Embed Size (px)
Citation preview

Clinical Neurology and Neurosurgery 122 (2014) 23–28
Operative management of patients with radiosurgery-relatedtrigeminal neuralgia: Analysis of the surgical morbidity and painoutcome
Gerganov Venelin M.1, Giordano Mario *, Erck Elolf 2, Almarzooq Osamah 3, Samii Amir 4
, Samii Madjid 5
International Neuroscience Institute, Rudolf Pichlmayr Str. 4, Hannover 30625, Germany
A R T I C L E I N F O
Article history:Received 9 November 2013Received in revised form 2 March 2014Accepted 13 April 2014Available online 22 April 2014
Keywords:Trigeminal neuralgiaRadiosurgeryGamma knifeCerebellopontine angleVestibular schwannoma
A B S T R A C T
Object: Trigeminal neuralgia (TGN) occurring after radiosurgical treatment of cerebellopontine orpetroclival tumors may be very difficult to control. Our aim was to determine the efficacy of neurosurgicaltreatment in regards to pain control and to evaluate the procedure-related complication and morbidityrates.Methods: Retrospective study of a series of operated patients with radiosurgery-induced TGN. Theprimary goal of the surgery was to inspect and decompress the trigeminal nerve; the second goal was toremove the tumor remnant completely, if safely feasible. The main outcome measures were pain control,time to onset of pain relief and its duration, occurrence of new neurological deficits or worsening of theexisting one and completeness of tumor removal.Results: The four patients met the inclusion criteria: 2 with vestibular schwannomas, 1 with petroclivalmeningioma and 1 with an epidermoid. TGN occurred 12–60 months after radiosurgery (mean 39months). At presentation the pain attacks occurred multiple timesdaily and lasted from a few seconds to2–3 min. The Complete tumor removal via the retrosigmoid approach was achieved in all cases. Therewere no major operative complications or persistent morbidity, besides one patient with trochlear nervepalsy. All patients experienced immediate pain relief after surgery. At follow-up (median duration – 42.5months) the three patients reported complete pain resolution. One patient had occasional slight pain butdid not need any medications.Conclusion: Surgery is safe and effective treatment option of patients with intractable radiosurgery-induced TGN. It leads to excellent pain control and is curative in regards to the neoplastic disease.
ã 2014 Published by Elsevier B.V.
Contents lists available at ScienceDirect
Clinical Neurology and Neurosurgery
journal homepage: www.else vie r .com/locate /c l ine uro
1. Introduction
Radiosurgery is widely used as an alternative to microsurgery incase of small cerebellopontine angle (CP angle) or petroclival tumorsor as an adjunctive treatment following incomplete tumor removal.The reduction of prescription doses to 12–15 Gy led to decline in the
* Corresponding author. Tel.: +49 511 27092865; fax: +49 511 27092706.E-mail addresses: [email protected] (V.M. Gerganov),
[email protected] (M. Giordano), [email protected] (E. Elolf),[email protected] (A. Osamah), [email protected](S. Amir), [email protected] (S. Madjid).
1 Tel.: +49 511 270 92 835.2 Tel.: +49 511 270 92 306.3 Tel.: +49 511 270 92 809.4 Tel.: +49 511 270 92 400.5 Tel.: +49 511 270 92 840.
http://dx.doi.org/10.1016/j.clineuro.2014.04.0160303-8467/ã 2014 Published by Elsevier B.V.
posttreatment morbidity rates [1–5]. Trigeminal neuropathy – facialparesthesias or numbness – is by far the most common non-audiofacial radiosurgery-relatedneuropathyand develops in2–8%ofthe patients [1,3,4,6–8]. Trigeminal neuralgia (TGN) as a complica-tion of radiosurgical treatment has been occasionally reported.Putative pathogenetic mechanisms are direct radiation-inducedinjury of the trigeminal fibers in the brainstem or of the compressedby the tumor trigeminal nerve root. Although the trigeminal pain isusually transient [9], insome patients, itmay persist and isextremelydifficult to control. The systematic analyses of the managementoptions and outcome of treatment of intractable radiosurgery-induced trigeminal neuralgia have never been published in theliterature. Some patients have been treated with medications, someunderwent second radiosurgery, while in others the tumor remnantwas removed via the translabyrinthine approach [1,18,24]. Thesuccess rate of these procedures in terms of pain control, however,has not been reported.

Table 1General patient’s characteristics.
Patientcharacteristics
Number
Total number ofpatients
4
Age (months) � Mean: 46.5� Range: 38–55
MaleFemale
40
Duration ofsymptoms(months)
� Mean: 39� Range: 12–60
Pain distribution V1–2:1V2–3:1V1–3:1V3:1
Previous paintreatment
Medications:4Thermocoagulation:2
Pain intensityscore(BNI scale)
IV/V (some pain, not adequately controlled withmedications:1V/V (severe pain or no pain relief):3
Pain relief(modified BNIscale)
I/V (no pain, off medications):2II/V (occasional pain, off medications):2
24 V.M. Gerganov et al. / Clinical Neurology and Neurosurgery 122 (2014) 23–28
We evaluated retrospectively, our experience with the surgicalmanagement of the patients with CP angle or petroclival tumorswith intractable radiosurgery-induced TGN. Our goal was todetermine the efficacy of neurosurgical treatment in regards topain control and to evaluate the procedure-related complicationrates.
2. Patients and methods
2.1. Patient population
All the patients operated at our institution for a CP angle orpetroclival tumor following previous radiosurgical treatment werereviewed retrospectively. Their documentation, pre- and postop-erative neuroradiological data, operative reports, operative videosand follow-up data were collected in a database. In particular thefollowing information was recorded: patients age, sex, initialdiagnosis and treatment; type of radiosurgery; neurological statusbefore and after radiosurgery and at presentation; tumor type, sizeand location; characteristics of the trigeminal pain, previous painmanagement; outcome of surgery and neurological status atdischarge and follow-up.
2.2. Inclusion criteria
Included in the current study were patients with intractableTGN, which occurred after the radiosurgical treatment. TGN wasdefined as paroxysmal lancinating unilateral pain in the distribu-tion of the trigeminal nerve lasting from several seconds tominutes. Possible trigger points or trigger actions were recorded.The pain intensity was evaluated using the Barrow NeurologicalInstitute pain intensity score [10].
2.3. Indications for surgery and surgical procedure
Indications for the current surgery were inadequate pain reliefwith the medical therapy (at least 2 different medications,including high dose of carbamazepine therapy for at least 12months) and/or failure of previous invasive procedures. Theprimary goal of surgery was to inspect and decompress thetrigeminal nerve from any possible tumor- or scar-inducedcompression. Second goal was to remove the tumor remnantcompletely, if safely feasible. All patients were operated in thesemi-sitting position via the retrosigmoid approach. Details of theoperative technique have been presented earlier [11,12].
2.4. Outcome and follow-up
The main outcome measures were pain control, time to onset ofthe pain relief and its duration, occurrence of new neurologicaldeficits or worsening of the existing one, and completeness oftumor removal. The modified Barrow Neurological Institute painintensity score was utilized to evaluate the pain relief [13]. Thefacial nerve function was categorized using the House–Brackmann(HB) scale [14].
Long-term follow-up was established either by direct exami-nation of the patients or by telephone interview. The following twoissues were inquired: (1) type, intensity and location of pain aftersurgery; (2) need and type of additional medical therapy.
3. Results
Four patients met the inclusion criteria of the study (Tables 1and 2). Their mean age was 46.5 years, ranging from 38 to 55 years.Two of them had vestibular schwannomas, one had petroclivalmeningioma and one – an extensive CP angle epidermoid. Three
patients (N: 1, 2 and 4) have been operated initially at anotherhospital: partial tumor removal was performed, followed bygamma knife treatment because of further growth of the tumorremnant. The trigeminal pain occurred 12–60 months afterradiosurgery (mean 39 months): paroxysmal lancinating pain inthe distribution of the ipsilateral trigeminal nerve. At presentationthe pain attacks occurred multiple times each day and lasted froma few seconds to 2–3 min. Trigger points, however, were notidentified. In 3 patients the pain intensity score was V/V (severepain or no pain relief) and in 1 was IV/V (some pain, not adequatelycontrolled with medications). All patients have been treatedunsuccessfully with various pain medications. In 2 of themradiofrequency thermocoagulation of the trigeminal ganglionhas been also performed: it had no effect on the pain but causedtrigeminal sensory changes (V2 in Patient N:1 and V2, 3 in PatientN:4).
3.1. Neurological outcome
The outcome of surgery is presented in Table 2. The Completetumor removal could be achieved in all cases. After surgery onepatient (Patient N:3) had a trochlear nerve dysfunction. Theanatomical integrity of the facial nerve was preserved in allpatients with intact facial nerve function prior to surgery. PatientN:4 presented with HB Grade 4/6 facial nerve palsy. His facial nerveat surgery was found to be atrophic and responded poorly toelectrostimulation. It was therefore excised and reconstructedprimarily in the CP angle with an interpositional sural nerve graft.The follow-up of this patient is six months. All other patients atfollow-up had excellent facial nerve function: HB Grade I in 2 andGrade II in 1 of them (the patient had a HB Grade II facial functionprior to surgery). CSF leak occurred in the two patients and weremanaged successfully with lumbar drainage for 7 days.
3.2. Intraoperative findings
In all the patients the tumor remnant caused compression ofthe trigeminal nerve and was strongly attached to its surface. Thethickening of the arachnoidea around the trigeminal nerve was afurther universal finding. The vascular compression of the nerve,however, has never been found. In Patient N:4 the whole nerve was

Table
2Pa
tien
tpop
ulation
includingclinical
dataan
dfollow
up.
Age
Sex
Tumor
type
Type
ofradios
urgery
Timeto
occu
rren
ceof
TGN
(mon
ths)
Duration
ofTG
N(m
onths)
Pain
distribution
andintensity
(BNIscore)
Prev
iouspain
trea
tmen
tNeu
rologicalstatus
Surgical
morbidityan
dou
tcom
ePa
inrelief
Follow
-up
(mon
ths)
38M
VS,
1.9cm
Gam
makn
ifefollow
ing
partial
remov
al(twice)
3612
-V2,3
-BNI-V
Med
ications
Thermoc
oagu
lation
-V2hy
pesthesia
-Anacusis
-Nonew
defi
cits
-CSF
leak
BNI-I
Immed
iate
improve
men
t
120
46M
VS,
1.5cm
Gam
makn
ife(twice)
follow
ingpartial
remov
al2
36-V1,2
-BNI-V
Med
ications
-Anacusis
-Facial
palsy
HB
GradeII
-Te
mporary
wors-
ened
facial
function;
HB
Grade
IIat
fol-
low-u
p
BNI-I
Immed
iate
improve
men
t
24
55M
Petroc
lival
men
ingiom
a,2.5cm
Gam
makn
ife
660
-V3
-BNI-IV
Med
ications
-V1–
3hy
pesthesia
-CSF
leak
-Troc
hlear
nerve
dys-
function
BNI-II
Immed
iate
improve
men
t
20
47M
Epidermoid,
diffuse
Gam
makn
ifefollow
ing
partial
remov
al12
48-V1–
3;
-BNI-V
Med
ications
Thermoc
oagu
lation
-V2,3hy
pesthesia
-Anacusis
-Facial
palsy
HB
GradeIV
-Nonew
defi
cits
-Facial
nerve
reco
n-
stru
ction
BNI-II
Immed
iate
improve
men
t
6
V.M. Gerganov et al. / Clinical Neurology and Neurosurgery 122 (2014) 23–28 25
engulfed by the tumor. In Patient N:3 the meningioma severelycompressed and dislocated the nerve caudally. Furthermore, thetumor expanded and compressed the nerve roots and ganglion inthe Meckels’ cave.
3.3. Pain outcome
All the patients experienced immediate pain relief after surgery.The pain medication was gradually tapered of and then stoppedcompletely in all 4 patients. Median follow-up in the group was42.5 months (range, 6–120 months). At follow-up 3 patientsreported complete resolution of the pain and one patient hadoccasional slight pain but did not need any medications.
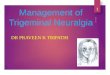
Fig. 1 shows the MRI at admission in our institute of a patientaffected by vestibular schwannoma previously operated and thentreated twice with radiosurgery in another institution who came toour attention with medication-resistant trigeminal pain startedone month after first radiosurgical procedure. We performed acomplete tumor removal and a complete pain relief was obtained(follow up 24 months).
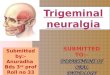
The MRI study presented in Fig. 2 shows an epidermoid tumorthat, as the previous case, was first partial resected and thenirradiated. The trigeminal pain started 4 months after lastprocedure. We performed a retrosigmoid approach with aid ofendoscope obtaining removal of the lesion and pain resolution.
4. Discussion
Radiosurgery is a widely applied management option inpatients with CP angle or petroclival tumors. Although thereduction in the prescription dose led to a marked reduction inthe frequency of adverse side effects, cranial nerve morbidityremains a concern [3,12,25,27]. The radiation injury of cranialnerves is supposed to be caused by damage of their feeding vesselsor Schwann cell/oligodendroglia covering [5].
Gamma knife radiosurgery may provoke transient trigeminalnerve sensory changes, such as facial paresthesias, numbness ortingling. The trigeminal nerve is fairly radioresistant and itsfunction can be preserved in the majority of patients [2,3,5–8]. Inthe large reported series the rate of persistent trigeminalneuropathy varies from 1.6 to 36% [1,8,15,16]. In a largemetaanalysis Kaylie et al. found trigeminal neuropathies in 154/427 patients with vestibular schwannomas, varying in severityfrom transient hypesthesia to disabling neuralgia [17].
Radisourgery-induced TGN has been reported to be typicallytransient and do not need surgical therapy [9]. In some patients,however, it persists and may become extremely severe. Such caseshave been mentioned in many large series published in theliterature and can develop both in patients with vestibularschwannomas or with meningiomas [2,16,18–21]. One of the 55young patients with vestibular schwannomas analyzed by Lobato-Polo et al. [18] developed typical trigeminal neuralgia after thegamma knife treatment. Lunsford et al. [2] report on 2 such cases(0.2%) in a large series of 829 patients with vestibular schwanno-mas treated with gamma knife. In a series of 195 patients withvestibular schwannoma Chung et al. [19] described 2 patients withtrigeminal neuralgia that developed 8 months and 28 months,respectively, after gamma knife. Pollock et al. [20] also mentionthat 1 patient with vestibular schwannoma developed trigeminalneuralgia after radiosurgery.
Trigeminal pain syndrome has been described followingradiosurgery of CP angle or petroclival meningiomas. Moritaet al. [16] observed nine radiosurgery-induced permanenttrigeminal neuropathies in 90 nerves at risk after a latent intervalof 2–7 months. Roche et al. [22] described four patients withmeningioma involving the cavernous sinus with disease
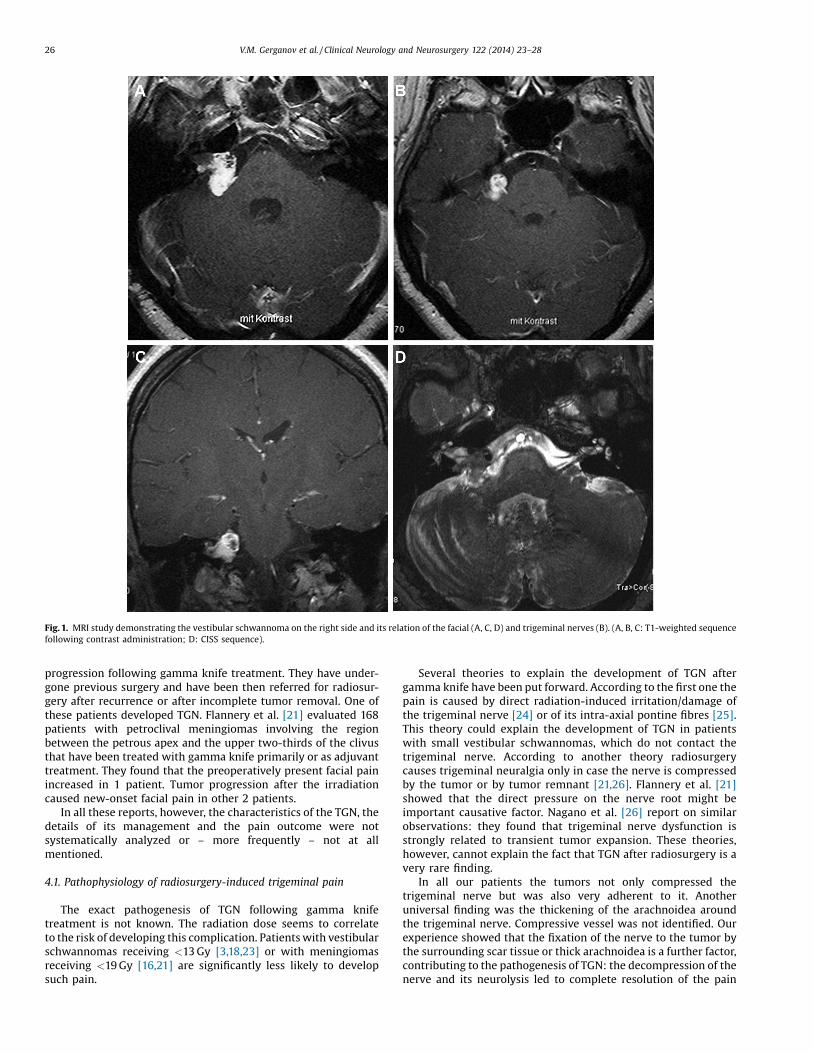
Fig. 1. MRI study demonstrating the vestibular schwannoma on the right side and its relation of the facial (A, C, D) and trigeminal nerves (B). (A, B, C: T1-weighted sequencefollowing contrast administration; D: CISS sequence).
26 V.M. Gerganov et al. / Clinical Neurology and Neurosurgery 122 (2014) 23–28
progression following gamma knife treatment. They have under-gone previous surgery and have been then referred for radiosur-gery after recurrence or after incomplete tumor removal. One ofthese patients developed TGN. Flannery et al. [21] evaluated 168patients with petroclival meningiomas involving the regionbetween the petrous apex and the upper two-thirds of the clivusthat have been treated with gamma knife primarily or as adjuvanttreatment. They found that the preoperatively present facial painincreased in 1 patient. Tumor progression after the irradiationcaused new-onset facial pain in other 2 patients.
In all these reports, however, the characteristics of the TGN, thedetails of its management and the pain outcome were notsystematically analyzed or – more frequently – not at allmentioned.
4.1. Pathophysiology of radiosurgery-induced trigeminal pain
The exact pathogenesis of TGN following gamma knifetreatment is not known. The radiation dose seems to correlateto the risk of developing this complication. Patients with vestibularschwannomas receiving <13 Gy [3,18,23] or with meningiomasreceiving <19 Gy [16,21] are significantly less likely to developsuch pain.
Several theories to explain the development of TGN aftergamma knife have been put forward. According to the first one thepain is caused by direct radiation-induced irritation/damage ofthe trigeminal nerve [24] or of its intra-axial pontine fibres [25].This theory could explain the development of TGN in patientswith small vestibular schwannomas, which do not contact thetrigeminal nerve. According to another theory radiosurgerycauses trigeminal neuralgia only in case the nerve is compressedby the tumor or by tumor remnant [21,26]. Flannery et al. [21]showed that the direct pressure on the nerve root might beimportant causative factor. Nagano et al. [26] report on similarobservations: they found that trigeminal nerve dysfunction isstrongly related to transient tumor expansion. These theories,however, cannot explain the fact that TGN after radiosurgery is avery rare finding.
In all our patients the tumors not only compressed thetrigeminal nerve but was also very adherent to it. Anotheruniversal finding was the thickening of the arachnoidea aroundthe trigeminal nerve. Compressive vessel was not identified. Ourexperience showed that the fixation of the nerve to the tumor bythe surrounding scar tissue or thick arachnoidea is a further factor,contributing to the pathogenesis of TGN: the decompression of thenerve and its neurolysis led to complete resolution of the pain

Fig. 2. Epidermoid tumor in patient N:4. Note the intimate relation of the epidermoid to the trigeminal nerve on the left side. (A, B: T1-weighted sequences following contrastadministration; C, D: T2-weighted MR sequences; E, F: postoperative MRI).
V.M. Gerganov et al. / Clinical Neurology and Neurosurgery 122 (2014) 23–28 27
syndrome in all cases. In all cases, however, the volume of tumorremnant did not change essentially during the follow-up. The paindeveloped only after the radiosurgical treatment, which indicatesthat the radiation contributed essentially to the pathogenesis ofthe pain syndrome.
4.2. Management options
The patients with trigeminal neuralgia, described in previouspublications, have been treated medically [20], with repeatedgamma knife irradiation targeting to the trigeminal nerve [19] or

28 V.M. Gerganov et al. / Clinical Neurology and Neurosurgery 122 (2014) 23–28
surgically [24]. The pain outcome in most studies is not specificallyaddressed. Schulder et al. [24] presented a patient with a vestibularschwannoma who developed pain in the trigeminal nervedistribution following gamma knife treatment. The patient wasoperated three years later because of tumor growth. Followingsurgery the patient was neurologically unchanged. In this patientthe pain was certainly caused purely by the irradiation: in contrastto our cases the tumor had no relation to the trigeminal nerve. Thesurgery may not be efficient in the absence of nerve compressionor fixation by scar tissue. Kano et al. stated that multimodality painmanagement strategies were required in most patients with skullbase meningiomas associated with trigeminal neuralgia [27]. Theepidermoids are not considered suitable for radiosurgery and theexperience is rather limited [28].
The trigeminal neuropathy after radiosurgery may be transientand spontaneous pain alleviation may occur [14]. Moreover, insome cases, it may improve with medical therapy. Hence, werecommend initial medical therapy trial with at least two differentdrugs in sufficient dosage. If the pain severity does not decrease fora period of at least twelve months, the patient should be offeredthe option of microsurgical management. In our series all thepatients had inadequate pain relief with the medical therapy and/or failure of the percutaneous radiofrequency thermocoagulation.The primary goal of surgery in our cases was to inspect anddecompress the trigeminal nerve from any possible tumor- or scar-induced compression. The removal of the tumor remnant was asecondary goal. The extent of resection was estimated at surgery,considering the intraoperative findings: preservation of neurolog-ical functions had a priority. Safe complete tumor removal turnedout to be feasible in all patients. There was no major persistentmorbidity in the series. The outcome in regards to pain control wasexcellent: three patients reported at follow up complete resolutionof the pain and one patient had occasional slight pain but did notneed any medications.
5. Conclusion
Surgery is safe and effective treatment option of patients withtumor remnants and intractable radiosurgery-induced TGN. Itleads to excellent pain control and is curative in regards to theneoplastic disease.
References
[1] Prasad D, Steiner M, Steiner L. Gamma surgery for vestibular schwannoma. JNeurosurg 2000;92:745–59.
[2] Lunsford LD, Niranjan A, Flickinger JC, Maitz A, Kondziolka D. Radiosurgery ofvestibular schwannomas: summary of experience in 829 cases. J Neurosurg2005;102(Suppl):195–9.
[3] Sughrue ME, Yang I, Han SJ, Aranda D, Kane AJ, Amoils M, Smith ZA, Parsa AT.Non-audiofacial morbidity after gamma knife surgery for vestibular schwan-noma. Neurosurg Focus 2009;27:E4.
[4] Iwai Y, Yamanaka K, Shiotani M, Uyama T. Radiosurgery for acoustic neuromas:results of low-dose treatment. Neurosurgery 2003;53:287–8 discussion 287–288.
[5] Steiner LSJ, Lindquist C, Stroila M, Steiner M. Gamma knife surgery for cerebralvascular malformations, tumors and functional disorders. In: Schmidek HRD,
editor. Schmidek and Sweet operative neurosurgical techniques: indicaions,methods, and results. fifth ed. Philadelphia: WB Saunders; 2005530–76.
[6] Nettel B, Niranjan A, Martin JJ, Koebbe CJ, Kondziolka D, Flickinger JC, LunsfordLD. Gamma knife radiosurgery for trigeminal schwannomas. Surg Neurol2004;62:436–44 discussion 436–444.
[7] Sheehan J, Yen CP, Arkha Y, Schlesinger D, Steiner L. Gamma knife surgery fortrigeminal schwannoma. J Neurosurg 2007;106:839–45.
[8] Hempel JM, Hempel E, Wowra B, Schichor C, Muacevic A, Riederer A.Functional outcome after gamma knife treatment in vestibular schwannoma.Eur Arch Otorhinolaryngol 2006;263:714–8.
[9] Phi JH, Kim DG, Chung HT, Lee J, Paek SH, Jung HW. Radiosurgical treatment ofvestibular schwannomas in patients with neurofibromatosis type 2: tumorcontrol and hearing preservation. Cancer 2009;115:390–8.
[10] Rogers CL, Shetter AG, Fiedler JA, Smith KA, Han PP, Speiser BL. Gamma kniferadiosurgery for trigeminal neuralgia: the initial experience of The BarrowNeurological Institute. Int J Radiat Oncol Biol Phys 2000;47:1013–9.
[11] Samii M, Matthies C. Management of 1000 vestibular schwannomas (acousticneuromas): surgical management and results with an emphasis oncomplications and how to avoid them. Neurosurgery 1997;40:11–21 discus-sion 13–21.
[12] Samii M, Gerganov V, Samii A. Improved preservation of hearing and facialnerve function in vestibular schwannoma surgery via the retrosigmoidapproach in a series of 200 patients. J Neurosurg 2006;105:527–35.
[13] McNatt SA, Yu C, Giannotta SL, Zee CS, Apuzzo ML, Petrovich Z. Gamma kniferadiosurgery for trigeminal neuralgia. Neurosurgery 2005;56:1295–301discussion 1293–1301.
[14] House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head NeckSurg 1985;93:146–7.
[15] Karpinos M, Teh BS, Zeck O, Carpenter LS, Phan C, Mai WY, Lu HH, Chiu JK,Butler EB, Gormley WB, Woo SY. Treatment of acoustic neuroma: stereotacticradiosurgery vs. microsurgery. Int J Radiat Oncol Biol Phys 2002;54:1410–21.
[16] Morita A, Coffey RJ, Foote RL, Schiff D, Gorman D. Risk of injury to cranialnerves after gamma knife radiosurgery for skull base meningiomas:experience in 88 patients. J Neurosurg 1999;90:42–9.
[17] Kaylie DM, Horgan MJ, Delashaw JB, McMenomey SO. A meta-analysiscomparing outcomes of microsurgery and gamma knife radiosurgery.Laryngoscope 2000;110:1850–6.
[18] Lobato-Polo J, Kondziolka D, Zorro O, Kano H, Flickinger JC, Lunsford LD.Gamma knife radiosurgery in younger patients with vestibular schwannomas.Neurosurgery 2009;65:294–300 discussion 291–300.
[19] Chung WY, Liu KD, Shiau CY, Wu HM, Wang LW, Guo WY, Ho DM, Pan DH.Gamma knife surgery for vestibular schwannoma: 10-year experience of 195cases. J Neurosurg 2005;102(Suppl):87–96.
[20] Pollock BE, Driscoll CL, Foote RL, Link MJ, Gorman DA, Bauch CD, Mandrekar JN,Krecke KN, Johnson CH. Patient outcomes after vestibular schwannomamanagement: a prospective comparison of microsurgical resection andstereotactic radiosurgery. Neurosurgery 2006;59:77–85 discussion 77–85.
[21] Flannery TJ, Kano H, Lunsford LD, Sirin S, Tormenti M, Niranjan A, Flickinger JC,Kondziolka D. Long-term control of petroclival meningiomas throughradiosurgery. J Neurosurg 2014;112:957–64.
[22] Roche PH, Regis J, Dufour H, Fournier HD, Delsanti C, Pellet W, Grisoli F, PeragutJC. Gamma knife radiosurgery in the management of cavernous sinusmeningiomas. J Neurosurg 2000;93(Suppl 3):68–73.
[23] Yang I, Sughrue ME, Han SJ, Fang S, Aranda D, Cheung SW, Pitts LH, Parsa AT.Facial nerve preservation after vestibular schwannoma gamma kniferadiosurgery. J Neurooncol 2009;93:41–8.
[24] Schulder M, Sreepada GS, Kwartler JA, Cho ES. Microsurgical removal of avestibular schwannoma after stereotactic radiosurgery: surgical and patho-logic findings. Am J Otol 1999;20:364–7 discussion 368.
[25] Ganz JC, Reda WA, Abdelkarim K. Adverse radiation effects after gamma knifesurgery in relation to dose and volume. Acta Neurochir (Wien) 2009;151:9–19.
[26] Nagano O, Higuchi Y, Serizawa T, Ono J, Matsuda S, Yamakami I, Saeki N.Transient expansion of vestibular schwannoma following stereotacticradiosurgery. J Neurosurg 2008;109:811–6.
[27] Kano H, Awan NR, Flannery TJ, Iyer A, Flickinger JC, Lunsford LD, KondziolkaD. Stereotactic radiosurgery for patients with trigeminal neuralgia associat-ed with petroclival meningiomas. Stereotact Funct Neurosurg 2010;89:17–24.
[28] Kida Y, Yoshimoto M, Hasegawa T, Fujitani S. Radiosurgery of epidermoidtumors with gamma knife: possiblility of radiosurgical nerve decompression.No Shinkei Geka 2006;34:375–81.