Embed Size (px)
Citation preview

NCRP Report No. 142
Operational Radiation SafetyProgram for Astronauts in Low-Earth Orbit: A Basic Framework
Recommendations of theNATIONAL COUNCIL ON RADIATIONPROTECTION AND MEASUREMENTS
Issued November 30, 2002
National Council on Radiation Protection and Measurements7910 Woodmont Avenue, Suite 400 / Bethesda, Maryland 20814

LEGAL NOTICEThis Report was prepared by the National Council on Radiation Protection and
Measurements (NCRP). The Council strives to provide accurate, complete and useful
information in its documents. However, neither the NCRP, the members of NCRP,
other persons contributing to or assisting in the preparation of this Report, nor
any person acting on the behalf of any of these parties: (a) makes any warranty or
representation, express or implied, with respect to the accuracy, completeness or
usefulness of the information contained in this Report, or that the use of any informa-
tion, method or process disclosed in this Report may not infringe on privately owned
rights; or (b) assumes any liability with respect to the use of, or for damages resulting
from the use of any information, method or process disclosed in this Report, under
the Civil Rights Act of 1964, Section 701 et seq. as amended 42 U.S.C. Section 2000e
et seq. (Title VII) or any other statutory or common law theory governing liability.
Library of Congress Cataloging-in-Publication Data
National Council on Radiation Protection and Measurements.
Operational radiation safety program for astronauts in low-earth orbit : a basic
framework : recommendations of the National Council on Radiation Protection
and Measurements.
p. cm. — (NCRP report ; no. 142)
‘‘Issued November 2002.’’
Includes bibliographical references and index.
ISBN 0-929600-75-4
1. Extraterrestrial radiation—Safety measures. 2. Astronauts—Health and
hygiene. 3. Space medicine. I. Title. II. Series
RA1151.R33 N38 2002
616.9�80214—dc21 2002037861
Copyright © National Council on Radiation
Protection and Measurements 2002
All rights reserved. This publication is protected by copyright. No part of this publica-
tion may be reproduced in any form or by any means, including photocopying, or
utilized by any information storage and retrieval system without written permission
from the copyright owner, except for brief quotation in critical articles or reviews.
[For detailed information on the availability of NCRP publications see page 150.]

Preface
This Report was developed under the auspices of Scientific Com-
mittee 46, the National Council on Radiation Protection and
Measurements (NCRP) program area committee concerned with
operational safety. This Report addresses the operational radiation
safety program for astronauts working in low-Earth orbit, with par-
ticular attention to the radiation dosimetry needed, the radiation
exposure information that should be recorded, and ways to imple-
ment the radiation protection principle of ‘‘as low as reasonably
achievable’’ for activities involving the Space Shuttle and the Inter-
national Space Station. It is a companion document to NCRP Report
No. 132, Radiation Protection Guidance for Activities in Low-Earth
Orbit, published in December 2000, and provides advice on imple-
mentation of NCRP Report No. 132 guidance.
This work was performed at the request of the National Aeronau-
tics and Space Administration (NASA) and NCRP gratefully
acknowledges NASA’s support. The Scientific Committee that pre-
pared this Report also benefited from a series of briefings from NASA
staff at the Committee’s first meeting in December 1999 in Houston.
This Report was prepared by Scientific Committee 46-15 on Opera-
tional Radiation Safety Program for Astronauts. Serving on Scien-
tific Committee 46-15 were:
Richard J. Vetter, Chairman
Mayo Clinic
Rochester, Minnesota
Members
Ellen S. Baker David T. Bartlett
National Aeronautics and National Radiological
Space Administration Protection Board
Lyndon B. Johnson Space Chilton, Oxon, United
Center Kingdom
Houston, Texas
Thomas B. Borak Susan M. Langhorst
Colorado State University Washington University in
Fort Collins, Colorado St. Louis School of Medicine
St. Louis, Missouri
iii
iv / PREFACE
Stephen W.S. McKeever Jack Miller
Oklahoma State University Lawrence Berkeley National
Stillwater, Oklahoma Laboratory
Berkeley, California
R. Julian Preston John W. Wilson
U.S. Environmental Protection National Aeronautics and
Agency Space Administration
Research Triangle Park, Langley Research Center
North Carolina Hampton, Virginia
Advisor
Charles B. Meinhold
National Council on Radiation Protection and Measurements
Bethesda, Maryland
NCRP Secretariat
Marvin Rosenstein, Consultant
Cindy L. O’Brien, Managing Editor
The Council wishes to express its appreciation to the Committee
members for the time and effort devoted to the preparation of this
Report.
Thomas S. Tenforde
President

Contents
Preface ........................................................................................ iii
1. Summary and Recommendations ................................... 1
1.1 Components of an Operational Radiation Safety
Program ......................................................................... 1
1.2 Team Management in the Radiation Safety Program 2
1.3 Sources of Radiation in Space ...................................... 3
1.4 Dose Limits for Astronauts ........................................... 3
1.5 Sources of Exposure Included in the Dose Limits
for Astronauts ................................................................ 4
1.6 Types of Radiation to be Assessed ............................... 5
1.7 Approach to Dose Assessment for Astronauts ........... 6
1.8 Operational Radiation Monitoring ............................... 7
1.8.1 Area Monitoring .................................................. 7
1.8.2 Personal Dosimetry ............................................. 8
1.8.3 Calibration ........................................................... 10
1.9 Biodosimetry .................................................................. 11
1.10 Immediate Dose Management and ‘‘As Low As
Reasonably Achievable’’ ................................................ 11
1.11 Radiation Safety Training ............................................ 12
1.12 Dosimetry Record .......................................................... 13
2. Objectives of the Operational Radiation Safety
Program for Astronauts .................................................... 15
2.1 The Low-Earth Orbit Program ...................................... 15
2.2 Dose Limits for Astronauts ........................................... 17
2.2.1 Deterministic Limits ............................................. 18
2.2.2 Stochastic Limits .................................................. 18
2.3 Operational Radiation Protection Considerations ........ 22
3. Current Management of Astronaut Radiation Safety
Program ................................................................................. 24
3.1 Flight Rules for Management of Dose ........................... 24
3.2 Biomedical Research ....................................................... 26
3.3 Individuals Involved in Management of Dose ............... 26
3.3.1 Astronaut ............................................................. 26
3.3.2 Flight Director ...................................................... 26
3.3.3 Flight Surgeon ...................................................... 27
3.3.4 Radiation Health Officer ..................................... 27
3.3.5 Space Radiation Analysis Group ......................... 28
v
vi / CONTENTS
4. Radiation Environment in Low-Earth Orbit ............... 294.1 Trapped Electrons (0.5 to 6 MeV; �0.2 keV �m�1) ...... 304.2 Reentrant and Splash Albedo Electrons (1 MeV to
�1 GeV; 0.2 to �3 keV �m�1) ........................................ 314.3 Trapped Protons (�10 MeV; �5 keV �m�1) .................. 314.4 Trapped and Solar Protons and Light Nuclear
Particles (10 to 400 MeV; 0.3 to 5 keV �m�1) .................. 314.5 Galactic Cosmic Radiation Ions and High-Energy
Secondary Fragments (�50 MeV n�1; Z � 1; 1 to
1,000 keV �m�1) .............................................................. 324.6 Charged Target Fragments (�10 MeV n�1; 2 to
1,200 keV �m�1) .............................................................. 324.7 Neutrons (0.1 to 500 MeV) ............................................. 334.8 Summary for Particle Types ........................................... 33
5. Approach to Dose Assessment for Astronauts ............. 355.1 Exterior Exposure Field ................................................. 38
5.1.1 Radiation Environment Models ........................... 385.1.2 Spacecraft External Measurements .................... 39
5.2 Interior Exposure Field ................................................... 395.2.1 Shielding Models for the Space Shuttle,
International Space Station, and Space Suits .... 395.2.2 Spacecraft Internal Measurements ..................... 40
5.3 Tissue Exposure Fields ................................................... 415.3.1 Human Shielding Models ..................................... 415.3.2 Occupancy Factors ................................................ 41
6. Data Collection and Interpretation for Dose
Assessment ........................................................................... 426.1 Introduction .................................................................... 426.2 Dose Quantities to be Determined ................................ 436.3 Proposed Measurement Package .................................... 44
6.3.1 General Discussion ............................................... 446.3.2 Proposed Measurement Package: Active
Devices ................................................................... 466.3.2.1 Tissue Equivalent Proportional
Counters ................................................... 476.3.2.2 Solid-State Detectors ............................... 476.3.2.3 Active Electronic Personal Dosimeters .... 486.3.2.4 Active Detectors for Electrons ................ 48
6.3.3 Proposed Measurement Package: Passive
Devices .................................................................. 496.3.3.1 Low Linear Energy Transfer
Dosimetry: Thermoluminescent
Dosimeters ............................................... 506.3.3.2 Direct Ion Storage Dosimeters ............... 51
CONTENTS / vii
6.3.3.3 Neutron and High Atomic Number,
High-Energy Particle Dosimetry:
Plastic Nuclear Track Detectors ............ 51
6.3.3.4 Use of Thermoluminescent Dosimeters
and Plastic Nuclear Track Detectors to
Estimate Effective Dose .......................... 52
6.3.3.5 Superheated Drop/Bubble Dosimeters ..... 52
6.3.4 Recommendations for Measurement Packages .. 53
6.3.4.1 Recommendations for Area Monitoring ... 53
6.3.4.2 Recommendations for Personal
Dosimetry ................................................ 54
6.4 Accuracy, Performance Testing, and Calibration ........ 55
6.4.1 Operational Radiation Protection Requirements
on Accuracy of Dose Measurements .................... 55
6.4.1.1 Recommendations of ICRP and ICRU ... 55
6.4.1.2 General Requirements ........................... 56
6.4.2 Tests of Instrument and Dosimeter
Performance .......................................................... 56
6.4.3 Calibration ............................................................ 57
7. Role of Biodosimetry in Dose Assessment .................. 59
7.1 Electron Spin Resonance ................................................ 59
7.2 Biochemical Indicators ................................................... 60
7.3 Erythrocytes with Transferrin Receptors ...................... 60
7.4 Gene Mutation Assays ................................................... 60
7.5 Cytogenetic Alterations ................................................... 61
7.5.1 Micronuclei ............................................................ 61
7.5.2 Acentric Fragments in Prematurely Condensed
Chromosomes ........................................................ 62
7.5.3 Chromosomal Aberrations .................................. 62
7.6 Summary for Methods .................................................... 63
7.7 Current NASA (Lyndon B. Johnson Space Center)
Methods ........................................................................... 63
7.8 Recommendations and Future Considerations ............. 64
8. Recommended Management of Astronaut Radiation
Safety Program .................................................................... 66
8.1 Components of a Low-Earth Orbit Operational
Radiation Safety Program ............................................. 66
8.2 Radiation Protection Principles Applied to Low-Earth
Orbit Missions ................................................................ 67
8.3 Sources of Exposure Included in NCRP Dose Limits
for Astronauts ................................................................. 68

viii / CONTENTS
8.4 Immediate Dose Management and Basic ‘‘As Low As
Reasonably Achievable’’ Concepts .................................. 69
8.4.1 Immediate Dose Management Issues ................. 70
8.4.2 Basic ‘‘As Low As Reasonably Achievable’’
Concepts ................................................................ 70
8.4.3 Considerations for Spacecraft and Space Suit
Design .................................................................... 70
8.4.4 Considerations for Preflight Planning ................ 71
8.4.5 Considerations for Continuous In-Flight
Review ................................................................... 71
8.4.6 Considerations for Postflight Review .................. 72
8.5 Radiation Safety Training for NASA Personnel ........... 72
8.5.1 Astronauts ............................................................. 73
8.5.2 Flight Directors ..................................................... 74
8.5.3 Flight Surgeons ..................................................... 75
8.5.4 Radiation Health Officer and Radiation Safety
Support Groups .................................................... 75
8.5.5 Other Supporting Specialists ............................... 76
9. Radiation Safety Records ................................................. 77
9.1 Content of Records .......................................................... 78
9.1.1 Records of Career Doses ....................................... 80
9.1.2 Records of Prospective and Retrospective
Studies .................................................................. 81
9.2 Continuity of Records Over Time ................................... 82
9.2.1 Existing Records and Unanalyzed Data Files .... 82
9.2.2 Future Adjustment of Records ............................. 82
9.3 Retention of Records ....................................................... 83
Appendix A. Time-Dependent Variations in the Space
Radiation Environment and the Need for Active
Real-Time Monitoring ........................................................ 84
A.1 Background ..................................................................... 84
A.2 Types of Active Detectors Used in Space ...................... 86
A.2.1 Tissue Equivalent Proportional Counters .......... 86
A.2.2 Semiconductor Detectors ..................................... 91
A.2.3 Cerenkov Counters ............................................. 93
A.2.4 Ionization Chambers ........................................... 93
Appendix B. Computational Methods ................................ 95
Appendix C. Thermoluminescence Dosimetry
Materials ............................................................................... 99
CONTENTS / ix
C.1 Lithium Fluoride, Doped with Magnesium and
Titanium ........................................................................ 99
C.2 Calcium Fluoride, Doped with Thulium ..................... 105
C.3 Lithium Fluoride, Doped with Magnesium, Copper
and Phosphorus ............................................................ 107
C.4 Aluminum Oxide, Doped with Carbon ........................ 108
C.5 Evaluation of Absorbed Dose and Dose Equivalent ..... 110
C.5.1 Equivalent Gamma-Ray Dose ........................... 110
C.5.2 Mean, or Effective, Linear Energy Transfer .... 111
C.5.3 Dose Equivalent ................................................. 112
Appendix D. Plastic Nuclear Track Detectors ................. 115
D.1 Description of Method .................................................. 115
D.2 Neutron Dosimetry ..................................................... 116
D.3 Dosimetry of Cosmic Radiation Fields ....................... 117
Glossary .................................................................................... 122
Acronyms, Abbreviations, and Main Symbols .................. 126
References ................................................................................ 128
The NCRP .................................................................................. 141
NCRP Publications .................................................................. 150
Index ........................................................................................... 160
1. Summary andRecommendations
Astronauts are living and working for extended periods in low-
Earth orbit (LEO) during Space Shuttle missions and construction,
maintenance and operation of the International Space Station (ISS).
The radiation environment they encounter in space is complex, with
unique high-LET (linear energy transfer) and high-energy compo-
nents, as distinct from the predominately low-LET and low-energy
radiation environments encountered by most radiation workers on
Earth. The primary purpose of an operational radiation safety pro-
gram for astronauts working in LEO is to assess and control the
radiation exposure of individual astronauts commensurate with mis-
sion tasks and the prevailing radiation conditions in LEO.
1.1 Components of an Operational Radiation
Safety Program
The main components of an operational radiation safety program
designed to implement the principles of dose limitation and ALARA
(as low as reasonably achievable) for astronauts working in LEO are:
● to facilitate actions, both in advance of a mission and in-flight,
that respond to space radiation conditions or mission decisions
that significantly affect the level of radiation exposure to the
astronauts, and radiation protection decisions that significantly
influence the conduct of the mission;
● to collect and record data to assess astronaut doses for individual
mission and cumulative career records; and
● to identify, plan and carry out practical ALARA actions to avoid
unnecessary levels of radiation exposure.
Recommendation 1: National Aeronautics and Space Admin-
istration (NASA) management should implement and main-
tain an effective radiation safety program with the following
features: clear definition of the goals of the program, state-
ment of the organization’s commitment to the application
1

2 / 1. SUMMARY AND RECOMMENDATIONS
of the ALARA principle, statement of management’s com-
mitment to provide adequate budgetary support for the
program, and periodic review of the overall program
performance.
Recommendation 2: NASA management should clearly assign
responsibility for ensuring the translation of radiation pro-
tection strategies and instrumentation from design and
development through engineering, preparation for flight,
and use in orbit.
1.2 Team Management in the Radiation Safety Program
Management of the radiation safety program in LEO is a team
effort, involving the astronauts, the flight director, the flight surgeon,
the radiation health officer (RHO), and the Space Radiation Analysis
Group (SRAG). Typically, astronauts do not play an active role in
decision making and policy regarding radiation protection issues.
Instead, the flight director and flight surgeon direct their radiation
protection actions, with the help of radiation experts. The current
roles of these individuals are noted below.
Usually, one or two astronauts with medical backgrounds repre-
sent the U.S. Astronaut Office’s position regarding radiation protec-
tion at the various meetings and committees. If radiation exposure
is expected to be more than minimal, the affected astronauts may
participate more actively concerning their particular flight.
The flight director is the final decision maker in the Mission Con-
trol Center with regard to all aspects of a mission, and the flight
director relies heavily on the radiation team and flight surgeon when
decisions regarding radiation protection issues need to be made.
The flight surgeon is responsible for the crew’s health and safety
during all aspects of flight, and briefs the crew pre- and postflight
regarding radiation protection issues and personal radiation dose.
The RHO is involved in development and design of radiation pro-
tection strategies and provides recommendations to minimize crew
exposures during mission planning and during space missions,
tracks crew exposures against career limits, and provides risk inter-
pretation for acute exposures.
SRAG consists of NASA radiation specialists who are responsible
for promoting ALARA in development and design of radiation protec-
tion strategies and ensuring compliance with ALARA procedures.
During a mission, SRAG provides an interface to update mission
significant radiation events, particularly when transient events in

1.4 DOSE LIMITS FOR ASTRONAUTS / 3
the space radiation environment produce a potential for high doses
to the astronauts.
Recommendation 3: NASA’s operational radiation safety pro-
gram for LEO should have clearly defined responsibilities
given to an individual or group to ensure overall implementa-
tion of the program. This individual or group may include
individuals from those listed above, and/or members of NASA
management who are able to work across all levels of opera-
tion to ensure radiation safety actions are considered for
implementation.
1.3 Sources of Radiation in Space
The predominant sources of radiation in LEO are galactic cosmic
radiation (GCR) (high-energy protons, helium ions, and heavy ions
of extra-solar origin); solar particle events (SPE) (primarily medium-
energy protons of solar origin); the radiation belts outside Earth’s
atmosphere (high-energy protons and electrons trapped in Earth’s
magnetic field); and scattering from Earth’s atmosphere (albedo neu-
trons, electrons and protons). There is a real potential that high
transient radiation doses to astronauts will occur occasionally during
construction and operation of ISS, particularly from SPEs and rela-
tivistic electrons from the outer radiation belt.
1.4 Dose Limits for Astronauts
The current recommended dose limits for astronauts in LEO were
developed in NCRP Report No. 132 (NCRP, 2000a). The limits for
bone marrow, lens of the eye, and skin are for protection against
deterministic effects. The career limits are for protection against
delayed stochastic effects and are based on a lifetime excess risk of
cancer mortality of three percent.
The following formulations and terminology are used in this Report
for the dose-limit quantities for space activities:
● The dose limits for the relevant organs or tissues for determinis-
tic effects are expressed in terms of gray equivalent, where gray
equivalent is the mean absorbed dose in an organ or tissue
modified by a recommended value, for radiation protection pur-
poses, of the relative biological effectiveness of a given particle
type, as given in NCRP Report No. 132 (NCRP, 2000a). The
4 / 1. SUMMARY AND RECOMMENDATIONS
recommended values and dose limits for deterministic effects
are given in Tables 2.2 and 2.3, respectively. A conventional
notation GT � RiDT is proposed for gray equivalent and used in
this Report. GT is gray equivalent, Ri is the recommended value
for relative biological effectiveness of a given particle type i, and
DT is the mean absorbed dose in an organ or tissue.
● The career limits for delayed stochastic effects are expressed in
terms of effective dose (E), where:
E � �T
wTHT . (1.1)
HT is the equivalent dose and wT is the tissue weighting factor.
The career limits are given in Table 2.4 and are specified by
gender and age.
● For the complex mixtures of high- and low-LET radiations exper-
ienced in LEO, the practice in the space radiation protection com-
munity is to obtain point values of absorbed dose (D) and dose
equivalent (H) {using D and the quality factor relationship as a
function of LET [Q(L)]}. The point quantities are then averaged
over the organ or tissue of interest by means of computational
models to obtain the organ dose equivalent (ICRU, 1993), which
has been assigned the symbol HT in this Report. This practice
permits more complete consideration of the Q(L) relationship for
these complex radiation environments. The currently recom-
mended Q(L) relationship is given in NCRP Report No. 116
(NCRP, 1993) and is shown in Equation 2.5. For space radiations,
NCRP Report No. 132 (NCRP, 2000a) adopted HT, for operational
radiation protection purposes, as an acceptable approximation for
HT for stochastic effects.
Recommendation 4: For the operational radiation safety pro-
gram in LEO, organ dose equivalent (HT) should be used as
the approximation for equivalent dose (HT).
1.5 Sources of Exposure Included in the Dose Limits
for Astronauts
Recommendation 5: The dose limits for astronauts should
include the cumulative dose from space flight, the dose asso-
ciated with mission-related aviation activities (excluding
commercial flights), the dose from biomedical research con-
ducted as part of the astronaut’s mission duties, and any

1.6 TYPES OF RADIATION TO BE ASSESSED / 5
other occupational doses including any received prior to
work as an astronaut.
The dose limits do not include normal background radiation on
Earth or radiation dose received from diagnostic and therapeutic
medical procedures conducted as part of the astronaut’s overall
health care. In addition, previous medical radiation doses, from diag-
nostic and therapeutic medical procedures, are assumed to have
provided the individual a greater benefit than the risk associated
with the doses and should not be used in determining qualification
for future occupational exposure.
1.6 Types of Radiation to be Assessed
The radiation environment external to a spacecraft in LEO con-
sists of electrons, positrons, neutrons, protons and heavier nuclei
[up to particle charge (Z) � 92]. Energies range from a few electron
volts for trapped electrons and albedo neutrons to in excess of
1014 MeV for GCR ions. Most of the electrons will not penetrate the
wall of the spacecraft, but could penetrate the space suits worn
during extravehicular activity (EVA), resulting in doses to the skin
and eyes. Nuclear interactions of neutrons, protons and heavier
nuclei with spacecraft, space suits, Earth’s atmosphere, and the
human body produce secondary particles, which add to the radiation
field. Radiation monitoring strategies vary according to particle
charge, particle type, energy, and measurement location. The envi-
ronment can be classified according to particle types and energies
and where the measurements are to be made (i.e., outside the space-
craft, inside the spacecraft, and inside EVA suits), as listed below
(see also Table 4.1):
● trapped electrons—outside spacecraft and inside EVA suits● reentrant and splash albedo electrons—outside and inside
spacecraft, and inside EVA suits● trapped protons (�10 MeV)—do not penetrate spacecraft or
EVA suits● protons and light nuclear particles (�10 MeV)—outside and
inside spacecraft, and inside EVA suits● GCR ions and secondary charged fragments—outside and inside
spacecraft, and inside EVA suits● charged-particle fragments—inside spacecraft and inside EVA
suits● neutrons—outside and inside spacecraft, and inside EVA suits
6 / 1. SUMMARY AND RECOMMENDATIONS
The relative contributions from each component (including the
secondary radiation) at each location will vary according to several
factors, including the mass distribution inside the spacecraft, the
EVA suit design and materials, and the site of interest within the
human body.
1.7 Approach to Dose Assessment for Astronauts
Recommendation 6: Dose assessment for astronauts should
utilize a combination of radiation transport calculations and
measurements as illustrated in Figure 5.1. The main features
of the approach should include sequential assessment of the
radiation environment at the exterior surface of the space-
craft, the interior radiation environments in the spacecraft
and EVA suits, and the transmission of radiation to internal
organs or tissues in order to estimate the dose-limit quanti-
ties. The radiation transport calculations are not intended
to be a substitute for measured data, but are designed to
augment the measurements such that the combination of
measurements and calculations should provide an estimate
of the dose-limit quantities in Table 2.1 to within a factor of
1.5 at the 95 percent confidence level.
Environmental models for GCR (and the associated albedo neu-
trons), trapped radiations, and SPEs are used to represent the exte-
rior radiation field in LEO. External measurements can be made
outside the spacecraft to allow correction to the models to reduce
uncertainties.
Shielding models for the Space Shuttle, ISS, and EVA suits allow
evaluation of the radiation environment to which the astronaut is
exposed. Except for the absolute intensity of the trapped radiation
or a SPE, the interior radiation environment can be evaluated with
high-speed computational models. The interior radiation environ-
ments of the Space Shuttle and ISS can be monitored with various
instruments and the measurements can be used to adjust the esti-
mate of the trapped-particle intensity, reduce the uncertainty in
the model estimates, evaluate transmission factors, and evaluate
calculated dosimetric quantities. Personal dosimeters can provide
estimates of absorbed dose at points on the surface of the astro-
naut’s body.
The evaluation of organ or tissue doses for astronauts can be
performed with computerized male and female anthropomorphic
models. The models allow the evaluation of the relationships between

1.8 OPERATIONAL RADIATION MONITORING / 7
absorbed dose (D) and dose equivalent (H ) at points on the surface
of the body and the required quantities in deeper-lying organs [i.e.,
mean absorbed dose in an organ or tissue (DT) and organ dose equiva-
lent (HT), the surrogate for equivalent dose (HT)] that are needed to
obtain the dose-limit quantities effective dose (E) and gray equiva-
lent (GT).
In addition, occupancy factors keyed to individual astronaut activ-
ity can be used to estimate exposures from the personal dosimeter
measurements. This is especially true during EVA where large fluc-
tuations in the trapped electron environment or SPEs could occur.
1.8 Operational Radiation Monitoring
Recommendation 7: Operational radiation monitoring con-
sisting of area monitors and personal dosimeters should pro-
vide measured data of sufficient accuracy:
● for determination of field quantities and organ or tis-
sue doses to be used for normalizing radiation transport
calculations
● for dose assessment and record keeping purposes
● for real-time or near real-time estimates of dose rates for
purposes of immediate dose management or ALARA
1.8.1 Area Monitoring
Recommendation 8: Tissue equivalent proportional counters
(TEPC) should be utilized during manned space flight for
real-time measurements of absorbed dose and absorbed dose
rate, and estimates of quality factor and dose equivalent to
a small mass of tissue.
A TEPC is an active detector that is designed to measure energy
deposition in volumes of tissue comparable to the dimensions of the
nuclei of mammalian cells. Data are recorded on an event-by-event
basis such that one can obtain a distribution of biologically relevant
energy deposition events. Its tissue equivalence and large dynamic
range make it sensitive to photons, neutrons and charged particles
from electrons and protons to heavy ions.
When the data are integrated over the complete distribution of
lineal energy (y), TEPCs can generate absorbed dose (D) and ab-
sorbed dose rate (D·). The distribution of energy deposition events
depends on characteristics of the radiation field and the response of

8 / 1. SUMMARY AND RECOMMENDATIONS
the detector, and can serve as a test for radiation transport models
or to obtain an approximation to the quality factor (Q) for protons
and heavier particles. This detector provides a reliable estimate of
D from protons through high atomic number, high-energy (HZE)
particles as well as photons, electrons and neutrons. Although the
data in terms of y are not a direct replicate of the distributions of
fluence [&(L)] or absorbed dose [D(L)] as a function of LET (L),
average values of y, in particular dose-averaged y, are numerically
similar to L. Data from a TEPC can be displayed continuously and
stored for later transmission to the Mission Control Center.
Recommendation 9: Solid-state detectors should be utilized
during manned space flight for real-time measurements of
LET distributions both inside and outside of the spacecraft.
Solid-state detectors record the energy deposited by a charged
particle. The ratio of the deposited energy to the thickness of the
detector yields the approximate LET for the incident particle. Thus
a single detector can provide data that yield absorbed dose (D) and
absorbed dose rate (D·) for protons and heavier charged particles. It
can be fabricated into a compact detector for use as portable area
monitor or personal dose-rate meter with on-demand readout. Sev-
eral of these detectors can be combined to point in different directions
to provide a more complete description of the radiation field either
outside or inside of the spacecraft.
Recommendation 10: An active detector sensitive to electrons
should be installed outside of the spacecraft to serve as a
monitor for fluctuations in the electron component of the
space radiation environment, which can change by many
orders of magnitude during and following an SPE due to
short-term perturbations of the geomagnetic field.
The fluctuations of the electron component could be of concern
during an EVA, since electrons above a few hundred kiloelectron
volts can penetrate the space suits. Such a monitor could be a simple
ionization chamber with a wall thickness sufficient to attenuate very
low-energy electrons but thin enough to record electrons that could
penetrate a space suit.
1.8.2 Personal Dosimetry
Recommendation 11: A measurement package consisting of a
thermoluminescent dosimeter (TLD) or optically stimulated

1.8 OPERATIONAL RADIATION MONITORING / 9
luminescence dosimeter (OSLD) for measurement of the low-
LET component, and a stack of plastic nuclear track detec-
tors (PNTD) to determine the high-LET component should
be used for passive personal dosimetry in the complex radia-
tion field experienced in space.
LiF:Mg,Cu,P (lithium fluoride, doped with magnesium, copper and
phosphorus) would appear to be an attractive TLD material. Alterna-
tively, Al2O3:C (aluminum oxide, doped with carbon) is the best cur-
rently available OSLD material. To measure the dose equivalent (H)
from the high-LET components, polyallyl diglycol carbonate [PADC/
CR-39� (trade name CR-39, PPG Industries, Inc., Pittsburgh, Penn-
sylvania)] is the PNTD material proposed. Such devices have been
used as part of the area monitoring or personal dosimeter packages
on the Space Shuttle, but are not currently planned for ISS. It is
recommended that they be used as personal dosimeters on both
vehicles. CaF2:Tm (calcium fluoride, doped with thulium) [e.g., TLD-
300� (Bicron, Saint-Gobain Industries, Cleveland, Ohio)] could also
be used as an adjunct personal dosimeter to provide additional infor-
mation to normalize radiation transport models, but not for quantita-
tive determination of dose quantities.
With these detection elements in a passive personal dosimeter
package, H at a point in adjacent tissue is then obtained by using
a combination of TLDs (or OSLDs) and PNTDs, as described in
Section 6.3. In this recommendation, TLDs (or OSLDs) are used to
measure D in the low-LET region (L � 10 keV �m�1) for which
Q � 1. It is further recommended that D in the high-LET region
(L � 10 keV �m�1) be monitored using PNTDs. In this region Q
is dependent on L. Correction may be needed for any overlap of
the two responses so that intermediate LET components are not
double-counted.
Verification of LET-dependence of the TLD response of LiF:
Mg,Cu,P and of the OSLD response of Al2O3:C will be required. Until
such time as these data are available, LiF:Mg,Ti-based dosimeters
[e.g., TLD-100� or TLD-700� (Bicron, Saint-Gobain Industries,
Cleveland, Ohio)] may still be used, along with PNTDs, in order to
provide LET data suitable for correcting the TLD dose response for
the L � 10 keV �m�1 component, and for estimating H for this
component from the PNTD results. If PNTDs cannot be used, a
different, less desirable approach has to be adopted using TLDs
and data from a TEPC or particle spectrometer, as described in
Section 6.3.4.2.
For purposes of active personal dosimetry, a thick silicon detector
may be able to provide an approximation to D, D�, and D(L) for

10 / 1. SUMMARY AND RECOMMENDATIONS
protons and heavier particles. These have been designed in a suffi-
ciently compact configuration to be worn by the astronauts and can
be read on demand. In the case of currently available active personal
electronic dosimeters, most are used routinely to measure low-LET
radiation and have not been characterized for the types and energies
of particles comprising the fields in spacecraft. Such dosimeters,
when well characterized, may perform a useful role. Future consider-
ations for active electronic personal dosimeters are noted in Sec-
tion 6.3.2.3.
In those cases where active personal dosimeters are not used,
onboard systems for analysis of passive personal dosimeters may be
required, especially on long-duration ISS flights. Onboard systems
for readout of TLDs and OSLDs are certainly possible. However,
onboard readout of PNTDs is not feasible. Therefore, onboard read-
out of passive dosimeters will provide only part of the dose record
(for low-LET) and development of such systems should only be con-
sidered if active personal dosimetry is unavailable.
The potential for developing a set of conversion coefficients that
directly relate H obtained with TLDs and PNTDs at the surface to
E for the space radiation environment, similar in concept to those
used in other occupational radiation environments, would be worth
investigating.
1.8.3 Calibration
Recommendation 12: Response data for the active and passive
devices used should be determined for the following energy
ranges as appropriate: protons from 10 to 800 MeV; high-Z,
high-energy ions (e.g., helium, carbon, silicon, iron) from
50 MeV n�1 to 1 GeV n�1; electrons from 0.5 to 10 MeV; and
neutrons from 1 to 180 MeV, in fields that are monoenergetic
or quasi-monoenergetic, plus response data for fields which
replicate the neutron field produced by the interactions of
GCR with shielding material.
The response characteristics of all the types of devices should be
determined prior to use. This will normally be accomplished by a
combination of experiment and calculation. The response determina-
tions should normally be in terms of the quantity fluence. An excep-
tion would be for the determination of photon response, for which
air or tissue kerma will be more appropriate. For the determination
of the response characteristics of personal dosimeters, some irradia-
tions should be performed on either an anthropomorphic phantom
or a surrogate. Sufficient angle dependence of response data should

1.10 IMMEDIATE DOSE MANAGEMENT / 11
be available to estimate the isotropic response. Where needed and
where available, recommended fluence to D and fluence to H conver-
sion coefficients should be used.
1.9 Biodosimetry
Recommendation 13: NASA should continue to use biodosime-
try as an ancillary component of radiation dose assessment
for astronauts during extended space flights.
The unique contribution of a biodosimetry program is that it pro-
vides an individual’s dose assessment as estimated from a biological
endpoint. Thus, it includes the response to the cumulative exposure
and allows for an assessment of variations in individual sensitivity.
The fluorescence in situ hybridization (FISH) method is the most
appropriate approach based upon available knowledge, technical
availability, and experience. The current approach of using FISH
for analyzing stable chromosomal translocations in peripheral lym-
phocytes both in preflight and postflight samples appears to be
providing useful information on exposures. The establishment of
calibration curves from individual preflight blood samples increases
the sensitivity. Incorporating analysis of prematurely condensed
chromosomes (PCC) will provide more analyzable cells within a sam-
ple. Improvements that can be envisaged are using chromosome
painting probes and computer analysis that allow for assessment of
translocations in all chromosomes at the same time. This method
has been used successfully for tumor analysis. Automating the vari-
ous FISH methods will increase throughput enormously.
Future considerations for biodosimetry in the area of genomics
or molecular profiling, and technologies for measuring changes in
cellular markers (in response to radiation) are noted in Section 7.
1.10 Immediate Dose Management and ‘‘As Low As
Reasonably Achievable’’
Immediate dose management refers to actions taken to address
high transient exposures in the space radiation environment that
could impact the conduct or completion of the mission or mission
tasks.
Recommendation 14: Implementation of immediate dose man-
agement actions is the responsibility of all team members
12 / 1. SUMMARY AND RECOMMENDATIONS
involved with work impacting the astronaut’s exposure to
radiation. A written plan (notably the flight rules mecha-
nism) should contain the implementing procedures.
ALARA refers to actions taken to keep the doses in all cases as
low as reasonably achievable, by balancing the mission objectives
with practical dose reduction steps.
Recommendation 15: The RHO should assess the opportuni-
ties to apply ALARA. However, an effective ALARA program
depends on everyone involved in the design and management
of spacecraft and missions understanding the space radia-
tion environment and its impact on astronaut radiation expo-
sure. ALARA concepts should be incorporated into the design
of the spacecraft and suits, the preflight planning (including
the planned in-flight procedures), an in-flight review, and a
postflight review.
A number of suggestions bearing on immediate dose management
and ALARA are given in Section 8.4. Three examples are:
● place radiation instruments at locations that provide the best
real-time information on radiation exposure to the astronauts
(for both immediate dose management and ALARA);
● provide areas where astronauts could be moved during high
transient exposures, i.e., move to a safe haven with additional
shielding, and/or reposition the Space Shuttle (for immediate
dose management); and
● provide areas used during off-duty hours and sleeping quarters
with optimized shielding (for ALARA).
1.11 Radiation Safety Training
Recommendation 16: All personnel whose work impacts on
astronaut radiation exposure should be trained in the tech-
niques of radiation protection, with emphasis on implemen-
tation of immediate dose management and ALARA.
The scope and depth of this training should be related to the
corresponding level of impact the individual may have on astronaut
dose. Section 8.5 presents suggested radiation protection training
topics for astronauts, flight directors, flight surgeons, RHOs, other
radiation safety professionals, and other individuals whose work can
affect the astronaut’s radiation exposure. All of these individuals
should be trained in NASA’s operational radiation safety program

1.12 DOSIMETRY RECORD / 13
and how immediate dose management and ALARA actions are
proposed, implemented and made part of the review of actual events,
especially those events involving high transient exposures.
Recommendation 17: Astronauts should be trained in the
proper wearing and care of personal dosimeters. NASA
should have a clear requirement and related training for the
use of personal dosimeters by astronauts in-flight to ensure
that each astronaut has an accurate mission and career
dose record.
1.12 Dosimetry Record
Recommendation 18: The dosimetry record constitutes the
formal documentation for each astronaut’s space-related
radiation exposure history and should contain the cumula-
tive dose from space flight, mission-related aviation activi-
ties, and mission-related biomedical research. The dosimetry
record should contain, or be linked to, all the basic informa-
tion that is necessary to obtain the required dose-limit quan-
tities [gray equivalent (GT) and effective dose (E)], and should
include the low- and high-LET components of the radiation
field.
The dosimetry record, and the other supporting records linked to
it, should be kept in a manner to satisfy a number of purposes
as described in Section 9. These records are important to protect
astronauts and to document radiation exposures. Other radiation
exposure files, such as diagnostic and therapeutic medical radiation
exposures from overall health care that are maintained in the medi-
cal department, should also be linked to the dosimetry record. How-
ever, the diagnostic and therapeutic medical radiation doses should
not be added to occupational doses either for planning purposes or
to limit occupational exposures.
Recommendation 19: Astronauts should receive an annual
confidential report on their radiation dose assessment. The
report should include career radiation doses in terms of effec-
tive dose (E) for stochastic effects and monthly and annual
doses in terms of gray equivalent (GT) for deterministic
effects.
Recommendation 20: The dosimetry record should be
updated retrospectively whenever there is a systematic

14 / 1. SUMMARY AND RECOMMENDATIONS
change in methodology or new information becomes avail-
able. Astronaut dose estimates should be adjusted whenever
differences in the revised dose assessments exceed 30 percent
of the original dose assessment (see discussion of accuracy
in Sections 6.4.1 and 6.4.2).
Existing data related to space missions should be examined and
compared to the dosimetry record to confirm that radiation dose
estimates are based on all available data. If previously unanalyzed
data are found, the data should be identified and representative
samples of the data should be fully analyzed to determine the extent
of their effect on current dose estimates.

2. Objectives of theOperational RadiationSafety Program forAstronauts
There are currently 160 astronauts in the U.S. Astronaut Office
(137 United States astronauts and 23 other international astronauts)
and approximately 40 Russian cosmonauts. The number of United
States astronauts involved in the foreseeable future in LEO activities
is anticipated to be between 200 and 250. Therefore, the operational
radiation safety program for astronauts is for a small population.
The overall objective to assess and control the radiation exposure
of individual astronauts can be broken down as follows: (1) keep
individual doses below the established dose limits to avoid determin-
istic effects; (2) keep accumulated doses over an astronaut’s career
below the established dose limits for stochastic effects; and (3) keep
all astronaut doses as low as reasonably achievable, economic and
social factors being taken into account (i.e., follow the standard
ALARA principle of radiation protection). In the context of near-
Earth space activities, one must also take into account the mission
requirements and the prevailing radiation conditions in LEO.
2.1 The Low-Earth Orbit Program
There are unique considerations in balancing mission objectives
in LEO against the resulting levels of radiation exposure. The deci-
sion to incorporate Russian launch capabilities into the construction
and operation of ISS placed the Station in a high-inclination orbit,
comparable to the previous Russian Mir Space Station. The higher
inclination places ISS in orbits that increase the residence time in
radiation zones where the probability for high-exposure events from
solar energetic particles and penetrating electrons in the outer
radiation belts to occur is higher, compared to the original plan
for a low-inclination orbit, which would have mostly avoided these
radiation zones (NAS/NRC, 2000). This is a particularly important
15

16 / 2. OBJECTIVES OF THE SAFETY PROGRAM
consideration given the extensive extravehicular activities planned
during ISS construction, which will also span the maximum of the
current 11 y solar cycle.
A helpful description of the impact of the high-inclination orbit in
which the astronauts will work is given in a report by the National
Academy of Sciences/National Research Council (NAS/NRC, 2000).
In the quoted text below, abbreviations have been spelled out in
italics.
‘‘As originally conceived in the early 1980s, ISS [the International
Space Station] was to have a low-inclination (28.5 degrees), low-
altitude (350 km) orbit. Then, the SAA [South Atlantic Anomaly . . .
part of the Van Allen Belts] and GCRs [galactic cosmic radiations]
would have been the only significant sources of radiation. SRAG [the
Space Radiation Analysis Group . . . the operational radiation safety
unit at Lyndon B. Johnson Space Center] knows how to design mis-
sion schedules to minimize astronaut exposure to the SAA during
EVAs [extravehicular activities . . . astronauts in space suits outside
a Space Shuttle or station], and there is little anyone can do to
minimize GCR exposure. In 1993, however, the United States agreed
with the Russian Federation to incorporate Russian launch capabili-
ties into ISS construction and maintenance. That agreement brought
with it the need to place ISS in a high-inclination orbit, essentially
the same as that of the Mir space station, 51.6 degrees geographic
[350 to 450 km altitude]. Consequently, ISS and the astronauts who
construct and use it run the risk of being exposed to solar energetic
particles and penetrating electrons in the horns of the outer belt.
Exposure from these sources will be sporadic since SPEs [solar parti-
cle events] follow solar storms and HREs [highly relativistic electrons]
follow magnetic storms and impacts by strong solar wind shocks.
During the declining phase of a solar cycle—perhaps late in ISS
construction—HRE events are also associated with times, lasting
about a week, when solar wind streams are especially fast. Whereas
satellite encounters with the SAA are as predictable as the tides,
usually solar energetic particles, geomagnetic storms, and high-
speed solar wind streams are not reliably predictable, nor is the
intensity of the associated radiation event. The high-inclination orbit
of ISS therefore introduces a new radiation risk factor.
‘‘ISS construction plans call for approximately 33 U.S. shuttle
flights and 10 Russian flights. The construction phase will extend
from 1998 to 2004, which spans the maximum of solar cycle 23, when
SPEs are expected to be most frequent. NASA estimates that during
those years astronaut and cosmonaut construction crews may have
to perform more than 160 EVAs totaling more than 1,100 hours.
During those same years, there will be more than 400 additional

2.2 DOSE LIMITS FOR ASTRONAUTS / 17
hours of EVAs by astronauts and cosmonauts to service and main-
tain the station. The total exceeds 1,500 hours, or 1,000 ISS orbits,
of EVA time.’’
The very real potential that high transient radiation doses to
astronauts will occur occasionally during construction and operation
of ISS was also documented by NAS/NRC (2000). The following two
statements from the report address the potential for high radiation
doses from SPEs and relativistic electrons from the outer belt,
respectively.
‘‘. . . the high-latitude zones to which solar energetic particles have
access show a marked tendency to widen over the polar latitudes
reached by the ISS orbit when SPEs are in progress, a tendency that
becomes more pronounced as SPEs intensify. Two storms during
1989, near the maximum of the last solar cycle, illustrate the point.
The areas around the poles accessible to SPE particles enlarged until
they engulfed more than a quarter of the ISS orbit, and the flux of
particles was high enough to have pushed an astronaut over the
short-term limit for irradiation of skin and eyes during a single ill-
timed 6-hour EVA.’’
‘‘For a portion of nearly every day, some fraction of the ISS orbit lies
within the outer radiation belt, where relativistic electrons reside. At
its maximum, this fraction is about 20 percent. During occasions
called relativistic electron events, which happen on average about
once per month and last several days, the intensity of relativistic
electrons in the belt increases by up to four orders of magnitude.
When the intensity of relativistic electrons is greatest, a single ill-
timed EVA could deliver a radiation dose big enough to push an
astronaut over the short-term limit for skin and eyes.’’
NAS/NRC (2000) also made recommendations for improving the
real-time forecasting of space weather events such as solar wind
conditions (particularly during the current 11 y solar maximum
cycle) and outer radiation belt conditions, and the need for improved
coordination of existing and future space weather forecasting capa-
bilities within NASA, and with the National Oceanic and Atmo-
spheric Administration and the U.S. Air Force. Most of these
improvements will take some time to implement.
2.2 Dose Limits for Astronauts
NCRP reviewed the evolution of dose limits for astronauts and
recommended dose limits specifically for astronauts in LEO in NCRP
Report No. 98 (NCRP, 1989). NCRP recently updated the dose limits

18 / 2. OBJECTIVES OF THE SAFETY PROGRAM
in NCRP Report No. 132 (NCRP, 2000a) to take account of more
recent information on estimates of radiation health effects. The dose
limits for bone marrow, lens of the eye, and skin are for protection
against deterministic effects. The career dose limits are for protection
against delayed stochastic effects and are based on a lifetime excess
risk of cancer mortality of three percent.1 The main features of the
current dose limits and the quantities used to assess astronaut expo-
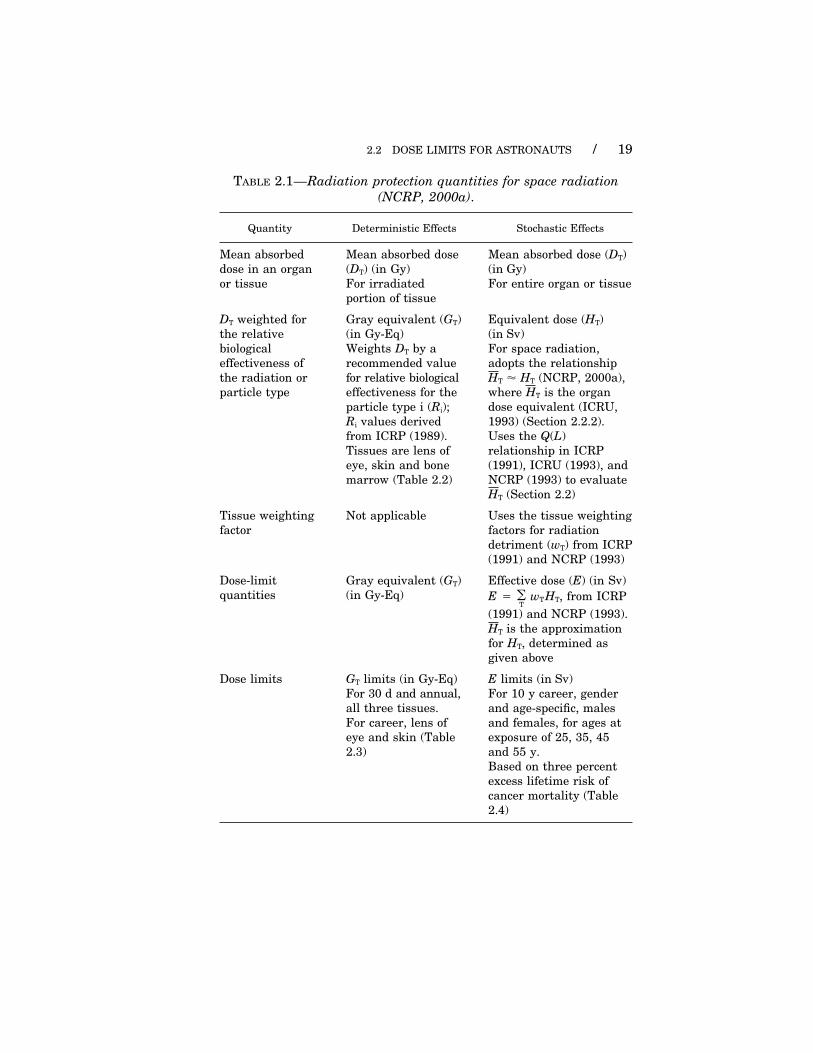
sures against the dose limits are summarized in Table 2.1.
2.2.1 Deterministic Limits
The dose limits for deterministic effects are expressed in terms of
gray equivalent, where gray equivalent is the mean absorbed dose
in an organ or tissue modified by a recommended value, for radiation
protection purposes, of the relative biological effectiveness (i.e., a
best estimate) of a given particle type, as given in NCRP (2000a).2
In this Report, a conventional notation is used for the quantity gray
equivalent, namely:
GT � RiDT, (2.1)
where GT is gray equivalent, Ri is the recommended value of the
relative biological effectiveness for particle type i referred to above,
and DT is the mean absorbed dose in an organ or tissue.
The values for Ri are given in Table 2.2. The dose limits for deter-
ministic effects are given in Table 2.3. The special name for the unit
of DT is gray (Gy) and the name of the unit for GT is gray equivalent,
with the notation Gy-Eq (NCRP, 2000a).
2.2.2 Stochastic Limits
The career limits for delayed stochastic effects are expressed in
effective dose (E), where:
E � �T
wTHT. (2.2)
1The recommended dose limit for an astronaut entails a similar lifetime excess risk
of cancer mortality (three percent) as the dose limit for a terrestrial worker, if both
an astronaut and a terrestrial worker reached the maximum value of the respective
dose limit during their working lifetimes.2NCRP (2000a) recommended that the mean absorbed dose in an organ or tissue
(DT) be modified by the recommended values for relative biological effectiveness to
adjust for radiation quality for deterministic effects because the usual formulation
for equivalent dose (HT) is obtained by applying radiation weighting factors (wR) which
are applicable to stochastic effects.
2.2 DOSE LIMITS FOR ASTRONAUTS / 19
TABLE 2.1—Radiation protection quantities for space radiation
(NCRP, 2000a).
Quantity Deterministic Effects Stochastic Effects
Mean absorbed Mean absorbed dose Mean absorbed dose (DT)
dose in an organ (DT) (in Gy) (in Gy)
or tissue For irradiated For entire organ or tissue
portion of tissue
DT weighted for Gray equivalent (GT) Equivalent dose (HT)
the relative (in Gy-Eq) (in Sv)
biological Weights DT by a For space radiation,
effectiveness of recommended value adopts the relationship
the radiation or for relative biological HT � HT (NCRP, 2000a),
particle type effectiveness for the where HT is the organ
particle type i (Ri); dose equivalent (ICRU,
Ri values derived 1993) (Section 2.2.2).
from ICRP (1989). Uses the Q(L)
Tissues are lens of relationship in ICRP
eye, skin and bone (1991), ICRU (1993), and
marrow (Table 2.2) NCRP (1993) to evaluate
HT (Section 2.2)
Tissue weighting Not applicable Uses the tissue weighting
factor factors for radiation
detriment (wT) from ICRP
(1991) and NCRP (1993)
Dose-limit Gray equivalent (GT) Effective dose (E) (in Sv)
quantities (in Gy-Eq) E � �T
wTHT, from ICRP
(1991) and NCRP (1993).
HT is the approximation
for HT, determined as
given above
Dose limits GT limits (in Gy-Eq) E limits (in Sv)
For 30 d and annual, For 10 y career, gender
all three tissues. and age-specific, males
For career, lens of and females, for ages at
eye and skin (Table exposure of 25, 35, 45
2.3) and 55 y.
Based on three percent
excess lifetime risk of
cancer mortality (Table
2.4)

20 / 2. OBJECTIVES OF THE SAFETY PROGRAM
TABLE 2.2—Ri values for converting DT to GT for deterministic
effects (adapted from ICRP, 1989; NCRP, 2000a).a
Particle Type Ri (range for value)
1 to 5 MeV neutrons 6.0b (4–8)
5 to 50 MeV neutrons 3.5b (2–5)
Heavy ions (e.g., helium, carbon, neon, argon) 2.5 c (1–4)
Protons �2 MeV 1.5 (—)
aRBE values3 for late deterministic effects are higher than for early effects
in some tissues and are influenced by the doses used to determine the
RBE values.bThere are not sufficient data on which to base an Ri for early or late
effects4 induced by neutrons of energies �1 MeV or greater than about
25 MeV. However, based on the induction of chromosome aberrations, using
250 kVp x rays as the reference radiation, RBE values for neutrons �1 MeV
are comparable to those for fission spectrum neutrons. It is reasonable to
assume that RBE values for neutrons �50 MeV will be equal or less than
those for neutrons in the 5 to 50 MeV range.cThere are few data for the tissue effects of ions with Z � 18, but RBE
values for iron ions (Z � 26) are comparable to those for argon. Based on
the available data, an Ri of 2.5 for heavy ions is reasonable. One possible
exception is cataract of the lens of the eye because high RBE values for
cataracts in mice have been reported.
HT is the equivalent dose and wT is the tissue weighting factor (ICRP,
1991; NCRP, 1993). The career limits are specified by gender and
age, and take into account the gender and age-adjusted cancer mor-
tality risk coefficients (i.e., the differential risk per unit dose) for the
same overall three percent excess lifetime risk. The career dose limits
are given in Table 2.4.
The quantity E is obtained as follows for the space radiations.
First, the dose equivalent (H ) is defined at a point in tissue and can
be directly measured (ICRU, 1993). H is given by:
H � �L
Q(L) D(L) dL. (2.3)
Q(L) is the quality factor (Q) for particles as a function of LET (L)
and D(L) is the spectral distribution in terms of L of the absorbed
3The acronym RBE refers to experimental data on relative biological effectiveness.4The symbol Ri refers to recommended values of relative biological effectiveness
(i.e., best estimates) for radiation protection purposes that are used for obtaining GT,
as discussed in NCRP (2000a).

2.2 DOSE LIMITS FOR ASTRONAUTS / 21
TABLE 2.3—Recommended GT limits for deterministic effects
(all ages) (NCRP, 2000a).
GT Limit
(Gy-Eq)
Bone Marrow Lens of the Eye Skin
Career —a 4.0 6.0
1 y 0.50 2.0 3.0
30 d 0.25 1.0 1.5
aThe career limits for stochastic effects given in Table 2.4 are considered
to be more than adequate for protection of bone marrow against deterministic
effects for a career. The career limits are expressed in terms of E. The wR
values (for stochastic effects) used to convert DT to E are based on Q(L) and
are higher than the Ri values (for deterministic effects) used to convert DT
to GT. Therefore, there is no need for a career deterministic limit for the
bone marrow. The career stochastic limit is more restrictive and would
always be expected to result in a lower DT to the bone marrow for irradiation
conditions in space.
TABLE 2.4—Ten-year career E limits based on three percent excess
lifetime risk of fatal cancer (NCRP, 2000a).a,b
E Limit
(Sv)Age at Exposureb
(y) Female Male
25 0.4 0.7
35 0.6 1.0
45 0.9 1.5
55 1.7 3.0
aA three percent excess lifetime risk of cancer mortality has additional
components of detriment associated with it, namely the risk of heritable
effects (0.6 percent) and the detriment associated with nonfatal cancer (also
0.6 percent), for a total detriment of 4.2 percent. These nominal risks are
as given in ICRP (1991) and NCRP (1993).bThe career E limits are for a 10 y career beginning at the age of first
exposure. For situations in which careers differ in length from 10 y, or for
careers that start at other than the designated ages, additional advice is
provided in Section 6.4 of NCRP (2000a).

22 / 2. OBJECTIVES OF THE SAFETY PROGRAM
dose at the point (D). For the complex mixtures of high- and low-LET
radiations experienced in LEO, the practice in the space radiation
protection community is to average the point quantity H over the
organ or tissue of interest by means of computational models to
obtain the organ dose equivalent (ICRU, 1993), which is required
for radiation protection purposes but cannot be directly measured.
In this Report, the symbol HT is used for the quantity organ dose
equivalent. NCRP (2000a) adopted HT as an acceptable approxima-
tion for HT for stochastic effects: Therefore, in general terms:
HT � MT�1 �
x�
L
Q(L) D(L) �(x) dL dx, (2.4)
where there is a second integration over the points x in tissue T with
tissue density �(x) and total mass MT. For the radiations in LEO,
the quantities HT and HT are interchangeable for radiation protection
purposes. The methods used to evaluate HT are discussed in Sections
5 and 6. Therefore, E � wT HT, and E, H, HT and HT are expressed
in sievert (Sv).5
The Q(L) relationship is given in ICRP (1991), ICRU (1993), and
NCRP (1993), where:
Q(L) � 1 for: L � 10 keV �m�1
Q(L) � 0.32 L � 2.2 for: L � 10 to 100 keV �m�1 (2.5)
Q(L) � 300 L�1/2 for: L � 100 keV �m�1
The Q(L) relationship is consistent with current knowledge of the
general trend of relative biological effectiveness for cell killing and
induction of mutation from HZE particles.
2.3 Operational Radiation Protection Considerations
This Report concentrates on the specific technical considerations
necessary to implement an operational radiation safety program for
the principles of dose limitation and ALARA for astronauts working
in LEO. In particular, the Report describes the radiation components
5This procedure for obtaining E for space radiations differs from that used for
terrestrial radiation environments, in that HT (calculated as given above) replaces
HT � wR DT, where wR (for external radiation) is a nominal value based on the type
and energy of the radiation incident on the body (ICRP, 1991; NCRP, 1993). The
practice of obtaining HT permits more complete consideration of the Q(L) relationship
for the complex space radiation environments.

2.3 OPERATIONAL RADIATION PROTECTION CONSIDERATIONS / 23
of the space environment (Section 4) from the perspective of the
measurements needed to support the dose assessment approach (Sec-
tion 5) used to generate values for the radiation protection quantities
recommended for space activities, that is, GT, HT (i.e., the surrogate
for HT), and E. A key aspect of the Report is the recommendations
for collection of observable data (Section 6) in both active and passive
modes. The observable data help implement the recommended dose
assessment approach, in conjunction with an array of radiation
transport models and codes (Section 5). These recommendations are
developed fully in this Report, taking into account the practical
limitations on the radiation detection devices and protective systems
that can be available in-flight.
The availability of credible estimates for the recommended radia-
tion protection quantities would help accomplish the following objec-
tives of the operational radiation safety program:
● to facilitate actions, both in advance of a mission and in-flight,
that respond to space radiation conditions or mission decisions
that in turn significantly influence the levels of radiation expo-
sure to the astronauts, and radiation protection decisions that
in turn significantly influence the conduct of the mission;
● to collect and record astronaut doses for individual mission and
cumulative career records. These records can also be used in
prospective radiation-related health studies of the Astronaut
Corps or to assist retrospective dosimetry to update the records
for previous activities of individual astronauts; and
● to identify, plan and inform practical ALARA actions to avoid
unnecessary levels of radiation exposure. These ALARA actions
would address both radiation exposures that are adjunct to a
mission (e.g., ground-based space-related biomedical research)
and those that occur in-flight (e.g., mission experiments using
radiation sources, or avoidance of higher exposure locations in
space vehicles when an ongoing mission task or activity does
not require presence there).
3. Current Management ofAstronaut RadiationSafety Program
The management of radiation dose received by astronauts in LEO
involves many individuals. Typically, astronauts do not play an
active role in decision making and policy regarding radiation issues.
Instead, the flight director and flight surgeon direct their actions,
with the help of radiation experts.
At the Lyndon B. Johnson Space Center (JSC), there are two
radiation expert resources, SRAG and the RHO. These individuals
work with the medical officers, the payload officers, mission planners,
outside agencies, and the flight directors to provide radiation exper-
tise in developing and interpreting radiation flight rules that govern
the conduct of a flight, from mission planning through the end of a
space flight, with regard to crew radiation exposure and adherence
to ALARA. Dose limits and administrative levels are developed and
are then written as flight rules by NASA radiation experts.6 The
flight rule approval process involves a variety of NASA managers
from different departments so that management becomes very famil-
iar with the rules and supporting rationale. In the process of approv-
ing flight rules, program management is educated and trained on
the risks associated with radiation exposure. A flight director chairs
the Flight Rule Change Board, which approves and incorporates all
new rules and rule changes. Once approved and incorporated, the
flight rules are ‘‘tested’’ during simulations to ensure proper interpre-
tation and response to a given scenario.
3.1 Flight Rules for Management of Dose
The flight rules are a comprehensive set of rules, reviewed and
updated continuously, governing all the procedures and operation
6 Dose limits are developed through input from NCRP and the Occupational Safety
and Health Administration recommendations. Administrative levels are developed
internally by NASA.
24

3.1 FLIGHT RULES FOR MANAGEMENT OF DOSE / 25
of space vehicles. Extensive rules regulate management of normal
operations and off-nominal operations of all Space Shuttle and ISS
systems, such as main engines, life support, computer, electrical,
and hydraulic systems. The flight rules that govern measurement
of the radiation environment and management of crew exposure to
radiation are contained in one section of the flight rules titled ‘‘Space
Environment,’’ which incorporates the following:
● general definitions which define event conditions (e.g., SPE,
energetic SPE, geomagnetic storm) and ALARA;
● radiation subsystem loss definitions which define what deter-
mines monitoring and measuring equipment to be out of service;
● crew exposure management which defines actions to assist in
management of the crew exposures;
● rules that are in place to maintain exposure ALARA and below
legal limits;
● radiation subsystem management which are special rules for
radiation equipment operation; and
● designated maintenance items which are additional criteria that
indicate hardware may be inoperable.
Administrative limits or ‘‘action levels’’ are published in the flight
rules to serve as a guide, with ALARA, to initiate more stringentdose management activities for a mission if there is a higher thanprojected accumulated exposure. The administrative limits for a mis-sion are monthly, cumulative limits 5 mGy above the projectedabsorbed dose for that part of the solar cycle. There are also 30 dand 1 y maximum allowable exposure limits to manage acute expo-sures. If the exposure on a particular mission is greater thanexpected, actions are detailed in the flight rules to remain withinthe crew administrative limits. Some actions that the ground andcrew might consider are: restricting crew location within ISS,rescheduling EVAs, reducing the number of EVAs, terminatingan EVA in progress, deferring ISS reboost, shortening crew timein orbit, or returning the crew to Earth. Crew safety is the high-est priority. Many factors determine the course of action during aflight. SRAG, the RHO, and the flight surgeon work with the flightdirector to determine the best course of action when these rules areconsidered.
The NASA term ‘‘administrative limit’’ or ‘‘action level’’ corres-ponds to the term ‘‘administrative level’’ used elsewhere in thisReport. The NASA term ‘‘exposure limit’’ corresponds to the term‘‘dose limit’’ used elsewhere in this Report.
There is a set of flight rules governing the conduct of a SpaceShuttle mission (e.g., NASA, 2000a), and a set governing the conductof an ISS mission (e.g., NASA, 2000b).
26 / 3. CURRENT MANAGEMENT OF SAFETY PROGRAM
3.2 Biomedical Research
Because astronauts may also receive occupational radiation dose
during the conduct of biomedical experiments associated with space
flights, these experiments need to be approved for funding and perfor-
mance during flight at NASA Headquarters. Exposure to radionu-
clides and x rays associated with biomedical experiments may
contribute substantially to an astronaut’s total dose. Any biomedical
experiment involving radiation exposure is approved by an expert
NASA radiation panel. The RHO, a flight surgeon, and a senior
medical officer are among those who serve on this panel. After
approval by this group, the JSC Institutional Review Board reviews
the experiment and may give approval. As with all biomedical experi-
ments, astronauts may choose whether or not to volunteer to partici-
pate. If astronauts choose to volunteer, they do so with informed
consent.
3.3 Individuals Involved in Management of Dose
3.3.1 Astronaut
Approximately 160 astronauts are active in the U.S. Astronaut
Office. One or two astronauts (generally astronauts with medical
backgrounds) represent the Astronaut Office’s position regarding
radiation protection policy, procedures and concerns in the various
meetings and committees. Prior to their flight, if radiation exposure
is expected to be more than minimal, the affected astronauts may
participate more actively in the decision-making process concerning
their particular flight. In general, astronauts assigned to fly longer
missions on ISS show more interest in radiation protection issues
and take a more active role in developing procedures to reduce expo-
sure, such as determining the ‘‘best’’ sleep location.
3.3.2 Flight Director
Approximately 20 flight directors are stationed at JSC. Each mis-
sion is assigned a ‘‘lead’’ flight director who provides input and makes
decisions during the planning and training period preflight. During
a mission, the flight director is the final decision maker in the Mission
Control Center with regard to all aspects of the mission including
mission replanning, and flight rule interpretation and implementation.

3.3 INDIVIDUALS INVOLVED IN MANAGEMENT OF DOSE / 27
The flight director weighs all risks and benefits during this process
with the aid of systems experts on the flight control team and relies
heavily on the RHO, SRAG and the flight surgeon when decisions
regarding radiation protection issues need to be made. The flight
director weighs the radiation risks against the risks and mission
impacts of altering other flight procedures (for example, delayed or
shortened EVA, or early deorbit and landing at a contingency landing
site). The Chief of the Flight Director’s Office chairs the NASA Flight
Techniques Board that approves flight rules.
3.3.3 Flight Surgeon
Approximately 15 NASA flight surgeons are stationed at JSC.
When serving as a crew surgeon for a specific flight crew, the flight
surgeon is responsible for that crew’s health and safety during all
aspects of flight training, mission execution, and postflight rehabili-
tation and recovery. The flight surgeon briefs the crew preflight
and postflight regarding radiation protection issues and personal
radiation dose. During a space flight the flight surgeon is the primary
interface between SRAG and the flight director in the Mission Con-
trol Center when issues arise pertaining to radiation exposure. Dur-
ing a mission, the flight surgeon and SRAG provide expert flight
rule interpretation for the flight director and mission management,
and assist in mission replanning, when necessary. Generally, one
member of the Flight Surgeon’s Office is designated to be the ‘‘resi-
dent expert’’ on radiation protection issues. This flight surgeon serves
on various committees and groups that address radiation protection
issues. One committee is the Radiation Integrated Product Team,
which is co-chaired by the RHO and the flight surgeon and also
includes experts outside of NASA. This committee meets quarterly
to discuss and formulate possible flight research projects, and to
consider operational issues, such as adequacy of onboard radiation
monitoring. This flight surgeon is also the point of contact to commu-
nicate new information to the rest of the flight surgeon community.
3.3.4 Radiation Health Officer
The RHO provides recommendations to minimize crew exposures
through design and development of radiation protection strategies,
in NASA policy documents, during mission planning, and real-time
during space missions. The RHO tracks crew exposures against
career limits, provides risk interpretation for acute exposures, and
interfaces with the RHOs from the international partners.

28 / 3. CURRENT MANAGEMENT OF SAFETY PROGRAM
3.3.5 Space Radiation Analysis Group
SRAG, along with the RHO, are the NASA radiation specialists
responsible for promoting ALARA and ensuring compliance with
procedures to implement ALARA during all phases of mission design,
planning and flight. They serve as the interface to all other groups
and individuals in the space flight program who have responsibilities
that can affect crew radiation exposure. With the exception of the
flight surgeons, no other individuals involved in mission planning
and operational decision making have in-depth training or experi-
ence in radiation protection issues. During space flights, SRAG has
the following responsibilities: monitoring of space weather; space
radiation environment contingency response and analysis; radiation
instrument operations; tracking of crew daily and cumulative dose;
EVA planning, support and monitoring; and interfacing with outside
support groups (i.e., National Oceanic and Atmospheric Administra-
tion, U.S. Department of Defense). During a mission, SRAG inter-
faces with mission planners and flight controllers, including the
flight director, to update mission significant radiation events and
provide expertise, particularly when transient events in the space
radiation environment produce a potential for high doses to the
astronauts.
4. Radiation Environmentin Low-Earth Orbit
The radiation environment external to a spacecraft in LEO con-
sists of electrons, positrons, neutrons, protons and heavier nuclei
(up to Z � 92). Sources include: GCR from deep space; SPEs produced
by coronal mass ejections or by acceleration in solar flare events;
particles trapped in Earth’s magnetic field; and scattering from
Earth’s atmosphere (albedo neutrons, electrons and protons). Energ-
ies range from a few electron volts for trapped electrons and albedo
neutrons to in excess of 1014 MeV for GCR ions.
The space radiation environment is modulated by spatial and tem-
poral factors including the 11 y solar cycle and the solar wind, and
Earth’s magnetic field, which traps some particles and deflects oth-
ers. The particle distributions are sensitive to both inclination and
altitude. GCR is approximately isotropic in deep space, but in LEO
the GCR intensity is modulated by the geomagnetic field. Due to the
shape of Earth’s magnetic field lines, high-inclination Space Shuttle
flights and ISS (51.6 degrees) are exposed to higher GCR fluxes than
are low-inclination Space Shuttle flights (e.g., 28.5 degrees). Earth’s
magnetic field varies in strength and configuration over timescales
from days to years. It is influenced by changes in activity on the
surface of the sun over the 11 y solar cycle, but can also exhibit acute
changes as a result of solar storms. The January 1997 geomagnetic
storm moved the South Atlantic Anomaly (SAA) by nearly 80 km
(Badhwar, 2001).7
Protons and electrons are trapped in belts at various altitudes
and inclinations. If a spacecraft orbit intersects a belt, the intensity
of the charged particles and the corresponding dose rate onboard
will increase. These belts are slowly modulated by solar activity;
however, the major influence on dose rate is the frequency and dura-
tion of spacecraft transits through the belts, which are on the order of
minutes to tens of minutes in LEO. Active dosimeters can distinguish
between trapped particles and GCR by separating the data into time
7 Badhwar, G.D. (2001). Personal communication (Lyndon B. Johnson Space Center,
National Aeronautics and Space Administration, Houston, Texas).
29

30 / 4. RADIATION ENVIRONMENT IN LOW-EARTH ORBIT
periods corresponding to the parts of the orbit that intersect the
trapped radiation belts.
Coronal mass ejections or flares can generate high intensities of
charged solar energetic particles, primarily protons, that may even-
tually intercept the spacecraft. The occurrence of SPEs is unpredict-
able. Real-time detectors are needed to confirm the onset and
duration of an event in order to initiate countermeasures in the
spacecraft and to avoid high exposures during an EVA.
Although an SPE may last for a short period of time, disturbances
of the trapped belts, and consequently elevated radiation levels, in
particular the intensity of electrons outside of the spacecraft, can
persist for times on the order of several days. Most of these electrons
will not penetrate the wall of the spacecraft, but could penetrate the
space suits worn during EVA, resulting in substantial doses to the
skin and eyes. Time-dependent factors are discussed in greater detail
in Appendix A.
Nuclear interactions of neutrons, protons and heavier nuclei with
spacecraft, space suits, Earth’s atmosphere, and the human body
produce secondary particles that add to the radiation field.
A more detailed summary of the near-Earth radiation environment
and the factors that modulate it can be found in NAS/NRC (2000)
and NCRP (2000a) and references therein.
Radiation monitoring instrumentation and measurement strate-
gies vary according to charge, particle type, energy, and where the
measurements are made. For purposes of this Report, we will classify
the radiation environment according to particle types and energies
and where the measurements are to be made, namely: outside the
spacecraft, inside the spacecraft, and inside EVA suits. The figures
in parentheses are the approximate particle ranges of interest in
energy (in MeV) and the unrestricted linear energy transfer (L�) in
water (in keV �m�1).
4.1 Trapped Electrons (0.5 to 6 MeV; �0.2 keV �m�1)
Trapped electrons with energies �0.5 MeV will penetrate some
parts of EVA suits. Electrons experience primarily electromagnetic
interactions. Because they are singly charged point particles and
not subject to strong nuclear interactions, secondary particle produc-
tion is limited to electrons, positrons and photons (through annihila-
tion and bremsstrahlung), which do not contribute substantially to
the radiation dose. Principal measurement locations are outside the
spacecraft and inside EVA suits. For aluminum shielding, primary

4.4 TRAPPED AND SOLAR PROTONS / 31
electrons are the dominant source of dose only for shields with areal
densities �0.15 g cm�2 (NCRP, 2000a). The relative importance of
electron and proton doses inside EVA suits is under study (Wilson
et al., 2001; Zeitlin, 20008).
4.2 Reentrant and Splash Albedo Electrons
(1 MeV to �1 GeV; 0.2 to �3 keV �m�1)
Reentrant electrons are the decay products of unstable nuclei pro-
duced by the nuclear interactions of trapped GCR ions. Splash albedo
electrons are scattered upward by interactions in the atmosphere.
The high energies of the parent nuclei boost these electrons to much
higher energies than trapped electrons. Badhwar et al. (2001)
recently made a detailed study of the contribution of reentrant and
albedo electrons at ISS altitude and inclination to the dose to the
bone marrow during EVA. They found the dose to be more than 10
times greater than the dose from trapped electrons. Moreover, the
hardness of the reentrant electron spectrum makes the dose from
those electrons rather insensitive to the addition of shielding, at
least at the level practical for an EVA suit. So while the trapped
electron dose will still dominate in thinly shielded locations, the
reentrant and splash electron dose dominates as the shielding thick-
ness is increased. The high energies of these electrons dictate that
measurements be made inside and outside the spacecraft, and inside
EVA suits.
4.3 Trapped Protons (�10 MeV; �5 keV �m�1)
Protons at energies �10 MeV (on the order of the nuclear binding
energy) will produce slow target fragments through compound
nucleus formation and decay. However, they will not penetrate space-
craft or EVA suits and therefore are not a measurement objective.
4.4 Trapped and Solar Protons and Light
Nuclear Particles (10 to 400 MeV; 0.3 to 5 keV �m�1)
Protons with energies greater than approximately 10 MeV will
penetrate EVA suits and spacecraft walls, and more energetic protons
8 Zeitlin, C.J. (2000). Personal communication (Lawrence Berkeley National Labora-
tory, Berkeley, California).

32 / 4. RADIATION ENVIRONMENT IN LOW-EARTH ORBIT
will penetrate into locations that are more heavily shielded, e.g., by
equipment racks or storage lockers. Nuclear interactions in materi-
als and tissue will produce low-energy, highly ionizing target frag-
ments and will knock out light nuclear particles (Z � 1, 2 and
neutrons) with velocities comparable to that of the projectile. There
is a small component of low-energy SPE light ions, but they are
thought to contribute a negligible amount to radiation risk (NCRP,
2000a). Radiation monitors and dosimeters sensitive to high-energy
SPE protons and light nuclear particles can be placed inside and
outside EVA suits and spacecraft.
4.5 Galactic Cosmic Radiation Ions and High-Energy
Secondary Fragments
(�50 MeV n�1; Z � 1; 1 to 1,000 keV �m�1)
The GCR ion spectrum peaks at energies around a few hundred
MeV n�1. Charged particles at these energies can penetrate into
the interior at many spacecraft locations and through substantial
thicknesses of tissue. Nuclear interactions will produce high- and
low-energy secondary charged particles, which are often more pene-
trating, including pions. The high-energy secondary particles arise
mainly from projectile fragmentation and will have velocities compa-
rable to that of the primary. Pions are created in nuclear interactions
above a few tens of million electron volts. The contribution of pions
to the dose is not known, but is under study at this writing (Wilson,
2000).9 Primary and secondary ions over a wide energy range will
be present at all locations of interest, both inside and outside EVA
suits and spacecraft.
4.6 Charged Target Fragments
(�10 MeV n�1; 2 to 1,200 keV �m�1)
Target fragments (i.e., pieces of the struck atomic nucleus) pro-
duced in nuclear interactions have very short range and therefore
deposit a large amount of energy very close to the location where
they are created. If this is within the human body, they can produce
substantial biological effects. The most probable energy is �5 MeV,
9 Wilson, J.W. (2000). Personal communication (Langley Research Center, National
Aeronautics and Space Administration, Hampton, Virginia).

4.8 SUMMARY FOR PARTICLE TYPES / 33
the average kinetic energy is 10 MeV, and the distribution falls to
one percent of the peak at 40 MeV (Shavers, 1999; Wilson et al.,
1988a; 1988b). Measurements of these particles would be needed
only inside space suits and spacecraft.
4.7 Neutrons (0.1 to 500 MeV)
Neutrons present in LEO are produced by nuclear interactions in
the upper atmosphere (albedo neutrons), and by interactions of high-
energy protons and heavier nuclei in shielding and tissue. The neu-
trons in turn interact with atomic nuclei to produce highly ionizing
charged secondary particles.
Measurements at high orbital inclination (57 degrees, slightly
higher than the 51.6 degrees for ISS) showed that at moderately
shielded locations most of the neutron H came from neutrons above
1 MeV (Badhwar et al., 1996a). Armstrong and Colborn (1992) calcu-
lated that for GCR-produced neutrons, almost half of the neutron H
is from neutrons above 10 MeV, and Armstrong recently calculated
that up to 20 percent of the total H on ISS from all particle types
will be from neutrons with energies �10 MeV (NASA, 2001).
A recent workshop considered the contribution of neutrons to radi-
ation dose to crews in LEO (NASA, 2001). The workshop concluded
that no single detector can cover the wide energy range of interest,
and that the detectors currently in use have not been adequately
calibrated. TLDs used on the Space Shuttle and ISS are ‘‘almost
completely insensitive to neutrons’’ and ‘‘measure absorbed dose and
not the biologically important dose equivalent.’’ Because of the high
penetrating power of neutrons, measurements are needed internal
and external to spacecraft, and inside EVA suits.
4.8 Summary for Particle Types
Table 4.1 summarizes the locations where radiation measure-
ments are needed as a function of the particle types discussed in
Section 4.1 through 4.7. The relative contributions to D and H from
each component (including the secondary radiation) at each location
will vary according to several factors, including the spacecraft inter-
nal mass distribution, the EVA suit design and materials, and the
site of interest within the human body. As a rule, D due to electrons
will be insignificant for all but the most thinly shielded locations of
an EVA suit.
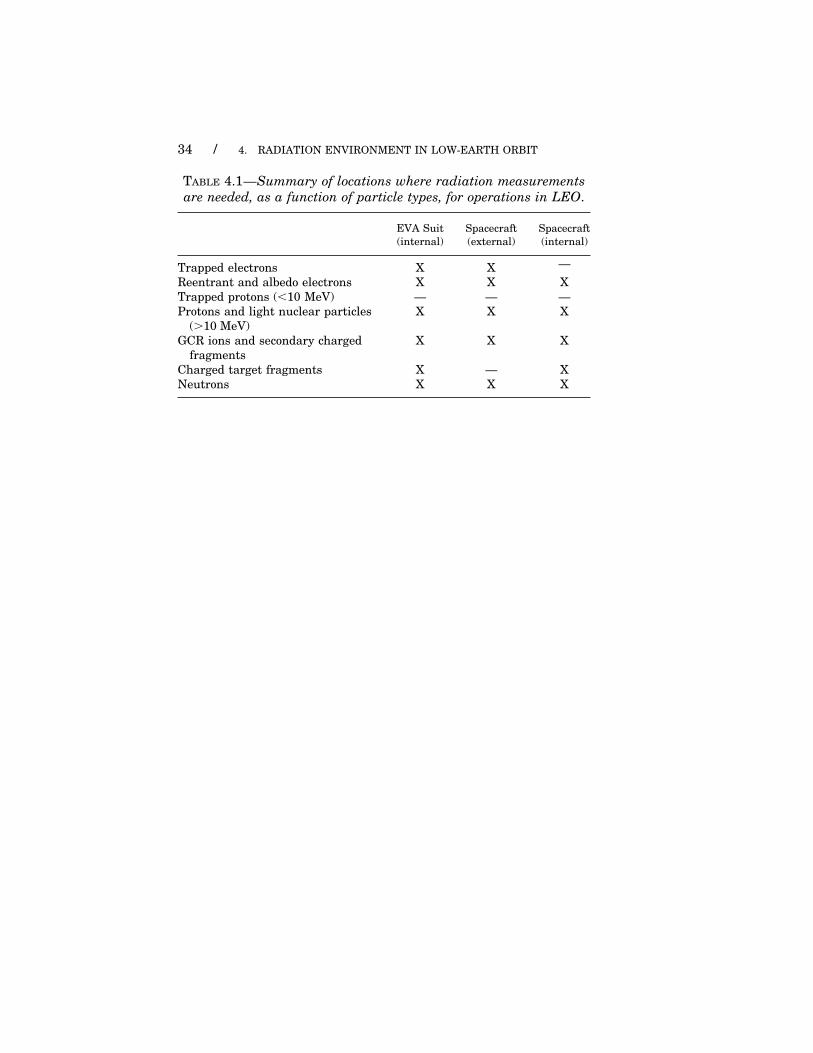
34 / 4. RADIATION ENVIRONMENT IN LOW-EARTH ORBIT
TABLE 4.1—Summary of locations where radiation measurements
are needed, as a function of particle types, for operations in LEO.
EVA Suit Spacecraft Spacecraft
(internal) (external) (internal)
Trapped electrons X X —
Reentrant and albedo electrons X X X
Trapped protons (�10 MeV) — — —
Protons and light nuclear particles X X X
(�10 MeV)
GCR ions and secondary charged X X X
fragments
Charged target fragments X — X
Neutrons X X X

5. Approach to DoseAssessment forAstronauts
Dose assessment requires evaluation of specific quantities to man-
age exposures at the time of operation and for implementation of
career and short-term limits. The basic quantities to be evaluated
are given in Table 2.1 and the corresponding limitations are given
in Tables 2.3 and 2.4. The means by which dose is evaluated in
practice will be discussed in this Section, as well as the relationship
of radiation environment models, shielding models, and radiation
monitoring both inside the spacecraft and outside.
A basic quantity is mean absorbed dose in an organ or tissue (DT).
It is calculated from the distribution of D at points in the relevant
organ or tissue in terms of the L contributions at the specific points
[Di(L,x)], and averaged over the organ or tissue, as shown below.
The dose contribution from particles of type i with L at point x is:
Di(L,x) � � dt � �(x)�1 L &i[Ei(L),�,x,t] � dEi(L)/dL � d�, (5.1)
where &i[Ei(L),�,x,t] is the fluence of particle type i at the point x
at time t with energy Ei(L) (the multi-valued energy for given L of
a particle i) moving in direction �, L is the linear energy transfer
in appropriate units, � dEi(L)/dL � is the multi-branched derivative,
and �(x) is the tissue mass density.
DT is evaluated as the mean absorbed dose over all radiation com-
ponents i and organ tissue T as:
DT � MT�1 �
x
�(x) dx �i
� Di(L,x) dL, (5.2)
where MT is the total tissue mass.
The dose equivalent is defined at a point x in the tissue as:
H(x) � �i
� Qi[Li (E)] Di(L,x) dL, (5.3)
where Qi[Li(E)] is the quality factor for particle type i with Li(E)
(the multi-valued L for a given E of a particle i).
35

36 / 5. APPROACH TO DOSE ASSESSMENT FOR ASTRONAUTS
The organ dose equivalent (HT) is determined as an average of H
over all points in the organ or tissue as:
HT � MT�1 �
x
�(x) H(x) dx (5.4)
where the bar denotes the averaging process and T denotes the
organ or tissue over which the average is performed. Since, for space
radiations, HT is an acceptable approximation for HT (Section 2.2),
the effective dose (E) is then given as:
E � �T
wT HT � �T
wT HT. (5.5)
The evaluation of gray equivalent (GT) in a specific tissue of type T
is given in terms of the field-weighted quantities as:
GT � �i
Ri DT,i (5.6)
where DT,i is the mean absorbed dose to tissue T from the interior
field component i and Ri is the recommended value of the relative
biological effectiveness (i.e., a best estimate) for the specified particle
type i given in Table 2.2. Note that GT is not a point function and
leads to computational complexity. Note that the Ri values are energy
independent except those for neutrons (Table 2.2). A dose-averaged
value for neutrons (Rn,T) can be evaluated for specific tissues knowing
the neutron field and the appropriate tissue dose conversion factors
[Cn,T(E)] (ICRP, 1996; ICRU, 1998; Yoshizawa et al., 2000) as:
Rn,T �� dt � Rn(E) Cn,T(E) &n(E,�,x,t) dE d�
� dt � Cn,T(E) &n(E,�,x,t) dE d�, (5.7)
where &n(E,�,x,t) is the ambient neutron interior fluence at the
astronaut location in the spacecraft. The use of Rn,T reduces the
computational complexity but there is as yet insufficient RBE data
for most radiation types to evaluate these quantities for the full
interior radiation field. NCRP (2000a) has discussed the use of
conservative values for Ri components for which RBE values are
unknown (Table 2.2).
Figure 5.1 outlines the dose assessment scheme for use in LEO.
The knowledge required for evaluation of organ or tissue dose and
the dose-limit quantities for the astronaut includes the:
● radiation environment at the exterior surface of the spacecraft
● relationship of the exterior radiation environment to the interior
radiation environments of the Space Shuttle, ISS, and space suit

5. APPROACH TO DOSE ASSESSMENT FOR ASTRONAUTS / 37
Dose Records:
E, GT,H
T
Human Shielding Model
Linked personal records
External: I
Internal: D, H, D(L), f (y)
Personal: D, H, D(L)
Measurements Records:
Crew Personal Dosimetry
Measurements:
D, H, D(L)
D, ),)
Spacecraft External
Measurements:
, I
Occupancy
Factors
Internal Environment
STS/ISS/Spacesuit
Shielding models
Environmental Models:
Galactic Cosmic Rays
Albedo Neutrons
Trapped Particles
Solar Particle Events
List of quantities:
&i(E,�,t ): external or internal fluence; with particle type i, time t, energy E, direction �
I: ionization current in a tissue-equivalent ion chamber
D: absorbed dose, at a point
H: dose equivalent, at a point
D(L): absorbed dose distribution over L, at a point
f(y): frequency distribution of lineal energy
E: effective dose
GT: gray equivalent
HT: organ dose equivalent; approximation to equivalent dose (HT)
Fig. 5.1. Recommended dose assessment method.
● timeline of astronaut activity within those environments
● transmission of radiation from the internal radiation environ-
ment to specific organ tissues
● relationship of the organ exposure field to organ or tissue dose
● relationship of organ or tissue dose to the dose-limit quantities
Use of data measured during a mission relies on the knowledge
of a relation between the measured values and computed results.
This is accomplished with an adequate understanding of the
response function of the measurement device to predict the response
from the expected particle field. Adjustments in the estimated fields
from calculations are obtained by comparing predictions and actual
measured results, and this will then allow improvements in radiation

38 / 5. APPROACH TO DOSE ASSESSMENT FOR ASTRONAUTS
environment characterizations and dose estimates. In this respect,
the correction to the interior fields associated with the less known
trapped radiations will be a prime target of such procedures.
5.1 Exterior Exposure Field
5.1.1 Radiation Environment Models
In practice, the external radiation environment in LEO is repre-
sented by various predictive models and descriptive fits. Best known
are GCRs (Badhwar and O’Neill, 1992; Davis et al., 2001) and their
associated quiet-time geomagnetic transmission factors. Periods of
geomagnetic storms provide only small corrections to the long-term
averaged fields in LEO. The albedo neutrons produced by the impact
of GCR with Earth’s atmosphere are also well known (Korff et al.,
1979; Lockwood, 1972; Preszler et al., 1972). GCR models are well
developed and the predictive model of Badhwar and O’Neill (1992)
gives a reasonable representation of the local radiation environment
outside Earth’s geomagnetic field. More recent descriptive fits associ-
ated with the Advanced Composition Explorer spacecraft project are
now available and have the advantage of validation by measure-
ments with high-quality instrumentation in the L1 libration point
(i.e., about 1.5 million kilometers from Earth in the sun’s direction)
where Earth and solar gravitational strengths balance each other
(Davis et al., 2001).
The current trapped radiation models are uncertain by a factor of
two for geomagnetic quiet times and the trapped radiation experi-
ences large fluctuations during geomagnetic storms for which there
are no predictive models. In addition to the uncertainty in intensity,
the trapped radiations are highly directional and their velocity vec-
tors are constrained to lie within several degrees of a plane normal
to the local geomagnetic field line. The AP-8 (Aerospace Proton Envi-
ronment, Version 8) model for protons and AE-8 (Aerospace Electron
Environment, Version 8) model for electrons (Vette, 1991) represent-
ing the trapped radiation environment are the basic standard, based
on data obtained by NASA and Air Force measurements from 1958
to 1970. The AP-8 model includes angular dependence and both
AP-8 and AE-8 provide the omnidirectional fluence estimates for
geomagnetic quiet conditions in current usage.
SPEs occur mainly during times of elevated solar activity and
are unpredictable in magnitude and exact time of occurrence. Their
detection must rely on satellite measurements available in real-time

5.2 INTERIOR EXPOSURE FIELD / 39
from some space platforms. Transmission through the geomagnetic
field to LEO is normally represented by the vertical cutoff model
derived transmission factors for 20 km height (Shea et al., 1988) and
scaled in altitude according to a magnetic dipole approximation.
Recent tables of global vertical cutoff transmission factors have not
been published.
5.1.2 Spacecraft External Measurements
External measurements can be made of the outside radiation envi-
ronment to allow correction to the models to reduce the uncertainties.
An ion chamber with well-defined wall thickness can serve to monitor
the short-term variations in the electron environment for EVA opera-
tions and particle spectrometers provide useful data to reduce the
uncertainty in the trapped particle fields and during SPEs. Recom-
mended instrumentation is discussed in Section 6. The principal
external measurements are: &i(E,�,t), the external fluence for parti-
cles of type i at time t with energy E moving in direction �; and I,
the ionization current in a tissue-equivalent ion chamber.
5.2 Interior Exposure Field
5.2.1 Shielding Models for the Space Shuttle, International
Space Station, and Space Suits
Shielding models are required for the Space Shuttle, ISS, and
space suits to allow evaluation of the interior radiation environment
to which the astronaut is exposed. The models consist of the distribu-
tion of materials about each field point within the vehicle and appro-
priate computational procedures to evaluate the interior field of
transmitted particles. The internal radiation environment generally
shows high directionality with large spatial gradients and varies
over time with both short- and long-term temporal scales. The distri-
bution of materials within the three structures (Space Shuttle, ISS
and space suit) is represented with computer generated solid geome-
try models. The Space Shuttle model (Atwell et al., 1989) is assumed
to be made totally of aluminum alloy 2219. Higher fidelity ISS and
space suit models allowing a distribution of materials are desirable.
With the exception of the absolute intensity of the trapped radia-
tion environment and possible SPEs, the interior radiation environ-
ment can be evaluated with high-speed computational models as

40 / 5. APPROACH TO DOSE ASSESSMENT FOR ASTRONAUTS
has been demonstrated for Space Shuttle flight measurements
(Badhwar et al., 1995a; Shinn et al., 1998). High-speed computational
procedures allow rapid mapping of the interiors of the Space Shuttle
and ISS. The computational procedures are outlined in Appendix B.
Fast computational procedures for charged ions and neutrons are
well developed (Clowdsley et al., 2000; Cucinotta et al., 1997; Wilson
et al., 1995). Fast computational procedures of electron and photon
transport are available for limited shielding materials (Seltzer, 1980)
and more general codes are still being developed. This series of
electron and photon transport codes requires the approximation of
shielding (including tissue) to be taken as equivalent amounts of
aluminum and only provides dose, with no information on electron
and photon spectra.
5.2.2 Spacecraft Internal Measurements
Selectively located active and passive instrumentation allows fur-
ther adjustments to the evaluated internal radiation environment,
thus reducing uncertainty. Particle spectrometers allow some evalu-
ation of transmission factors and dosimetric devices allow evaluation
of calculated dosimetric quantities. Both active and passive dosimet-
ric devices are useful for evaluation of D, D(L), the frequency distri-
bution of lineal energy [ f (y)], and H, as discussed in Appendix A.
Personal dosimeters worn by astronauts can determine some or all
of these quantities in adjacent tissues.
The interior radiation environments of the Space Shuttle and ISS
will be monitored by various instruments, and the measurements
can be used to adjust the modeled trapped particle intensity, thereby
reducing the uncertainty in estimates of the interior radiation envi-
ronment. There are long-term variations depending on solar activity,
which modify the environmental spectra as well as intensity, so
that spectrum-sensitive instrumentation is desirable. Furthermore,
active instrumentation is desirable to allow detection of time-
resolved trapped and GCR components. Whatever instrumentation
is used within the Space Shuttle or ISS, the instrument response
needs to be accurately defined for direct comparison of measurement
with predicted response as the basis for modifying the calculated
results to reduce uncertainty in estimates of the interior radiation
environment. The principal internal measurements are: &i(E,�,t)

5.3 TISSUE EXPOSURE FIELDS / 41
(the internal fluence for particles of type i at time t with energy E
moving in direction �), D, D(L), f(y), and H.
5.3 Tissue Exposure Fields
5.3.1 Human Shielding Models
Shielding models for astronaut tissues are required to evaluate
the fields present at specific sensitive tissues. The models consist of
the distribution of the specific sensitive organs in the body and the
surrounding distribution of the astronaut tissues about each point
in that organ and computational models to evaluate the transmitted
fields. The presence of high directionality and large spatial gradients
coupled to the mobility of the astronaut poses a challenge to evalua-
tion of the exposure fields at specific tissue points. In addition, astro-
naut shielding models allow the evaluation of the effect of the
presence of the astronauts in the radiation environment on the local
interior field and in particular on the exposure of the personal dosim-
eter, and on the relationships between D and H at points on the
surface of the body and these quantities in deeper-lying organs. The
evaluation of organ or tissue dose for the astronauts is performed
with computerized anatomical models for both a male and a female
(Atwell et al., 1993). The models provide the distribution of tissues
with relatively high fidelity. A male data set derived from computed
tomography scans has also been developed but is not fully utilized
in protection practice (Qualls and Boykin, 1997).
5.3.2 Occupancy Factors
Occupancy factors keyed to known individual activity can be used
to estimate an astronaut’s exposures and can be corrected by the
personal dosimeter measurements. This is especially true during
EVA where large fluctuations in the trapped electron environment
or SPEs could greatly alter the dose gradients within the astronaut
tissues. In addition, one could have a combination of shielded and
unshielded TLDs in a personal dosimeter such that the shielded
dosimeters did not record trapped electrons during EVA.
6. Data Collection andInterpretation forDose Assessment
6.1 Introduction
Data collection and interpretation are essential components of
an operational radiation safety program for space activities. Mea-
surements from onboard detectors in combination with radiation
transport calculations should be designed to provide sufficient
information to:
● assess career exposures
● assess short-term exposures
● manage the exposures during all mission segments
There are several purposes of in-flight measurements. These
include the provision of field data (fluence, dose) both integral and
differential (with respect to time, LET, energy or direction, as appro-
priate), normalization of the calculations of the radiation field compo-
nents, and, in the case of personal dosimeters, the determination of
D and H. The quantities D and H refer to determinations averaged
over the sensitive volume of the detector as measures of D and H to
a point in the adjacent tissue.
In order to perform these functions, instrumentation must be able
to accommodate the complex nature of the radiation environment
in space and a range of mission profiles. Additional complications
are introduced by the variety of astronaut activities both inside and
outside the spacecraft.
Several types of instrumentation are required. Area monitors,
fixed or portable, will be used to measure fluence and fluence rate,
D and absorbed dose rate (D·), from which H and dose equivalent
rate (H·) may be calculated. Due to the complex nature of the radiation
field it may be necessary to differentiate fluence and D with respect to
particle type and energy, LET, and direction. Active instrumentation
should have a time resolution sufficient to identify temporal varia-
tions in the radiation field. These temporal variations may be associ-
ated with the characteristics of the orbit or other external factors.
42

6.2 DOSE QUANTITIES TO BE DETERMINED / 43
Personal dosimeters can be used to make measurements of D or H
to tissue at a point on the surface of the body and assign these
directly to individuals. In addition, alarm or warning instruments
can be used to support in-flight implementation of dose management
and ALARA actions.
6.2 Dose Quantities to be Determined
The objective of the adopted dose assessment approach (Section 5)
is to determine the necessary radiation protection quantities for the
limitation of stochastic and deterministic effects. For stochastic
effects this quantity is E determined from E � �T
wT HT, where HT
is used as the surrogate for HT (Section 2.2.2). For deterministic
effects the quantity is GT determined from GT � Ri DT, where DT is
weighted by Ri for the particle type (Section 2.2.1). Passive personal
dosimeters can be used to determine D and H to a point in adjacent
tissues. The quantities DT and HT to organs and tissues, and thus
E and GT are determined from a combination of radiation transport
computations and dosimetry measurements (Section 5).
Thus, an appropriate measurement package should provide:
● input data for the radiation transport calculations. The combina-
tion of calculations and measurements will yield estimates of E
and GT ;
● measurement of desired point quantities such as D, the spectrum
D(L), and H to adjacent tissues; and
● measurements in support of in-flight dose management and
ALARA actions.
Calculations serve a dual purpose. Firstly, they are essential to
mission planning in that they provide preflight estimates of the doses
that would be received by the astronauts during the different phases
of the proposed mission. Secondly, they are an essential component
of the dose assessment process for determining the actual doses
received by the astronauts during the mission. In the latter role,
the calculations are combined with measurements from area and
personal dosimeters in order to arrive at the final values of HT, E
and GT.
As described in Section 5 (Figure 5.1), data from the area monitors,
both internal and external to the spacecraft, are used to determine
essential field quantities as input to the calculations in order to define
the internal radiation environment at different locations inside the
space vehicle. Data from the measurement package [i.e., D, D(L),

44 / 6. DATA COLLECTION AND INTERPRETATION
and H] are then used along with the calculations to provide estimates
of HT, E, and GT. As already described, this can be achieved by using
the measured D, D(L), and H to normalize the computations before
proceeding to compute values for each astronaut. Alternatively, the
computations may provide correction factors for each astronaut to
convert H values determined from personal dosimeters into HT, E
and GT values. In either approach, it is a combination of radiation
transport computations and dosimetry measurements that is used
to provide the ultimate values for entering into the record.
The measurement packages described in this Section have suffi-
cient flexibility to support either approach. The proposed packages
consist of:
● active devices, including TEPCs and particle spectrometers in
strategic locations within the spacecraft, to collect data for short-
term and career records;
● passive devices, including TLDs and PNTDs as personal dosime-
ters for the crew; and
● active devices to act as alerts for high transient doses and dose
rates.
In this Section potential alternative, or additional, dosimetry
devices that may be employed in the future are discussed, including
solid-state active personal dosimeters, solid-state ionization cham-
bers, and high-intensity electron field monitors.
6.3 Proposed Measurement Package
6.3.1 General Discussion
The measurement package proposed by NCRP follows naturally from
the determination of the observables to be measured (Section 6.2)
and the capabilities of available and planned instrumentation. No
single device can determine the required dose quantities for all com-
ponents of the radiation field. Since there are large variations in the
magnitudes of the contributions to total D and H from the different
particle types it is not generally possible to determine D or H from
just one component (or components) and apply a correction factor to
determine D or H for the whole field. Therefore, practical measure-
ment and dose assessment considerations suggest the need to evalu-
ate three main components of energy deposition, namely: (1) low-
LET charged particles and photons; (2) neutrons, and protons that
undergo nuclear interactions which produce high-LET secondary

6.3 PROPOSED MEASUREMENT PACKAGE / 45
particles; and (3) energetic charged nuclear fragments with Z � 1
(HZE particles).
The rationale for the recommended measurement package is to
ensure that suitable measurements are made in each of the above
three categories, that will allow determination of the dose-limit
quantities, without unnecessary overlap or duplication that might
result in ‘‘double counting.’’ The choice of measurement device or
devices is dictated by radiation response characteristics (particle
type, particle energy, quantity to be determined), operational charac-
teristics (direct determination of dose quantities, input to model
calculations, desired accuracy, dose management, and ALARA sup-
port), as well as practical issues such as reliability, robustness and
availability.
An additional important consideration is the time required for
analysis of the devices compared with the duration of the mission.
Long duration ISS missions may place constraints upon the fre-
quency of analysis of passive dosimeters. If the personal measure-
ment package on ISS does not include active dosimeters, facilities
to read passive devices onboard the spacecraft may be necessary to
fully implement dose management and ALARA. Such facilities may
not be necessary on the Space Shuttle. Furthermore, the proposed
passive personal dosimeter package is to be used both when the
astronaut is inside the spacecraft and during EVA. However, supple-
mental passive personal dosimeters may be needed for additional
locations on the astronaut during EVA because of spatial variations
in the degree of shielding provided by the space suit.
The addition of TEPC (Section 6.3.2.1) to routine area dosimetric
evaluation in the mid-1990s provided direct information on energy
deposition in tissue by both high- and low-LET particles. The data
provided are in terms of D in a small mass of tissue collected in real-
time, and can be used to determine D·. Energy deposition events can
be combined to give distributions in lineal energy (y) that are related
to LET of the incident radiation. It may also be possible to use this
information to estimate unrestricted LET (L�) distributions, which
are required for determination of Q and thus H to a small mass
of tissue. Radiation transport models have been used to predict y
distributions measured by TEPCs (Badhwar et al., 1996c; Shinn
et al., 1999). From these calculations estimates of the radiation envi-
ronment within the space vehicle have been made. The success of
this approach relies upon an accurate estimate of the external radia-
tion field, the geometry and composition of the spacecraft, and the
response of TEPC detectors to HZE particles. In general, TEPCs
have little dependence of response on angle of incidence, that is,
their response is approximately isotropic.

46 / 6. DATA COLLECTION AND INTERPRETATION
Particle spectrometers (Section 6.3.2.2) can identify particles individ-ually by charge and energy. This is necessary information when consid-ering radiation effects that are sensitive to particle type and fluence,as opposed to D and LET. It is also possible to make comparisonsbetween the data and calculations. Particle spectrometers generallyhave limited angular acceptance and energy, and poor statistics forZ � 2. Details of properties and performance of both TEPCs and parti-cle spectrometers can be found in Appendices B and C.
Thermoluminescent dosimeters (of type TLD-100� or TLD-700�)have been used routinely for both passive personal dosimeters andpassive area dosimeters since the Skylab mission. In addition toTLD, high-LET passive dosimeters have been flown on almost allmissions. TLDs record the energy deposited for photons, electrons,positrons, pions, protons and heavier charged particles. The responseis dependent upon particle type and energy. For example, whencalibrated in terms of tissue kerma to high-energy photons, TLD-100� and TLD-700� overestimate D in tissue (by several percent)for high-energy protons and begin to underestimate D in tissue forparticles with LET (in water) above approximately 10 keV �m�1.The underestimation has been shown to be approximately 50 percentat 100 keV �m�1. However, the exact values of the over- and under-response for a given LET and particle type are not well established.The values vary from material to material and, for a given TLDmaterial, values vary in the published literature. Furthermore, TLDsprovide a single number related to D and provide limited spectro-scopic information on the quality of the radiation field, i.e., D(L).Because of these properties, TLDs alone do not provide sufficientinformation to determine H. Furthermore, the design of the TLDpackage may introduce an unwanted dependence of response onangle of incidence. Details of TLD properties and performance canbe found in Appendix C.
PNTDs have been a standard component in crew and area dosime-try packages. These detectors respond to high-LET particles, includ-ing secondary charged particles from neutron interactions, but areinsensitive to photons, electrons and other charged particles withLET (in water) values less than approximately 10 keV �m�1, depend-ing upon PNTD material. Processing of PNTD can yield LET distri-butions for the radiation field, as well as particle type and energy.PNTDs have a strong dependence of response on angle of incidence.Details of the properties and performance of PNTDs can be foundin Appendix D.
6.3.2 Proposed Measurement Package: Active Devices
Active devices record and display data in real-time, or near real-time. For most applications both the readout time and time resolution

6.3 PROPOSED MEASUREMENT PACKAGE / 47
are significantly shorter than the time for Space Shuttle or ISS to
complete one orbit. This makes it possible to obtain measurements of
rates as well as time integrated values. In most cases the time resolu-
tion is sufficient to select data from defined portions of the orbit (e.g.,
when traversing SAA). Most active instruments can be turned on or
off so as to operate in specific circumstances and conditions (EVA,
SPE). Active detectors require electrical power that can be provided
through connections with power supplies in the spacecraft or through
batteries. They can be used as fixed or portable area monitors and
devices are under development that are sufficiently small to be carried
on an astronaut’s person. The types and characteristics of detectors
to be used in LEO should be determined by the requirements of dose
assessment, as specified in Section 5. The following detectors can
provide sufficient data to fulfill those recommendations.
6.3.2.1 Tissue Equivalent Proportional Counters. A TEPC is an
active detector that is designed to measure energy deposition in
volumes of tissue comparable to the dimensions of the nuclei of
mammalian cells. Data are recorded on an event-by-event basis such
that one can obtain a distribution of biologically relevant energy
deposition events. The wall and gas cavity can be designed to make
a TEPC sensitive to incident photons, neutrons and charged particles
from protons to heavy ions.
When the data are integrated over the complete distribution of y,
TEPCs can generate D and D·. The frequency distribution of lineal
energy [ f (y)] depends on characteristics of the radiation field
[&i(E,�,t)] (i.e., the distribution of fluence for particle type i as a
function of energy E, direction �, and time t) and the response of
the detector. Therefore, f(y) can serve as a test for radiation transport
models. It can also be used to obtain D in terms of lineal energy
[D(y)]. This is not a replicate of D(L), but can be used to obtain an
approximation to Q for protons and heavier particles. The detector
has a large dynamic range such that it can identify signals from
charged particles that deposit energy from 0.2 to 800 keV in the
sensitive volume. It is also sensitive to neutrons and this contri-
bution is also included in D(y). Data from a TEPC can be displayed
continuously and also stored for later transmission to the Mission
Control Center.
6.3.2.2 Solid-State Detectors. Solid-state detectors record the
energy deposited by a charged particle. The ratio of the deposited
energy (dE) to the thickness of the detector (dx) yields the approxi-
mate L� for the incident particle. Thus, a single detector can provide
an estimate of &(L,t) [i.e., the distribution of fluence as a function

48 / 6. DATA COLLECTION AND INTERPRETATION
of LET (L) and time (t)] that can be integrated to yield D and D·
for
protons and heavier charged particles. It can be fabricated into a
compact detector for use as a portable area monitor or personal dose
rate meter with on-demand readout (Badhwar, 2000).
Often several of these detectors are combined to form a particle
telescope that measures both energy deposition and position. When
these data are combined, this detector yields a more accurate esti-
mate of L� and thus &(L,�,t) (i.e., the distribution of fluence as a
function of L, � and t). It can also be used to obtain D(L) and Q for
heavy particles, but with the restriction that the incident particles
originate from a fixed direction depending on the orientation of the
detector. Because of size limitations this type of detector is sensitive
over a restricted solid angle (d�).
The energy lost in one or more solid-state detectors can be used
to identify the particle charge (Z) as well as the incident energy (E)
to ultimately obtain &i(E,Z,t) (i.e., the distribution of fluence as a
function of E, Z and t). Several of these detectors can be combined
to point in different directions to provide a more complete description
of the radiation field either outside or inside of the spacecraft.
6.3.2.3 Active Electronic Personal Dosimeters. There are a num-
ber of real-time electronic personal dosimeters available, mostly
using silicon-based detectors (Ortega et al., 2001; Texier et al., 2001).
Most of these have been designed to measure photon and beta radia-
tion, and might be considered for the measurement of the low-LET
component of the fields in spacecraft. Several have tissue-equivalent
encapsulation. However, even if used only to determine the low-
LET component, a full characterization of the charged-particle and
neutron response is necessary before any can be recommended. Neu-
tron and total field electronic personal dosimeters are not as fully
developed as are those designed to determine photon and beta radia-
tion fields. Direct ion storage dosimeters, described in Section 6.3.3.2,
can be operated as real-time devices to determine the low-LET
component.
6.3.2.4 Active Detectors for Electrons. Active detectors should be
specially configured to measure low-LET radiations, in particular,
electrons. This is normally not an issue inside the spacecraft but
could be of concern during EVA, since electrons above a few hundred
kiloelectron volts can penetrate the space suits. Since the trapped
electron intensity can change by many orders of magnitude during
and following a large magnetic storm, due to short-term perturba-
tions of the geomagnetic field, it is recommended that an active
detector sensitive to electrons be installed outside of the spacecraft

6.3 PROPOSED MEASUREMENT PACKAGE / 49
to serve as a monitor for fluctuations in the electron component of
the space radiation environment for dose management during EVAs.
Such a monitor could be a simple ionization chamber with a wall
thickness sufficient to attenuate very low-energy electrons but thin
enough to record electrons that could penetrate a space suit. The
output would be the ionization current (I). Because the trapped elec-
trons occur intermittently, it will be necessary to monitor or suppress
the signal from background radiation that occurs continuously.
6.3.3 Proposed Measurement Package: Passive Devices
Passive devices can be used as both area and personal dosimeters.
Since no single passive device is capable of dose measurement across
the full spectrum of LET, measurement packages should be designed
to have optimum performance in the three different regions noted
above, namely: (1) low-LET charged particles and photons,
(2) neutrons and protons that undergo nuclear interactions, and
(3) HZE particles. Passive dosimeters currently in use on LEO Space
Shuttle flights are TLDs, specifically TLD-100� or TLD-700�, to
obtain D in tissue (in gray) calibrated against 137Cs gamma rays.
That is, the 137Cs gamma-ray dose in tissue (or kerma in tissue)
required to give the same thermoluminescent (TL) response in TLD
as the space irradiation is reported as D in tissue at the location of
the TLD detector. However, TLD-100� and TLD-700� are not the
best TLD materials to use, since they have a variable and decreasing
response at high-LET. Other TLD materials may be better, in that
they may be more suited for use at low-LET (i.e., �10 keV �m�1)
with very little sensitivity to higher-LET particles. Furthermore,
since there may be a need for some passive elements to be read out
frequently onboard, and others that are read only on return to Earth,
the mode of readout of the luminescence dosimeters should be care-
fully considered. OSLDs and electronic dosimeters may be viable
options. However, any new TLD or OSLD material, or new electronic
dosimeters, will need to be fully characterized for the space radiation
environment.
To read the high-LET component of the radiation field PNTDs can
be employed. These are generally insensitive below a LET in water
of approximately 10 keV �m�1 (depending on material) and may be
employed in a mode that provides D, D(L) (or D averaged over certain
ranges of L), and H.
The various elements of the proposed packages are discussed
below.

50 / 6. DATA COLLECTION AND INTERPRETATION
6.3.3.1 Low Linear Energy Transfer Dosimetry: Thermolumines-
cent Dosimeters. As noted, after calculation of the equivalent 137Cs
dose the TLD response needs to be corrected for the variation in the
efficiency of TLD as a function of particle LET and for the neutron
response of the dosimeter. This would require taking into account
the best estimates of the radiation field components at an appropri-
ate spacecraft location. Therefore, it is recommended that passive
dosimetry using TLDs or OSLDs be limited to the determination of
D from the low-LET charged particle and photon component only
(i.e., for L � 10 keV �m�1). This can be achieved by choosing a
device (a luminescence dosimeter, i.e., a TLD or an OSLD) that has
a minimal response to the other high-LET components. Dosimeters
LiF:Mg,Cu,P (for TLD) and Al2O3:C (for OSLD) should be considered
since they are predicted to be very sensitive to low-LET radiation,
and very insensitive to high-LET radiation. This prediction is based
on their gamma-ray dose response, which shows a considerably lower
saturation dose for the former materials compared with, say, TLD-
100�. For 5 MeV alpha particles this prediction has been shown to
be true (Appendix C). Lithium fluoride (LiF) is a tissue-equivalent
material for low-LET radiations and for photons. Al2O3:C is less
tissue equivalent but still acceptable. One advantage of switching
to OSLDs would be the possibility of providing small, lightweight,
low-power OSL readers for the spacecraft so that the astronauts
could read their own dosimeters during long-duration flights. In
either case, these materials may provide excellent discrimination
between low- and high-LET radiation.
As an alternative to OSLDs, one could consider radiophotolumi-
nescence (RPL) glasses (Piesch et al., 1990; 1993). Like OSLDs, these
are optical-readout dosimeters, but they provide a permanent inte-
gration of the dose and cannot be re-used. Readout equipment is
similar to that of OSLDs. However, like OSLDs, RPL glass dosime-
ters have not been tested for their response to particle radiation
over a wide range of LET. Thus, before adoption of OSLDs, or RPL
dosimeters, research is required to fully characterize their response
in detail.
CaF2:Tm dosimeters (such as TLD-300�) can provide useful quali-
tative information about the particle LET spectrum using the peak-
height-ratio method (Appendix C). It has been suggested that the
variation of the peak height ratio with LET for either LiF:Mg,Ti-
based detectors (e.g., TLD-100� or TLD-700�) or CaF2:Tm detectors
(e.g., TLD-300�) could be used to provide information about the
quality of the incident radiation field by calculating a ‘‘TLD average
Q,’’ namely a parameter QTLD (Appendix C). However, the variation
of the peak-height-ratio with LET is nonlinear. Furthermore, it is

6.3 PROPOSED MEASUREMENT PACKAGE / 51
unclear what the obtained value of QTLD means. In general, where
the radiation field has a significant neutron component, QTLD will
differ from Q for tissue because of the lower neutron kerma and
absorbed dose in CaF2:Tm than in tissue. Despite claims by some
authors that the QTLD value matches well the ‘‘true’’ average value
for the low- and high-LET components, comparisons of QTLD with QD
(D averaged Q) calculated from the TEPC data differ by as much as
a factor of two. Thus, we recommend the use of CaF2:Tm only as
additional input into the model calculations and not as a quantitative
method to obtain H for low- plus high-LET components.
6.3.3.2 Direct Ion Storage Dosimeters. In addition to personal
dose rate meters discussed in Section 6.2.2.3 there are new solid-
state detectors that combine an ionization chamber with a semicon-
ductor. Specifically, the direct ion storage dosimeter is based on
coupling a gas-filled ion chamber with a semiconductor nonvolatile
memory cell (Wernli and Kahilainen, 2001). These are compact integ-
rating devices that can be read out periodically and used to estimate
accumulated doses over periods of several hours to at least a year.
6.3.3.3 Neutron and High Atomic Number, High-Energy Particle
Dosimetry: Plastic Nuclear Track Detectors. To determine the neu-
tron and HZE components, a separate device (comprising one etched
track detector, or two or more such detectors of different response
characteristics) should be used (see Appendix D for descriptions of
methods and for references). From such a dosimeter, the point values
for H in adjacent tissues can be determined. Materials that can be
used are PADC/CR-39�, cellulose nitrate, and polycarbonate [Lexan
(General Electric Company Corporation, New York); Makrofol�
(Bayer Aktiengesellschaft Corporation, Leverkasen-Bayerwerk,
Germany)]. Herein we refer to all such materials as PNTDs.
The LET (in water) threshold of PADC/CR-39� is in the range 5
to 10 keV �m�1, enabling protons of energy up to about 10 MeV to
be detected directly, as well as HZE particles. Secondary charged
particles from nuclear interactions of higher energy protons and of
neutrons, in the detector material itself or surrounding material,
are also detected. Full etch track analysis of stacks of PNTDs allows
the determination of HZE particle fluence and fluence rate, but is
very time consuming. By a measurement of the distribution of D
(fluence times LET) as a function of LET, H can be determined for
energy deposition by all particles in the (approximate) LET range
of 5 to 1,000 keV �m�1. This can be done using single detectors, but
is still time consuming. Automated analysis systems have been used
but further development is needed. Another, more approximate

52 / 6. DATA COLLECTION AND INTERPRETATION
approach, is to use a series of different materials each of different
LET threshold to obtain particle fluence in a number of LET ‘‘bins.’’ In
both approaches, although LET calibration of the detector response is
in terms of LET in water, the numbers and types of secondary parti-
cles generated, for example by the neutron and higher energy proton
components, will be different than those generated in tissue. There-
fore, the determination of H (to tissue) will be approximate. PNTDs
may also be used to estimate the higher-LET component of GCR
using the simpler, less time consuming techniques developed for
neutron personal dosimetry. Electrochemically etched pits are iden-
tified and counted. Readout procedures are fully automated. HZE
particles will also produce an etchable track and be counted as if
produced by a neutron, or neutron-like iterations of high-energy
protons, and the same response factor applied (about 10 �Sv per
track for a typical electrochemical etch system), which will over-
estimate the HZE component of H. However, an additional chemical
etch allows discrimination. The response of PNTDs is angle depen-
dent and, in general, the interpretation of results requires assump-
tions with respect to the direction distribution of the field to which
PNTDs were exposed.
6.3.3.4 Use of Thermoluminescent Dosimeters and Plastic Nuclear
Track Detectors to Estimate Effective Dose. Measurements of H
with TLDs and PNTDs located at the surface and HT with TLDs and
PNTDs located in the organs of an anthropomorphic phantom were
made during a Space Shuttle mission to Mir (Yasuda et al., 2000).
The results indicate that the determination of H at the body surface
may be able to provide an assessment of the effective dose (E) for
the radiation field inside ISS. However, this conclusion needs to be
supported by further investigations for other shielding configura-
tions. The potential for developing a set of conversion coefficients
that directly relate H at the surface to E for the space radiation
environment, similar in concept to those used in other occupational
radiation environments (ICRP, 1996; ICRU, 1998), would be worth
investigating.
6.3.3.5 Superheated Drop/Bubble Dosimeters. Superheated drop/
bubble neutron personal dosimeters are available, and have been
flown on Mir and the Space Shuttle (Ing, 2001). These dosimeters
respond to thermal neutrons and fast neutrons upwards from about
100 keV, but require a normalization of the neutron response to the
neutron spectrum in spacecraft and corrections for proton and other
ion-induced bubbles. The use of this type of device must take into
account dynamic range limitations, the temperature dependence of

6.3 PROPOSED MEASUREMENT PACKAGE / 53
response or the efficiency of the correction applied for this effect,
and the possibility of false readings due to microphonics.
6.3.4 Recommendations for Measurement Packages
6.3.4.1 Recommendations for Area Monitoring. Active detectors
play an important role in terms of characterizing the radiation fields
inside and outside of the spacecraft. Detectors with time resolutions
on the order of minutes can be used to distinguish regular changes
in radiation during portions of the orbit (i.e., trapped radiation in
polar regions and SAA, galactic cosmic rays) as well as identify other
intermittent changes due to solar activity and magnetic storms.
A TEPC can provide dose and dose rate measurements with suffi-
cient time resolution. It is sensitive to photons, protons, helium, HZE
particles, and neutrons. It has the additional capability of providing
information on f (y) that can be used to obtain D(y). Although D(y)
is not identical to D(L), dose-averaged values of y have values very
similar to those for L and thus can be used to estimate Q (Appen-
dix A). A TEPC can be placed at fixed locations within the spacecraft
or can be operated as a survey meter if necessary.
Active solid-state detectors can provide a direct measurement of
particle fluence for protons and heavier particles in terms of &(L)
(i.e., the distribution of fluence as a function of L) for a single detector
or &(L,�) (i.e., the distribution of fluence as a function of L and �)
and &(Z,E,�) (i.e., the distribution of fluence as a function of Z, E
and �) using multiple detectors. These data can serve as calibration
points for particle transport codes used for dose assessment. When
integrated, they also provide an estimate of D to silicon that can be
converted to D to tissue. Because they estimate LET, they can also
provide estimates of Q. Active solid-state detectors can be used as
area monitors inside and outside of the spacecraft. A compact porta-
ble version has been developed and could be used as a personal
dosimeter with on-demand readout.
An active detector sensitive to electrons should be installed outside
of the spacecraft to serve as a monitor for fluctuations in the electron
component of the space radiation environment that can change by
many orders of magnitude during and following an SPE due to short-
term perturbations of the geomagnetic field. This could be of serious
concern during an EVA since electrons above a few hundred kiloelec-
tron volts can penetrate the space suits. Such a monitor could be a
simple ionization chamber with a wall thickness sufficient to attenu-
ate very low-energy electrons but thin enough to record electrons
that could penetrate a space suit.

54 / 6. DATA COLLECTION AND INTERPRETATION
The deployment of active instruments can be usefully supple-
mented by passive devices, for example, by PNTD stacks to deter-
mine both HZE particle fluence rates and LET distributions, and by
TLDs or OSLDs to examine the spatial distribution of the low-LET
component.
6.3.4.2 Recommendations for Personal Dosimetry. A measure-
ment package consisting of a TLD material for measurement of the
low-LET component and a PNTD stack to determine the high-LET
component would appear to provide the best current solution for
passive personal dosimetry in the complex radiation field experi-
enced in space. For TLD, LiF:Mg,Cu,P would appear to be an attrac-
tive material. Alternatively, Al2O3:C is the best currently available
OSLD material. To measure H from the high-LET components, the
use of PADC/CR-39� etched track detectors is proposed. Such devices
have been used as a part of the area monitoring or personal dosimeter
packages on the Space Shuttle, but are not currently planned for
ISS. It is recommended that they be used as personal dosimeters on
both vehicles. CaF2:Tm (e.g., TLD-300�) could also be used as an
adjunct personal dosimeter to provide additional information for
model normalization purposes, but not for quantitative determina-
tion of dose quantities.
With this measurement package for passive personal dosimetry,
H at a point in adjacent tissue is then obtained from:
H � DTLD/OSLD � � DPNTD(L) Q(L) dL (6.1)
where DTLD/OSLD is absorded dose recorded by TLD or OSLD in the
low-LET region (L � 10 keV �m�1) for which Q � 1. DPNTD(L) is the
D distribution in LET determined by PNTD over the high-LET range
(L � 10 keV �m�1) and for which Q is dependent upon L. Correction
may be needed for any overlap of the two responses so that intermedi-
ate-LET components are not double-counted.
It is recognized that this recommendation requires verification of
LET dependence of the TLD response of LiF:Mg,Cu,P and of the
OSLD response of Al2O3:C. Until such time as these data are avail-
able, therefore, LiF:Mg,Ti dosimeters (e.g., TLD-100� or TLD-700�)
may still be used. If so, however, this should still be along with
PNTDs, as part of the passive personal dosimetry package, in order
to provide LET data suitable for correcting the TLD dose response
for the L � 10 keV �m�1 component, and for estimating H for this
component from the PNTD results.
If PNTDs cannot be flown, a different approach has to be adopted.
Data needs to be obtained from a TEPC or particle spectrometer
used as a passive area dosimeter. If appropriate LET information

6.4 ACCURACY, PERFORMANCE TESTING, AND CALIBRATION / 55
is available from the area dosimeter, then correction of the TLD
response may be made by extracting (i.e., from TEPC data) a dose-
averaged LET (LD), from which one can evaluate a mean Q (Q) from
the known Q(L) relationship, and an effective efficiency (�) from a
measured �(L) relationship (Appendix C).
The value of H to the adjacent tissue is then approximated by:
H �Q D
�, (6.2)
where D is the dose of 137Cs or 60Co that is found to give the same
TL response from TLD as the space irradiation. This approach suffers
from the drawback that DTLD for the neutron component of the fields
will, in general, be significantly less than D in tissue for this compo-
nent. The Q derived from TEPC measurements should be applied
to D from all components to obtain the total H. The degree of approxi-
mation resulting from the adoption of the approach described will
depend on the proportions of the different field components and
therefore location in the spacecraft. Some new designs of passive
electronic dosimeters function as small tissue equivalent ionization
chambers. For these devices, an appropriate Q derived from a TEPC
may be applied to determine H at a point in adjacent tissue.
Most currently available active electronic personal dosimeters are
used routinely to measure low-LET radiation and have not been
characterized for the types and energies of the particles comprising
the fields in spacecraft. Such dosimeters, when well characterized
may perform a useful role. The ideal dosimeter would be active, store
integrated dose data and dose rate time profiles, and respond to
all field components, allowing a good determination of D·
and H·
to
adjacent tissues.
If active personal dosimeters are not used, then it may be necessary
to develop onboard readout capabilities for the passive dosimeters,
especially on long-duration ISS missions. Although onboard readout
of PNTDs is not feasible, onboard systems for readout of TLDs,
OSLDs and electronic dosimeters are certainly possible. Develop-
ment in this area is therefore recommended.
6.4 Accuracy, Performance Testing, and Calibration
6.4.1 Operational Radiation Protection Requirements on
Accuracy of Dose Measurements
6.4.1.1 Recommendations of ICRP and ICRU. International and
national requirements, where they exist, are derived, in general,

56 / 6. DATA COLLECTION AND INTERPRETATION
from ICRP and ICRU recommendations. ICRP (1997) states, ‘‘In
practice, it is usually possible to achieve an accuracy of about 10
percent at the 95 percent confidence level for measurements of radia-
tion fields in good laboratory conditions. In the workplace, where
the energy spectrum and orientation of the radiation field are gener-
ally not well known, the uncertainties in a measurement made with
an individual dosimeter will be significantly greater. Nonuniformity
and uncertain orientation of the radiation field will introduce errors
in the use of standard models. The overall uncertainty at the 95
percent confidence level in the estimation of effective dose around
the relevant dose limit may well be a factor of 1.5 in either direction
for photons and may be substantially greater for neutrons of uncer-
tain energy, and for electrons. Greater uncertainties are also inevita-
ble at low levels of effective dose for all qualities of radiation.’’ ICRU
(1992) recommends, ‘‘in most cases, an overall uncertainty of one
standard deviation of 30 percent should be acceptable’’ (instrumental
error only).
6.4.1.2 General Requirements. The radiation exposure of astro-
nauts is to complex, multi-component fields that are difficult to deter-
mine routinely. Nevertheless, one of the objectives of the
measurement program should be to meet the general requirement
for the total measurement uncertainty of the quantity being deter-
mined of a factor of 1.5 at the 95 percent confidence level. The total
uncertainty in a subsequent estimate of the effective dose will be
greater.
6.4.2 Tests of Instrument and Dosimeter Performance
There are two accreditation programs for routine personal dose
measurements of external radiation, namely those of NVLAP
(National Voluntary Laboratory Accreditation Program) (White
et al., 2001) that uses the American National Standards Institute
standard (ANSI, 1993) and DOELAP (U.S. Department of Energy
Laboratory Accreditation Program) (DOE, 1986). The requirements
of these programs are broadly related to the recommendations of
ICRP and ICRU. For both accreditation programs there is a limit
on the normal incidence response characteristics determined under
laboratory conditions as the sum of bias (B) and standard deviation
(S). For DOELAP the criterion is: B � S � � � 0.30, where � is
the uncertainty of the conventionally true value of the quantity being
estimated. The DOELAP test criterion is interpreted as providing
approximately 70 percent confidence that a dosimeter reading would
be within 30 percent of the conventionally true value.

6.4 ACCURACY, PERFORMANCE TESTING, AND CALIBRATION / 57
Instruments and dosimeters used to assess doses to astronauts
should meet the DOELAP or NVLAP requirements for determina-
tions of the dependence of instrument response on energy and angle
of incidence combined, plus one standard deviation, for appropriate
calibration/test radiation fields. This requirement should enable the
overall accuracy requirement of a factor of 1.5 to be met for actual
conditions of use in fields of mixed particle types with broad energy
and direction distributions.
6.4.3 Calibration
Calibration is the set of operations that establishes, under specified
conditions, the relationship between values indicated by a measure-
ment, and the corresponding known values of the quantity to be
measured (ISO, 1993). The calibration factor (N) is the factor by
which the instrument- or dosimeter-corrected reading (M) is multi-
plied to obtain the value of the quantity to be measured, determined
under reference conditions. In the case of particle fluence (&) the
calibration factor is given by N � &/M. The inverse of the calibration
factor is the response (R � M/&). The response can be determined
at other than reference conditions when R � 1/kN, where k is the
field specific correction factor. The most complete calibration proce-
dure is as part of a full type test, in which a device is exposed to a
range of radiation energies and angles of incidence in a full determi-
nation of its response characteristics, as well as to other parameters
which may influence its reading (e.g., temperature, humidity). A full
type test is extensive and time-consuming, and is therefore generally
performed on only a few samples of a particular instrument or type
of dosimeter to determine its overall properties.
For a laboratory calibration to be meaningful, it is necessary to
clearly specify the relevant calibration conditions, including the char-
acteristics of the reference radiation source, the irradiation facility,
and the conversion coefficients used. Periodic, accurate calibrations
are an essential part of any quality assurance program, as are mean-
ingful intercomparisons. General guidance on calibration procedures
is given in NCRP Report No. 112 and Report No. 127 (NCRP, 1991;
1998).
The response characteristics (ISO, 1993) of all the types of devices
should be determined prior to use. In particular, the dependence of
response on energy, angle, fluence/dose, and fluence/dose rate should
be determined for the particle types to be measured. In addition,
any interfering (influence) effects, such as those from other radiation
types, temperature, vibration or electromagnetic fields, should be

58 / 6. DATA COLLECTION AND INTERPRETATION
determined. This will normally be accomplished by a combination
of experiment and calculation. The response determinations should
normally be in terms of the quantity fluence. An exception would be
for the determination of photon response, for which air or tissue
kerma will be more appropriate. For the determination of the
response characteristics of personal dosimeters, some irradiations
should be performed on either an anthropomorphic phantom or a
surrogate. Sufficient data should be available to estimate depen-
dence of response on angle of incidence. Where needed and where
available, recommended fluence to D and fluence to H conversion
coefficients should be used.
The statistical uncertainty of laboratory calibrations is commonly
far less than the above uncertainties. However, the D and H response
of devices is frequently appreciably energy- and angle-dependent.
In order to assess whether the above requirements on total uncer-
tainty can be achieved in practical measurements, either determina-
tion of the response is required for the radiation field in which it is
to be used, or in a simulation of this field, or it should be possible
to calculate the response in this field from the knowledge of the field
and of the detailed energy- and angle-dependence of response of
the device.
Response data for the types of devices to be used should be deter-
mined for the following energy ranges as appropriate: protons from
10 to 800 MeV; HZE ions (e.g., helium, carbon, silicon, iron) from
50 MeV n�1 to 1 GeV n�1; electrons from 0.5 to 10 MeV; and neutrons
from 1 to 180 MeV, monoenergetic or quasi-monoenergetic, plus
response data for fields which replicate the neutron field produced
by the interactions of GCR with shielding material.
7. Role of Biodosimetry inDose Assessment
Biodosimetry is the use of a biological marker for assessing the
magnitude of an exposure to radiations or chemicals. The unique
contribution of a biodosimetry program is that it provides an individ-
ual’s dose assessment as estimated from a biological endpoint. Thus,
it includes the response to the cumulative exposure and allows for
an assessment of variations in individual sensitivity.
A number of different biological markers have been utilized for
assessing ionizing radiation exposures with the most frequent being
genetic alterations, such as chromosomal aberrations and gene
mutations, and electron spin resonance in teeth and fingernails, for
example. These methods have been employed for dose estimation
for a wide range of accidental exposures and in occupational settings,
generally with a good level of success. However, there are challenges
associated with biological dosimetry for astronauts that were not
addressed in these previous studies, specifically calibration for the
unique radiation qualities and dose distributions encountered in
space.
The choice of method depends upon the specific exposure scenarios
being estimated, namely, duration of exposure and whether it is
fractionated, together with time of sampling in relation to exposure,
number of individuals involved and speed with which results can be
obtained. In the following discussion particular attention is given to
the aspect of how readily exposure assessment could be made while
the astronauts are still in space. Several methods are discussed in
the following sections.
7.1 Electron Spin Resonance
The use of electron spin resonance with teeth or fingernails is
problematic given that there is little information on its application
with high-LET radiations and nonuniform exposures. Furthermore,
the equipment necessary for the analysis would not be available
until the return to Earth. Thus, its use would be restricted to longer-
term evaluation.
59

60 / 7. ROLE OF BIODOSIMETRY IN DOSE ASSESSMENT
Recent intercomparisons on coded samples of artificially irradiated
whole teeth indicate that with certain methodologies doses of about
100 mGy can be accurately measured (Egersdorfer et al., 1996).
However, for the same studies, a high degree of variability in accu-
racy between laboratories and for different methods was observed.
7.2 Biochemical Indicators
As noted by Muller and Streffer (1991), the use of changes in the
chemical composition of body fluids (saliva, blood, urine) for the
estimation of radiation dose is an attractive idea. Following radiation
exposure, there is a release of enzymes or degradation of proteins
and nucleic acids, leading to shifts in the concentration of a number
of substances, e.g., amylase, taurine, thymidine, deoxycytidine (Kaul
et al., 1986). The apparent attractiveness of this approach is out-
weighed by the fact that there is a high variability, within and
between individuals, of the concentration of the molecule being stud-
ied. None of the biochemical indicators that have been described
have been (or can be) used as a quantitative dosimeter. Thus, no
lower level of detection can be established for these markers.
7.3 Erythrocytes with Transferrin Receptors
A recently described approach (Gong et al., 1999) utilizes the pro-
longed life span of erythrocytes bearing transferrin receptors on their
membrane as a proposed dosimeter. The authors describe a logarith-
mic-quadratic dose response over a 1 mGy to 1.5 Gy x-ray range. At
this time the approach has only been tested in rats, and only with
x rays. A number of assay parameters and the range of interindividual
variation need to be more clearly delineated. In addition, the assay,
as described in rats, is conducted some six weeks after exposure to
allow for the prolonged life-span phenotype to develop. This assay
cannot be recommended for use on astronauts exposed to high-LET
radiations in space. This method has not been applied to humans
thus no lower limit of detection has been established.
7.4 Gene Mutation Assays
The gene mutation assay that would appear to have the greatest
potential for the assessment of exposures to ionizing radiations
7.5 CYTOGENETIC ALTERATIONS / 61
would be that of glycophorin A mutations (Bigbee et al., 1997). The
method is rapid, relatively easy to conduct, and relatively sensitive.
The drawbacks are that there is very little experience with the use
of the assay for high-LET exposures. In addition, the nonuniform
nature of the exposure would be detrimental to the use of the assay
as a whole-body dosimeter.
While the assessment of low level of detection for the glycophorin A
assay has been studied in a limited way, the study of Tucker et al.
(1997) for radiation workers at the Sellafield Nuclear Facility indi-
cated that no increase in variant frequency was observed up to
an effective dose of 1.1 Sv, with the majority of individuals having
�500 mSv, the lower detection level. In contrast, the frequency of
stable chromosomal translocations assessed by fluorescence in situ
hybridization (FISH) increased with dose over this range for the
same individuals. An additional note is that these exposures were
chronic.
7.5 Cytogenetic Alterations
7.5.1 Micronuclei
Micronuclei result from loss of whole chromosomes or acentric
chromosome fragments from daughter nuclei following cell division.
They appear as small, membrane-bounded inclusions in the cyto-
plasm. Their assessment is relatively easy and rapid. The frequency
of micronuclei has been used for estimating exposures for a number
of radiation accidents with reasonable agreement with physical esti-
mates. The drawbacks are that few studies have been conducted
with high-LET exposures, and the assay is not reliable for partial
body exposures. In addition, the sensitivity is marginal at low expo-
sure levels. Thus, the micronucleus assay would not be suitable as
a biodosimeter in astronauts exposed to space radiations.
The incorporation of the cytochalasin B technique, whereby cells
in their second post-exposure cycle can be specifically analyzed for
micronuclei, has greatly increased the sensitivity of the assay. If
individual pre-exposure levels of micronucleus frequency are avail-
able, an absorbed dose of 50 mGy can be detected; without knowledge
of this background frequency the level of detection is estimated to
be 100 mGy (Prosser et al., 1988).

62 / 7. ROLE OF BIODOSIMETRY IN DOSE ASSESSMENT
7.5.2 Acentric Fragments in Prematurely Condensed
Chromosomes
Interphase chromosomes can be prematurely condensed to be
observable microscopically either by fusion with mitotic cells by
treatment with a phosphatase inhibitor (okadaic acid) and a protein
kinase (p34cdc2/cyclinB) (Prasanna et al., 2000), or using calyculin A
(Kawata et al., 2000). Structural and numerical chromosomal alter-
ations can be observed as an increase (or decrease) in centric chromo-
some number or from the presence of acentric fragments. The method
has been used in a laboratory setting to assess exposure to x and
gamma rays (Kawata et al., 2000; Prasanna et al., 2000) and several
high-LET radiations (Kawata et al., 2000). The advantages are that
nondividing cells can be used for assay and the analysis is quite
straightforward. The current drawback is that the assay has had no
application as a true biodosimeter, and issues such as responsiveness
to partial body exposures or chronic exposures have not been
addressed. Further investigation appears warranted for assessing
the value of prematurely condensed chromosomes (PCC) as a biodosi-
meter in the space radiation environment.
The fact that this PCC method has not been used in biodosimetry
means that a lower detection level has not been established. A rea-
sonable assumption is that it will be no more sensitive than other
cytogenetic methods, given similar cell numbers analyzed. The
advantage is that by analyzing interphase cells a larger number of
cells are available for analysis.
7.5.3 Chromosomal Aberrations
The method that has been used the most extensively for radiation
biodosimetry is that of the analysis of structural chromosome alter-
ations. The most recent incorporation of FISH techniques has
allowed for the assessment of symmetrical (transmissible) transloca-
tions. This allows for fairly reliable dose estimation at long times
after exposure. Chromosome aberration dosimetry has been success-
fully applied to radiation accident victims, atomic-bomb survivors,
and a wide range of occupationally and medically exposed persons.
These scenarios include chronic exposures and partial body expo-
sures for which specific methods have been developed to aid in expo-
sure estimation. The distribution of aberrations among cells is useful
in this regard. Even with this strong record of success, the application
of the method for dosimetry in astronauts in space has significant
drawbacks as evidenced by published studies (reviewed in Testard

7.7 CURRENT NASA (JSC) METHODS / 63
and Sabatier, 1999). The major problems are interindividual varia-
tions in response and the nature of the exposures by which only a
small number of cells will actually be hit. This latter concern is
accentuated when the consequence of a hit by a high-energy particle
is taken into account; such a cell might well be so damaged that it
will not contribute to the analyzed cell population.
Additional laboratory investigation is required in order to consider
using cytogenetic analysis as a reliable dosimeter for space flights.
The problem will remain that analysis is technically demanding and
time consuming.
The lower level of dose detection using chromosomal aberrations
is dependent upon the number of cells analyzed. This point is
addressed by Bauchinger (1995) who estimates that for 5,000 cells
analyzed (using a generalized background frequency for dicentrics)
a significant increase in dicentrics should be observed at about
100 mGy for a group of individuals. Twenty thousand cells would
need to be analyzed to detect 50 mGy. Knowledge of the pre-exposure
dicentric frequency can lower this detection level without increasing
the number of cells analyzed.
The study by Tucker et al. (1997) reports a lower detection level of
about 500 mSv effective dose for occupationally exposed individuals
using FISH analysis of stable aberrations. The exposure was chronic
in this case; a situation for which this type of translocation anal-
ysis is particularly applicable. Again, the sensitivity of the assay
would be increased by having available the pre-exposure aberrations
frequency.
7.6 Summary for Methods
Based upon the specific requirements for a biological dosimeter
for assessing radiation exposure to astronauts in space, namely high-
LET exposures, highly nonuniform exposure, ease of analysis, and
rapidity of obtaining reliable dose estimates, it is proposed that a
version of the premature chromosome condensation method or FISH
analysis of metaphase cells are the most likely to be viable. Addi-
tional laboratory research is needed for both to validate their utility
for the stated purpose.
7.7 Current NASA (Lyndon B. Johnson Space Center)
Methods
Until fairly recently, JSC used the conventional cytogenetic
method for biodosimetry for astronauts. The approach, still used

64 / 7. ROLE OF BIODOSIMETRY IN DOSE ASSESSMENT
by many surveillance laboratories, is to assess the frequencies of
chromosomal dicentrics in Giemsa-stained metaphase preparations
and estimate dose using standard dose-response curves developed
from in vitro exposures of human lymphocytes. Most of the published
literature on estimated doses for astronauts was obtained utilizing
this method. Recently, JSC has begun to use the assessment of
chromosomal translocations in metaphase by FISH for estimating
radiation exposures to astronauts from extended periods in space
(Yang et al., 1997). The FISH method used involves chromosome
painting with probes for pairwise combinations of chromosomes 1,
2 and 4 or simultaneous use of all three probes. The use of all three
probes allows for assessment of about 24 percent of the genome. As
with the conventional method, dose estimation is achieved by utiliz-
ing standard translocation calibration curves from in vitro exposure
of human lymphocytes. The difficulty of this method is how to handle
mixed radiation exposures. The current approach is to use the x- or
gamma-ray combined calibration curve (or gamma-ray curve) that
uses preflight blood samples from all astronauts on a particular
mission taken three months or less prior to flight. The postflight
samples are typically obtained within two weeks of return. The blood
samples are grown in culture for 48 h after mitogenic stimulation,
at which time metaphase cell preparations are produced.
The sensitivity of this approach has been tested only to a limited
extent. As an example, the analysis of blood samples from six crew-
members gave in-flight estimates of 0, 90, 180, 210, 210 or 270 mGy
of equivalent gamma-ray absorbed dose to the whole body. In general,
based upon the usual number of cells analyzed (about 4,000) the
sensitivity would allow for the detection of 50 mGy and higher. The
analysis of more cells would clearly increase the sensitivity. It is also
proposed by JSC to use gamma-ray calibration curves obtained for
each individual for use in postflight dose estimation for that particular
individual. This approach takes into account individual variations
in radiation sensitivity, and the fact that background translocation
frequencies vary quite considerably among individuals.
7.8 Recommendations and Future Considerations
Use of the FISH method as described in Section 7.7 is the most
appropriate biodosimetry approach for astronauts based upon avail-
able knowledge, technical availability, and experience. JSC is collect-
ing PCC preparations with the aim of determining if their use might
be advantageous, particularly to alleviate the need for obtaining

7.8 RECOMMENDATIONS AND FUTURE CONSIDERATIONS / 65
metaphase preparations using in vitro culture (see Kawata et al.,
2000 for description of methods).
NASA should continue to use biodosimetry as an ancillary compo-
nent of radiation dose assessment for astronauts during extended
space flights. The current JSC approach of using FISH for analyzing
stable chromosomal translocations in peripheral lymphocytes both
in pre- and postflight samples appears to be providing useful informa-
tion on exposures. The establishment of calibration curves from
individual preflight blood samples increases the sensitivity. Incorpo-
rating analysis of PCC will provide larger analyzable cell samples.
Improvements that can be envisaged are using chromosome painting
probes and computer analysis that allow for assessment of transloca-
tions in all chromosomes at the same time. This method has been
used successfully for tumor analysis. Automating the various FISH
methods will increase throughput enormously.
The area of genomics or molecular profiling is receiving consider-
able attention as an approach for assessing perturbations in gene
or protein expression at the total cell level. Ongoing studies in a
number of laboratories are beginning to describe alterations in gene
expression patterns after radiation exposures over a broad dose
range (e.g., Amundson et al., 2000). Specific gene expression patterns
could be used as biodosimeters once genes have been identified whose
expression remains elevated or decreased for extended periods of
time. An automated analysis of specifically constructed gene arrays
is quite feasible.
The rapid enhancement of technologies for measuring changes
in cellular markers (in response to radiation) will mean that new
biodosimeters will be developed that will be anticipated to detect
very specific exposures, i.e., cellular fingerprints.
8. RecommendedManagement of AstronautRadiation Safety Program
While a team of experts at the Mission Control Center directs
radiation protection actions for astronauts by means of flight rules
(Section 3.1), the overall concept for a radiation protection program
for astronauts is essentially the same as for other radiation workers.
Dose management and ALARA program recommendations estab-
lished for other types of radiation workers can provide NASA man-
agement useful guidance in setting up an effective operational
radiation safety program (NCRP, 1990; 1994; 1998; 1999). Specific
recommendations for the program are provided in this Section.
8.1 Components of a Low-Earth Orbit Operational
Radiation Safety Program
The main components of an operational radiation safety program
designed to implement the principles of dose limitation and ALARA
for astronauts working in LEO are:
● to facilitate actions, both in advance of a mission and in-flight,
that respond to space radiation conditions or mission decisions
that significantly affect the level of radiation exposure to the
astronauts, and radiation protection decisions that significantly
influence conduct of the mission;
● to collect and record data to assess astronaut doses for individual
mission and cumulative career records; and
● to identify, plan and carry out practical ALARA actions to avoid
unnecessary levels of radiation exposure.
NASA management should implement and maintain an effective
radiation safety program with the following features: clear definition
of the goals of the program, statement of the organization’s commit-
ment to the application of the ALARA principle, statement of manage-
ment’s commitment to provide adequate budgetary support for the
program, and periodic review of the overall program effectiveness.
66

8.2 RADIATION PROTECTION PRINCIPLES / 67
The radiation safety program organizational structure and lines of
authority should be clearly delineated and easily understood by all
individuals having radiation safety responsibilities in the program.
In particular, the radiation safety roles and responsibilities of the
flight director, flight surgeon, RHO, and SRAG, for both individual
flights and for the overall program, should be clearly delineated.
This Report provides several recommendations for improvements
in monitoring and controlling radiation dose to astronauts. With an
effective operational radiation safety program, individuals within
NASA will be able to identify the individual or group to whom they
could go to ensure that implementation of a proposed ALARA action
would be considered. Responsibility should be clearly assigned for
ensuring the translation of radiation protection strategies and
instrumentation from design and development through engineering,
preparation for flight, and in-orbit use.
8.2 Radiation Protection Principles Applied to Low-Earth
Orbit Missions
As with all radiation workers, the following principles of radiation
protection apply to astronauts during LEO missions (NCRP, 1993;
2000a):
● any activity that involves radiation exposure must be justified
on the basis that the expected benefits to society exceed the
overall societal cost (justification);
● the total societal detriment from such justifiable activities or
practices is to be maintained ALARA, economic and social factors
being taken into account; and
● individual dose limits are applied to ensure that the principles
of justification and ALARA are not applied in a manner that
would result in individuals or groups of individuals exceeding
levels of acceptable risk (limitation).
Radiation exposure from space flight is justified by the fact that
it is an environmental reality associated with the exploration of
space. The dose limits established for astronauts (NCRP, 2000a)
reflect the importance given space explorations and the limited and
closely monitored population of astronauts. These two principles of
radiation protection (the first and third items above) are already
factored into the overall protection efforts provided for the astronauts
who are subject to multiple high-risk activities.

68 / 8. RECOMMENDED MANAGEMENT OF SAFETY PROGRAM
The sources of exposure that should be included in NCRP dose
limits for astronauts and the actions that constitute an appropriate
approach to immediate dose management and ALARA during LEO
missions are the subject of this Section. In this Report, ‘‘immediate
dose management’’ refers to actions taken to address the potential
for high doses that result from transient events in the space radiation
environment that could impact the conduct or completion of the
mission or mission tasks, and ALARA refers to actions taken to keep
all doses as low as reasonably achievable by balancing the mission
objectives with practical dose reduction steps.
8.3 Sources of Exposure Included in NCRP Dose Limits
for Astronauts
The dose limits for astronauts include the cumulative dose from
space flight, the dose associated with mission-related aviation activi-
ties (excluding commercial flights), the dose from biomedical
research conducted as part of the astronaut’s mission duties, and
any other occupational doses including any received prior to work
as an astronaut. The dose limits do not include normal background
radiation on Earth or radiation dose received from diagnostic and
therapeutic medical procedures conducted as part of the astronaut’s
overall health care.
Astronauts perform significant noncommercial aviation activities
as part of their training for space missions, and the doses from
such activities should be included in the cumulative career dose for
stochastic effects. The doses can be estimated based on total flight
time and average dose rate for the given activity, unless specific
measured data are available.
Dose from mission-related biomedical research prior to, during or
after a given mission should be included in the cumulative career
dose for stochastic effects because the dose is a consequence of partici-
pation in that mission. Radiation doses from diagnostic and therapeu-
tic medical procedures should not be included in the career dose
because they have personal benefit in assessing or improving the
astronaut’s health. In addition, previous medical radiation doses, from
diagnostic or therapeutic medical procedures, are assumed to have
provided the individual a greater benefit than the risk associated
with the doses and should not be used in determining qualification
for future occupational exposure. In some cases, it may be difficult to
distinguish biomedical research from standard medical care for an
astronaut. Determination of which activities are biomedical research

8.4 IMMEDIATE DOSE MANAGEMENT / 69
and which are not is made by the Institutional Review Board govern-
ing astronaut activities.
8.4 Immediate Dose Management and Basic ‘‘As Low As
Reasonably Achievable’’ Concepts
While there are many differences in the way astronauts receive
their radiation exposure from that of a typical radiation worker, the
basic concepts of radiation protection remain the same. Radiation
protection actions based on time and shielding may be utilized in
unique ways to maintain radiation exposure below the administra-
tive levels (Section 3.1) and the dose limits, and these actions also can
be used effectively in maintaining the astronaut’s radiation exposure
ALARA. Specific in-flight radiation protection actions must be based
on real-time information of space radiation environments and on
effective communication of this information to the flight control team.
Good decisions on radiation protection actions require training and
understanding of radiation fields by astronauts, by the entire flight
control team, and by the entire flight management and design team.
As in conventional radiation protection programs, decisions to take
action to avoid radiation exposure of an astronaut are easily identi-
fied when they are related directly to preventing a person from
reaching an administrative level or a dose limit. The recognition and
decision to take specific action to maintain radiation doses ALARA
are based on the organization’s commitment to continually assess
reasonable steps that can be taken to reduce doses. Thus, established
radiation protection and ALARA program models, philosophies and
lessons learned can be used to further enhance radiation safety
programs for astronauts.
Preplanning (i.e., engineering design and mission planning) and
the modification of activities in-flight are important components of
the radiation safety program. Occasionally, it may be necessary to
modify astronaut activities quickly to keep doses below administra-
tive levels or dose limits (immediate dose management). The ability
to predict the space radiation environs and to measure space radia-
tion levels in real-time are paramount to implementing immediate
dose management and ALARA actions.
Immediate dose management and ALARA actions may differ
between Space Shuttle missions and for ISS missions. In spite of
these differences, actions to reduce radiation exposure comprise a
continuum of effort to keep astronaut doses below dose limits, admin-
istrative levels, or ALARA. Longer ISS missions may result in a

70 / 8. RECOMMENDED MANAGEMENT OF SAFETY PROGRAM
considerably higher dose to the astronaut. However, ISS mission
objectives may allow more flexibility in the timing of certain proce-
dures, like an EVA, to avoid a high-dose environment.
8.4.1 Immediate Dose Management Issues
To be effective, immediate dose management in the NASA team
environment requires all individuals involved to understand the
resources available and their individual responsibilities with respect
to corresponding actions, and to establish effective lines of communi-
cation. Implementation of immediate dose management actions is
the responsibility of all team members involved with work impacting
the astronaut’s exposure to radiation. As soon as it is recognized that
a specific activity, e.g., an extended EVA, may cause an astronaut to
exceed the administrative level or the dose limit, action should be
considered to amend or terminate the activity. A written plan, nota-
bly the flight rules mechanism (Section 3.1), should contain the
implementing procedures.
8.4.2 Basic ‘‘As Low As Reasonably Achievable’’ Concepts
An effective ALARA program depends on everyone involved in
design and management of spacecraft and missions understanding
the space radiation environment and its impact on astronaut radia-
tion exposure.
The RHO should assess the opportunities to apply ALARA. All
levels of management should be involved in establishing the objec-
tives of the program to stimulate interest and involvement and to
foster ‘‘ownership’’ in activities. Real-time data on the radiation envi-
ronment during a flight are essential for the management team.
Postflight review of exposure data and assessment of actions taken
are necessary to provide the management team with feedback on
the effectiveness of their actions. The ALARA program should be
supported by senior management and should be reviewed periodi-
cally to determine its effectiveness.
8.4.3 Considerations for Spacecraft and Space Suit Design
The need for immediate dose management and ALARA actions
should be actively considered when designing or modifying the Space
Shuttle, ISS, and EVA suits.

8.4 IMMEDIATE DOSE MANAGEMENT / 71
The placement of radiation instruments should be chosen to pro-
vide the best real-time information on astronaut radiation exposure
(Section 6). Immediate dose management includes providing areas
where astronauts could be moved (i.e., to a safe haven providing
additional shielding, and/or by repositioning of the Space Shuttle),
and in the case of extreme exposures providing for emergency return
of the astronaut. To minimize career doses, optimized shielding
should be provided for those areas of higher occupancy, such as
areas used during off-duty hours and sleeping quarters. For example,
model calculations and ground-based testing indicate that hydroge-
nous compounds are most effective at attenuating GCR radiation.
Polyethylene (CH2) is lightweight, safe and simple to install, and has
recently been added to some of the sleeping quarters onboard ISS.10
8.4.4 Considerations for Preflight Planning
Once again, the historical information on space radiation environ-
ments and information on projected radiation doses are necessary
in assessing the mission plan and its impact on astronaut exposures.
Choice of the flight path has significant impact on both immediate
dose management and ALARA. Some choice may be available in the
altitude, attitude, time and duration of the flight to affect exposures.
In planning EVAs, choice may be available in the timing and dura-
tion. Full utilization of the design features should be incorporated
into the in-flight procedures at the preflight planning stage.
8.4.5 Considerations for Continuous In-Flight Review
During flights, changes can occur in the mission plan, as well as
in the space radiation environment, which can affect an astronaut’s
exposure or potential exposure. As with any management of exposure
control, the level of effort to identify dose reduction strategies, the
involvement of management review and the immediacy of action
increase as higher doses are anticipated. Astronauts have important
responsibilities in their own dose management during flights. They
are responsible for wearing the assigned dosimeters, for taking the
necessary radiation measurements, and for taking the directed
actions.
10 Cucinotta, F.A. (2001). Personal communication (Lyndon B. Johnson Space Cen-
ter, National Aeronautics and Space Administration, Houston, Texas).
72 / 8. RECOMMENDED MANAGEMENT OF SAFETY PROGRAM
A model for immediate dose management and ALARA assessment
by astronauts and mission control during LEO flights may be as
follows:
● As the mission progresses, continually identify and assess rea-
sonable opportunities to reduce astronaut doses even if the
administrative levels are not being approached (ALARA action).
● If the astronaut’s dose is anticipated to exceed a pre-established
administrative level for the mission, an assessment should be
made of actions to reduce further dose or to prevent the antici-
pated dose from being received (immediate dose management
action).
● If the astronaut’s dose is anticipated to exceed the cumulative
short-term or career limit, an immediate assessment, including
consideration of ending the mission for this astronaut, should
be made to reduce additional dose or to prevent the anticipated
dose from exceeding the short-term or career limit (immediate
dose management action).
● If an astronaut has received greater than the cumulative short-
term or career limit, then the mission should end for that astro-
naut as soon as practical (immediate dose management action).
8.4.6 Considerations for Postflight Review
The dose placed in the record for an astronaut from a given mission
may not be known fully until after completion of the mission. Some of
the radiation measuring devices used are passive devices, requiring
processing upon return to Earth. Some data gathered may not be
sent back to Earth during the mission, but stored electronically.
Upon return to Earth, these data need to be processed to provide
the final dosimetry record.
The final dose should be determined as soon as possible following
the mission and that information reviewed with the astronaut. These
actions should be completed before the astronaut’s next mission or
within three months, whichever is sooner.
A review should be made of the immediate dose management and
ALARA actions associated with the mission. The review should be
taken into account when determining the need for changes in design
criteria, preflight planning, and flight rules used for future flights.
8.5 Radiation Safety Training for NASA Personnel
An NCRP symposium (NCRP, 1997) identified ‘‘a universal need
to educate those involved in applying radiation dose limits to ensure

8.5 RADIATION SAFETY TRAINING / 73
that they understand that the limits are not there to ‘be used up’;
rather their purpose is to serve as a constraint on operation and as
a guide for the design of the associated radiation protection systems.’’
All NASA personnel whose work has impact on astronaut exposure to
radiation should be trained in the techniques of radiation protection,
with emphasis on implementation of immediate dose management
and ALARA. The scope and depth of this training should be related
to the corresponding level of impact the individual may have on
astronaut dose.
8.5.1 Astronauts
Astronaut training concerning radiation is described in NASA
(2000c) for Space Shuttle crew and NASA (2000d) for ISS crew.
Astronauts currently receive radiation training at various times
throughout their career. During the astronaut candidate year they
receive a 1 h overview of the JSC Space Flight Radiation Program.
When training for a specific flight, Space Shuttle astronauts are
instructed on use of the radiation monitoring equipment, and in the
course of this discussion, they receive a refresher on the radiation
environment. ISS crewmembers receive the same training as Space
Shuttle crewmembers, but also receive more detailed information
on their projected dose, and the implications and possible health
consequences of this exposure.
Ten days before the flight, during the medical exam, crewmembers
are advised of the projected exposures and associated risks of both
in cabin and EVA exposure. They are also reminded to wear their
personal dosimeters throughout the mission. Space Shuttle crew-
members receive approximately 30 min of radiation training in the
preflight period. ISS crewmembers receive 2.5 h of radiation training
prior to flight. The dose received is communicated to the astronaut
during a postflight debrief.
The astronaut’s radiation protection training should focus on the
following:
● biological risks of radiation exposure, particularly for the high-
LET space radiations
● measurement of radiation and dose
● operation of and proper wearing of personal radiation measur-
ing devices
● techniques an astronaut can use to reduce dose in-flight
● specialized training specific to a given mission, such as operation
and maintenance of an area radiation monitor

74 / 8. RECOMMENDED MANAGEMENT OF SAFETY PROGRAM
● procedures and administrative controls including dose limits
and the flight rules (immediate dose management and ALARA)
● terminology associated with dose management activities to
ensure effective communications
● NASA’s operational radiation safety program and how ALARA
actions are proposed and implemented
● review of actual events, especially those involving high tran-
sient doses
8.5.2 Flight Directors
Flight director training concerning radiation is described in the
Flight Director Certification Guide (NASA, 1998). The flight director
is the individual responsible for a given mission. The current radia-
tion safety training for flight directors consists of an introductory
briefing at the start of their overall training, which includes radiation
protection terminology, description of the space radiation, radiation
risk versus dose, dose limits, and the ALARA philosophy. Beyond
this briefing, they generally receive little formal training in radiation
issues. Occasionally a special briefing is provided when there are
significant changes or significant updates to the flight rules. Most
training is informal, but can be substantial, occurring during devel-
opment of radiation flight rules and in the course of mission planning,
mission simulation, and flight training.
Like managers and supervisors of other radiation workers, the
flight directors should receive radiation protection training that par-
allels those they supervise, but not necessarily to the same depth.
The flight director’s radiation protection training should focus on
the following areas:
● policies and procedures affecting astronaut’s radiation dose
● implementation of immediate dose management and ALARA
actions and their importance
● interfaces of different NASA groups so that they are able to
identify and resolve conflicts in coordinating radiation protec-
tion activities
● terminology associated with dose management activities to
ensure effective communications
● NASA’s operational radiation safety program and how ALARA
actions are proposed and implemented
● review of actual events, especially those involving high transient
doses and those involving the actions of a flight director

8.5 RADIATION SAFETY TRAINING / 75
8.5.3 Flight Surgeons
Flight surgeon training concerning radiation is described in the
ISS Crew Surgeon Training Certification Plan (NASA, 1999).
A flight surgeon is assigned to each mission and is responsible for
that crew’s health and safety. The current radiation safety training
for flight surgeons consists of an initial 3 to 4 h of training in radia-
tion issues, including the ALARA principle. The RHO provides quar-
terly briefings to the flight surgeons as refresher training and to keep
them informed of changes and new radiation issues and concerns. In
the course of their duties flight surgeons may receive substantial
informal training as part of the team that is responsible for crew
health and safety. They also receive informal training through
involvement in mission planning and as participants in a variety of
activities that address radiation issues.
As with the flight directors, the flight surgeon should receive radia-
tion protection training that parallels those of the astronauts, and
particularly in regard to health effects. The flight surgeon’s radiation
protection training should focus on the following areas:
● biological risks of radiation exposure, particularly for the high-
LET space radiations
● procedures and administrative controls including dose limits
and flight rules (immediate dose management and ALARA)
● implementation of immediate dose management and ALARA
actions, and their importance
● interfaces of different NASA groups so that they are able to
identify and resolve conflicts regarding health consequences of
ongoing or projected radiation doses
● terminology associated with dose management activities to
ensure effective communications
● NASA’s operational radiation safety program and how ALARA
actions are proposed and implemented
● review of actual events, especially those involving high transient
doses and those involving the actions of a flight surgeon
8.5.4 Radiation Health Officer and Radiation Safety
Support Groups
The RHO and individuals in the radiation safety support groups
should have training equivalent to radiation protection professionals
in other professions who are assigned equivalent types of radiation
safety duties (NCRP, 1998; 2000b). Radiation protection training must
also be specific to the special circumstances of the space radiation

76 / 8. RECOMMENDED MANAGEMENT OF SAFETY PROGRAM
environment. They should also have training on the specifics of
NASA’s operational radiation safety program for LEO.
8.5.5 Other Supporting Specialists
Other individuals whose work can affect the astronaut’s radiation
exposure should have radiation safety training that is commensurate
with the level of effect their work might have on astronaut dose.
Among these individuals are engineers, designers and mission plan-
ners. These individuals’ radiation protection training should focus
on developing the following knowledge:
● how their work can affect astronaut dose
● what the immediate dose management and ALARA concepts
are, and how they can help implement them
● NASA’s operational radiation safety program and how ALARA
actions are proposed and implemented
● review of actual events, especially those involving high transient
doses and those involving the actions of individuals with similar
work responsibilities
9. Radiation Safety Records
The principal reason for keeping radiation safety records is protec-
tion of the astronauts. This Section describes the elements of a pro-
gram for operational radiation safety records, but does not prescribe
a particular methodology for construction or maintenance of the
records.
In this Report the terms ‘‘dosimetry records’’ and ‘‘radiation safety
records’’ are used. Dosimetry records are the collections of informa-
tion that document the radiation doses that astronauts receive from
space flight, mission-related aviation activities, mission-related bio-
medical research, and previous occupational work. The dosimetry
records contain, or are linked to, all the basic information that is
necessary to obtain the radiation doses, e.g., the personal dosimetry
measurement package (Section 6.3). Radiation safety records are the
broader collections of information that relate to radiation exposure of
the astronauts. The radiation safety records consist of multiple
sources of information that are linked (i.e., the dosimetry records
and their supporting data and files, and other information that bears
on the radiation exposure of astronauts). When the term ‘‘records’’
is used, the meaning is general.
The objectives of the overall radiation safety record-keeping pro-
gram are to:
● aid in the protection of astronauts
● evaluate the effectiveness of radiation protection programs
● advance the collection of data that are accurate, reliable, confi-
dential, and retrievable
● provide a uniform set of records
Dosimetry records for each astronaut should be kept in a manner
to satisfy the following purposes:
● inform astronauts of their mission and cumulative radiation
doses
● make decisions on crew selection and mission planning
● provide information for making decisions about the flight plan
● evaluate the operational radiation safety program to ensure
effective program operation
● demonstrate compliance with administrative levels and dose
limits
77
78 / 9. RADIATION SAFETY RECORDS
● provide reliable data for epidemiological studies
● provide information for making or contesting claims for radia-
tion-induced injury
All records should be maintained in accordance with the highest
standards of record keeping (ANSI, 1999; Fienberg et al., 1985;
NCRP, 1992) and should be legible, accurate, reliable and interpret-
able. Individuals who maintain the records should be diligent in
protecting the identity of astronauts and any proprietary informa-
tion. Information that may be separate from the dosimetry records,
but which is important to interpret doses or recalculate dose quanti-
ties, should be linked in a manner that assures all information will
be available for future interpretations or recalculations.
Records may take the form of hard copy, microform, or computer
readable media. Each form has its own strengths and limitations
and may be used for different purposes. Of particular importance is
the conversion of old data to new formats when changes in computer
hardware render old formats unreadable. Records should be stored
in a durable enough manner to limit the risk of loss from theft, fire
and water damage. A listing of content and location of records should
be maintained to facilitate their retrieval.
When data are stored on computer readable media, the original
or reproduced records from which the computer records were derived
should be maintained separately to help interpret ambiguous com-
puter data and to verify computer records if they become damaged
or unreadable. To enhance reliability, computer records should be
backed up on a regular basis.
9.1 Content of Records
Standard operating procedures should be written to enable those
responsible for generation and maintenance of the records to docu-
ment and retrieve information in a timely and reliable manner.
Procedures should address the indexing, linkage and storage of docu-
ments. Standard codes and coding conventions should be used, e.g.,
North American Industry Classification System (OMB, 1997) and
Standard Occupational Classifications Manual (OMB, 2000).
Information should be documented in as specific or quantitative
a form as is available. However, qualitative information should also
be kept when it may be useful for interpretation of the records or
recalculation of radiation doses. When quantities are derived or cal-
culated from measured quantities, both the measurement data and
the quantities derived from them, along with references to the

9.1 CONTENT OF RECORDS / 79
method used in the derivation should be maintained along with all
information that may be useful in the interpretation of the measure-
ment data. Missing information should be addressed in the records,
and data that were estimated or calculated rather than measured
directly should be documented. The records should contain adequate
information to facilitate the interpretation of an empty field or zero
value. Computations and estimates should be supported by records
that provide the method used to perform the calculation or to make
the estimate.
Dosimetry records and associated reports should include calendar
dates of radiation exposures and starting and stopping dates for
radiation monitoring as well as the date the records were generated.
These records should include the magnitude and dates of radiation
exposure and linkage to other records that identify the sources of
exposure, place where the exposure occurred, description of radiation
fields, description of physical factors that may alter the field, and
information about other potentially harmful exposures.
The dosimetry records should contain sufficient information to per-
mit unique identification of the individuals involved and information
on job or task assignments that should be updated at least annually.
Information on general work location (e.g., Space Shuttle, ISS, EVA)
should be linked to the dosimetry records to facilitate correlation
analysis. Other information, such as non-mission related diagnostic
and therapeutic medical radiation exposures, should be linked to the
dosimetry records, but the radiation doses from the medical proce-
dures should not be added to occupational doses either for planning
purposes or to limit occupational exposure. Medical radiation expo-
sures should be maintained in the medical department.
Information important to standard methodology, collection of data,
or calculation of radiation doses may exist in other files that are
separate from the dosimetry records. These files should be linked to
the dosimetry records in a manner that facilitates re-evaluation and
auditing of astronaut radiation doses. Files to be kept in or linked
to the dosimetry records include:
● standard operating procedures on how to maintain the record
● standard operating procedures on how to compute the radiation
dose of record
● personal data for each astronaut, e.g., age, sex, height and weight
● flight plans
● steps taken to avoid or minimize radiation exposure during a
flight, e.g., changes in the flight plan such as reduction of time
spent outside the spacecraft or moving to a shielded portion of
the spacecraft during increased solar activity

80 / 9. RADIATION SAFETY RECORDS
● raw data on the radiation environment and spacecraft character-
istics and orientation, which were collected at the time of the
astronaut’s exposure to the radiation
● information on radiation detectors and measurement equipment
including type, serial number, and calibration data
● biodosimetry data and computations that utilize these data
● computations of radiation doses, including method used to
account for radiation quality and the tissue weighting factor (wT)
● reports of monthly, annual and career radiation doses from space
flights for each astronaut
● radiation dose estimates for biomedical activities that are associ-
ated with specific flights or research protocols
● radiation dose estimates from associated noncommercial avia-
tion activities undertaken as part of mission requirements
9.1.1 Records of Career Doses
Dosimetry records constitute the formal documentation for each
astronaut’s space-related radiation exposure history and should con-
tain the cumulative dose from space flight, mission-related aviation
activities, and mission-related biomedical research. Since the radia-
tion doses for each astronaut may not be assigned until well after
completion of a flight (or may be revised as new information becomes
available), NCRP recommends that the dosimetry records be updated
as soon as possible after the radiation doses are assigned (or
changed). The new doses should be communicated to the astronauts.
The dosimetry records should contain, or be linked to, all the
basic information that is necessary to obtain the required dose-limit
quantities (GT and E). In addition to the astronaut’s measured radia-
tion doses (e.g., from personal dosimeters or area monitors) for each
point in time or monitoring period, the dosimetry records should
contain the assigned value of DT for each tissue or organ and the
method by which HT for each organ or tissue was obtained for use
in the computation of E for that astronaut. The computed value of
E should be linked to the standard operating procedure that
describes the computation. The value of GT for skin, lens of the eye,
and bone marrow should be based on surface measurements, which
are adjusted as described in Section 5. The dosimetry records should
also be linked to information on radiation exposure conditions at the
location and time of exposure.
Normally, astronauts are not exposed to radioactive materials that
may be ingested, inhaled or absorbed through the skin. Participation
in biomedical research studies that use radionuclides as tracers

9.1 CONTENT OF RECORDS / 81
would be an exception to this. When astronauts are monitored for
internal radiation sources, the dosimetry records should contain the
basic physical measurements (e.g., activity) used to determine DT
to organs and tissues. Information on mode of intake and, where
applicable, data on particle size distribution, chemical form, and
chelation or decorporation therapy, as well as, procedures, bioassay
data, biokinetic and dosimetric models, and other parameters used
to determine DT should be linked to the dosimetry records. For inter-
nally deposited radionuclides from these biomedical studies, HT
should be obtained using NCRP (1993) radiation weighting factors
(wR) and then used to compute E.
If an astronaut received occupational exposure from previous
employment or military service, information on the identity of each
former employer and the radiation exposure for each period of
employment should be obtained. This information may be included
directly in each astronaut’s dosimetry records or may be kept in
other files that are linked to the astronaut’s dosimetry records.
Annually, each astronaut should receive a confidential report of
his or her radiation dose assessment and information on the signifi-
cance of the doses. The report should include career radiation doses
in terms of E for stochastic effects and monthly and annual doses
in terms of GT for deterministic effects to skin, lens of the eye, and
bone marrow.
In addition to occupational radiation dose, the report may contain
information on radiation doses from diagnostic or therapeutic medi-
cal procedures. Astronauts should be provided with information that
describes the significance of these nonoccupational doses and the
potential biological effects.
9.1.2 Records of Prospective and Retrospective Studies
The probability that particular records will need to be retrieved
depends on the purpose for which the records are to be used. The
four major potential uses of archived dosimetry records are:
● evaluation of the radiation safety program
● compliance with the dose limits
● use in epidemiological research
● use in litigation
If dosimetry records for short term or career doses are updated
(revised) in a timely fashion whenever relevant new information
(e.g., new values for wT) becomes available, they will have greater
value for prospective use in planning astronaut activities and in
82 / 9. RADIATION SAFETY RECORDS
retrospective studies. Linkages to other information as described
above (Section 9.1) will facilitate broader analysis of calculations,
computations, flight control plans, and other variables that may
have affected the recorded doses.
9.2 Continuity of Records Over Time
Dosimetry records should provide continuity of career radiation
doses from past, present and future missions. Continuity is impor-
tant to evaluate trends in radiation doses among astronauts over
time, for prospective estimation of doses, and for assessment of cumu-
lative career doses. As discussed in Section 6.3.3, NCRP recommends
that the dosimetry records include the low- and high-LET compo-
nents of the radiation field. If possible, the dosimetry records for the
high-LET component should be divided into its neutron plus high-
energy secondary particle (from protons) component and its HZE-
particle component.
9.2.1 Existing Records and Unanalyzed Data Files
As a general recommendation, NCRP advises that any existing
data related to space missions be examined and compared to dosime-
try records to confirm that radiation dose estimates are based on
all available data. If previously unanalyzed data are found, NCRP
recommends that they be analyzed and that a determination be
made of the value of the data in estimating astronaut doses.
The amount of data that may exist, which could change the current
career dose estimate for astronauts, may be considerable. Analysis
of all these data may or may not have a significant effect on the
recorded annual dose estimate. Therefore, NCRP recommends that
the data be identified and that representative samples of the data
be fully analyzed to determine the extent of their effect on current
dose estimates.
9.2.2 Future Adjustment of Records
Dosimetry records should be updated retrospectively whenever
there is a systematic change in methodology (e.g., method of account-
ing for radiation qualities or wT) or new information becomes avail-
able (e.g., previously unanalyzed data). Any data that could affect
the estimation of astronaut doses should be analyzed as soon as

9.3 RETENTION OF RECORDS / 83
possible or retrospectively to provide the best estimate. NCRP recom-
mends that astronaut dose estimates be adjusted whenever differ-
ences in revised dose assessments exceed 30 percent of the original
dose assessment (see discussion of accuracy in Sections 6.4.1 and
6.4.2).
9.3 Retention of Records
Determination of the retention period depends on the conse-
quences of having or not having the information available when it
is needed. Regulations specify minimum retention periods for the
first two potential uses given in Section 9.1.2, generally within a
time frame of years or possibly the lifetime of the individual. Conse-
quences associated with potential future need for records for epide-
miological research and litigation are difficult to predict. Need of
records for these purposes may not arise for decades. NCRP (1992)
recommends that records be maintained for specific periods of time
appropriate for their intended purposes. Because of the unique fea-
tures of astronaut radiation exposures, NCRP recommends at this
time that records be maintained indefinitely.
Appendix A
Time-Dependent Variationsin the Space RadiationEnvironment and the Needfor Active Real-TimeMonitoring
A.1 Background
Temporal changes in the external radiation environment occur by
two major processes and one minor process:
● precession of the orbit within Earth’s asymmetric magnetic field
● modulation of the sources by solar activity (both short- and long-
term variations)
● change in altitude due to atmospheric drag and re-boost
In addition, there are local spatial variations within the Space
Shuttle, ISS, or space suit due to the relative differences in shielding
at locations visited by the astronaut. This requires an accurate
knowledge of the time spent by the astronaut within the spatially
distributed fields and the temporal field changes during those visits.
There are uncertainties in the external radiation environment.
The properties of GCR are well known and the transmission through
the geomagnetic field is adequately understood except during brief
periods of large geomagnetic storms. Such storms result in little
uncertainty in the accumulated fluence over a Space Shuttle or ISS
mission. The neutron albedo is directly correlated to the GCR intensity
and has been well characterized by satellite and balloon measurements
and theoretical models. The LEO trapped proton environment is rel-
atively stable with mainly long-term variations over the solar cycle
but this time variation is poorly represented in current environmental
84

A.1 BACKGROUND / 85
models and is a major source of uncertainty in Space Shuttle
or ISS exposures. In addition, the trapped radiations are highly
anisotropic; this anisotropy is not part of the usual environmental
models.
SPEs cause short-term enhancements in the extraterrestrial radi-
ation environment, the effects of which are mainly limited to the
geomagnetic polar regions. Due to orbit precession, the worst-case
SPE exposure occurs when the line of nodes (i.e., the intersection of
the equatorial plane with the orbital plane) is near 210 degrees
longitude. Only the two prior and two succeeding orbits are impor-
tant to exposure if the 210 degree line of nodes is coincident with
the peak of the SPE intensity. The time of particle arrival relative
to orbital precession is critical to exposure evaluation. A large geo-
magnetic storm could greatly enhance the radiation exposure if the
peak storm is at the SPE peak intensity while the orbit plane is
aligned in the worst-case orbit. The expected exposures from an SPE
and their associated uncertainties depend on many variables. The
above considerations apply to both Space Shuttle and ISS and during
EVA. In addition to these sources, the trapped electrons are impor-
tant for EVA. They are filtered from the interior of the Space Shuttle
or ISS radiation environment by the micrometeoroid/debris bumper
and pressure vessel and the resulting bremsstrahlung is unimpor-
tant compared to other LEO sources. The trapped electrons are
highly variable with relativistic electron precipitation events occur-
ring every few to several weeks. During these events, the fluence
can rise suddenly by up to four orders of magnitude with slow decline
over several days. These events are most important to skin exposures
during EVA. The helmet provides significant protection to the lens
of the eye especially with the visor in the down position.
Active detectors provide information, in real-time, on radiation
fields inside and outside the spacecraft. This information is used for
direct determination of D and H. Active dosimeters can be either
area monitors or personal dosimeters. Active instruments can also
measure particle fluence and fluence rates as a function of particle
charge and energy. Active devices, by virtue of their immediate
availability, are valuable sources of data needed for timely imple-
mentation of immediate dose management and routine ALARA.
The instrumentation should be capable of providing dose rate as
well as integrated doses with time resolution from several minutes
to several days.
Information should, where possible, be immediately available to
astronauts in space as well as through downlink to the ground where
more extensive analysis can be performed.

86 / APPENDIX A
Active dosimeters should be used inside and outside of the space-
craft. Some serve as area monitors at fixed locations while others
are portable area monitors that can be moved to various locations,
or even carried on the astronaut’s person, including during EVA.
A.2 Types of Active Detectors Used in Space
A.2.1 Tissue Equivalent Proportional Counters
A TEPC is a gas filled detector that is operated in the proportional
mode such that the signal generated is proportional to the initial
ionization generated in the gas (Rossi and Rosenweig, 1955). The
tissue equivalence of a TEPC is based on the composition of the wall
that defines the gas cavity as well as the composition of the gas
itself. Generally the wall is fabricated from a conducting plastic such
as A-150� (Standard Imaging Inc., Middleton, Wisconsin). Since a
low-density gas is used to simulate very small volumes of material,
the Bragg-Gray cavity theory would apply for any gas mixture. How-
ever, in order to avoid variations in stopping power ratios (Swall/Sgas)
for the vast array of incident particles, the gas is also chosen to have
an atomic composition of soft tissue as well as retain the properties
necessary for gas multiplication in a high electric field. It is usually
a combination of carbon dioxide, argon, and either methane or
propane.
Another feature of a TEPC is that the quantity of gas in the cavity
is carefully regulated. The reason for this is that energy deposition
from the passage of a charged particle in the gas can simulate energy
deposition by that particle in a volume of tissue having dimensions
similar to a mammalian cell. Thus, energy deposition events mea-
sured by TEPC should reflect the pattern of energy deposition in
microscopic volumes. This in turn provides information on the qual-
ity of the incident radiations.
The basis for simulating small volumes of tissue rests in the fact
that cross sections for ionization at the atomic and molecular level
are independent of density. For example, energy transfer is con-
served providing that:
�t xt � �g xg, (A.1)
where:

A.2 TYPES OF ACTIVE DETECTORS USED IN SPACE / 87
xt � the thickness of tissue to be simulated
�t � the density of tissue, taken to be 1 g cm�3
xg � the thickness of the gas cavity in the detector
�g � the density of the gas in the detector
A common case is when a spherical or cylindrical detector with a
diameter of 10 mm is used to simulate a volume of tissue with a
diameter of 1 �m. For this situation, the gas pressure in the cavity
would be about 6,700 Pa. These conditions can be achieved routinely
and provide signals that are reasonably easy to process and record.
They have been successfully used for dosimetry in mixed fields con-
sisting of fast neutrons and photons, as well as for manned space
missions.
For heavy charged particles passing through a very small amount
of material, the energy lost is small and LET remains unchanged.
If all of the energy transferred to the volume of material is absorbed
within the volume then:
� � L x (A.2)
where:
� � the energy deposited (keV)
L � LET (keV �m�1)
x � the path length through the material (�m)
Thus, energy deposition in a cell for this case depends on both
LET and path length or trajectory through the volume. This should
also be the case for a TEPC.
Microdosimetry was developed to accommodate these principles
(ICRU, 1983). It is known that there is an association between RBE
and LET. This has been extended to radiation protection where Q
is also a function of LET. Thus, the energy deposition in a cell should
be divided by a length if it is to be related to LET. However, the
length through the cell may not be known and this changes from
event to event. Thus, a quantity called lineal energy (y) was defined
such that:
y ��
�, (A.3)
where:
y � the lineal energy for an event (keV �m�1)
� � the energy deposition associated with the event (keV)
� � the mean chord length for the distribution of possible trajecto-
ries through the simulated volume of tissue (�m)

88 / APPENDIX A
Thus, y is a random variable that depends on the distribution of
energy deposition events in the volume of interest and a constant
that depends on the geometry of the tissue. The mean chord length
was chosen for the denominator of y because for a distribution of
random events with constant LET, the mean value of y will be numer-
ically equivalent to LET.
For the case where LET of the particles is constant, the response
of a TEPC will reflect the chord length distribution for the simulated
volume of interest. Figure A.1 shows the expected distribution of
f (y) for a uniform isotropic particle fluence [&(L)] having a single
value of L equal to 215 keV �m�1. Curve 1 represents a sphere with
a diameter of 1 �m and Curve 2 represents a cylinder with diameter
and length equal to 1 �m. Although the mean chord length happens
to be the same for both of these distributions, the pattern of energy
deposition events is distinctly different.
It is clear that even for an idealized case, the measured distribution
f (y) will not be a direct representation of the distribution of LET for
the incident &(L). The distribution of f (y) is a convolution of &(L)
and f (x), the distribution of path lengths (x). Thus, if f (x) is known,
it should be possible to deconvolute f (y) and obtain &(L). When f (x)
is the triangular distribution for a sphere, the deconvolution reduces
to an analytical expression that is easy to solve. Other distributions
of f (x), including that for a cylinder, usually require complicated
numerical procedures.
The situation for heavy nuclei is more complicated. The energy
deposition does not occur in a limited region surrounding the track.
High-energy delta rays remove energy away from the axis of the
track. Some of the energy can actually escape from the volume of
interest. For the same reason, there can be energy deposition in a
volume of material that was not traversed by a track at all. In
addition to these factors, there is additional variance in the measured
signals due to energy straggling, gas multiplication, and effects due
to the fact that the density of the wall surrounding the cavity is
40,000 times greater than the density of the gas.
Curve 3 in the following Figure A.1 is the distribution f (y) mea-
sured in a spherical TEPC exposed to 56Fe particles at 400 MeV n�1
(L � 215 keV �m�1) (Gersey et al., 2002). It clearly is not a simple
triangle. There is a broad peak in the distribution that resembles a
triangle. These events are from particles that pass through the gas
cavity, but the energy absorbed in the cavity is less than L times x
because some high-energy delta rays escape the sensitive volume.
There is also a pronounced peak of events with very small values of
energy deposition. These events correspond to particles that do not
pass through the gas cavity but intersect the plastic wall surrounding

A.2 TYPES OF ACTIVE DETECTORS USED IN SPACE / 89
f(y) 4
32
1
y (keV µm –1)
0 100 200 300 400 500
Fig. A.1. Distributions of y in a TEPC for a uniform fluence of 56Fe
at 400 MeV n�1. Curves 1 and 2 represent the case where energy deposited
is equal to L times the chord length in a sphere (Curve 1) and a cylinder
(Curve 2). Curve 3 is data from measurements with a spherical detector.
Curve 4 is the result from a calculation using restricted LET (L�) and
straggling.
the cavity. Some of the delta rays originating in the plastic manage
to enter the cavity and deposit energy. There is also a tail of events
that corresponds to very large energy depositions. These events are
caused by particles that just graze the inside wall of the detector. This
produces a flood of low-energy delta rays that combine to generate a
very large energy deposition event in the gas (Rademacher et al.,
1998). These patterns have been observed for 56Fe from 200 to
1,000 MeV n�1 as well as for other ions such as 28Si, 16O, and 12C.
The magnitude of these effects will change with the charge and
velocity of the heavy ion making the deconvolution process even
more complicated when L has a large range of values.
A model has been developed to compute energy deposition by HZE
particles in order to predict the measured distribution of f (y) by a
TEPC exposed to space radiation (Shinn et al., 1999; Xapsos, 1992).
This computation takes into account chord-length distributions
through the detector similar to Curves 1 and 2 in Figure A.1. Energy
deposition is obtained using a model for restricted LET (L�) to simu-
late delta-ray escape and a lognormal distribution of energy lost
along the track to simulate particle straggling. The results of this
model for a 1 �m diameter sphere are shown as Curve 4 in
Figure A.1. When compared with the expected triangle for a sphere,
there is a decrease in energy deposition as well as a smoothing effect
due to straggling. The model does not however reproduce the data

90 / APPENDIX A
corresponding to very low and very high-energy depositions gener-
ated in the wall of a TEPC.
Although TEPC does not provide a direct measurement of LET
distribution of the incident particles, it does provide valuable infor-
mation relating to the quality of the radiation, and therefore allows
an estimate of H to a small mass of tissue at the location of TEPC.
One important issue is related to the integrated spectrum of energy
deposition in terms of D. Energy that is lost by the escape of delta
rays when the particles pass through the sensitive volume must be
replaced by delta rays that originate outside of the volume (i.e., from
the wall). Table A.1 shows results for the fraction of D obtained for
a uniform fluence of 56Fe particles at 400 MeV n�1 from the data
shown in Figure A.1. Also shown are results for the first and second
moments of the lineal energy.
The measured data for 56Fe at 400 MeV n�1 indicate that TEPC does
satisfy charged-particle equilibrium and therefore gives a correct
estimate of D to tissue for this HZE particle. However the restricted
stopping power model underestimates the dose by about 20 percent
because it does not consider energy transfer from particles that pass
near but not through the sensitive volume of the detector. Additional
experiments and data will be required to determine the extent to
which charged-particle equilibrium is achieved for HZE particles
other than 56Fe.
As expected, the frequency-averaged lineal energy (yf) is numeri-
cally equivalent to LET for the idealized distributions with a sphere
and cylinder. However this relationship is not preserved for the 56Fe
data or L� model. This is further confirmation that f (y) is not a
surrogate for &(L). It is however interesting that the dose-averaged
lineal energy (yD) is also different for all four distributions but the
value from the 56Fe data is numerically equivalent to LET. This has
been demonstrated for 56Fe from 200 to 1,000 MeV n�1 (Gersey et al.,
TABLE A.1—Estimates of the fraction of D, yf and yD associated
with the curves shown in Figure A.1.
yf yD
D (%) (keV �m�1)
LET in spherea 100 215 241
LET in cylindera 100 215 270
Fe-56 data 104 146 216
L� model 81 174 193
aRefers to the ideal case where energy deposited is equal to LET times
chord length.

A.2 TYPES OF ACTIVE DETECTORS USED IN SPACE / 91
2002). Thus, it is possible that even though the measured spectrum
from a TEPC is not a direct determination of LET, yD is coupled to
LET in a way that is useful for radiation protection purposes.
A TEPC is also sensitive to high-energy neutrons (Badhwar et al.,
2000; in press). Charged particles generated in the walls of a TEPC
will deposit energy in the gas cavity. The pattern of energy deposition
is similar to charged particles originating outside of the detector.
Thus, a TEPC automatically includes the contribution from neutrons
that either interact in the detector or elsewhere in the spacecraft.
A TEPC could be placed within a hydrogenous phantom to create
the charged-particle intensity that would be expected from neutron
interactions in a person.
TEPC systems currently used by NASA resolve energy deposi-
tion events in the range from a fraction of a kiloelectron volt
(y � 0.3 keV �m�1) to 800 keV (y � 1,000 keV �m�1). The lower bound
is determined by electronic noise. The upper bound by saturation of
shaping amplifiers. As electronic components improve, it should be
possible to reduce noise and extend the range of these detectors.
A.2.2 Semiconductor Detectors
Detectors based on thin semiconductor crystals measure the ion-
ization energy loss of an incident particle. Energy deposited within
the detector can be collected and analyzed in real-time, and data
from one or more such detectors can be convoluted to determine a
particle’s charge and total energy. The average energy necessary to
create an electron hole pair (ion pair) is approximately 10 times
lower in a silicon diode compared with gas. This results in improved
energy resolution and thus provides an opportunity for precise esti-
mates of LET for the incident particles.
The detectors are planar with a thickness ranging from 50 to
5,000 �m and diameters ranging from 10 to 60 mm. High-energy
charged particles pass through the sensitive volume. The magnitude
of the signal (dE) registered by the detector is related to the trajectory
(angle of incidence) and LET of the incident particle. Energy resolu-
tion improves as dE increases. If the acceptance is restricted to small
angles, the path through the detector is approximately equal to the
thickness (xd) and L � dE/xd. Under this approximation, a detector
can yield D, Q and H for charged particles. If the variation in path
length is restricted to 10 percent, the incidence angle must be limited
to 26 degrees, which corresponds to a solid angle acceptance of 0.1.
This means that approximately 90 percent of the incident particles
must be rejected.

92 / APPENDIX A
Some of these restrictions can be eliminated by adding one or
more position sensitive solid-state detectors (PSD) to the system.
For example, resistive charge division is used to determine the loca-
tion of the incident particle in the plane of the detector. Data from
two or more PSDs placed a fixed distance apart can be used to
reconstruct the trajectory (incident angle) of the particle and thus
the true path length (dx) through the dE detector. The dE/dx thus
obtained is L�. There must be sufficient separation between the PSDs
in order to measure the incident angle. Limits on the sensitive area,
and separation between PSDs have the effect of restricting the angu-
lar acceptance of this system.
For dosimetry purposes alone, a thick detector (xd � 500 �m) with
an area of about 300 mm2 (diameter �20 mm) should be sufficient
for a first approximation to D and Q, and devices of this type that
are sufficiently compact to be worn on an astronaut’s person exist.
For this case the interpretation of the pulse height spectrum in terms
of H must take into consideration that some of the particles were
incident directly upon the dosimeter and some went through the
astronaut’s body. In addition, this system cannot distinguish slow
particles that stop in the detector from those that penetrate. Thus,
dE may be correct for estimating D, but setting dx � xd may under-
estimate L.
Detector systems that contain several solid-state detectors can
eliminate some of the problems mentioned above (Badhwar et al.,
1995b; Doke et al., 2001). These arrangements are often called parti-
cle telescopes since they view a selected region of space. PSDs can
be used to define the trajectory. The distribution of energy loss in
successive detectors is a unique signature of a particle’s charge and
energy, and instruments of this type have been flown on satellites;
however, the number of detectors required may render this method
impractical for dosimetry. Combining a thin detector with one suffi-
ciently thick to stop a charged particle is effective for charge identifi-
cation, but also may be impractical for many of the highly energetic
particles found in space.
There have been attempts to make omnidirectional detector
arrays, in contrast to the collinear pattern used in particle telescopes.
One design is based on making a cube from silicon strip detectors
(Yoshihira et al., 2000). The detector would measure dE and position
of the incident particle as it entered and exited the cube. The position
information is used to compute the trajectory of the particle and dx
in each detector. This could then provide &(L)/d� as a function of
direction or &(L) integrated over all directions.
A single active silicon detector system has been made compact
enough to serve as a personal dosimeter (Badhwar, 2000). It provides

A.2 TYPES OF ACTIVE DETECTORS USED IN SPACE / 93
on-demand readout of accumulated D as well as D·. Power is obtained
from a stack of lithium batteries that last for about 28 d. It can be
modified to operate from space suit power during an EVA.
A.2.3 Cerenkov Counters
An alternative approach is to make a determination of dE/dx and
velocity (�). One way to do this is by measuring Cerenkov radiation.
The procedure is based on using thin solid-state detectors to measure
dE/dx and a Cerenkov counter to measure the photon emission
(dN/dx) in a gas or liquid. These are related to the incident particle
in the following manner:
dE/dx �Z2
�2, (A.4)
dN/dx � Z2 1 �1
�2n2, (A.5)
where n is the refractive index of the medium in the Cerenkov
counter. The two equations can be solved simultaneously to obtain
the charge of the incident particle (Z) and velocity (�).
The Cerenkov counters used in these applications generally have
a threshold of about � � 0.5 (200 MeV n�1) and saturate at about
� � 0.75 (500 MeV n�1).
A.2.4 Ionization Chambers
Ionization chambers can be used to measure D. They, however,
do not give information on the quality of the incident radiation for
mixed radiation fields. There is also a problem of recombination
along the track of high-LET particles.
However, ionization chambers can be used as screening detectors
for solar events or to monitor enhanced electron intensity following
magnetic storms. They could be employed as area monitors inside
and outside of the spacecraft in order to confirm that dose rates do
not approach or exceed specified values.
Ionization chambers have been designed to obtain the quality fac-
tor in mixed radiation fields based on columnar recombination of
high-LET radiation (Zielczynski, 1962). Measurements are made
over a range of voltages from 2 to 1,200 V. The data are used to
determine the change (slope) of the measured current as a function
of voltage. This slope is related to the quality factor through an
empirical formula (Baarli and Sullivan, 1965). Recombination

94 / APPENDIX A
chambers have been used to obtain the quality factor for mixed
fields at high-energy particle accelerators (Cossairt and Elwyn, 1987;
Hofert and Raffnsoe, 1980). It is not known if the empirical relation-
ships will remain the same for space radiations such as a trapped
protons or GCR. It is also imperative that the dose rate remains
constant while sweeping the voltage, which can take up to an hour
at low dose rates. This may be impractical in LEO and therefore a
second ion chamber with constant voltage would be necessary for
normalization.

Appendix B
Computational Methods
The determination of the types and energy distributions of parti-
cles, transmitted through a shield material and through astronaut
tissues, requires the solution to radiation transport equations of the
process with appropriate boundary conditions for the external space
radiation environment. The relevant transport equations are the
linear Boltzmann equations derived on the basis of conservation
principles (Wilson et al., 1991) for the fluence &i(x,�,E) of particles
of type i moving in direction � with energy E as:
� � �&i(x,�,E) � ����ik(�,��,E,E�) &k(x,��,E�) d�� dE��
� �i(E) &i(x,�,E), (B.1)
where �i(E) is the rate of removal of particles of type i with energy
E moving in direction �, �ik(�,��,E,E�) are the media macroscopic
cross sections for various atomic and nuclear processes k producing
particles of type i with energy E moving in direction �, including
spontaneous disintegration. In general, there are hundreds of fluence
terms [&i (x,�,E)] with several thousand cross-coupling terms
[�ik(�,��,E,E�)] through the integral operator in Equation B.1. The
total cross section [�i(E)] with the medium for each particle type of
energy E may be expanded as:
�i(E) � �i,at(E) � �i,el(E) � �i,r(E), (B.2)
where the first term refers to collision with atomic electrons (at),
the second term is for elastic nuclear scattering (el), and the third
term describes nuclear reactive processes (r). The microscopic cross
sections and average energy transfer are ordered as follows:
�i,at(E) � 10�16 cm2 for which �Eat � 102 eV; (B.3)
�i,el(E) � 10�19 cm2 for which �Eel � 106 eV; and (B.4)
�i,r(E) � 10�24 cm2 for which �Er � 108 eV. (B.5)
95

96 / APPENDIX B
This ordering allows flexibility in expanding solutions to the
Boltzmann equation as a sequence of physical perturbative approxi-
mations. It is clear that many atomic collisions (�106) occur in a
centimeter of ordinary matter but transferring little energy per colli-
sion, whereas �103 nuclear coulomb elastic collisions occur per centi-
meter but with significant energy transfer. In distinction, nuclear
reactions are separated by a fraction to many centimeters depending
on energy and particle type but with large energy transfers. Atomic
interactions are treated with an energy moments expansion in which
the first term is related to LET and higher order moments are related
to range straggling. The secondary electrons form the energy deposit
around the ion path. The elastic scattering is treated as lateral
diffusion. Special problems arise in the perturbation approach for
neutrons for which �i,at(E) � 0, and the nuclear elastic process
appears as the first-order perturbation. The neutron-coupling prob-
lem has been the recent focus of research (Clowdsley et al., 2000)
and further described below along with the reactive processes.
The double differential particle production and fragmentation
cross sections [�ik(�,��,E,E�)] of Equation B.1 are separated into
an isotropic contribution and a remainder as:
� � �F � �iso , (B.6)
where the remainder �F consists of only forward directed secondary
particles and �iso is dominated by lower energy particles produced
in the reaction. The low-energy charged particles are of short range
due to atomic interaction processes and may be solved analytically
(Wilson et al., 1991) but the low-energy neutrons have no atomic
interactions and require a different solution technique (Clowdsley
et al., 2000). The solution to Equation B.1 can likewise be separated
into two parts for which �F appears only in Equation B.1 with solution
&F and a second equation in which �iso appears in Equation B.1 but
with source terms from coupling to the &F field through �iso. The
solution to Equation B.1 for &F can be written in operational form as:
&F � GF &B , (B.7)
where &B is the inbound field at the boundary, and GF is the Green’s
function associated with �F, which reduces to a unit operator on
the boundary denoted by '. Standard practice in space radiation
protection replaces ' as required at some point on the boundary and
along a given ray by the corresponding 'N evaluated for normal
incidence (N) on a semi-infinite slab (Wilson et al., 1994). The errors
in this approximation are made only for the &F field and are second
order in the ratio of beam divergence and radius of curvature of the
object, rarely exceed a few percent for space radiations, and are

COMPUTATIONAL METHODS / 97
always conservative (Wilson et al., 1994). The replacement of ' by
'N as a highly accurate approximation for space applications has the
added advantages that 'N is the natural quantity for comparison
with laboratory experiments and has the following property: if 'N is
known at a plane a distance xo from the boundary (assumed at the
origin), then the value of 'N at any plane x � xo is:
GN(x) � GN(x � xo) GN(xo). (B.8)
Setting x � xo� h, where h is small and of fixed step size gives rise
to highly efficient marching procedure of the radiation transport
code HZETRN (Wilson et al., 1997). Allowing x and xo to take arbi-
trary values gives rise to the nonpertabative solution methods. There
remains the evaluation of the remainder terms �iso of Equation B.1,
especially the low-energy neutron transport.
The remainder of Equation B.1 following the separation given by
Equation B.6 is:
� � �&i(x,�,E) � ����iso,ik(E,E�) &k(x,��,E�) d�� dE�)�
� �i(E)&i(x,�,E) � gi(E,x), (B.9)
where the source term [gi(E,x)] results from the collisional �iso source
with the &F field. As mentioned above, the charged particle fields
of Equation B.9 can be solved analytically leaving the low-energy
neutrons fields to be evaluated. Energy multigroup methods are
currently used for evaluation of Equation B.9 for the neutron fields
(Clowdsley et al., 2000). The solution for the diffuse component
depends on the surrounding material and the accumulation of the
neutrons produced in and scattered from the massive material of
human occupied spacecraft is an essential part of solution of the
Boltzmann equation. The diffuse charged particle component is sim-
pler since the atomic interactions tend to dominate in the appropriate
energy range.
The extent of the nuclear interaction cross section database
required for the transport of cosmic rays spans most nuclear-reaction
physics from thermal energies to energies above tens of GeV n�1,
including a large number of projectile and target material combina-
tions. The types of cross sections required for the transport involve
total yields and secondary energy spectra for one-dimensional trans-
port and double differential cross sections in angle and energy for
three-dimensional transport. Fortunately, neutron and proton cross
sections have been studied at some length in the past. Nuclear-
reaction modeling is required, especially for light and heavy ion
projectiles, to understand the basic physical processes, and to extra-
polate the limited, available experimental data between projectile

98 / APPENDIX B
energies and projectile-target combinations. The usual approach to
database generation is the use of Monte Carlo models or hydrody-
namic models with limited usefulness and success. The best approach
has been to develop solution procedures of the basic quantum
mechanics (Cucinotta et al., 1993; Wilson, 1974).
A microscopic theory for the description of nuclear fragmentation is
being developed through the study of the summation of the nucleus-
nucleus, multiple-scattering series for inclusive reactions where a
single reaction species is considered. This approach originated in a
theory for high-energy alpha-particle fragmentation (Cucinotta
et al., 1993) and has been extended to recast the abrasion-ablation
model in microscopic form (Cucinotta and Dubey, 1993). The micro-
scopic theory represents a unified approach where a single formalism
generates all the cross sections required for heavy-ion transport.
The evaluation of the microscopic theory requires the interaction
amplitudes among basic nuclear constituents. The strong interaction
and quantum phase space limitations (Pauli principle) modify the
amplitudes for bound constituents and have important impact on
elastic and reactive processes (Tripathi et al., 1999). Basic nuclear
theory and media modified interaction amplitudes with the optical
theorem can now, for the first time provide high quality total and
reactive cross sections as recently incorporated into the Langley 90
database (Tripathi et al., 1998; 1999) and have been adopted by other
groups and agencies and stand ready for application to the HZE
fragmentation process. A recent blind test in iron fragmentation
experiments of various models has been very encouraging for future
database generation (Cucinotta et al., 1998; Zeitlin et al., 1997).
Appendix C
ThermoluminescenceDosimetry Materials
The more usual TLD materials for passive personal radiation
dosimetry have been reviewed and described by McKeever et al.
(1995). For dosimetry in LEO, two materials have been used most
often, namely, lithium fluoride, doped with magnesium and titanium
(LiF:Mg,Ti) and calcium fluoride, doped with thulium (CaF2:Tm).
C.1 Lithium Fluoride, Doped with Magnesium
and Titanium
Radiation dosimetry-quality lithium fluoride generally comes in
three forms. The differences between them lie in the isotopic abun-
dance of lithium, thus: natural abundance (92.5 percent 7Li and 7.5
percent 6Li), enriched in 6Li (95.5 percent), and enriched in 7Li (99.5
percent). Such detectors are available from a variety of manufactur-
ers. Perhaps the most widely known forms are known as TLD-100�,
TLD-600� and TLD-700�, respectively, using the original trade
names of the old Harshaw Chemical Company (now Saint-Gobain
Industries). Each of these is doped with magnesium, titanium and
hydroxyl impurities. Since 6Li has a large cross section for neutron
interaction, via the reaction 6Li(n,�)3H, then 6Li-enriched versions
(e.g., TLD-600�) are more sensitive to thermal neutrons (below
�1 keV) than either of the other versions (such as TLD-100� or
TLD-700�).
The usual procedure for using LiF TLDs is to anneal the sample at
400 °C for 1 h. This is then followed by either a slow cool to 80 °C, and
a hold at this temperature for 24 h, or a slow cool to 100 °C, and a
hold at this temperature for 2 h (although other similar recipes are
often used) (Furetta and Weng, 1998; Horowitz, 1984b; McKeever,
99

100 / APPENDIX C
1985; McKeever et al., 1995; Niewiadomski, 1993). Reproducible con-
trol of the temperature and the timing of the heating and cooling cycles
are considered to be critical. The purpose of the heating schemes is
two-fold: (1) to reset the defect equilibrium state within the samples
after each use, and (2) to empty charge from stable defects which may
remain after the first irradiation and readout cycle. To ensure stable
resetting of the defect equilibrium the lengthier, but more reliable,
400 °C for 1 h plus 80 °C for 24 h is often recommended (McKeever
et al., 1995).
A typical glow curve for LiF:Mg,Ti (in this case TLD-100�) treated
by annealing at 400 °C for 1 h plus 100 °C for 2 h is shown in
Figure C.1. Although these data were obtained with the faster 400 °C
for 1 h plus 100 °C for 2 h anneal, they serve to demonstrate the
complexity of the glow curve. The sample has been irradiated with
1.5 MeV protons (1.8 � 1010 protons cm�2). The glow curve is a
complex overlap of several individual signals. The figure shows two
methods for deconvoluting the signal into its component parts. No
single deconvolution model has yet been agreed upon for the glow
curve from LiF:Mg,Ti but, nevertheless, the data of Figure C.1 show
the complexity of the glow curve with its multiple components. Glow
curves for other versions of LiF:Mg,Ti (e.g., TLD-600� and TLD-
700�) are similar.
The TL signal corresponding to Peak 5 (Figure C.1) is usually
taken to be the signal of interest. The response of LiF:Mg,Ti to
absorbed dose from gamma rays indicates a linear-supralinear
behavior, with saturation occurring near 103 Gy (McKeever et al.,
1995). Supralinearity of the signal starts at a few gray (McKeever
and Horowitz, 1990). The dose response of this material to all low-
LET (i.e., �10 keV �m�1) radiation is essentially identical to that
of 60Co or 137Cs irradiation. Likewise, the dose responses of other
versions of LiF:Mg,Ti (e.g., TLD-600� and TLD-700�) are generally
considered to be similar to that of TLD-100�.
The response of the material to heavier charged particles, however,
changes considerably from that resulting from irradiation with low-
LET irradiation. The increased ionization density around the track
of the incident particle results in a decrease in sensitivity and a
decrease in supralinearity for Peak 5, but with a concomitant
increase in sensitivity and supralinearity for the higher temperature
peaks (i.e., Peaks 6 to 10 in Figure C.1). The change in the shape of
the LiF glow curve as a function of LET of the particle is represented
in the data of Figures C.2 and C.3.
The normal approach for determining the absorbed dose from a
radiation source (photon or particle) using LiF:Mg,Ti dosimeters is
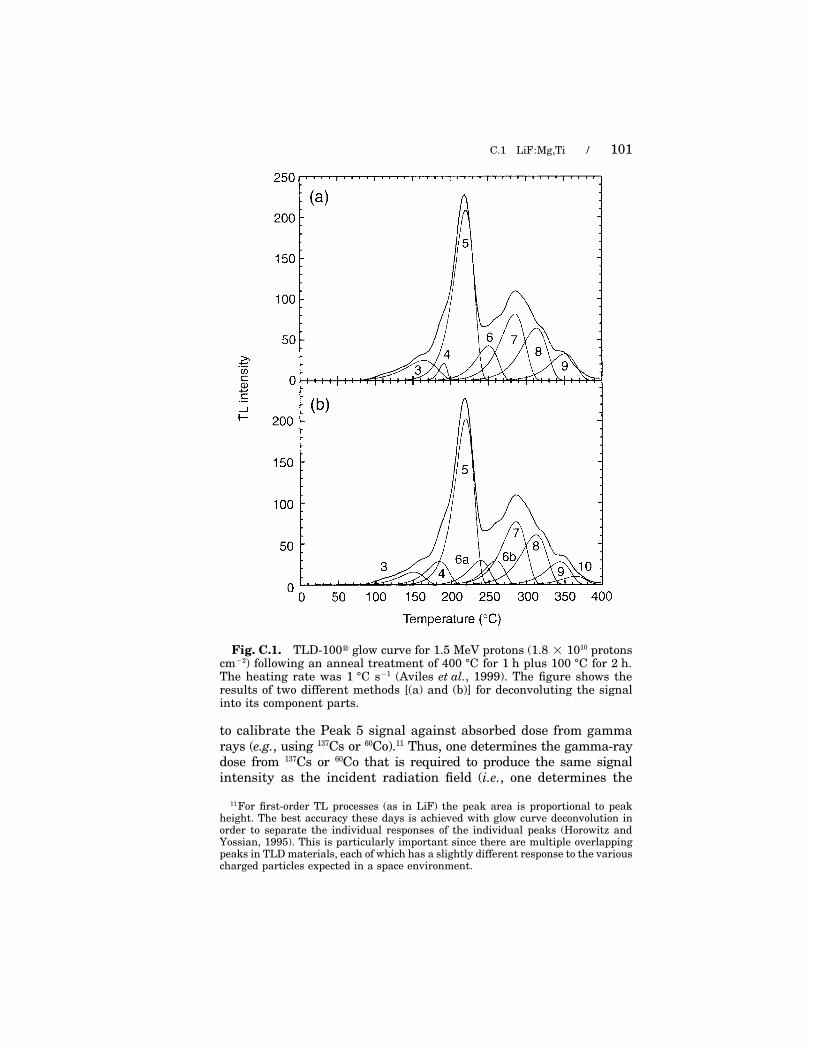
C.1 LiF:Mg,Ti / 101
Fig. C.1. TLD-100� glow curve for 1.5 MeV protons (1.8 � 1010 protonscm�2) following an anneal treatment of 400 °C for 1 h plus 100 °C for 2 h.The heating rate was 1 °C s�1 (Aviles et al., 1999). The figure shows theresults of two different methods [(a) and (b)] for deconvoluting the signalinto its component parts.
to calibrate the Peak 5 signal against absorbed dose from gamma
rays (e.g., using 137Cs or 60Co).11 Thus, one determines the gamma-raydose from 137Cs or 60Co that is required to produce the same signalintensity as the incident radiation field (i.e., one determines the
11 For first-order TL processes (as in LiF) the peak area is proportional to peakheight. The best accuracy these days is achieved with glow curve deconvolution inorder to separate the individual responses of the individual peaks (Horowitz andYossian, 1995). This is particularly important since there are multiple overlappingpeaks in TLD materials, each of which has a slightly different response to the variouscharged particles expected in a space environment.
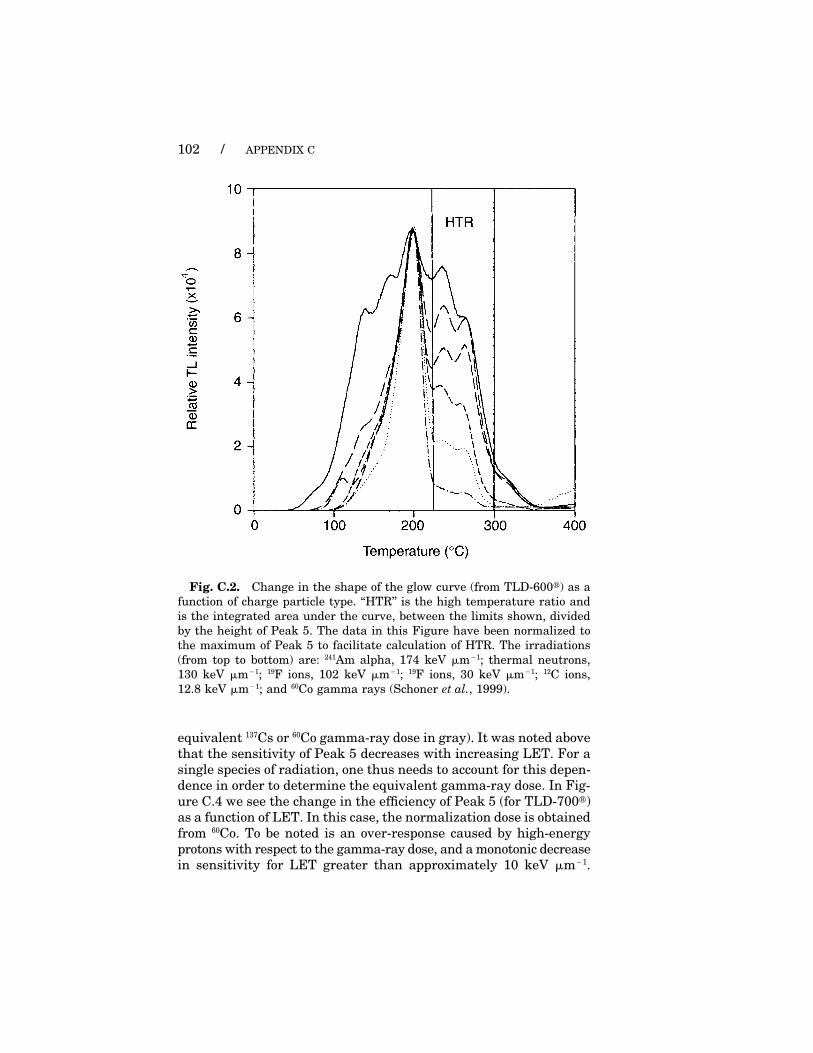
102 / APPENDIX C
Fig. C.2. Change in the shape of the glow curve (from TLD-600�) as a
function of charge particle type. ‘‘HTR’’ is the high temperature ratio and
is the integrated area under the curve, between the limits shown, divided
by the height of Peak 5. The data in this Figure have been normalized to
the maximum of Peak 5 to facilitate calculation of HTR. The irradiations
(from top to bottom) are: 241Am alpha, 174 keV �m�1; thermal neutrons,
130 keV �m�1; 19F ions, 102 keV �m�1; 19F ions, 30 keV �m�1; 12C ions,
12.8 keV �m�1; and 60Co gamma rays (Schoner et al., 1999).
equivalent 137Cs or 60Co gamma-ray dose in gray). It was noted above
that the sensitivity of Peak 5 decreases with increasing LET. For a
single species of radiation, one thus needs to account for this depen-
dence in order to determine the equivalent gamma-ray dose. In Fig-
ure C.4 we see the change in the efficiency of Peak 5 (for TLD-700�)
as a function of LET. In this case, the normalization dose is obtained
from 60Co. To be noted is an over-response caused by high-energy
protons with respect to the gamma-ray dose, and a monotonic decrease
in sensitivity for LET greater than approximately 10 keV �m�1.

C.1 LiF:Mg,Ti / 103
Fig. C.3. High temperature ratio (HTR) plotted against LET (L�) for
TLD-100� (●), TLD-600� (�), and TLD-700� (�) (Schoner et al., 1999).
Similar data have been published elsewhere (e.g., Horowitz, 1984b;
McKeever, 1985; Yasuda and Fujitaka, 2000). The proton over-
response indicated in Figure C.4 is �10 percent, which is about
the same as that reported elsewhere (Horowitz, 1984b; Yasuda and
Fujitaka, 2000). However, larger over-responses have been reported
[e.g., Schoner et al. (1999) report a proton over-response of �20 percent].Benton et al. (2000) define the efficiency function �(L) in three
regions of LET, thus:
�(L) � 1, (C.1a)
for L � 2 keV �m�1;
�(L) � a1 � b1(log L) � c1(log L)2, (C.1b)
for 2 � L � 50 keV �m�1; and
�(L) � a2 � b2(log L) � c2(log L)2, (C.1c)
for L � 50 keV �m�1;

104 / APPENDIX C
[ ]
L
L
Fig. C.4. Response of Peak 5 from TLD-600� and TLD-700� to dose-
averaged LET (Equation C.1). The response is normalized to 60Co gamma
rays, and is therefore defined as the TL efficiency [�(L)] with respect to 60Co
(adapted from Benton et al., 2000).
where a1 � 0.9650, b1 � 0.1805, c1 � 0.2100, a2 � 1.7536, b2 �
0.8060, and c2 � 0.1016. This ignores the proton overresponse at low-
LET. From the available published data the conclusion is reached
that this material does indeed overrespond to high-energy protons.
However, some of the data are equivocal, and the extent of the over-
response is not clear, differing by several percent from report to report.
Important issues include the precise batch of LiF used, the exact
annealing conditions used (temperatures, duration, cooling rates, etc.)
and the region of interest used in the determination of the TLD
response (i.e., integration between temperature X and Y, peak height
calculation, etc.) and, of course, the reliability of the dosimetry in the
individual reports.
Since the detailed TLD response is a function of the pattern of
energy deposition around the particle track (i.e., the track structure),

C.2 CaF2:Tm / 105
the precise behavior will be dependent upon both particle energy (E)
and particle charge (Z). In particular, the radius of the track
increases as Z increases and thus two particles having the same E
but different Z are not expected to produce the same value of �(L).
Data by Avila et al. (1999) and Geiss et al. (1998) on the efficiency
of TL from LiF:Mg,Ti for several particles as a function of both E
and Z illustrate the difficulty of providing a simple correction for
the E,Z-dependence. An effective means to deal with this through
calibration of TLDs for each particle type is not trivial since the
number of different types of charged particle in the space radiation
field is too large. However, an algorithm to calculate the efficiency
(�) as functions of both E and Z is described by Geiss et al. (1998)
and this may prove to be a promising approach.
For space flight, particles of Z � 26 are of less importance (Benton
et al., 2000). Also to be noted is a reported ‘‘non-universality’’ of
�(L) for a given material (Horowitz, 1984b). Variations in the defect
structure (impurity content, defect equilibrium, etc.) lead to varia-
tions in the exact shape of the �(L) curve. Reproducibility in the
heating and cooling cycles during annealing is considered essential
and calibration of each TLD batch may be necessary in critical
situations.
C.2 Calcium Fluoride, Doped with Thulium
Calcium fluoride comes in several forms for use in TL dosimetry,
but the form of interest for space dosimetry applications is CaF2:Tm,
known as TLD-300�. The material is generally considered to be
reusable without any thermal annealing treatments if used for
absorbed doses �200 mGy, although annealing at �400 °C for at
least 30 min is recommended for low-dose (�30 mGy) applications
(McKeever et al., 1995).
The TLD-300� glow curve is shown in Figure C.5. As with LiF,
the glow curve consists of multiple overlapping peaks. The main
signals used in dosimetry are Peak 3, and Peaks (5 � 6) together
(Figure C.5b). The gamma-ray dose response shows linear behavior
for Peak 3 up to �10 Gy, followed by saturation. Peak 5, however,
shows linearity up to �1 Gy, followed by supralinearity, with maxi-
mum supralinearity at �105 Gy. This difference in behavior in the
responses of Peaks 3 and 5 to gamma-ray dose results in a markedly
different behavior for charged-particle irradiation. Specifically, the
ratio of Peaks (5 � 6) to Peak 3 increases with increasing LET, as
Figure C.6 illustrates for the TLD-300� glow curve after irradiation
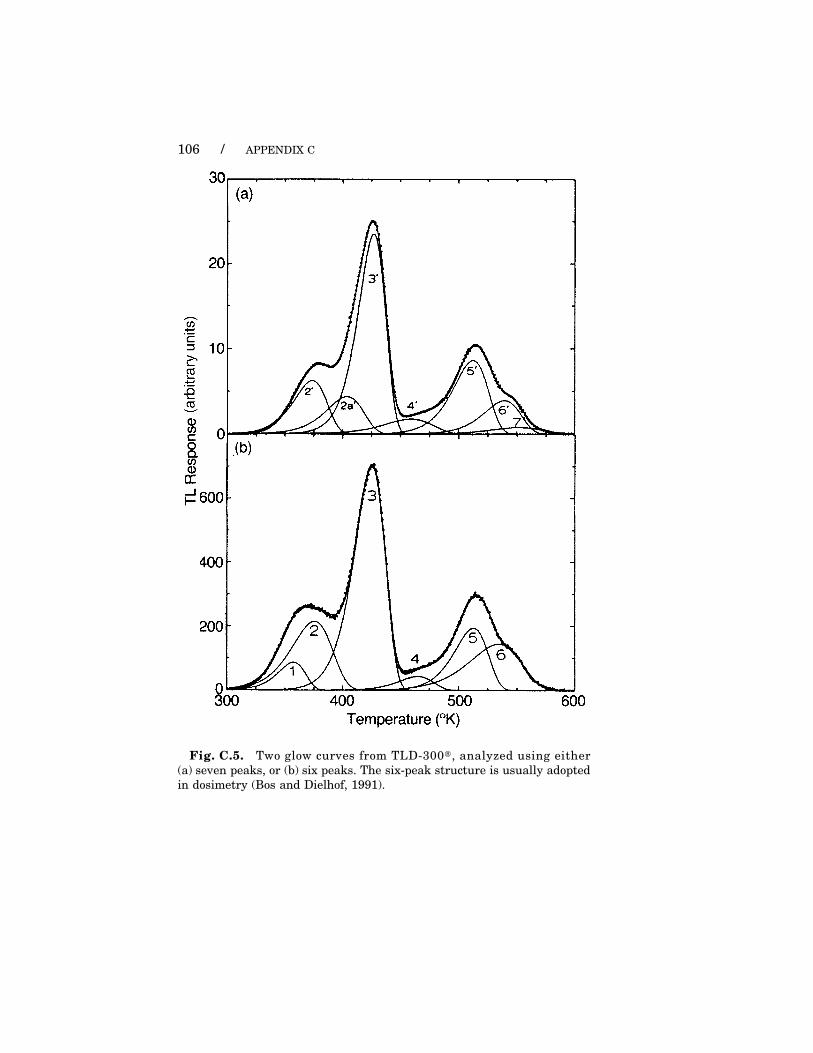
106 / APPENDIX C
Fig. C.5. Two glow curves from TLD-300�, analyzed using either
(a) seven peaks, or (b) six peaks. The six-peak structure is usually adopted
in dosimetry (Bos and Dielhof, 1991).
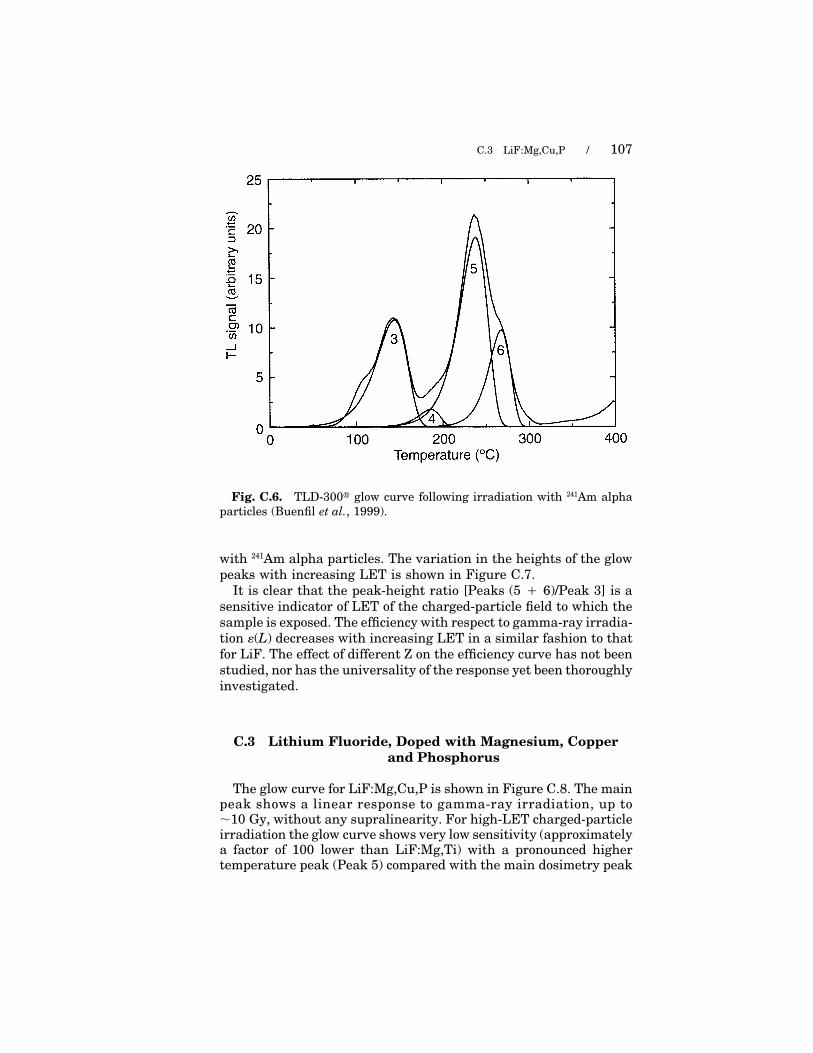
C.3 LiF:Mg,Cu,P / 107
Fig. C.6. TLD-300� glow curve following irradiation with 241Am alpha
particles (Buenfil et al., 1999).
with 241Am alpha particles. The variation in the heights of the glow
peaks with increasing LET is shown in Figure C.7.
It is clear that the peak-height ratio [Peaks (5 � 6)/Peak 3] is a
sensitive indicator of LET of the charged-particle field to which the
sample is exposed. The efficiency with respect to gamma-ray irradia-
tion �(L) decreases with increasing LET in a similar fashion to that
for LiF. The effect of different Z on the efficiency curve has not been
studied, nor has the universality of the response yet been thoroughly
investigated.
C.3 Lithium Fluoride, Doped with Magnesium, Copper
and Phosphorus
The glow curve for LiF:Mg,Cu,P is shown in Figure C.8. The mainpeak shows a linear response to gamma-ray irradiation, up to�10 Gy, without any supralinearity. For high-LET charged-particleirradiation the glow curve shows very low sensitivity (approximatelya factor of 100 lower than LiF:Mg,Ti) with a pronounced highertemperature peak (Peak 5) compared with the main dosimetry peak

108 / APPENDIX C
Fig. C.7. Variation in the heights of Peaks 3 and 5, normalized to the
heights of these peaks after 60Co gamma-ray irradiation, for various heavy
charged particles (HCP) (RHCP/RCo-60). The arrows indicate the entrance and
exit LET values for the particles indicated. (�) helium ions, () neon ions,
(�) 0.7 MeV protons, () 5.3 MeV alpha particles, (●) 120 MeV 12C ions. The
maximum fluence was 1011 particles cm�2 (Buenfil et al., 1999).
(Peak 4 in Figure C.8.) The low sensitivity is a result of the microdosi-metric distribution of trapped charge along the track of the chargedparticle and the rapid saturation of the TL signal at high ionizationdensities (Horowitz and Stern, 1990). The sensitivity to gamma raysand low-LET irradiations, however, is considerably higher than thatof LiF:Mg,Ti. Thus, this material acts as an efficient discriminatorin mixed low- and high-LET fields. However, a detailed study of the�(L) function for this material has not yet been performed.
C.4 Aluminum Oxide, Doped with Carbon
Figure C.9 shows the glow curve for Al2O3:C irradiated by gammarays. The main peak shows a linear response to gamma-ray irradi-ation, up to �50 Gy, without any significant supralinearity. The
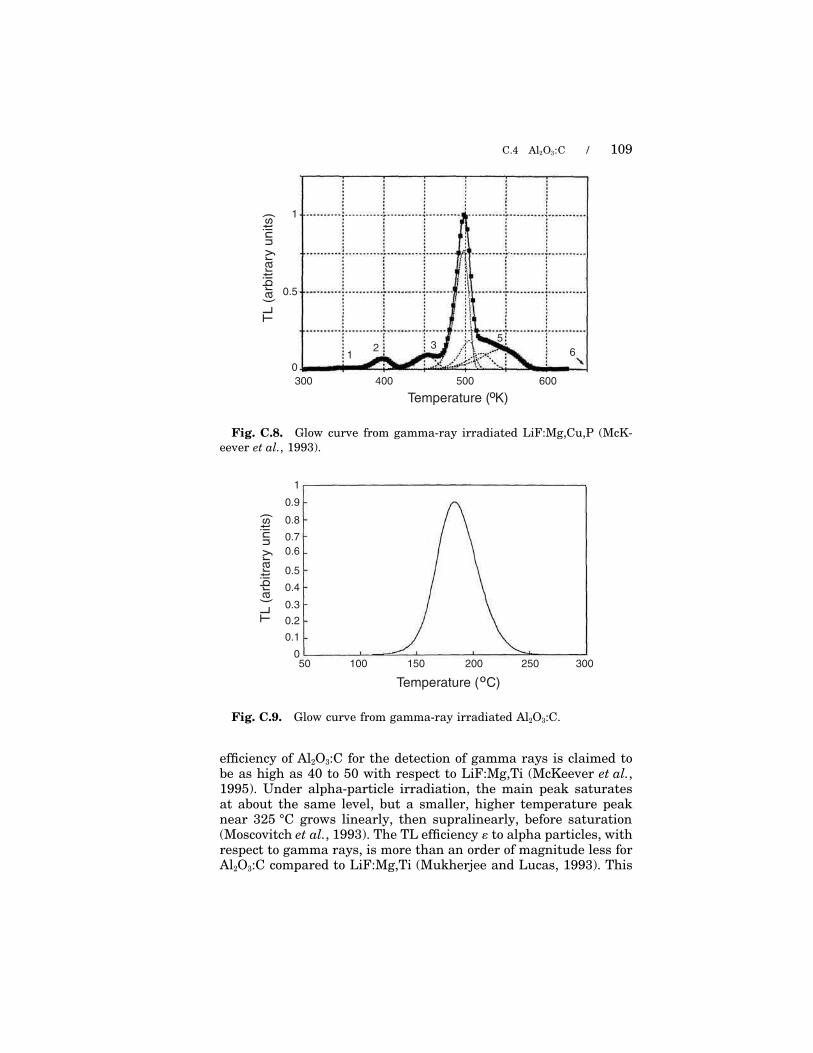
C.4 Al2O3:C / 109
TL (
arb
itra
ry u
nits) 1
0.5
Temperature ( K)
300 400 500 600
6
532
01
º
Fig. C.8. Glow curve from gamma-ray irradiated LiF:Mg,Cu,P (McK-
eever et al., 1993).
TL
(a
rbitra
ry u
nits)
0.5
0.9
0.8
0.7
0.6
0.4
0.3
0.2
0.1
0100 150 200 250 30050
1
Temperature ( C) º
Fig. C.9. Glow curve from gamma-ray irradiated Al2O3:C.
efficiency of Al2O3:C for the detection of gamma rays is claimed tobe as high as 40 to 50 with respect to LiF:Mg,Ti (McKeever et al.,1995). Under alpha-particle irradiation, the main peak saturatesat about the same level, but a smaller, higher temperature peaknear 325 °C grows linearly, then supralinearly, before saturation(Moscovitch et al., 1993). The TL efficiency � to alpha particles, withrespect to gamma rays, is more than an order of magnitude less forAl2O3:C compared to LiF:Mg,Ti (Mukherjee and Lucas, 1993). This

110 / APPENDIX C
is consistent with the differences observed in the gamma-ray dose
response and suggests that this material (like LiF:Mg,Cu,P) would
be very effective at discriminating against high-LET particles in
mixed low-LET/high-LET fields.
A disadvantage of Al2O3:C for TL dosimetry is an observed heating
rate dependence due to thermal quenching of the luminescence effi-
ciency (Akselrod et al., 1998). This disadvantage can be overcome,
however, by using this material as an OSLD instead of a TLD. Here
one measures the radiation-induced luminescence signal using light
from a laser beam to stimulate the luminescence. Several OSL read-
out modes have been suggested and successfully developed (Akselrod
and McKeever, 1999; Botter-Jensen et al., 1997).
A complete description of �(L), using either TL or optically stimu-
lated luminescence, for this material is not yet available.
C.5 Evaluation of Absorbed Dose and Dose Equivalent
C.5.1 Equivalent Gamma-Ray Dose
For a linear growth of a TL signal with gamma-ray dose (from60Co or 137Cs):
TL � D, (C.2)
where is a proportionality constant describing the efficiency of TL
production for gamma-ray irradiation (in TL units per unit gamma-
ray dose). For linear growth of TL with absorbed dose from a particle
with linear energy transfer L:
TLL � � D, (C.3)
with � � 1.
For a mixed particle field of fluence &(L), the delivered absorbed
dose to TLD is �D(L)dL, summed over all angles and all times. Here,
D is the absorbed dose delivered to TLD by particles of linear energy
transfer L and is a function of L. Thus:
TLL � � �(L) D(L) dL. (C.4)
The desired quantity at this stage is D � �D(L) dL. The difficulty
is that TLL is a single number whereas �(L) and D(L) are functions.
Thus, the problem is ‘‘ill-posed.’’ The simplest, and least satisfactory,
solution is to determine that gamma-ray dose which gives rise to
the same TL signal as that due to the particle irradiation. That is,

C.5 EVALUATION OF ABSORBED DOSE / 111
one uses D for the absorbed dose in TLD due to the charged-particle
field, where:
D � � �(L) D(L) dL. (C.5)
C.5.2 Mean, or Effective, Linear Energy Transfer
An improved approach is to independently measure the LET flu-
ence spectrum [&(L)] and obtain an effective efficiency (�) determined
from either a mean or an effective LET (Li) suitably averaged over
some i. For example, from the known &(L) one can obtain a dose-
averaged LET, thus:
LD �� D(L) L dL
� D(L) dL, (C.6)
or a fluence-averaged LET, thus:
L& �� &(L) L dL
� &(L) dL. (C.7)
One can use the value of Li to determine � from an experimentally
measured function �(L) for the specific TLD being used. Alterna-
tively, one can define a mean efficiency from:
� �� �(L) D(L) dL
� D(L) dL, (C.8)
using an experimentally measured �(L) curve (e.g., Figure C.4).
Using �, one then approximates Equation C.5, thus:
D � � �(L) D(L) dL � � � D(L) dL, (C.9)
and obtains the equivalent gamma-ray dose delivered by the particle
field from:
D �D
�. (C.10)
An effective LET for TL can also be evaluated using either the
LiF or CaF2 glow curves. Since the TL glow curve from a mixed
particle field can be viewed as the superposition of TL glow curves
due to individual particles [i.e., TL � � TL(L) dL] then one may use,
for example, the LiF (TLD-100�) glow curve to determine the HTR
value for the mixed particle space radiation field and compare this
with Figure C.3 to arrive at an ‘‘effective’’ LET (LTLD) (Schoner et al.,

112 / APPENDIX C
1999; Vana et al., 1996). The glow curve from CaF2 (TLD-300�)
(Figure C.7) can be used in the same way. A question arises, however,
concerning how well the effective LET calculated in this way com-
pares with the mean LET calculated using Equations C.6 or C.7.
Yasuda and Fujitaka (2000) demonstrate considerable differences
between LTLD and LD (4.6 and 14 keV �m�1, respectively) using a
typical space radiation field spectrum as estimated from data from
a TEPC (Badhwar et al., 1996a). Nevertheless, using an effective
LET value determined in this way, one can also determine an effec-
tive efficiency �TLD from the known �(L) function and estimate the
equivalent gamma-ray dose using Equation C.9.
C.5.3 Dose Equivalent
The quantity of interest is H (in sievert) determined from:
H � Q D. (C.11)
Q is a function of LET and for a spectrum of charged particles in a
mixed particle field:
H � � Q(L) D(L) dL. (C.12)
Using the calculated equivalent gamma-ray dose in TLD (Equation
C.9), H can be approximated by:
Hi � Qi � D(L) dL � Qi D � Qi
D
�, (C.13)
where the subscript i refers to either D (dose-averaged) or & (fluence-
averaged), and Qi can be determined from ICRP (1991) using the
mean or effective LET value (Li) determined from one of the above
methods.12
12 From an analysis based on photon interaction coefficients, tabulations of electron
and proton stopping powers, and data on muon stopping powers, it is concluded that
for a 137Cs calibration in terms of tissue kerma, the TLDs (LiF) will give an estimate
of absorbed dose to a small mass of tissue for all low-LET components to within five
percent. The energy ranges taken into account include the majority of the low-LET
contributions to dose—for photons up to 10 MeV there would be less than a five
percent overestimate; for electrons up to 50 MeV, an estimate within two percent;
for protons from a few MeV up to 2 GeV an estimate within two percent if only coulomb
interactions are considered; for the cosmic radiation secondary muon spectrum, there
would be an underestimate of about five percent. In these calculations, it was assumed
that the relative light conversion efficiencies for energy deposition by these radiations
in the 7LiF:Mg,Ti remained close to unity (Bartlett et al., 2000).

C.5 EVALUATION OF ABSORBED DOSE / 113
Using the TEPC fluence data of Badhwar et al. (1996a) one gets
QTLD � 1.3 if one uses LTLD from the LiF HTR method, or QD � 2.5
if one uses LD calculated directly from the TEPC data (Yasuda and
Fujitaka, 2000). However, difficulties with such comparisons arise
if there is a significant neutron component and if LiF has a low
response to these components, and/or there is a different secondary
charged-particle spectrum compared to that in tissue.
Yasuda (2001) combined LET dependencies of the low temperature
and high temperature TL peaks from TLD-700� to provide a function
�HL(L) to mimic the Q(L) function and thereby calculate H from:
H � (1 � ) XHT � XLT, (C.14)
when
�HL(L) � ( � 1) �HT (L) � �LT (L), (C.15)
where �HL (L) and �LT(L) are the TL efficiencies of the high tempera-
ture (HT) and low temperature (LT) peaks, respectively; XHT and XLT
are the TL values for the high temperature and low temperature
TL glow peaks, respectively; and is an empirically determined
constant selected to satisfy the relationship �HL(L) � Q(L) over the
entire range of L. There are difficulties associated with this approach
if there is a significant neutron component of the radiation field.
An alternate approach is to limit the use of TLDs to the measure-
ment of absorbed dose from the low-LET (�10 keV �m�1) region for
which Q � 1. In this region, H � QD � D. To do so one needs to
employ a TLD material with excellent discrimination between high-
and low-LET particles. As already described, LiF:Mg,Cu,P or Al2O3:C
may be suitable, but LiF:Mg,Ti or CaF2:Tm would be unsuitable.
One should still take account of differences between absorbed dose
to TLD and absorbed dose to tissue.
To determine H from the high-LET region of the incident field
spectrum one could use a PNTD. Thus, if information is available
about the LET spectrum &(L), then one can calculate H from
H � � D(L) Q(L) dL (Appendix D) and the total H would then be
given by a combination of TLDs and PNTDs, thus:
H � (DQ)TLD � �� D(L) Q(L) dL�PNTD
(C.16)
To provide the best discrimination between the low- and high-LET
regions of the incident spectrum, PADC/CR-39� would be a suitable

114 / APPENDIX C
PNTD material. Since there would be some overlap between the
two detectors each device (TLD and PNTD) would have to be fully
characterized as a function of LET and corrections made to avoid
‘‘double counting’’ the absorbed dose in the overlapping region.
Appendix D
Plastic Nuclear TrackDetectors
D.1 Description of Method
PNTDs register charged particles by means of etchable damage
to the detector structure. The damage trail in a material, which
constitutes a charged-particle track, is a result of local deposition of
energy during the passage of the particle and as such may be related
to restricted LET (L�) or to lineal event density (Paretzke, 1977) or
to radial dose (Butts and Katz, 1967) (see also discussion of Paretzke,
1982). The damage is generally permanent but may be partly
repaired or may be modified over time, influenced by factors such
as temperature, humidity, and the local presence of oxygen or other
gases. The particle tracks, the damage ‘‘trails,’’ may be viewed
directly with an electron microscope in some instances (Price and
Walker, 1962; Silk and Barnes, 1959) or may be rendered visible
under an optical microscope by etching with a suitable solvent
(Young, 1958). The track is developed to form a pit of approximately
conical shape by the preferential dissolution along the particle track,
with the condition that the track etch rate vT is greater than the
bulk etch rate vB. The resulting conical etched pits have entrance
diameters in the range of a few tenths to a few tens of microns. For
an observable track to be formed vT /vB must exceed some threshold
value and this in turn is related to L� or similar parameter of the
particle. The value of vT /vB will also determine the maximum ‘‘accep-
tance’’ angle of incidence for tracks to be made visible. For different
particle parameters, the different values of vT will result in different
evolutions of the etched pit shape with time of etching for a given
set of etchant parameters (chemical composition, molarity and tem-
perature). The measurement of the dimensions of etched pits and
their dependence on etching time allows an estimation to be made
115

116 / APPENDIX D
of the charged particle’s L� and residual range, and, not always
unambiguously, allows identification of particle charge and energy.
Stacks of thin sheets of detector material are used to trace the paths
of particles. An introduction to the more general study of track etch-
ing and its many applications may be found, for example, in Durrani
and Bull (1987) and Fleischer et al. (1975).
D.2 Neutron Dosimetry
Until the late 1970s, neutron detection using PNTDs was only
possible by means of (n,�) or (n,f) reactions and for neutron energies
above about 1.5 MeV by the detection of recoil nuclei. The situation
changed with the discovery of the proton response of the commonly
used plastic, PADC/CR-39�13 (Cartwright et al., 1978; Cassou and
Benton, 1978). Other track etch materials, notably some forms of
cellulose nitrate are also able to register protons, but with low sensi-
tivity. Depending on the etch process used, protons of energies up
to about 10 MeV may be detected by PADC/CR-39�, corresponding
to LETs (in water) down to about 5 keV �m�1.
The application of PADC/CR-39� to neutron personal dosimetry
was recognized and demonstrated by several authors (Al-Najjar
et al., 1979; Benton et al., 1980; Griffith et al., 1981; Ruddy et al.,
1981; Somogyi and Hunyadi, 1980). The addition of a converter layer
for the neutron energy region from thermal to a few kiloelectron
volts (Bartlett et al., 1986) produces a dosimeter with acceptable
energy dependence of response for most practical purposes. The early
widespread application however, was hampered by problems of plas-
tic consistency. There have been recent improvements in the methods
of material manufacture (Ahmad and Stejny, 1991).
For neutron dosimetry applications, the counting of low track den-
sities can be accomplished for etched tracks in thin films by rapid
readout techniques using highly colored detector films or electroni-
cally by the development of spark counting. The process of electro-
chemical etching (Sohrabi, 1974; Tommasino, 1970; Tommasino and
Armellini, 1973) greatly increases the size of the etched pits such
that they are visible to the unaided eye and can be counted automati-
cally by simple low-power optical systems. In electrochemical etching,
13 Polyallyl diglycol carbonate is the polymeric form of allyl diglycol carbonate, which
is the commercial name for the chemical diethylene glycol bis (allyl carbonate), also
known as 2,2�oxydiethylene bis (allyl carbonate) or as the oxydi-2, 1-ethanedyl d-2-
propanyl diester of carbonic acid.

D.3 DOSIMETRY OF COSMIC RADIATION FIELDS / 117
a high alternating electric field is applied across the detector foil
during chemical etching. The field strengths are typically in the
range of 20 to 50 kVRMS cm�1 at frequencies in the range 50 Hz to
10 kHz. For pits, which attain a sharply pointed shape as the chemi-
cal etching proceeds, the field strength is enhanced at the tip and
local breakdown of the material leads to catastrophic damage. The
characteristic ‘‘tree’’ shaped formation produced has a diameter in
the range of 10 to several hundred microns compared to chemically-
etched pit diameters of a few tenths to a few tens of microns. The
electrochemically-etched pits are visible to the naked eye and can
be counted by simple automated low magnification optical systems.
A variation on this process is electro-etching, or ‘‘blow up’’; in which
small pits which have been produced by chemical etching, or rela-
tively underdeveloped pits produced by low-frequency electric field
electrochemical etching, or a combination of both, are subjected to
a short accelerated high-frequency electro-etch. Electrochemical
etching is sometimes preceded by a short chemical etch.
Detailed descriptions of fundamental aspects of neutron dosimetry
using PNTDs, including information on the different etch processes
and dosimetric characteristics may be found in two review papers
(Harrison and Tommasino, 1985; Tommasino and Harrison, 1985),
and in a recent survey of the status of development in Europe (Harvey
et al., 1998).
D.3 Dosimetry of Cosmic Radiation Fields
PNTDs, in particular, PADC/CR-39�, can be used to determine the
neutron and HZE components, and, in part, the proton component of
the cosmic radiation field in spacecraft. The material type, and in
some cases the batch, needs to be calibrated (see calibration curves,
adapted from Keegan, 1996, Figure D.1) either for a sample from
the batch used, or by a combination of an a priori calibration curve
for a material plus an in-flight self-calibration (Gunther et al., 1999;
Wiegel et al., 1988). The in-flight self-calibration takes account of
changes in sensitivity of the detector owing to flight conditions. Full
etch track analysis allows the determination of HZE particle fluence
and fluence rate, but is extremely time consuming unless automated.
The LET threshold of PADC/CR-39� is in the range 5 to 10 keV �m�1,
enabling protons of energy up to about 10 MeV to be detected directly,
as well as HZE particles. Secondary charged particles from nuclear
(strong force) interactions of higher energy protons and of neutrons,
in the detector material itself or surrounding material, are also
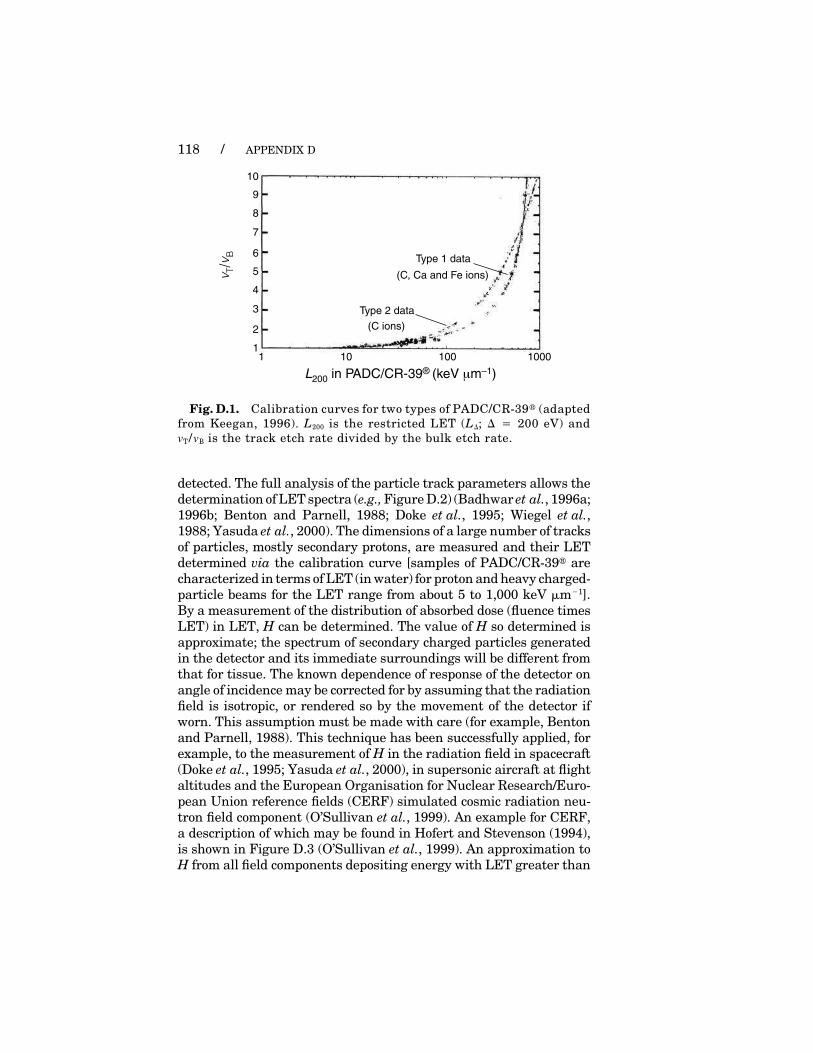
118 / APPENDIX D
vT/ v
B
10 100 10001
2
1
3
4
5
6
7
8
9
10
L200 in PADC/CR-39® (keV µm–1)
Type 2 data
Type 1 data
(C, Ca and Fe ions)
(C ions)
Fig. D.1. Calibration curves for two types of PADC/CR-39� (adapted
from Keegan, 1996). L200 is the restricted LET (L�; � � 200 eV) and
vT /vB is the track etch rate divided by the bulk etch rate.
detected. The full analysis of the particle track parameters allows the
determination of LET spectra (e.g., Figure D.2) (Badhwar et al., 1996a;
1996b; Benton and Parnell, 1988; Doke et al., 1995; Wiegel et al.,
1988; Yasuda et al., 2000). The dimensions of a large number of tracks
of particles, mostly secondary protons, are measured and their LET
determined via the calibration curve [samples of PADC/CR-39� are
characterized in terms of LET (in water) for proton and heavy charged-
particle beams for the LET range from about 5 to 1,000 keV �m�1].
By a measurement of the distribution of absorbed dose (fluence times
LET) in LET, H can be determined. The value of H so determined is
approximate; the spectrum of secondary charged particles generated
in the detector and its immediate surroundings will be different from
that for tissue. The known dependence of response of the detector on
angle of incidence may be corrected for by assuming that the radiation
field is isotropic, or rendered so by the movement of the detector if
worn. This assumption must be made with care (for example, Benton
and Parnell, 1988). This technique has been successfully applied, for
example, to the measurement of H in the radiation field in spacecraft
(Doke et al., 1995; Yasuda et al., 2000), in supersonic aircraft at flight
altitudes and the European Organisation for Nuclear Research/Euro-
pean Union reference fields (CERF) simulated cosmic radiation neu-
tron field component (O’Sullivan et al., 1999). An example for CERF,
a description of which may be found in Hofert and Stevenson (1994),
is shown in Figure D.3 (O’Sullivan et al., 1999). An approximation to
H from all field components depositing energy with LET greater than

D.3 DOSIMETRY OF COSMIC RADIATION FIELDS / 119
Inte
gra
l N
um
be
r F
Iux (
cm
–2 s
r –1d
–1)
L∞ in tissue (keV µm-1)
105
104
103
102
101
100
10–1
10–2
10–3
10–4
10–1 100 101 103102
10–4
105
104
102
103
101
100
10–1
10–2
10–3
104
Fig. D.2. LET (L�) spectrum for PADC/CR-39� compared with that
obtained with TEPC (adapted from Badhwar et al., 1996a).
Fig. D.3. Integral dose equivalent as a function of LET (L�) for CERF
top concrete neutron field, using Q(L) from ICRP (1991) (adapted from
O’Sullivan et al., 1999).
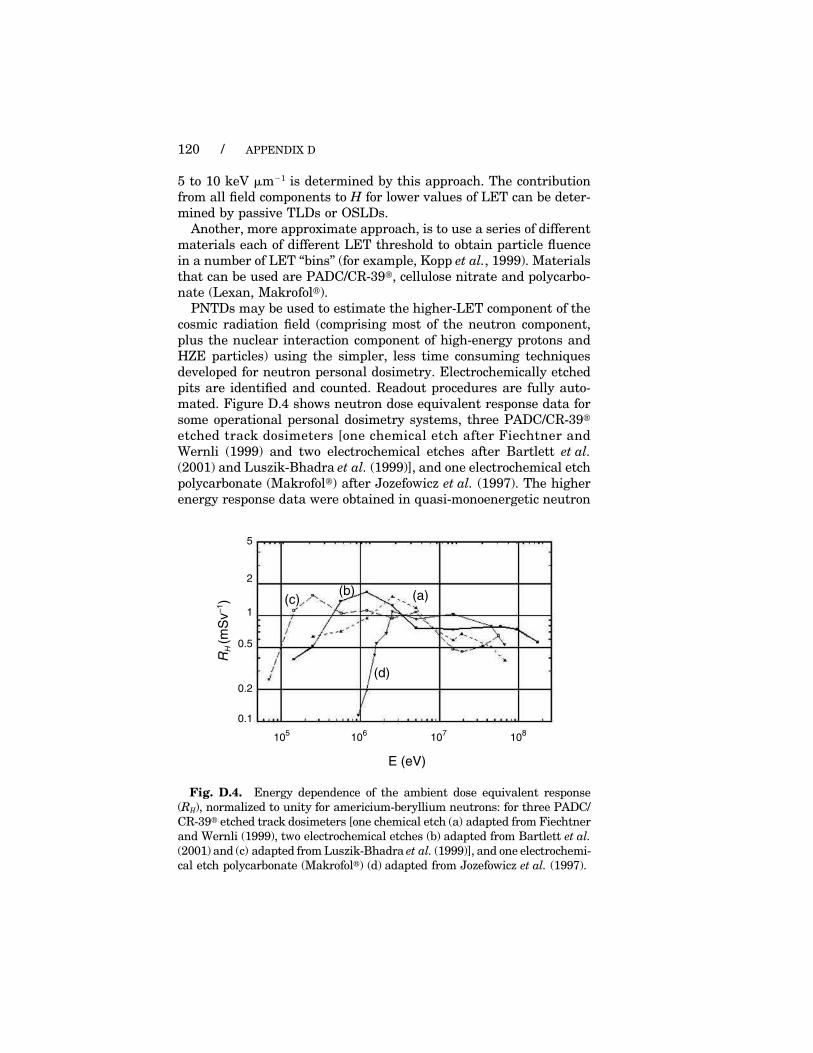
120 / APPENDIX D
5 to 10 keV �m�1 is determined by this approach. The contribution
from all field components to H for lower values of LET can be deter-
mined by passive TLDs or OSLDs.
Another, more approximate approach, is to use a series of different
materials each of different LET threshold to obtain particle fluence
in a number of LET ‘‘bins’’ (for example, Kopp et al., 1999). Materials
that can be used are PADC/CR-39�, cellulose nitrate and polycarbo-
nate (Lexan, Makrofol�).
PNTDs may be used to estimate the higher-LET component of the
cosmic radiation field (comprising most of the neutron component,
plus the nuclear interaction component of high-energy protons and
HZE particles) using the simpler, less time consuming techniques
developed for neutron personal dosimetry. Electrochemically etched
pits are identified and counted. Readout procedures are fully auto-
mated. Figure D.4 shows neutron dose equivalent response data for
some operational personal dosimetry systems, three PADC/CR-39�
etched track dosimeters [one chemical etch after Fiechtner and
Wernli (1999) and two electrochemical etches after Bartlett et al.
(2001) and Luszik-Bhadra et al. (1999)], and one electrochemical etch
polycarbonate (Makrofol�) after Jozefowicz et al. (1997). The higher
energy response data were obtained in quasi-monoenergetic neutron
RH
(m
Sv
–1)
1
2
0.5
0.2
0.1
5
E (eV)
105
106
107
108
(d)
(c)(b) (a)
Fig. D.4. Energy dependence of the ambient dose equivalent response
(RH), normalized to unity for americium-beryllium neutrons: for three PADC/
CR-39� etched track dosimeters [one chemical etch (a) adapted from Fiechtner
and Wernli (1999), two electrochemical etches (b) adapted from Bartlett et al.
(2001) and (c) adapted from Luszik-Bhadra et al. (1999)], and one electrochemi-
cal etch polycarbonate (Makrofol�) (d) adapted from Jozefowicz et al. (1997).

D.3 DOSIMETRY OF COSMIC RADIATION FIELDS / 121
fields at the Paul Scherrer Institute for the neutron energy range 20
to 70 MeV and at 160 and 180 MeV at the Svedberg Laboratory,
Uppsala University. The quasi-monoenergetic fields have about 50
percent of the neutron fluence in the peak and the remainder distrib-
uted in approximately uniform lethargy down to thermal (Blomgren,
1997; Schrewe, 1997).14 The lower energy response must be ‘‘stripped
off’’ to obtain the response for the peak neutrons, a procedure that
results in significant uncertainties in the high-energy response data.
The high-energy response data given in Figure D.4 show reasonable
agreement between four different etched track systems. These data
are also broadly in agreement with those obtained for high-energy
protons (Spurny, 1995). HZE particles will also produce an etchable
track and be counted as if produced by a neutron, or neutron-like
iterations of high-energy protons, and the same response factor
applied (about 5 to 10 �Sv per track for a typical electrochemical etch
system), which will overestimate the HZE component of H. However,
an additional chemical etch allows discrimination.
14Blomgren, J. (1997). Personal communication (Svedberg Laboratory, Uppsala Uni-
versity, Uppsala, Sweden);
Schrewe, U.J. (1997). Personal communication (Physikalisch-Techiseche Bunde-
sanstalt, Braunschweig, Germany).
Glossary
absorbed dose (D): The quotient of d� by dm, where d� is the mean energy
imparted to matter of mass dm, i.e., D � d�/dm. The unit for D is joule
per kilogram (J kg�1) with the special name gray (Gy).
administrative level: A predetermined reference value of a quantity, below
a dose limit, that triggers a specified course of action when the value is
exceeded or is expected to be exceeded. In the case of space activities,
NASA sets administrative levels for a given mission.
albedo neutrons: Secondary neutrons produced by interactions of galactic
cosmic radiation and the atmosphere, and reflected back into space.
as low as reasonably achievable (ALARA): A principle of radiation
protection philosophy that requires that exposures to ionizing radiation
should be kept as low as reasonably achievable, economic and social factors
being taken into consideration. The protection from radiation exposure
is ALARA when the expenditure of further resources would be unwar-
ranted by the reduction in exposure that would be achieved. In the case
of space activities, ALARA applies to actions taken to keep all doses to
the astronauts as low as reasonably achievable, balancing the mission
objectives with practical dose reduction steps.
coronal mass ejection: A transient outflow of plasma from or through
the solar corona, which may be associated with the generation of solar
particle events.
deterministic effects: Effects for which the severity varies with dose and
for which a threshold usually exists, e.g., cataracts and skin burns.
dose: A general term used when the context is not specific to a particular
dose quantity. When the context is specific, the name or symbol for the
quantity is used, i.e., absorbed dose (D), mean absorbed dose (DT), dose
equivalent (H), effective dose (E), equivalent dose (HT), or organ dose
equivalent (HT).
dose equivalent (H): The absorbed dose (D) at a point in tissue, modified
by the quality factor (Q) at that point, i.e., H � QD. The unit for dose
equivalent (H ) is the joule per kilogram (J kg�1) with the special name
sievert (Sv).
dose limit: A limit on radiation dose that is applied for exposure to individu-
als or groups of individuals in order to prevent the occurrence of radiation-
induced deterministic effects or to limit the probability of radiation related
stochastic effects to an acceptable level. For astronauts working in LEO,
unique dose limits for deterministic and stochastic effects have been rec-
ommended by NCRP.
dosimetry records: The collections of information that document the radia-
tion doses that astronauts receive from space flight, mission-related
122

GLOSSARY / 123
aviation activities, mission-related biomedical research, and any other
occupational doses. The dosimetry records contain, or are linked to, all
the basic information that is necessary to obtain the radiation doses.
effective dose (E): The sum over specified tissues of the products of the
equivalent dose in a tissue (HT) and the weighting factor for that tissue
or organ (wT), i.e., E � �T
wTHT. Effective dose (E) applies only to stochastic
effects and is expressed in sievert (Sv).
equivalent dose (HT): The product of the mean absorbed dose in an organ
or tissue (DT) (i.e., DT, R for a given type of radiation R), and the radiation
weighting factor (wR) that accounts for the relative biological effectiveness
of the radiation type. For external exposure, wR applies to the radiation
type incident on the body. When there is more than one type of radiation,
the products are summed, i.e., HT � �R
wR DT,R. For space radiation, applies
only to stochastic effects and is expressed in sievert (Sv).
fluence (&): The quotient of dN by da, where dN is the number of particles
incident on a sphere of cross-sectional area da, i.e., & � dN/da. The unit
for fluence is m�2, commonly given in cm�2. In this Report, distributions
of fluence are also noted variously as a function of one or more other
variables [e.g., &(L,t), the distribution of fluence as a function of LET (L)
and time (t)].
galactic cosmic radiation (GCR): The charged-particle radiation outside
the magnetosphere, which comprise two percent electrons and positrons
and 98 percent nuclei, the latter component consisting (by fluence) of 87
percent protons, 12 percent helium ions, and 1 percent high atomic num-
ber, high-energy (HZE) particles.
gray (Gy): The special name for the unit of absorbed dose (D), kerma and
specific energy imparted, 1 Gy � 1 J kg�1.
gray equivalent (Gy-Eq): The name (NCRP, 2000a) for the unit of the
quantity gray equivalent (GT), 1 Gy-Eq � 1 J kg�1 [see also gray equiva-
lent (GT)].
gray equivalent (GT): The product of DT and Ri, where DT is the mean
absorbed dose in an organ or tissue and Ri is a recommended value for
relative biological effectiveness for deterministic effects for a given particle
type i, i.e., GT � Ri DT. An Ri value applies to the particle type incident
on the body. The dose limits for deterministic effects from space radiation
are given in the quantity GT [see also gray equivalent (Gy-Eq)].
high atomic number, high-energy (HZE) particles: Heavy ions having
an atomic number greater than that of helium (such as nitrogen, carbon,
boron, neon, argon or iron ions that are positively charged) and having
high kinetic energy.
immediate dose management: Actions taken to address the potential for
high doses from transient events in the space radiation environment that
could impact the conduct or completion of the mission or mission tasks.
Immediate dose management actions may be taken to avoid exceeding
administrative levels or dose limits.
lineal energy (y): The quotient of � by �, where � is the energy imparted
to the matter in a given volume by a single (energy deposition) event and

124 / GLOSSARY
� is the mean chord length of that volume, i.e., y � � /�. The unit for lineal
energy is J m�1, commonly given in keV �m�1.
linear energy transfer, unrestricted (L or L�): The quotient of dE by
d�, where dE is the mean energy lost by the particle, due to collisions
with electrons, in traversing a distance d�, i.e., L � dE/d�. The unit for
linear energy transfer is J m�1, commonly given in keV �m�1. Low linear
energy transfer radiations include electrons, x rays, and gamma rays.
High linear energy transfer radiations include alpha particles, heavy ions,
and interaction products of fast neutrons.
mean absorbed dose (DT): The mean absorbed dose in an organ or tissue,
obtained by integrating or averaging absorbed doses at points in the organ
or tissue.
organ dose equivalent (HT): The mean dose equivalent for an organ or
tissue, obtained by integrating or averaging dose equivalents at points in
the organ or tissue. It is the practice in the space radiation protection
community to obtain point values of absorbed dose (D) and dose equivalent
(H ) using the accepted quality factor-LET relationship [Q(L)], and then
to average the point quantities over the organ or tissue of interest by
means of computational models to obtain the organ dose equivalent (HT).
For space radiations, NCRP adopted the organ dose equivalent as an
acceptable approximation for equivalent dose (HT) for stochastic effects.
personal dosimeter: A radiation detection device worn or carried by an
individual to monitor the individual’s radiation exposure. For space activi-
ties, a device worn or carried by an astronaut in-flight.
quality factor (Q): The factor by which absorbed dose (D) at a point is
modified to obtain the dose equivalent (H) at the point, i.e., H � QD, in
order to express the effectiveness of an absorbed dose (in inducing stochas-
tic effects) on a common scale for all types of ionizing radiation. There is
a specified dependence [Q(L)] of the quality factor (Q) as a function of the
unrestricted linear energy transfer (L) in water at the point of interest.
Ri (recommended value for relative biological effectiveness): A best
estimate, for radiation protection purposes, of the relative biological effec-
tiveness for deterministic effects of a given particle type, by which the
mean absorbed dose in an organ or tissue (DT) is modified to obtain gray
equivalent (GT).
radiation safety records: The collections of information that relate to
radiation exposure of the astronauts. The radiation safety records consist
of multiple sources of information that are linked (i.e., the dosimetry
records and their supporting data and files, and other information that
bears on the radiation exposure of astronauts).
radiation weighting factor (wR): A factor used to allow for differences in
the biological effectiveness between different radiations when calculating
equivalent dose (HT) (see equivalent dose). These factors are independent
of the tissue or organ irradiated.
reentrant electrons: Decay products of unstable nuclei produced by the
nuclear interactions of trapped galactic cosmic radiation (GCR) ions.
relative biological effectiveness (RBE): A factor used to compare the
biological effectiveness of absorbed doses from different types of ionizing

GLOSSARY / 125
radiation, determined experimentally. RBE is the ratio of the absorbed
dose of a reference radiation (usually taken as 250 kVp x rays) to the
absorbed dose of the radiation in question required to produce an identical
biological effect in a particular experimental organism or tissue.
sievert (Sv): The special name for the unit of effective dose (E), equiva-
lent dose (HT), dose equivalent (H), and organ dose equivalent (HT),
1 Sv � 1 J kg�1.
solar particle event (SPE): An eruption at the sun that releases a large
number of particles (primarily protons) over the course of hours or days.
splash albedo electrons: Electrons scattered upward by interactions in
the atmosphere.
stochastic effects: Effects, the probability of occurrence which, rather
than their severity, is a function of radiation dose without threshold,
e.g., cancer.
tissue weighting factor (wT): A factor representing the ratio of risk of
stochastic effects attributable to irradiation of a given organ or tissue to
the total risk when the whole body is irradiated uniformly. The factor is
independent of the type of radiation or energy of the radiation.
Acronyms, Abbreviations,and Main Symbols
AE-8 Aerospace Electron Environment, Version 8
(a model of trapped electron radiation)
ALARA as low as reasonably achievable
AP-8 Aerospace Proton Environment, Version 8
(a model of trapped proton radiation)
CERF European Organisation for Nuclear Research/
European Union reference field
D absorbed dose (at a point)
D·
absorbed dose rate (at a point)
DT mean absorbed dose in an organ or tissue
DOELAP U.S. Department of Energy Laboratory
Accreditation Program
E effective dose
E particle energy
EVA extravehicular activity (astronaut in space suit
outside Space Shuttle or ISS)
FISH fluorescence in situ hybridization
f (y) frequency distribution of lineal energy
GT gray equivalent, when used as a quantity
GCR galactic cosmic radiation
Gy-Eq gray equivalent, when used as the name of the
unit for the quantity GT
H dose equivalent (at a point)
HT equivalent dose
HT organ dose equivalent
HRE highly-relativistic electron
HTR high temperature ratio
HZE high atomic number, high-energy
ISS International Space Station
L (or L�) unrestricted linear energy transfer
L� restricted linear energy transferLEO low-Earth orbitLET linear energy transferMir the Russian orbital space stationn�1 per nucleonNVLAP National Voluntary Laboratory Accreditation
Program
126

ACRONYMS, ABBREVIATIONS, AND MAIN SYMBOLS / 127
OSL optically stimulated luminescence
OSLD optically stimulated luminescent dosimeter
PADC/CR-39� polyallyl diglycol carbonate [trade name CR-39
(PPG Industries, Inc., Pittsburgh, Pennsylvania)]
PCC prematurely condensed chromosome
& fluence
PNTD plastic nuclear track detector
PSD position sensitive solid-state detector
Q quality factor
Q(L) quality factor, as a function of linear energy
transfer
Ri recommended value (best estimate) for relative
biological effectiveness of a given particle type i
(deterministic effects)
RBE relative biological effectiveness (experimental)
RHO radiation health officer
RPL radiophotoluminescense
SAA South Atlantic Anomaly
SPE solar particle event
SRAG Space Radiation Analysis Group
t time
TEPC tissue equivalent proportional counter
TL thermoluminescence
TLD thermoluminescent dosimeters
TLD-100� lithium fluoride, doped with magnesium and
titanium (92.5 percent 7Li, 7.5 percent 6Li)
(Bicron, Saint-Gobain Industries, Cleveland,
Ohio)
TLD-300� calcium fluoride, doped with thulium (Bicron,
Saint-Gobain Industries, Cleveland, Ohio)
TLD-600� lithium fluoride, doped with magnesium and
titanium (enriched to 95.5 percent 6Li) (Bicron,
Saint-Gobain Industries, Cleveland, Ohio)
TLD-700� lithium fluoride, doped with magnesium and
titanium (enriched to 99.5 percent 7Li) (Bicron,
Saint-Gobain Industries, Cleveland, Ohio)
y lineal energy
Z atomic number or particle charge (the atomic
number is numerically equal to the electrical
charge on the nucleus of a heavy ion)
References
AHMAD, S. and STEJNY, J. (1991). ‘‘Polymerisation, structure and track
recording properties of CR-39,’’ Nucl. Tracks Radiat. Meas. 19, 11–16.
AKSELROD, M.S. and MCKEEVER, S.W.S. (1999). ‘‘A radiation dosimetry
method using pulsed optically stimulated luminescence,’’ Radiat. Prot.
Dosim. 81, 167–175.
AKSELROD, M.S., AGERSNAP LARSEN, N., WHITLEY, V. and
MCKEEVER, S.W.S. (1998). ‘‘Thermal quenching of F-center lumines-
cence in Al2O3:C,’’ J. Appl. Phys. 84, 3364–3373.
AL-NAJJAR, S.A.R., BULL, R.K. and DURRANI, S.A. (1979). ‘‘Electrochem-
ical etching of CR-39 plastic applications to radiation dosimetry,’’ Nucl.
Tracks 3, 169–183.
AMUNDSON, S.A., DO, K.T., SHAHAB, S., BITTNER, M., MELTZER, P.,
TRENT, J. and FORNACE, A.J., JR. (2000). ‘‘Identification of potential
mRNA biomarkers in peripheral blood lymphocytes for human exposure
to ionizing radiation,’’ Radiat. Res. 154, 342–346.
ANSI (1993). American National Standards Institute. American National
Standard, Criteria for Testing Personnel Dosimetry Systems, ANSI
N13.11-1993 (Health Physics Society, McLean, Virginia).
ANSI (1999). American National Standards Institute. American National
Standard, Practice for Occupational Radiation Exposure Records Systems,
ANSI/HPS N13.6-1999 (Health Physics Society, McLean, Virginia).
ARMSTRONG, T.W. and COLBORN, B.L. (1992). ‘‘Predictions of induced
radioactivity for spacecraft in low-Earth orbit,’’ Nucl. Tracks Radiat. Meas.
20, 101–130.
ATWELL, W., BEEVER, E.R., HARDY, A.C. and CASH, B.L. (1989).
‘‘A radiation shielding model of the Space Shuttle for space radiation dose
exposure estimations,’’ page 11:1 in Proceedings of a Topical Meeting on
Advances in Nuclear Engineering Computation and Radiation Shielding
(American Nuclear Society, LaGrange Park, Illinois).
ATWELL, W., WEYLAND, M.D. and SIMONSEN, L.C. (1993). ‘‘Solar parti-
cle dose rate buildup and distribution in critical body organs,’’ pages 831
to 844 in Biological Effects and Physics of Solar and Galactic Cosmic
Radiation, Swenberg, C.E., Horneck, G. and Stassinopoulos, E.G., Eds.
(Plenum Press, New York).
AVILA, O., GAMBOA-DEBUEN, I. and BRANDAN, M.E. (1999). ‘‘Study of
the energy deposition in LiF by heavy charged particle irradiation and
its relation to the thermoluminescent efficiency of the material,’’ J. Phys.
D. Appl. Phys. 32, 1175–1181.
AVILES, P., GAMBOA-DEBUEN, I., RODRIGUEZ-VILLAFUERTE, M.,
BUENFIL, A.E., RUIZ-TREJO, C., LOPEZ, K. and BRANDAN, M.E.
128
REFERENCES / 129
(1999). ‘‘Thermoluminescent response of TLD-100 to low energy protons,’’
Radiat. Prot. Dosim. 84(1–4), 83–86.
BAARLI, J. and SULLIVAN, A.H. (1965). ‘‘Radiation dosimetry for protec-
tion purposes near high-energy particle accelerators,’’ Health Phys. 11,
353–361.
BADHWAR, G.D. and O’NEILL, P.M. (1992). ‘‘An improved model of galactic
cosmic radiation for space exploration missions,’’ Nucl. Tracks Radiat.
Meas. 20, 403–410.
BADHWAR, G.D., PATEL, J.U., CUCINOTTA, F.A. and WILSON, J.W.
(1995a). ‘‘Measurements of the secondary particle energy spectra in the
Space Shuttle,’’ Radiat. Meas. 24, 129–138.
BADHWAR, G.D., ATWELL, W., BENTON, E.V., FRANK, A.L., KEEGAN,
R.P., DUDKIN, V.E., KARPOV, O.N., POTAPOV, Y.V., AKOPOVA, A.B.,
MAGRADZE, N.V., MELKUMYAN, L.V. and RSHTUNI, S.B. (1995b).
‘‘A study of the radiation environment on board the Space Shuttle flight
STS-57,’’ Radiat. Meas. 24, 283–289.
BADHWAR, G.D., GOLIGHTLY, M.J., KONRADI, A., ATWELL, W., KERN,
J.W., CASH, B., BENTON, E.V., FRANK, A.L., SANNER, D., KEEGAN,
R.P., FRIGO, L.A., PETROV, V.M., TCHERNYKH, I.V., AKATOV, Y.A.,
SHURSHAKOV, V.A., ARKHANGELSKY, V.V., KUSHIN, V.V., KLYA-
CHIN, N.A., VANA, N. and SCHONER, W. (1996a). ‘‘In-flight radiation
measurements on STS-60,’’ Radiat. Meas. 26, 17–34.
BADHWAR, G.D., ATWELL, W., CASH, B., WEYLAND, M., PETROV,
V.M., TCHERNYKH, I.V., AKATOV, Y.A., SHURSHAKOV, V.A.,
ARKHANGELSKY, V.V., KUSHIN, V.V., KLYACHIN, N.A., BENTON,
E.V., FRANK, A.L., BENTON, E.R., FRIGO, L.A., DUDKIN, V.E.,
POTAPOV, Y.V., VANA, N., SCHONER, W. and FUGGER, M. (1996b).
‘‘Intercomparison of radiation measurements on STS-63,’’ Radiat. Meas.
26, 901–916.
BADHWAR, G.D., KONRADI, A., ATWELL, W., GOLIGHTLY, M.J.,
CUCINOTTA, F.A., WILSON, J.W., PETROV, V.M., TCHERNYKH, I.V.,
SHURSHAKOV, V.A. and LOBAKOV, A.P. (1996c). ‘‘Measurements of
the linear energy transfer spectra on the MIR Orbital Station and compari-
son with radiation transport models,’’ Radiat. Meas. 26, 147–158.
BADHWAR, G.D. (2000). ‘‘A crew active dosimeter and its calibration,’’ in
Workshop on Radiation Measurements for the ISS, Technical Report No.
2000-01 (Advanced Research Institute for Science and Engineering,
Waseda University, Tokyo).
BADHWAR, G.D., HUFF, H. and WILKINS, R. (2000). ‘‘Alterations in dose
and lineal energy spectra under different shieldings in the Los Alamos
high energy neutron field,’’ Radiat. Res. 154, 697–704.
BADHWAR, G.D., WATTS, J. and CLEGHORN, T.E. (2001). ‘‘Radiation
dose from reentrant electrons,’’ Radiat. Meas. 33, 369–372.
BADHWAR, G.D., ROBBINS, D.E., GIBBONS, F. and BRABY, L.A. (in
press). ‘‘Response of a tissue equivalent proportional counter to neutrons,’’
Radiat. Meas.
BARTLETT, D.T., STEELE, J.D. and STUBBERFIELD, D.R. (1986). ‘‘Devel-
opment of a single element neutron personal dosemeter for thermal, epith-
ermal and fast neutrons,’’ Nucl. Tracks Radiat. Meas. 12, 645–648.

130 / REFERENCES
BARTLETT, D.T., HAGER, L.G., IRVINE, D. and BAGSHAW, M. (2000).
‘‘Measurements on Concorde of the cosmic radiation field at aviation alti-
tudes,’’ Radiat. Prot. Dosim. 91(4), 365–376.
BARTLETT, D.T., HAGER, L.G., TANNER, R.J. and STEELE, J.D. (2001).
‘‘Measurements of the high energy neutron component of cosmic radiation
fields in aircraft using etched track dosemeters,’’ Radiat. Meas. 33,
243–253.
BAUCHINGER, M. (1995). ‘‘Quantification of low-level radiation exposure
by conventional chromosome aberration analysis,’’ Mutat. Res. 339,
177–189.
BENTON, E.V. and BADHWAR, G.D., Eds. (2001). ‘‘Prediction and measure-
ments of secondary neutrons in space,’’ Radiat. Meas. 33, 227–391.
BENTON, E.V., PRESTON, C.C., RUDDY, F.H., GOLD, R. and ROBERTS,
J.M. (1980). ‘‘Proton and alpha particle response characteristics of
CR-39 polymer for reactor and dosimetry application,’’ pages 459 to 467
in Proceedings of the 10th International Conference on Solid State Nuclear
Track Detectors (Elsevier Science, New York).
BENTON, E.V. and PARNELL, T.A. (1988). ‘‘Space radiation dosimetry on
U.S. and Soviet manned missions,’’ pages 729 to 794 in Terrestrial Space
Radiation and its Biological Effects, McCormack, P.D., Swenberg, C.E.
and Bucker, H., Eds. (Kluwer, New York).
BENTON, E.R., FRANK, A.L. and BENTON, E.V. (2000). ‘‘TLD efficiency
of 7LiF for doses deposited by high-LET particles,’’ Radiat. Meas. 32,
211–214.
BIGBEE, W.L., JENSEN, R.H., VEIDEBAUM, T., TEKKEL, M., RAHU,
M., STENGREVICS, A., AUVINEN, A., HAKULINEN, T., SERVOMAA,
K., RYTOMAA, T., OBRAMS, G.I. and BOICE, J.D., JR. (1997). ‘‘Biodosi-
metry of Chernobyl cleanup workers from Estonia and Latvia using the
glycophorin A in vivo somatic cell mutation assay,’’ Radiat. Res. 147,
215–224.
BOS, A.J.J. and DIELHOF, J.B. (1991). ‘‘The analysis of thermoluminescent
glow peaks in CaF2:Tm (TLD-300),’’ Radiat. Prot. Dosim. 37(4), 231–239.
BOTTER-JENSEN, L., AGERSNAP LARSEN, N., MARKEY, B.G. and
MCKEEVER, S.W.S. (1997). ‘‘Al2O3:C as a sensitive OSL dosemeter for
rapid assessment of environmental photon dose rates,’’ Radiat. Meas.
27, 295–298.
BUENFIL, A.E., GAMBOA-DEBUEN, I., RUIZ-TREJO, C., OLVERA, C.,
RODRIGUEZ-VILLAFUERTE, M., ROGERS, R.C. and BRANDAN, M.E.
(1999). ‘‘Response of TLD-300 to heavy charged particles,’’ Radiat. Prot.
Dosim. 84(1–4), 273–275.
BUTTS, J.J. and KATZ, R. (1967). ‘‘Theory of RBE for heavy ion bombard-
ment of dry enzymes and viruses,’’ Radiat. Res. 30, 855–871.
CARTWRIGHT, B.G., SHIRK, E.K. and PRICE, P.B. (1978). ‘‘A nuclear-
track-recording polymer of unique sensitivity and resolution,’’ Nucl. Instr.
Methods 153, 457–460.
CASSOU, R.M. and BENTON, E.V. (1978). ‘‘Properties and applications of
CR-39 polymeric nuclear track detector,’’ Nucl. Track Det. 2, 173–179.

REFERENCES / 131
CLOWDSLEY, M.S., HEINBOCKEL, J.H., KANEKO, H., WILSON, J.W.,
SINGLETERRY, R.C. and SHINN, J.L. (2000). ‘‘A comparison of the
multigroup and collocation methods for solving the low-energy neutron
Boltzmann equation,’’ Can. J. Phy. 78, 45–56.
COSSAIRT. J.D. and ELWYN A.J. (1987). ‘‘Personal dosimetry in a mixed
field of high-energy muons and neutrons,’’ Health Phys. 52, 813–818.
CUCINOTTA, F.A., TOWNSEND, L.W. and WILSON, J.W. (1993). Descrip-
tion of Alpha-Nucleus Interaction Cross Sections for Cosmic Ray Shielding
Studies, NASA-TP-3285 (National Aeronautics and Space Administration,
Center for AeroSpace Information, Hanover, Maryland).
CUCINOTTA, F.A. and DUBEY, R.R. (1993). Final State Interactions
and Inclusive Nuclear Collisions, NASA-TP-3353 (National Aeronautics
and Space Administration, Center for AeroSpace Information, Hanover,
Maryland).
CUCINOTTA, F.A., WILSON, J.W., SHINN, J.L., TRIPATHI, R.K.,
MAUNG, K.M., BADAVI, F.F., KATZ, R. and DUBEY, R.R. (1997). ‘‘Com-
putational procedures and database development,’’ pages 153 to 211 in
Shielding Strategies for Human Space Exploration, Wilson, J.W., Miller,
J., Konradi, A. and Cucinotta, F.A., Eds., NASA-CP-3360 (National Aero-
nautics and Space Administration, Center for AeroSpace Information,
Hanover, Maryland).
CUCINOTTA, F.A., WILSON, J.W., TRIPATHI, R.K. and TOWNSEND,
L.W. (1998). ‘‘Microscopic fragmentation model for galactic cosmic ray
studies,’’ Adv. Space Res. 22, 533–537.
DAVIS, A.J, MEWALDT, R.A., COHEN, C.M.S., CUMMINGS, A.C.,
GEORGE, J.S., LESKE, R.A., STONE, E.C., WIEDENBECK, M.E.,
YANASAK, N.E., CHRISTIAN, E.R., VON ROSENVINGE, T.T., BINNS,
W.R and HINK, P.L. (2001). ‘‘Solar minimum spectra of galactic cosmic
rays and their implications for models of the near-Earth radiation environ-
ment,’’ J. Geophys. Res. 106, 29,979–29,988.
DOE (1986). U.S. Department of Energy. Department of Energy Standard for
the Performance Testing of Personnel Dosimetry Systems, DOE Laboratory
Accreditation Program for Personnel Dosimetry Systems, DOE/EH-0027
(U.S. Department of Energy, Washington).
DOKE, T., HAYASHI, T., NAGAOKA, S., OGURA, K. and TAKEUCHI, R.
(1995). ‘‘Estimation of dose equivalent in STS-47 by a combination of
TLDs and CR-39,’’ Radiat. Meas. 24, 75–82.
DOKE, T., HAYASHI, T. and BORAK, T.B. (2001). ‘‘Comparisons of LET
distributions measured in low-Earth orbit using tissue-equivalent propor-
tional counters and the position-sensitive silicon-detector telescope
(RRMD – III),’’ Radiat. Res. 156, 310–316.
DURRANI, S.A. and BULL, R.K. (1987). Solid-State Nuclear Track Detec-
tion: Principles, Methods and Applications (Elsevier Science, New York).
EGERSDORFER, S., WIESER, A. and MULLER, A. (1996). ‘‘Tooth enamel
as a detector material for retrospective EPR dosimetry,’’ Appl. Radiat.
Isot. 47, 1299–1303.
FIECHTNER, A. and WERNLI, C. (1999). ‘‘Individual neutron monitoring
with CR-39 detectors at an accelerator center,’’ Radiat. Prot. Dosim.
85(1–4), 35–38.
132 / REFERENCES
FIENBERG, S.E., MARTIN, M.E. and STRAF, M.L., Eds. (1985). Sharing
Research Data (National Academy Press, Washington).
FLEISCHER, R.L., PRICE, P.B. and WALKER, R.M. (1975). Nuclear Tracks
in Solids: Principles and Applications (University of California Press,
Berkeley, California).
FURETTA, C. and WENG, P.S. (1998). Operational Thermoluminescence
Dosimetry (World Scientific, River Edge, New Jersey).
GEISS, O.B., KRAMER, M. and KRAFT, G. (1998). ‘‘Efficiency of thermolu-
minescent detectors to heavy charged particles,’’ Nucl. Instr. Methods
Phys. Res. B. 142, 592–598.
GERSEY, B.B., BORAK, T.B., GUETERSLOH, S.B., ZEITLIN, C., MILLER,
J., HEILBRONN, L., MURAKAMI, T. and IWATA, Y. (2002). ‘‘The
response of a spherical tissue-equivalent proportional counter to iron par-
ticles from 200 to 1000 MeV/nucleon,’’ Radiat. Res. 157, 350–360.
GONG, J.K., GLOMSKI, C.A. and GUO, Y. (1999). ‘‘A lifelong, wide-range
radiation biodosimeter: Erythrocytes with transferrin receptors,’’ Health
Phys. 77, 713–718.
GRIFFITH, R.V., THORNGATE, J.H., DAVIDSON, K.J., RUEPPEL, D.W.,
FISHER, J.C., TOMMASINO, L. and ZAPPAROLLI, G. (1981). ‘‘Monoen-
ergetic neutron response of selected etch plastics for personnel neutron
dosimetry,’’ Radiat. Prot. Dosim. 1(1), 61–71.
GUNTHER, W., LEUGNER, D., BECKER, E., FLESCH, F., HEINRICH,
W., HUNTRUP, G., REITZ, G., ROCHER, H. and STREIBEL, T. (1999).
‘‘Energy spectrum of iron nuclei measured inside the MIR space craft
using CR-39 track detectors,’’ Radiat. Meas. 31, 585–590.
HARRISON, K.G. and TOMMASINO, L. (1985). ‘‘Damage track detectors
for neutron dosimetry : II. Characteristics of different detection systems,’’
Radiat. Prot. Dosim. 10(1–4), 219–235.
HARVEY, J.R., TANNER, R.J., ALBERTS, W.G., BARTLETT, D.T.,
PIESCH, E.K.A. and SCHRAUBE, H. (1998). ‘‘The contribution of
EURADOS and CENDOS to track etch neutron dosimetry: The current
status in Europe,’’ Radiat. Prot. Dosim. 77(4), 267–304.
HOFERT, M. and STEVENSON, G.R. (1994). The CERN-CEC High-Energy
Reference Field Facility, CERN Report CERN/TIS-RP/94-02/CF (Euro-
pean Organisation for Nuclear Research, Geneva).
HOFERT, M. and RAFFNSOE, C. (1980). ‘‘Measurement of absolute
absorbed dose and dose equivalent response for instruments used around
high-energy accelerators,’’ Nucl. Inst. Methods 176, 443–448.
HOROWITZ, Y.S. (1984a). ‘‘General characteristics of TL materials,’’ page
89 in Thermoluminescence and Thermoluminescent Dosimetry, I, Horo-
witz, Y., Ed. (CRC Press, Boca Raton, Florida).
HOROWITZ, Y.S. (1984b). ‘‘Thermoluminescence radiation dosimetry,’’ page
43 in Thermoluminescence and Thermoluminescent Dosimetry, II, Horo-
witz, Y., Ed. (CRC Press, Boca Raton, Florida).
HOROWITZ, Y.S. and STERN, N. (1990). ‘‘Relative thermoluminescent effi-
ciency of LiF:Cu,Mg,P to alpha particles: Theory and experiment,’’ Radiat.
Prot. Dosim. 33(1–4), 287–290.

REFERENCES / 133
HOROWITZ, Y.S. and YOSSIAN, D. (1995). ‘‘Computerized glow curve
deconvolution: Application to thermoluminesence dosimetry,’’ Radiat.
Prot. Dosim. 60(1), 3.
ICRP (1989). International Commission on Radiological Protection. RBE
for Deterministic Effects, ICRP Publication 58, Annals of the ICRP 20
(Elsevier Science, New York).
ICRP (1991). International Commission on Radiological Protection. 1990
Recommendations of the International Commission on Radiological Pro-
tection, ICRP Publication 60, Annals of the ICRP 21 (Elsevier Science,
New York).
ICRP (1996). International Commission on Radiological Protection. Conver-
sion Coefficients for Use in Radiological Protection Against External Radi-
ation, ICRP Publication 74, Annals of the ICRP 26 (Elsevier Science,
New York).
ICRP (1997). International Commission on Radiological Protection. General
Principles for the Radiation Protection of Workers, ICRP Publication 75,
Annals of the ICRP 27 (Elsevier Science, New York).
ICRU (1983). International Commission on Radiation Units and Measure-
ments. Microdosimetry, ICRU Report 36 (International Commission on
Radiation Units and Measurements, Bethesda, Maryland).
ICRU (1992). International Commission on Radiation Units and Measure-
ments. Measurement of Dose Equivalents from External Photon and Elec-
tron Radiations, ICRU Report 47 (International Commission on Radiation
Units and Measurements, Bethesda, Maryland).
ICRU (1993). International Commission on Radiation Units and Measure-
ments. Quantities and Units in Radiation Protection Dosimetry, ICRU
Report 51 (International Commission on Radiation Units and Measure-
ments, Bethesda, Maryland).
ICRU (1998). International Commission on Radiation Units and Measure-
ments. Conversion Coefficients for Use in Radiological Protection Against
External Radiation, ICRU Report 57 (International Commission on Radia-
tion Units and Measurements, Bethesda, Maryland).
ING, H. (2001). ‘‘Neutron measurements using bubble detectors – terrestrial
and space,’’ Radiat. Meas. 33, 275–286.
ISO (1993). International Organization for Standardization. International
Vocabulary of Basic and General Terms in Metrology (International Orga-
nization for Standardization, Geneva).
JOZEFOWICZ, K., BURGKHARDT, B., VILGIS, M. and PIESCH, E. (1997).
‘‘Polycarbonate track detectors with a flat energy response for measure-
ment of high energy neutrons at accelerators and airflight altitudes,’’
Radiat. Prot. Dosim. 70(1–4), 143–148.
KAUL, A., DEHOS, A., BOGL, W., HINZ, G., KOSSEL, F., SCHWARZ, E.R.,
STAMM, A. and STEPHAN, G., Eds. (1986). Biological Indicators for
Radiation Dose Assessment (MMV Medizin, Verlag, Munich).
KAWATA, T., GOTOH, E., DURANTE, M., WU, H., GEORGE, K., FURU-
SAWA, Y. and CUCINOTTA, F.A. (2000). ‘‘High-LET radiation-induced
aberrations in prematurely condensed G2 chromosomes of human fibro-
blasts,’’ Int. J. Radiat. Biol. 76, 929–937.
134 / REFERENCES
KEEGAN, R. (1996). LET Spectrum Generation and Proton Induced Second-
ary Contribution to Total Dose Measured in Low-Earth Orbit, Ph.D. Thesis
(University College, Dublin.)
KOPP, J., BEAUJEAN, R., REITZ, G. and ENGE, W. (1999). ‘‘HZE dosimetry
in space using plastic track detectors,’’ Radiat. Meas. 31, 573–578.
KORFF, S.A., MENDELL, R.B., MERKER, M., LIGHT, E.S., VERSCHELL,
H. J. and SANDIE, W.S. (1979). Atmospheric Neutrons, NASA-CR-3126
(National Aeronautics and Space Administration, Center for AeroSpace
Information, Hanover, Maryland).
LOCKWOOD, J.A. (1972). ‘‘Neutron measurements in space,’’ Space Sci.
Rev. 14, 663–719.
LUSZIK-BHADRA, M., MATZKE, M., OTTO, T., REITZ, G. and SCHUH-
MACHER, H. (1999). ‘‘Personal neutron dosimetry in the Space Station
MIR and the Space Shuttle,’’ Radiat. Meas. 31, 425–430.
MCKEEVER, J., WALKER, F.D. and MCKEEVER, S.W.S. (1993). ‘‘Proper-
ties of the thermoluminscence emission from LiF(Mg,Cu,P),’’ Nucl. Tracks
Radiat. Meas. 21, 179–183.
MCKEEVER, S.W.S. (1985). Thermoluminescence of Solids (Cambridge Uni-
versity Press, Cambridge, England).
MCKEEVER, S.W.S. and HOROWITZ, Y.S. (1990). ‘‘Charge trapping mech-
anisms and microdosimetry processes in lithium fluoride,’’ Radiat. Phys.
Chem. 36, 35–46.
MCKEEVER, S.W.S., MOSCOVITCH, M. and TOWNSEND, P.D. (1995).
Thermoluminescence Dosimetry Materials: Properties and Uses (Nuclear
Technology Publishing, Ashford, Kent, England).
MOSCOVITCH, M., TAWIL, R.A. and SVINKIN, M. (1993). ‘‘Light induced
fading in alpha—Al2O3:C,’’ Radiat. Prot. Dosim. 47(1–4), 251– 253.
MUKHERJEE, B. and LUCAS, A.C. (1993). ‘‘Light conversion efficiency of
aluminum oxide dosemeters irradiated with 241Am alpha particles,’’
Radiat. Prot. Dosim. 47(1–4), 177–179.
MULLER, W.U. and STREFFER, C. (1991). ‘‘Biological indicators for radia-
tion damage,’’ Int. J. Radiat. Biol. 59, 863–873.
NASA (1998). National Aeronautics and Space Administration. Flight Direc-
tor Certification Guide, Document DA8-0010 (internal JSC document)
(National Aeronautics and Space Administration, Lyndon B. Johnson
Space Center, Houston, Texas).
NASA (1999). National Aeronautics and Space Administration. ISS Crew
Surgeon Training Certification Plan (MCC-H Position), JSC 26546, Vol.
II (internal JSC document) (National Aeronautics and Space Administra-
tion, Lyndon B. Johnson Space Center, Houston, Texas).
NASA (2000a). National Aeronautics and Space Administration. ‘‘Space
environment,’’ Section 14 in Space Shuttle Operational Flight Rules, Vol-
ume A, All Flights (1996), including PCN-1 through PCN-10, 1996 through
2000, NSTS-12820 (National Aeronautics and Space Administration,
Lyndon B. Johnson Space Center, Houston, Texas).
NASA (2000b). National Aeronautics and Space Administration. ‘‘Space envi-
ronment,’’ Section 14 in ISS Generic Operational Flight Rules, Volume B,

REFERENCES / 135
NSTS-12820 (National Aeronautics and Space Administration, Lyndon
B. Johnson Space Center, Houston, Texas).
NASA (2000c). National Aeronautics and Space Administration. Crew Train-
ing Catalog, SFOC FL 0258 Rev D (National Aeronautics and Space
Administration, Lyndon B. Johnson Space Center, Houston, Texas).
NASA (2000d). National Aeronautics and Space Administration. ISS Crew
Training Catalog, JSC 36301 Rev D (National Aeronautics and Space
Administration, Lyndon B. Johnson Space Center, Houston, Texas).
NASA (2001). National Aeronautics and Space Administration. ‘‘Prediction
and measurements of secondary neutrons in space,’’ Benton, E.V. and
Badhwar, G.D., Eds., Radiat. Meas. 33, 227–387.
NAS/NRC (2000). National Academy of Sciences/National Research Council.
Radiation and the International Space Station: Recommendations to
Reduce Risk, Report of the Committee on Solar and Space Physics and
the Committee on Solar-Terrestrial Research (National Academy Press,
Washington).
NCRP (1989). National Council on Radiation Protection and Measurements.
Guidance on Radiation Received in Space Activities, NCRP Report No. 98
(National Council on Radiation Protection and Measurements,
Bethesda, Maryland).
NCRP (1990). National Council on Radiation Protection and Measurements.
Implementation of the Principle of as Low as Reasonably Achievable
(ALARA) for Medical and Dental Personnel, NCRP Report No. 107
(National Council on Radiation Protection and Measurements,
Bethesda, Maryland).
NCRP (1991). National Council on Radiation Protection and Measurements.
Calibration of Survey Instruments Used in Radiation Protection for the
Assessment of Ionizing Radiation Fields and Radioactive Surface Contam-
ination, NCRP Report No. 112 (National Council on Radiation Protection
and Measurements, Bethesda, Maryland).
NCRP (1992). National Council on Radiation Protection and Measurements.
Maintaining Radiation Protection Records, NCRP Report No. 114
(National Council on Radiation Protection and Measurements,
Bethesda, Maryland).
NCRP (1993). National Council on Radiation Protection and Measurements.
Limitation of Exposure to Ionizing Radiation, NCRP Report No. 116
(National Council on Radiation Protection and Measurements,
Bethesda, Maryland).
NCRP (1994). National Council on Radiation Protection and Measurements.
Dose Control at Nuclear Power Plants, NCRP Report No. 120 (National Coun-
cil on Radiation Protection and Measurements, Bethesda, Maryland).
NCRP (1997). National Council on Radiation Protection and Measurements.
Acceptability of Risk from Radiation – Application to Human Space Flight,
NCRP Symposium Proceedings No. 3 (National Council on Radiation Pro-
tection and Measurements, Bethesda, Maryland).
NCRP (1998). National Council on Radiation Protection and Measurements.
Operational Radiation Safety Program, NCRP Report No. 127 (National
Council on Radiation Protection and Measurements, Bethesda, Maryland).

136 / REFERENCES
NCRP (1999). National Council on Radiation Protection and Measurements.
The Application of ALARA for Occupational Exposures, NCRP Statement
No. 8 (http://www.ncrp.com/statemnt.html) (National Council on Radia-
tion Protection and Measurements, Bethesda, Maryland).
NCRP (2000a). National Council on Radiation Protection and Measure-
ments. Radiation Protection Guidance for Activities in Low-Earth Orbit,
NCRP Report No. 132 (National Council on Radiation Protection and
Measurements, Bethesda, Maryland).
NCRP (2000b). National Council on Radiation Protection and Measure-
ments. Operational Radiation Safety Training, NCRP Report No. 134
(National Council on Radiation Protection and Measurements, Bethesda,
Maryland).
NIEWIADOMSKI, T. (1993). ‘‘Lithium fluoride in thermoluminescence
materials,’’ page 142 in Thermoluminescent Materials, Vij, D.R., Ed. (Pren-
tice Hall, Englewood Cliffs, New Jersey).
OMB (1997). Office of Management and Budget. North American Industry
Classification System Manual (National Technical Information Service,
Springfield, Virginia).
OMB (2000). Office of Management and Budget. Standard Occupational
Classifications Manual (National Technical Information Service, Spring-
field, Virginia).
ORTEGA, X., GINJAUME, M., HERNANDEZ, A., VILLANUEVA, I. and
ARMOR, I. (2001). ‘‘The outlook for the application of electronic doseme-
ters as legal dosimetry,’’ Radiat. Prot. Dosim. 96(1–3), 87–91.
O’SULLIVAN, D., ZHOU, D., HEINRICH, W., ROESLER, S., DONNELLY,
J., KEEGAN, R., FLOOD, E. and TOMMASINO, L. (1999). ‘‘Cosmic rays
and dosimetry at aviation altitudes,’’ Radiat. Meas. 31, 579–584.
PARETZKE, H.G. (1977). ‘‘On primary damage and secondary electron dam-
age in heavy ion tracks in plastics,’’ Radiat. Effects 34, 3–8.
PARETZKE, H.G. (1982). ‘‘Can dosimetric quantities describe charged parti-
cle tracks in matter?’’ pages 3 to 14 in Proceedings of the 11th International
Conference on Solid State Nuclear Track Detectors, Fowler, P.H. and
Clapham, V.M., Eds. (Elsevier Science, New York).
PIESCH, E., BURGKHARDT, B. and VILGIS, M. (1990). ‘‘Photolumi-
nescense dosimetry: Progress and present state of the art,’’ Radiat. Prot.
Dosim. 33(1–4), 215–226.
PIESCH, E., BURGKHARDT, B. and VILGIS, M. (1993). ‘‘Progress in phos-
phate glass dosimetry: Experiences and routine monitoring with a modern
dosimetry system,’’ Radiat. Prot. Dosim. 47(1–4), 409–414.
PRASANNA, P.G.S., ESCALADA, N.D. and BLAKELY, W.F. (2000). ‘‘Induc-
tion of premature chromosome condensation by a phosphatase inhibitor
and a protein kinase in unstimulated human peripheral blood lympho-
cytes: A simple and rapid technique to study chromosome aberrations
using specific whole-chromosome DNA hybridization probes for biological
dosimetry,’’ Mutat. Res. 466, 131–141.
PRESZLER, A.M., SIMNETT, G.M. and WHITE, R.S. (1972). ‘‘Earth albedo
neutrons from 10 to 100 MeV,’’ Phys. Rev. Lett. 28, 982–985.

REFERENCES / 137
PRICE, P.B. and WALKER, R.M. (1962). ‘‘Electron microscope observation of
etched tracks from spallation recoils in mica,’’ Phys. Rev. Lett. 8, 217–219.
PROSSER, J.S., MOQUET, J.E., LLOYD, D.C. and EDWARDS, A.A. (1988).
‘‘Radiation induction of micronuclei in human lymphocytes,’’ Mutat. Res.
199, 37–45.
QUALLS, G.D. and BOYKIN, R. (1997). ‘‘Space radiation shielding analysis
by CAD techniques,’’ pages 365 to 382 in Shielding Strategies for Human
Space Exploration, Wilson, J.W., Miller, J., Konradi, A. and Cucinotta,
F.A., Eds., NASA-CP-3360 (National Aeronautics Space Administration,
Center for AeroSpace Information, Hanover, Maryland).
RADEMACHER, S.E., BORAK, T.B., ZEITLIN, C., HEILBROON, L. and
MILLER, J. (1998). ‘‘Wall effects observed in tissue-equivalent propor-
tional counters from 1.05 GeV/nucleon 56Fe particles,’’ Radiat. Res. 149,
387–395.
ROSSI, H.H. and ROSENWEIG, W. (1955). ‘‘A device for the measurement
of dose as a function of specific ionization,’’ Radiology 64, 404–410.
RUDDY, F.H., GOLD, R., ROBERTS, J.H., BENTON, E.V. and SCHRAUBE,
H. (1981). ‘‘Neutron response characteristics of CR-39 polymer for reactor
and dosimetry applications,’’ pages 437 to 440 in Proceedings of the 11th
International Conference on Solid State Nuclear Track Detectors, Fowler,
P.H. and Clapham, V.M., Eds. (Elsevier Science, New York).
SELTZER, S.M. (1980). SHIELDOSE: A Computer Code for Space-Shielding
Radiation Dose Calculations, National Bureau of Standards Technical
Note 1116 (National Technical Information Service, Springfield, Virginia).
SCHONER, W., VANA, N. and FUGGER, M. (1999). ‘‘The LET dependence
of LiF:Mg,Ti dosemeters and its application for LET measurements in
mixed radiation fields,’’ Radiat. Prot. Dosim. 85(1–4), 263–266.
SHAVERS, M.R. (1999). Biological Effectiveness of Nuclear Fragments Pro-
duced by High-Energy Protons Interacting in Tissues Near the Bone-Soft
Tissue Interface, Ph.D. Dissertation (Texas A&M University, College Sta-
tion, Texas).
SHEA, M.A., SMART, D.F. and MCCALL, J.R. (1988). ‘‘A five degree by
fifteen degree world grid of trajectory determined vertical cutoff rigidities,’’
Can. J. Phys. 46, S1098–S1102.
SHINN, J.L., CUCINOTTA, F.A., SIMONSEN, L.C., WILSON, J.W.,
BADAVI, F.F. , BADHWAR, G.D. , MILLER, J. , ZEITLIN, C. ,
HEILBRONN, L., TRIPATHI, R.K., CLOWDSLEY, M.S., HEINBOCKEL,
J.H. and XAPSOS, M.A. (1998). ‘‘Validation of a comprehensive space
radiation transport code,’’ IEEE Trans. Nucl. Sci. 45, 2711–2719.
SHINN, J.L., BADHWAR, G.D., XAPSOS, M.A., CUCINOTTA, F.A. and
WILSON, J.W. (1999). ‘‘An analysis of energy deposition in a tissue equiva-
lent proportional counter onboard the Space Shuttle,’’ Radiat. Meas.
30, 19–28.
SILK, E.C.H. and BARNES, R.S. (1959). ‘‘Examination of fission fragment
tracks with an electron microscope,’’ Phil. Mag. 4, 970–971.
SOHRABI, M. (1974). ‘‘The amplification of recoil particle tracks in polymers
and its application in fast neutron personnel dosimetry,’’ Health Phys.
27, 598–600.
138 / REFERENCES
SOMOGYI, G. and HUNYADI, I. (1980). ‘‘Etching properties of the CR-39
polymeric nuclear detector,’’ pages 443 to 452 in Proceedings of the 10th
International Conference on Solid State Nuclear Track Detectors (Elsevier
Science, New York).
SPURNY, F. (1995). ‘‘Dosimetry of neutrons and high energy particles with
nuclear track detectors,’’ Radiat. Meas. 25, 429–436.
TESTARD, I. and SABATIER, L. (1999). ‘‘Biological dosimetry for astro-
nauts: A real challenge,’’ Mutat. Res. 430, 315–326.
TEXIER, C., ITIE, C., SERVIERE, H., GRESSIER, V. and BOLOGNESE-
MILSZTAJN, T. (2001). ‘‘Study of the photon radiation performance of
electronic personal dosemeters,’’ Radiat. Prot. Dosim. 96, 245–249.
TOMMASINO, L. (1970). ‘‘Electrochemical etching of damaged track detec-
tors by h.v. pulse and sinusoidal waveforms,’’ pages 213 to 218 in Compte
Rendo du 7eme Colloque International de Photographie Corpusculaire et
des Detecteurs Visuels Solides, Cuer, P. and Schmitt, Eds. (Laboratoire
de Physique Corpusoulaire, Strasbourg, France).
TOMMASINO, L. and ARMELLINI, C. (1973). ‘‘New etching technique for
damage track detectors,’’ Radiat. Effects 20, 253–255.
TOMMASINO, L. and HARRISON, K.G. (1985). ‘‘Damage track detectors
for neutron dosimetry: I. Registration and counting methods,’’ Radiat.
Prot. Dosim. 10(1–4), 207–217.
TRIPATHI, R.K., CUCINOTTA, F.A. and WILSON, J.W. (1999). ‘‘Medium
modified nucleon-nucleon cross sections in a nucleus,’’ Nucl. Instr. Meth-
ods Phys. Res. B 152, 425–431.
TRIPATHI, R.K., WILSON, J.W. and CUCINOTTA, F.A. (1998). ‘‘Nuclear
absorption cross sections using medium modified nucleon-nucleon ampli-
tudes,’’ Nucl. Instr. Methods Phys. Res. B 145, 277–282.
TUCKER, J.D., TAWN, E.J., HOLDSWORTH, D., MORRIS, S., LANGLOIS,
R., RAMSEY, M.J., KATO, P., BOICE, J.D., JR., TARONE, R.E. and
JENSEN, R.H. (1997). ‘‘Biological dosimetry of radiation workers at the
Sellafield nuclear facility,’’ Radiat. Res. 148, 216–226.
VANA, N., SCHONER, W., FUGGER, M. and AKATOV, Y. (1996). ‘‘Absorbed
dose measurement and LET determination with TLDs in space,’’ Radiat.
Prot. Dosim. 66(1–4), 145–152.
VETTE, J.I. (1991). The NASA/National Space Science Data Center Trapped
Radiation Environment Model Program (1964–1991), NASA-TM-107993
(National Aeronautics Space Administration, Center for AeroSpace Infor-
mation, Hanover, Maryland).
WERNLI, C. and KAHILAINEN, J. (2001). ‘‘Direct ion storage dosimetry
systems for photon, beta and neutron radiation with instant readout capa-
bilities,’’ Radiat. Prot. Dosim. 96(1–3), 255–259.
WHITE, V.R., ALDERMAN, D.F. and FAISON, C.D. (2001). National Volun-
tary Laboratory Accreditation Program. Procedures and General Require-
ments (NVLAP), National Institute of Standards and Technology
Handbook 150 (National Technical Information Service, Springfield,
Virginia).
WIEGEL, B., OHRNDORF, T. and HEINRICH, W. (1988). ‘‘Measurements
of cosmic ray LET-spectra for the D1,’’ pages 795 to 808 in NATO Advanced

REFERENCES / 139
Study Institute on Terrestrial Space Radiation and Its Biological Effects,
McCormack, P.D., Swenberg, C.E. and Bucker, H., Eds. (Plenum Press,
New York).
WILSON, J.W. (1974). ‘‘Multiple scattering of heavy ions, glauber theory,
and optical model,’’ Phys. Lett. 52, 149–152.
WILSON, J.W., CHUN, S.Y., BUCK, W.W. and TOWNSEND, L.W. (1988a).
‘‘High energy nucleon data bases,’’ Health Phys. 55, 817–819.
WILSON, J.W., TOWNSEND, L.W., CHUN, S.Y., BUCK, W.W., KAHN, F.
and CUCINOTTA, F.A. (1988b). BRYNTRN: A Baryon Transport Com-
puter Code, Computation Procedures and Data Base, NASA TM-4037
(National Aeronautics Space Administration, Center for AeroSpace Infor-
mation, Hanover, Maryland).
WILSON, J.W., TOWNSEND L.W., SCHMMERLING, W.S., KHANDEL-
WAL, G.S., KHAN, F.S., NEALY, J.E., CUCINOTTA, F.A., SIMONSEN,
L.C., SHINN, J.L. and NORBURG, J.W.L. (1991). Transport Methods and
Interactions for Space Radiations, NASA-RP-1257 (National Aeronautics
Space Administration, Center for AeroSpace Information, Hanover,
Maryland).
WILSON, J.W., TOWNSEND, L.W., SHINN, J.L., CUCINOTTA, F.A.,
COSTEN, R.C., BADAVI, F.F. and LAMKIN, S.L. (1994). ‘‘Galactic cosmic
ray transport methods: Past, present, and future,’’ Adv. Space Res. 14,
841–852.
WILSON, J.W., BADAVI, F.F., CUCINOTTA, F.A., SHINN, J.L.,
BADHWAR, G.D., SILBERBERG, R., TSAO, C.H., TOWNSEND, L.W.
and TRIPATHI, R.K. (1995). HZETRN: Description of a Free-Space Ion
and Nucleon Transport and Shielding Computer Program, NASA-
TP-3495 (National Aeronautics Space Administration, Center for Aero-
Space Information, Hanover, Maryland).
WILSON, J.W., MILLER, J., KONRADI, A. and CUCINOTTA, F.A., Eds.
(1997). Shielding Strategies for Human Space Exploration, NASA-
CP-3360 (National Aeronautics Space Administration, Center for Aero-
Space Information, Hanover, Maryland).
WILSON, J.W., TWEED, J., NEALY, J.E., ZEITLIN, C., KIM, M.H.Y.,
ANDERSON, B.M., WARE, J. and PERSANS, A.E. (2001). Shuttle Space-
suit: Fabric/LCVG Model Validation, SAE 2001-01-2372 (Society of Auto-
motive Engineers, Warrendale, Pennsylvania).
XAPSOS, M.A. (1992). ‘‘A spatially restricted linear energy transfer equa-
tion,’’ Radiat. Res. 132, 282–287.
YANG, T.C., GEORGE, K., JOHNSON, A.S., DURANTE, M. and
FEDORENKO, B.S. (1997). ‘‘Biodosimetry results from space flight
Mir-18,’’ Radiat. Res. 148, S17–S23.
YASUDA, H. and FUJITAKA, K. (2000). ‘‘Non-linearity of the high tempera-
ture peak area ratio of 6LiF:Mg,Ti (TLD-600),’’ Radiat. Meas. 32, 355–360.
YASUDA, H., BADHWAR, G.D., KOMIYAMA, T. and FUJITAKA, K. (2000).
‘‘Effective dose equivalent on the ninth shuttle – Mir mission (STS-91),’’
Radiat. Res. 154, 705–713.
YASUDA, H. (2001). ‘‘Conservative evaluation of space radiation dose equiv-
alent using the glow curve of 7Lif:Mg,Ti (TLD-700),’’ Health Phys. 80,
576–582.
140 / REFERENCES
YOSHIHIRA, E., DOKE, T., HARA, T., HAYASHI, T., KIKUCHI, J., KONO,
S., SAKAGUCHI, T., TAKAHASHI, K., TANIHATA, C. and MURAKAMI,
T. (2000). ‘‘Omni-directional silicon detector telescope for measurement
of LET distribution is space,’’ in Workshop on Radiation Measurements
for the ISS, Technical Report No. 2000-21 (Advanced Research Institute
for Science and Engineering, Waseda University, Tokyo).
YOSHIZAWA, N., SATO, O., TAKAGI, S., FURIHATA, S., FUNABIKI, J.,
IWAI, S., UEHARA, T., TANAKA, S. and SAKAMOTO, Y. (2000). ‘‘Fluence
to dose conversion coefficients for high-energy neutron, proton, and alpha
particles,’’ J. Nucl. Sci. Technol. (Suppl. 1), 865–869.
YOUNG, D.A. (1958). ‘‘Etching of radiation damage in lithium fluoride,’’
Nature 182, 357–377.
ZEITLIN, C., HEILBRONN, L., MILLER, J., RADEMACHER, S.E.,
BORAK, T., CARTER, T.R., FRANKEL, K.A., SCHIMMERLING, W. and
STRONACH, C. (1997). ‘‘Heavy fragment production cross sections from
1.05 GeV/nucleon 56Fe in C, Al, Cu, Pb, and CH2 targets,’’ Phys. Rev.
56, 388–397.
ZIELCZYNSKI, M. (1962). ‘‘Use of columnar recombination to determine the
effectiveness of radiation,’’ Nukleonika (English Translation) 7, 213–223.

The NCRP
The National Council on Radiation Protection and Measurements is a
nonprofit corporation chartered by Congress in 1964 to:
1. Collect, analyze, develop and disseminate in the public interest informa-
tion and recommendations about (a) protection against radiation and
(b) radiation measurements, quantities and units, particularly those con-
cerned with radiation protection.
2. Provide a means by which organizations concerned with the scientific
and related aspects of radiation protection and of radiation quantities,
units and measurements may cooperate for effective utilization of their
combined resources, and to stimulate the work of such organizations.
3. Develop basic concepts about radiation quantities, units and measure-
ments, about the application of these concepts, and about radiation
protection.
4. Cooperate with the International Commission on Radiological Protection,
the International Commission on Radiation Units and Measurements,
and other national and international organizations, governmental and
private, concerned with radiation quantities, units and measurements
and with radiation protection.
The Council is the successor to the unincorporated association of scien-
tists known as the National Committee on Radiation Protection and Mea-
surements and was formed to carry on the work begun by the Committee
in 1929.
The participants in the Council’s work are the Council members and
members of scientific and administrative committees. Council members are
selected solely on the basis of their scientific expertise and serve as individu-
als, not as representatives of any particular organization. The scientific
committees, composed of experts having detailed knowledge and competence
in the particular area of the committee’s interest, draft proposed recommen-
dations. These are then submitted to the full membership of the Council
for careful review and approval before being published.
The following comprise the current officers and membership of the
Council:
Officers
President Thomas S. TenfordeVice President Kenneth R. KaseSecretary and Treasurer William M. BecknerAssistant Secretary Michael F. McBride
141
142 / THE NCRP
Members
John F. Ahearne Ethel S. Gilbert Bruce A. NapierLarry E. Anderson Joel E. Gray Carl J. PaperielloBenjamin R. Archer Andrew J. Grosovsky Ronald C. PetersenMary M. Austin-Seymour Raymond A. Guilmette R. Julian PrestonHarold L. Beck William R. Hendee Jerome S. PuskinEleanor A. Blakely John W. Hirshfeld Marvin RosensteinJohn D. Boice, Jr. David G. Hoel Lawrence N. RothenbergThomas B. Borak F. Owen Hoffman Henry D. RoyalAndre Bouville Geoffrey R. Howe Michael T. RyanLeslie A. Braby Kenneth R. Kase Jonathan M. SametDavi J. Brenner Ann R. Kennedy Stephen M. SeltzerAntone L. Brooks David C. Kocher Roy E. ShoreJerrold T. Bushberg Ritsuko Komaki Edward A. SicklesJohn F. Cardella Amy Kronenberg David H. SlineyShih-Yew Chen Charles E. Land Paul SlovicChung-Kwang Chou Susan M. Langhorst Daniel J. StromMary E. Clark Richard W. Leggett Louise C. StrongJames E. Cleaver Howard L. Liber Thomas S. TenfordeJ. Donald Cossairt James C. Lin Lawrence W. TownsendAllen G. Croff Jill Lipoti Lois B. TravisFrancis A. Cucinotta John B. Little Robert L. UllrichPaul M. DeLuca Jay H. Lubin Richard J. VetterCarter Denniston C. Douglas Maynard Daniel WartenbergGail de Planque Claire M. Mays David A. WeberJohn F. Dicello Barbara J. McNeil F. Ward WhickerSarah S. Donaldson Fred A. Mettler, Jr. Chris G. WhippleWilliam P. Dornsife Charles W. Miller J. Frank WilsonStephen A. Feig Jack Miller Susan D. WiltshireH. Keith Florig Kenneth L. Miller Marco ZaiderKenneth R. Foster William F. Morgan Pasquale ZanzonicoJohn F. Frazier John E. Moulder Marvin C. ZiskinThomas F. Gesell David S. Myers
Honorary Members
Lauriston S. Taylor, Honorary PresidentWarren K. Sinclair, President Emeritus; Charles B. Meinhold, President Emeritus
S. James Adelstein, Honorary Vice PresidentW. Roger Ney, Executive Director Emeritus
Seymour Abrahamson Patricia W. Durbin Robert J. NelsenEdward L. Alpen Keith F. Eckerman Wesley L. NyborgLynn R. Anspaugh Thomas S. Ely John W. Poston, Sr.John A. Auxier Richard F. Foster Andrew K. PoznanskiWilliam J. Bair R.J. Michael Fry Chester R. RichmondBruce B. Boecker Robert O. Gorson William L. RussellVictor P. Bond Arthur W. Guy Eugene L. SaengerRobert L. Brent Eric J. Hall William J. SchullReynold F. Brown Naomi H. Harley J. Newell StannardMelvin C. Carter Donald G. Jacobs John B. StorerRandall S. Caswell Bernd Kahn John E. TillFrederick P. Cowan Roger O. McClellan Arthur C. UptonJames F. Crow Dade W. Moeller George L. VoelzGerald D. Dodd A. Alan Moghissi Edward W. Webster

THE NCRP / 143
Lauriston S. Taylor Lecturers
Herbert M. Parker (1977) The Squares of the Natural Numbers in RadiationProtection
Sir Edward Pochin (1978) Why be Quantitative about Radiation RiskEstimates?
Hymer L. Friedell (1979) Radiation Protection—Concepts and Trade OffsHarold O. Wyckoff (1980) From ‘‘Quantity of Radiation’’ and ‘‘Dose’’ to
‘‘Exposure’’ and ‘‘Absorbed Dose’’—An Historical ReviewJames F. Crow (1981) How Well Can We Assess Genetic Risk? Not VeryEugene L. Saenger (1982) Ethics, Trade-offs and Medical RadiationMerril Eisenbud (1983) The Human Environment—Past, Present and FutureHarald H. Rossi (1984) Limitation and Assessment in Radiation ProtectionJohn H. Harley (1985) Truth (and Beauty) in Radiation MeasurementHerman P. Schwan (1986) Biological Effects of Non-ionizing Radiations:
Cellular Properties and InteractionsSeymour Jablon (1987) How to be Quantitative about Radiation Risk
EstimatesBo Lindell (1988) How Safe is Safe Enough?Arthur C. Upton (1989) Radiobiology and Radiation Protection: The Past
Century and Prospects for the FutureJ. Newell Stannard (1990) Radiation Protection and the Internal Emitter
SagaVictor P. Bond (1991) When is a Dose Not a Dose?Edward W. Webster (1992) Dose and Risk in Diagnostic Radiology: How Big?
How Little?Warren K. Sinclair (1993) Science, Radiation Protection and the NCRPR.J. Michael Fry (1994) Mice, Myths and MenAlbrecht Kellerer (1995) Certainty and Uncertainty in Radiation ProtectionSeymour Abrahamson (1996) 70 Years of Radiation Genetics: Fruit Flies, Mice
and HumansWilliam J. Bair (1997) Radionuclides in the Body: Meeting the Challenge!Eric J. Hall (1998) From Chimney Sweeps to Astronauts: Cancer Risks in the
WorkplaceNaomi H. Harley (1999) Back to BackgroundS. James Adelstein (2000) Administered Radioactivity: Unde Venimus Quoque
ImusWesley L. Nyborg (2001) Assuring the Safety of Medical Diagnostic
UltrasoundR. Julian Preston (2002) Developing Mechanistic Data for Incorporation into
Cancer Risk Assessment: Old Problems and New Approaches
Currently, the following committees are actively engaged in formulating
recommendations:
SC 1 Basic Criteria, Epidemiology, Radiobiology and Risk
SC 1-4 Extrapolation of Risks from Non-Human Experimental
Systems to Man
SC 1-7 Information Needed to Make Radiation Protection
Recommendations for Travel Beyond Low-Earth Orbit
SC 1-8 Risk to Thyroid from Ionizing Radiation
SC 1-10 Review of Cohen’s Radon Research Methods
SC 1-11 Radiation Protection and Measurement for Neutron
Surveillance Scanners
144 / THE NCRP
SC 1-12 Exposure Limits for Security Surveillance Devices
SC 9 Structural Shielding Design and Evaluation for Medical Use of
X Rays and Gamma Rays of Energies Up to 10 MeV
SC 46 Operational Radiation Safety
SC 46-8 Radiation Protection Design Guidelines for Particle
Accelerator Facilities
SC 46-13 Design of Facilities for Medical Radiation Therapy
SC 46-16 Radiation Protection in Veterinary Medicine
SC 46-17 Radiation Protection in Educational Institutions
SC 57-15 Uranium Risk
SC 57-17 Radionuclide Dosimetry Models for Wounds
SC 64 Environmental Issues
SC 64-22 Design of Effective Effluent and Environmental
Monitoring Programs
SC 64-23 Cesium in the Environment
SC 66 Biological Effects and Exposure Criteria for Ultrasound
SC 72 Radiation Protection in Mammography
SC 85 Risk of Lung Cancer from Radon
SC 87 Radioactive and Mixed Waste
SC 87-1 Waste Avoidance and Volume Reduction
SC 87-3 Performance Assessment
SC 87-5 Risk Management Analysis for Decommissioned Sites
SC 89 Nonionizing Electromagnetic Fields
SC 89-3 Biological Effects of Extremely Low-Frequency Electric
and Magnetic Fields
SC 89-4 Biological Effects and Exposure Recommendations for
Modulated Radiofrequency Fields
SC 89-6 Wireless Telecommunications Safety Issues for Building
Owners and Managers
SC 91 Radiation Protection in Medicine
SC 91-1 Precautions in the Management of Patients Who Have
Received Therapeutic Amounts of Radionuclides
SC 91-2 Radiation Protection in Dentistry
SC 92 Public Policy and Risk Communication
SC 93 Radiation Measurement and Dosimetry
In recognition of its responsibility to facilitate and stimulate cooperation
among organizations concerned with the scientific and related aspects of
radiation protection and measurement, the Council has created a category
of NCRP Collaborating Organizations. Organizations or groups of organiza-
tions that are national or international in scope and are concerned with
scientific problems involving radiation quantities, units, measurements and
THE NCRP / 145
effects, or radiation protection may be admitted to collaborating status by
the Council. Collaborating Organizations provide a means by which the
NCRP can gain input into its activities from a wider segment of society.
At the same time, the relationships with the Collaborating Organizations
facilitate wider dissemination of information about the Council’s activities,
interests and concerns. Collaborating Organizations have the opportunity
to comment on draft reports (at the time that these are submitted to the
members of the Council). This is intended to capitalize on the fact that
Collaborating Organizations are in an excellent position to both contribute
to the identification of what needs to be treated in NCRP reports and to
identify problems that might result from proposed recommendations. The
present Collaborating Organizations with which the NCRP maintains liai-
son are as follows:
Agency for Toxic Substances and Disease Registry
American Academy of Dermatology
American Academy of Environmental Engineers
American Academy of Health Physics
American Association of Physicists in Medicine
American College of Medical Physics
American College of Nuclear Physicians
American College of Occupational and Environmental Medicine
American College of Radiology
American Dental Association
American Industrial Hygiene Association
American Institute of Ultrasound in Medicine
American Insurance Services Group
American Medical Association
American Nuclear Society
American Pharmaceutical Association
American Podiatric Medical Association
American Public Health Association
American Radium Society
American Roentgen Ray Society
American Society for Therapeutic Radiology and Oncology
American Society of Health-System Pharmacists
American Society of Radiologic Technologists
Association of University Radiologists
Bioelectromagnetics Society
Campus Radiation Safety Officers
College of American Pathologists
Conference of Radiation Control Program Directors, Inc.
Council on Radionuclides and Radiopharmaceuticals
Defense Threat Reduction Agency
Electric Power Research Institute
Federal Communications Commission
Federal Emergency Management Agency
Genetics Society of America
146 / THE NCRP
Health Physics Society
Institute of Electrical and Electronics Engineers, Inc.
Institute of Nuclear Power Operations
International Brotherhood of Electrical Workers
National Aeronautics and Space Administration
National Association of Environmental Professionals
National Electrical Manufacturers Association
National Institute for Occupational Safety and Health
National Institute of Standards and Technology
Nuclear Energy Institute
Office of Science and Technology Policy
Oil, Chemical and Atomic Workers
Radiation Research Society
Radiological Society of North America
Society for Risk Analysis
Society of Chairmen of Academic Radiology Departments
Society of Nuclear Medicine
Society of Skeletal Radiology
U.S. Air Force
U.S. Army
U.S. Coast Guard
U.S. Department of Energy
U.S. Department of Housing and Urban Development
U.S. Department of Labor
U.S. Department of Transportation
U.S. Environmental Protection Agency
U.S. Navy
U.S. Nuclear Regulatory Commission
U.S. Public Health Service
Utility Workers Union of America
The NCRP has found its relationships with these organizations to be
extremely valuable to continued progress in its program.
Another aspect of the cooperative efforts of the NCRP relates to the
Special Liaison relationships established with various governmental organi-
zations that have an interest in radiation protection and measurements.
This liaison relationship provides: (1) an opportunity for participating orga-
nizations to designate an individual to provide liaison between the organiza-
tion and the NCRP; (2) that the individual designated will receive copies of
draft NCRP reports (at the time that these are submitted to the members
of the Council) with an invitation to comment, but not vote; and (3) that new
NCRP efforts might be discussed with liaison individuals as appropriate, so
that they might have an opportunity to make suggestions on new studies
and related matters. The following organizations participate in the Special
Liaison Program:
Australian Radiation Laboratory
Bundesamt fur Strahlenschutz (Germany)
THE NCRP / 147
Canadian Nuclear Safety Commission
Central Laboratory for Radiological Protection (Poland)
China Institute for Radiation Protection
Commisariat a l’Energie Atomique
Commonwealth Scientific Instrumentation Research Organization
(Australia)
European Commission
Health Council of the Netherlands
International Commission on Non-Ionizing Radiation Protection
Japan Radiation Council
Korea Institute of Nuclear Safety
National Radiological Protection Board (United Kingdom)
Russian Scientific Commission on Radiation Protection
South African Forum for Radiation Protection
World Association of Nuclear Operations
The NCRP values highly the participation of these organizations in the
Special Liaison Program.
The Council also benefits significantly from the relationships established
pursuant to the Corporate Sponsor’s Program. The program facilitates the
interchange of information and ideas and corporate sponsors provide valu-
able fiscal support for the Council’s program. This developing program cur-
rently includes the following Corporate Sponsors:
3M Corporate Health Physics
Amersham Health
Duke Energy Corporation
ICN Biomedicals, Inc.
Landauer, Inc.
Nuclear Energy Institute
Philips Medical Systems
Southern California Edison
The Council’s activities are made possible by the voluntary contribution
of time and effort by its members and participants and the generous support
of the following organizations:
3M Health Physics Services
Agfa Corporation
Alfred P. Sloan Foundation
Alliance of American Insurers
American Academy of Dermatology
American Academy of Health Physics
American Academy of Oral and Maxillofacial Radiology
American Association of Physicists in Medicine
American Cancer Society
American College of Medical Physics
American College of Nuclear Physicians
American College of Occupational and Environmental Medicine
148 / THE NCRP
American College of Radiology
American College of Radiology Foundation
American Dental Association
American Healthcare Radiology Administrators
American Industrial Hygiene Association
American Insurance Services Group
American Medical Association
American Nuclear Society
American Osteopathic College of Radiology
American Podiatric Medical Association
American Public Health Association
American Radium Society
American Roentgen Ray Society
American Society of Radiologic Technologists
American Society for Therapeutic Radiology and Oncology
American Veterinary Medical Association
American Veterinary Radiology Society
Association of University Radiologists
Battelle Memorial Institute
Canberra Industries, Inc.
Chem Nuclear Systems
Center for Devices and Radiological Health
College of American Pathologists
Committee on Interagency Radiation Research and Policy
Coordination
Commonwealth of Pennsylvania
Consumers Power Company
Council on Radionuclides and Radiopharmaceuticals
Defense Nuclear Agency
Eastman Kodak Company
Edison Electric Institute
Edward Mallinckrodt, Jr. Foundation
EG&G Idaho, Inc.
Electric Power Research Institute
Federal Emergency Management Agency
Florida Institute of Phosphate Research
Fuji Medical Systems, U.S.A., Inc.
Genetics Society of America
Health Effects Research Foundation (Japan)
Health Physics Society
Institute of Nuclear Power Operations
James Picker Foundation
Martin Marietta Corporation
Motorola Foundation
National Aeronautics and Space Administration
National Association of Photographic Manufacturers
National Cancer Institute
National Electrical Manufacturers Association

THE NCRP / 149
National Institute of Standards and Technology
Picker International
Public Service Electric and Gas Company
Radiation Research Society
Radiological Society of North America
Richard Lounsbery Foundation
Sandia National Laboratory
Siemens Medical Systems, Inc.
Society of Nuclear Medicine
Society of Pediatric Radiology
U.S. Department of Energy
U.S. Department of Labor
U.S. Environmental Protection Agency
U.S. Navy
U.S. Nuclear Regulatory Commission
Victoreen, Inc.
Westinghouse Electric Corporation
Initial funds for publication of NCRP reports were provided by a grant
from the James Picker Foundation.
The NCRP seeks to promulgate information and recommen-dations
based on leading scientific judgment on matters of radiation protection and
measurement and to foster cooperation among organizations concerned with
these matters. These efforts are intended to serve the public interest and
the Council welcomes comments and suggestions on its reports or activities
from those interested in its work.

NCRP Publications
Information on NCRP publications may be obtained from the NCRP
website (http://www.ncrp.com), e-mail ([email protected]), by telephone
(800-229-2652, Ext. 25), or fax (301-907-8768). The address is:
NCRP Publications
7910 Woodmont Avenue
Suite 400
Bethesda, MD 20814-3095
Abstracts of NCRP reports published since 1980, abstracts of all NCRP
commentaries, and the text of all NCRP statements are available at the
NCRP website. Currently available publications are listed below.
NCRP Reports
No. Title
8 Control and Removal of Radioactive Contamination in
Laboratories (1951)
22 Maximum Permissible Body Burdens and Maximum Permissible
Concentrations of Radionuclides in Air and in Water for
Occupational Exposure (1959) [Includes Addendum 1 issued in
August 1963]
25 Measurement of Absorbed Dose of Neutrons, and of Mixtures of
Neutrons and Gamma Rays (1961)
27 Stopping Powers for Use with Cavity Chambers (1961)
30 Safe Handling of Radioactive Materials (1964)
32 Radiation Protection in Educational Institutions (1966)
35 Dental X-Ray Protection (1970)
36 Radiation Protection in Veterinary Medicine (1970)
37 Precautions in the Management of Patients Who Have Received
Therapeutic Amounts of Radionuclides (1970)
38 Protection Against Neutron Radiation (1971)
40 Protection Against Radiation from Brachytherapy Sources (1972)
41 Specification of Gamma-Ray Brachytherapy Sources (1974)
42 Radiological Factors Affecting Decision-Making in a Nuclear
Attack (1974)
150

NCRP PUBLICATIONS / 151
44 Krypton-85 in the Atmosphere—Accumulation, Biological
Significance, and Control Technology (1975)
46 Alpha-Emitting Particles in Lungs (1975)
47 Tritium Measurement Techniques (1976)
49 Structural Shielding Design and Evaluation for Medical Use of
X Rays and Gamma Rays of Energies Up to 10 MeV (1976)
50 Environmental Radiation Measurements (1976)
52 Cesium-137 from the Environment to Man: Metabolism and Dose
(1977)
54 Medical Radiation Exposure of Pregnant and Potentially
Pregnant Women (1977)
55 Protection of the Thyroid Gland in the Event of Releases of
Radioiodine (1977)
57 Instrumentation and Monitoring Methods for Radiation
Protection (1978)
58 A Handbook of Radioactivity Measurements Procedures, 2nd ed.
(1985)
60 Physical, Chemical, and Biological Properties of Radiocerium
Relevant to Radiation Protection Guidelines (1978)
61 Radiation Safety Training Criteria for Industrial Radiography
(1978)
62 Tritium in the Environment (1979)
63 Tritium and Other Radionuclide Labeled Organic Compounds
Incorporated in Genetic Material (1979)
64 Influence of Dose and Its Distribution in Time on Dose-Response
Relationships for Low-LET Radiations (1980)
65 Management of Persons Accidentally Contaminated with
Radionuclides (1980)
67 Radiofrequency Electromagnetic Fields—Properties, Quantities
and Units, Biophysical Interaction, and Measurements (1981)
68 Radiation Protection in Pediatric Radiology (1981)
69 Dosimetry of X-Ray and Gamma-Ray Beams for Radiation
Therapy in the Energy Range 10 keV to 50 MeV (1981)
70 Nuclear Medicine—Factors Influencing the Choice and Use of
Radionuclides in Diagnosis and Therapy (1982)
72 Radiation Protection and Measurement for Low-Voltage Neutron
Generators (1983)
73 Protection in Nuclear Medicine and Ultrasound Diagnostic
Procedures in Children (1983)
74 Biological Effects of Ultrasound: Mechanisms and Clinical
Implications (1983)
75 Iodine-129: Evaluation of Releases from Nuclear Power
Generation (1983)
77 Exposures from the Uranium Series with Emphasis on Radon
and Its Daughters (1984)
78 Evaluation of Occupational and Environmental Exposures to
Radon and Radon Daughters in the United States (1984)

152 / NCRP PUBLICATIONS
79 Neutron Contamination from Medical Electron Accelerators
(1984)
80 Induction of Thyroid Cancer by Ionizing Radiation (1985)
81 Carbon-14 in the Environment (1985)
82 SI Units in Radiation Protection and Measurements (1985)
83 The Experimental Basis for Absorbed-Dose Calculations in
Medical Uses of Radionuclides (1985)
84 General Concepts for the Dosimetry of Internally Deposited
Radionuclides (1985)
85 Mammography—A User’s Guide (1986)
86 Biological Effects and Exposure Criteria for Radiofrequency
Electromagnetic Fields (1986)
87 Use of Bioassay Procedures for Assessment of Internal
Radionuclide Deposition (1987)
88 Radiation Alarms and Access Control Systems (1986)
89 Genetic Effects from Internally Deposited Radionuclides (1987)
90 Neptunium: Radiation Protection Guidelines (1988)
92 Public Radiation Exposure from Nuclear Power Generation in
the United States (1987)
93 Ionizing Radiation Exposure of the Population of the United
States (1987)
94 Exposure of the Population in the United States and Canada
from Natural Background Radiation (1987)
95 Radiation Exposure of the U.S. Population from Consumer
Products and Miscellaneous Sources (1987)
96 Comparative Carcinogenicity of Ionizing Radiation and
Chemicals (1989)
97 Measurement of Radon and Radon Daughters in Air (1988)
99 Quality Assurance for Diagnostic Imaging (1988)
100 Exposure of the U.S. Population from Diagnostic Medical
Radiation (1989)
101 Exposure of the U.S. Population from Occupational Radiation
(1989)
102 Medical X-Ray, Electron Beam and Gamma-Ray Protection for
Energies Up to 50 MeV (Equipment Design, Performance and
Use) (1989)
103 Control of Radon in Houses (1989)
104 The Relative Biological Effectiveness of Radiations of Different
Quality (1990)
105 Radiation Protection for Medical and Allied Health Personnel
(1989)
106 Limit for Exposure to ‘‘Hot Particles’’ on the Skin (1989)
107 Implementation of the Principle of As Low As Reasonably
Achievable (ALARA) for Medical and Dental Personnel (1990)108 Conceptual Basis for Calculations of Absorbed-Dose
Distributions (1991)109 Effects of Ionizing Radiation on Aquatic Organisms (1991)110 Some Aspects of Strontium Radiobiology (1991)

NCRP PUBLICATIONS / 153
111 Developing Radiation Emergency Plans for Academic, Medical orIndustrial Facilities (1991)
112 Calibration of Survey Instruments Used in Radiation Protectionfor the Assessment of Ionizing Radiation Fields andRadioactive Surface Contamination (1991)
113 Exposure Criteria for Medical Diagnostic Ultrasound: I. CriteriaBased on Thermal Mechanisms (1992)
114 Maintaining Radiation Protection Records (1992)115 Risk Estimates for Radiation Protection (1993)116 Limitation of Exposure to Ionizing Radiation (1993)117 Research Needs for Radiation Protection (1993)118 Radiation Protection in the Mineral Extraction Industry (1993)119 A Practical Guide to the Determination of Human Exposure to
Radiofrequency Fields (1993)120 Dose Control at Nuclear Power Plants (1994)121 Principles and Application of Collective Dose in Radiation
Protection (1995)122 Use of Personal Monitors to Estimate Effective Dose Equivalent
and Effective Dose to Workers for External Exposure to Low-LET Radiation (1995)
123 Screening Models for Releases of Radionuclides to Atmosphere,Surface Water, and Ground (1996)
124 Sources and Magnitude of Occupational and Public Exposuresfrom Nuclear Medicine Procedures (1996)
125 Deposition, Retention and Dosimetry of Inhaled RadioactiveSubstances (1997)
126 Uncertainties in Fatal Cancer Risk Estimates Used in RadiationProtection (1997)
127 Operational Radiation Safety Program (1998)128 Radionuclide Exposure of the Embryo/Fetus (1998)129 Recommended Screening Limits for Contaminated Surface Soil
and Review of Factors Relevant to Site-Specific Studies (1999)130 Biological Effects and Exposure Limits for ‘‘Hot Particles’’ (1999)131 Scientific Basis for Evaluating the Risks to Populations from
Space Applications of Plutonium (2001)132 Radiation Protection Guidance for Activities in Low-Earth Orbit
(2000)133 Radiation Protection for Procedures Performed Outside the
Radiology Department (2000)134 Operational Radiation Safety Training (2000)135 Liver Cancer Risk from Internally-Deposited Radionuclides
(2001)
136 Evaluation of the Linear-Nonthreshold Dose-Response Model forIonizing Radiation (2001)
137 Fluence-Based and Microdosimetric Event-Based Methods forRadiation Protection in Space (2001)
138 Management of Terrorist Events Involving Radioactive Material(2001)
141 Managing Potentially Radioactive Scrap Metal (2002)
142 Operational Radiation Safety Program for Astronauts in Low-Earth Orbit: A Basic Framework (2002)
154 / NCRP PUBLICATIONS
Binders for NCRP reports are available. Two sizes make it possible
to collect into small binders the ‘‘old series’’ of reports (NCRP Reports
Nos. 8-30) and into large binders the more recent publications (NCRP Reports
Nos. 32-138, 141-142). Each binder will accommodate from five to seven
reports. The binders carry the identification ‘‘NCRP Reports’’ and come with
label holders which permit the user to attach labels showing the reports
contained in each binder.
The following bound sets of NCRP reports are also available:
Volume I. NCRP Reports Nos. 8, 22
Volume II. NCRP Reports Nos. 23, 25, 27, 30
Volume III. NCRP Reports Nos. 32, 35, 36, 37
Volume IV. NCRP Reports Nos. 38, 40, 41
Volume V. NCRP Reports Nos. 42, 44, 46
Volume VI. NCRP Reports Nos. 47, 49, 50, 51
Volume VII. NCRP Reports Nos. 52, 53, 54, 55, 57
Volume VIII. NCRP Report No. 58
Volume IX. NCRP Reports Nos. 59, 60, 61, 62, 63
Volume X. NCRP Reports Nos. 64, 65, 66, 67
Volume XI. NCRP Reports Nos. 68, 69, 70, 71, 72
Volume XII. NCRP Reports Nos. 73, 74, 75, 76
Volume XIII. NCRP Reports Nos. 77, 78, 79, 80
Volume XIV. NCRP Reports Nos. 81, 82, 83, 84, 85
Volume XV. NCRP Reports Nos. 86, 87, 88, 89
Volume XVI. NCRP Reports Nos. 90, 91, 92, 93
Volume XVII. NCRP Reports Nos. 94, 95, 96, 97
Volume XVIII. NCRP Reports Nos. 98, 99, 100
Volume XIX. NCRP Reports Nos. 101, 102, 103, 104
Volume XX. NCRP Reports Nos. 105, 106, 107, 108
Volume XXI. NCRP Reports Nos. 109, 110, 111
Volume XXII. NCRP Reports Nos. 112, 113, 114
Volume XXIII. NCRP Reports Nos. 115, 116, 117, 118
Volume XXIV. NCRP Reports Nos. 119, 120, 121, 122
Volume XXV. NCRP Report No. 123I and 123II
Volume XXVI. NCRP Reports Nos. 124, 125, 126, 127
Volume XXVII. NCRP Reports Nos. 128, 129, 130
Volume XXVIII. NCRP Reports Nos. 131, 132, 133
Volume XXIX. NCRP Reports Nos. 134, 135, 136, 137
(Titles of the individual reports contained in each volume are
given above.)
NCRP PUBLICATIONS / 155
NCRP Commentaries
No. Title
1 Krypton-85 in the Atmosphere—With Specific Reference to the
Public Health Significance of the Proposed Controlled Release
at Three Mile Island (1980)
4 Guidelines for the Release of Waste Water from Nuclear
Facilities with Special Reference to the Public Health
Significance of the Proposed Release of Treated Waste Waters
at Three Mile Island (1987)
5 Review of the Publication, Living Without Landfills (1989)
6 Radon Exposure of the U.S. Population—Status of the Problem
(1991)
7 Misadministration of Radioactive Material in Medicine—
Scientific Background (1991)
8 Uncertainty in NCRP Screening Models Relating to Atmospheric
Transport, Deposition and Uptake by Humans (1993)
9 Considerations Regarding the Unintended Radiation Exposure of
the Embryo, Fetus or Nursing Child (1994)
10 Advising the Public about Radiation Emergencies: A Document
for Public Comment (1994)
11 Dose Limits for Individuals Who Receive Exposure from
Radionuclide Therapy Patients (1995)
12 Radiation Exposure and High-Altitude Flight (1995)
13 An Introduction to Efficacy in Diagnostic Radiology and Nuclear
Medicine (Justification of Medical Radiation Exposure) (1995)
14 A Guide for Uncertainty Analysis in Dose and Risk Assessments
Related to Environmental Contamination (1996)
15 Evaluating the Reliability of Biokinetic and Dosimetric Models
and Parameters Used to Assess Individual Doses for Risk
Assessment Purposes (1998)
Proceedings of the Annual Meeting
No. Title
1 Perceptions of Risk, Proceedings of the Fifteenth Annual
Meeting held on March 14-15, 1979 (including Taylor Lecture
No. 3) (1980)
3 Critical Issues in Setting Radiation Dose Limits, Proceedings of
the Seventeenth Annual Meeting held on April 8-9, 1981
(including Taylor Lecture No. 5) (1982)
4 Radiation Protection and New Medical Diagnostic Approaches,
Proceedings of the Eighteenth Annual Meeting held on April
6-7, 1982 (including Taylor Lecture No. 6) (1983)
156 / NCRP PUBLICATIONS
5 Environmental Radioactivity, Proceedings of the Nineteenth
Annual Meeting held on April 6-7, 1983 (including Taylor
Lecture No. 7) (1983)
6 Some Issues Important in Developing Basic Radiation Protection
Recommendations, Proceedings of the Twentieth Annual
Meeting held on April 4-5, 1984 (including Taylor Lecture No. 8)
(1985)
7 Radioactive Waste, Proceedings of the Twenty-first Annual
Meeting held on April 3-4, 1985 (including Taylor Lecture No. 9)
(1986)
8 Nonionizing Electromagnetic Radiations and Ultrasound,
Proceedings of the Twenty-second Annual Meeting held on
April 2-3, 1986 (including Taylor Lecture No. 10) (1988)
9 New Dosimetry at Hiroshima and Nagasaki and Its Implications
for Risk Estimates, Proceedings of the Twenty-third Annual
Meeting held on April 8-9, 1987 (including Taylor Lecture No. 11)
(1988)
10 Radon, Proceedings of the Twenty-fourth Annual Meeting held
on March 30-31, 1988 (including Taylor Lecture No. 12) (1989)
11 Radiation Protection Today—The NCRP at Sixty Years,
Proceedings of the Twenty-fifth Annual Meeting held on
April 5-6, 1989 (including Taylor Lecture No. 13) (1990)
12 Health and Ecological Implications of Radioactively
Contaminated Environments, Proceedings of the Twenty-sixth
Annual Meeting held on April 4-5, 1990 (including Taylor
Lecture No. 14) (1991)
13 Genes, Cancer and Radiation Protection, Proceedings of the
Twenty-seventh Annual Meeting held on April 3-4, 1991
(including Taylor Lecture No. 15) (1992)
14 Radiation Protection in Medicine, Proceedings of the Twenty-
eighth Annual Meeting held on April 1-2, 1992 (including
Taylor Lecture No. 16) (1993)
15 Radiation Science and Societal Decision Making, Proceedings of
the Twenty-ninth Annual Meeting held on April 7-8, 1993
(including Taylor Lecture No. 17) (1994)
16 Extremely-Low-Frequency Electromagnetic Fields: Issues in
Biological Effects and Public Health, Proceedings of the
Thirtieth Annual Meeting held on April 6-7, 1994 (not
published).
17 Environmental Dose Reconstruction and Risk Implications,
Proceedings of the Thirty-first Annual Meeting held on April
12-13, 1995 (including Taylor Lecture No. 19) (1996)
18 Implications of New Data on Radiation Cancer Risk,
Proceedings of the Thirty-second Annual Meeting held on
April 3-4, 1996 (including Taylor Lecture No. 20) (1997)
19 The Effects of Pre- and Postconception Exposure to Radiation,
Proceedings of the Thirty-third Annual Meeting held on April
2-3, 1997, Teratology 59, 181–317 (1999)

NCRP PUBLICATIONS / 157
20 Cosmic Radiation Exposure of Airline Crews, Passengers and
Astronauts, Proceedings of the Thirty-fourth Annual Meeting
held on April 1-2, 1998, Health Phys. 79, 466–613 (2000)
21 Radiation Protection in Medicine: Contemporary Issues,
Proceedings of the Thirty-fifth Annual Meeting held on April
7-8, 1999 (including Taylor Lecture No. 23) (1999)
22 Ionizing Radiation Science and Protection in the 21st Century,
Proceedings of the Thirty-sixth Annual Meeting held on April
5-6, 2000, Health Phys. 80, 317–402 (2001)
23 Fallout from Atmospheric Nuclear Tests—Impact on Science and
Society, Proceedings of the Thirty-seventh Annual Meeting
held on April 4-5, 2001, Health Phys. 82, 573–748 (2002)
Lauriston S. Taylor Lectures
No. Title
1 The Squares of the Natural Numbers in Radiation Protection by
Herbert M. Parker (1977)
2 Why be Quantitative about Radiation Risk Estimates? by Sir
Edward Pochin (1978)
3 Radiation Protection—Concepts and Trade Offs by Hymer L.
Friedell (1979) [Available also in Perceptions of Risk, see
above]
4 From ‘‘Quantity of Radiation’’ and ‘‘Dose’’ to ‘‘Exposure’’ and
‘‘Absorbed Dose’’—An Historical Review by Harold O. Wyckoff
(1980)
5 How Well Can We Assess Genetic Risk? Not Very by James F.
Crow (1981) [Available also in Critical Issues in Setting
Radiation Dose Limits, see above]
6 Ethics, Trade-offs and Medical Radiation by Eugene L. Saenger
(1982) [Available also in Radiation Protection and New
Medical Diagnostic Approaches, see above]
7 The Human Environment—Past, Present and Future by Merril
Eisenbud (1983) [Available also in Environmental
Radioactivity, see above]
8 Limitation and Assessment in Radiation Protection by Harald H.
Rossi (1984) [Available also in Some Issues Important in
Developing Basic Radiation Protection Recommendations, see
above]
9 Truth (and Beauty) in Radiation Measurement by John H.
Harley (1985) [Available also in Radioactive Waste, see above]
10 Biological Effects of Non-ionizing Radiations: Cellular Properties
and Interactions by Herman P. Schwan (1987) [Available also
in Nonionizing Electromagnetic Radiations and Ultrasound,
see above]

158 / NCRP PUBLICATIONS
11 How to be Quantitative about Radiation Risk Estimates by
Seymour Jablon (1988) [Available also in New Dosimetry at
Hiroshima and Nagasaki and its Implications for Risk
Estimates, see above]
12 How Safe is Safe Enough? by Bo Lindell (1988) [Available also
in Radon, see above]
13 Radiobiology and Radiation Protection: The Past Century and
Prospects for the Future by Arthur C. Upton (1989) [Available
also in Radiation Protection Today, see above]
14 Radiation Protection and the Internal Emitter Saga by J. Newell
Stannard (1990) [Available also in Health and Ecological
Implications of Radioactively Contaminated Environments, see
above]
15 When is a Dose Not a Dose? by Victor P. Bond (1992) [Available
also in Genes, Cancer and Radiation Protection, see above]
16 Dose and Risk in Diagnostic Radiology: How Big? How Little? by
Edward W. Webster (1992)[Available also in Radiation
Protection in Medicine, see above]
17 Science, Radiation Protection and the NCRP by Warren K.
Sinclair (1993)[Available also in Radiation Science and
Societal Decision Making, see above]
18 Mice, Myths and Men by R.J. Michael Fry (1995)
19 Certainty and Uncertainty in Radiation Research by Albrecht M.
Kellerer. Health Phys. 69, 446–453 (1995).
20 70 Years of Radiation Genetics: Fruit Flies, Mice and Humans
by Seymour Abrahamson. Health Phys. 71, 624–633 (1996).
21 Radionuclides in the Body: Meeting the Challenge by William J.
Bair. Health Phys. 73, 423–432 (1997).
22 From Chimney Sweeps to Astronauts: Cancer Risks in the Work
Place by Eric J. Hall. Health Phys. 75, 357–366 (1998).
23 Back to Background: Natural Radiation and Radioactivity
Exposed by Naomi H. Harley. Health Phys. 79, 121–128
(2000).
24 Administered Radioactivity: Unde Venimus Quoque Imus by
S. James Adelstein. Health Phys. 80, 317–324 (2001).
25 Assuring the Safety of Medical Diagnostic Ultrasound by Wesley
L. Nyborg. Health Phys. 82, 578–587 (2002)
Symposium Proceedings
No. Title
1 The Control of Exposure of the Public to Ionizing Radiation in
the Event of Accident or Attack, Proceedings of a Symposium
held April 27-29, 1981 (1982)
2 Radioactive and Mixed Waste—Risk as a Basis for Waste
Classification, Proceedings of a Symposium held November 9,
1994 (1995)
NCRP PUBLICATIONS / 159
3 Acceptability of Risk from Radiation—Application to Human
Space Flight, Proceedings of a Symposium held May 29, 1996
(1997)
4 21st Century Biodosimetry: Quantifying the Past and Predicting
the Future, Proceedings of a Symposium held on February 22,
2001, Radiat. Prot. Dosim. 97, No. 1, 7–80 (2001)
NCRP Statements
No. Title
1 ‘‘Blood Counts, Statement of the National Committee on
Radiation Protection,’’ Radiology 63, 428 (1954)
2 ‘‘Statements on Maximum Permissible Dose from Television
Receivers and Maximum Permissible Dose to the Skin of the
Whole Body,’’ Am. J. Roentgenol., Radium Ther. and Nucl.
Med. 84, 152 (1960) and Radiology 75, 122 (1960)
3 X-Ray Protection Standards for Home Television Receivers,
Interim Statement of the National Council on Radiation
Protection and Measurements (1968)
4 Specification of Units of Natural Uranium and Natural
Thorium, Statement of the National Council on Radiation
Protection and Measurements (1973)
5 NCRP Statement on Dose Limit for Neutrons (1980)
6 Control of Air Emissions of Radionuclides (1984)
7 The Probability That a Particular Malignancy May Have Been
Caused by a Specified Irradiation (1992)
8 The Application of ALARA for Occupational Exposures (1999)
9 Extension of the Skin Dose Limit for Hot Particles to Other
External Sources of Skin Irradiation (2001)
Other Documents
The following documents of the NCRP were published outside of the
NCRP report, commentary and statement series:
Somatic Radiation Dose for the General Population, Report of
the Ad Hoc Committee of the National Council on Radiation
Protection and Measurements, 6 May 1959, Science, February
19, 1960, Vol. 131, No. 3399, pages 482-486
Dose Effect Modifying Factors In Radiation Protection, Report of
Subcommittee M-4 (Relative Biological Effectiveness) of the
National Council on Radiation Protection and Measurements,
Report BNL 50073 (T-471) (1967) Brookhaven National
Laboratory (National Technical Information Service
Springfield, Virginia)
Index
Absorbed dose (D) 4, 7, 122
mean absorbed dose in an
organ or tissue (DT) 7
Accreditation programs 56–57
National Voluntary Laboratory
Accreditation Program
(NVLAP) 56–57
U.S. Department of Energy
Laboratory Accreditation
Program (DOELAP) 56–57
Active detectors 7–10, 29–30,
46–48, 53, 85–94
Cerenkov counters 93
characteristics 47
electronic personal dosimeters
10, 48
for electrons 8, 48
ionization chambers 93–94
response time 47
semiconductor detectors 91–93
solid-state detectors 47–48
tissue equivalent proportional
counters (TEPC) 8, 47, 86–91
Active real-time monitoring
84–94
local spatial variations 84
uncertainties in external
radiation 84
Administrative levels 69–70, 72,
122
Albedo neutrons 3, 38, 122
Alpha particles 108
Aluminum oxide, doped with
carbon (Al2O3:C) 9, 108–110,
113
efficiency function 108–109
glow curve 108–109
Americium-241 102, 107
Area monitoring 7, 42–43, 53
for electrons 53
recommendations 53
160
solid-state detectors 53
tissue equivalent proportional
counters (TEPC) 53
As low as reasonably achievable
(ALARA) 1, 2, 7, 11–12, 23,
68–69, 70–73, 122
continuous in-flight review
71–72
definition 68
examples 12
graded approach to
implementation 72
postflight review 70, 72
preflight planning 71
radiation safety training 73
role of radiation health officer
(RHO) 70
spacecraft and space suit
design 70–71
Astronauts 1, 2, 13, 15, 26, 71,
73–74
role in management of dose 26
wearing of personal dosimeters
13, 71, 73
Aviation activities 68, 80
estimating dose 68
Background radiation 68
Biochemical indicators 60
Biodosimetry 11, 59–65, 80
biochemical indicators 60
changes in cellular markers 65
chromosomal aberrations 59
cytogenetic alterations 61–63
definition and purpose 59
electron spin resonance 59–60
erythrocytes with transferrin
receptors 60
fluorescence in situ
hybridization (FISH) 11, 64
future considerations 11, 65
INDEX / 161
gene mutation assays 60–61
gene mutations 59
molecular profiling 65
recommendations 64–65
summary for methods 63
use in space program 63–64
Biomedical research 4, 26, 68, 80
expert radiation panel 26
informed consent 26
Institutional Review Board 26
internal radiation 80
Boltzmann equation 95
Bone marrow 31, 80
Bragg-Gray cavity theory 86
Bremsstrahlung 30, 85
Carbon-12 89, 102
Calcium fluoride, doped with
thulium (CaF2:Tm) 105–108,
113
annealing treatments 105
efficiency function 107–108
glow curve 105–108
peak-height ratio 105–107
Calibration of dose measurements
10, 57
angle dependence 10
conditions 57
definition 57
determination of response
characteristics 57
particle energy ranges 10
response characteristics 10, 57
Cancer mortality risk coefficients
20
Cataracts 20
Cellulose nitrate 120
Cerenkov counters 93
design and operation 93
Cesium-137 49–50, 55, 100–101,
112
Charged ions 40, 45
nuclear fragments 45
radiation transport codes 40
Chromosomal aberrations 62–63
application to astronauts 62–63
application to radiation
accidents 62
atomic-bomb survivors 62
fluorescence in situ
hybridization (FISH) 62–63
lower level of detection 63
occupationally and medically
exposed persons 62
Cobalt-60 55, 100–102, 104, 108,
110
Computational methods 95–98
basic quantum mechanics 98
Boltzmann equation 95
collision with atomic electrons
95–96
cross sections 95–97
elastic nuclear scattering 95–96
for space applications 96–97
Monte Carlo 98
nuclear reactive processes
95–96
Pauli principle 98
Computerized anatomical models
41
female 41
male 41
Conversion coefficients 10–11, 52,
57–58
in calibration 57–58
Coronal mass ejection 122
Cesium-137 110
Cytogenetic alterations 61–63
chromosomal aberrations 62–63
cytochalasin B technique 61
micronuclei 61
prematurely condensed
chromosomes 62–63
Delta rays 88–90
Deterministic effects 4, 18, 20,
122
Diagnostic and therapeutic
medical procedures 68, 79, 81
linkage to dosimetry records 79
Direct ion storage dosimeters 51
design and characteristics 51
Dose assessment 6, 35–43, 59
approach for space radiation
35, 37
biodosimetry 59
162 / INDEX
exterior exposure field 38
interior exposure field 39
tissue exposure fields 41
Dose equivalent (H) 4, 7, 20, 35,
42, 55, 112–114, 122
calculation procedure 35
determination in combined
high- and low-LET fields
113–114
estimation from
thermoluminescent dosimeter
(TLD) data 112–114
limitations in use of
thermoluminescent
dosimeters (TLD) with
neutrons 113
Dose limits 3–4, 17–19, 21,
68–70, 72, 122
bone marrow 18, 21
deterministic effects 3, 21
lens of the eye 18, 21
skin 18, 21
sources of exposure included 68
stochastic effects 3
ten-year career limits 21
Dose measurements 55–58
accuracy 55–57
calibration 55–58
dependence of response on
energy and angle of incidence
57
general requirements 56
National Voluntary Laboratory
Accreditation Program
(NVLAP) 57
performance testing 55–56
recommendations of ICRP and
ICRU 55–56
response characteristics 58
uncertainty of laboratory
calibrations 58
U.S. Department of Energy
Laboratory Accreditation
Program (DOELAP) 57
Dosimetry measurements 42–45
radiation response
characteristics 45
time considerations 45
Dosimetry records 13–14,
122–123
annual confidential record 13
cumulative dose from space
flight 13
effective dose (E) 13
gray equivalent (GT) 13
mission-related aviation
activities 13
mission-related biomedical
research 13
other information linked to
dosimetry record 13
purposes 13
updates of record 13–14
Earth’s geomagnetic field 38
Effective dose (E) 4, 7, 13, 18–20,
22, 36, 52, 56, 80–81, 123
approach for space radiation
20, 22
calculation procedure 36
direct estimation with
thermoluminescent
dosimeters (TLD) and plastic
nuclear track detectors
(PNTD) 52
records 80–81
uncertainty in estimation 56
Efficiency function 103–105,
107–109, 110–114
Electron detectors 48–49
ionization chamber 49
Electron spin resonance 59
Electronic personal dosimeters
48, 55
design and characteristics 48
direct ion storage dosimeters 48
for low-LET radiation 55
Electrons 5, 10, 30, 38-40, 58, 112
energy ranges for calibration of
measurements 58
radiation transport codes 38, 40
reentrant electrons 5
splash albedo electrons 5
trapped electrons 5
Environmental models 6
INDEX / 163
Equivalent dose (HT) 4, 19–20,
22, 123
Equivalent gamma-ray dose
110–111
Erythrocytes with transferrin
receptors 60
Exterior exposure field 38–39
radiation environment models
38
spacecraft external
measurements 39
trapped radiation models 38
Extravehicular activity (EVA) 5,
16, 41
Extravehicular activity (EVA)
suit 31, 33
design and materials 33
Flight director 2, 26, 74
radiation safety training 74
role in management of dose 26
Flight rules 26, 70, 74
Flight Techniques Board 26
Flight surgeon 2, 26, 75
Radiation Integrated Product
Team 26
radiation safety training 75
role in management of dose 26
Fluorescence in situ hybridization
(FISH) 11, 61–65
analysis of prematurely
condensed chromosomes 11
calibration curves 11
use in space program 64
Fluorine-19 102
Galactic cosmic radiation (GCR)
3, 5, 16, 32, 38, 53, 123
Gene mutation assays 60–61
glycophorin A 61
Gray equivalent (GT) 3, 7, 13,
18–19, 36, 80–81, 123
calculation procedure 36
records 80–81
Helium 108
High atomic number, high-energy
(HZE) ions 5, 10, 20, 58, 123
argon 20
carbon 10
energy ranges for calibration of
measurements 58
helium 10
iron 10, 20
silicon 10
High transient doses 12, 17, 44,
74–76
Immediate dose management 7,
11–12, 68–72, 123
continuous in-flight review
71–72
definition 68
examples 12
flight rules 12
graded approach to
implementation 72
high transient exposures 11
in-flight radiation protection
actions 69
postflight review 72
preflight planning 71
spacecraft and space suit
design 70–71
Institutional Review Board 69
Interior exposure field 39–40, 43
shielding models 39
spacecraft internal
measurements 40
Internal radiation 80–81
biomedical research 80–81
computation of effective dose
(E) 81
records 80–81
International Commission on
Radiation Units (ICRU) 56
International Commission on
Radiological Protection (ICRP)
56
Ionization chamber 8, 53, 93–94
design and operation 93–94
for electrons 53
Ionization current 39, 49
Iron-56 89
Lens of the eye 80, 85

164 / INDEX
Lineal energy (y) 7, 40, 45, 47,
87, 123–124
Linear energy transfer (LET) 30,
45, 48, 89, 92, 115–116, 124
restricted (L�) 89, 115–116
unrestricted (L�) 30, 45, 48, 92,
124
Lithium fluoride, doped with
magnesium and titanium
(LiF:Mg,Ti) 9, 99–105,
107–109, 112–113
annealing 99–100
cross section for neutron
interaction 99
deconvoluting glow curve into
component parts 100–101
dependence on particle energy
and charge 105
dose response to high-LET
radiation 100–103
dose response to low-LET
radiation 100–103
efficiency function 103–105
glow curve 100–105
high temperature ratio
102–103
isotopic abundance of lithium
99
response to high-energy protons
102–104
Lithium fluoride, doped with
magnesium, copper and
phosphorus (LIF:Mg,Cu,P) 9,
107–109, 113
glow curve 107–109
Low-Earth orbit 5, 15–16, 29–34
albedo electrons 34
charged target fragments 32,
34
coronal mass ejections 30
Earth’s magnetic field 29
galactic cosmic radiation (GCR)
32, 34
high-energy secondary
fragments 32
high-inclination flights 29
high-inclination orbit 16
light nuclear particles 5, 31–32,
34
low-inclination flights 29
neutrons 33–34
pions 32
protons 34
radiation environment 29–30
radiation measurements 33–34
reentrant electrons 31, 34
secondary charged fragments
34
solar cycle 29
solar protons 31–32
solar wind 29
South Atlantic Anomaly (SAA)
29
splash albedo electrons 31
summary for particle types 33
trapped electrons 30, 34
trapped radiation belts 30
Mean absorbed dose in an organ
or tissue (DT) 6, 18–19, 35, 42,
124
calculation procedure 35
Mean, or effective, linear energy
transfer 111–112
Microdosimetry 87
Mir Space Station 15, 52
Molecular profiling 65
Muons 112
National Voluntary Laboratory
Accreditation Program
(NVLAP) 56–57
Neon 108
Neutrons 5, 10, 20, 33, 40, 44, 58,
84, 102
albedo neutrons 5, 33, 84
energy ranges for calibration of
measurements 58
fission spectrum neutrons 20
radiation transport codes 40
secondary particles 33
Occupancy factors 7, 41
Occupational dose 5

INDEX / 165
Occupational Safety and Health
Administration (OSHA) 24
Operational radiation monitoring
7
area monitors 7
personal dosimeters 7
Optically stimulated
luminescence dosimeter (OSLD)
8–9, 50, 54, 110
Al2O3:C 9, 50, 54
dependence on LET 54
determination of low-LET
component 50
Orbital precession 85
Organ dose equivalent (HT) 4, 7,
19, 22, 36, 124
calculation procedure 36
Oxygen-16 89
Particle spectrometers 9, 39–40,
44, 46, 48, 54, 92
Passive devices 10, 49–52, 54, 55
direct estimate of effective dose
(E) 52
direct ion storage dosimeters 51
electronic dosimeters 49
limitations 49
optically stimulated
luminescent dosimeter
(OSLD) 49, 50
plastic nuclear track detector
(PNTD) 49, 51–52,
radiophotoluminescence (RPL)
glass dosimeters 50
superheated drop/bubble
dosimeters 52
thermoluminescent dosimeters
(TLD) 49, 50, 51
uses 49
Peak-height-ratio method 50
Personal dosimeters 6, 8, 10, 40,
43–44, 53, 54–55, 124
onboard readout 10
optically stimulated
luminescent dosimeters
(OSLD) 54
plastic nuclear track detectors
(PNTD) 44, 54
readout capabilities 55
recommendations 54–55
thermoluminescent dosimeters
(TLD) 44, 54
Photons 40, 44, 112
radiation transport codes 40
Plastic nuclear track detectors
(PNTD) 9, 44, 46, 51–52, 54,
113, 115–121
cellulose nitrate 51
dependence of response on
angle of incidence 46, 52
description of method 115–116
design and characteristics
51–52
determination of high-LET
component 51–52
dosimetry of cosmic radiation
fields 117–121
high-energy protons 121
HZE particles 121
neutron dosimetry 116–117
particle tracks 115–116
response to high-LET particles
46
polyallyl diglycol carbonate
(PADC) 9, 51
polycarbonate 51
proton response 116
Pions 32
Polyallyl diglycol carbonate
(PADC) 9, 113, 116–121
calibration 117
comparison of LET spectrum
and tissue equivalent
proportional counters (TEPC)
119
dependence of response on
angle of incidence 118
determination of dose
equivalent (H) 118
electrochemical etching
116–117
energy dependence 116
LET response 117
LET threshold 117
neutron dose equivalent (H)
response 120–121

166 / INDEX
personal dosimetry systems
120–121
proton response 116
Polycarbonate 120
Polyethylene (CH2) 71
Positrons 5
Prematurely condensed
chromosomes (PCC) 62, 64–65
Previous occupational exposure
81
Protons 5, 10, 31, 38, 44, 58, 101,
108, 112
energy ranges for calibration of
measurements 58
target fragments 31
trapped radiation models 38
Quality assurance 57
Quality factor (Q) 4, 20, 22, 55,
124
as a function of linear energy
transfer 22
Radiation belt 3
Radiation detriment 21
cancer mortality 21
heritable effects 21
nonfatal cancer 21
Radiation environment 5
Radiation Health Officer (RHO)
2, 26
role in management of dose 26
Radiation protection principles 67
applied to low-Earth orbit
(LEO) missions 67
as low as reasonably achievable
(ALARA) 67
individual dose limits 67
justification 67
Radiation-related health study 23
Radiation safety program 1–3, 15,
22–25, 66–76
administrative levels 24–25
as low as reasonably achievable
(ALARA) 24–25, 66–76
astronauts 24, 73–74
dose limit 24
extravehicular activity (EVA)
25
flight director 24–25
flight rules 24–25
flight surgeon 24–25
immediate dose management
66–76
lines of authority 67
management 24, 66–76
objectives 15, 23
organizational structure 67
preplanning 69
Radiation Health Officer (RHO)
24–25
radiation safety training 72–76
Space Radiation Analysis
Group (SRAG) 24–25
Radiation safety records 77–83,
124
annual report to astronaut 81
content of records 78–80
continuity over time 82
definition 77
dosimetry records 77
existing records 82
files linked to the dosimetry
record 79–80
future adjustment of records
82–83
maintenance 78
missing information 79
objectives 77
prospective and retrospective
studies 81–82
records of career doses 80
retention 83
unanalyzed data files 82
updates of records 80
Radiation safety training 12–13,
72–76
astronaut 12
flight director 12, 74
flight surgeon 12, 75
other individuals 12
Radiation Health Officer (RHO)
12, 75
radiation safety professionals
12

INDEX / 167
radiation safety support groups
75
supporting specialists 76
wearing of personal dosimeters
13, 71, 73
Radiation transport calculations
6, 42–45, 47, 95, 97
anthropomorphic models 6
radiation transport code,
HZETRN 97
radiation transport equations
95
radiation transport models 45,
47
Radiation weighting factor (wR)
18, 22, 124
Radiophotoluminescence (RPL)
glasses 50
Recommended value of the
relative biological effectiveness
(Ri) 18
Record keeping 7
Reentrant electrons 31, 124
Refractive index 93
Relative biological effectiveness
(RBE) 20, 36, 87, 124–125
Relativistic electrons 16–17
Restricted linear energy transfer
(L�) 89, 115–116
Retrospective dosimetry 23
Secondary particles 44–45
Semiconductor detectors 91–93
as a personal dosimeter 92–93
design and operation 91–92
particle telescopes 92
position sensitive solid-state
detectors 92
Shielding models 6, 39
extravehicular activity (EVA)
suits 6, 39
International Space Station
(ISS) 6, 39
Space Shuttle 6, 39
Silicon-28 89
Skin 80
Solar cycle 16–17
Solar particle event (SPE) 3, 16,
85, 125
Solid-state detectors 8, 47–48, 53
design and characteristics
47–48
Sources of exposure 4, 5
background radiation 5
biomedical research 4
diagnostic and therapeutic
medical procedures 5
occupational 5
South Atlantic Anomaly (SAA)
16, 47, 53
Space Radiation Analysis Group
(SRAG) 2, 27
implementation of as low as
reasonable achievable
(ALARA) 27
role in management of dose 27
Space-related biomedical research
23
Splash albedo electrons 31, 125
Stochastic effects 4, 18, 125
lifetime excess risk of cancer 18
Stopping power ratios 86
Superheated drop/bubble
dosimeters 52
design and characteristics 52
Ten-year career limits 21
age at exposure 21
female 21
male 21
other than ten-year career
length 21
Thermoluminescent dosimeters
(TLD) 8–9, 33, 41, 44, 46,
50–51, 54–55, 99–114
Al2O3:C 108
CaF2:Tm 9, 50, 51, 54, 99
correction of response for high-
LET radiation 54
dependence of response on
angle of incidence 46
dependence on LET 54
dependency on particle type
and energy 46

168 / INDEX
determination of low-LET
component 50
discrimination between high-
and low-LET particles 113
evaluation of absorbed dose (D)
and dose equivalent (H)
110–114
glow curves 111–112
high temperature ratio 111
LiF:Mg,Cu,P 9, 50, 54, 107–108
LiF:Mg,Ti 9, 50, 54, 99–105
peak-height-ratio method 50
uncertainty in absorbed dose
(D) estimate 112
variation in efficiency 50
Tissue equivalent proportional
counters (TEPC) 7, 44–45, 47,
53–55, 86–91, 112
charged-particle equilibrium 90
design and characteristics 47
distributions of lineal energy
(y) 89
dosimetry of mixed fields 87
estimation of absorbed dose (D)
90
estimation of dose equivalent
(H) 90
estimation of LET 91
model for HZE particles 89–90
operation 86
regulation of gas 86
response for constant LET 88
sensitivity to neutrons 91
simulation of small tissue
volumes 86–87
Tissue exposure fields 41
human shielding models 41
occupancy factors 41
Tissue weighting factor (wT) 4,
19–20, 125
Trapped electrons 30, 85
Trapped protons 84
Unrestricted linear energy
transfer (L�) 30, 45, 48, 92, 124
U.S. Department of Energy
Laboratory Accreditation
Program (DOELAP) 56–57