Embed Size (px)
Citation preview

Policy No: OP41 Version: 2.0
Name of Policy: Central Venous Line Policy
Effective From: 29/10/2009
Date Ratified 31/07/2009 Ratified Infection, Prevention and Control Committee Review Date 01/07/2011 Sponsor Director of Nursing & Midwifery Expiry Date 30/07/2012 Withdrawn Date
This policy supersedes all previous issues.

OP 41 Central Venous Line Policy
Page 2 of 21
Contents Page(s) 1.0 Introduction 3 2.0 Insertion of Central Venous Catheters 4 – 5 2.1 Patient Selection 2.2 Setting 2.3 Infection Prevention
2.4 Use of Ultrasound Guidance 2.5 Choice of Line 2.6 TPN 2.7 Critically Ill Patients 2.8 Poor Access 2.9 Bionectors 2.10 Lumens Not in Use 3.0 Documentation 6 4.0 Care of the CVC Line 6 - 9 4.1 Multi-lumen Central Venous Catheter 4.2 Use 4.3 Insertion Sites 4.4 Care of the Insertion Site 4.5 Table – to be named 4.6 On Critical Care 4.7 On Removal 4.8 Table to be named 5.0 Replacing and Removing Lines 10
5.1 Review and Removal 5.2 Removal of Groshong/Hickman Lines
6.0 Training
6.1 Monitoring Compliance/Effectiveness of the Policy
Appendix 1 - CVC availability within QEH site 11 Appendix 2 – NICE Guidance 49 12 Appendix 3 – Care of Groshong or PICC 13 - 17 Appendix 4 – Care of Hickman lines 18 - 21

OP 41 Central Venous Line Policy
Page 3 of 21
1.0 INTRODUCTION Central venous catheters (CVC) are inserted for many reasons including haemodynamic monitoring, intravenous delivery of blood products and drugs, haemodialysis, total parenteral nutrition, cardiac pacemaker placement and management of perioperative fluids. NICE have provided guidance on the methods used for placement of CVC. Their subsequent management has been mentioned in government documents such as Winning Ways and Saving Lives and is also been the subject of a review by EPIC. High impact Intervention No 1 – Central Venous Catheter Care bundle found at website - http://www.clean-safe-care.nhs.uk/index.php?pid=4 should also be use as part of normal practice for any area using and caring for central lines. CVC’s are sited in a number of clinical areas within the Trust by clinicians from various specialties. This policy aims to aid all professionals in applying best practice within the setting of Gateshead Health NHS Foundation Trust. This policy has been compiled by a multidisciplinary group in consultation with the Clinical Directors of each Division. Paediatric practice is beyond the scope of this policy. Please refer to Consultant Paediatrician at RVI. The Chemotherapy Day Unit has issued further separate guidance on the use of tunneled, long term CVC which is attached to this document as Appendix 3 (page 14) Back to contents

OP 41 Central Venous Line Policy
Page 4 of 21
2.0 INSERTION OF CENTRAL VENOUS CATHETERS 2.1 Patient Selection The clinician placing the line is responsible for ensuring that any contraindications have been addressed for example coagulopathy The procedure should be explained to the patient. 2.2 Setting Groshong or Hickman lines for long-term access and CVC lines for TPN should be sited in a Theatre environment. Thereafter for management, ie dressing changes a clean clinical area such a treatment room should be used whenever possible. Open wards of critical care areas such as CCD, A&E and CCU are acceptable due to the nature of the patients treated. The urgency of placement and the stability of the patient should be taken into account. 2.3 Infection Prevention With reference to the MRSA policy all in- patients should use the octenisan body wash. This is irrespective of their MRSA status. 2.4 Use of Ultrasound Guidance Training in the use of ultrasound guidance is now routine in anaesthetic practice. NICE published guidance on this in 2002 and reviewed it in 2009 with no change to guidance from 2002. http://www.nice.org.uk/cat.asp?c=36752 The grade and training of the clinician inserting CVC’s will vary between Divisions depending upon the level of expertise available. Anyone undertaking insertion should be competent to do so either as demonstrated by their training documents or experience. 2.5 Choice of Line There is a need to balance infection control issues with the possible complications of having to insert further lines or renew existing lines with those with more lumens. There is no strong evidence for the use of antimicrobial or silver bonded lines as routine for short term cannulation. See appendix 1 for line availability within QEH. Back to contents

OP 41 Central Venous Line Policy
Page 5 of 21
2.6 TPN If this is being administered prior to surgery a double lumen line should be used. In other circumstances consideration should be made as to whether a long term line should be requested. The lumen dedicated to TPN use should ideally be the smallest lumen on the line. It should be capped with a brown bionector and once a bionector is used there is no need for betadine soak. Once TPN has been commenced the line should not be used for any other purpose. Three way taps are not acceptable for TPN 2.7 Critically Ill Patients This encompasses patients in A&E, MAU, CCU, CCD, maternity and theatre. The standard line for these patients is a quad lumen line with a port reserved for TPN. Specifically designed lines for pacing should be available on CCU or catheter laboratory. 2.8 Poor Access If a CVC is being sited due to poor venous access in a non perioperative situation a double lumen line should be used. Double lumen lines are to be held by theatres, MAU, CCD and CCU only. 2.9 Bionectors TPN should be administered using a dedicated lumen (EPIC CVAD 37) with a brown Bionector in place. Disinfect the bionector before and after use with ChloraPrep Replace Bionector after 7 days. Patients discharged from Critical Care with a central line in situ will have 3 way taps removed from the line and replaced with bionectors prior to discharge. 2.10 Lumens not in use Lumens not in use should be flushed and capped with a white bung and flushed daily. Flushing 0.9% sodium chloride is advised for routine flushes unless the line is a Hickman line. The policy for care and flushing of these lines is attached in Appendix 3. Back to contents

OP 41 Central Venous Line Policy
Page 6 of 21
3.0 DOCUMENTATION The procedure should be documented in the patient’s case notes. This will include the date, time and operators name, signature, grade and contact number, plus type of line inserted. 4.0 CARE OF THE CVC LINE Within Gateshead Health NHS Foundation Trust central lines are usually: • non tunneled short term use/multi lumen (Acutely ill patients) • Tunnelled, long term use (Groshong/Hickman) Please ensure you are aware of the type of line inserted prior to any care being given to the line. 4.1 Multi-lumen Central Venous Catheters
4.2 Use Used predominantly within Critical Care, Theatres and A&E. Used for : monitoring haemodynamic status (CVP); administration of inotropes /vaso-active medication; administration of TPN (via a dedicated lumen); administration of medications which are irritant and are likely to cause phlebitis if administered via a peripheral vein. 4.3 Insertion sites Neck (internal jugular vein), chest (sub clavian vein), or groin (femoral vein). Back to contents

OP 41 Central Venous Line Policy
Page 7 of 21
4.4 Care of the Insertion Site As for other CVCs. Clean with 2% chlorhexidine / 70% isopropyl alcohol (EPIC CVAD 24), dress with transparent semi permeable dressing (EPIC CVAD 19) renewed every 7 days or more often if necessary (EPIC CVAD 20). A sterile gauze dressing may be indicated if there is bleeding from the insertion site or profuse perspiration. This will need changing if it becomes damp, soiled or displaced, or to inspect the site, and should be substituted with a transparent semi permeable dressing as soon as appropriate (EPIC CVAD 21 & 22). Condition of the insertion site should be observed and documented daily by nursing staff, and medical staff informed of any inflammation or discharge at site. CVCs placed in neck or chest veins should have their position confirmed by x-ray prior to use – also to exclude pneumothorax caused during insertion. Line manipulation must be kept to a minimum and flushed daily when not in use. The flush should be recorded in the nursing record 4.5 Procedure for Administering Medication via a CVC ACTION RATIONALE
1 Staff should wear a clean apron and wash hands thoroughly.
To reduce the potential for the spread of infection.
2
An aseptic non-touch technique should be followed throughout.
To reduce the potential for the spread of infection.
3
Clean the injection bung / hub thoroughly with 2% chlorhexidine / 70% isopropyl alcohol (Sani-cloth) (EPIC CVAD 33)
To reduce the number of microbiological organisms that may be colonizing the injection bung.
4
With a 5 ml syringe, aspirate the lumen to be used until 2-3 ml blood withdrawn
This confirms the patency of the lumen and ensures there are no clots or residual medication in the lumen.
5
Administer the medication or commence the infusion as prescribed.
6
After use of the lumen: using a 5 ml syringe, aspirate until 2-3 ml blood withdrawn, then flush and lock the line gently using 5 ml normal saline (EPIC CVAD 38).
Maintains patency
Back to contents

OP 41 Central Venous Line Policy
Page 8 of 21
4.6 On Critical Care CVCs should not routinely be used to take blood samples. However they may be used in the absence of an arterial line in patients where phlebotomy is particularly difficult. 4.7 On Removal All CVC tips (4CM distal segment) should go to microbiology for culture and sensitivity. 4.8 Continuous Veno-Venous Haemofiltration (CVVH catheters)
Used within Critical Care to provide vascular access for Continuous Veno-Venous Haemofiltration (CVVH). Insertion sites: as for multi-lumen CVCs Care of the insertion site: as for multi-lumen CVCs Use of the CVVH catheter is only within the Critical Care Department. Back to contents

OP 41 Central Venous Line Policy
Page 9 of 21
4.8 Procedure for Using a Double Lumen Haemofiltration Catheter
ACTION RATIONALE Staff should wear a clean apron and wash hands thoroughly.
To reduce the potential for the spread of infection.
An aseptic non-touch technique should be followed throughout.
To reduce the potential for the spread of infection.
Clean the injection bung / hub thoroughly with 2% chlorhexidine / 70% isopropyl alcohol (Sani-cloth) (EPIC CVAD 33)
To reduce the number of microbiological organisms that may be colonizing the injection bung.
With a 10 ml syringe, aspirate the lumen to be used until 10 mls blood withdrawn, empty this blood onto a clean piece of gauze and examine for the presence of clots. Continue this until aspirate is free from clots.
This confirms the patency of the lumen, ensures there are no clots or residual locking dose of Heparin in the lumen, and allows for assessment flow rate through the lumen
The lumen should then be flushed with 5-10 ml normal saline
Ensure patency and assess flow rates.
The cannula can then be attached to the extra corporeal circuit and treatment commence.
Back to contents

OP 41 Central Venous Line Policy
Page 10 of 21
5.0 REPLACING AND REMOVING LINES • CVCs should not be replaced over a guide wire if infection is present or suspected. If infection is present a new site should be chosen and a 4cm tip of the old line sent to microbiology for culture and sensitivity. (See section 4.7) All line tips should routinely be sent to Microbiology for culture and sensitivity (as section 4.7) If an infection is suspected and the line is the suspected source blood cultures should be sent from both the line and peripherally at the same time. If exit site suspicious (redness, leakage, inflammation) swab exit site for C & S. Any further questions contact microbiology – or Microbiologist if considering treatment for a suspected line infection. 5.1 Review and Removal • Daily consideration should be given as to the need for CVC lines. They should be
removed as soon as possible. Exceptions may include difficult access when long-term line placement should be considered. • The date and time of removal, reason why and name of person who removed the line
should be documented in the patient’s notes. 5.2 Removal of Groshong/Hickman lines Removal of CVCs: should only be undertaken by staff with the appropriate skills and knowledge. On removal, all CVC tips should go to microbiology for culture and sensitivity. See section 4.7 6.0 Training Scheduled from January 2010 formal training and competency assessment will be available via in house training programme on a monthly basis. All trust staff who are required to manage central venous access devices (CVAD) will be expected to attend and complete competency training. On going education and training is available via critical care outreach team (CCOT). 6.1 Monitoring Compliance/Effectiveness As reflected in section 6.0, it is the managers responsibility to ensure that appropriate staff are released fro training and competency assessment. This should form part of their professional development and incorporated in review. A record will be kept at corporate level of staff who have received CVAD training. CCOT will work with the Lead Infection Prevention and Control Nurse for CVAD management to provide targeted training and education.
OP 41 Central Venous Line Policy
Page 11 of 21
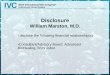
Appendix 1
Clinical Area Arrow Double
lumen Edwards
Quad lumen Certofix
Edwards CVVH
Catheter+
PA catheter sheath Other
MAU # #
CCU # #
Theatre QEH # # Quin lines and Paediatric
lines
Theatre NESC #
CCD # # # # # Arrow Quin lines
A & E # # Paediatric lines
Maternity #
Radiology
Bard single lumen Groshong
Hickman double and single lumen
Ward 20 Paediatric lines
Manufacturer Lumens Size Length Code
Paediatric lines Arrow 2 4 Fr 13cm CS- 14402
Double lumen Arrow 2 8 Fr 20 cm CS – 25802-
E
Quad lumen Edwards 4 8.5 Fr 16cm M8416E
Certofix Quinto V Braun 5 12Fr 20 cm 416668
PA catheter sheaths
Edwards 1 8.5 Fr 1651 BF 85
5-lumen Arrow 5 8.5Fr
CVVH Catheter Edwards 2 14Fr 15 + 24
cm
Single lumen Bard 1 7711800 Hickman 1 2193-960
Double lumen Hickman 2 2293-95 Back to contents

OP 41 Central Venous Line Policy
Page 12 of 21
Appendix 2 NICE guidance 49 In September 2002 NICE issued guidance on the use of 2-D ultrasound. NICE guidelines state that • The use of 2-D ultrasound is the preferred method for the insertion of CVCs into the
internal jugular vein (IJV) in adults and children in the elective situation. • Its use should be considered in most clinical circumstances where CVC insertion is
necessary either electively or in an emergency situation. • That those involved in placing CVCs using 2-D imaging ultrasound guidance should
undertake appropriate training to achieve competence. However it also states that • Practitioners should consider the most appropriate method of CVC insertion in the
best interest of the patient and that this will be informed by the competence and experience of the operator, the anatomical site of CVC insertion, other anticipated difficulties and the urgency of clinical need.
A subsequent survey commissioned by NICE has shown that only one third of Trusts have a framework to implement the use of ultrasound guidance. Opinions are polarized as to whether it is indeed the preferred method of placement. Within the QE use of 2D ultrasound is one element of the care bundle for the insertion of internal jugular central lines. Back to contents

OP 41 Central Venous Line Policy
Page 13 of 21
Appendix 3
Gateshead Health NHS Foundation Trust Guidelines for Nursing Staff on the Care and Management of
Groshong or PICC
The following guidelines are a reference material to professionals caring for central venous access devices within Gateshead Health NHS Foundation Trust. However, any professional performing these cares must first have been assessed and deemed competent within the Trust/Organisation. All practitioners must ensure they are aware of and working within their personal and professional accountability. The term Central Venous Access Device (CVAD) or Central Venous Catheter (CVC) implies that the tip of the device is positioned in the lower third of the superior vena cava (SVC). For the purpose of this document CVC will include:
• Tunnelled catheters – generally inserted via the jugular vein, with the other end being tunnelled under the skin and exiting on the chest.
• Peripherally inserted catheters (PICC’s) – which are inserted through an antecubital
vein or upper arm vein and threaded up to the SVC. Groshong Catheters Groshong catheters can be single or double lumen. Double lumen Groshong lines have a red lumen for blood sampling and infusion of blood products, and a white lumen for infusion of other crystalloid products. They are soft, silicone tubes with radiopaque stripes and tips. They have winged connectors for injection cap placement. Groshong catheters have a valve. The Groshong valve remains closed at normal central venous pressure. The valve is designed to restrict blood backflow and air embolism when closed. The valve will remain closed between –7 and 80mm Hg. PICC lines have a Groshong valve.
Back to contents

OP 41 Central Venous Line Policy
Page 14 of 21
It is important to remember that only 10ml or larger syringes should be used for infusing with Groshong catheters. Infusion pressures should not exceed 25psi. Maintaining Patency The catheter should be flushed every 7 days when not in use. It should also be flushed after administration of medications, fluid/blood transfusion, TPN, blood aspiration or if blood is observed in the line. Preventing Infection The exit site should be dressed every 7 days if using a transparent dressing. This may need to be changed more regularly if loosened or if the patient is neutropenic. Maintaining patency of a Groshong central venous catheter (single or double lumen) Equipment required:
1 dressing pack 1 pair of sterile gloves 2 x 10ml luer lock syringes (4 if double lumen) 20mls 0.9% sodium chloride (40mls if double lumen) 1 needle free bung (2 if double lumen) ChloraPrep 3ml Solution 1 Sani cloth CHG 2% for cleansing line 1 x 21G needle (green for drawing up saline) 1 x 25G needle (orange for injecting through bung) (2 if double lumen) 1 apron 1 pair of non sterile gloves 1 sharps bin and a orange clinical waste bag transparent, occlusive dressing e.g. IV 3000

OP 41 Central Venous Line Policy
Page 15 of 21
Procedure ACTION RATIONALE 1 Explain and discuss the procedure
with the patient. To gain the patient’s co-operation and understanding as well as informed consent.
2 Apply apron and wash hands thoroughly.
To reduce the potential for the spread of infection.
3 Clean trolley - open the dressing pack and place equipment onto sterile field.
To provide a sterile working area.
4 Remove old dressing with non-sterile gloves. Remove old dressing with non-sterile gloves. Check exit site of line for any signs of infection. Redness, swelling, oozing. If present inform clinician.
Safety of patient – line may need removed or antibiotic cover given.
5 Wash hands. Put on sterile gloves and draw up 10ml of saline into the two syringes.
To maintain a sterile working area.
6 Place sterile drape under the CVC. To provide a sterile working area and prevent contaminating the CVC during the procedure.
7 Swab the injection bung with Sani cloth on gauze and allow to dry.
To reduce the number of microbiological organisms that may be colonizing the injection bung.
8 Pre-fill the new injection cap with saline. Remove the old injection cap and attach a syringe.
To establish a connection between the line and the syringe.
9 Draw back approximately 3 - 4 mls of blood.
Ensures line patent.
10 Attach a pre-filled syringe. 11 Using a push-pause method (inject
1ml at a time), inject the contents of the syringe.
To create turbulence in order to flush the catheter thoroughly.
12 Remove syringe and replace with new needle free bung. Irrigate the catheter through the injection cap using the second syringe and a 25G needle. Use a push-pause method. Withdraw the needle as the last 0.5ml is being injected. If flushing a double lumen line, treat each lumen separately and repeat these steps for the second lumen.
Withdrawing the needle under positive pressure helps to prevent a vacuum occurring which may cause a small amount of blood to enter the tip of the catheter.
13 Clean the exit site with ChloraPrep 3ml solution
To reduce the number of microbiological organisms.
14 Apply new dressing. Dispose of equipment safely and in accordance with Trust policy. Document procedure.
To prevent contamination of others and maintain safe practice. Occlusive dressing helps to prevent bacterial contamination.
Blood sampling from a Groshong central venous catheter (single or double lumen)

OP 41 Central Venous Line Policy
Page 16 of 21
Equipment required:
Use equipment as for line flush. Also include the additional items listed below. 2 x 10ml syringes blood collection tubes
Procedure Follow the procedure for maintaining line patency through steps 1-7. Please note: When obtaining a blood sample from a double lumen line the sample should be taken from the RED lumen as outlined in the table below. The WHITE lumen just needs to be flushed as outlined above. The white lumen can be used for sampling if you are unable to use the red lumen.
ACTION RATIONALE 8 Pre-fill the new injection cap with
saline. Remove the old injection cap and attach one of the empty syringes.
To establish a connection between the line and the syringe.
9 Pull back on the syringe plunger 1-2ml and pause for 2 seconds. Aspirate 5ml blood and discard.
To allow the valve to open. The saline in the blood may dilute the specimen and alter results.
10 Attach an empty syringe and aspirate the required amount of blood.
To obtain specimen.
11 Remove syringe and attach a saline filled syringe.
To establish a connection between the line and the syringe.
12 Using a push-pause method (inject 1ml at a time), inject the contents of the syringe.
To create turbulence in order to flush the catheter thoroughly.
13 Remove syringe and replace with new needle free cap. Irrigate the catheter through the needle free bung using the second syringe. Use a push-pause method. Withdraw the needle as the last 0.5ml is being injected.
Withdrawing the needle under positive pressure helps to prevent a vacuum occurring which may cause a small amount of blood to enter the tip of the catheter.
14 Place blood in collection tubes and label correctly as per hospital policy.
To ensure positive patient identification.
15 Clean the exit site with ChloraPrep 3ml solution. Allow to dry.
To reduce the number of microbiological organisms.
16
Apply new dressing. Dispose of equipment safely and in accordance with Trust policy. Document procedure.
To prevent contamination of others and maintain safe practice. Occlusive dressing helps to prevent bacterial contamination.
Back to contents

OP 41 Central Venous Line Policy
Page 17 of 21
The following gives guidance on the management of possible line infections (intra/extra luminal or skin). All practitioners caring for these lines need to ensure they observe for any signs of infections and inform medical staff at each episode of care if concerned. BCSH Guidelines on the Management of CVAD Associated Infection Category of Infection Non-neutropenic Patient Neutropenic patient Exit site infection Remove catheter if no longer
needed. Treat empirically with *flucloxacillin
Remove catheter if no longer needed. Initial empirical therapy including glycopeptide Treat for 10-14 days or longer until infection resolved.
Modify according to isolates Remove catheter if evidence of progression or if blood cultures are positive for Staph. aureus, Pseudomonas spp, Mycobacterium spp., or fungi
Tunnel infection Remove catheter if no longer needed Treat empirically with *flucloxacillin *Unless patient known or suspected to be MRSA positive.
Remove catheter if no longer needed. Initial empirical therapy including glycopeptide Treat for 10-14 days or longer until resolution of soft tissue infection. Modify according to isolates. If tracking continues to spread remove catheter.
Presumed catheter-related bloodstream infection
Remove catheter if no longer needed. Treat empirically with antibiotics targeted against isolates. *Unless patient known or suspected to be MRSA positive.
Remove catheter if no longer needed. Initial empirical antibiotic therapy. Modify according to isolates.
Treat for at least 10-14 days Remove catheter if cultures remain positive after 48 hours of therapy or if proven catheter-related infection with Staph. aureus, Pseudomonas spp,, Mycobacterium spp., or fungi
* Unless known to be colonised with MRSA, when a glycopeptide should be used. Removal of Groshong/Hickman lines Removal of CVCs: should only be undertaken by staff with the appropriate skills and knowledge. On removal, all CVC tips should go to microbiology for culture and sensitivity.

OP 41 Central Venous Line Policy
Page 18 of 21
Appendix 4
Gateshead Health NHS Foundation Trust
Guidelines for nursing staff on the care and management of Hickman Lines
The following guidelines are a reference material to professionals caring for central venous access devices within Gateshead Health NHS Foundation Trust. However, any professional performing these cares must first have been assessed and deemed competent within the Trust/organisation. All practitioners must ensure they are aware of and working within their personal and professional accountability. The term Central Venous Access Device (CVAD) or Central Venous Catheter (CVC) implies that the tip of the device is positioned in the lower third of the superior vena cava (SVC). For the purpose of this document CVC will include:
• Tunneled catheters – generally inserted via the jugular vein, with the other end being tunnelled under the skin and exiting on the chest.
• Peripherally inserted catheters (PICC’s) – which are inserted through an antecubital
vein or upper arm vein and threaded up to the SVC.
Hickman Catheters A Hickman line is a narrow tube, made of silicone rubber or polyurethane. It can be single or double lumen. Double lumen Hickman lines have a red lumen for blood sampling and infusion of blood products, and a white lumen for infusion of other crystalloid products. These catheters have an open ended tip and therefore have a clamp on each lumen to prevent bleeding and air embolism.
Back to contents

OP 41 Central Venous Line Policy
Page 19 of 21
Maintaining patency of a Hickman central venous catheter (single or double lumen) Equipment required:
*Clean trolley 1 dressing pack 1 pair of sterile gloves 1 x 10ml luer lock syringes (2 if double lumen) 6mls heparin sodium solution 10units/ml (12mls if double lumen) 1 needle free bung (2 if double lumen) ChloraPrep 3ml solution 1 Sani cloth to cleanse line(2 needed if double lumen line) 1 x 21G needle (green for drawing up heparin) 1 apron 1 pair of non sterile gloves 1 sharps bin and a orange clinical waste bag transparent, occlusive dressing e.g. IV 3000
Procedure

OP 41 Central Venous Line Policy
Page 20 of 21
ACTION RATIONALE 1 Explain and discuss the procedure with
the patient. To gain the patient’s co-operation and understanding as well as informed consent.
2 Apply apron and wash hands thoroughly. To reduce the potential for the spread of infection.
3 Clean trolley. Open the dressing pack and place equipment onto sterile field.
To provide a sterile working area.
4 Remove old dressing with non-sterile gloves. Check exit site of line for any signs of infection. Redness, swelling, oozing. If present inform clinician.
Safety of patient – line may need removed or antibiotic cover given.
5 Wash hands. Put on sterile gloves and draw up 6ml of heparin into the syringe.
To maintain a sterile working area.
6 Place sterile drape under the CVC. To provide a sterile working area and prevent contaminating the CVC during the procedure.
7 Swab the injection bung with Sane cloth and allow to dry.
To reduce the number of microbiological organisms that may be colonizing the injection bung.
8 Ensuring the clamp is closed, remove the old injection cap and attach a syringe.
9 Draw back approximately 3 - 4 mls of blood. Close clamp.
Ensures line patent.
10 Ensuring clamp is closed attach the pre-filled syringe. Then open clamp.
To establish a connection between the line and the syringe and minimize the risk of air embolism.
11 Using a push-pause method (inject 1ml at a time), inject the contents of the syringe. Apply the clamp, whilst pushing, when last 0.5 mls remain.
To create turbulence in order to flush the catheter thoroughly. Applying the clamp whilst still injecting the heparin helps to prevent blood from backing up into the catheter.
12 Remove syringe and replace with new injection cap. If flushing a double lumen line, treat each lumen separately and repeat these steps for the second lumen.
To keep lumen sterile.
13 Clean the exit site with ChloraPrep 3 ml solution
To reduce the number of microbiological organisms.
14 Apply new dressing. Dispose of equipment safely and in accordance with Trust policy. Document procedure.
To prevent contamination of others and maintain safe practice. Occlusive dressing helps to prevent bacterial contamination.

OP 41 Central Venous Line Policy
Page 21 of 21
Blood sampling from a Hickman central venous catheter (single or double lumen) Equipment required:
Use equipment as for line flush. Also include the additional items listed below. 2 x 10ml syringes (4 if double lumen) blood collection tubes
Procedure Follow the procedure for maintaining line patency through steps 1-7. Please note: When obtaining a blood sample from a double lumen line the sample should be taken from the RED lumen as outlined in the table below. The WHITE lumen just needs to be flushed as outlined above. The white lumen can be used for sampling if you are unable to use the red lumen. BLOOD SAMPLING
ACTION RATIONALE 8 Ensuring the clamp is closed, remove
the old injection cap and attach one of the empty syringes.
To establish a connection between the line and the syringe and minimize the risk of air embolism.
9 Pull back the syringe plunger whilst releasing the clamp. Aspirate 5ml of blood, re-apply the clamp and discard the syringe.
The heparin solution in the blood may dilute the specimen and alter results.
10 Attach an empty 10 or 20ml syringe (depending on samples required) and aspirate, whilst opening the clamp, required amount of blood.
To obtain specimen.
11 Re-apply clamp, remove syringe and attach a pre-filled syringe of heparin sodium solution.
To establish a connection between the line and the syringe.
12 Using a push-pause method (inject 1ml at a time), inject the contents of the syringe. Apply the clamp, whilst pushing, when last 0.5 mls remain.
To create turbulence in order to flush the catheter thoroughly. Applying the clamp whilst still injecting the heparin helps to prevent blood from backing up into the catheter.
13 Remove syringe and replace with new injection cap.
To keep lumen sterile.
14 Place blood in collection tubes and label correctly as per hospital policy.
To ensure positive patient identification.
15 Clean the exit site with ChloraPrep 3 ml solution. Allow to dry.
To reduce the number of microbiological organisms.
16 Apply new dressing. Dispose of equipment safely and in accordance with Trust policy. Document procedure.
To prevent contamination of others and maintain safe practice. Occlusive dressing helps to prevent bacterial contamination.




















![[Clarinet Institute] Andersen Etudes Op41](https://img.pdfslide.us/doc/110x75/5695d4f31a28ab9b02a36d1a/clarinet-institute-andersen-etudes-op41.jpg)