Embed Size (px)
Citation preview

Physiotherapy rehabilitation forwhiplash associated disorder II:a systematic review and meta-analysis ofrandomised controlled trials
Alison Rushton,1 Chris Wright,1 Nicola Heneghan,1 Gillian Eveleigh,1
Melanie Calvert,1 Nick Freemantle2
ABSTRACTObjective: To evaluate effectiveness of physiotherapymanagement in patients experiencing whiplashassociated disorder II, on clinically relevant outcomesin the short and longer term.
Design: Systematic review and meta-analysis. Tworeviewers independently searched informationsources, assessed studies for inclusion, evaluated riskof bias and extracted data. A third reviewer mediateddisagreement. Assessment of risk of bias wastabulated across included trials. Quantitativesynthesis was conducted on comparable outcomesacross trials with similar interventions. Meta-analysescompared effect sizes, with random effects as primaryanalyses.
Data sources: Predefined terms were employed tosearch electronic databases. Additional studies wereidentified from key journals, reference lists, authorsand experts.
Eligibility criteria for selecting studies: Randomisedcontrolled trials (RCTs) published in English before 31December 2010 evaluating physiotherapy managementof patients (>16 years), experiencing whiplashassociated disorder II. Any physiotherapy interventionwas included, when compared with other types ofmanagement, placebo/sham, or no intervention.Measurements reported on $1 outcome from thedomains within the international classification offunction, disability and health, were included.
Results: 21 RCTs (2126 participants, 9 countries)were included. Interventions were categorised asactive physiotherapy or a specific physiotherapyintervention. 20/21 trials were evaluated as high risk ofbias and one as unclear. 1395 participants wereincorporated in the meta-analyses on 12 trials. Inevaluating short term outcome in the acute/sub-acutestage, there was some evidence that activephysiotherapy intervention reduces pain and improvesrange of movement, and that a specificphysiotherapy intervention may reduce pain. However,moderate/considerable heterogeneity suggested thattreatments may differ in nature or effect in differenttrial patients. Differences between participants,interventions and trial designs limited potential meta-analyses.
ARTICLE SUMMARY
Article focus- Physiotherapy intervention is recommended in
whiplash associated disorder II, although themost beneficial intervention and the effectivenessof physiotherapy management are unclear.
- Systematic reviews have not focused on whip-lash associated disorder II, which representsapproximately 93% of patients presenting formanagement post-whiplash injury.
- The objective of this systematic review was toevaluate the effectiveness of physiotherapymanagement in patients experiencing whiplashassociated disorder II, on clinically relevantoutcomes in the short and longer term.
Key messages- This systematic review demonstrates inconclu-
sive very low/low quality evidence for theeffectiveness of physiotherapy management forwhiplash associated disorder II.
- There is potential benefit for improving pain andrange of movement short term through activephysiotherapy and for improving pain throughspecific physiotherapy interventions.
- This potential benefit merits further considerationin a properly powered clinical trial with attentionto ensure low risk of bias.
Strengths and limitations of this study- The strengths of this review are its focus to
physiotherapy intervention and the mostcommon whiplash associated disorder II classi-fication requiring physiotherapy intervention.
- A limitation is that differences between partici-pants, interventions and trial designs limitedpotential meta-analyses.
- Surprisingly, no chronic interventions werecomparable for analysis, considering the highnumber of patients experiencing chronicity withwhiplash associated disorder.
To cite: Rushton A, Wright C,Heneghan N, et al.Physiotherapy rehabilitationfor whiplash associateddisorder II: a systematicreview and meta-analysis ofrandomised controlled trials.BMJ Open 2011;1:e000265.doi:10.1136/bmjopen-2011-000265
< Prepublication history andadditional tables for thispaper are available online. Toview these files please visitthe journal online (http://bmjopen.bmj.com).
Received 26 July 2011Accepted 30 September 2011
This final article is availablefor use under the terms ofthe Creative CommonsAttribution Non-Commercial2.0 Licence; seehttp://bmjopen.bmj.com
1School of Health andPopulation Sciences, Collegeof Medicine and Dentistry,University of Birmingham,Edgbaston, Birmingham, UK2Department of Primary Careand Population Health, UCLMedical School (Royal FreeCampus), London, UK
Correspondence toDr Alison Rushton;[email protected]
Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265 1
Open Access Research
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

Conclusions: Inconclusive evidence exists for the effectiveness ofphysiotherapy management for whiplash associated disorder II.There is potential benefit for improving range of movement and painshort term through active physiotherapy, and for improving painthrough a specific physiotherapy intervention.
INTRODUCTIONRoad traffic accidents are the primary cause of whiplash,a soft tissue injury to the neck following an accel-erationedeceleration mechanism of injury.1 The cumu-lative incidence of patients seeking healthcare post-whiplash from a road traffic accident has increased duringthe last 30 years to recent estimates of>3/1000 inhabitantsin North America and Western Europe2 and 1.0e3.2/1000inhabitants in Sweden.3 In the UK, insurance statisticsindicate that 300000 patients present per annum withwhiplash associated disorders.4 Whiplash associated disor-ders are the resulting clinical presentations following theinjury and can range in severity, clinical symptoms andphysical findings.1 Many patients with whiplash associateddisorders experience persistent pain and disability, withreports suggesting that 40e60% of those injured havechronic symptoms.5e8 The annual economic cost associ-ated with management of whiplash associated disordersand associated time off work is estimated as $3.9 billion inthe USA,9 and V10 billion in Europe.10
Patients experiencing whiplash associated disordersmay be regarded as a distinct group within the broadernon-specific neck pain population,1 2 7 11e13 althoughfollowing review of trial data (n¼4 trials), recentevidence questions this distinction for a primary carepopulation and has identified a need for furtherresearch.14 Whiplash associated disorders can be cate-gorised as grades 0eIV,1 where a higher grade indicatesincreased severity. The classification system is widelyused in clinical practice15 and guidelines.16 Patientswith whiplash associated disorder II who experienceneck pain accompanied by stiffness or tenderness, andmusculoskeletal signs, for example a reduced range ofavailable movement, form the major group of patients(93.4%)15 who might benefit from conservativemanagement, commonly involving physiotherapy inter-vention. A recent best evidence synthesis3 recom-mended a focus of research to the most commonwhiplash associated disorder I and II classifications,excluding classification III and above (ie, patients withneurological signs and fracture and/or dislocation) andclassification 0 (no complaint at the neck, and nophysical signs).1 However, a classification of whiplashassociated disorder I is less commonly seen by physio-therapists as there are no accompanying physical find-ings (neck pain, stiffness or tenderness but with nophysical findings) and patients are known to recoverwithin 6 months post-injury.15
Evidence of the effectiveness of physiotherapy inter-vention for the treatment of whiplash associated
disorder II is scarce. Existing systematic reviews insteadtend to focus on a range of whiplash associated disorderclassifications and a broad range of conservativeintervention strategies such as educational videos,include studies of non-traumatic neck pain, and lackrigorous assessment of the risk of bias of includedstudies. The most robust evidence, a Cochrane review,17
on the management of whiplash associated disorder I/IIpatients does not specifically assess physiotherapy. Noreview has included trials published post-2006. Theeffectiveness of physiotherapy for the whiplash associ-ated disorder II population is therefore unclear.The objective of this systematic review was to investi-
gate the short and longer term effectiveness of physio-therapy outpatient management of patients presentingwith whiplash associated disorder II, in terms of func-tion, disability and health,18 in patients aged >16 years.
MATERIALS AND METHODSA systematic review was conducted according toa predefined protocol based on the method guidelinesof the Back Review Group of the Cochrane Collabora-tion19 and the Cochrane handbook.20 It is reported inline with the PRISMA statement.21
Eligibility criteriaStudiesRandomised controlled trials (RCTs) evaluating theeffectiveness of physiotherapy outpatient managementof patients experiencing whiplash associated disorder IIwere included. Studies not written in English wereexcluded rather than restricting the inclusion of studies,thereby providing information of potential bias.22 Norestrictions were placed on publication date.
ParticipantsPatients aged >16 years who had experienced a whiplashinjury, classified as whiplash associated disorder II, wereincluded. Acute and chronic presentations wereincluded and analysed separately. Mixed populations ofdifferent classifications of whiplash associated disorderwere included if patients presenting with whiplash asso-ciated disorder II formed part of the population.
InterventionsAny physiotherapy outpatient management interventionwas included.
Outcome measuresMeasures addressing domains within the internationalclassification of function, disability and health,18 in theshort term (approximately 3 months post-injury/inter-vention) and/or longer term (approximately12 months) were included.
Information sourcesEach of the following databases was searched usingsensitive topic based search strategies to the end ofDecember 2010:
2 Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

< The Cochrane Library: Controlled Trials Register,Health Technology Assessment Database, NHSEconomic Evaluation Database.
< CINAHL, EMBASE, MEDLINE, PEDro, ZETOC data-bases.
< Selected internet sites and indexes: Turning Researchinto Practice, Health Services/Technology Assess-ment, PUBMED.
< National Research Register, Current Controlled Trialswebsite (York).
< Cochrane Back Review Group.< Cochrane Cervical Overview Group.< Hand searches in key journals, for example Spine,
Manual Therapy, Physiotherapy, Physical Therapy, Austra-lian Journal of Physiotherapy.
< Science Citation Index and Social Science CitationIndex.
< Unpublished research22: British National Bibliog-raphy for Report literature, Dissertation Abstracts,Index to Scientific and Technical Proceedings,National Technical Information Service, System forInformation on Grey Literature.
< Personal citations for key authors in the field.The searches used predefined terms. Box 1 provides
two examples of the searches utilised.
Study selectionTwo subject experts independently searched informa-tion sources (GE/NH), and independently assessedidentified studies for inclusion by grading each criterion
Box 1 Examples of search strategies
Medline (Ovid) 1948e31 December 20101. Acute whiplash or cervical spine disorder or cervicalspine injury.mp2. Manual therapy or manipulation or massage.mp3. Clinical trial or randomised controlled trial or RCT.mp4. 1 and 25. 3 and 46. WAD II or whiplash associated disorders or whiplashinjury or whiplash patients or whiplash syndrome.mp7. 2 and 68. 3 and 79. Conservative approach or conservative intervention orconservative management or conservative therapy.mp10. Physical approach or physical intervention or physicalmanagement or physical therapy.mp11. Exercise or active range of motion exercise$ orstrengthening exercise$ or stretching exercise$ or thera-peutic exercise$ or endurance training or home exercise$ orproprioception exercise$12. Transcutaneous electrical nerve stimulation or TENS orthermotherapy or electrical stimulation or heat or electro-therapy.mp13. Pain management program$.mp14. Patient education or educational or self managementprogram$.mp15. Posture or (postural and balance) or traction.mp16. 1 and 917. 3 and 1618. 6 and 919. 3 and 1820. 1 and 1021. 3 and 2022. 6 and 1023. 3 and 2224. 1 and 1125. 3 and 2426. 6 and 1127. 3 and 2628. 1 and 1229. 3 and 2830. 6 and 1231. 3 and 30
Embase (Ovid) 1947e31 December 20101. Acute whiplash or cervical spine disorder or cervicalspine injury.mp2. Manual therapy or manipulation or massage.mp3. Clinical trial or randomised controlled trial or RCT.mp4. 1 and 25. 3 and 46. WAD II or whiplash associated disorders or whiplashinjury or whiplash patients or whiplash syndrome.mp7. 2 and 68. 3 and 79. Conservative approach or conservative intervention orconservative management or conservative therapy.mp10. Physical approach or physical intervention or physicalmanagement or physical therapy.mp
Box 1 Continued
11. Exercise or active range of motion exercise$ orstrengthening exercise$ or stretching exercise$ or thera-peutic exercise$ or endurance training or home exercise$ orproprioception exercise$12. Transcutaneous electrical nerve stimulation or TENS orthermotherapy or electrical stimulation or heat or electro-therapy.mp13. Pain management program$.mp14. Patient education or educational or self managementprogram$.mp15. Posture or (postural and balance) or traction.mp16. 1 and 917. 3 and 1618. 6 and 919. 3 and 1820. 1 and 1021. 3 and 2022. 6 and 1023. 3 and 2224. 1 and 1125. 3 and 2426. 6 and 1127. 3 and 2628. 1 and 1229. 3 and 2830. 6 and 1231. 3 and 30
Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265 3
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

(table 1) as eligible/not eligible/might be eligible.19
A study was potentially relevant and its full text wasobtained, when it could not be unequivocally excludedon the basis of its title and abstract22 following discussionbetween the two independent reviewers. In a situation ofdisagreement or when abstracts contained insufficientinformation, the full text was obtained. A study wasincluded in the review when both reviewers indepen-dently assessed it as satisfying the inclusion criteria fromthe full text. If agreement was not obtained, a thirdreviewer (AR, subject and methodological expert)mediated following discussion.19
Risk of bias was independently assessed by the samereviewers for each included study. Risk of bias, andhomogeneity of participants, interventions andoutcomes were key considerations informing thepotential for including trials in meta-analyses, in linewith Cochrane.20 The third reviewer again mediated.20
Agreement between reviewers was evaluated usingCohen’s k.23 All processes and tools were piloted.
Data collection processTwo reviewers (AR/CW) independently extracted thedata20 24 using a standardised form. A third independentreviewer (NH) checked for consistency and clarity.
Data itemsData extracted for each trial included: design, partici-pants and indication, whiplash associated disordercategorisation, interventions, study setting, outcomemeasures, timing of assessments, power calculations, lossto follow-up, intention to treat analyses and main results.Key outcome measures were predefined as valid tools tomeasure pain, disability, function, physical impairment,social impact and patient satisfaction, reflecting domainsfrom the International Classification of Functioning,Disability and Health.18 Based on recommendations,a maximum of two primary outcomes were consideredacceptable,25 when more than one primary outcome wasreported and alpha spend was not considered.
Risk of bias in individual studiesThe Cochrane ‘risk of bias’ assessment tool was used toappraise the internal validity of each included trial.21 26
In contrast to the majority of quality scales used in healthresearch,21 27 28 the Cochrane tool is informed byempirical research.26 Each component of bias wasreported independently and considered with regard toeach key outcome measure.26 29 The componentincluding ‘blinding’ the treating therapist has beenacknowledged as generally impossible26 and this formedpart of the appraisal by the reviewers as the Cochranetool also permits evaluation of the likely influence of anylack of blinding. The rigour of the risk of bias assessmentwas ensured through strict application of the definedcriteria to inform conclusions, making explicit the trialsof high risk of bias or poor reporting.30
Summary measuresQuantitative synthesis was conducted in line with theprotocol on comparable key outcomes across trialsevaluating similar interventions (nature of intervention,and timing of assessments at approximately 3 monthsand/or 12 months post-injury or intervention). Resultswere reported in the context of overall risk of bias.Comparable outcomes were defined as tools developedto measure the same underlying domain. Two subjectexperts and two methodological experts identified thecombinations of studies and outcomes on which toconduct meta-analyses.
Table 1 Criteria for inclusion and exclusion of studies inthe review
Criteria
Inclusion criteriaStudy design RCTPopulationAge 16 years or olderSubjects Human; outpatientsCondition Post-whiplash injury
Experiencing whiplashassociated disorder II
Intervention Conservative physiotherapyoutpatient management
Comparisongroup(s)
At least one comparisongroup: placebo/otherintervention/no intervention
Outcome Measurement of at least oneof the following outcomes:disability; functional status;physical impairment; impacton social and occupationallevels of fitness; pain; qualityof life; patient satisfactionMeasurement of short termoutcome (approx 3 monthspost-surgery) and/or longterm outcomes ($1 yearpost-surgery)
Time frame All studies conducted from1979 onwards
Exclusion criteriaStudy design Initial search: studies stated
as RCTs but do not have acomparison group or randomallocation to groups
Participantcharacteristics
Multiple pathologyWhiplash associated disordernot classified according toseverity to provide clarity ofwhiplash associated disorderII population
Intervention NoneOutcome NoneLanguage Full article not written in
English
RCT, randomised controlled trial.
4 Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

Using RevMan,31 meta-analyses compared stand-ardised differences in means using DerSimonianeLairdrandom effects32 for the principal analyses to allow forsystematic differences in effects estimated across theincluded trials.22 32 For summary statistics, 95% CIs werereported. Standardised mean differences were selectedto make comparisons across studies that used differenttools to measure the same outcome,22 or reporteda mixture of final value scores and change from baselinescores.33 HedgeseOlkin fixed effects34 were used as thesupportive analyses.
Planned methods of analysisData were requested from all authors, except for thosewith no comparability of outcome measures to othertrials.35 36 Data defined by whiplash associated disorderclassification was also requested from all authors of trialsthat reported combined whiplash associated disorderclassifications. Analyses were conducted on finalsummary statistics when reported or the raw data wheresupplied. When necessary, standard deviations wereestimated from reported CIs or percentiles.33 In linewith the use of random effects as primary analyses,32
change scores were used for studies when no other datawere forthcoming. Heterogeneity in treatment effectswas evaluated through computation of I2.
Risk of bias across studiesA summary assessment for risk of bias was tabulatedacross studies, and consensus agreed concerning theoverall potential risk of bias. It was not helpful to attemptto assess potential publication bias visually usingFunnel plots22 as less than 10 trials were included inmeta-analyses.37
Additional analysesNo post-hoc supportive analyses were conducted owing tothe inconsistency of outcome measures across the trials.
RESULTSStudy selectionIncluded trials were grouped according to the whiplashassociated disorder classification1 into five categories:< Whiplash associated disorder II: five articles and five
trials,36 38e41 from four countries were included.< Whiplash associated disorders I/II: eight articles and
eight trials,42e49 from six countries were included.< Whiplash associated disorders II/III: four articles and
four trials,35 50e52 from three countries wereincluded.
< Whiplash associated disorders 0/I/II: three articles andtwo trials,53e55 from two countries were included.
< Whiplash associated disorders I/II/III: three articles andtwo trials,56e58 from one country were included.Most retrieved trials were published in English with
only two in other languages. One relevant unpublishedstudy was found (Managing Injuries of the Neck Trial,accessible at http://www.hta.ac.uk/1399, due to bepublished 2011). Figure 1 presents the numbers of
studies at each stage of selection. Complete inter-reviewer agreement was achieved on study inclusionacross all categories following discussion.
Study characteristicsDescriptive data for the 21 included trials are summar-ised in online table 1.
MethodsEighteen trials randomised participants across twogroups, one trial across three groups, and two trialsacross four groups. Eight trials compared a specificphysiotherapy intervention, for example manipulation,to no management, sham or placebo. Thirteen trialscompared an active physiotherapy intervention to stan-dard care; the active approaches were characterised byadditional interventions, a multimodal intervention ora progressive intervention. Duration of interventionsranged from one treatment session to 12 months. Thenumber of assessments varied from 1 to 4, occurringimmediately post-treatment to 3 years.
ParticipantsThe 21 trials randomised 2126 participants. Age variedfrom 16 to 70 years. A total of 271/2126 participantswere randomised in trials focused to whiplash associateddisorder II.i Of the authors who responded, no authorswere able to provide data for their included whiplash
Figure 1 Study selection flow diagram (from Moher et al21).WAD, whiplash associated disorder.
iIn Aigner et al38, three subject experts agreed that the Kramer grade II
evaluated as equivalent to the WADII classification.
Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265 5
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

associated disorder classifications separately. In the eightwhiplash associated disorder I/II category trials, 934participants were randomised but no distinction ofwhiplash associated disorder II participants was possible.In the four whiplash associated disorder II/III categorytrials, 333/409 (81.5%, two trials) participants wereclassified as whiplash associated disorder II; in a further111 participants (two trials), no distinction of whiplashassociated disorder II participants was possible. In thetwo whiplash associated disorder O/I/II category trials,302 participants were randomised with no distinction ofwhiplash associated disorder II participants possible. Inthe two whiplash associated disorder I/II/III categorytrials, 49/66 (74%, 1 trial) participants were classified aswhiplash associated disorder II; in a further 33 partici-pants (1 trial), no distinction of whiplash associateddisorder II participants was possible. A total of 1395participants were randomised in the 12 trials included inthe meta-analyses.
InterventionsEight trials were conducted at single centres that includedphysiotherapy clinics or outpatient departments. Botha clinic and home setting were used in one trial. Thesetting was unclear in 12 trials. One trial investigateda group intervention. Interventions could be groupedaccording to whether they were a specific physiotherapyintervention or an active intervention comprisingdifferent components. Timing of interventions includedacute/sub-acute (13 trials) and chronic stages (8 trials),ranging from 2 days to 15 years post-injury.
Primary outcomesOnly six (28.5%) trials specified primary outcomesa priori that included: Neck Pain and Disability Index,Nociceptive Flexion Reflex, Neck Disability Index, PainVisual Analogue Scale (VAS), Pain VAS and Work Activ-ities VAS, and Pain VAS and Disability VAS. One trial46
specified three primary outcome measures with noadjustment for alpha spend and was therefore evaluatedas unacceptable in specifying primary outcomes.25
Secondary and additional outcomesMost trials reported some assessment of pain (general orspecific to the neck) (15 trials), and range of movement(ROM) (13 trials). Nine trials reported assessment ofdisability. A wide range of other outcomes included:work status, SF36, Tampa, patient satisfaction, musclestability, posture and kinaesthetic sensibility. Two trialsreported outcomes that were not consistent with anyother trial, for example temperature pain threshold36
and the tandem standing balance test.35
Risk of bias within studies‘Almost perfect’59 93% inter-reviewer agreement wasachieved on risk of bias assessment prior to discussion(Cohen’s k¼0.90, p<0.0005) and 100% agreement wasreached following discussion. Only two trial protocols wereavailable.60 61Of the 21 included trials, 20were evaluated as
high risk of bias and one as unclear risk of bias (table 2).The very high proportion of trials identified as high risk ofbias should affect the interpretation of results.26
Risk of bias across studiesOnly trials evaluated as high risk of bias were availablefor meta-analysis. Although reasons for the high riskcomponents provided concern for potential bias, resultsfrom meta-analyses evaluated critically within this contextenabled an overview of the evidence to be presented,strength of effect to be presented, and tentative conclu-sions to be proposed to advance research.
Results of individual studies and synthesis of resultsComparability of interventions, timing of assessmentsand outcome measures were considered to determineappropriate quantitative syntheses of trials.22 Inexploring the compatibility of outcomes for managementin the acute/sub-acute and chronic stages, no possiblequantitative syntheses within the five categories of whip-lash associated disorders were possible. No furtherinformation regarding whiplash associated disorder clas-sification was provided by authors to assist potentialcomparisons regarding whiplash associated disorder II.In comparing across categories, no comparison waspossible for intervention in the chronic stage or longterm. The following meta-analyses were conducted in theacute/sub-acute stage in the short term:< Active intervention versus standard intervention for:
pain, 4e12 weeks (n¼6 trials); ROM flexion/exten-sion (flex/ext), 12 weeks (n¼3 trials); ROM rotation(Rot), 12 weeks (n¼4); ROM side flexion (SF),12 weeks (n¼3); total ROM, 4e12 weeks (n¼3)ii;disability, 6e12 weeks (n¼5).
< Specific intervention versus control post-interventionfor: pain (n¼4 trials)iii; ROM flex/ext, ROM Rot, andROM SF (n¼3 trials).iv
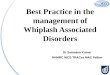
Active versus standard intervention short termEvidence from two trials39 48 suggested that interventionmight reduce pain, with active intervention beingbeneficial compared to standard intervention (figure 2).This was not supported by four trials.42 45 55 56 Thepooled random effects (�0.35, 95% CI �0.63 to �0.07)did support evidence of an effect short term. Evidencefrom one trial43 suggested that intervention mightimprove ROM flex/ext and ROM SF, with active inter-vention being beneficial compared to standard inter-vention (figures 3 and 4). This was not supported by twotrials.42 45 The pooled random effects (ROM flex/ext:0.39, 95% CI 0.04 to 0.74; ROM SF: 0.45, 95% CI 0.17 to0.73) did support evidence of an effect short term.Evidence from three trials43 45 56 suggested that
iiExcluded Rosenfeld et al53 54 as short term assessment was 6 at
months.iiiIncluded Thuile and Walzl47 although timing of intervention and
assessment was unclear from trial.ivAigner et al38 n¼5 loss to follow up but not clear from which group.
6 Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

Table
2Summary
assessmentoftheoverallriskofbiasforeachtrial
Study(authors,year,country)
Components
ofriskofbias
Summary
riskofbias
Comments,highriskcomponents
12
34
5a
5b
6
WAD
IIAigneretal3
8(2006)
UU
UU
UU
HHigh(1)
Unclear(6)
Onehighriskcomponent:6
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
Dehneretal3
9(2009)
LL
UU
UN/A
HHigh(1)
Unclear(3)
Low
(2)
N/A
(1)
Onehighriskcomponent:6
Designproblematicwithcomparisonto
apreviousnon-randomisedgroup.
AssessmentROBexcludedpreviousgroup
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
Gonzalez-Inglesiasetal4
0
(2009)
LL
LL
UN/A
HHigh(1)
Unclear(1)
Low
(4)
N/A
(1)
Onehighriskcomponent:6
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
Julletal4
1(2007)
LL
LL
UN/A
LUnclear(1)
Low
(5)
N/A
(1)
Nohighriskcomponents
Sterlingetal3
6(2010)
LU
LL
UN/A
HHigh(1)
Unclear(2)
Low
(3)
N/A
(1)
Onehighriskcomponent:6
NoITTreported
WAD
I/II
Asketal4
2(2009)
UL
LL
UU
HHigh(1)
Unclear(3)
Low
(3)
Onehighriskcomponent:6
Noprimary
endpointspecified
Bonketal4
3(2000)
UU
HL
UN/A
HHigh(2)
Unclear(3)
Low
(1)
N/A
(1)
Twohighriskcomponents:3,6
3:Assessors
notblindedbeyondbaseline
6:Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
Pato
etal4
4(2010)
UU
LL
UN/A
HHigh(1)
Unclear(3)
Low
(2)
N/A
(1)
Onehighriskcomponent:6
Noprimary
endpointspecified
NoITTreported
Scholten-Peeters
etal4
5
(2006)[Scholten-Peeters
etal6
0(2003)trialprotocol]
LL
LL
LL
HHigh(1)
Low
(6)
Onehighriskcomponent:6
Noprimary
endpointspecified
Con
tinued
Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265 7
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

Table2
Con
tinued
Study(authors,year,country)
Components
ofriskofbias
Summary
riskofbias
Comments,highriskcomponents
12
34
5a
5b
6
Stewartetal4
6(2007),
[Stewartetal6
1
(2003)trialprotocol]
LL
LL
LN/A
HHigh(1)
Low
(5)
N/A
(1)
Onehighriskcomponent:6
Co-interventionsby6weeks:A:n¼1
0(15%)andB:n¼1
5(23%)reported
seekingadditionaltreatm
ent
Co-interventionsby12months:
A:n¼1
8(29%)andB:n¼3
5(56%)
reportedseekingadditionaltreatm
ent
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
Thuile
andWalzl47(2002)
UU
UU
UN/A
HHigh(1)
Unclear(5)
N/A
(1)
Onehighriskcomponent:6
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
Poorreporting,lackingdetailacrossall
components
Vassiliouetal4
8(2006)
LL
LH
UN/A
HHigh(2)
Unclear(1)
Low
(3)
N/A
(1)
Twohighriskcomponent:4,6
4:Lossesat6weeks(6
months):
A:15%
(30%)
B:36%
(46%)
n¼1
2(6%)participants
excludeddue
toincomplete
outcomedata.
6:Noprimary
endpointspecified
Vikneetal4
9(2007)
UL
LH
UU
HHigh(2)
Unclear(3)
Low
(2)
Twohighriskcomponents:4,6
4:Lossesof20%
at12months(10%
at
4months)
6:Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
WAD
II/III
Arm
strongetal5
0(2005)
UU
UL
UN/A
HHigh(1)
Unclear(4)
Low
(1)
N/A
(1)
Onehighriskcomponent:6
Problematicdesignanddata
analysis
combininggroups
Noprimary
outcomemeasure
specified
NoITTreported
Fernandez-de-las-Penas51
(2004a)
LU
UU
UN/A
HHigh(1)
Unclear(4)
Low
(1)
N/A
(1)
Onehighriskcomponent:6
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
Selectionbiasasparticipants
were
volunteers
Con
tinued
8 Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

Table2
Con
tinued
Study(authors,year,country)
Components
ofriskofbias
Summary
riskofbias
Comments,highriskcomponents
12
34
5a
5b
6
Fernandez-de-las-Penas52
(2004b)
LU
UU
UN/A
HHigh(1)
Unclear(4)
Low
(1)
N/A
(1)
Onehighriskcomponent:6
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
Hanssonetal35(2006)
LL
LH
UN/A
HHigh(2)
Unclear(1)
Low
(3)
N/A
(1)
Twohighriskcomponents:4,6
4:Dropouts
38%
6:Differencesatbaselineontwooutcomes
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
WAD
0/I/II
Rosenfeld
etal5
4(2003),
[Rosenfeld
etal(2006)
reportingsametrial]
UL
LH
UU
HHigh(2)
Unclear(3)
Low
(2)
Twohighriskcomponents:4,6
4:Highlossto
follow-up.Dropoutat
6months(and3years):8%
(13%).
Exclusionsat6months(and3years):
11%
(8%).Includeseligibility
errors
with
participants
excludedpost-randomisation
fornotmeetinginclusioncriteria
6:Co-interventions:25%
participants
receivedtreatm
ent
outsideofstudyby6months;nearly
50%
by3years
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
Schnabeletal5
5(2004)
HU
UH
UN/A
HHigh(3)
Unclear(3)
N/A
(1)
Threehighriskcomponents:1,4,6
1:Inappropriate
methodofrandomisation
4:Lossto
follow-upfrom
groups:A:36%
B:15%
6:Noprimary
outcomemeasure
specified
NoITTreported
WAD
I/II/III
Soderlundetal5
6(2000)
UU
UL
UN/A
HHigh(1)
Unclear(4)
Low
(1)
N/A
(1)
Onehighriskcomponent:6
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
SoderlundandLindberg
57(2001),
[SoderlundandLindberg
58(2007)
reportingsametrial]
UU
LL
UN/A
HHigh(1)
Unclear(3)
Low
(2)
N/A
(1)
Onehighriskcomponent:6
Noprimary
outcomemeasure
specified
Noprimary
endpointspecified
NoITTreported
Components
ofriskofbias:
1,sequencegeneratio
n;2,allocationconcealm
ent;3,blindingofparticipants,personnelandoutcomeasse
ssors;4,incomplete
outcomedata;5a,shortterm
selective
outcomereporting;5b,longterm
selectiveoutcomereporting;6,otherpotentia
lthreats
tovalidity.
Levels
ofriskofbias:H,highriskofbias;
U,unclearriskofbias;
L,low
riskofbias.
N/A,notapplicable,noinvestigationoflongterm
outcome.
Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265 9
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

intervention might improve ROM Rot, with activeintervention being beneficial compared to standardintervention (figure 5). This was not supported by onetrial.42 The pooled random effects (0.68, 95% CI 0.38 to0.99) did support evidence of an effect short term.Overall, there was no evidence of short term benefit of
active over standard intervention on total ROM (pooledrandom effects 0.28, 95% CI �0.03 to 0.59) or disability(figure 6: �0.26, 95% CI �0.57 to 0.05).
Specific physiotherapy intervention versus controlEvidence from four trials40 47 51 52 suggested that inter-vention might reduce pain short term, with specificphysiotherapy intervention being beneficial comparedto control. The pooled random effects (�2.11, 95% CI�3.85 to �0.36) did support evidence of an effect shortterm. Overall, there was no evidence of short termbenefit of specific physiotherapy intervention overcontrol on ROM flex/ext (pooled random effects 0.83,95% CI �3.79 to 5.44), ROM Rot (pooled randomeffects �1.02, 95% CI �3.73 to 1.68) or ROM SF (pooledrandom effects �1.21, 95% CI �3.11 to 0.69).
DISCUSSIONSummary of evidenceEvidence was assessed from 21 RCTs (2126 participants)conducted across nine countries. Only one trial inves-tigated a group intervention. Interventions weregrouped into active versus standard intervention, andspecific physiotherapy intervention versus control. Nometa-analyses were possible exclusively on a whiplashassociated disorder II population, as most trials
included combined classifications of whiplash associ-ated disorders in their populations. Disappointingly, asmany trials were recent, 20/21 trials were assessed ashigh risk of bias, and one as unclear risk. All 12 trials(1395 participants from six countries) included in themeta-analyses were assessed as high risk. Comparableoutcomes across trials included pain, ROM flex/ext,ROM Rot, ROM SF, total ROM and disability in theshort term. There was no evidence beyond individualresults of benefit in the longer term as no meta-analyseswere possible. The one trial that evaluated as unclearrisk of bias was, therefore, not included in any meta-analyses.41
In evaluating short term outcome in the acute/sub-acute stage, there was some evidence that active physio-therapy intervention reduces pain. This was supportedby statistically significant differences in two trials.39 48
Although the finding is interesting, further trials arerequired since one trial possessed one high riskcomponent of bias, and the other possessed two. Onlyone trial43 suggested that active physiotherapy interven-tion changes ROM (flex/ext and SF); three trials43 45 56
suggested a change in ROM Rot. There was evidencefrom the meta-analyses to support this. Again, risk of biaswas high for all trials, with two high risk components forone trial43 and one high risk component for the twoother trials. There was no evidence that active physio-therapy intervention affects disability.In evaluating short term outcome in the acute/sub-
acute stage, there was some evidence that specificphysiotherapy intervention reduces pain. This wassupported by statistically significant differences found
Figure 3 ROM (range ofmovement) flexion/extensionshort-term.
Study or subgroup
Bonk 2000
Ask 2009
Scholten-Peeters 2006
Total (95% CI)
Heterogeneity: t² = 0.03; c² = 2.89, df = 2 (p = 0.24); I² = 31%
Test for overall effect: Z = 2.19 (p = 0.03)
Mean
19.4
109.7
13.7
SD
1.8
22.2
22.1
Total
47
11
38
96
Mean
18.3
100.1
11.1
SD
1.6
24.9
20.3
Total
50
14
42
106
Weight
43.6%
16.4%
40.0%
100.0%
IV, random, 95% CI
0.64 (0.23 to 1.05)
0.39(-0.41 to 1.19)
0.12 (-0.32 to 0.56)
0.39 (0.04 to 0.74)
Active intervention Standard intervention Std. mean difference Std. mean difference
IV, random, 95% CI
-2 -1 0 1 2Favours standard Favours active
Figure 2 Pain short-term.Study or subgroup
Denher 2009 (1)
Ask 2009
Scholten-Peeters 2006
Vassiliou 2006
Schnabel 2004
Soderlund 2000
Total (95% CI)
Heterogeneity: t² = 0.06; c² = 11.60, df = 5 (p = 0.04); I² = 57%
Test for overall effect: Z = 2.45 (p = 0.01)
Mean
4.7
27
-23.3
1.49
1.04
2.6
SD
9.51
3.16
29.8
2.26
1.81
2.4
Total
32
11
38
92
88
27
288
Mean
15.7
26.5
-13.2
2.7
1.6
2.2
SD
12.12
6.39
25.9
2.78
2.15
2
Total
32
14
42
81
62
26
257
Weight
14.9%
8.9%
17.4%
22.7%
21.8%
14.3%
100.0%
IV, random, 95% CI
-1.00 (-1.52 to -0.48)
0.09 (-0.70 to 0.88)
-0.36 (-0.80 to 0.08)
-0.48 (-0.78 to -0.18)
-0.28 (-0.61 to 0.04)
0.18 (-0.36 to 0.72)
-0.35 (-0.63 to -0.07)
Active intervention Standard intervention Std. mean difference
(1) Scholten-Peeters reported change in pain
Std. mean difference
IV, random, 95% CI
-2 -1 0 1 2Favours active Favours standard
10 Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

in four trials40 47 51 52 using interventions of Kinesiotaping, magnetic therapy and manipulation. Althoughthe finding is interesting, further trials are requiredbecause all trials possessed one high risk component ofbias and two trials had an additional four unclear risks.Only one individual trial47 suggested that specificphysiotherapy intervention (magnetic therapy)changes ROM (flex/ext or Rot or SF) in the short term.There was no evidence from the meta-analyses tosupport this.
LimitationsThe strengths of this review are its focus to physiotherapyintervention and the most common whiplash associateddisorder II classification requiring physiotherapy inter-vention. Heterogeneity in treatment effects can beexplained by variation in the quality of administration ofinterventions. Differences were evident in the outcomemeasures, assessment points, and classification of whip-
lash associated disorder participants, where many trialscombined whiplash associated disorder classificationseven though interventions in practice would vary betweenclassifications.15 16 Differences in components of thephysiotherapy interventions were also evident, with somevariation explained by diversity in practice across coun-tries. The differences limited the possible comparisons inthe meta-analyses. Surprisingly, no chronic interventionswere comparable for analysis, considering the highnumber of patients experiencing chronicity with whip-lash associated disorder.7 8 Also surprisingly, work statuswas not possible for analysis considering the economicimplications of whiplash associated disorder.9 10
Moderate heterogeneity (I2¼57%) was present in theevidence for active intervention for pain,33 identifyingsignificant difference in treatment effects between trials.However, heterogeneity might not be important forROM flex/ext, Rot and SF (I2¼31%, 25% and 0%,respectively). Substantial heterogeneity (I2¼64%) was
Figure 5 ROM (range ofmovement) rotation right/leftshort-term.
Study or subgroup
Bonk 2000
Ask 2009
Scholten-Peeters 2006
Soderlund 2000
Total (95% CI)
Heterogeneity: t² = 0.02; c² = 4.00, df = 3 (p = 0.26); I² = 25%
Test for overall effect: Z = 4.45 (p < 0.00001)
Mean
178.5
141.9
18.4
5.53
SD
4.6
20.4
19.5
1
Total
47
11
38
26
122
Mean
175.4
127.5
5.5
4.34
SD
8.1
27
20
1
Total
50
14
42
29
135
Weight
35.6%
12.2%
30.8%
21.4%
100.0%
IV, random, 95% CI
0.46 (0.06 to 0.87)
0.57 (-0.24 to 1.38)
0.65 (0.20 to 1.10)
1.17 (0.60 to 1.75)
0.68 (0.38 to 0.99)
Active intervention Standard intervention Std. mean difference Std. mean difference
IV, random, 95% CI
-2 -1 0 1 2Favours standard Favours active
Figure 4 ROM (range ofmovement) right side flexion/leftside flexion short-term.
Study or subgroup
Bonk 2000
Ask 2009
Scholten-Peeters 2006
Total (95% CI)
Heterogeneity: t² = 0.00; c² = 0.71, df = 2 (p = 0.70); I² = 0%
Test for overall effect: Z = 3.18 (p = 0.001)
Mean
88.3
76.6
11.1
SD
4.2
14.3
13.5
Total
47
11
38
96
Mean
85.7
69.1
7.1
SD
4.9
14.2
12.2
Total
50
14
42
106
Weight
47.6%
12.1%
40.3%
100.0%
IV, random, 95% CI
0.56 (0.16 to 0.97)
0.51 (-0.30 to 1.31)
0.31 (-0.13 to 0.75)
0.45 (0.17 to 0.73)
Active intervention Standard intervention Std. mean difference Std. mean difference
IV, random, 95% CI
-2 -1 0 1 2Favours standard Favours active
Figure 6 Disability short-term.
Study or subgroup
Ask 2009
Scholten-Peeters 2006
Vassiliou 2006
Schnabel 2004
Soderlund 2000
Total (95% CI)
Heterogeneity: t² = 0.08; c² = 11.07, df = 4 (p = 0.03); I² = 64%
Test for overall effect: Z = 1.64 (p = 0.10)
Mean
8
5.3
1.31
0.92
19.6
SD
2.21
6.8
2.19
1.7
16.5
Total
11
38
92
88
27
256
Mean
10
5.2
2.49
1.56
15.6
SD
1.54
19.6
2.69
2.22
14.8
Total
14
165
81
62
26
348
Weight
9.6%
23.5%
25.5%
24.6%
16.7%
100.0%
IV, random, 95% CI
-1.04 (-1.89 to -0.19)
0.01 (-0.35 to 0.36)
-0.48 (-0.79 to -0.18)
-0.33 (-0.66 to -0.00)
0.25 (-0.29 to 0.79)
-0.26 (-0.57 to 0.05)
Active intervention Standard intervention Std. mean difference Std. mean difference
IV, random, 95% CI
-2 -1 0 1 2Favours active Favours standard
Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265 11
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

present in the evidence for active intervention fordisability, perhaps explaining the lack of evidence of aneffect. Considerable heterogeneity33 was present in theevidence for specific physiotherapy intervention forpain, ROM flex/ext, Rot, and SF (I2¼98.1%, 99.0%,98.1% and 96.6%, respectively), perhaps explaining thelack of evidence of an effect for all ROM evaluations.This anticipated heterogeneity was accounted for byusing the random effects model.Using GRADE62 (the Grading of Recommendations
Assessment, Development and Evaluation system), thequality of the body of evidence for physiotherapy reha-bilitation in the management of whiplash associateddisorder II, based on the 12 trials included in the meta-analyses, is ‘very low’ for pain, ROM flex/ext and SF(active vs standard intervention), and ‘low’ for ROM Rot(active vs standard intervention) and pain (specific inter-vention vs control) in the short term. These estimates areinterpreted as ‘little confidence in the effect estimate: thetrue effect is likely to be substantially different from theestimate of effect’ (very low) and ‘confidence in the effectestimate is limited: the true effect may be substantiallydifferent from the estimate of the effect’ (low).62
Downgrading of quality was due to high risk of bias, andissues of imprecision and inconsistency.62
The limitations in the context of the high risk of biasand number of trials available necessitate urgent atten-tion to focus a future high quality and properly poweredtrial to evaluate a whiplash associated disorder II popu-lation. The very low/low quality of trials is consistent withearlier findings for physiotherapy management post-lumbar discectomy.30 63 There is limited scope at presentfor good quality meta-analyses in physiotherapy withrigorous and well reported trial inclusion. Physiotherapytrials need to avoid risk of bias. Planning for quality isimportant, particularly for issues that present knownproblems for physiotherapy trials, for example loss tofollow-up. Consensus for minimum core sets of outcomemeasures for specific populations is also required.
ConclusionsThis systematic review has identified inconclusive verylow/low quality evidence for the effectiveness of phys-iotherapy management for whiplash associated disorderII. Inclusion of large numbers of participants in thepoorly designed trials published to date is unethical. Bestpractice for physiotherapy management, therefore,remains unclear. This lack of clarity might explain thevariability of interventions across the trials that madecomparability of interventions difficult. There is poten-tial benefit for improving pain and ROM flex/ext, Rotand SF short term through active physiotherapy, and forimproving pain through specific physiotherapy inter-ventions. This potential benefit merits further consider-ation in a properly powered clinical trial with attentionto ensure low risk of bias.
Funding This research received no specific grant from any funding agency inthe public, commercial or not-for-profit sectors.
Competing interests None
Contributors AR and GE are senior lecturers in Physiotherapy and NH isa lecturer. MC and CW are both senior lecturers. NF is Professor of ClinicalEpidemiology and Biostatistics. AR, MC, CW and NF have longstandingprofessional interests in the quality and reporting of randomised controlledtrials in medicine and physiotherapy. AR, NH and GE have a professional focusto musculoskeletal physiotherapy. AR and CW were responsible for theconception of the study. All authors have contributed to the systematic reviewand have been involved in developing the content of the article. AR wrote thefirst draft of the paper and developed it initially with CW. AR has worked withall authors reworking content into subsequent drafts. All authors gave finalapproval of the version to be published. AR is the guarantor.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data available.
REFERENCES1. Spitzer WO, Skovron ML, Salmi LR, et al. Scientific monograph of the
Quebec Task Force on Whiplash Associated Disorders: redefining‘whiplash’ and its management. Spine (Phila Pa 1976) 1995;20(8Suppl):1Se73S.
2. Holm LW, Carroll LJ, Cassidy JD, et al. The burden and determinantsof neck pain in Whiplash associated disorders after traffic collisions,results of the Bone and Joint Decade 2000-2010 Task Force on Neckpain and its Associated Disorders. Spine (Phila Pa 1976) 2008;33(4 Suppl):S52e9.
3. Jansen GB, Edlund C, Grane P, et al; The Swedish Society ofMedicine and the Whiplash Commission Medical Task Force.Whiplash injuries: diagnosis and early management. Eur Spine J2008;17(Suppl 3):S359e418.
4. Burton K. Treatment guidelines: is there a need? Proceedings ofWhiplash Conference 2003, Bath, England, 6e8th May. Bristol: LyonsDavidson Solicitors, 2003.
5. Barnsley L, Lord S, Bogduk N. Whiplash injury: clinical review. Pain1994;58:283e307.
6. Scholten-Peeters GG, Verhagen AP, Bekkering GE, et al. Prognosticfactors of whiplash-associated disorders: a systematic review ofprospective cohort studies. Pain 2003;104:303e22.
7. Carroll LJ, Hurwitz EL, Cote P, et al. Research priorities andmethodological implications. The Bone and Joint Decade 2000-2010Task Force on Neck Pain and its Associated Disorders. Spine(Phila Pa 1976) 2008;33(4 Suppl):S214e20.
8. Kampner SJ, Rebbeck TJ, Maher CG, et al. Course and prognosticfactors of whiplash: a systematic review and analysis. Pain2008;138:617e29.
9. Eck JC, Hodges SD, Humphreys SC. Whiplash: a review ofa commonly misunderstood injury. Am J Med 2001;110:651e6.
10. Galasko CSB, Murray P, Stephenson W. Incidence of whiplash-associated disorder. BC Med J 2002;44:237e40.
11. Field S, Treleaven J, Jull G. Standing balance: a comparison betweenidiopathic and whiplash-induced neck pain. Man Ther2008;13:183e91.
12. Chien A, Sterling M. Sensory hypoaesthesia is a feature of chronicwhiplash but not chronic idiopathic neck pain. Man Ther2010;15:48e53.
13. Woodhouse A, Liljeback P, Vasseljen O. Reduced head steadiness inwhiplash compared with non-traumatic neck pain. J Rehabil Med2010;42:35e41.
14. Verhagen AP, Lewis M, Schellingerhout JM, et al. Do whiplashpatients differ from other patients with non-specific neck painregarding pain, function or prognosis? Man Ther 2011;16:452e62.
15. Sterling M. A proposed new classification system for whiplashassociated disordersdimplications for assessment andmanagement. Man Ther 2004;9:60e70.
16. Moore A, Jackson A, Jordan J, et al. Clinical Guidelines for thePhysiotherapy Management of Whiplash Associated Disorder (WAD).London: Chartered Society of Physiotherapy, 2005.
17. Verhagen AP, Scholten-Peeters GG, van Wijngaarden S, et al.Conservative treatments for whiplash. Cochrane Database Syst Rev2007;(2):CD003338.
18. World Health Organization. International Classification ofFunctioning, Disability and Health: ICF. Geneva, Switzerland: WorldHealth Organization, 2001.
19. Furlan AD, Pennick V, Bombardier C, et al; Editorial Board of theCochrane Collaboration Back Review Group. 2009 updated methodguidelines for systematic reviews in the Cochrane Collaboration BackReview Group. Spine 2009;34:1929e41.
12 Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from

20. Higgins JPT, Green S, eds. Cochrane Handbook for SystematicReviews of Interventions Version 5.1.0. The CochraneCollaboration, 2011. http://www.cochrane-handbook.org/(accessed Mar 2011).
21. Moher D, Liberati A, Tetzlaff J, et al; PRISMA Group. Preferredreporting items for systematic reviews and meta-analyses: thePRISMA statement. PLoS Med 2009;6:e1000097.
22. Centre for Reviews and Dissemination (CRD). Systematic Reviews:CRD’s Guidance for Undertaking Reviews in Healthcare. 3rd edn.York: CRD University of York, York Publishing Services Ltd, 2009.
23. Cohen J. A coefficient of agreement for nominal scales. Educ PsycholMeas 1960;20:37e46.
24. Higgins JPT, Deeks JJ, eds. Chapter 7: selecting studies andcollecting data. In: Higgins JPT, Green S, eds. Cochrane Handbookfor Systematic Reviews of Interventions Version 5.1.0. The CochraneCollaboration, 2011. http://www.cochrane-handbook.org (accessedMar 2011).
25. Machin D, Fayers PM. Randomized Clinical Trials: Design, Practiceand Reporting. West Sussex: Wiley-Blackwell, 2010.
26. Higgins JPT, Altman DG, Sterne JAC, eds. Chapter 8: assessing riskof bias in included studies. In: Higgins JPT, Green S, eds. CochraneHandbook for Systematic Reviews of Interventions Version 5.1.0. TheCochrane Collaboration, 2011. http://www.cochrane-handbook.org(accessed Mar 2011).
27. Juni P, Witschi A, Bloch R, et al. The hazards of scoring the quality ofclinical trials for meta-analysis. JAMA 1999;282:1054e60.
28. Katrak P, Bialocerkowski AE, Massy-Westropp N, et al. A systematicreview of the content of critical appraisal tools. BMC Med ResMethodol 2004;4:22.
29. Olivio SA, Macedo LG, Gadotti IC, et al. Scales to assess the qualityof randomized controlled trials: a systematic review. Phys Ther2008;88:156e75.
30. Rushton A, Calvert M, Wright C, et al. Physiotherapy trials for the21st centurydtime to raise the bar? J Roy Soc Med. In press.
31. Green S, Higgins JPT, eds. Chapter 2: preparing a Cochranereview. In: Higgins JPT, Green S, eds. Cochrane Handbook forSystematic Reviews of Interventions Version 5.1.0. The CochraneCollaboration, 2011. http://www.cochrane-handbook.org(accessed Mar 2011).
32. DerSimonian R, Laird N. Meta-analyses in clinical trials. Control ClinTrials 1986;7:177e88.
33. Deeks JJ, Higgins JPT, Altman DG, eds. Chapter 9: analyzing dataand undertaking meta-analyses. In: Higgins JPT, Green S, eds.Cochrane Handbook for Systematic Reviews of Interventions Version5.1.0. The Cochrane Collaboration, 2011. http://www.cochrane-handbook.org (accessed Mar 2011).
34. Hedges LV, Olkin I. Statistical Methods for Meta-Analyses. SanDiego: Academic Press Inc., 1985.
35. Ekvall Hansson E, Mansson NO, Ringsberg KA, et al. Dizzinessamong patients with whiplash-associated disorder: a randomisedcontrolled trial. J Rehabil Med 2006;38:387e90.
36. Sterling M, Pedler A, Chan C, et al. Cervical lateral glide increasesnociceptive flexion reflex threshold but not pressure or thermal painthresholds in chronic whiplash associated disorders: a pilotrandomised controlled trial. Man Ther 2010;15:149e53.
37. Sterne JAC, Egger M, Moher D; on behalf of the Cochrane BiasMethods Group. Chapter 10: addressing reporting biases. In: HigginsJPT, Green S, eds. Cochrane Handbook for Systematic Reviewsof Interventions Version 5.1.0. The Cochrane Collaboration, 2011.http://www.cochrane-handbook.org (accessed Mar 2011).
38. Aigner N, Fialka C, Radda C, et al. Adjuvant laser acupuncturein the treatment of whiplash injuries: a prospective, randomizedplacebo-controlled trial. Wein Klin Wochenschr 2006;118:95e9.
39. Dehner C, Elbel M, Strobel P, et al. Grade II whiplash injuries to theneck: what is the benefit for patients treated by different physicaltherapy modalities? Patient Saf Surg 2009;3:2.
40. Gonzalez-Inglesias J, Fernandez-de-las-Penas C, Cleland J, et al.Short-term effects of cervical kinesio taping on pain and cervicalrange of motion in patients with acute whiplash injury: a randomizedclinical trial. J Orthop Sports Phys Ther 2009;39:515e21.
41. Jull G, Sterling M, Kenardy J, et al. Does the presence of sensoryhypersensitivity influence outcomes of physical rehabilitation forchronic whiplash? A preliminary RCT. Pain 2007;129:28e34.
42. Ask T, Strand LI, Skouen JS. The effect of two exercise regimes;motor control versus endurance/strength training for patients with
whiplash-associated disorders: a randomized controlled pilot study.Clin Rehabil 2009;23:812e23.
43. Bonk AD, Ferrari R, Giebel GD, et al. Prospective, randomized,controlled study of activity versus collar, and the natural history forwhiplash injury, in Germany. J Muscoskel Pain 2000;8:123e32.
44. Pato U, Di Stefano G, Fravi N, et al. Comparison of randomizedtreatments for late whiplash. Neurology 2010;74:1223e30.
45. Scholten-Peeters GG, Neeleman-van der Steen CW, van der WindtDA, et al. Education by general practitioners or education withexercises by physiotherapists for patients with whiplash-associateddisorders? A randomized clinical trial. Spine (Phila Pa 1976)2006;31:723e31.
46. Stewart MJ, Maher CG, Refshauge KM, et al. Randomized controlledtrial of exercise for chronic whiplash-associated disorders. Pain2007;128:59e68.
47. Thuile C, Walzl M. Evaluation of electromagnetic fields in thetreatment of pain in patients with lumbar radiculopathy or the whiplashsyndrome. NeuroRehabilitation 2002;17:63e7.
48. Vassiliou T, Kaluza G, Putzke C, et al. Physical therapy and activeexercisesdan adequate treatment for prevention of late whiplashsyndrome? Randomized controlled trial in 200 patients. Pain2006;124:69e76.
49. Vikne J, Oedegaard A, Laerum E, et al. A randomized study of newsling exercise treatment vs traditional physiotherapy for patients withchronic whiplash-associated disorders with unsettled compensationclaims. J Rehabil Med 2007;39:252e9.
50. Armstrong BS, McNair PJ, Williams M. Head and neck position sensein whiplash patients and healthy individuals and the effect of thecranio-cervical flexion action. Clin Biomech (Bristol, Avon)2005;20:675e84.
51. Fernandez-de-las-Penas C, Fernandez-Carnero J, Fernandez AP,et al. Dorsal manipulation in whiplash injury treatment: a randomisedcontrolled trial. J Whiplash & Relat Disord 2004a;3:55e72.
52. Fernandez-de-las-Penas C, Fernandez-Carnero J, Palomeque delCerro L, et al. Manipulative treatment vs conventional physiotherapytreatment in whiplash injury: a randomised controlled trial. J Whiplash& Relat Disord 2004b;3:73e90.
53. Rosenfeld M, Seferiadis A, Carlsson J, et al. Active intervention inpatients with whiplash associated disorders improves long termprognosis. Spine 2003;28:2491e8.
54. Rosenfeld M, Seferiadis A, Gunnarsson R. Active involvement andintervention in patients exposed to whiplash trauma in automobilecrashes reduces costs. Spine 2006;31:1799e804.
55. Schnabel M, Ferrari R, Vassiliou T, et al. Randomised, controlledoutcome study of active mobilisation compared with collar therapy forwhiplash injury. Emerg Med J 2004;21:306e10.
56. Soderlund A, Olerud C, Lindberg P. Acute whiplash-associateddisorders (WAD): the effects of early mobilization and prognosticfactors in long-term symptomatology. Clin Rehabil 2000;14:457e67.
57. Soderlund A, Lindberg P. Cognitive behavioural components inphysiotherapy management of chronic whiplash associated disorders(WAD)da randomised group study. Physiother Theor Pract2001;17:229e38.
58. Soderlund A, Lindberg P. Cognitive behavioural components inphysiotherapy management of chronic whiplash associated disorders(WAD)da randomised group study. G Ital Med Lav Ergon 2007;29(1Suppl A):A5e11.
59. Landis JR, Koch GG. The measurement of observer agreement forcategorical data. Biometrics 1977;33:159e74.
60. Scholten-Peeters GG, Verhagen AP, Neeleman-van der Steen CW,et al. Randomized clinical trial of conservative treatment withwhiplash-associated disorders: considerations for the design anddynamic treatment protocol. J Manipulative Physiol Ther2003;26:412e20.
61. Stewart MJ, Maher CG, Refshauge KM, et al. Advice or exercise forchronic whiplash-associated disorders? Design of a randomizedcontrolled trial. BMC Musculoskelet Disord 2003;4:18.
62. Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3.Rating the quality of evidence. J Clin Epidemiol 2011;64:401e6.
63. Rushton A, Wright C, Goodwin P, et al. Physiotherapy rehabilitationpost first lumbar discectomy: a systematic review and meta-analysisof Randomised Controlled Trials. Spine (Phila Pa 1976) 2011;36:E961e72.
Rushton A, Wright C, Heneghan N, et al. BMJ Open 2011;1:e000265. doi:10.1136/bmjopen-2011-000265 13
Systematic review of physiotherapy management post-whiplash
on February 24, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2011-000265 on 14 N
ovember 2011. D
ownloaded from