Embed Size (px)
Citation preview

Sahand Ensafi PA, CCPA, B.H.Sc.,Department of Emergency Medicine,
University Health Network
Assistant Professor, DFM, PAEP, McMaster University
ePBL Facilitator, PA Program, University of Toronto
OPHTHALMOLOGY:
PEARLS & PITFALLS

SPECIAL THANKS
• Dr. Jason Kwok, Resident Physician, Department of
Ophthalmology and Vision Services, University of Toronto
• UHN Department of Ophthalmology

DISCLOSURES
• No Disclosures

Overview
• 3 Cases
• Common ED Eye
Presentations
• Emphasis on common pitfalls and
how to improve

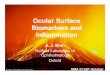
CASE 1
• 65 year-old male with sudden onset of painless vision “loss”
in right eye.

CRAO - PITFALLS
• Lack of timely assessment
of “vision loss”
• Incomplete assessment of
visual acuity
• Hours before “classic”
findings

CRAO - PEARLS
• High index of suspicion
• CRAO = History
• Sudden/severe vision loss
• CF HM LP
• RAPD

CRAO – ACT FAST
• STROKE of the eye
• CBC, lytes, coags, ECG
• ?GCA
• Consider ESR/CRP
especially if age > 50
• Time is of the essence


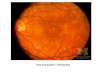
CASE 2
• 62 year-old female with gradually increasing
“deep/boring” right-eye pain and redness x 2
weeks.

RED EYE - PITFALLS
• Locking on benign causes vs
glaucoma
• Quick to diagnose
“conjunctivitis”
• Incomplete History
• Lack of physical exam

?SCLERITIS ?EPISCLERITIS

CASE 2: SCLERITIS
• Severe pain
• ?Connective Tissue Disease
• Scleral Thinning
• Vision Changes
• ?Phenylephrine
• Fixed vessels

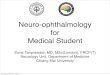
CASE 3
• 45 year-old, myopic male with flashes and floaters in the
right eye x 1day. No curtain or VF defect. Visual Acuity –
10/25 Right and 10/10 Left.

FLASHES/FLOATERS - PITFALLS
• Lack of guidelines around referral / follow-up

CASE 3 - ?RETINAL DETACHMENT
• Follow – up?
• 1. Hollands H, et al. Acute-Onset Floaters and Flashes: Is this Patient at Risk for
Retinal Detachment? JAMA 2009;302(20):2243-2249.

FOLLOW – UP: TAKE HOME MESSAGE
• Flashes and Floaters?
High risk features – urgent referral
1) Subjective or objective decrease in vision
2) Visual field defect
Low risk features – elective referral (1 - 2 weeks)
1) Stable symptoms (weeks to months)
2) Absence of high risk features above

SUMMARY
Acute Vision Loss
• High index of suspicion for CRAO
• If truly acute – act fast!
Red Eye
• Severe Pain
• Blue hue
• Fixed Vessels
Flashes/Floaters
• Subjective or objective vision change or visual field defect?

THANK YOU!

REFERENCES
• Friedman, Neil J., Peter K. Kaiser, and Roberto Pineda. The Massachusetts Eye and Ear Infirmary Illustrated Manual of Ophthalmology. Philadelphia, PA: Saunders/Elsevier, 2009. PDF.
• Hockberger, Robert S., and Ron M. Walls. "Acute Visual Loss." Rosen's Emergency Medicine - Concepts and Clinical Practice 8th Ed. Ed. John A. Marx. 8th ed. Vol. 1. N.p.: Elsevier, n.d. 968-81. Print.
• Hollands H, et al. Acute-Onset Floaters and Flashes: Is this Patient at Risk for Retinal Detachment? JAMA 2009;302(20):2243 -2249.
• Jogi, Renu. Basic Ophthalmology. New Delhi: Jaypee Brothers Medical, n.d. PDF.
• Long, Brit. "Acute Visual Loss in the Emergency Department: Pearls and Pitfalls - Emdocs." Emdocs. Emdocs, 26 Apr. 2016. Web. 10 Oct. 2016.
• Tintinalli, Judith E. "Eye Emergencies." Tintinallis Emergency Medicine A Comprehensive Study Guide . 7th ed. N.p.: McGraw Hill, 2011. 1517+. Print.
• Tsai, James C. Oxford American Handbook of Ophthalmology. Oxford: Oxford UP, 2011. Print.
• Hockberger, Robert S., and Ron M. Walls. ”Red and Painful Eye." Rosen's Emergency Medicine - Concepts and Clinical Practice 8th Ed. Ed. John A. Marx. 8th ed. Vol. 1. N.p.: Elsevier, n.d. Print.
• Pflipsen, Matthew, et al. “Evaluation of the Painful Eye.” American Family Physician, 15 June 2016, www.aafp.org/afp/2016/0615/p991.html.