Embed Size (px)
Citation preview

Page 1
Learning Objectives
1. Discuss the role of the B‐cell receptor (BCR) pathway in the survival and proliferation of cancer cells.
2. Evaluate clinical efficacy data for first‐ and second‐generation BTK inhibitors in select B‐cell malignancies (e.g., CLL/SLL, MCL) and explore the rationale for combination therapy with other antineoplastic agents.
3. Assess potential toxicities that may arise with the use of BTK inhibitors and explore evidence‐based strategies to ensure the timely recognition and proper management of these adverse events.
4. Using a case‐based approach, examine effective strategies that oncology nurses can employ to optimize therapy, anticipate and manage adverse events, improve adherence to oral chemotherapy, and promote collaborative discussion with other members of the oncology care team to ensure optimal patient outcomes.
BCR=B‐cell receptor; BTK=Bruton’s tyrosine kinase; CLL=chronic lymphocytic leukemia; MCL=mantle cell lymphoma; SLL=small lymphocytic lymphoma.

Page 2
Disclaimer
• This slide deck in its original and unaltered format is for educational purposes and is current as of May
18, 2018. All materials contained herein reflect the views of the faculty, and not those of Creative
Educational Concepts, Inc. or the commercial supporter(s).
• Participants have an implied responsibility to use the newly acquired information to enhance patient
outcomes and their own professional development. The information presented in this activity is not
meant to serve as a guideline for specific patient management.
• Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this
activity should not be used by clinicians without evaluation of their patient’s conditions and possible
contraindications on dangers in use, review or any applicable manufacturer’s product information, and
comparison with recommendations of other authorities.
• Usage Rights: This slide deck is provided for educational purposes and individual slides may be used for
personal, non‐commercial presentations only if the content and references remain unchanged. No part
of this slide deck may be published or distributed in print or electronic format without prior written
permission from Creative Educational Concepts, Inc. Additional terms and conditions may apply.
Introduction to the BCR Pathway and its Role in B‐cell Malignancies
Nina Wagner, BSN, MDAssociate Professor of OncologyJohns Hopkins Sidney KimmelComprehensive Cancer Center
Baltimore, Maryland

Page 3
Objectives
• Discuss the role of the BCR pathway in the survival and proliferation of cancer cells
• Evaluate clinical efficacy data for BTK inhibitors in select B‐cell malignancies
• Explore the rationale for combination therapy
Outline
• Overview of the BCR pathway• Pathogenesis
• BTK, SYK, PI3K
• BTK inhibitors in B‐cell lymphomas• Efficacy as single agents
• Rationale for combination
• Resistance mechanisms
SYK=spleen tyrosine kinase; PI3K=phosphoinositide 3‐kinase.

Page 4
• Located on outer surface of B lymphocytes
• Extends above/below the plasma membrane
• Controls B‐cell activation
• Required for antibody production
What is the B‐cell Receptor?
Rye C, et al. Biology. 2017.Ig=immunoglobulin.
Antigen binding site
Disulfidebridge
Light chain
Heavy chain
Variableregion
Constantregion
Signal transduction region
B‐cell plasmamembrane
IgαIgβ
Critical Enzymes Control BCR Pathway
Choi MY, Kipps TJ. Cancer J. 2012.

Page 5
Recurrent Mutations in BCR Pathway Identified in Lymphoma
Krysiak K, et al. Blood. 2017.
Inhibitors of Critical Enzymes in the BCR Pathway
Choi MY, Kipps TJ. Cancer J. 2012; FDA Prescribing Information; Clinicaltrials.gov.
Fostamatinib
IbrutinibAcalabrutinib
IdelalisibCopanlisibDuvelisib
TemsirolimusEverolimus

Page 6
Bruton’s Tyrosine KinaseCritical Kinase for Lymphoma Cell Survival and Proliferation
Davids M, et al. Future Oncol. 2014.
Cytogenetics Drive CLL Biology
Zenz T, et al. Blood. 2009; Stilgenbauer S, et al. J Clin Oncol. 2009; Rossi D, et al. Clin Cancer Res. 2009; Zenz T, et al. J Clin Oncol. 2010; Gonzalez D, et al. J Clin Oncol. 2011; Badoux XC, et al. Blood. 2011; Zainuddin N, et al. Leuk Res. 2011; Hernandez JA, et al. PLoS One. 2015.
del(17p)Complex karyotypedel(11q)Trisomy 12del(13q)Others
Months
PFS (probab
ility)
1.0
0.8
0.6
0.4
0.2
0.0
0 24 48 84 10812 36 60 9672
PFS in Cytogenetic SubgroupsPhase II Study of ≥2 line Chemoimmunotherapy
LesionPrevalence at CLL Diagnosis, %
Prevalence in Relapsed/refractory
CLL, %
TP53 mutation ~5–10% ~40%
del(11q) ~11% ~20%
del(17p) alone ≤5% ~30%
PFS=progression‐free survival.

Page 7
IbrutinibBTK Inhibitor, Highly Active in CLL
Byrd JC, et al. N Engl J Med. 2013; O’Brien S, et al. Blood. 2018.
ORR: 71%ORR: 89% PR with lymphocytosis
ORR=objective response rate; PR=partial response.
Progression‐free survival, %
Months from Initiation of Study Treatment
0 12 24 42 546 18 30 4836 66 787260
0
20
40
60
80
100
del(17p)
del(11q)Trisomy 12
del(13q)No abnormality
Patients with a Response (%)
Month
Complete response plus partial response
Partial response with lymphocytosis
Stable disease
Phase II Study of Ibrutinib in Mantle Cell Lymphoma
Comparison with previously available agents for mantle cell
• Bortezomib
• ORR: 33%; CR: 8%
• Lenalidomide
• ORR: 28%; CR: 7.5%
Fisher RI, et al. J Clin Oncol. 2006; Goy A, et al. J Clin Oncol. 2013; Wang ML, et al. N Engl J Med. 2013.CR=complete response.
Median 3 prior treatmentsORR: 68%CR: 21%Median PFS: 13.9 mo
Page 8
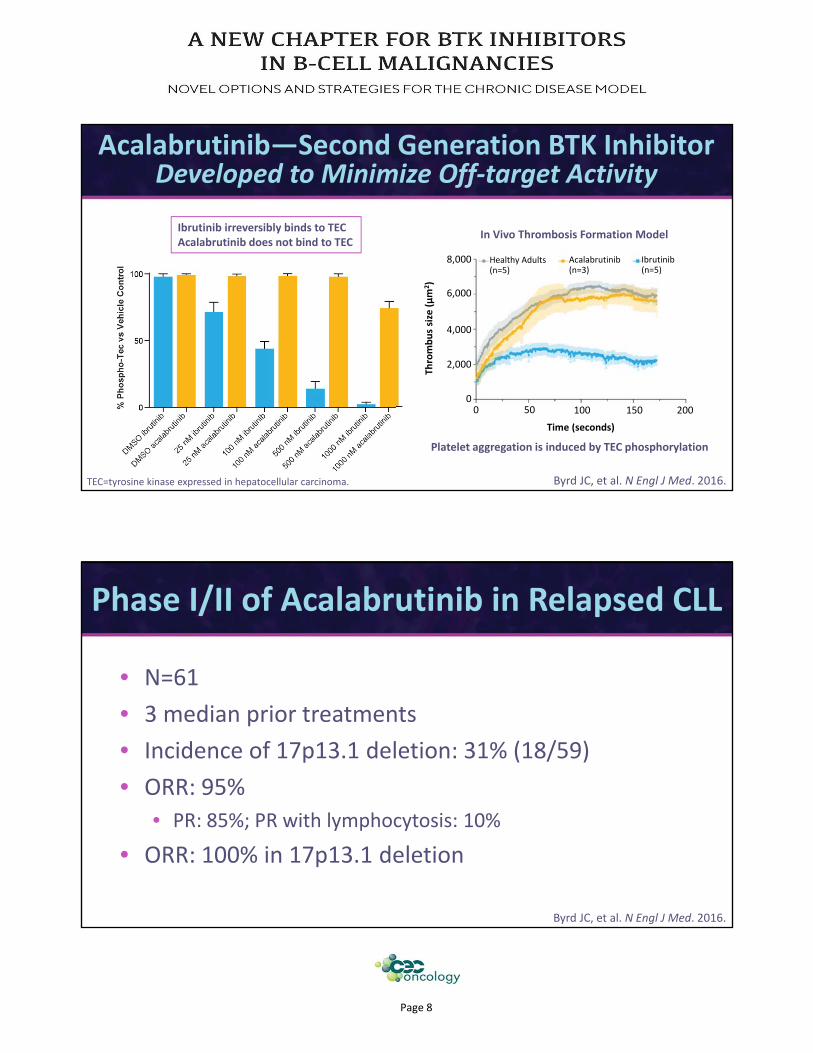
Acalabrutinib—Second Generation BTK Inhibitor Developed to Minimize Off‐target Activity
Byrd JC, et al. N Engl J Med. 2016.
In Vivo Thrombosis Formation Model
Platelet aggregation is induced by TEC phosphorylation
Ibrutinib irreversibly binds to TECAcalabrutinib does not bind to TEC
TEC=tyrosine kinase expressed in hepatocellular carcinoma.
0 20050 1500
8,000 Healthy Adults (n=5)
Acalabrutinib(n=3)
Ibrutinib(n=5)
Time (seconds)
100
2,000
4,000
6,000
Thrombus size (µm
2)
• N=61
• 3 median prior treatments
• Incidence of 17p13.1 deletion: 31% (18/59)
• ORR: 95%
• PR: 85%; PR with lymphocytosis: 10%
• ORR: 100% in 17p13.1 deletion
Phase I/II of Acalabrutinib in Relapsed CLL
Byrd JC, et al. N Engl J Med. 2016.

Page 9
• Excluded prior BCR pathway inhibitors or BCL‐2 inhibitors
• Median 2 prior therapies
• ORR: 81%; CR: 40%
• Median PFS not reached at median follow‐up of 15.2 months
• 12 month PFS: 67%
Phase II Study of Acalabrutinib in Mantle Cell Lymphoma
Wang ML, et al. Lancet. 2018.BCL=B‐cell lymphoma.
• Tirabrutinib (ONO‐4059/GS‐4059)
• Phase I data reported in relapsed/refractory B‐cell/NHL
• Phase II studies underway in CLL
• Zanubrutinib (BGB‐3111)
• Phase I data reported in advanced B‐cell/NHL
• No related bleeding or Afib in early evaluation
• Phase III studies underway in CLL/SLL, WM
BTK InhibitorsInvestigational Agents
Morschhauser F, et al. ICML. 2017. Abstract 276; Clinicaltrials.gov; Tam CS, et al. ASH. 2017. Abstract 152.
WM=Waldenstrom macroglobulinemia;Afib=atrial fibrillation; NHL=non‐Hodgkin lymphoma.

Page 10
Comparison of Single Agent Ibrutinib to Ibrutinib + Rituximab
ALC=absolute lymphocyte count. Adapted from Burger JA, et al. ASH. 2017. Abstract 427.
ORRIbrutinib: 98% Ibrutinib + Rituximab: 100%
0 2 4 16 361 3 8 2412 60 847248 96 120 144
0
50
100
150Ibrutinib
Ibrutinib + Rituximab
Time, weeks
ALC (K/µL)
363024181260
02849728495102
12850688292104
No. at RiskIbrutinib
Ibrutinib + Rituximab
MonthsProportion Progression‐free
0.00
0.25
0.50
0.75
1.00
Ibrutinib: 102 (9) 94% (87‐98)Ibrutinib + Rituximab: 104 (10) 93% (84‐97)
N (Deaths) 2 year (95% CI)
P=0.788
Ibrutinib Interferes with Cell‐mediated Anti‐tumor Activities of Anti‐CD20 Antibodies
Da Roit F, et al. Haematologica. 2015.
ADCC=antibody‐dependent cell‐mediated cytotoxicity;NK=natural killer (cells); OBZ=obinutuzumab; OFA=ofatumumab; PBMC=peripheral blood mononuclear cells; RTX=rituximab; TRZ=trastuzumab.

Page 11
Phase III Study of Bendamustine and Rituximab ± Ibrutinib in Relapsed CLL
Chanan‐Khan A, et al. Lancet Oncol. 2016.
Less Lymphocytosis
OR=overall response; PD=progressive disease; CRi=complete remission with incomplete hematologic recovery; PR+L=partial response with lymphocytosis; SD=stable disease.
Progression‐free survival (%)
Time (months)
Ibrutinib, bendamustine, and rituximab
Placebo, bendamustine, and rituximab
0 8 16 284 12 20 32240
20
40
60
80
100OR 82.7% vs 67.8% (P<0.0001)
Proportion of patients (%)
0
20
40
60
80
100
Ibrutinib, bendamustine,and rituximab
Placebo, bendamustine,and rituximab
CRCRiPR
CRCRiPR
PR+L PR+L SDSD PD PD
72.3%
10.4%
2.8%
23.9%
2.1%
8.7%
65.1%
0.7% 0.3% 0.0%
Arguments For/Against Chemotherapy Combinations
FOR• BTK gene modulation may overcome chemo resistance (bortezomib)
AGAINST• BTK inhibition arrests G1 phase of cell cycle which may decrease activity of chemo that works at later cell cycle phases
Is it Rational to Combine BTK Inhibitors with Cytotoxic Agents?
Murray MY, et al. Cell Cycle. 2015; Yue C, et al. J Exp Clin Cancer Res. 2017.

Page 12
• Horizontal BCR Inhibitor Combinations• PI3K• SYK
• Downstream Combinations• Resistance due to activation of transcription downstream or outside of PI3K (e.g., MYC amplification)
• BET inhibitor → downregulates transcrip on of MYC• CDK4/6 inhibitor (palbociclib)• BCL‐2 inhibitor (venetoclax)
What are Potential Rational Combinations with BTK inhibitors?
Ilic N, et al. Proc Nat Acad Sci USA. 2011; Chiron D, et al. Cancer Discov. 2014; Boi M, et al. Clin Cancer Res. 2015;
Barr PM, et al. Blood. 2016; Kuo HP, et al. Mol Cancer Ther. 2017; Bernasconi E, et al. Br J Haematol. 2017; Tam CS, et al. N Engl J Med. 2018.
BTKi is mostly cytostatic“Apoptotic Priming” with BTKi
CDK=cyclin‐dependent kinase;BTKi=Bruton’s tyrosine kinase inhibitor;BET=bromodomain and extraterminal motif.
• Historically, each produces CR rates of 21%
• At week 16, ORR: 71%, CR: 62%
• Overall CR rate: 71%
Phase II Study of Ibrutinib and Venetoclax(BCL‐2 inhibitor) for Mantle Cell Lymphoma
Tam CS, et al. N Engl J Med. 2018.
Estimated 18 mo PFS: 57%
0 6 12 213 9 15 24180
20
40
60
80
100
Months
10
30
50
70
90
24 18 18 121 18 10 17No. at Risk
Patients Alive an
d Free
from Progression (%)

Page 13
• BTK structure has cysteine in ATP‐binding pocket. BTK inhibitors bind covalently to Cys481.
• Mutations of the cysteine residue (Cys481) where binding occurs identified in ibrutinib and acalabrutinib.
• Mutations of PLCγ2 and CARD11 immediately downstream of BTK.
Resistance Mechanisms for BTK Inhibitors
Woyach JA, et al. N Engl J Med. 2014; Byrd JC, et al. N Engl J Med. 2016; Xu L, et al. Blood. 2017.
ATP=adenosine triphosphate; CARD11=caspase recruitment domain‐containing protein 1; PLCγ2=phospholipase C gamma 2
Ibrutinib (nM)
1.0
0.8
0.6
0.4
0.2
0.0
‐0.2
Kinase Activity
(norm
alized to activity in untreated control)
0 1 10 100 1000 10,000
Mutant BTK
Non‐mutant BTK
Dismal Outcomes in MCL Patients Who Progress After Ibrutinib
Adapted from Martin P, et al. Blood. 2016.
Median OS following ibrutinibcessation was 2.9 mo
3111473
0 10 20 30 40
24038
01818
1010
66
44
33
11
00
Overall Survival (Month)
Survival Probab
ility
Group
Did not receive subsequent treatment
Received subsequent treatmentOverall
1.0
0.8
0.6
0.4
0.2
0.0123
+ CensoredLog rank P<0.0001
OS=overall survival.

Page 14
• BTK is an integral component of the BCR pathway
• BTK inhibitors are highly effective as single agents in CLL and MCL
• Resistance, while rare, is a well‐recognized phenomena with poor prognosis
Conclusions
BTK Inhibitor Toxicities
Mollie E. Moran, MSN, CNP, AOCNPOncology Nurse Practitioner
Division of Hematology and OncologyArthur G. James Cancer Hospital
The Ohio State UniversityColumbus, Ohio

Page 15
Potential Toxicities with BTK Inhibitors
• Understand how BTK inhibitor off‐target activity can lead to the formation of certain toxicities
• Differences between first‐ and second‐generation inhibitors (selectivity, off target effects, monitoring considerations)
• Therapy management considerations based on patient specific factors (age, prior treatments, comorbidities, tolerability)
aPatients in the ibrutinib arm had a >50% longer AE reporting period than those on ofatumumab (median of treatment duration 8.6 vs. 5.3 months, respectively); there was no adjustment for exposure duration; bTEAEs reported in all patients who received study drug.
Ibrutinib Side Effects—RESONATE Trial Safety Adverse Events (≥15%) Regardless of Attributiona
Ibrutinib(N=195)
Ofatumumab(N=191)
Any Grade Grade 3/4 Any Grade Grade 3/4
Any TEAE, % 99 51 98 39
Diarrhea 48 4 18 2
Fatigue 28 2 30 2
Nausea 26 2 18 0
Pyrexia 24 2 15 1
Anemia 23 5 17 8
Neutropenia 22 16 15 14
Cough 19 0 23 1
Thrombocytopenia 17 6 12 4
Arthralgia 17 1 7 0
Upper respiratory tract infection 16 1 10 2
Constipation 15 0 9 0
Infusion‐related reaction 0 0 28 3
Byrd JC, et al. N Engl J Med. 2014.AE=adverse event; TEAE=treatment‐emergent adverse event.

Page 16
1Ibrutinib Prescribing Information. 2Leong DP, et al. Blood. 2016. 3Byrd JC, et al. Blood. 2015. 4Lipsky AH, et al. Haemotolgica. 2015. 5Mato AR, et al. Blood. 2016. 6Byrd JC, et al. N Engl J Med. 2013. 7Bitar C, et al. JAMA Dermatol. 2016.
Adverse Effect Incidence
Afib1,2~5x increase with ibrutinib
3.3 events per 100 person‐years; RR: 3.9 vs. comparator; (P<0.0001)
Bleeding3,461% (53% grade 1/2)
55% (all grade 1/2)
Hypertension1 6%–17% (Median time to onset: ~5 months)
Pneumonitis5 Not yet defined
Skin (rash)6 27%
Hair/Nail Changes7 67% nail, 26% hair
Diarrhea1 43% all grades (Median time to onset: ~10 days; ~74 days for ≥grade 3)
Lymphocytosis1CLL: 66% all grades (Median time to onset: ~4 weeks)MCL: 33% all grades (Median time to onset: first few weeks)
RR=relative risk.
IbrutinibSafety
IbrutinibSafety
Hypertension (HTN)• Increases in patients on ibrutinib over time and often requires initiation or increase
of anti‐hypertensive therapy (monitor patients for new onset HTN that is not adequately controlled)
• The ≥grade 3 incidence is 4%–13% at years 1–2 but rises to 25%–32% with 5‐year follow‐up in clinical trials. However, frequency has been found to be relatively constant after second year of therapy.
• Note: Over 60% of patients who experienced ≥grade 3 HTN had pre‐existing HTN
• Across trials, ibrutinib discontinuation/dose reduction was infrequent, suggesting that with appropriate management, patients can remain on therapy.
• “2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines”
FDA Prescribing Information; Byrd JC, et al. N Engl J Med. 2013; Burger JA, et al. N Engl J Med. 2015; Byrd JC, et al. Blood. 2015; O’Brien S, et al. Lancet Oncol. 2016; Coutre SE, et al. Clin Cancer Res. 2017;
Whelton PK, et al. J Am Coll Cardiol. 2017; O’Brien S, et al. Blood. 2018; Brown JR, et al. Leukemia. 2018.

Page 17
• MCL and MZL: 560 mg PO once daily
• CLL/SLL, WM, and cGVHD: 420 mg PO once daily
• Take with a glass of water
• Do not open, break, or chew capsules or tablets
• Missed dose: Take as soon as possible on same day, returning to normal schedule following day. Extra doses should not be taken.
Ibrutinib Dose and Administration
FDA Prescribing Information.cGVHD=chronic graft versus host disease; MZL=marginal zone lymphoma.
• New formulation ibrutinib tablets are available in 140 mg, 280 mg, 420 mg, and 560 mg dosage strengths
• Now comes in a 28‐day blister pack
• Ibrutinib 140 mg capsules no longer available after May 15, 2018
• Be sure that patients are aware of the change to the number of pills they will be taking on a daily basis
Ibrutinib Dose and Administration
FDA Prescribing Information.

Page 18
Second‐Generation BTKis
• Up to 20% of patients discontinue ibrutinib due to toxicities• Next‐generation agents have thus far been associated with comparable efficacy
to ibrutinib but with greater tolerability in R/R MCL. Studies in MCL and other B‐cell malignancies (e.g., CLL/SLL) are ongoing.
• Compared to ibrutinib, newer agents associated with reduction or elimination of:• Atrial fibrillation• Skin toxicity• Pneumonitis• Bleeding complications
• Acalabrutinib indicated for the treatment of adult patients with mantle cell lymphoma who have received at least one prior therapy
Walter HS, et al. Blood. 2017; FDA Prescribing Information.R/R=relapsed and/or refractory.
• Second‐generation, selective, irreversible inhibitor of BTK
• Improved pharmacologic features
• Favorable plasma exposure
• Rapid oral absorption
• Short half‐life
• Absence of irreversible targeting to alternative kinases (greater selectivity for BTK leads to fewer off‐target effects)
• EGFR (epidermal growth factor receptor)
• TEC (tyrosine kinase expressed in hepatocellular carcinoma)
• ITK (interleukin‐2–inducible T‐cell kinase)
Byrd JC, et al. N Engl J Med. 2016.
AcalabrutinibAgent Overview

Page 19
• Well tolerated• Most common AEs: headache, diarrhea, weight gain
• Compared to ibrutinib• Overlapping toxicities: mild diarrhea, infections
• New toxicities: headache, weight gain
• Less commonly seen with acalabrutinib: Afib, significant skin toxicity, pneumonitis, major hemorrhage
AcalabrutinibSafety
Byrd JC, et al. N Engl J Med. 2016; Wang M, et al. Lancet. 2018; FDA Prescribing Information.
Adverse Events All Grades Grades 1–2 Grades 3–4
Number of patients (%)
Headache 26 (43) 26 (43) 0
Diarrhea 24 (39) 23 (38) 1 (2)
Increased weight 16 (26) 15 (25) 1 (2)
Pyrexia 14 (23) 12 (20) 2 (3)
Upper respiratory tract infection
14 (23) 14 (23) 0
Fatigue 13 (21) 11 (18) 2 (3)
Peripheral edema 13 (21) 13 (21) 0
Hypertension 12 (20) 8 (13) 4 (7)
Nausea 12 (20) 12 (20) 0
Contusion 11 (18) 11 (18) 0
Arthralgia 10 (16) 9 (15) 1 (2)
Petechiae 10 (16) 10 (16) 0
Decreased weight 10 (16) 10 (16) 0
• MCL: 100 mg PO every 12 hours
• Take with a glass of water
• Do not open, break, or chew capsules or tablets
• Missed dose: If missed by >3 hours, skip dose and take the next dose at the regularly scheduled time. Extra doses should not be taken.
FDA Prescribing Information.
Acalabrutinib Dose and Administration
Page 20
Management of Common BTK Inhibitor Toxicities
Lymphocytosis
• Usually peaks after the first few weeks of therapy (up to 19 weeks has been observed with ibrutinib therapy)
• Does not signify disease progression
• Lymphocytosis usually asymptomatic
• Resolves with continued therapy
Neutropenia
• Consider growth factor support
Byrd JC, et al. Blood. 2015; NCCN CLL/SLL Guidelines. v5.2018.
Management of Common AEs in BTKis

Page 21
Cytopenias (≥grade 3)
FDA Prescribing Information.
Management of Common AEs in BTKis
Monitor blood counts monthly while on therapy or per institutional protocol (i.e., weekly for the first month, monthly for 3 months, then every 3 months while on therapy).
Neutropenia
• Ibrutinib: 13%–29%
• Acalabrutinib: 23%
Thrombocytopenia
• Ibrutinib: 5–17%
• Acalabrutinib: 8%
Anemia
• Ibrutinib: 0%–13%
• Acalabrutinib: 11%
Bleeding
• Fatal bleeding events have occurred in in patients treated with BTK inhibitors.
• The risk/benefit ratio should be evaluated for patients on any anti‐platelet or anticoagulant therapies. Concomitant administration of BTKis with warfarin should be avoided.
• BTKis should be held at least 3–7 days pre‐ and post‐surgery depending on the surgery and risk of bleeding.
Cardiac Arrhythmias
• Obtain ECG for patients who are symptomatic (e.g., palpitations, light headedness, syncope, chest pain, etc.)
• Afib/flutter
• Acalabrutinib: 1% grade 3
• Ibrutinib: up to 6% ≥grade 3FDA Prescribing Information; NCCN CLL/SLL Guidelines. v5.2018.
• Ventricular tachyarrythmias
• Ibrutinib: 0%–1% ≥grade 3
Management of Common AEs in BTKis
Any grade (~50% of patients treated with BTKis)≥ Grade 3 (ibrutinib: 6%; acalabrutinib: 2%)
ECG=electrocardiogram.

Page 22
Nausea and Vomiting (~20% all grades)
• BTKis have minimal to low emetic risk (<30% frequency of emesis)
• 5‐HT3 receptor antagonists (dolasetron, granisetron, ondansetron), metoclopramide, and prochlorperazine
• Recommended PRN. Start before therapy and continue daily.
Diarrhea (~40% all grades)
• Generally self‐limiting, typically resolving without additional therapy
• Symptomatic management with anti‐motility agents once infectious etiologies have been ruled out
Management of Common AEs in BTKis
NCCN Antiemesis Guidelines. v2.2018; Byrd JC, et al. Blood. 2015; FDA Prescribing Information.
Infection• Continues to be one of the main problems in CLL/SLL patients
• Identify early and treat as indicated
• CLL/SLL has an intermediate risk of infection. NCCN recommends the following prophylactic measures during neutropenia:
• Fluoroquinolone and TMP/SMX (PCP prophylaxis)
• Fluconazole or micafungin
• Acyclovir, famciclovir, or valacyclovir (HSV prophylaxis—Consider during active therapy and possibly longer depending on degree of immunosuppression)
• While IVIG has been used as a supportive care measure in clinical trials and has been associated with a significant decrease in the occurrence of infections, there has been no demonstrable improvement in OS outcomes with its use
Byrd JC, et al. Blood. 2015; NCCN CLL/SLL Guidelines. v5.2018; NCCN Prevention and Treatment of Cancer‐related Infections Guidelines. v1.2018.
Management of Common AEs in BTKis
PCP=Pneumocystis pneumonia; SMX=sulfamethoxazole; TMP=trimethoprim;HSV=herpes simplex virus; IVIG=intravenous immunoglobulin.

Page 23
Toxicity Occurrence
Dose Modification
Ibrutinib 560 mg Ibrutinib 420 mg Acalabrutinib 100 mg
FirstInterrupt therapy until resolved to grade 1 or baseline. May be initiated at starting dose.
Interrupt therapy until resolved to
grade 1 or baseline level. May be
resumed at 100 mg daily.
Second
Interrupt therapy until resolved to grade 1. Restart at
420 mg daily.
Interrupt therapy until resolved to grade 1. Restart at
280 mg daily.
Third
Interrupt therapy until resolved to grade 1. Restart at
280 mg daily.
Interrupt therapy until resolved to grade 1. Restart at
140 mg daily.
Fourth Discontinue
Dose Modifications Due to AEs
FDA Prescribing Information.
• Ibrutinib: ≥grade 3 non‐hematological toxicities, ≥grade 3 neutropenia with infection or fever, or grade 4 hematological toxicities.
• Acalabrutinib: ≥grade 3 non‐hematological toxicities, grade 3 thrombocytopenia with bleeding, grade 4 thrombocytopenia, and grade 4 neutropenia lasting longer than 7 days.
CYP3A4/5 Inhibitors*
Clarithromycin
Itraconazole
Ketoconazole
Ritonavir
Erythromycin
Diltiazem
Fluconazole
Grapefruit juice
Seville oranges
Verapamil
Cimetidine
SafetyConcomitant Medications
*Not a complete list
https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm093664.htm.
• Avoid co‐administration with strong CYP3A4 inhibitors/inducers
• If CYP3A inhibitors are to be used short‐term (such as anti‐infectives for up to 7 days, interrupt therapy)
• Dose reductions are recommended when BTK inhibitor is co‐administered with moderate CYP3A inhibitors
• Acalabrutinib: Avoid co‐administration with proton pump inhibitors (e.g., omeprazole), take 2 hours before taking H2‐receptor antagonists (e.g., ranitidine), and separate dosing by at least 2 hours with antacids.
CYP3A4/5 Inducers*
Carbamazepine
Phenytoin
Rifampin
St. John’s wort
Modafinil
Rufinamide

Page 24
Shifting to a Chronic Disease Model in B‐cell Malignancies: Case‐based Treatment
Strategies for the Oncology Nurse
Katherine Stephans, MS, ANPDivision of Hematologic Malignancies
Lymphoma and Stem Cell Transplant ProgramsDana‐Farber Cancer Institute
Boston, Massachusetts
NCCN CLL Guidelines: Preferred Regimens
NCCN CLL/SLL Guidelines. v5.2018.
First‐line
Later‐line Frail w/ significant
comorbidities
≤65 w/o significant
comorbidities
Ibrutinib* FCR* Ibrutinib*
Obinutuzumab+ chlorambucil*
IbrutinibIdelalisib + rituximab*
Rituximab + chlorambucil
Bendamustine ±CD20 mAb
Venetoclax + rituximab*
Rituximab + ofatumumab
—— ——
*Category 1.
BTK InhibitorsThe “No Chemo” Era
CLL without del17p CLL with del17p
First‐line Later‐line
Ibrutinib
Ibrutinib*
Venetoclax + rituximab*
Idelalisib + rituximab
Venetoclax
FCR=fludarabine, cyclophosphamide, rituximab; mAb=monoclonal antibody.

Page 25
• New standards of oncologic therapy require new mindset for patient management• Therapy moving from the controlled, clinic setting to the home• Therapy moving from short‐term to long‐term, possibly lifetime
• With these changes, cancer care more closely follows the chronic disease model• Substantial number of patients struggle to adhere to oral anticancer regimens
• Studies of Americans with cancer suggest that most prefer learning detailed information about their disease and its prognosis in a direct and honest manner• However, many patients have little understanding of their disease prognosis,
treatment options or sources of support
AdherenceA New Challenge in Era of Targeted Therapies
Stacey D, et al. Cochrane Database Syst Rev. 2017; Greer JA, et al. Oncologist. 2016; https://www.ahrq.gov/professionals/education/curriculum‐tools/shareddecisionmaking/index.html.
• When clinician and patient work together to make a healthcare decision that is best for the patient
• Optimal decision takes into account evidence‐based information about available options, the provider's knowledge and experience, and the patient's values and preferences
• Patients who are engaged in SDM are more often satisfied with their outcomes, even when met with unexpected or unfavorable side effects
Improving Adherence Shared Decision Making (SDM)
Stacey D, et al. Cochrane Database Syst Rev. 2017;http://connect.ons.org/issue/february‐2016/up‐front/making‐treatment‐decisions‐together.

Page 26
• Barriers to effective use of SDM among healthcare providers (HCPs)• Lack of familiarity with SDM approaches• Lack of familiarity of the role of the nurse navigator • Providers feels threatened by involvement of the nurse navigator
• Time Although time is among the biggest perceived barriers, research shows that clinicians can implement SDM without increasing visit duration.
Stacey D, et al. Cochrane Database Syst Rev. 2017;http://connect.ons.org/issue/february‐2016/up‐front/making‐treatment‐decisions‐together.
Improving Adherence Shared Decision Making (SDM)
• BF is a 79‐year‐old female diagnosed in 2016 with CLL with a 17p deletion. She is married to a 72‐year‐old professor who still teaches part time at the local university.
• She is struggling with some early dementia, but still has a good quality of life, enjoying knitting, playing regular bridge games with friends, and traveling to England from time to time to visit family.
• Watchful waiting for 2 years, but she has become increasingly fatigued with recurrent infections. Hgb of 10.2 g/dL, platelet count of 82K.
• BF is originally from England; she has no family nearby and, due to her husband’s schedule, is alone from 8:00 AM–12:00 PM each day.
Case 1CLL
Hbg=hemoglobin.

Page 27
Goals of care: BF wants to have more energy, experience fewer
infections, and have as much time as she can.
Know your options at the start: Ideally, plan is developed over a few
visits. BF wants both written and verbal information about traditional IV
treatment and oral medication.
• BF lives 40 minutes from treatment facility; prefers the oral option of
ibrutinib over the IV option of obinutuzumab/chlorambucil
• She is willing to give up toast with marmalade and take her
medication daily before her husband leaves for work
Using the Shared Care Model, How Do We Help Identify the Best Treatment for BF?
After two months on ibrutinib, BF presents to the clinic…so how is she doing?
• BF and her husband keep track of her pills daily. Her fatigue and blood counts have improved, but she is experiencing 2–3 loose stools per day, as well as some arthralgias and a rash.
• Assess grade of toxicity
• Loose stool: rule out infectious etiology
• Arthralgias:
• Magnesium: yes or no?
• Oral pain medications?
Case 1Conclusion

Page 28
The SHARE ApproachCreated by the Agency for Healthcare Research and Quality (AHRQ)
to foster practitioner utilization of SDM
Seek patient's participation
Help patient explore and compare treatments
Assess patient's values and preferences
Reach a decision with your patient
Evaluate your patient’s decision
https://www.ahrq.gov/professionals/education/curriculum‐tools/shareddecisionmaking/index.html.
Improving AdherenceSHARE
https://www.ons.org/practice‐resources/toolkits/oral‐adherence.
Communication Approaches
Traditional Counseling Motivational Interviewing
• HCP is the healthcare expert• Assumes patient lacks knowledge• Tells patient what to do• Hopes patient follows instructions
• HCP develops partnership with patient• Exchanges information to facilitate an informed decision• Patient has the right to decide own care
• HCP provides definitive information• Directives are presumed to be non‐negotiable
• HCP provides information to patient for the purpose of developing discrepancy between present behavior and goal
• HCP dictates healthcare behavior • HCP and patient negotiate behavior and reach agreement
• Goal is to motivate the patient• Goal is to assess motivation and elicit patient’s
commitment to change behavior
• HCP persuades patient to change behavior • HCP understands and accepts patient’s actions
• HCP expects respect from patient • HCP must earn respect from patient
Improving AdherenceONS Toolkit

Page 29
Barriers to Adherence
https://www.ons.org/practice‐resources/toolkits/oral‐adherence.
Dimension Barriers
Personal and Patient Factors
• Emotional and mental status• Physical status and comorbid conditions• Social supports• Feelings about disease, self‐efficacy, and outcome expectation• Socioeconomic status
Treatment‐related Factors
• Goal of therapy• Complexity of treatment regimen• Immediacy and evidence of benefit• Short‐ and long‐term side effects• Cost of medication and copay
Healthcare System
• Relationship with providers• Communication with providers• Education of patient and caregivers• Satisfaction with care• Insurance coverage• Access to convenient and efficient clinic
Improving AdherenceONS Toolkit
https://www.ons.org/practice‐resources/toolkits/oral‐adherence.
A treatment regimen that is not a good lifestyle fit may result in poor adherence to therapy, and changing one’s lifestyle can be challenging. • Begin by assessing the individual’s readiness to change.• Ask patient to rate how ready he/she is for change by drawing an arrow to or
circling a number in the appropriate area on the scale. • A score >5 indicates patient is ready to work toward changing behavior.
Readiness to Change Scale
0 1 2 3 4 5 6 7 8 9 10
Not Ready Considering Change Ready
Readiness Ruler
Improving AdherenceONS Toolkit

Page 30
• The introduction of kinase inhibitors, with unique toxicities and indefinite dosing, has exponentially increased the monitoring required for a panel of CLL patients
• Collaboration between physicians, nurse practitioners, nurses, and pharmacists is essential to effectively manage these patients• APP‐run oral therapy clinics• APP‐driven toxicity monitoring and therapy• Pharmacist counseling and assistance with insurance approval
APP=advanced practice provider.
Collaborative Management of Patients Receiving Kinase Inhibitors
• AB is a 68‐year‐old female with MCL who is receiving ibrutinib 560 mg PO daily as second‐line therapy
• On treatment for 14 months with good disease control
• AB had been feeling well until 2 months ago, when she began experiencing heart palpitations
• Holter monitor demonstrated intermittent Afib with RVR
• Treatment with calcium channel blocker initiated, followed by amiodarone, without significant decrease in symptoms
• AB reports skipping ibrutinib doses because of fear she’ll have a heart attack
Case Study 2R/R MCL
RVR=rapid ventricular rate.

Page 31
• Switch to acalabrutinib
• Atrial fibrillation likely due to off‐target effects, potentially through TEC leading to PI3K/AKT inhibition
• Acalabrutinib does not appear to be associated with atrial fibrillation, so would be a good choice for this patient
McMullen JR, et al. Blood. 2014.
Case Study 2Conclusion
• JK is a 65‐year‐old female with CLL who receives ibrutinib as third‐line therapy; she has been on treatment for 3 years and feels well
• On routine exam, you note that she has no palpable lymphadenopathy, but ALC has increased from 3000/mL to 6000/mL
• JK reports compliance with ibrutinib• You ask her to return in 2 months
At that time: JK’s ALC has risen to 8000/mL; she remains asymptomatic; new 1.5 cm cervical lymph nodes are noted
Case 3R/R CLL

Page 32
Patient is relapsing on ibrutinib
• Relapse evidenced by increasing WBC count and presence of new palpable adenopathy
With other agents, immediate discontinuation of therapy would be warranted
• Tempo of relapse tends to escalate when ibrutinib is discontinued
• Ibrutinib should be continued until next therapy is started
Case 3Conclusion
• CLL therapy has advanced significantly with the introduction of kinase inhibitors and venetoclax
• With the rapid approval of new agents in CLL with new toxicities and the potential for life‐long therapy, a collaborative approach is necessary to manage these increasingly complex patients
• Collaboration between RNs, APPs, and physicians is especially important during therapy transitions with these novel agents
Conclusions

Page 33
ReferencesAgency for Healthcare Research and Quality (AHRQ). The SHARE Approach. U.S. Department of Health and Human Services website. February 2017. https://www.ahrq.gov/professionals/education/curriculum‐tools/shareddecisionmaking/index.html. Accessed May 2018.
Badoux XC, Keating MJ, Wang X, et al. Fludarabine, cyclophosphamide, and rituximab chemoimmunotherapy is highly effective treatment for relapsed patients with CLL. Blood. 2011;117(11):3016–3024.
Barr PM, Saylors GB, Spurgeon SE, et al. Phase 2 study of idelalisib and entospletinib: pneumonitis limits combination therapy in relapsed refractory CLL and NHL. Blood. 2016;127(20):2411–2415.
Bernasconi E, Gaudio E, Lejeune P, et al. Preclinical evaluation of the BET bromodomain inhibitor BAY 1238097 for the treatment of lymphoma. Br J Haematol. 2017;178(6):936–948.
Bitar C, Farooqui MZ, Valdez J, et al. Hair and nail changes during long‐term therapy with ibrutinib for chronic lymphocytic leukemia. JAMA Dermatol. 2016;152(6):698–701.
Boi M, Gaudio E, Bonetti P, et al. The BET bromodomain inhibitor OTX015 affects pathogenetic pathways in preclinical B‐cell tumor models and synergizes with targeted drugs. Clin Cancer Res. 2015;21(7):1628–1638.
Brown JR, Hillmen P, O'Brien S, et al. Extended follow‐up and impact of high‐risk prognostic factors from the phase 3 RESONATE study in patients with previously treated CLL/SLL. Leukemia. 2018;32(1):83–91.
Burger JA, Tedeschi A, Barr PM, et al; RESONATE‐2 Investigators. Ibrutinib as initial therapy for patients with chronic lymphocytic leukemia. N Engl J Med. 2015;373(25):2425–2437.
Burger JA, Sivina M, Ferrajoli A, et al. Randomized trial of ibrutinib versus ibrutinib plus rituximab (Ib + R) in patients with chronic lymphocytic leukemia (CLL). Abstract 427. Presented at: American Society of Hematology Annual Meeting and Exposition; December 9–12, 2017; Atlanta, Georgia.
Byrd JC, Furman RR, Coutre SE, et al. Targeting BTK with ibrutinib in relapsed chronic lymphocytic leukemia. N Engl J Med. 2013;369(1):32–42.Byrd JC, Brown JR, O'Brien S, et al; RESONATE Investigators. Ibrutinib versus ofatumumab in previously treated chronic lymphoid leukemia. N Engl J Med. 2014;371(3):213–223.
ReferencesByrd JC, Furman RR, Coutre SE, et al. Three‐year follow‐up of treatment‐naïve and previously treated patients with CLL and SLL receiving single‐agent ibrutinib. Blood. 2015;125(16):2497–2506.
Byrd JC, Harrington B, O’Brien S, et al. Acalabrutinib (ACP‐196) in relapsed chronic lymphocytic leukemia. N Engl J Med. 2016;374(4):323–332.Chanan‐Khan A, Cramer P, Demirkan F, et al. Ibrutinib combined with bendamustine and rituximab compared with placebo, bendamustine, and rituximab for previously treated chronic lymphocytic leukaemia or small lymphocytic lymphoma (HELIOS): a randomised, double‐blind, phase 3 study. Lancet Oncol. 2016;17(2):200–211.
Chiron D, Di Liberto M, Martin P, et al. Cell‐cycle reprogramming for PI3K inhibition overrides a relapse‐specific C481S BTK mutation revealed by longitudinal functional genomics in mantle cell lymphoma. Cancer Discov. 2014;4(9):1022–1035.
Choi MY, Kipps TJ. Inhibitors of B‐cell receptor signaling for patients with B‐cell malignancies. Cancer J. 2012;18:404‐410.Clinicaltrials.gov. U.S. National Institutes of Health website. https://clinicaltrials.gov. Accessed May 2018. Coutré SE, Furman RR, Flinn IW, et al. Extended treatment with single‐agent ibrutinib at the 420 mg dose leads to durable responses in chronic lymphocytic leukemia/small lymphocytic lymphoma. Clin Cancer Res. 2017;23(5):1149–1155.
Da Roit F, Engelberts PJ, Taylor RP, et al. Ibrutinib interferes with the cell‐mediated anti‐tumor activities of therapeutic CD20 antibodies: implications for combination therapy. Haematologica. 2015;100(1):77–86.
Davids MS, Brown JR. Ibrutinib: a first in class covalent inhibitor of Bruton’s tyrosine kinase. Future Oncol. 2014;10(6):957‐967.Drug Development and Drug Interactions: Table of Substrates, Inhibitors and Inducers. U.S. Food and Drug Administration website. November 2017. https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DevelopmentResources/DrugInteractionsLabeling/ucm093664.htm. Accessed May 2018.
FDA Approved Drug: Acalabrutinib. U.S. Food and Drug Administration website. October 2017. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/210259s000lbl.pdf. Accessed May 2018.
FDA Approved Drug: Copanlisib. U.S. Food and Drug Administration website. September 2017. https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/209936s000lbl.pdf. Accessed May 2018.

Page 34
ReferencesFDA Approved Drug: Everolimus. U.S. Food and Drug Administration website. April 2018. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/022334s040,203985s013lbl.pdf. Accessed May 2018.
FDA Approved Drug: Fostamatinib. U.S. Food and Drug Administration website. April 2018. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/209299lbl.pdf. Accessed May 2018.
FDA Approved Drug: Ibrutinib. U.S. Food and Drug Administration website. February 2018. https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/205552Orig2lbl.pdf. Accessed May 2018.FDA Approved Drug: Idelalisib. U.S. Food and Drug Administration website. July 2014. https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/206545lbl.pdf. Accessed May 2018.
FDA Approved Drug: Temsirolimus. U.S. Food and Drug Administration website. March 2018. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/022088s021s023lbl.pdf. Accessed May 2018.
Fisher RI, Bernstein SH, Kahl BS, et al. Multicenter phase II study of bortezomib in patients with relapsed or refractory mantle cell lymphoma. J Clin Oncol. 2006;24(30):4867–4874.
Gonzalez D, Martinez P, Wade R, et al. Mutational status of the TP53 gene as a predictor of response and survival in patients with chronic lymphocytic leukemia: results from the LRF CLL4 trial. J Clin Oncol. 2011;29(16):2223‐2229.
Goy A, Sinha R, Williams ME, et al. Single‐agent lenalidomide in patients with mantle‐cell lymphoma who relapsed or progressed after or were refractory to bortezomib: phase II MCL‐001 (EMERGE) study. J Clin Oncol. 2013;31(29):3688–3695.
Greer JA, Amoyal N, Nisotel L, et al. A systematic review of adherence to oral antineoplastic therapies. Oncologist. 2016;21(3):354–376.Hernández JÁ, Hernández‐Sánchez M, Rodríguez‐Vicente AE, et al; Grupo Cooperativo Español de Citogenética Hematológica (GCECGH) and Grupo Español de Leucemia Linfática Crónica (GELLC). A low frequency of losses in 11q chromosome Is associated with better outcome and lower rate of genomic mutations in patients with chronic lymphocytic leukemia. PLoS One. 2015;10(11):e0143073.
Ilic N, Utermark T, Widlund HR, et al. PI3K‐targeted therapy can be evaded by gene amplification along the MYC‐eukaryotic translation initiation factor 4E (eIF4E) axis. Proc Natl Acad Sci USA. 2011;108(37):E699–E708.
ReferencesKrysiak K, Gomez F, White BS, et al. Recurrent somatic mutations affecting B‐cell receptor signaling pathway genes in follicular lymphoma. Blood. 2017;129(4):473–483.
Kuo HP, Ezell SA, Schweighofer KJ, et al. Combination of ibrutinib and ABT‐199 in diffuse large B‐cell lymphoma and follicular lymphoma. Mol Cancer Ther. 2017;16(7):1246–1256.
Leong DP, Caron F, Hillis C, et al. The risk of atrial fibrillation with ibrutinib use: a systematic review and meta‐analysis. Blood. 2016;128(1):138–140. Lipsky AH, Farooqui MZ, Tian X, et al. Incidence and risk factors of bleeding‐related adverse events in patients with chronic lymphocytic leukemia treated with ibrutinib. Haematologica. 2015;100(12):1571–1578.
Martin P, Maddocks K, Leonard JP, et al. Postibrutinib outcomes in patients with mantle cell lymphoma. Blood. 2016;127(12):1559–1563.Mato AR, Islam P, Daniel C, et al. Ibrutinib‐induced pneumonitis in patients with chronic lymphocytic leukemia. Blood. 2016;127(8):1064–1067.McMullen JR, Boey EJ, Ooi JY, et al. Ibrutinib increases the risk of atrial fibrillation, potentially through inhibition of cardiac PI3K‐Akt signaling. Blood. 2014;124(25):3829–3830. Morschhauser F, Danilov AV, Hodson DJ, et al. Preliminary results of a phase Ib study of tirabrutinib (GS‐4059/ONO‐4059) in combination with entospletinib in patients with B‐cell malignancies. Abstract 276. Presented at: International Conference on Malignant Lymphoma; June 14–17, 2017; Lugano, Switzerland.
Murray MY, Zatseva L, Auger MJ, et al. Ibrutinib inhibits BTK‐drive NF‐κB p65 activity to overcome bortezomib‐resistance in multiple myeloma. Cell Cycle. 2015;14(14):2367‐2375.
NCCN Practice Guidelines. Antiemesis, v2. 2018. April 30, 2018. National Comprehensive Cancer Network website. https://www.nccn.org/professionals/physician_gls/pdf/antiemesis.pdf. Accessed May 2018.
NCCN Clinical Practice Guidelines. Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma, v5.2018. March 26, 2018. NationalComprehensive Cancer Network website. https://www.nccn.org/professionals/physician_gls/pdf/cll.pdf. Accessed May 2018.NCCN Clinical Practice Guidelines. Prevention and Treatment of Cancer‐related Infections, v1.2018. December 1, 2017. https://www.nccn.org/professionals/physician_gls/pdf/infections.pdf. Accessed May 2018.

Page 35
ReferencesO'Brien S, Furman RR, Coutre S, et al. Single‐agent ibrutinib in treatment‐naïve and relapsed/refractory chronic lymphocytic leukemia: a 5‐year experience. Blood. 2018;131(17):1910‐1919.
O'Brien S, Jones JA, Coutre SE, et al. Ibrutinib for patients with relapsed or refractory chronic lymphocytic leukaemia with 17p deletion (RESONATE‐17): a phase 2, open‐label, multicentre study. Lancet Oncol. 2016;17(10):1409–1418.
ONS Oral Adherence Toolkit. The Oncology Nursing Society website. https://www.ons.org/practice‐resources/toolkits/oral‐adherence.Accessed May 2018.
Rossi D, Cerri M, Deambrogi C, et al. The prognostic value of TP53 mutations in chronic lymphocytic leukemia is independent of del17p13: implications for overall survival and chemorefractoriness. Clin Cancer Res. 2009;15(3):995‐1004.
Rye C, Wise R, Jurukovski V, et al. Biology. Houston, Texas: OpenStax; 2017.Shrner T. Making Treatment Decisions Together. February 2, 2016. ONS Voice website. http://connect.ons.org/issue/february‐2016/up‐front/making‐treatment‐decisions‐together. Accessed May 2018.
Stacey D, Légaré F, Lewis K, et al. Decision aids for people facing health treatment or screening decisions. Cochrane Database Syst Rev. 2017;4:CD001431.
Stilgenbauer S, Zenz T, Winkler D, et al. Subcutaneous alemtuzumab in fludarabine‐refractory chronic lymphocyctic leukemia: clinical results and prognostic marker analyses from the CLL2H study of the German Chronic Lymphocytic Leukemia Study Group. J Clin Oncol. 2009;27:3994–4001.
Tam CS, Anderson MA, Pott C, et al. Ibrutinib plus venetoclax for the treatment of mantle‐cell lymphoma. N Engl J Med. 2018;378(13):1211–1223.
Tam CS, Simpson D, Opat S, et al. Safety and activity of the highly specific BTK inhibitor BGB‐3111 in patients with indolent and aggressive non‐Hodgkin’s lymphoma. Abstract 152. Presented at: American Society of Hematology Annual Meeting; December 9–12, 2017; Atlanta, Georgia.
Walter HS, Jayne S, Rule SA, et al. Long‐term follow‐up of patients with CLL treated with the selective Bruton's tyrosine kinase inhibitor ONO/GS‐4059. Blood. 2017;129(20):2808–2810.
ReferencesWang ML, Rule S, Martin P, et al. Targeting BTK with ibrutinib in relapsed or refractory mantle‐cell lymphoma. N Engl J Med. 2013;369(6):507–516.
Wang ML, Rule S, Zinzani PL, et al. Acalabrutinib in relapsed or refractory mantle cell lymphoma (ACE‐LY‐004): a single‐arm, multicentre, phase 2 trial. Lancet. 2018;391(10121):659–667.
Whelton PK, Carey RM, AronowWS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of The American College of Cardiology/American Heart Association Task Force on clinical practice guidelines. J Am Coll Cardiol. 2017. [Epub ahead of print]
Woyach JA, Furman RR, Liu TM, et al. Resistance mechanisms for the Bruton's tyrosine kinase inhibitor, ibrutinib. N Engl J Med. 2014;370(24):2286–2294.
Xu L, Tsakmaklis N, Yang G, et al. Acquired mutations associated with ibrutinib resistance in waldenstrom macroglobulinemia. Blood. 2017;129(18):2519–2525.
Yue C, Niu M, Shan QQ, et al. High expression of Bruton's tyrosine kinase (BTK) is required for EGFR‐induced NF‐κB activation and predicts poor prognosis in human glioma. J Exp Clin Cancer Res. 2017;36(1):132.
Zainuddin N, Murray F, Kanduri M, et al. TP53 Mutations are infrequent in newly diagnosed chronic lymphocytic leukemia. Leuk Res. 2011;35(2):272–274.
Zenz T, Häbe S, Denzel T, et al. Detailed analysis of p53 pathway defects in fludarabine‐refractory chronic lymphocytic leukemia (CLL): dissecting the contribution of 17p deletion, TP53 mutation, p53‐p21 dysfunction, and miR34a in a prospective clinical trial. Blood. 2009;114(13):2589–2597.
Zenz T, Eichhorst B, Busch R, et al. TP53 mutation and survival in chronic lymphocytic leukemia. J Clin Oncol. 2010;28(29):4473–4479.

Page 36
Abbreviations• AAPA=American Academy of Physician
Assistants
• ABC=Association of Black Cardiologists
• ACC=American College of Cardiology
• ACPM=American College of Preventive
Medicine
• ADCC=antibody‐dependent cell‐mediated
cytotoxicity
• AE=adverse event
• Afib=atrial fibrillation
• AGS=American Geriatrics Society
• AHA=American Heart Association
• AHRQ=Agency for Healthcare Research and
Quality
• ALC=absolute lymphocyte count
• APhA=American Pharmacists Association
• APP=advanced practice provider
• ASH=American Society of Hypertension
• ASPC=American Society for Preventive
Cardiology
• ATP=adenosine triphosphate
• BCL=B‐cell lymphoma
• BCR=B‐cell receptor
• BET=bromodomain and extraterminal motif
• BTK=Bruton’s tyrosine kinase
• BTKi=Bruton’s tyrosine kinase inhibitor
• CARD11=caspase recruitment domain‐
containing protein 1
• CDK=cyclin‐dependent kinase
Abbreviations• cGVHD=chronic graft versus host disease
• CLL=chronic lymphocytic leukemia
• CR=complete response
• CRi=complete remission with incomplete
hematologic recovery
• ECG=electrocardiogram
• EGFR=epidermal growth factor receptor
• FCR=fludarabine, cyclophosphamide,
rituximab
• Hbg=hemoglobin
• HCP=healthcare provider
• HSV=herpes simplex virus
• HTN=hypertension
• Ig=immunogloblin
• ITK=interleukin‐2–inducible T‐cell kinase
• IV=intravenous
• IVIG=intravenous immunoglobulin
• mAb=monoclonal antibody
• MCL=mantle cell lymphoma
• MZL=marginal zone lymphoma
• NCCN=National Comprehensive Cancer
Network
• NHL=non‐Hodgkin lymphoma
• NK=natural killer (cells)
• NMA=National Medical Association
• N/V=nausea and vomiting
• OBZ=obinutuzumab
• OFA=ofatumumab

Page 37
Abbreviations• OR=overall response
• ORR=objective response rate
• OS=overall survival
• PBMC=peripheral blood mononuclear cells
• PCNA=Preventative Cardiovascular Nurses
Association
• PCP=Pneumocystis pneumonia
• PD=progressive disease
• PFS=progression‐free survival
• PI3K=phosphoinositide 3‐kinase
• PLCγ2=phospholipase C gamma 2
• PO=by mouth
• PR=partial response
• PR + L=partial response with lymphocytosis
• SD=stable disease
• SDM=shared decision making
• SLL=small lymphocytic leukemia
• SMX=sulfamethoxazole
• SYK=spleen tyrosine kinase
• TEAE=treatment‐emergent adverse event
• TEC=tyrosine kinase expressed in
hepatocellular carcinoma
• TMP=trimethoprim
• TRZ=trastuzumab
• UA=urinalysis
• WBC=white blood cell
• WM=Waldenstrommacroglobulinemia
Notes
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________
_________________________________________





























