and block opioid analgesiaAntagonists: no obvious effects

Homologousrecombination
Mu KO mice have no classical morphine effects (analgesia, respiratorydepression, reward, immune modulation). No longer are alcohol, nicotine orTHC rewarding! Reviews by Kieffer’s group Curr Opin Neurobiology, 2004

BUPRENORPHINE (κ antagonist, µ/δ /ORL-1 partial agonist)HAS NO ANALGESIC EFFICACY IN MU RECEPTOR KO MICE
0
3
6
9
12
15
Baseline 0.1 mg/kg0.3 mg/kg 1 mg/kg 3 mg/kg
Buprenorphine (s.c.)
Tail
flick
late
ncy
(sec
)
WTMuKO

0
3
6
9
12
Cut off
Baseline 0.1 0.3 1 3Bup. (mg/kg s.c.)
WTORL-1KO
Bup. (0.3mg/kg s.c.)Baseline Cont.
0
3
6
9
12
WTORL-1KO
+J-113397
BUPRENORPHINE HAS INCREASED ANALGESIC EFFICACYIN ORL-1 RECEPTOR KO MICE
ORL-1 Receptor KO Mice Courtesy of Hiroshi Takeshima, J-113397 Ivy Carroll
Tail
flick
late
ncy
(sec
)

ACUTE OPIOID EFFECTSAnalgesia, AntitussiveConstipation, Euphoria,
Nausea*, Calming*Decreased Respiration
WITHDRAWAL
oxycontin, vicodin
heroin, morphine
Hyperalgesia, Dysphoria, Anxiety,Sweating, Runny nose, Chills,
Diarrhea, Nausea
CHRONIC OPIOID EFFECTSTolerance to acute effects,normalization of physiology &psychology in presence of drug
molecular
, cellula
r
and be
haviora
l
adapta
tions
relapse?
?
drug/actionassociations

LikingTaking the drug feels good
- is rewarding and/orsatisfies the reasons for
taking the drug.
WantingThe drug is desired for its
remembered effects (analgesia,rewarding, calming, combating
withdrawal, physiologic effect).In extreme cases this can
become craving
HabitTaking the drug as a result of
automatic response to a stimulus -after eating - smoke
Stressed or anxious - drink ortake a vicodin

REWARD(CPP)
Activation of Mesolimbic Dopamine system
CB-1 and NK-1receptor activation by
endogenous ligands
THCNicotineAlcohol
Mu receptoractivation by
endogenous opioids
Morphine/HeroinCB-1AChGABA/NMDA Mu Opioid
Receptors
Kappareceptoractivation
AVERSION
AntagonismNaloxone
SYSTEM INTERDEPENDANCE FOR REWARD

Methadone Maintained Patients are Hyperalgesicin Cold Pressor Test.
0
10
20
30
40
50
60
70
Control
MM
*
***
***
Detection Tolerance Detection Tolerance
0 HOURS 3 HOURS
•••
•••
COLD PRESSOR TEST
••• p<0.0001
***p<0.0001
*p=0.023
T
i
m
e
(
s
e
c
o
n
d
s
)
Tim
e in
ice-
cold
wat
er (s
econ
ds)
Slide kindly provided by Walter Ling, UCLA
3hr after Methadone
PainDetection
PainTolerance
PainDetection
PainTolerance
Control
MethadoneMaintained

0
1
2
3
4
5
salinecontrol
chronic morphine
base
line
tail
with
draw
alLa
tenc
y (s
)
hot p
late
late
ncy
(s)
0
5
10
15
20
25
30
salinecontrol
chronic morphine
150’ post-morphine
A B
Hyperalgesia Following Chronic Morphine (TAD)- Pain Paradigm Specific
48ºC
**
*

[cAM
P ] % C
HANGE
FORSKOLIN-STIMULATED cAMP ACCUMULATION FOLLOWING ACUTEAND CHRONIC OPIOID TREATMENT - CYCLASE SUPERSENSITIVITY
RTI-1d
0
100
[DAMGO]
Control
Acute:opiod +forskolin
400
200
300
Chronic: 24hopioid thenwash out+forskolin
0.1nM 1nM 10nM 100nM

100+proteins100+proteins
MU OPIOID RECEPTOR COMPLEX (diversity)
SIGNALING8+proteins
100+proteins
COMPLEX DETERMINATION
1. Cellular Proteome2. Mu receptor alternative splicing3. Cellular Compartment4. Oligomerization (Hetro/Homo)5. The Receptor Activation State6. History of Receptor/Environment
Arrestins/G-proteins/GRK’s/Src’s/RGS’s
TRAFFICKING2+proteins
REGULATION5+proteins
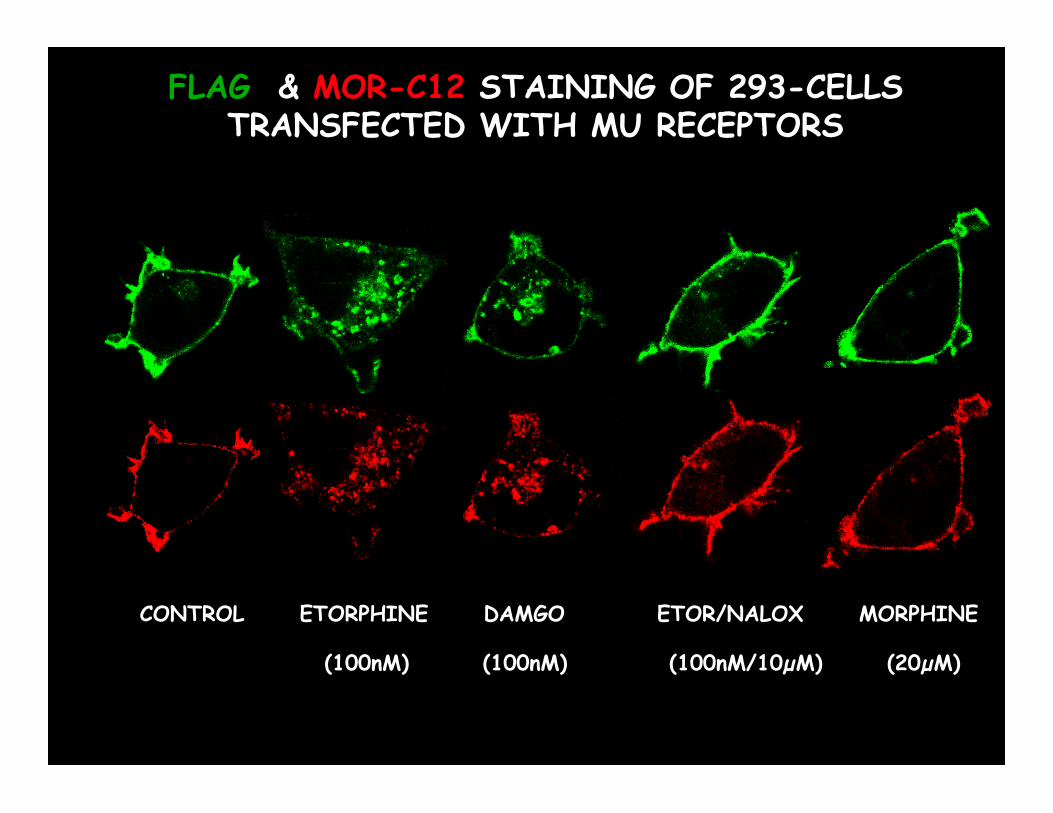
FLAG & MOR-C12 STAINING OF 293-CELLSTRANSFECTED WITH MU RECEPTORS
CONTROL ETORPHINE DAMGO ETOR/NALOX MORPHINE
(100nM) (100nM) (100nM/10µM) (20µM)

Agonist Binding
P P
Beta-arrestin 1-2 (cSrc)
DesensitizedReceptor
Severing of CCV byDynamin
Recruitment ofClathrin
EndosomeP
Recycling (µ)
Uncoating ofCCV and Fusionwith Endosome
Dephosphorylation
LysosomesDownregulation (δ)
P P
GRK 2 (1-6)Phosphorylation
P
P
P
Re-sensitizedReceptor
Signaling Signaling Signaling
4 hr
0 min
µ α2A Merged
DAMGO
4 hr+PD16
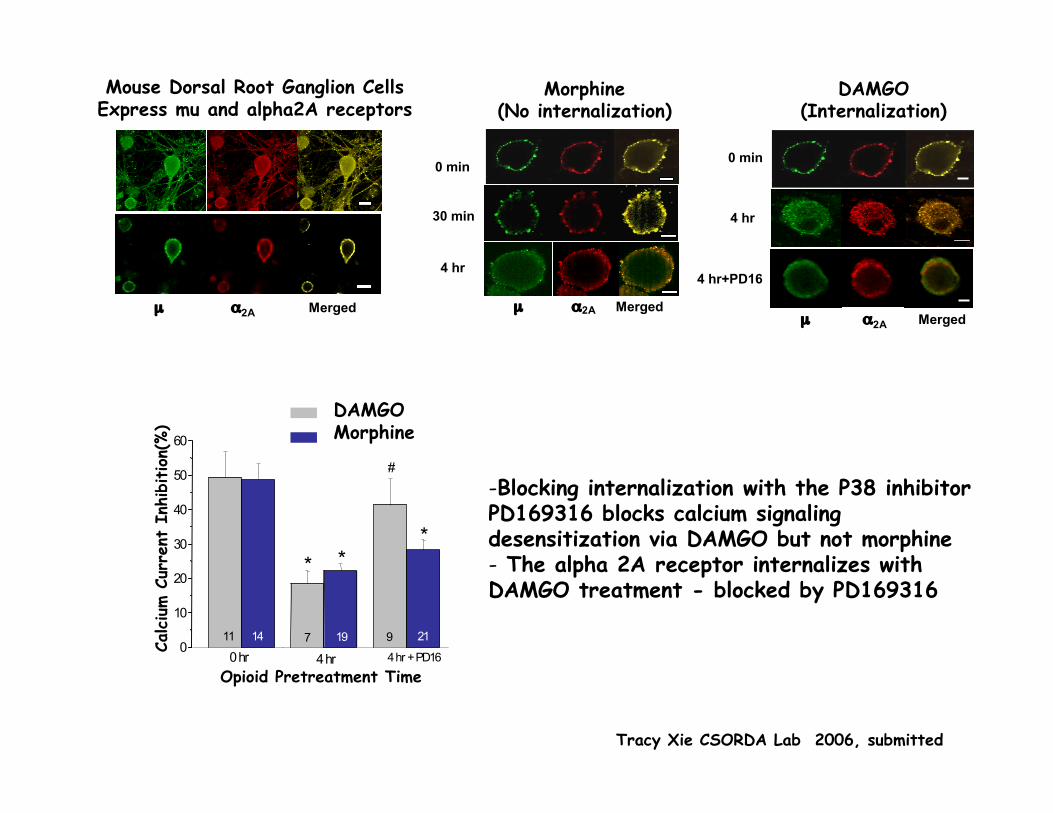
Tracy Xie CSORDA Lab 2006, submitted
µ α2A Merged
Mouse Dorsal Root Ganglion CellsExpress mu and alpha2A receptors
Opioid Pretreatment Time
Calcium C
urre
nt I
nhib
ition(
%)
DAMGOMorphine
0
10
20
30
40
50
60
*
#
**
9711 211914
4 hr + PD164 hr0 hr
0 min
30 min
4 hr
µ α2A Merged
Morphine
Morphine(No internalization)
DAMGO(Internalization)
-Blocking internalization with the P38 inhibitorPD169316 blocks calcium signalingdesensitization via DAMGO but not morphine- The alpha 2A receptor internalizes withDAMGO treatment - blocked by PD169316

4 hr
0 min
µ α2A Merged
DAMGO
0 min
µ α2A Merged
4 hr
Clonidine
Clonidine and DAMGO but not morphine induce both mu andalpha2A internalization and desensitization.
0
10
20
30
40
#
*
76120 hr 4 hr 4 hr+CT
Clonidine Challenge
0 hr 4 hr
Morphine Pretreated
1112
DAMGO Pretreated
Calcium C
urre
nt I
nhib
ition(
%)
0
10
20
30
40
50
60#
**
81862
4 hr0 hr 4 hr +Yoh4 hr +Yoh4 hr0 hr
Morphine testDAMGO test
#
*
7910
DAMGO Challenge
MorphineChallenge
Clonidine Pretreated
Calcium C
urre
nt I
nhib
ition(
%)
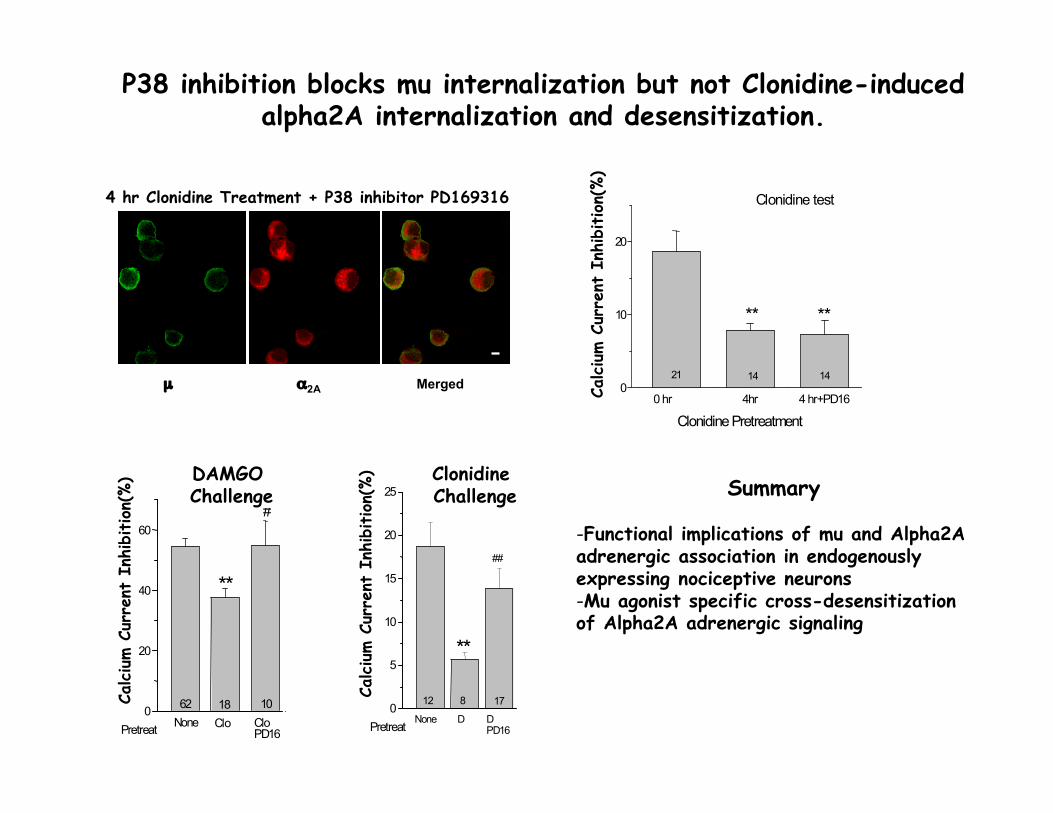
4 hr Clonidine Treatment + P38 inhibitor PD169316
µ α2A Merged
P38 inhibition blocks mu internalization but not Clonidine-inducedalpha2A internalization and desensitization.
0
20
40
60#
**
CloPD16
CloNonePretreat
101862
DAMGO Challenge
Calcium C
urre
nt I
nhib
ition(
%)
0
5
10
15
20
25
##
**
DPD16
17
PretreatDNone
812
Clonidine Challenge
Calcium C
urre
nt I
nhib
ition(
%)
0
10
20
****
Clonidine Pretreatment
Clonidine test
0 hr 4hr 4 hr+PD16
141421
Summary
-Functional implications of mu and Alpha2Aadrenergic association in endogenouslyexpressing nociceptive neurons-Mu agonist specific cross-desensitizationof Alpha2A adrenergic signaling
Calcium C
urre
nt I
nhib
ition(
%)

?Sugar Sugar
Sugar
noyes noyesSugar Sugar
Sugar
Mu opiate receptor knockout mice.- Lack reward-directed behaviors to many rewarding drugs- Phenotype of sibling response to mother absence
Sugar
15 20 25 30 35 40 45 500
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 10
1st 10 rewards Blocks of 5 rewards
MU -/-WT
Leve
r pre
ss p
er m
in
Acquisition
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0NonDEV
MOR WT
Leve
r pre
sses
per
min
0
1
2
3
4
5
6
7
1 2 3 4 5
4-min bins
devnon
devnon
MOR
WT
DevaluationExtinction Punishment
Maidment and Balleine Labs CSORDA 2006
Role of Opioid System in Habit and Goal-Directed Behaviors
grain
graingrain
grain
grain
grain
grain

Enkephalin knockout mice.
sugar grainsugar
? SugarSugar
Sugar piles upin food tray inEnk-KO trials
grain grain sugar
1h 10’ 10’
No food
Sugar SugarSugar
noyes noyesSugar Sugar
grain
graingrain
grain
grain
grain
grain

Summary
100
Dev
alua
tion
% to
tal r
espo
ndin
g
Retrieved value: Extinction
0
20
40
60
80
10
30
50
70
90DevaluedValued
D V
WT
D V
pENK
D V
Mu
0
20
40
60
80
10
30
50
70
90
DevaluedValued
D V
WT
D V
pENK
D V
Mu
Punishment
Mu -/- appear to have a problem with retrieving reward value:They are sensitive to changes in value but are unable to retrieve changes in a test of free recallbut can when the outcome is delivered.
pENK -/- are unable to control their actions when faced with lack of salience. They appear tohave a specific problem with goal-directed actions. Performance is likely controlled by a stimulus-response process and is habitual.
100

�
WITHDRAWALSymptom alleviation NK-1antagonist hyperalgesia
REWARD/ANALGESIAKappa antagonists?(JD-Tic)
� PLASTICITYENVIRONMENTDRUG ACCESS�
�
Adaptive Changes. Tolerance.Salience for rewards likelydisruptedPartial Agonists?Mu-agonists that show selectivesignaling and trafficking
�
1) +NK-1/CB-1 antagonist2) Slow on and off rate +/-3) Partial agonist - safety
RELAPSE
�