Embed Size (px)
Citation preview

OPIOID ANALGESICS
Dr. Hazar 2011

NEURAL MECHANISMS OF PAIN
• Pain is a subjective experience, hard to define exactly, even though we all know what we mean by it. Typically, it is a direct response to an untoward event associated with tissue damage, such as injury, inflammation or cancer, but severe pain can arise independently of any obvious predisposing cause (e.g. trigeminal neuralgia), or persist long after the precipitating injury has healed (e.g. phantom limb pain).

• It can also occur as a consequence of brain or nerve injury (e.g. following a stroke or herpes infection). Painful conditions of the latter kind, not directly linked to tissue injury, are very common and a major cause of disability and distress, and in general they respond less well to conventional analgesic drugs than do conditions where the immediate cause is clear. In these cases, we need to think of pain in terms of disordered neural function, comparable with schizophrenia or epilepsy, rather than simply as a 'normal' response to tissue injury.

• Therefore it is useful to distinguish two components, either or both of which may be involved in pathological pain states:
• the peripheral nociceptive afferent neuron, which is activated by noxious stimuli
• the central mechanisms by which the afferent input generates a pain sensation

Mechanisms of pain and nociception
• Nociception is the mechanism whereby noxious peripheral stimuli are transmitted to the central nervous system. Pain is a subjective experience not always associated with nociception.
• Polymodal nociceptors (PMNs) are the main type of peripheral sensory neuron that responds to noxious stimuli. The majority are non-myelinated C fibres whose endings respond to thermal, mechanical and chemical stimuli.

• Chemical stimuli acting on PMNs to cause pain include bradykinin, protons, ATP and vanilloids (e.g. capsaicin ). PMNs are sensitised by prostaglandins, which explains the analgesic effect of aspirin-like drugs, particularly in the presence of inflammation.
• The vanilloid receptor TRPV1 (transient receptor potential vanilloid receptor 1) responds to noxious heat as well as capsaicin-like agonists. The lipid mediator anandamide is an agonist at vanilloid receptors, as well as being an endogenous cannabinoid receptor agonist.

• Nociceptive fibres terminate in the superficial layers of the dorsal horn, forming synaptic connections with transmission neurons running to the thalamus.
• PMN neurons release glutamate (fast transmitter) and various peptides (especially substance P) that act as slow transmitters. Peptides are also released peripherally and contribute to neurogenic inflammation.
• Neuropathic pain, associated with damage to neurons of the nociceptive pathway rather than an excessive peripheral stimulus, is frequently a component of chronic pain states and may respond poorly to opioid analgesics





Modulation of pain transmission
• Transmission in the dorsal horn is subject to various modulatory influences, constituting the 'gate control' mechanism.
• Descending pathways from the midbrain and brain stem exert a strong inhibitory effect on dorsal horn transmission. Electrical stimulation of the midbrain periaqueductal grey area causes analgesia through this mechanism.

• The descending inhibition is mediated mainly by enkephalins, 5-hydroxytryptamine, noradrenaline and adenosine . Opioids cause analgesia partly by activating these descending pathways, partly by inhibiting transmission in the dorsal horn, and partly by inhibiting excitation of sensory nerve terminals in the periphery.
• Repetitive C-fibre activity facilitates transmission through the dorsal horn ('wind-up') by mechanisms involving activation of NMDA and substance P receptors



Opioid analgesics
• Opioid drugs include: – phenanthrene derivatives structurally related to
morphine – synthetic compounds with a variety of dissimilar
structures but similar pharmacological effects.
• Important morphine-like agonists include diamorphine and codeine; other structurally related compounds are partial agonists (e.g. nalorphine and levallorphan) or antagonists (e.g. naloxone).

• The main groups of synthetic analogues are the piperidines (e.g. pethidine and fentanyl), the methadone-like drugs, the benzomorphans (e.g. pentazocine) and the thebaine derivatives (e.g. buprenorphine ).
• Opioid analgesics may be given orally, by injection, or intrathecally to produce analgesia.

Opioid receptors• μ-Receptors are thought to be responsible for most of the
analgesic effects of opioids, and for some major unwanted effects (e.g. respiratory depression, euphoria, sedation and dependence). Most of the analgesic opioids are μ-receptor agonists.
• δ-Receptors are probably more important in the periphery but may also contribute to analgesia.
• κ-Receptors contribute to analgesia at the spinal level and may elicit sedation and dysphoria, but produce relatively few unwanted effects and do not contribute to dependence. Some analgesics are relatively κ-selective.
• σ-Receptors are not true opioid receptors but are the site of action of certain psychotomimetic drugs, with which some opioids interact.

• All opioid receptors are linked through G-proteins to inhibition of adenylate cyclase. They also facilitate opening of potassium channels (causing hyperpolarisation) and inhibit opening of calcium channels (inhibiting transmitter release). These membrane effects are not linked to the decrease in cAMP formation.
• Functional heterodimers, formed by combination of different types of opioid receptor, may occur and give rise to further pharmacological diversity.

Actions of morphine
• The main pharmacological effects are: – analgesia – euphoria and sedation – respiratory depression and suppression of cough – nausea and vomiting – pupillary constriction – reduced gastrointestinal motility, causing
constipation – histamine release, causing bronchoconstriction
and hypotension.

• The most troublesome unwanted effects are constipation and respiratory depression.
• Morphine may be given by injection (intravenous or intramuscular) or by mouth, often as slow-release tablets.
• Acute overdosage with morphine produces coma and respiratory depression.
• Morphine is metabolised to morphine-6-glucuronide, which is more potent as an analgesic.
• Morphine and morphine-6-glucuronide are the active metabolites of diamorphine and codeine.

Tolerance and dependence
• Tolerance develops rapidly, accompanied by physical withdrawal syndrome.
• The mechanism of tolerance may involve adaptive up-regulation of adenylyl cyclase. It is not pharmacokinetic in origin, and receptor down-regulation is not a major factor.
• Dependence is satisfied by μ-receptor agonists, and the withdrawal syndrome is precipitated by μ-receptor antagonists.

• Dependence comprises two components: (i) physical dependence, associated with the withdrawal syndrome and lasting for a few days; and (ii) psychological dependence, associated with craving and lasting for months or years. Psychological dependence rarely occurs in patients being given opioids as analgesics.
• Weak, long-acting μ-receptor agonists such as methadone may be used to relieve withdrawal symptoms.
• Certain opioid analgesics, such as codeine, pentazocine, buprenorphine and tramadol, are much less likely to cause physical or psychological dependence.

Opioid antagonists
• Pure antagonists include naloxone (short acting) and naltrexone (long acting). They block μ, δ and κ-receptors more or less equally. Selective antagonists are available as experimental tools.
• Other drugs, such as nalorphine and pentazocine, produce a mixture of agonist and antagonist effects.

• Naloxone does not affect pain threshold normally but blocks stress-induced analgesia and can exacerbate clinical pain.
• Naloxone rapidly reverses opioid-induced analgesia and respiratory depression, and is used mainly to treat opioid overdose or to improve breathing in newborn babies affected by opioids given to the mother.
• Naloxone precipitates withdrawal symptoms in morphine-dependent patients or animals. Pentazocine may also do this.

Other analgesic drugs
• Paracetamol resembles non-steroidal anti-inflammatory drugs and is effective as an analgesic, but it lacks anti-inflammatory activity. It may act by inhibiting cyclo-oxygenase (COX)-3, a splice variant of COX-1, but probably has other effects as well. In overdose, it causes hepatotoxicity.

• Various antidepressants (e.g. amitriptyline), as well as antiepileptic drugs (e.g. carbamazepine , gabapentin ), are used mainly to treat neuropathic pain.
• Other drugs occasionally used include the NMDA receptor antagonist ketamine and the local anaesthetic drug lignocaine (lidocaine

History of Opioids
• Opium is extracted from poppy seeds (Paper somniforum)
• Used for thousands of years to produce:– Euphoria– Analgesia– Sedation– Relief from diarrhea– Cough suppression

History cont’d
• Used medicinally and recreationally from early Greek and Roman times
• Opium and laudanum (opium combined with alcohol) were used to treat almost all known diseases
• Morphine was isolated from opium in the early 1800’s and since then has been the most effective treatment for severe pain

History and Background
• Invention of the hypodermic needle in 1856 produced drug abusers who self administered opioids by injection
• Controlling the widespread use of opioids has been unsuccessful because of the euphoria, tolerance and physiological dependence that opioids produce

Terminology
• “opium” is a Greek word meaning “juice,” or the exudate from the poppy
• “opiate” is a drug extracted from the exudate of the poppy
• “opioid” is a natural or synthetic drug that binds to opioid receptors producing agonist effects

Natural opioids occur in 2 places:
• 1) In the juice of the opium poppy (morphine and codeine)
• 2) As endogenous endorphins
• All other opioids are prepared from either morphine (semisynthetic opioids such as heroin) or they are synthesized from precursor compounds (synthetic opioids such as fentanyl)

Pharmacological Effects
• Sedation and anxiolysis– Drowsiness and lethargy– Apathy– Cognitive impairment– Sense of tranquility
• Depression of respiration– Main cause of death from opioid overdose– Combination of opioids and alcohol is especially dangerous
• Cough suppression– Opioids suppress the “cough center” in the brain
• Pupillary constriction– pupillary constriction in the presence of analgesics is
characteristic of opioid use

Pharmacological effects cont’d.
• Nausea and vomiting– Stimulation of receptors in an area of the medulla called the
chemoreceptor trigger zone causes nausea and vomiting– Unpleasant side effect, but not life threatening
• Gastrointestinal symptoms– Opioids relieve diarrhea as a result of their direct actions on the
intestines
• Other effects– Opioids can release histamines causing itching or more severe
allergic reactions including bronchoconstriction– Opioids can affect white blood cell function and immune function

Mechanism of action
• Activation of peripheral nociceptive fibers causes release of substance P and other pain-signaling neurotransmitters from nerve terminals in the dorsal horn of the spinal cord
• Release of pain-signaling neurotransmitters is regulated by endogenous endorphins or by exogenous opioid agonists by acting presynaptically to inhibit substance P release, causing analgesia



Primary Effect of Opioid Receptor Activation
• Reduction or inhibition of neurotransmission, due largely to opioid-induced presynaptic inhibition of neurotransmitter release
• Involves changes in transmembrane ion conductance– Increase potassium conductance (hyperpolarization)– Inactivation of calcium channels

Three Opioid Receptors
• Mu
• Kappa
• Delta

Delta Receptor
• It is unclear what delta’s responsible for.
• Delta agonists show poor analgesia and little addictive potential
• May regulate mu receptor activity

Mu-Receptor: Two Types
• Mu-1– Located outside spinal
cord– Responsible for
central interpretation of pain
• Mu-2– Located throughout
CNS– Responsible for
respiratory depression, spinal analgesia, physical dependence, and euphoria

Kappa Receptor
• Only modest analgesia
• Little or no respiratory depression
• Little or no dependence
• Dysphoric effects

Mu and Kappa Receptor Activation
Response Mu-1 Mu-2 Kappa
Analgesia
Respiratory Depression
Euphoria
Dysphoria
Decrease GI motility
Physical Dependence

Mu and Kappa Receptors
DRUGS MU KAPPA
Pure Agonists Agonist Agonist
Agonist-Antagonist
Antagonist Agonist
Pure Antagonists
Antagonist Antagonist

Terminology
• Pure Agonist: has affinity for binding plus efficacy
• Pure Antagonist: has affinity for binding but no efficacy; blocks action of endogenous and exogenous ligands
• Mixed Agonist-Antagonist: produces an agonist effect at one receptor and an antagonist effect at another
• Partial Agonist: has affinity for binding but low efficacy

AGONISTS
*Morphine
*Heroin
*Hydromorphone
*Fentanyl
*Codeine
*

General Pharmacokinetics
• LATENCY TO ONSET• *oral (15-30 minutes)• *intranasal (2-3 minutes)• *intravenous (15 – 30 seconds)• *pulmonary-inhalation (6-12 seconds)• DURATION OF ACTION – anywhere between 4 and 72
hours depending on the substance in question.• Metabolism – hepatic via phase 1 and phase 2
biotransformations to form a diverse array of metabolites ( ex., morphine to morphine-6-glucuronide).

Morphine• PHARMACOKINETICS• Routes of administration (preferred) *Oral- latency to onset –(15 – 60 minutes ) • * also sniffed, swallowed and injected. • * duration of action – ( 3 – 6 hours)• * First-pass metabolism results in poor • availability from oral dosing.• * 30% is plasma protein bound• EFFECTS AND MEDICAL USES• *symptomatic relief of moderate to severe pain• *relief of certain types of labored breathing• *suppression of severe cough (rarely)• *suppression of severe diarrhea • *AGONIST for mu, kappa, and delta receptors.

Hydromorphone• PHARMACOKINETICS• *Routes of administration (Preferred)• *Oral -latency to onset (15 – 30 minutes) • *Intravenous-Duration of Action (3-4 hours)• *Peak effect (30-60 minutes)• PROPERTIES AND EFFECTS • * potent analgesic like morphine but is 7-10
times as potent in this capacity.• *used frequently in surgical settings for
moderate to severe pain. (cancer, bone trauma, burns, renal colic.)

Fentanyl• Pharmacokinetics• Routes of Administration * Oral, and transdermal & possibly I.V *Highly lipophilic *latency to onset (7-15 min. oral; 12-17 hrs transdermal *duration of action ( 1-2 hours oral; 72 transdermal) *80 – 85% plasma protein bound *90 % metabolized in the liver to inactive metabolites Other properties * 80 times the analgesic potency of morphine and 10 times the analgesic potency of hydromorphone. *high efficacy for mu 1 receptors. *most effective opiate analgesic

Antagonists
• Naloxone
• Naltrexone

Naltrexone• PHARMACOKINETICS• *latency to onset (oral tablet 15-30 min.)• *duration of action 24-72 hours• *peak effect (6-12 hours)• STRUCTURAL DISTINCTION• *Differs from naloxone insofar as the• allyl group on the nitrogen atom is supplanted • by a cyclopromethyl group.• EFFECTS• *Reverses the psychotomimetic effects of opiate • agonists.• * Reverses hypotension and cardiovascular instability• secondary to endogeneous endorphins (potent
vasodilators)• *inhibits Mu, Delta, and Kappa receptors.

Tolerance and Dependence



Tolerance • Tolerance is a diminished responsiveness to the
drug’s action that is seen with many compounds• Tolerance can be demonstrated by a decreased
effect from a constant dose of drug or by an increase in the minimum drug dose required to produce a given level of effect
• Physiological tolerance involves changes in the binding of a drug to receptors or changes in receptor transductional processes related to the drug of action
• This type of tolerance occurs in opioids

Tolerance continued• Molecular basis of tolerance involves glutaminergic
mechanisms (glutamate-excitatory amino acid neurotransmitter)
• 1997, Gies and colleagues stated that activation of glutamate NMDA receptors correlates with resistance to opioids and the development of tolerance
• Mu-receptor mRNA levels are regulated by activation of these receptors
• NMDA receptor blocker ketamine prevented the development of this late-onset and long-lasting enhancement in pain sensitivity after the initial analgesia effect dissipated

Tolerance continued• Thus, glutaminergic NMDA receptors MAY regulate
mu-receptor mRNA, accounting for the development of tolerance to the continuous presence of opioid
• Cross-tolerance is the condition where tolerance for one drug produces tolerance for another drug – person who is tolerant to morphine will also be tolerant to the analgesic effect of fentanyl, heroin, and other opioids
• * note that a subject may be physically dependent on heroin can also be administered another opioid such as methadone to prevent withdrawl reactions
• Methadone has advantages of being more orally effective and of lasting longer than morphine or heroin

Tolerance continued • Methadone maintenance programs allow heroin
users the opportunity to maintain a certain level of functioning without the withdrawl reactions
• Although most opioid effects show tolerance, locomotor stimulation shows sensitization with repeated opioid administration
• Toxic effects of opioids are primarily from their respiratory depressant action and this effect shows tolerance with repeated opioid use
• Opioids might be considered “safer” in that a heroin addicts drug dose would be fatal in a first-time heroin user

Dependence• Physiological dependence occurs when
the drug is necessary for normal physiological functioning – this is demonstrated by the withdrawl reactions
• Withdrawl reactions are usually the opposite of the physiological effects produced by the drug

• Psychological factors involved in drug dependence

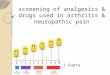
Biochemical mechanism postulated to explain morphine tolerance and dependence. Morphine inhibits adenylyl cyclase, thus reducing cAMP formation
(green line). A secondary rise in adenylyl cyclase expression occurs (red line), so that cAMP production recovers in the presence of morphine (i.e. tolerance
develops). On cessation of morphine treatment, excessive cAMP production occurs, causing withdrawal symptoms, until the high level of adenylyl cyclase expression returns to normal. Later work has shown that other elements in the
cAMP signalling pathway, in addition to adenylyl cyclase itself, are similarly affected by chronic drug exposure, in vivo as well as in vitro.

Cellular and physiological mechanisms involved in drug dependence showing the relationship between
the immediate and delayed effects of drug-taking and drug withdrawal. DA, dopamine.

Drug dependence• Dependence is defined as a compulsive craving that develops as
a result of repeated administration of the drug. • Dependence occurs with a wide range of psychotropic drugs,
acting by many different mechanisms. • The common feature of dependence-producing drugs is that they
have a positive reinforcing action ('reward') associated with activation of the mesolimbic dopaminergic pathway.
• Dependence is often associated with (i) tolerance to the drug, which can arise by various biochemical mechanisms; (ii) a physical abstinence syndrome, which varies in type and intensity for different classes of drug; (iii) psychological dependence (craving), which may be associated with the tolerance-producing biochemical changes.
• Psychological dependence, which usually outlasts the physical withdrawal syndrome, is the major factor leading to relapse among treated addicts.
• Although genetic factors contribute to drug-seeking behaviour, no specific genes have yet been identified

Clinical use of drugs in substance dependence؟؟؟
• Tobacco dependence: – short-term nicotine is the drug of choice as adjunct to behavioural therapy in
smokers committed to giving up – bupropion is also effective but lowers seizure threshold, so is contraindicated in
people with risk factors for seizures. • Alcohol dependence:
– long-acting benzodiazepines (e.g. chlordiazepoxide) can be used to reduce withdrawal symptoms and the risk of seizures; they should be tapered over 1-2 weeks and then discontinued because of their abuse potential
– disulfiram is used as an adjunct to behavioural therapy in suitably motivated alcoholics after detoxification; it is contraindicated for patients in whom a hypotensive acetaldehyde-induced reaction (p. 632) would be dangerous (e.g. those with coronary or cerebral vascular disease)
– acamprosate can help to maintain abstinence; it is started as soon as abstinence has been achieved and maintained if relapse occurs, and it is continued for 1 year.
• Opioid dependence: – opioid agonists or partial agonists (e.g., respectively, methadone and buprenorphine )
administered orally or sublingually may be substituted for injectable narcotics, many of whose harmful effects are attributable to the route of administration
– naltrexone, a long-acting opioid antagonist, is used as an adjunct to help prevent relapse in detoxified addicts (opioid-free for at least 1 week)
– lofexidine, an α2 agonist (cf. clonidine; Ch. 11) is used short term (usually up to 10 days) to ameliorate symptoms of opioid withdrawal, and is then tapered over a further 2-4 days

Pharmacology of nicotine• At a cellular level, nicotine acts on nicotinic acetylcholine
receptors (nAChRs), mainly of the α4β2 subtype, to cause neuronal excitation. Its central effects are blocked by receptor antagonists such as mecamylamine.
• At the behavioural level, nicotine produces a mixture of inhibitory and excitatory effects.
• Nicotine shows reinforcing properties, associated with increased activity in the mesolimbic dopaminergic pathway, and self-administration can be elicited in animal studies.
• Electroencephalography changes show an arousal response, and subjects report increased alertness accompanied by a reduction of anxiety and tension.
• Learning, particularly under stress, is facilitated by nicotine . • Peripheral effects of nicotine are due mainly to ganglionic
stimulation: tachycardia, increased blood pressure and reduced gastrointestinal motility. Tolerance develops rapidly to these effects.

• Nicotine is metabolised, mainly in the liver, within 1-2 hours. The inactive metabolite, cotinine, has a long plasma half-life and can be used as a measure of smoking habits.
• Nicotine gives rise to tolerance, physical dependence and psychological dependence (craving), and is highly addictive. Attempts at long-term cessation succeed in only about 20% of cases.
• Nicotine replacement therapy (chewing gum or skin patch preparations) improves the chances of giving up smoking but only when combined with active counsel

Harmful effects of smoking
• Smoking accounts for about 10% of deaths worldwide, mainly due to: – cancer, especially lung cancer, of which about 90% of
cases are smoking-related; carcinogenic tars are responsible
– ischaemic heart disease; both nicotine and carbon monoxide may be responsible
– chronic bronchitis; tars are mainly responsible. • Smoking in pregnancy reduces birth weight and retards
childhood development. It also increases abortion rate and perinatal mortality. Nicotine and possibly carbon monoxide are responsible.
• The incidence of Parkinson's disease is lower in smokers than in non-smokers

Cannabis• Main active constituent is Δ9-tetrahydrocannabinol
(THC), although pharmacologically active metabolites may be important.
• Actions on central nervous system (CNS) include both depressant and psychotomimetic effects.
• Subjectively, subjects experience euphoria and a feeling of relaxation, with sharpened sensory awareness.
• Objective tests show impairment of learning, memory and motor performance.
• THC also shows analgesic and antiemetic activity, as well as causing catalepsy and hypothermia in animal tests.
• Peripheral actions include vasodilatation, reduction of intraocular pressure, and bronchodilatation.

• Cannabinoid receptors belong to the G-protein-coupled receptor family, linked to inhibition of adenylyl cyclase and effects on calcium and potassium channel function, causing inhibition of synaptic transmission. The brain receptor (CB1) differs from the peripheral receptor (CB2), which is expressed mainly in cells of the immune system. Selective agonists and antagonists have been developed.
• Anandamide, an arachidonic acid derivative, is an endogenous ligand for the CNS cannabinoid receptor; its function has not yet been ascertained.
• Cannabinoids are less liable than opiates, nicotine or alcohol to cause dependence but may have long-term psychological effects.
• Nabilone , a THC analogue, has been developed for its antiemetic property.
• Although cannabinoids are not available for clinical use, trials are in progress for symptomatic treatment of multiple sclerosis and AIDS.

Withdrawl ReactionsAcute Action
• Analgesia• Respiratory Depression• Euphoria• Relaxation and sleep• Tranquilization• Decreased blood pressure• Constipation• Pupillary constriction• Hypothermia• Drying of secretions• Reduced sex drive• Flushed and warm skin
Withdrawl Sign• Pain and irritability• Hyperventilation• Dysphoria and depression• Restlessness and insomnia• Fearfulness and hostility• Increased blood pressure• Diarrhea• Pupillary dilation• Hyperthermia• Lacrimation, runny nose• Spontaneous ejaculation• Chilliness and “gooseflesh”

Dependence continued• Acute withdrawl can be easily precipitated in drug dependent
individuals by injecting an opioid antagonist such as naloxone or naltrexone – rapid opioid detoxification or rapid anesthesia aided detoxification
• The objective is to enable the patient to tolerate high doses of an opioid antagonist and undergo complete detox in a matter of hours while unconscious
• After awakening, the person is maintained on orally administered naltrexone to reduce opioid craving