Embed Size (px)
Citation preview
Ophthalmic Products
Dr. M. Wazaify, R Abu-Dahab
University of Jordan

Why study ophthalmic products?
Many common conditions cause ocular discomfort are minor and self-limiting.
However, relatively minor symptoms may be associated with severe, potentially blinding conditions
Thus, pharmacists should provide best possible guidance to patients who seek assistance in choosing between self-treatment or professional medical care

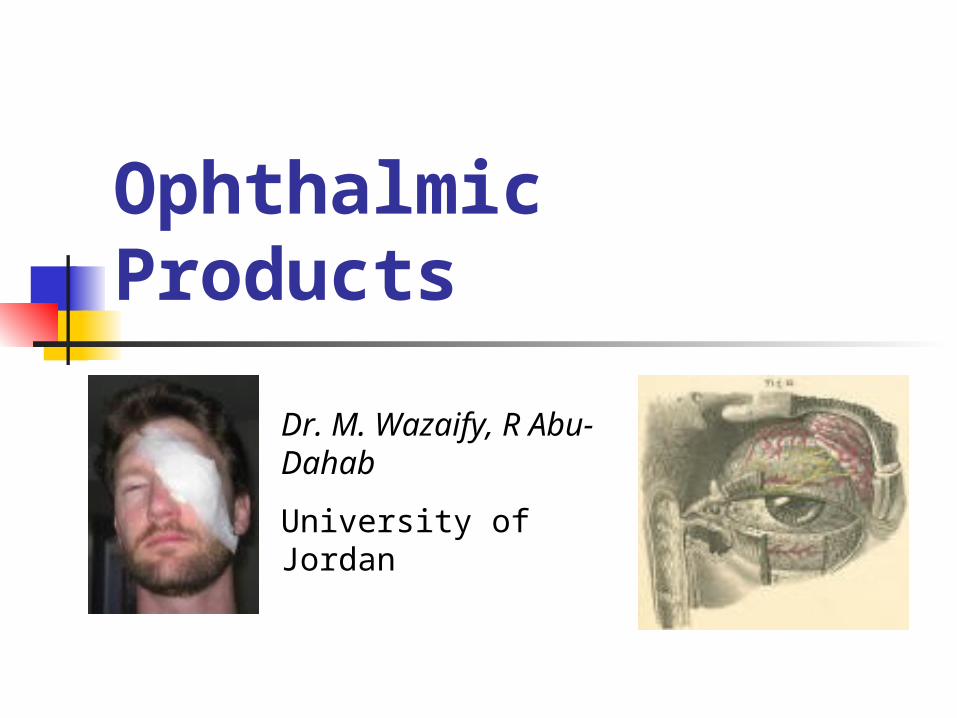
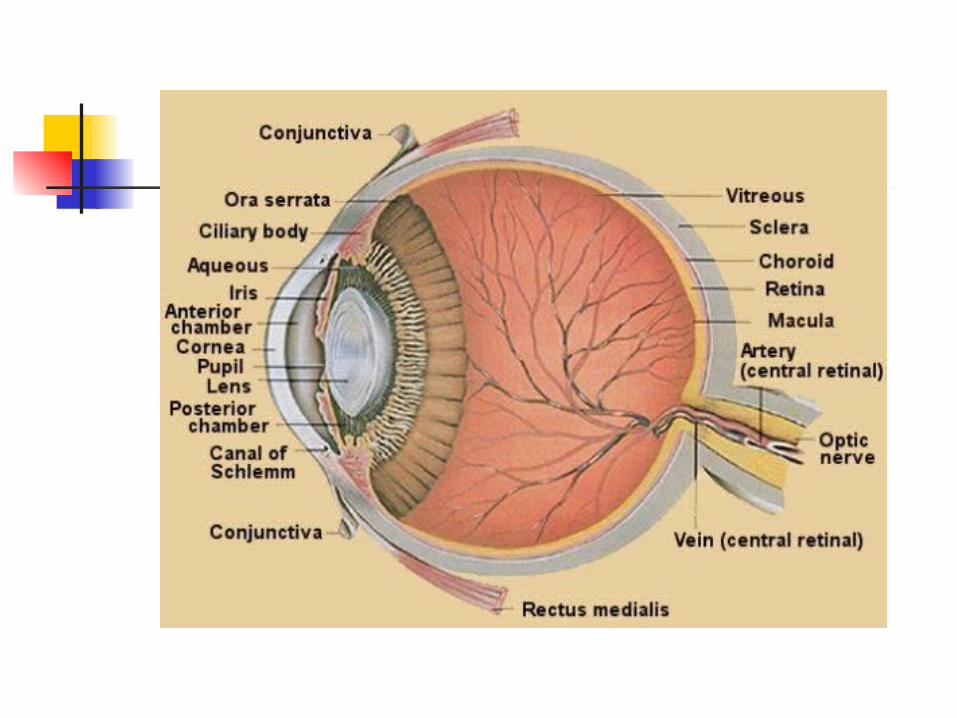
Eye Anatomy & Physiology
External Eye Location: susceptible to
environmental and microbial contamination
Many natural defence mechanisms to protect against such contamination:
1. Eyelids2. Eye-lashes3. Tears
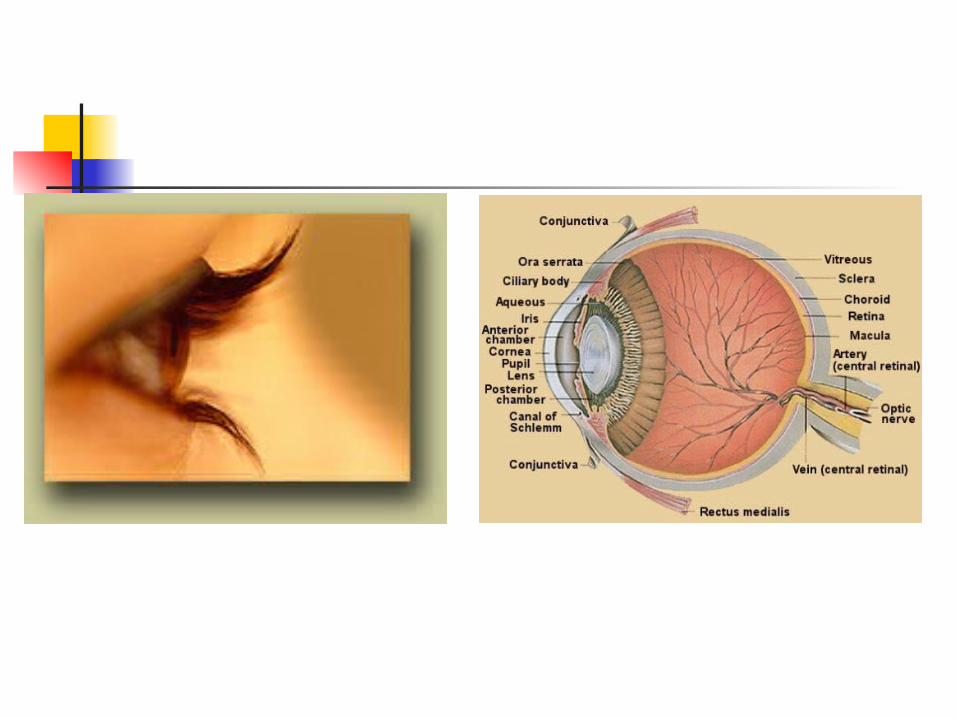
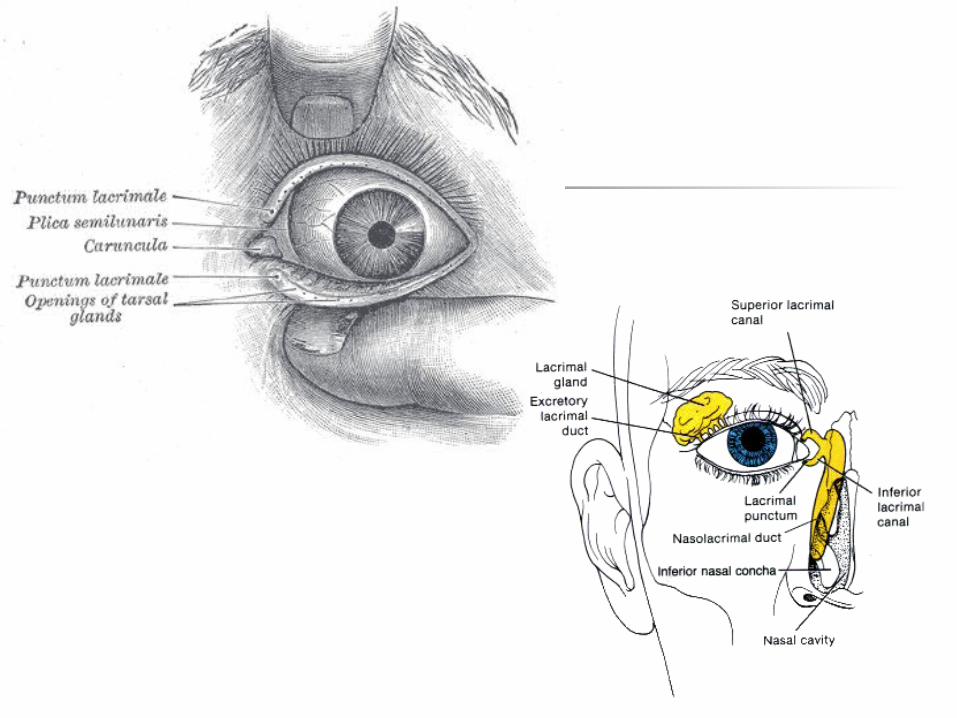
1. Eyelids a multi-layer tissue, covered
externally by the skin and internally by a thin, mucucutaneous epithelial layer (conjuctiva). It contains 5 glands: Meibomian, Zeis & Moll (sebaceous) + Krause & Wolfring’s (lacrimal)
The eyelids play important roles in the eye
1. Eyelids The functions of eyelid: (1) protect
front surface of the eye neural reflex mechanism blocks contaminants from reaching ocular surface(2) spread the tears produced by lacrimal glands(3) close by zipperlike manner force the tears towards the nose drainage
2. Eye-lashes Collect debris before it encounters the eye
N.B. The lacrimal drainage system is lined by a highly vascularised epithelium and & absorption into systemic circulation along this pathway gives rise to potential systemic effects of topically administered eye medication

3. Tears Functions of the tears:1. Lubricating ocular surface2. Provide mechanism for removing
debris drainage3. Potent antimicrobial action (e.g. IgA, enzymes)
Rate of tear production: 1-2 L/min (7-10 L is found on ocular surface at any point)
Upon irritation: tear production increases 300%

3. Tears The tear film is a tri-layer film: Outer (by sebaceous glands): lipid, prevent the
evaporation of the tears, Middle (by lacrimal lands): the largest layer,
aqueous, responsible for wetting properties Inner (by goblet cells): mucinous, allows the
lipid and aqueous layers to maintain adhesion across the cornea and conjuctiva
Abnormalities in any of these layers causes ocular discomfort
External Eye The visible external eye consists of the
sclera + cornea 1. Sclera: a tough, collagenous layer that
gives the eye rigidity & encases internal eye structures
Covered by 2 epithelial layers: epi-sclera + bulbar conjuctiva, contain the vascular & lymphatic systems of the anterior eye surface the source for visible eye redness during irritation & inflammation
External eye
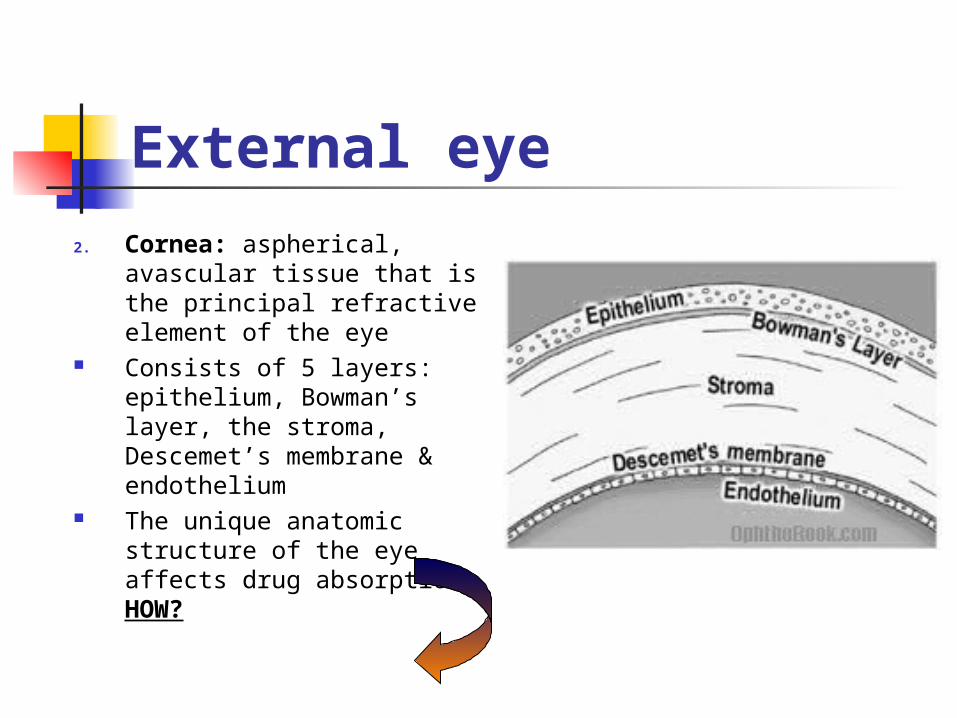
2. Cornea: aspherical, avascular tissue that is the principal refractive element of the eye
Consists of 5 layers: epithelium, Bowman’s layer, the stroma, Descemet’s membrane & endothelium
The unique anatomic structure of the eye affects drug absorption. HOW?
Drug absorption through cornea
Corneal epithelium is lipophilic: facilitates passage of fat-soluble drugsCorneal stroma is hydrophilic: allows passage of water-soluble drugs
Thus, optimum penetration of a drug through the cornea depends on biphasic solubility
Damage to corneal epithelium may markedly affect drug absorption rates
Comparative studies showed that drug penetration to the aqueous layer increased to threefold in compromised epithelium
Factors that may compromise epithelium:
Trauma Routine contact lens wear Topical ophthalmic anaesthetics Thermal or UV light exposure
Factors that may hinder efforts to maintain therapeutic drug level in the eye
1. Difficulty of drug to penetrate through the cornea
2. Dilution of the drug by reflex tearing (e.g. 2.5% NaCl 0.9-0.95% within 1-2 minutes)
3. Rapid removal of drug through the tear system
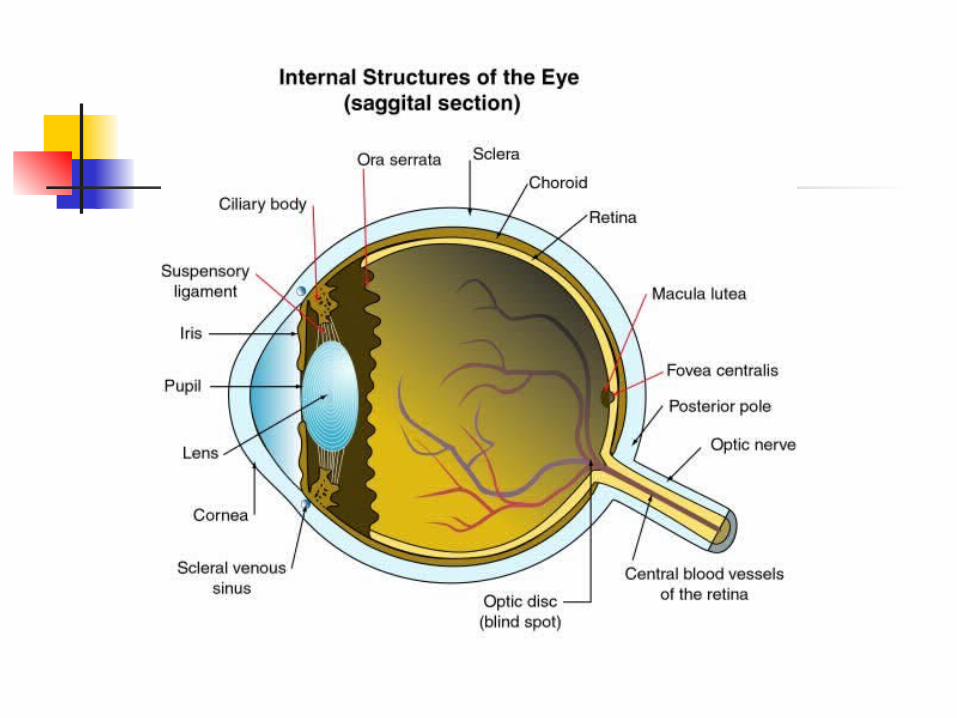
Internal Eye1. Anterior chamber (behind cornea): contains
aqueous humour a. maintains normal internal eye pressure; b. provides nutritional support for lens & cornea
2. Iris: visible coloured portion of the eye regulates light striking retina, contains 2 types of muscle (sphincter & dilator)
3. Pupil: central opening of iris, Prostaglandins secreted by iris during an inflammation stimulates sphincter muscles reduces the pupil diameter

Internal Eye4. Crystalline lens: avascular, biconvex
structure that alters its shape to focus light on retina “accommodation”
5. Ciliary body= ciliary muscle + epithelium
- the contraction of ciliary muscle helps in “accomodation”
- during inflamation spasm of ciliary muscle fluctuating vision and pain. Thus, inhibition of ciliary muscle (cycloplegia) by anticholinergic drugs frequent treatment drug of internal ocular inflammation
Internal Eye
6. Vitreous Body: (80% of total eye volume),
filled with vitreous humour, a gel like, fluid collagen matrix that helps maintain eye volume
7. Retina: multi-layer neural tissue that begins the visual pathways (capture light, rods & cons, photic message optic nerve to posterior cerebral cortex visual information decoded)

Common Ocular Disorders
• Eyelid Disorders
• Ocular Surface Disorders
• Internal Eye Conditions
Common Ocular Disorders Ocular inflammation and irritation can be
caused by many conditions, some of which can be treated safely and effectively by OTC drugs
OTC drugs relieve minor symptoms: burning, itching, stinging and watering
FDA suggested self-treatment indications:- tear insufficiency - blepharitis
- corneal edema - conjuctivitis- external inflammation & irritation- Hordeolum (stye)
Common Ocular Disorders
Referral is mandatory: Embedded foreign body Uveitis; ”uvea: middle coat of the eyeball, the
choroid, ciliary body & iris as a whole”
Flash burns Chemical burns Tear duct infection Corneal ulcer

IMPORTANT! Consumers should never self-treat
ophthalmic conditions more than 72 hours, especially if they were using ophthalmic decongestants (vasoconstrictors)
Care should be taken when counselling patients because many seemingly harmless ocular conditions can prove to be devastating
1. Eyelid Disorders:
Blunt Trauma: Highly vascularised eyelid blunt
traumableeding swelling and ocular discomfort Mostly, blunt trauma does not result in internal
damage & treatment is usually supportive: A. cold compresses; B. Oral OTC analgesics
However,all individuals should be evaluated by an optometrist or ophthalmologist ASAP after the event
Complications: internal eye bleeding, secondary glaucoma, retinal detachment
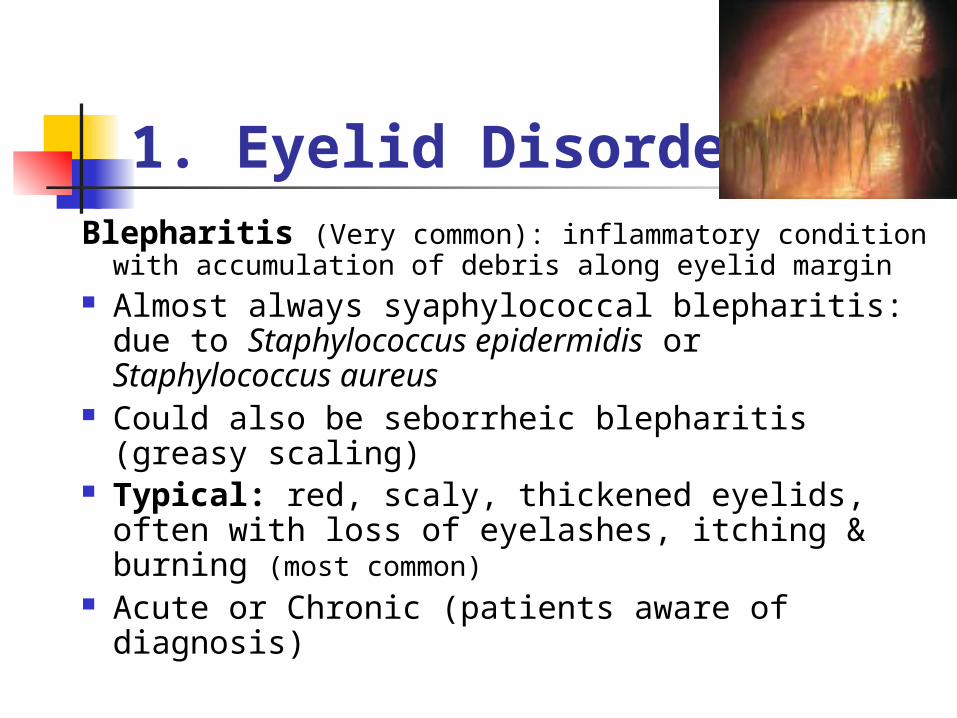
1. Eyelid Disorders:Blepharitis (Very common): inflammatory condition
with accumulation of debris along eyelid margin Almost always syaphylococcal blepharitis: due
to Staphylococcus epidermidis or Staphylococcus aureus
Could also be seborrheic blepharitis (greasy scaling)
Typical: red, scaly, thickened eyelids, often with loss of eyelashes, itching & burning (most common)
Acute or Chronic (patients aware of diagnosis)

Treatment: hot compress (2-4 times daily, 15 min. Each time), topical antibiotic & eyelid scrub using an OTC eyelid hygienic preparation (baby-shampoo).
1. Eyelid Disorders:
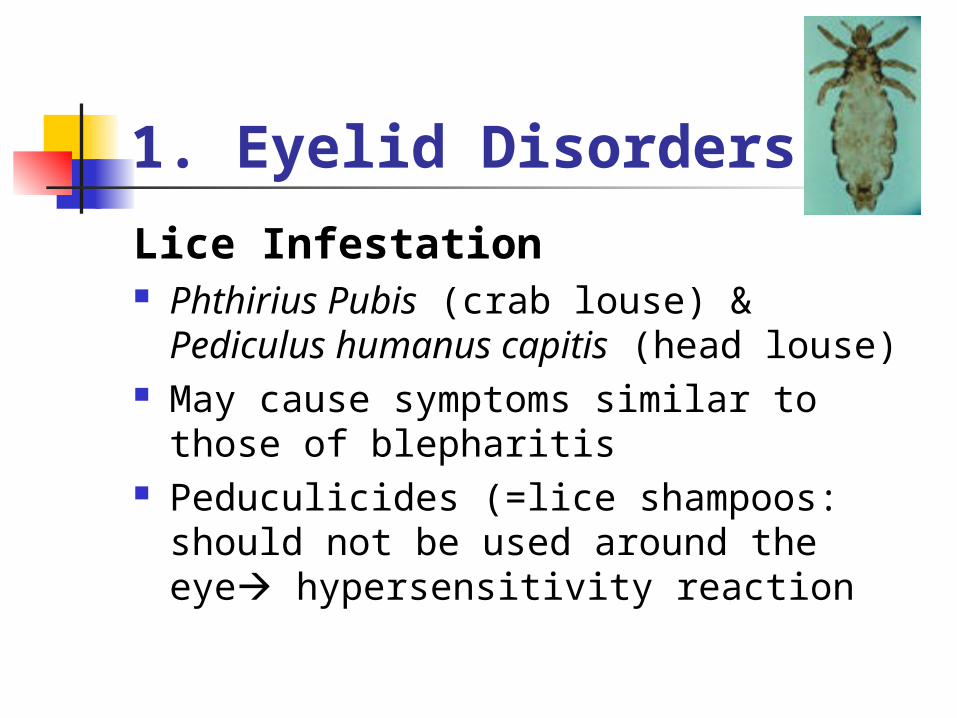
Lice Infestation Phthirius Pubis (crab louse) & Pediculus
humanus capitis (head louse) May cause symptoms similar to those of
blepharitis Peduculicides (=lice shampoos: should
not be used around the eye hypersensitivity reaction
Lice InfestationTreatment:
1. A bland ophthalmic ointment (e.g. petrolatum) used for 10 days effective because it suffocates the louse and deprives its eggs of oxygen
2. Hygienic measures: wash clothing & bedding that may contain unhatched eggs

Crab louse eyelid
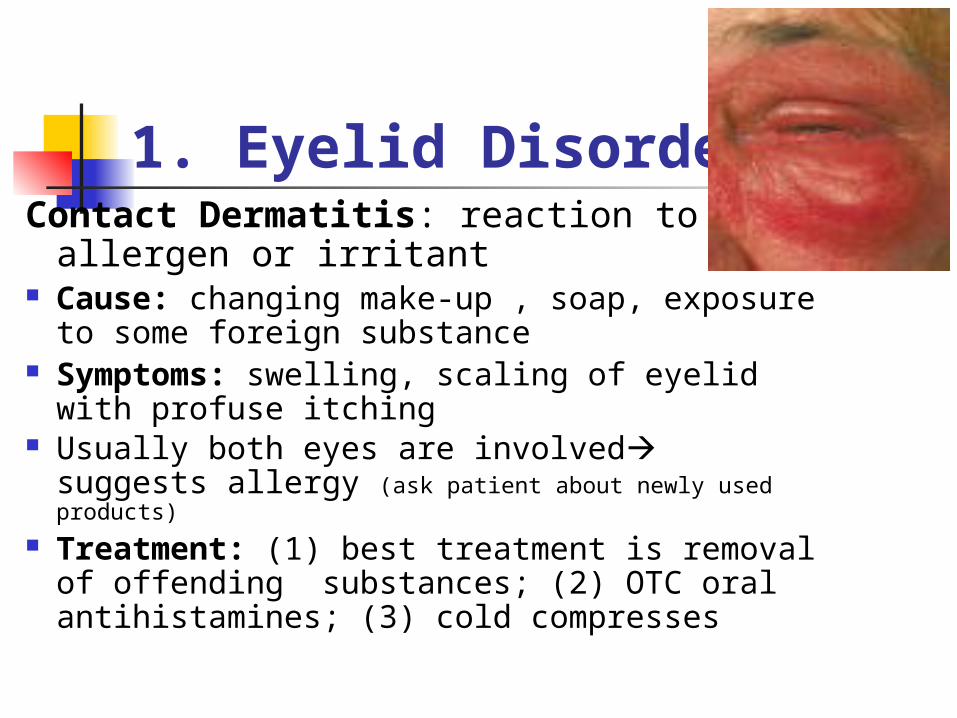
1. Eyelid DisordersContact Dermatitis: reaction to an
allergen or irritant Cause: changing make-up , soap,
exposure to some foreign substance Symptoms: swelling, scaling of eyelid
with profuse itching Usually both eyes are involved suggests
allergy (ask patient about newly used products)
Treatment: (1) best treatment is removal of offending substances; (2) OTC oral antihistamines; (3) cold compresses
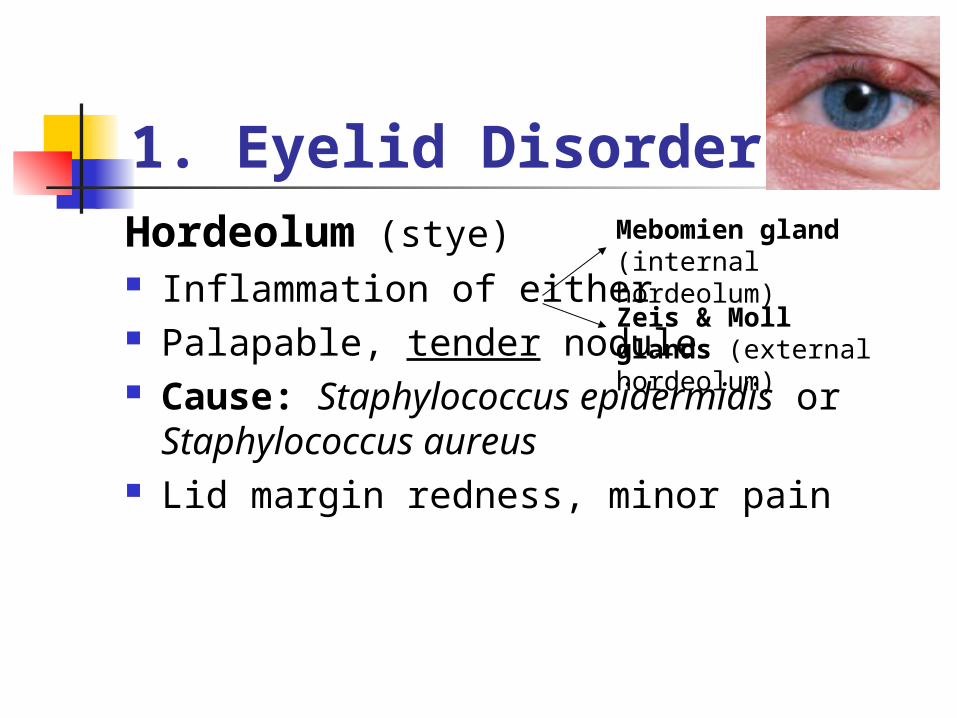
1. Eyelid DisordersHordeolum (stye) Inflammation of either Palapable, tender nodule Cause: Staphylococcus epidermidis or
Staphylococcus aureus Lid margin redness, minor pain
Mebomien gland (internal hordeolum)
Zeis & Moll glands (external hordeolum)
Treatment: (1) Hot compresses 3-4 times/day (5-10 minutes; clearing within 1 week), gentle rolling would help; (2) External hordeolum topical antibiotic; Internal hordeolum oral antibiotic; (3) if resistant surgical drainage
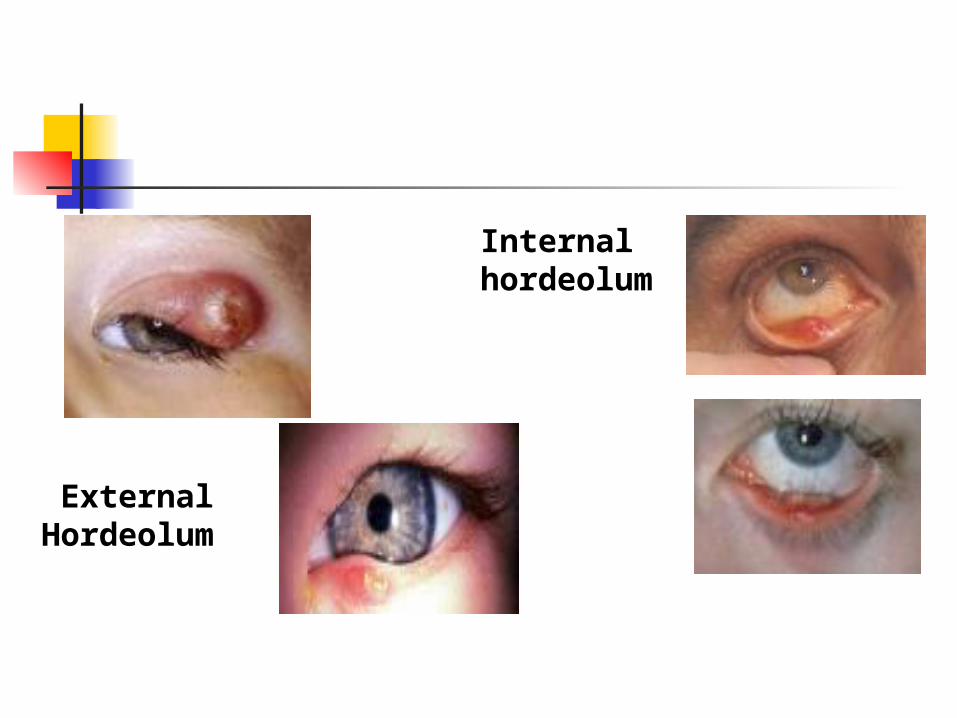
External Hordeolum
Internal hordeolum

1. Eyelid Disorders
Chalazion painless, slowly enlarging nodule on the eyelid
formed by inflammation of the meibomian glands (deep chalazion) or Zeis sebaceous glands (superficial chalazion). Not infectious. Granuloma.
difference:1. not tender to gentle touching and is painless.
Treatment: (1) hot compresses (2) oral antibiotics (3) if resistant: surgery, intralesional steroid injection
Recurrance of chalazia & hordeola maybe reduced by periodic use of lid scrubs
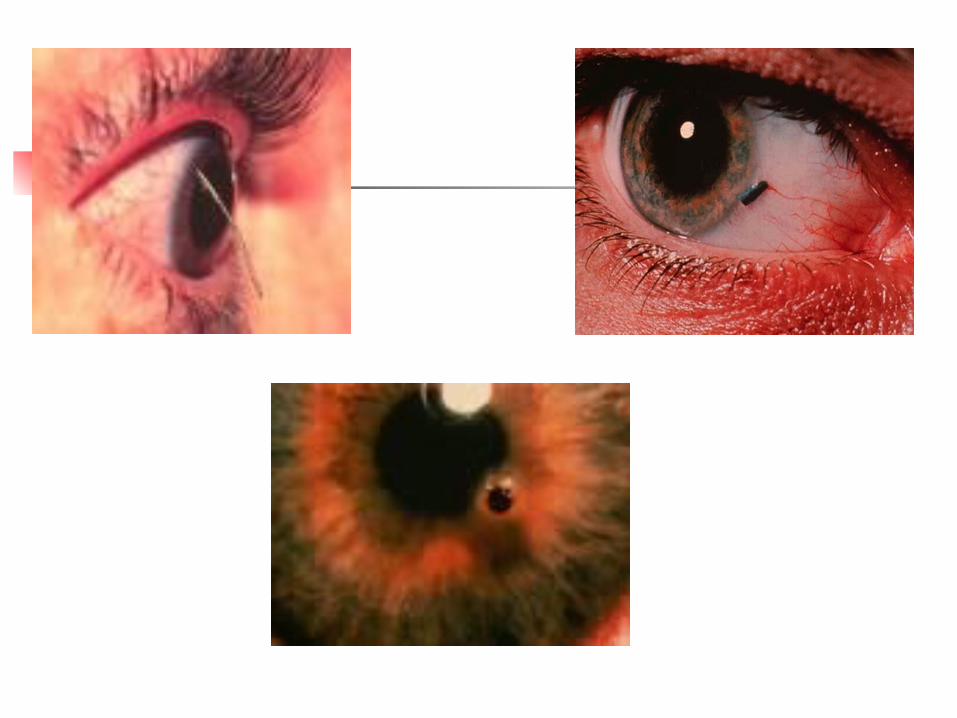
2. Ocular Surface Disorders
Foreign substance contact If reflex tearing does not remove the foreign
substance, the eye may need to be flushed with sterile saline or specific eye wash preparations (irrigants: baby shampoo)
If trapped up the eye lid may not go with flushing optometrist or ophthalmologist
Metallic foreign body NOT SELF-IRRIGATION (abrasion, scarring, chronic red eye)
Immediate medical referral
2. Ocular Surface Disorders
Abrasions “superficial injury to a skin or mucous membrane, in
this case, the cornea or conjuctiva” Causes: Scratches by fingernails or by foreign
bodies Such injuries cause partial or total loss of the
epithelium & are painful especially if cornea is involved
Self –treatment NOT RECOMMENDED because of the risk of bacteria or fungi contaminating and infecting the eye
2. Ocular Surface Disorders
Chemical Exposure Splash injury, fumes or solid
chemicals serious problem Medical Emergency immediate referral
Initial treatment: flushing eye with sterile saline or water for at least 10 minutes
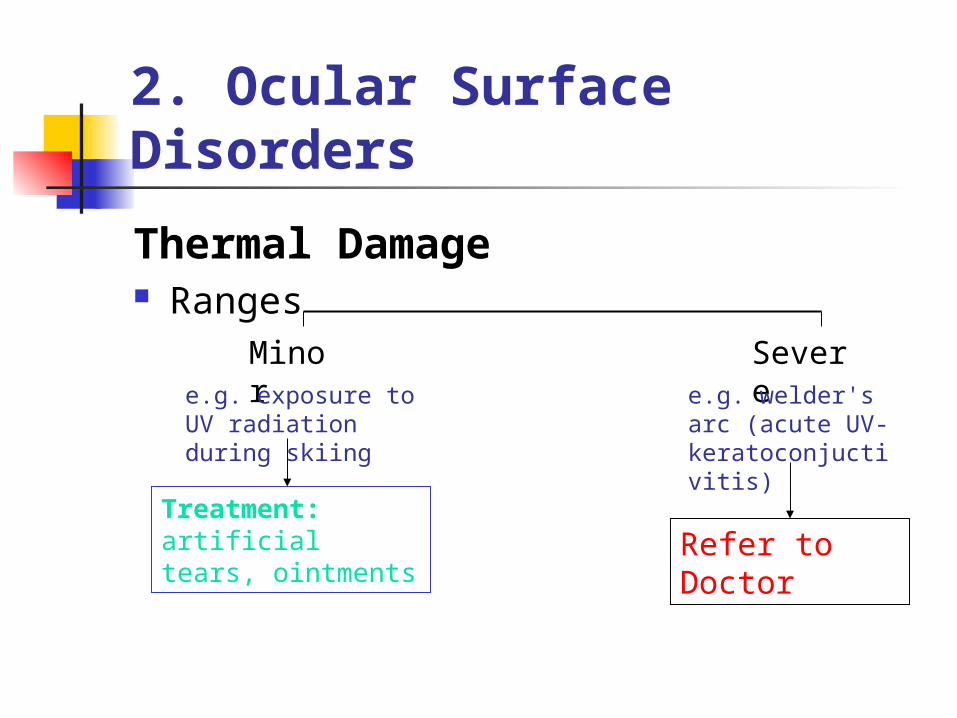
2. Ocular Surface Disorders
Thermal Damage Ranges
Minor Severee.g. exposure to UV
radiation during skiing
e.g. welder's arc (acute UV-keratoconjuctivitis)
Refer to Doctor
Treatment: artificial tears, ointments
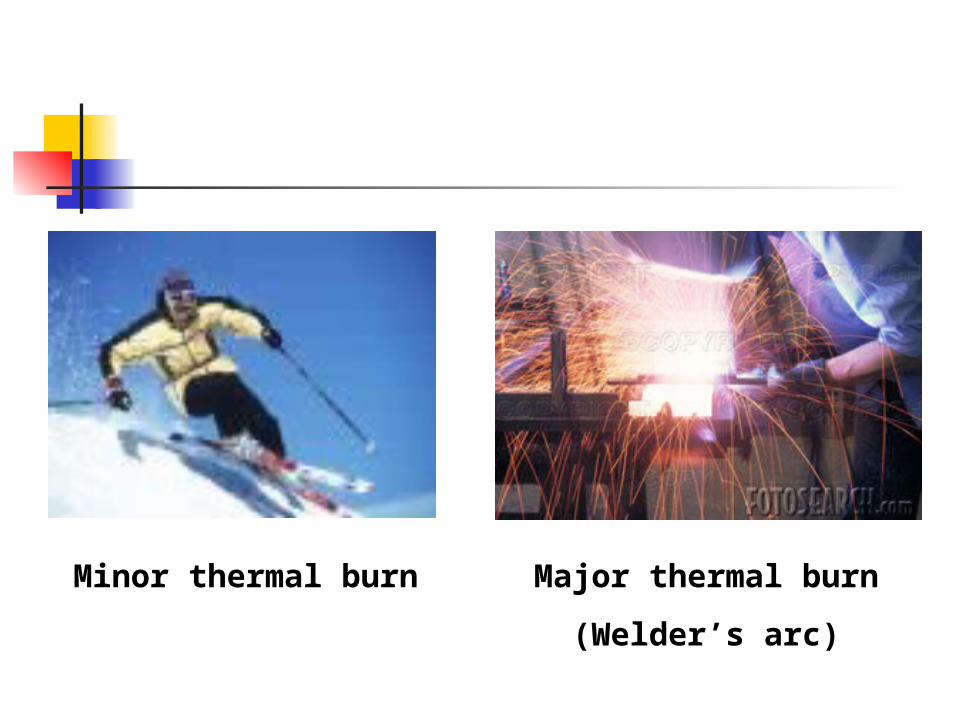
Minor thermal burn Major thermal burn
(Welder’s arc)
Arc Eye and Other Physical Hazards
ULTRAVIOLET RADIATIONUltraviolet radiation (UV) is generated by the electric arc in the welding process. Skin exposure to UV can result in severe burns, in many cases without prior warning. UV radiation can also damage the lens of the eye. Many arc welders are aware of the condition known as "arc-eye," a sensation of sand in the eyes. This condition is caused by excessive eye exposure to UV. Ultraviolet rays also increase the skin effects of some industrial chemicals (coal tar and cresol compounds, for example).INFRARED RADIATIONExposure to infrared radiation (IR), produced by the electric arc and other flame cutting equipment may heat the skin surface and the tissues immediately below the surface. Except for this effect, which can progress to thermal burns in some situations, infrared radiation is not dangerous to welders. Most welders protect themselves from IR (and UV) with a welder's helmet (or glasses) and protective clothing.INTENSE VISIBLE LIGHTExposure of the human eye to intense visible light can produce adaptation, pupillary reflex, and shading of the eyes. Such actions are protective mechanisms to prevent excessive light from being focused on the retina. In the arc welding process, eye exposure to intense visible light is prevented for the most part by the welder's helmet.
Signs of KeratoconjunctivitisSymptoms of keratoconjunctivitis include blurry vision, eye pain, eye redness, a hazy or cloudy cornea, increased sensitivity to light, conjunctival swelling, and eyelid swelling

2. Ocular Surface Disorders
Conjuctivitis: inflammation of bulbar conjuctiva
Viral conjuctivitis Allergic conjuctivitis Bacterial conjuctivitis Chlamydial conjuctivitis