Embed Size (px)
Citation preview

One-Hour Power Break webinar - Rather wreck my gums than my lungs: Smokeless tobacco and California rural adolescent males
Benjamin Chaffee, DDS, MPH, PhD
8/30/17

Moderator
Catherine Saucedo
Deputy Director Smoking Cessation Leadership Center University of California, San Francisco [email protected]
8/30/17 Smoking Cessation Leadership Center

Disclosures This UCSF CME activity was planned and developed to uphold academic standards to ensure balance, independence, objectivity, and scientific rigor; adhere to requirements to protect health information under the Health Insurance Portability and Accountability Act of 1996 (HIPAA); and include a mechanism to inform learners when unapproved or unlabeled uses of therapeutic products or agents are discussed or referenced. The following faculty speakers, moderators, and planning committee members have disclosed they have no financial interest/arrangement or affiliation with any commercial companies who have provided products or services relating to their presentation(s) or commercial support for this continuing medical education activity: Benjamin Chaffee, DDS, MPH, PhD, Christine Cheng, Brian Clark, Jennifer Matekuare, Roxana Said, MPH, Catherine Saucedo, and Steven A. Schroeder, MD
8/30/17 Smoking Cessation Leadership Center

Thank you to our funders
8/30/17 Smoking Cessation Leadership Center

Housekeeping
• All participants will be in listen only mode.
• Please make sure your speakers are on and adjust the volume accordingly.
• If you do not have speakers, please request the dial-in via the chat box.
• This webinar is being recorded and will be available on SCLC’s website, along with the slides.
• Use the chat box to send questions at any time for the presenters.
8/30/17 Smoking Cessation Leadership Center

CME/CEU Statement Accreditation:
The University of California, San Francisco (UCSF) School of Medicine is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
UCSF designates this live activity for a maximum of 1.0 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the webinar activity.
Advance Practice Registered Nurses and Registered Nurses: For the purpose of recertification, the American Nurses Credentialing Center accepts AMA PRA Category 1 CreditTM issued by organizations accredited by the ACCME.
Physician Assistants: The National Commission on Certification of Physician Assistants (NCCPA) states that the AMA PRA Category 1 CreditTM are acceptable for continuing medical education requirements for recertification.
California Pharmacists: The California Board of Pharmacy accepts as continuing professional education those courses that meet the standard of relevance to pharmacy practice and have been approved for AMA PRA category 1 creditTM. If you are a pharmacist in another state, you should check with your state board for approval of this credit.
Respiratory Therapists: This program has been approved for a maximum of 1.0 contact hour Continuing Respiratory Care Education (CRCE) credit by the American Association for Respiratory Care, 9425 N. MacArthur Blvd. Suite 100 Irving TX 75063, Course # 149246000.
8/30/17 Smoking Cessation Leadership Center

Presenter
Benjamin Chaffee, DDS, MPH, PhD Assistant Professor Division of Oral Epidemiology and Dental Public Health University of California San Francisco
8/30/17 Smoking Cessation Leadership Center

Rather Wreck My Gums Than My Lungs: Smokeless Tobacco and California Rural Adolescent Males
Benjamin Chaffee, DDS MPH PhD UCSF School of Dentistry Division of Oral Epidemiology & Dental Public Health UCSF Center for Tobacco Control Research & Education

9
Acknowledgments
UCSF TCORS Project 3 UCSF TCORS & CTCRE
Funding:
NIH NCI/FDA P50CA180890 NIH NCATS KL2TR001870
Content solely the responsibility of authors and does not necessarily represent the official views of funding organizations
Neal Benowitz Victoria Campbell Taranvir Cheema Jing Cheng Elizabeth Couch Ellen Darius Gwen Essex Stuart Gansky Joanna Hill Catherine Kavanagh Janna Murray Archnaa Rajasekaran Janelle Urata Margaret Walsh
Janine Cataldo Stanton Glantz Bonnie Halpern-Felsher Jonathan Leff Pamela Ling Maria Roditis Karen Williams ...and entire TCORS team

10
Dr. Margaret (Peggy) Walsh
Dr. Walsh was a visionary leader in education and research

11
Smokeless Tobacco: Adverse Health Effects
Oral conditions Oral and pharyngeal cancer Mucosal lesions Gingival keratosis Periodontal disease Tooth discoloration Enamel erosion Gingival recession Dental caries
Other conditions Pancreatic cancer Stomach cancer Hypertension Cardiovascular Disease Smoking initiation among young users

12
Conventional Smokeless Tobacco (ST)
Oral moist snuff (“dip”) Finely ground tobacco Typically placed between buccal mucosa and gingiva and held in place
Chewing tobacco (“chew”) Coarsely shredded tobacco Sold in bricks, twists, or loose-leaf Placed in mouth and chewed

13
The Changing (Smokeless) Tobacco Landscape

14
The Changing (Smokeless) Tobacco Landscape
Acquisition of ST manufacturers by major cigarette companies

15
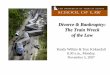
The Changing (Smokeless) Tobacco Landscape
ST Industry Marketing Expenditures Spike After Acquisition by Cigarette Makers
1985 1995 1990 2000 2010 2005
$100M
$400M
$300M
$200M
$500M
$600M
$700M
2015
Source: Federal Trade Commission
2006 - 2010: Altria & Reynolds Purchase Smokeless Companies

16
The Changing (Smokeless) Tobacco Landscape
Major growth in marketing expenditures on magazine ads & price discounts
Sources: Federal Trade Commission and http://www.tobaccofreekids.org/research/factsheets/pdf/0003.pdf
trinketsandtrash.org

17
The Changing (Smokeless) Tobacco Landscape
Greater diversity in ST product types and varieties
Options in price, flavor, cut & nicotine content may appeal to youth

18
The Changing (Smokeless) Tobacco Landscape
Rising popularity and normalization of other non-cigarette products (e.g. e-cigarettes, marijuana)

19
Adolescent Tobacco Use, United States (males, grade 9 -12)
Past Month Use, %
1999 ’01 ’03 ’05 ’07 ’09 ’11 ’13
Cigarettes
Source: Youth Risk Behavior Survey
2015

20
Source: Youth Risk Behavior Survey
Smokeless Tobacco
Past Month Use, %
1999 ’01 ’03 ’05 ’07 ’09 ’11 ’13
Cigarettes
2015
Adolescent Tobacco Use, United States (males, grade 9 -12)

21
Populations at risk of smokeless tobacco use
Male Young adult Non-Hispanic White Lower-income & education Rural
trinketsandtrash.org

22
Populations at risk of smokeless tobacco use
Male Young adult Non-Hispanic White Lower-income & education Rural
trinketsandtrash.org

23
(election map)
Map credit: Mark Newman http://www-personal.umich.edu/~mejn/election/2016/
United States 2016 Presidential Election: Voting by County

24
Why Study Smokeless Tobacco Use in California?

25
1.9 million Californians live in rural areas

26
California Counties: Population Density

27
California Counties: Population Density
California Counties: % ST Ever-Use
11th Grade
Data Source: California Healthy Kids Survey

28

Baseball teams at 36 rural California high schools (Recruited: 2014-2016)
Assess: • ST use patterns • Risk perceptions • Decision-making • Biological markers of nicotine
and carcinogen exposure
Smokeless Tobacco Use Among Rural High School Baseball Players in California
29

Smokeless Tobacco and Sports
Elevated ST use in baseball, hockey, football, rodeo, wrestling, auto racing
trinketsandtrash.org

Getty Images
Smokeless Tobacco and Sports
Elevated ST use in baseball, hockey, football, rodeo, wrestling, auto racing
Exceedingly high in organized baseball Modeled use by admired athletes during widely broadcast games Tobacco marketing infiltrates baseball culture and tradition

32
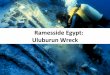
57%
37% 36% 31% 31%
22%
12%
Ever tried tobacco products (at least one time)
Any Tobacco
Dip/Chew E- Cigarettes
Cigars Hookah Cigarettes Snus
Rural California High School Males (N = 594)

33
Current (past month) tobacco use
Dip/Chew E-Cigarettes Cigars Hookah Cigarettes Snus
18%
9% 9% 8%
6%
4%
Rural California High School Males (N = 594)

34
Past month tobacco use & daily use
Dip/Chew E-Cigarettes Cigars Hookah Cigarettes Snus
Daily use 18%
9% 9% 8%
6%
4%
Rural California High School Males (N = 594)

No Combustible Use Combustible Use
14%
51%
Correlates of Past Month Smokeless Tobacco Use
Other Non-Hispanic White
13%
22%
< College Degree College Degree
16% 17%
9th 11th
9%
21%
10th 12th
13%
33% Race/Ethnicity
Parental Education
Grade in School
Other Tobacco Use

36
Correlates of Past Month Smokeless Tobacco Use
None ≥1 Family Member
13%
27%
Family Member ST Use Perceived Number of Teammates Who Use ST
None Few
4%
14%
Some Half Most
37% 36%
30%

Smokeless Tobacco in Major League Baseball

Officially banned in minor leagues (1993)
Cannot be carried in uniform (2012)
Some cities ban tobacco in ballparks (2015-2016)
New major leaguers cannot use in games (2017)
Smokeless Tobacco in Major League Baseball

Officially banned in minor leagues (1993)
Cannot be carried in uniform (2012)
Some cities ban tobacco in ballparks (2015-2016)
New major leaguers cannot use in games (2017)
Smokeless Tobacco in Major League Baseball
Momentum encouraging, but... Rules are patchwork and practically unenforceable

40 Ezra Shaw, Getty Images
2015 National League Most Valuable Player

41 Ezra Shaw, Getty Images
2015 National League Most Valuable Player

42
Do you think your favorite Major League Baseball player uses smokeless tobacco (dip or chew)?

43
Do you think your favorite Major League Baseball player uses smokeless tobacco (dip or chew)?
Definitely Yes
Probably Yes
Definitely No
Probably No

44
Do you think your favorite Major League Baseball player uses smokeless tobacco (dip or chew)?
Definitely Yes
Probably Yes
Definitely No
Probably No
Ever-tried ST: 25% Current ST: 8%

45
Do you think your favorite Major League Baseball player uses smokeless tobacco (dip or chew)?
Definitely Yes
Probably Yes
Definitely No
Probably No
Ever-tried ST: 38% Current ST: 18%
Ever-tried ST: 25% Current ST: 8%

46
Susceptibility to ST initiation High school baseball players (ST never-users)
Would Try ST if Best Friend Offered
10%
40%
30%
20%
Probably Yes
Definitely Yes
Probably Not
Definitely Not
Does Your Favorite MLB Player Use ST?
50%
Think You Will Use ST a Year from Now

47
Susceptibility to ST initiation High school baseball players (ST never-users)
Would Try ST if Best Friend Offered
10%
40%
30%
20%
Probably Yes
Definitely Yes
Probably Not
Definitely Not
Does Your Favorite MLB Player Use ST?
50%
Think You Will Use ST a Year from Now

48
Qualitative Study of Smokeless Tobacco Decision-Making

49
Qualitative Study of Smokeless Tobacco Decision-Making
Interviews with high school males (ST users and non-users)
Perceived acceptability, health risks, and social context of ST use

trinketsandtrash.org 50
• ST related to rural or country way of life
• Part of community tradition and culture
"Country" Culture

trinketsandtrash.org 51
• ST related to rural or country way of life
• Part of community tradition and culture
“The group I hang out with, like boots, blue jeans…they're like cowboys, like country kids – [ST] is really accepted. It's just like a thing that
happens. No one even takes a second look at it.” (current-user, age 17)
"Country" Culture

52
Never-users: Strong anti-tobacco expectations from parents motivated avoidance
Family Influences

53
ST Users: Modeling by family members reinforced acceptance
Never-users: Strong anti-tobacco expectations from parents motivated avoidance
Family Influences

54
ST Users: Modeling by family members reinforced acceptance
“[My parents] think [ST is] gross, but they also think that I'm old enough to make my own decisions.”
(current-user, age 17)
Never-users: Strong anti-tobacco expectations from parents motivated avoidance
ST Users: Parents superficially disapproving yet permissive or reluctantly accepting
Family Influences

55 trinketsandtrash.org
ST use a way to express newly earned independence
Chewing in light of health risks signaled reaching an age that required less protection from potential dangers
Maturity and Independent Choice

56 trinketsandtrash.org
ST use a way to express newly earned independence
“I'm doing it at my own risk, and it's something I decided to do.”
(current-user, age 18)
Chewing in light of health risks signaled reaching an age that required less protection from potential dangers
Maturity and Independent Choice

57
High awareness of oral health risks: mouth cancer, tooth loss, and gum disease
Perceived Health Risks

58
High awareness of oral health risks: mouth cancer, tooth loss, and gum disease
“Your teeth rot away. Makes your breath smell bad.
Makes your teeth turn different colors. Gums, you lose your
gums. Teeth start to fall out.” (experimenter, age 17)
Perceived Health Risks

59
Many users framed ST as an alternative to cigarettes with greatly reduced risk of systemic disease
“Cigarettes, it goes into your body and through your lungs and into everything like that... chewing
tobacco just stays in my mouth.”
(current-user, age 16)
“Cigarettes, you have lung damage. Makes your skin all wrinkly. Chew, just your gums and teeth.
Your lungs are fine still.”
Risks Relative to Cigarettes

60
Many users viewed health risks as distant and avoidable
“I haven't had any health problems with [ST] since I have been chewing… I know that if I did
have a health problem, that would probably motivate me to quit.”
(current-user, age 16)
Exceptionalism and Avoidable Risk
Risk mitigation strategies: Stay below a threshold of intensity or duration, practice good oral hygiene, not swallow tobacco juices

Smokeless Tobacco and Carcinogens
Tobacco-Specific Nitrosamines (TSNAs):
NNN - oral cancer
NNK - lung and pancreatic cancer

Smokeless Tobacco and Carcinogens
Tobacco-Specific Nitrosamines (TSNAs):
NNN - oral cancer
NNK - lung and pancreatic cancer
Swedish snus is a pasteurized, low-nitrosamine moist snuff smokeless tobacco Standards set the maximum allowable level of TSNAs

Smokeless Tobacco and Carcinogens
Tobacco-Specific Nitrosamines (TSNAs):
NNN - oral cancer
NNK - lung and pancreatic cancer
Smokeless tobacco products sold in the United States, including snus products, contain much higher TSNA levels Stepanov, et al. (2014) Nicotine Tob Res

Smokeless Tobacco and Carcinogens
Tobacco-Specific Nitrosamines (TSNAs):
NNN - oral cancer
NNK - lung and pancreatic cancer
Similar (or higher) levels of NNAL (urinary marker of NNK) in adult smokeless users vs. cigarette smokers Hecht, et al. (2007) Cancer Epidemiol Biomakers
Adult Smokers
Adult ST User

65
FDA estimates: 12,700 cases of oral cancer prevented 2,200 oral cancer deaths prevented in 20 years after implementation

66
FDA estimates: 12,700 cases of oral cancer prevented 2,200 oral cancer deaths prevented in 20 years after implementation

67
Quantifying Tobacco Risk Perceptions
creative commons image

68
In your opinion, how harmful is using dip or chew to general health?
Quantifying Tobacco Risk Perceptions

69
In your opinion, how harmful is using dip or chew to general health?
Quantifying Tobacco Risk Perceptions
Use this scale from 0 to 100
to demonstrate 100 = extremely harmful
0 = not at all harmful

70
In your opinion, how harmful is using dip or chew to general health?
Quantifying Tobacco Risk Perceptions
Use this scale from 0 to 100
to demonstrate 100 = extremely harmful
0 = not at all harmful

71
In your opinion, how harmful is using dip or chew to general health?
Quantifying Tobacco Risk Perceptions
Use this scale from 0 to 100
to demonstrate 100 = extremely harmful
0 = not at all harmful

72
In your opinion, how harmful is using dip or chew to general health?
Quantifying Tobacco Risk Perceptions
Use this scale from 0 to 100
to demonstrate 100 = extremely harmful
0 = not at all harmful

73
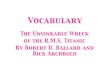
Cigarettes E-Cigarettes Dip/Chew Cigars Hookah
standardized for age, race/ethnicity, parental education, and intra-school clustering
90
74 74
61 57
Perceived Harm Differs by Tobacco Product
100 = extremely harmful
0 = not at all harmful

74
Cigarettes E-Cigarettes Dip/Chew Cigars Hookah
standardized for age, race/ethnicity, parental education, and intra-school clustering
Never
Tried/Former
Current
Product Use:
Never
Tried/Former
Current
Product Use (ST):
Perceived Harm Differs by Tobacco Product & Use Status

75
Cigarettes E-Cigarettes Dip/Chew Cigars Hookah
standardized for age, race/ethnicity, parental education, and intra-school clustering
Never
Tried/Former
Current
Product Use:
Never
Tried/Former
Current
Product Use (ST):
Perceived Harm Differs by Tobacco Product & Use Status

76
Cigarettes E-Cigarettes Dip/Chew Cigars Hookah
standardized for age, race/ethnicity, parental education, and intra-school clustering
Never
Tried/Former
Current
Product Use:
Never
Tried/Former
Current
Product Use (ST):
Perceived Harm Differs by Tobacco Product & Use Status

77
Cigarettes E-Cigarettes Dip/Chew Cigars Hookah
standardized for age, race/ethnicity, parental education, and intra-school clustering
Never
Tried/Former
Current
Product Use:
Never
Tried/Former
Current
Product Use (ST):
Perceived Harm Differs by Tobacco Product & Use Status

78
Smokeless Tobacco Use
Cigarettes
E-Cigarettes
Perceived ST Harm Declines with Use Frequency
Never Tried/Former 1-9 days/mo. >9 days/mo. Everyday
Smokeless Tobacco

79
Smokeless Tobacco Use
Cigarettes
E-Cigarettes
Perceived ST Harm Declines with Use Frequency
Never Tried/Former 1-9 days/mo. >9 days/mo. Everyday
Smokeless Tobacco

80
Smokeless Tobacco Use
Cigarettes
E-Cigarettes
Perceived ST Harm Declines with Use Frequency
Never Tried/Former 1-9 days/mo. >9 days/mo. Everyday
Smokeless Tobacco

81
Quantifying Specific Tobacco Risk Perceptions
Imagine you used dip/chew. How likely will happen to you?

82
Quantifying Specific Tobacco Risk Perceptions
Use this scale from 0% to 100% to demonstrate
Imagine you used dip/chew. How likely will happen to you?
Get into Trouble
Brown Teeth
Mouth Cancer

83
Quantifying Specific Tobacco Risk Perceptions
mouth cancer 78
59
ST never-user
68
40
How likely will happen to you?

84
Quantifying Specific Tobacco Risk Perceptions
mouth cancer 78
59
ST never-user
ST ever-user
68
40
How likely will happen to you?
How do users and non-users perceive each individual risk?

85
Quantifying Specific Tobacco Risk Perceptions
mouth cancer 78
59
ST never-user
ST ever-user
68
40
How likely will happen to you?
How do users and non-users perceive each individual risk?
Are different types of risks perceived in the same way?

86
Quantifying Specific Tobacco Risk Perceptions
mouth cancer 78
59
ST never-user
ST ever-user
68
40
How likely will happen to you?
How do users and non-users perceive each individual risk?
Are different types of risks perceived in the same way?
How are different types of risks perceived across tobacco products?

87
Smokeless Tobacco Risk Perceptions: Two Classes
“UNCERTAIN RISKS” “BELIEVABLE RISKS”
Mouth cancer Upset family Bad breath
Heart attack Lung cancer Harm someone nearby
How likely will happen to you?

88
Smokeless Tobacco Risk Perceptions: Two Classes
“UNCERTAIN RISKS” “BELIEVABLE RISKS”
Mouth cancer Upset family Bad breath
Heart attack Lung cancer Harm someone nearby
How likely will happen to you?

“UNCERTAIN RISKS” “BELIEVABLE RISKS” 89
Smokeless Tobacco Risk Perceptions: Two Classes
ST never-user
ST ever-user How likely will happen to you?
Heart attack Lung cancer Harm someone nearby
Mouth cancer Upset family Bad breath

“UNCERTAIN RISKS” “BELIEVABLE RISKS” 90
Smokeless Tobacco Risk Perceptions: Two Classes
ST never-user
ST ever-user How likely will happen to you?
Heart attack Lung cancer Harm someone nearby
Mouth cancer Upset family Bad breath

“UNCERTAIN RISKS” “BELIEVABLE RISKS” 91
Smokeless Tobacco Risk Perceptions: Two Classes
How likely will happen to you?
Heart attack Lung cancer Harm someone nearby
Mouth cancer Upset family Bad breath
Ciga
rett
es
Smok
eles
s
Ciga
rett
es
Smok
eles
s

92
Available nicotine & carcinogen content
Form, brand, flavors, price
Positioning of specific products to appeal to novice users
Variation in Smokeless Tobacco Products

93
Flavored ST associated with appealing non-tobacco products: chewing gum, breath mints, fruit, candy, and alcohol
Flavor Associations
trinketsandtrash.org trinketsandtrash.org

94
Flavor Associations
Others had negative perceptions of ST flavors, viewing them as unnatural in comparison to “regular” or “straight” ST
trinketsandtrash.org

95
Flavor Associations
Others had negative perceptions of ST flavors, viewing them as unnatural in comparison to “regular” or “straight” ST
trinketsandtrash.org
“Flavored [ST]... makes me feel like it's not real….The stuff that I used the most when I was on it a lot was straight, because in
my mind it was just straight tobacco. It didn't have all this
other stuff in it.” (former-user, age 16)

96
Users sampled brands, flavors out of curiosity or to “switch things up” Special or seasonal offers generated buzz and created urgency to purchase. Some followed ST websites to track new products
Product Switching & Special Offers
trinketsandtrash.org

97
Users perceived higher “strength” and nicotine content based on brand, type, or flavor
Perceived Product Qualities

98
Users perceived higher “strength” and nicotine content based on brand, type, or flavor
“Copenhagen Wintergreen will give you a real big head rush. It will make you feel different than
Copenhagen Straight.” (former-user, age 16)
Perceived Product Qualities

99
Social pressure was associated with using certain ST products, partly based on perceived product strength (and user toughness)
Perceived Brand Qualities

100
Social pressure was associated with using certain ST products, partly based on perceived product strength (and user toughness)
Perceived Brand Qualities
“They say if you chew Skoal, you're a little girl.” (current-user, age 17)

101
Many users also expressed loyalty when discussing their usual brand
“I think Copenhagen just doesn't need to advertise really. They're just like Marlboro is for cigarettes... Like Nike is for shoes. They're just
like the top of the top.” (current-user, age 17)
Perceived Brand Qualities

102

103

Smokeless tobacco is a sizeable, persistent public health problem; even in California
Implications Don’t overlook rural communities in policy & research

Smokeless tobacco is a sizeable, persistent public health problem; even in California
Aggressive, highly effective industry marketing targets young rural males
Implications Don’t overlook rural communities in policy & research
Forceful public health action needed as industry seeks profits beyond smoking

Smokeless tobacco is a sizeable, persistent public health problem; even in California
Aggressive, highly effective industry marketing targets young rural males
Implications
Perceived community norms and use by others puts youth at risk
Don’t overlook rural communities in policy & research
Forceful public health action needed as industry seeks profits beyond smoking
Go beyond half-measures: full ban with enforcement in professional baseball

Smokeless tobacco is a sizeable, persistent public health problem; even in California
Awareness of oral health risks, but these risks dismissed & related to smoked tobacco
Aggressive, highly effective industry marketing targets young rural males
Implications
Perceived community norms and use by others puts youth at risk
Don’t overlook rural communities in policy & research
Forceful public health action needed as industry seeks profits beyond smoking
Go beyond half-measures: full ban with enforcement in professional baseball
“Wrecks your gums” cannot be only message: emphasize addiction, chemicals

NNN limit Eliminate flavors Restrict ads in youth-oriented magazines Sever connection with sports
Smokeless tobacco is a sizeable, persistent public health problem; even in California
Awareness of oral health risks, but these risks dismissed & related to smoked tobacco
Aggressive, highly effective industry marketing targets young rural males
Relative harm beliefs associated with youth ST use To achieve harm reduction: make a less harmful product with less youth appeal
Implications
Perceived community norms and use by others puts youth at risk
Don’t overlook rural communities in policy & research
Forceful public health action needed as industry seeks profits beyond smoking
Go beyond half-measures: full ban with enforcement in professional baseball
“Wrecks your gums” cannot be only message: emphasize addiction, chemicals

Smokeless tobacco is a sizeable, persistent public health problem; even in California
Awareness of oral health risks, but these risks dismissed & related to smoked tobacco
Aggressive, highly effective industry marketing targets young rural males
Relative harm beliefs associated with youth ST use To achieve harm reduction: make a less harmful product with less youth appeal
Implications
Perceived community norms and use by others puts youth at risk
Today, nearly 1,000 males below age-18 will use ST for the first time
Don’t overlook rural communities in policy & research
Forceful public health action needed as industry seeks profits beyond smoking
Go beyond half-measures: full ban with enforcement in professional baseball
“Wrecks your gums” cannot be only message: emphasize addiction, chemicals
NNN limit Eliminate flavors Restrict ads in youth-oriented magazines Sever connection with sports

110

Q&A
• Submit questions via the chat box
8/30/17 Smoking Cessation Leadership Center

Contact us for technical assistance
• You will receive the webinar recording, presentation slides, information on certificates of attendance, and other resources, in our follow-up email. All of this information will be posted to our website.
• CME/CEUs of up to 1.0 credit is available to all attendees of this live session. Instructions will be emailed after the webinar.
• Visit us online at smokingcessationleadership.ucsf.edu
• Call us toll-free at 877-509-3786
• Please complete the post-webinar survey
8/30/17 Smoking Cessation Leadership Center

CME/CEU Statement Accreditation:
The University of California, San Francisco (UCSF) School of Medicine is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians.
UCSF designates this live activity for a maximum of 1.0 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the webinar activity.
Advance Practice Registered Nurses and Registered Nurses: For the purpose of recertification, the American Nurses Credentialing Center accepts AMA PRA Category 1 CreditTM issued by organizations accredited by the ACCME.
Physician Assistants: The National Commission on Certification of Physician Assistants (NCCPA) states that the AMA PRA Category 1 CreditTM are acceptable for continuing medical education requirements for recertification.
California Pharmacists: The California Board of Pharmacy accepts as continuing professional education those courses that meet the standard of relevance to pharmacy practice and have been approved for AMA PRA category 1 creditTM. If you are a pharmacist in another state, you should check with your state board for approval of this credit.
Respiratory Therapists: This program has been approved for a maximum of 1.0 contact hour Continuing Respiratory Care Education (CRCE) credit by the American Association for Respiratory Care, 9425 N. MacArthur Blvd. Suite 100 Irving TX 75063, Course # 149246000.
8/30/17 Smoking Cessation Leadership Center

American Association for Respiratory Care (AARC) • Free Continuing Respiratory Care Education credit (CRCEs) are
available to Respiratory Therapists who attend this live webinar
• Instructions on how to claim credit will be included in our post-webinar email
8/30/17 Smoking Cessation Leadership Center

Save the Date
SCLC’s next One-Hour Power Break webinar : “The Power of Partnerships: Behavioral health and public health working together to combat smoking in Kentucky”
with the National Behavioral Health Network for Tobacco & Cancer Control and the American Lung Association and the State of Kentucky
Tuesday, September 19, 2017 at 1pm EDT
Registration is open now!
8/30/17 Smoking Cessation Leadership Center

Contact us for technical assistance
• Visit us online at smokingcessationleadership.ucsf.edu
• Call us toll-free at 877-509-3786
• Please complete the post-webinar survey
8/30/17 Smoking Cessation Leadership Center