Embed Size (px)
Citation preview

I. INTRODUCTION
Cholecystectomy is the surgical removal of the gallbladder. Despite the
development of non-surgical techniques, it is the most common method for treating
symptomatic gallstones, although there are other reasons for having this surgery done.
Each year more than 500,000 Americans have gallbladder surgery. Surgery options
include the standard procedure, called laparoscopic cholecystectomy, and an older more
invasive procedure, called open cholecystectomy. A cholecystectomy is performed when
attempts to treat gallstones with ultrasound to shatter the stones or medications to
dissolve them have not proven feasible.
Gallbladder disease is cured by removal of the gallbladder in a procedure
referred to as a cholecystectomy—the most common surgical procedure performed on the
biliary tract. A cholecystectomy is performed to relieve the gastrointestinal distress
common in patients with acute or chronic cholecystitis (with or without gallstones); it
also removes a source of recurrent sepsis. Persistent infection in the biliary tract may
cause recurrent stones.
Open cholecystectomy is a surgery in which the abdomen is opened to permit
cholecystectomy -- removal of the gallbladder. This operation has been employed for
over 100 years and is a safe and effective method for treating symptomatic gallstones,
ones that are causing significant symptoms. At surgery, direct visualization and palpation
of the gallbladder, bile duct, cystic duct, and blood vessels allow safe and accurate
dissection and removal of the gallbladder. Intra-operative cholangiography has been
variably used as an adjunct to this operation. The rate of common bile duct exploration
for choledocholithiasis (gallstones in the bile duct) varies from 3% in series of patients
having elective operations to 21% in series that include all patients. Major complications
of open cholecystectomy are infrequent and include common duct injury, bleeding,
biloma, and infections.
With an open abdominal cholecystectomy, the gallbladder is usually exposed
through a right subcostal incision (Kocher incision) that may be extended over to the
midline at the level of the xiphoid. The incision should be adequate for good exposure of
the gallbladder and bile ducts. After exploration of the abdominal cavity, laparotomy
packs are used to wall off the surrounding organs for exposure. The bilious contents of
the gallbladder may be aspirated to prevent bile from spilling into the peritoneal cavity - a
potential source of peritonitis, especially if the gallbladder is inflamed and tightly
distended. The cystic duct, cystic artery, hepatic ducts, and common bile duct are
accurately identified.
Open cholecystectomy is the standard against which other treatments must be
compared and remains a safe surgical alternative.
The student chose this case study in the hope of gaining more insights,
realizations and helpful theory to lessen the vivacity of the disease, the surgery and its
post operative management of the patient as well as of imparting basic knowledge on the
disease process of cholecystitis, its medical management, the factors contributing to its
occurrence and the normal anatomy & physiology of the affected system. And lastly, may
this study serve as a comprehensive tool for better understanding of the nurse’s role in the
incidence of such case that may help her develop new skills in rendering holistic nursing
care.
II. OBJECTIVES
GENERAL OBJECTIVE
After 5 days of giving holistic nursing care, the patient and the significant others
will be able to gain knowledge, skills, and attitude in the care of the member who
undergone an open cholecystectomy.
SPECIFIC OBJECTIVES
After 5 days of student nurse - patient interaction, the student nurse will be able
to:
1. make a thorough assessment about the patient’s personal history, family
background, and lifestyle.
2. identify predisposing and precipitating factors that have contributed to the
patient’s present condition.
3. review the normal anatomy and physiology of the gallbladder.
4. discuss the pathophysiology of acute calculous cholecystitis.
5. identify the physiologic problems manifested by the patient.
6. formulate a comprehensive nursing care plan in the care for patient with
acute calculous cholecystitis.
8. implement health teachings for the improvement of the patient’s well being.
2. evaluate patient’s reaction, state or condition after are implementation of
care plan.
After 5 days of student nurse - patient interaction, the patient will be able to:
1. state information about self, family background, and history of condition
2. express feelings, perceptions and fears that cause disturbance.
3. verbalize physiologic, psychologic discomforts and other needs.
4. cooperate on the interventions to be rendered by the student nurse.
5. develop skills in immediate nursing measures on incidences of discomfort
or occurrences of possible complications.
6. develop self-care to the fullest possible level.
7. apply the learned nursing measures in her activities of daily living.

III. NURSING ASSESSMENT
1. PERSONAL HISTORY
1.1 Patient’s Profile
Name: Balansag, Nicolas
Age: 46 years old
Sex: Male
Civil Status: Married
Religion: Roman Catholic
Date of Admission: Aug. 8, 2007
Room No.: 424
Complaints: right upper quadrant pain,
general abdominal pain for 1 month
Diagnosis: Acute Calculous Cholecystitis
Physician: Dr. Bernadette Moscoso
1.2 Family and Individual Information, Social and Health History:
Mr. Balansag is residing at Dona Rita Village 1C Compound, Banilad,
Cebu City with her wife and their 2 daughters. Patient is working as a mechanic at Don
Bosco School. Patient is an occasional alcoholic drinker, a slight smoker which consumes
around 3 sticks per day. He has no known allergy to food and drugs. Patient is known to
be hypertensive at the age of 40. His usual blood pressure is 140/90 and has a highest
blood pressure of 160/100. He has been taking his maintenance drug for his BP which is
the Neobloc.
Patient had an STD during his 20’s. Patient is non-diabetic and non-asthmatic.

Patient complains of general abdominal pain for 1 month now and
that he hasn’t been able to sleep well because of the pain felt in his right upper
quadrant. He seek consult to Dr. Moscoso thus advised to be admitted to Cebu
Doctors’ Hospital on April 7, 2007.
1.3 Level of Growth and Development
1.3.1 Normal Development at Particular Stage
Physical Development
Integumentary system, appropriate distribution of pigmentation, slow
progressive decrease in skin turgor, skin turgor and moisture decrease, subcutaneous fat
decreases and wrinkling occursfatty tissue is redistributed, resulting in fat deposits in the
abdominal area, hair begins to thin, and gray hair appears.
Respiratory system, Anteroposterior diameter increased, respiratory rate
16-21 breaths per minute, normal tactile fremitus, resonance and breath sounds heard
throughout.
Cardiovascular System, Blood vessels lose elasticity and become thicker,
normal heart sounds (systole-S, < S2 at the base; diastole-S, > S2 at the apex), point of
maximal impulse at fifth intercoastal space in the mid-clavicular line and 2cm or less in
diameter, blood pressure: systolic 95 to 140 mmHg, diastolic 60 to 90 mmHg, all pulses
are palpable.
Reproductive System, normal penis and scrotum, prostatic enlargement in
some men, the climacteric (andropause) refers to the change of life in men, when sexual
activity decreases, androgen levels decrease very slowly.
Musculoskeletal System. Thinning of the intervertebral discs causes a
decrease in height of about 1 inch. Calcium loss from bone tissue is more common
among postmenopausal women. Muscle growth continues in proportion to use, decreased
muscle mass, pathologic fractures resulting from osteoporosis, decreased range of joint
motion.

Sensory Changes. Visual acuity declines, often by the late 40s, especially
for near vision (presbyopia),visual acuity by Snellen chart < 20/50, pupillary reaction to
light and accommodation, normal visual fields and extraocular movements, normal retina
structures, auditory acuity for high-frequency sounds decreases (presbycusis), particularly
in men, normal auditory structures and acuity, patent nares and intact sinuses, mouth and
pharynx, trachea at midline, lateral thyroid lobes and nonpalpable, taste senasations
diminish.
Psychosocial Development
Is in the generativity versus stagnation phase of Erikson’s stages of
development. Accept aging body. Feel comfortable and respect self. Enjoy new freedom
to be independent. Self seems more altruistic, and concepts of service to others and love
and compassion gain prominence. Accept changes in family roles (e.g., having teenaged
children and aging parents). Interact well and share companionable activities with life
partner. Expand and renew previous interests. Pursue charitable and altruistic activities.
Have meaningful philosophy of life. These concepts motivate charitable and altruistic
actions, such as church work, social work, political work, community fund raising drives,
and cultural endeavors. The middle-aged person looks older and feels older. People
usually accept the fact that they are aging; however, a few try to defy the years by
changing their dress and even their actions.
Cognitive development
Reaction time during the middle years stays much the same or diminishes
during the later part of the middle adulthood. Memory and problem solving are
maintained through middle adulthood. Learning continues and can be enhanced by
increased motivation at this time in life. Middle-aged adults are able to carry out all the
strategies. Some may use postformal operations strategies to assist them in understanding
the contradictions that exist in both personal and physical aspects of reality. The middle-

aged adult can “ reflect on the past and current experience and can imagine, anticipate,
plan and hope” (Muray and Zentner,2001, p.722)
Spiritual Development
In middle age, people tend to be less dogmatic about religious beliefs, and
religion often offers more comfort to the middle-aged person than it did previously.
People in this stage rely on spiritual beliefs to help them deal with illness, death and
tragedy. At this stage, the individual can view “truth” from a number of viewpoints.
1.3.2 The Ill Person at a Particular Stage of Patient
Physiological concerns for the middle adult include stress, level of
wellness, and formation of positive health habits.
Because middle adults are experiencing physiological changes and
face certain health realities, their perceptions of health and health behaviors
are often important factors in maintaining health.
Attention to risk factors that can be altered to improve the client's
health such as stress, obesity, use of tobacco, excessive alcohol consumption,
poor nutrition, and unsafe sexual practices, can increase the quality of life and
add years to it.
Anxiety is a critical maturational phenomenon related to change,
conflict, and perceived control of the environment. Adults often experience
anxiety in response to the physiological and psychosocial changes of middle
age. Depression that occurs during the middle years is commonly
characterized by moderate-to-high anxiety and physical complaints.
Chronic illnesses such as hypertension, diabetes mellitus, cancer may
affect the roles and responsibilities assumed by the middle adult. Strained
family relationships, modifications in family activities, increased health care
tasks, increased financial stress, the need for housing adaptation, social
isolation, medical concerns, and grieving may also result from chronic illness.
The degree of disability and the client's perception of both the illness and the
disability determine the extent to which lifestyle changes will occur. A few
examples of the problems experienced by clients who develop debilitating
chronic illness during adulthood include role reversal, changes in sexual
behavior, and alterations of self-image.

2. Diagnostic results
Radiology Department:
Operative Cholangiography
Remarks: Calcified galstones
Persistent filling defects in the common bile duct suggestive of radiolucent
Chest PA
Remarks: No significant cardiopulmonary finding
Ultrasound
Remarks: Cholelithiases, biliary tract obstruction secondary to choledocholothiasis
The rest of abdomen are unremarkable
Surgical Pathology / Cytology Report
Specimen:
GALLBLADDER
Remarks: Chronic calcolous cholecystitis
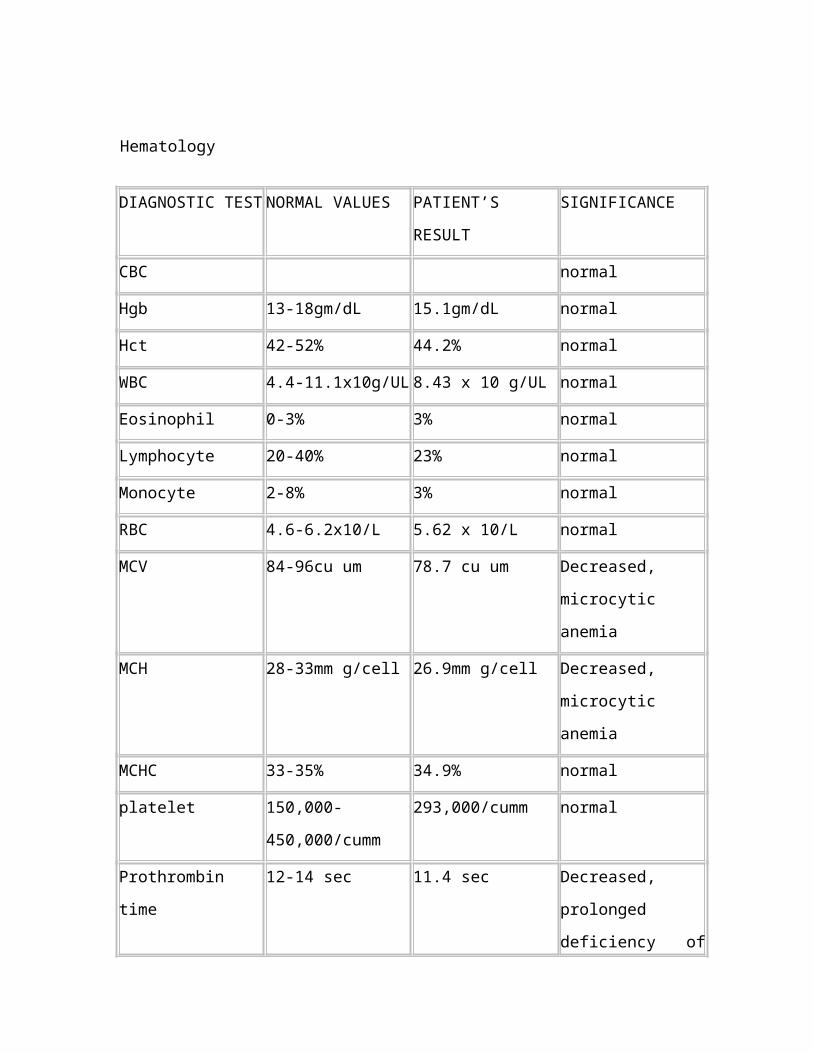
Hematology
DIAGNOSTIC TEST NORMAL VALUES PATIENT’S RESULT SIGNIFICANCE
CBC normal
Hgb 13-18gm/dL 15.1gm/dL normal
Hct 42-52% 44.2% normal
WBC 4.4-11.1x10g/UL 8.43 x 10 g/UL normal
Eosinophil 0-3% 3% normal
Lymphocyte 20-40% 23% normal
Monocyte 2-8% 3% normal
RBC 4.6-6.2x10/L 5.62 x 10/L normal
MCV 84-96cu um 78.7 cu um Decreased, microcytic
anemia
MCH 28-33mm g/cell 26.9mm g/cell Decreased, microcytic
anemia
MCHC 33-35% 34.9% normal
platelet 150,000-450,000/
cumm
293,000/cumm normal
Prothrombin time 12-14 sec 11.4 sec Decreased, prolonged
deficiency of factor
I,II,V,VII,X,fat
metabolism, severe
liver disease.
Conrol 10-14 sec 12.3 sec normal
Glucose blood 65-110mg/g: 94 mg/g normal
Phosphatase alkaline 38-126 U/L 251 U/L Increased, hepatic
disease
SGPT 11-66U/L 291 U/L Increased, hepatic
disease
3. Present Profile of Functional Health Pattern (Pre-operatively)
3.1 Health Perception / Health management
Before the diagnosis, the patient already complains of on and off tolerable pain
with a scale of 6 from 1-10 pain scale. Felt at the epigastric region radiating to back, that
would last for around 10 to 20 seconds. Pain is described as constant, aggravated usually
after eating relieved by rest and relaxation in bed and pain relievers. The patient has
described his health as poor, due to the known diagnosis at present, since he is aging, he
admits of some limitations in his activities as compared to his past health status. As of
now, he feels fine except from his experience of pain and reduced activity. Patient says
that he never tried any attempts of dieting or any weight loss programs; he had an apple
juice therapy. He is not completely immunized.
3.2 Nutritional-Metabolic Pattern
Prior to admission, patient’s meals usually consist of rice and dried fish, and
often pork during lunch and dinner time and usually eat bread with coffee during
breakfast. For his snacks he eats banana or bread. His fluid intake is about 8 glasses a day
and says that he drinks apple juice and carbonated drinks often. He does not have any
problems with his appetite. The patient takes in Shilintong tab a Chinese medicine as his
daily supplements and he often drinks 4 glasses/day of apple juice. His weight has not
changed for the last six months and he does not have any problems with his ability to eat
such as swallowing or chewing liquids and solids. He is currently on NPO status prior to
scheduled surgery tomorrow.
3.3 Elimination Pattern
Patient reports of very dark colored urine. He does not make use of any assistive
devices. He used to defecate once a day. He says that the usual characteristics of his
stools are clay colored, hard and well-formed. Patient does not make use any assistive
device. Patient has a good skin turgor but has jaundice and pruritus.

3.4 Activity / Exercise Pattern
Patient does not do routine exercises and considers household chores to be one of
his exercises. In addition, he also walks daily. He can ambulate freely.
3.5 Cognitive / Perceptual Pattern
Patient says that he has no hearing problems except for his visual acuity, since he
no longer sees fine fonts clearly without his glasses. He said that he used to wear glasses,
but unfortunately his glasses got lost. He does not use any hearing aids and he complains
of dizziness at times.
3.6 Rest / Sleep Pattern
He usually sleeps at 11:00 midnight and wakes up at around 7:00 am until now,
that he is hospitalized. He has problems with sleeping early, so he usually drinks a warm
cup of milk and some biscuits.
3.7 Self-perception Pattern
He is concerned about getting well and as much as possible be free of any illness,
but it does not bother him that well. Being ill has not changed or made him feel different
about himself although for him, aging has indeed led him to be more health conscious.
3.8 Role-relationship Pattern
He is married, a father of two children and is currently living with his eldest son
and grandchildren. He makes decisions with the help of his children.
3.9 Sexuality-Reproductive Pattern
The patient is being open minded to the things with regards to sexuality. He is
already a middle age adult and has no problem about his sexuality and his activities

regarding his life. He knows that he must start practicing good hygiene. Now he has
sexual activities for some time.
3.10 Coping ?Stress Tolerance Pattern
He usually sleeps at long hours or watch television when he feels tired. He makes
decisions together with his children. He is already retired, and says that he does not want
to change anything with his life. When is tense or under stress, he seeks help from his
children.
3.11 Value-belief System
The patient as well as significant others is a Roman Catholic. Patient claims to be
attending masses regularly but is inactive in any spiritual groups or activities.

IV. PATHOPHYSIOLOGY AND RATIONALE
The Normal Anatomy and Physiology of the Organ Affected
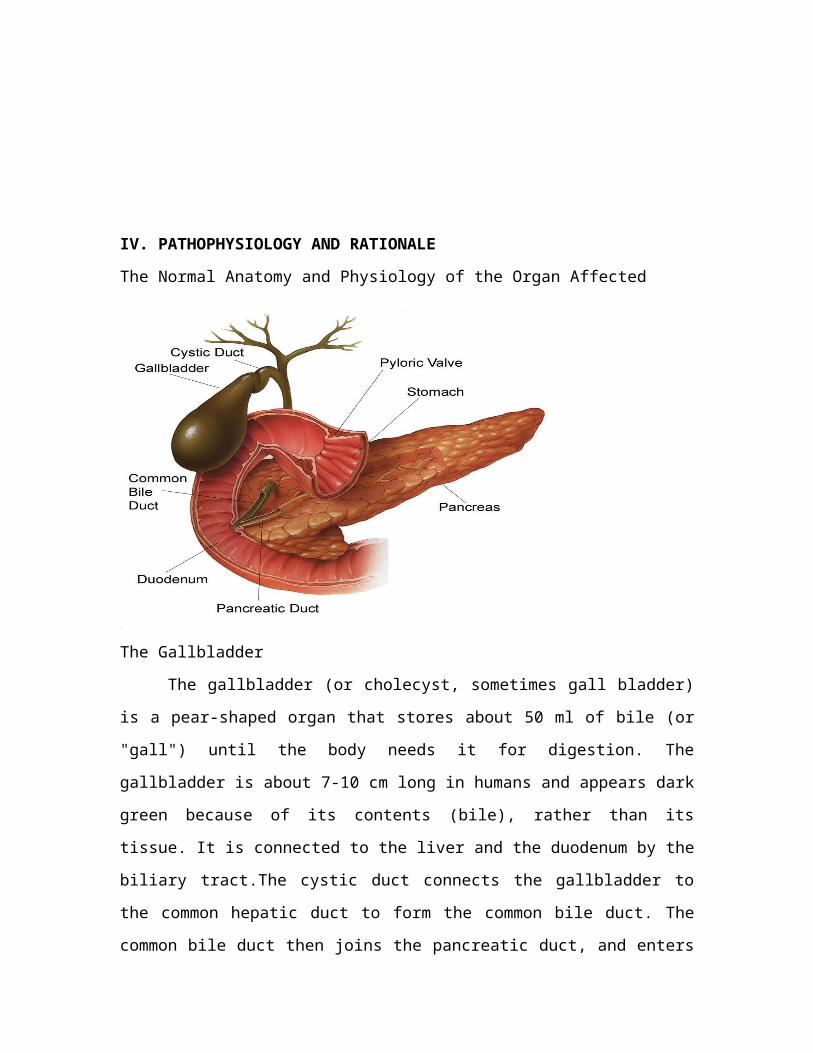
The Gallbladder
The gallbladder (or cholecyst, sometimes gall bladder) is a pear-shaped organ that
stores about 50 ml of bile (or "gall") until the body needs it for digestion. The gallbladder
is about 7-10 cm long in humans and appears dark green because of its contents (bile),
rather than its tissue. It is connected to the liver and the duodenum by the biliary tract.The
cystic duct connects the gallbladder to the common hepatic duct to form the common bile
duct. The common bile duct then joins the pancreatic duct, and enters through the
hepatopancreatic ampulla at the major duodenal papilla.
The gallbladder stores about 50ml of bile (1.7 US fluid ounces / 1.8 Imperial fluid
ounces), which is released when food containing fat enters the digestive tract, stimulating
the secretion of cholecystokinin (CCK). The bile, produced in the liver, emulsifies fats
and neutralizes acids in partly digested food.After being stored in the gallbladder, the bile
becomes more concentrated than when it left the liver, increasing its potency and
intensifying its effect on fats. Most digestion occurs in the duodenum.
4.2 DISEASE PROCESS AND ITS EFFECTS ON DEIFFERENT ORGAN/SYSTEM
Cholecystitis is a medical condition, in which gallbladder’s wall becomes inflamed, and
is usually caused by a gallstone in the cystic duct, that results in an attack of abrupt
severe pain. At least 95% of the patients with Cholecystitis have gallstones. In very rare
cases, a bacterial infection results in inflammation. Cholecystitis starts with sudden, sharp
pain in the upper abdomen. In most cases this medical condition is very severe and may
cause perforation of the gallbladder or gangrene. Prompt surgery is needed to remove the
diseased gallbladder. The symptoms of acute cholecystitis include pain in the right upper
area of the abdomen and it is a 1st sign of inflammation of the gallbladder. The pain may
become worse when a patient is breathing deeply and frequently extends to the lower area
of the right shoulder blade. Vomiting and nausea are common. A patient usually
experiences sharp pain when a physician presses the upper right area of the abdomen.
During a several hours, the muscles of the abdomen on the right side can become rigid.
At beginning, the patient can have only slight temperature, but later it tends to become
high. Usually Acute Cholecystitis attack is subsiding in two or three days and fully
disappears in 7 days. If it does not, the individual can have severe complications such as
high fever, gangrene, gallbladder perforation, shivering, and others. Prompt surgery is
required for these conditions. Acute Cholecystitis usually accompanied by jaundice or a
backup of bile into the liver, showing that the common bile duct can be partially
obstructed by inflammation or gallstone. If blood tests determine a higher level of the
enzyme amylase, a patient can have pancreatitis (pancreas inflammation), resulted from
gallstone obstruction of the pancreatic duct. Diagnosis of Acute Cholecystitis depends on
the patient’s symptoms and the results of specific tests. Ultrasound scan may help to
determine the presence of gallstones in the gallbladder and may show thickening of the
wall of gallbladder. The procedure called Hepatobiliary Scintigraphy provides more
accurate diagnosis. In this test, images of liver are taken, as well of galbladder, upper
portion of the small intestine and bile ducts. A patient with Acute Cholesystitis usually is
hospitalized, getting intravenous electrolytes and fluids, and not permitted eat or drink.
Physician can pass a tube through the nose and into the stomach, so that suctioning may
be used to maintain stomach empty and thus reduce gallbladder stimulation. Antibiotics

are given as soon as Acute Cholecystitis is suspected. If the diagnosis of acute
gallbladder inflammation is confirmed and the risk of operation is small, the gallbladder
is usually taken out within 1 or 2 days of the disease, but if a patient has another disease
that increases the surgery’s risk, the operation can be delayed until that illness is treated.
If Acute Cholecystitis attack subsides, the gallbladder can be taken out later approx after
1 1/2 months or more. If such side effects like gangrene, gallbladder perforation, abscess
occur, prompt surgery is usually required. Some individuals have recurring or new
incidences of pain that feel like Acute Cholesystitis attack even though they have no
gallbladder. The cause of these incidences is unknown, but they cab be caused by a
defected function of the sphincter of Oddi - the opening, that releases bile into the small
intestine. Pain is suggested to be caused by increased pressure in the duct resulted from
resistance to the bile flow or secretions of pancreatis. In some individuals, small
gallstones, which are remains after operation, can result in pain. Physician may use an
endoscope to widen the sphincter of Oddi. This procedure generally relieves symptoms in
patients with abnormal sphincter, but does not help people who only experience pain.
4.3 Classical and Clinical/Actual Symptoms (Pre-operatively)
Classical Symptom Clinical Symptom Rationale
Pain and Biliary Colic
Jaundice
Manifested
patient feels the pain
on her right upper
quadrant of her
abdomen
score of 6/10 in a
pain scale
facial grimace noted
pain radiates to the
back
Manifested
The skin of the
patient is slightly
yellowish in color.
Itching on the
extremities
If a gallstone obstructs the
cystic duct, the gallbladder
becomes distended,
inflamed, and eventually
`infected. The patient may
have biliary colic with
excruciating upper right
abdominal pain that radiates
to the back or right
shoulders, is usually
associated with nausea and
vomiting and is noticeable
several hours after a heavy
meal.
Jaundice occurs in a few
patients with gallbladder
disease and usually occurs
with obstruction of the
common bile duct. The bile
which is no longer carried
to the duodenum, is
absorbed by the blood and
gives the skin and mucous
membrane a yellow color.
This is frequently
accompanied by marked
Changes in Urine and Stool
Color
Vitamin Deficiency
Manifested
grayish stools
Tae colored urine
Not Manifested
itching of the skin.
The excretion of bile
pigments by the kidney give
the urine a very dark color.
The feces, no longer
colored with bile pigments,
are grayish, like putty and
usually described as clay-
colored.
Obstruction of the bile flow
also interferes with the
absorption of fat-soluble
vitamins A, D, E, K.
Therefore the patient may
exhibit deficiencies (eg,
bleeding caused by vitamin
K deficiency, which
interferes with normal
blood clotting) of these
vitamins if biliary
obstruction has been
prolonged.
4.4 Schematic Diagram of the of the Pathophysiology of Cholelithiasis
Precipitating Factors Predisposing Factors
- excessive fat ingestion - sex (female)
- decreased bile acid synthesis - age above 40 years old
- increased cholesterol synthesis - fertile women (estrogen)
in the liver - frequent weight changes
- infections in the biliary tract
Bile supersaturated with cholesterol
Bile forms into gallstones
Gallstones acts as an irritant
Inflammatory changes in the gallbladder
Clinical Manifestations
- Pain and Biliary Colic
- Jaundice
- Changes in urine and stool color
- Vitamin deficiency (A,D,E,K)
Medical Management Surgical Management Nursing Management
- NGT insertion- Antibiotic theraphy- Parenteral Fluids-Analgesic- Lithotripsy
-Laparoscopic Cholecystectomy- Open cholecystectomy
- rest for the client-monitoring client’s ability to digest bland diet.-observe for increased pain, shock, or signs of internal bleeding.
Present Profile of Functional Health Pattern (Post-operatively)
1 Health Perception / Health management
Patient appears tired as he has slow guarded movements and could only speak minimally. Discomforts of postoperative surgery were evident as the patient felt pain, constipation and feeling of weakness. However, he verbalizes that he is happy for a successful operation, and describes his health better, now that he is slowly recovering.
2 Nutritional-Metabolic Pattern
He is currently under NPO but is allowed to take sips of water and usually nibbles on some crackers.
3 Elimination Pattern
Patient is currently using a Foley bag catheter with 50cc urine,JP drain with 20cc of drainage and T tube with 15cc of drainage during the morning shift of her second post operative day. He has not defecated yet. Patient’s skin exhibits good color and turgor, stable temperature and no edema noted.
4 Activity / Exercise Pattern
Patient is found lying in bed and still asks assistance from significant others for help. He can change positions, as he complains. He looks tired. Before admission he exercises by walking and doing household chores.
5 Cognitive / Perceptual Pattern
He used to have glasses. He can read and write. However, as of now, he is tired and rests in bed most of the time
6 Rest / Sleep Pattern
Patient was seen sleeping most of the time after the surgical procedure.
7 Self-perception Pattern
He is much concerned of his health now. His present health goal is to get well as soon as possible after a successful surgery.
8 Role-relationship Pattern
His eldest son, who is currently working as a drug representative, helps him in the care and financial aspect of his present health condition.
9 Sexuality-Reproductive Pattern
He had just undergone Open Cholecystectomy.
10 Coping-Stress Tolerance Pattern
He is currently resting since he feels tired after the operation.
11 Value-belief System
For him, his condition had not changed his faith in God, however it has even
increased his faith since he believes that this is part of God뭩 purpose for him and that he
trusts God in his healing.

Classical and Clinical/Actual Symptoms (Post-operatively)
Classical Symptom Clinical Symptom Rationale
Pain and Biliary Colic
Jaundice
Not manifested
Manifested
Still the skin of the
patient is slightly
yellowish in color.
Itching on the
extremities
If a gallstone obstructs the
cystic duct, the gallbladder
becomes distended,
inflamed, and eventually
`infected. The patient may
have biliary colic with
excruciating upper right
abdominal pain that radiates
to the back or right
shoulders, is usually
associated with nausea and
vomiting and is noticeable
several hours after a heavy
meal.
Jaundice occurs in a few
patients with gallbladder
disease and usually occurs
with obstruction of the
common bile duct. The bile
which is no longer carried
to the duodenum, is
absorbed by the blood and
gives the skin and mucous
membrane a yellow color.
Changes in Urine and Stool
Color
Vitamin Deficiency
Not manifested
Not Manifested
This is frequently
accompanied by marked
itching of the skin.
The excretion of bile
pigments by the kidney give
the urine a very dark color.
The feces, no longer
colored with bile pigments,
are grayish, like putty and
usually described as clay-
colored.
Obstruction of the bile flow
also interferes with the
absorption of fat-soluble
vitamins A, D, E, K.
Therefore the patient may
exhibit deficiencies (eg,
bleeding caused by vitamin
K deficiency, which
interferes with normal
blood clotting) of these
vitamins if biliary
obstruction has been
prolonged.
V. Nursing Intervention
Relieving pain
The location of the subcostal incision in nonlaparoscopic gallbladder surgery disease
is likely to cause the patient to avoid turning and moving, to splint the affected site, and
to take shallow breaths to prevent pain. Because full exacerbation of the lings and
gradually increased activity are necessary to prevent postoperative complications, the
nurse should administer analgesic agents as prescribed to relieve pain and promote well-
being.
Improving respiratory status
Patients undergoing biliary tract surgery are prone to pulmonary complications, as are
all abdominal incision. Thus, the nurse remind patient to take deep breaths and cough
every hour to expand the lungs fully and prevent atelectasis.
Monitoring and Managing Potential Complications
Bleeding may occur as a result of inadvertent puncture or nicking of major blood
vessel. Post-operatively, the nurse closely monitors vital signs and inspects the surgical
incision and drains, if in place, for evidence of bleeding.
Improving Nutritional Status
The nurse encourages the patient to eat a diet low in fats and high in carbohydrates
and proteins especially after surgery. At the time of hospital discharge, these are usually
no special dietary instructions other than to maintain a nutritious diet and avoid excessive
fats. Fat restriction usually is lifted in 4-6 weeks when the biliary ducts dilate to
accommodate the volume of bile once held by the gallbladder and when the ampulla of
Vater again functions affectively.
Promote Skin and Biliary Drainage
In patient who have undergone cholecystectomy, the drainage tubes must be
connected immediately to a drainage receptacle. The nurse fasten tubing to the dressing,
with enough leeway for the patient to move without dislodging.
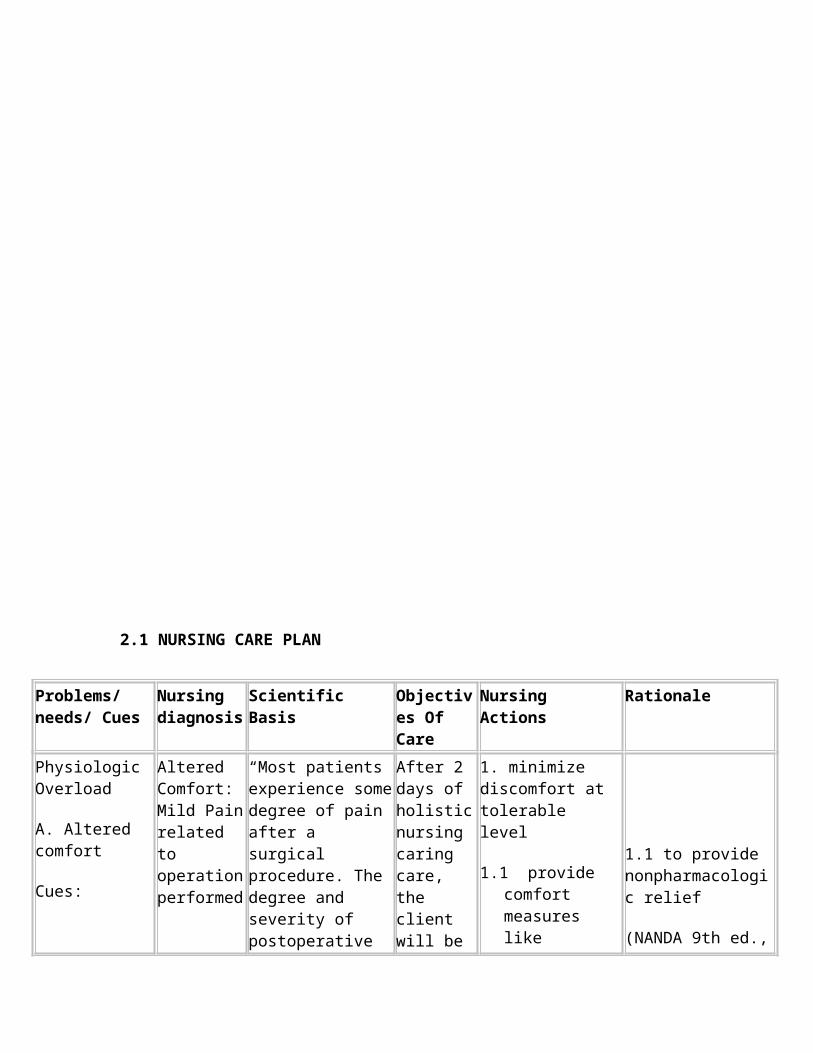
2.1 NURSING CARE PLAN
Problems/needs/ Cues
Nursing diagnosis
Scientific Basis Objectives Of Care
Nursing Actions Rationale
Physiologic Overload
A. Altered comfort
Cues:
-pain
-facial grimace
-guarded movements
-presence of operative wound
-throbbing pain on the abdomen radiating to the lower back lasting for 2-5 minutes that is aggravated by sudden movement but relieved by massage of surrounding areas and pain medication
“sakit man ang gi-operahan dong” as said by the patient
Altered Comfort: Mild Pain related to operation performed
“Most patients experience some degree of pain after a surgical procedure. The degree and severity of postoperative pain and the patient’s tolerance for pain depend on the incision site, the nature of the surgical procedure, the extent of surgical trauma, the type of anesthetic agent and how the agent was administered.”
Source: Medical-Surgical Nursing by Suzanne C. Smeltzer and Brenda G. Bare; 9th edition
p.355
After 2 days of holistic nursing caring care, the client will be able to:
1. minimize discomfort at tolerable level
1. minimize discomfort at tolerable level
1.1 provide comfort measures like therapeutic touch
1.2 perform assessment each time pruritus occurs
1.3 accept client’s description of itching
1.4 encourage adequate rest periods
1.5 perform tepid sponge bath
1.6 modify environment like using electric fan
1.7 review procedures to client like blood transfusion and sponge bath
1.8 advise client to wear loose clothing
1.9 provide diversional activities
1.1 to provide nonpharmacologic relief
(NANDA 9th ed., p.368)
1.2 to monitor progress of condition
(NANDA 9th ed., p.367)
1.3 it is a subjective experience and differs from others
(NANDA 9th ed., p.367)
1.4 to prevent fatigue
(NANDA 9th ed., p.369)
1.5 to prevent further itching and aid in healing process
(Potter and Perry, Fundamentals of Nursing p. 1062)

like social interaction, hanging out in the garden
1.10 administer medications as ordered
1.6 to provide comfort and relaxation
(NANDA 9th ed., p.368)
1.7 to reduce concern of the unknown and stress
(NANDA 9th ed., p.368)
1.8 itching may be initiated by physical substance
(Medical-Surgical Nursing by Black, 7th ed., p. 1394)
1.9 to relieve mind of discomfort
(NANDA 9th ed., p.368)
1.10 to medicate prophylactically as appropriate
(NANDA 9th ed., p.368)
Physiologic deficit
B Impaired Skin Integrity
Cues:
-incision site on abdomen 3-5 cm
Impaired skin integrity: presence of surgical incision related to operative procedure
“Surgery interrupts the integrity of the skin surface providing a potential portal of invasion of bacterial”
Medical-surgical Nursing p.1573 by Lemone and Burke ;10th edition
2. manifest timely wound healing as evidenced by the absence of dehiscence and evisceration
Measures to:
2. promote good wound healing
2.1 monitor site of impaired tissue integrity and determine etiology
2.1 Poor assessment of wound etiology is critical for proper identification of nursing interventions (Source: Nursing Care Plans by Doenges)
2.2 wound assessment is more reliable when

-dressing on site present
-bleeding still present on surgical site
-skin seems a dry and wrinkly
-“bag-o pa man ko gi-operahan dong” as verbalized by the client
2.2 determine size and depth of wound
2. 3.monitor site of impaired tissue integrity
2.4.monitor status of skin around wound, monitor client’s skin, practices, noting type of soap or other cleansing agents used and temperature of water
2.5 avoid massaging around site of impaired tissue integrity and over bony prominences
2.6 assist with general comfort and hygiene measures
2.7 maintain infection control standards
2.8 emphasize need of adequate nutrition or fluid intake of 8 – 10 glasses/day
2.9 reassess signs of infection
3.0 administer medications as ordered
performed by the same caregiver, the client is in the same position and same techniques (Source: Nursing Care Plans by Doenges)
(Source: Nursing Care Plans by Doenges)2.3 identify impending problems easily (Source: Nursing Care Plans by Doenges)(Source: Nursing Care Plans
2.4 individualize plan according to client’s skin condition, needs and preferences, avoid harsh cleansing agents, hot water and extreme friction. (Source: Nursing Care Plans by Doenges)
2.5 research suggests that massage may lead to deep tissue trauma (Source: Nursing Care Plans by Doenges)
2.6 to promote comfort and sense of well being (Source: Nursing Care Plans by Doenges)
2.7 to decrease risk of infection (Source: Nursing Care Plans by

Doenges)
2.8 to maintain general good health and skin turgor
(NANDA 9th ed., p.467)
2.9 to ensure free of infection(NANDA 9th ed., p.467)
3.0 to provide pharmacologic relief (NANDA 9th ed., p.467)
Physiologic Deficit
C. Activity Intolerance
Cues:
-difficulty in feeding herself
-tired looking eyes
-can’t walk without assistance
-thin looking appearance
-client has undergone surgery
Activity intolerance: difficulty in feeding herself related to weak muscle strength
After surgery, the body needs extra calories and protein for wound healing and recovery. At this time, many people have some pain and fatigue. In addition, they may be unable to eat a normal diet because of surgery-related side effects.
http://www.cancer.org
Perform activities of daily living at a tolerable level
3. Perform activities of daily living at a tolerable level
3.1 assess emotional / psychological factors
3.2 evaluate current limitations/degree of deficit in light of usual
3.3 cluster activities
3.4 increase activities or exercise gradually
3.5 plan care with rest periods between activities
3. 6 assist with activities and monitor use of assistive devices
3.1 stress and/or depression may be increasing the effect of an illness, or depression might be the result of being forced into inactivity
(NANDA 9th ed., p.61)
3.2 provides comparative baseline
(NANDA 9th ed., p.61)
3.3 to prevent overexertion
(NANDA 9th ed., p.61)
3.4 to conserve energy
(NANDA 9th ed., p.62)
3.5 helps to minimize frustration, rechannel

3.7 promote comfort measures and provide relief of pain
3.8 review expectations of client and/or significant others
3.9 assist client to learn and demonstrate appropriate safety measures
3.10 encourage client to maintain positive attitude
energy
(NANDA 9th ed., p.62)
3.6 to protect client from injury
(NANDA 9th ed., p.62)
3.7 enhance ability to participate in activities
(NANDA 9th ed., p.62)
3.8 to establish individual goals
(NANDA 9th ed., p.62)
3.9 to prevent injuries
(NANDA 9th ed., p.62)
3.10 to enhance sense of well-being
(NANDA 9th ed., p.63

SOAPIE CHARTING
SOAPIE NO.1
DAY 1(Aug 23, 2007)
S- “maayung buntag dong, o ugma na lagi ang schedule sako operation, nakuyawan ko,
unsaon diay ko ana?”as verbalized by the patient
O- seen patient lying on bed awake, conscious. With IV #3 with IVF D5LR 1L @
30gtts/min at the left hand. The patient’s temperature is 36.9 degrees Celsius, respiratory
rate of 20 breaths per minute, pulse rate of 80 beats per minute. The patient appears weak
and anxious as evidenced by frequent asking of questions about his surgery.
A- Knowledge Deficit related to unfamiliarity of the surgical procedure.
P- to encourage verbalizations about the understanding of the surgical procedure
I- introduced self to the patient, established rapport with the patient and significant
others, informed the patient of the surgery to be performed the following day, explained
the nature of the surgery(cholecystectomy), enumerated different preoperative care prior
to the surgery, cited some possible rare complications, explained what will happened
after the surgery, reassured the patient that he is in safe hands that the surgical team will
do their best
E- the patient was able to understand simple information about his operation and was able
to decreased his fear about the operation by saying “salamat dong, nakuhaan gamay
akong kulba”
SOAPIE NO.2
DAY 2(Aug 24, 2007)
S- “sakit ang akong samad” as verbalized by the patient
O- received a 46 y.o. male patient with wound dressing at the abdominal area, dry and
intact, with IVF D5LR 1L @ 30gtts/min at the left hand, lying in bed, weak and tired,
complains of throbbing pain felt at surgical site lasting from 2-5 minutes, located in the
right quadrant of the abdomen, sharp throbbing pain, aggrevated by sudden movements,
relieve by rest and proper positioning and pain medication, facial grimace noted
A- Altered Comfort: Mild Pain related to operation performed
P- minimize discomfort at tolerable level
I- assisted in transferring the patient to the Post Anesthesia care Unit, after care done-
assessed the dressing of the patient for presence of drainage, maintained comfortable and
calm environment, removed any instruments like stethoscope from the patient’s bed,
raised side rails of the bed to protect the patient, placed pillow on the side of the bed to
limit head movement of the patient, regulated IV line, changed patients gown, transferred
patient from the operating table to the stretcher,

E- Noted relief from pain after and experience comfort after interventions are
implemented as evidenced by the verbalization of the client. “ maagwanta na gamay ang
sakit, dili pareha ganiha”
2.4 Health Teaching Plan
Name of Patient: Mr. Balagtas, Nicolas
Age: 46 years old
Room No. 424
HEALTH TEACHING PLAN
OBJECTIVES CONTENTS METHODOLOGY EVALUATION
General Objectives
After 1 day of nurse-patient interaction the client will be able to gain knowledge, attitude and skills in the care for postoperative patients of Open Cholecystectomy.
Specific Objectives:
After 30 minutes of student nurse-client and significant others interaction, the client and the significant others will be able to:
1. define cholecystitis and cholelithiasis to their level of understanding.
2. cite importance of wound dressing
1. Definition of cholecystitis and cholecystectomy
Cholecystitis – acute inflammation of gallbladder
Cholelithiasis – calculi or gallstones, usually form in the gallbladder from solid constituents of bile.
2. Importance of wound dressing
2.1. treatment for wounds, ulcers and recalcitrant dermatitis
2.2.create an optimal environment for healing
Informal discussion
Sharing
The patient listened attentively and was able to understand the meaning of wound dressing, shared some importance of wound dressing.He was able to cooperate follow the right procedure of wound dressing, identified bed rest as a comfort measure to relieve pain, asked questions about wound dressing, demonstrated proper breathing techniques.

V. Evalutation and Recommendation
Evaluation:
The patient responded well to the care being rendered by the health care team. Both
nursing and medical interventions and health teachings contributed to the steady recovery
and improvement of the health condition of the patient. The client and the significant
others have partaken their part in utilizing the health teachings being taught by the
student nurse. The student nurse was able to accomplish all the objectives and health care
plan formulated for the client and thus there was a positive outlook in life by the client.
The prognosis is very good.
Recommendation:
The student nurse would like to suggest that the patient be consulted regularly by a
gynecologist for check up about the health condition of the client after surgery and
discharge from the health care facility.
On the other hand, the patient’s family must also be very supportive of her and should
help her meet more of her emotional and psychological needs since she is already old.
Though the family may be in a financial crisis, several non-government organizations
may be able to provide some extent of help.

Lastly, proper compliance of medication as ordered is also a very vital factor in
restoring the client’s former physiologic state.
VI. Evaluation and Implication of this Case Study To:
Nursing Practice
This case study provides information about chronic calculous cholecystitis and its
treatment which includes surgery. In this case, the surgery performed is open
cholecystectomy. This case study would serve as a help to the nursing practice since it
provides an appropriate plan of care for patients who undergo this operation for efficient
nursing care.
Nursing Education
To the nursing education, this case study would help in sharing data or information about
the disease condition, which is chronic calculous cholecystitis, and its management as
well as the preoperative and postoperative nursing interventions needed for the promotion
of patient’s recovery. With these, the students as well as the teachers would gain
additional information about the disease and patient’s condition so that it would equip
them for an efficient nursing care in the future.
Nursing Education
This case study would help in the nursing research as a source of data for example, in
tracking the population of persons with this condition. With this information, it would

make us aware of its growing incidence rate and the need to treatment and share the
importance of early detection or early prevention of this disease condition.
VII. Referral and follow-up
With proper compliance to medications and treatments prescribed, further complications
would be prevented. In contrast, patient must be alert for complications such as signs of
infection, hemorrhage. If signs occur, patient must refer to surgeon immediately. In
addition, follow-up visits are also recommended for continuous monitoring to ensure a
smooth recovery.

VIII. Bibliography
Black, Joyce M., et.al. Medical Surgical Nursing. 6th ed. Philadelphia: W.B. Saunders
Company. 2001, pg 991-994
Kozier, Barbara, et.al. Fundamentals of Nursing: Concepts, Process, and Practice. 7th ed.
USA: Pearson Education, Inc. 2004, p.629-636
Smeltzer, Suzanne C., Bare, Brenda G.. Brunner and Suddarth’s textbook of Medical
Surgical Nursing. 7th ed. USA: J.B. Lippincot Company. 1992. p. 1275, 1989-2006
Wilson, Kathleen J.W., Waugh, Anne. Ross and Wilson Anatomy and Physiology. 8th ed.
London. Churchill Livingstone. 1999. pg.
http://www.medterms.com/script/main/art.asp?articlekey=39742
http://www.healthatoz.com/Atoz/common/standard/transform.jsp?
requestURI=healthatoz/Atoz/ency/cholecystectomy.jsp)
http://www.surgerychannel.com/cholecystectomy/
http://www.consciouschoice.com/1999/cc1201/hmd1201.html






![Left Sided Laparoscopic Cholecystectomy: Case Report and ...open cholecystectomy - before laparoscopic era [2] and 1 case in 2008 [3] and about 50 cases of laparoscopic cholecystectomy](https://img.pdfslide.us/doc/110x75/5f6509906579645fd7227a11/left-sided-laparoscopic-cholecystectomy-case-report-and-open-cholecystectomy.jpg)