Embed Size (px)
Citation preview
Oncology Compass: Renal Cell Carcinoma
tivozanib
Navigation Hints:• Explore the current standard of care by selecting Line of Therapy - Key clinical trials are organized on a timeline to reflect changes in regulatory and clinical standards over time
• Review key competitive agents by selecting Mechanism of Action - Each competitor profile includes key preclinical and clinical data - Detailed summaries of ongoing trials include milestone estimates and impact analyses
• Emerging data on optimal sequence of targeted therapy can be viewed by selecting Sequencing MOAs• Review impact of risk stratification and histology on the RCC treatment paradigm by selecting Patient Subsets• (Click on the word Glossary here to view a list of defined terms)
Mec
hani
sm
of Action Line of Therapy
Sequencing MOAs
Click in upper right-hand corner to return to this overview page
P
atient Sub
sets
Oncology Compass: Renal Cell Carcinoma
MOA:
Immune Modulation
CytotoxicT cellCytotoxic
T cell
PD1
Antigenpresenting
cell
RCC Cell
Apoptosis
Necrosis
tumor antigen
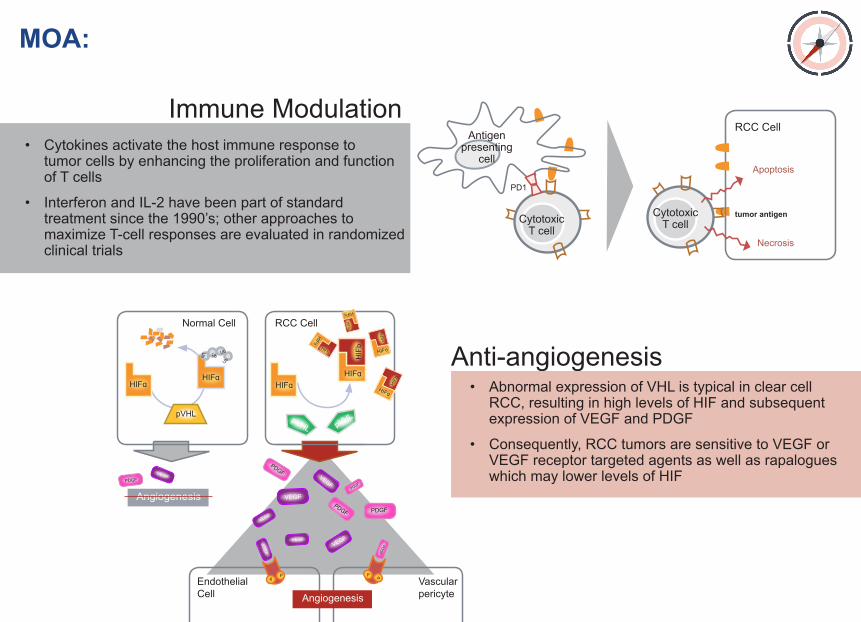
• Cytokines activate the host immune response to tumor cells by enhancing the proliferation and function of T cells
• Interferon and IL-2 have been part of standard treatment since the 1990’s; other approaches to maximize T-cell responses are evaluated in randomized clinical trials
Anti-angiogenesis• Abnormal expression of VHL is typical in clear cell RCC, resulting in high levels of HIF and subsequent expression of VEGF and PDGF
• Consequently, RCC tumors are sensitive to VEGF or VEGF receptor targeted agents as well as rapalogues which may lower levels of HIF
Ub Ub
Ub
Ub
Normal Cell
Endothelial Cell
RCC Cell
Vascular pericyteAngiogenesis
PP P P
Angiogenesis
HIFɑHIFɑ
HIFɑHIFɑ
HIFɑ
HIFɑ
HIFɑ
HIFɑ
pVHL pVHL
HIF
bHIFb
HIFb
HIF
b
HIFb
pVHL
PDGFVEGF
VEGF
VEGF
VEG
F VEGF
VEGF
VEGF
PDGFPDGF
PDGFPDG
F
PDGF
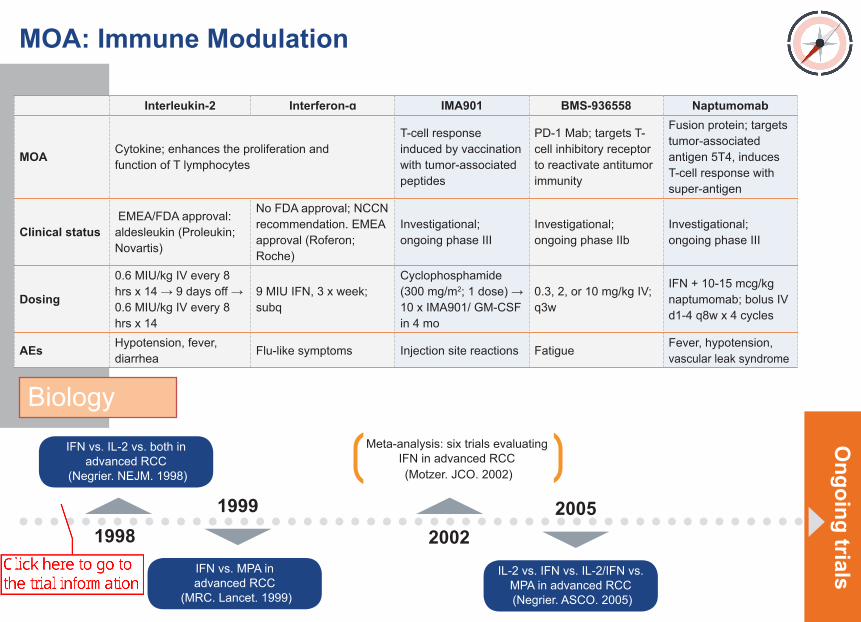
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
MOA: Immune Modulation
Interleukin-2 Interferon-ɑ IMA901 BMS-936558 Naptumomab
MOA Cytokine; enhances the proliferation and function of T lymphocytes
T-cell response induced by vaccination with tumor-associated peptides
PD-1 Mab; targets T-cell inhibitory receptor to reactivate antitumor immunity
Fusion protein; targets tumor-associated antigen 5T4, induces T-cell response with super-antigen
Clinical status EMEA/FDA approval: aldesleukin (Proleukin; Novartis)
No FDA approval; NCCN recommendation. EMEA approval (Roferon; Roche)
Investigational; ongoing phase III
Investigational; ongoing phase IIb
Investigational; ongoing phase III
Dosing
0.6 MIU/kg IV every 8 hrs x 14 → 9 days off → 0.6 MIU/kg IV every 8 hrs x 14
9 MIU IFN, 3 x week; subq
Cyclophosphamide (300 mg/m2; 1 dose) → 10 x IMA901/ GM-CSF in 4 mo
0.3, 2, or 10 mg/kg IV; q3w
IFN + 10-15 mcg/kg naptumomab; bolus IV d1-4 q8w x 4 cycles
AEs Hypotension, fever, diarrhea
Flu-like symptoms Injection site reactions FatigueFever, hypotension, vascular leak syndrome
Biology
Ongoing trials
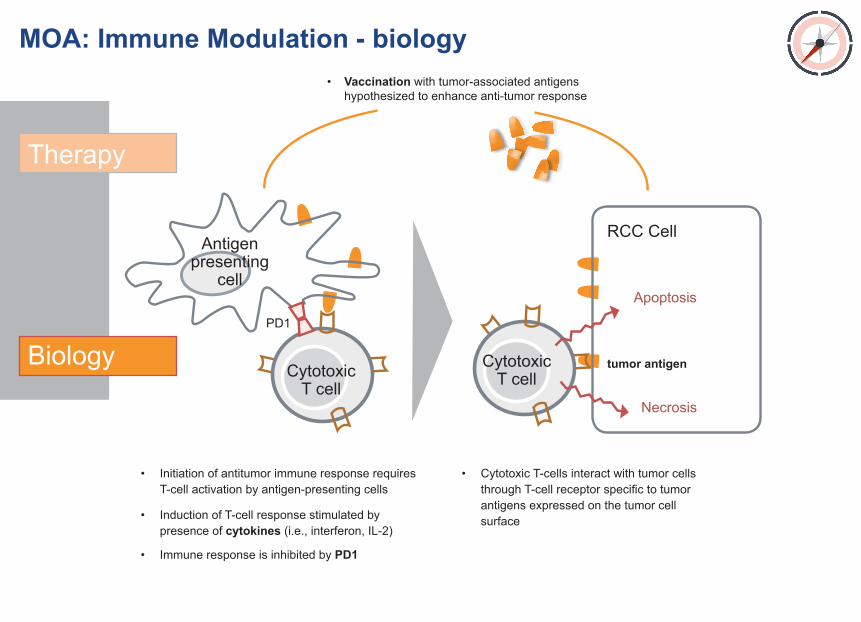
MOA: Immune Modulation - biology
• Initiation of antitumor immune response requires T-cell activation by antigen-presenting cells
• Induction of T-cell response stimulated by presence of cytokines (i.e., interferon, IL-2)
• Immune response is inhibited by PD1
• Cytotoxic T-cells interact with tumor cells through T-cell receptor specific to tumor antigens expressed on the tumor cell surface
CytotoxicT cellCytotoxic
T cell
PD1
• Vaccination with tumor-associated antigens hypothesized to enhance anti-tumor response
Antigenpresenting
cell
RCC Cell
Apoptosis
Necrosis
tumor antigen
Therapy
Biology
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
Ongoing trials
MOA: Immune Modulation
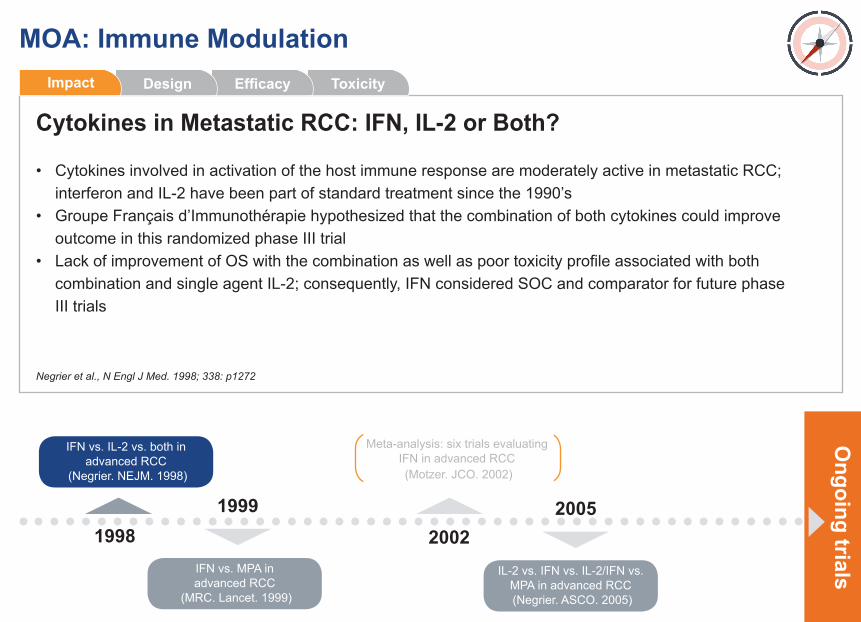
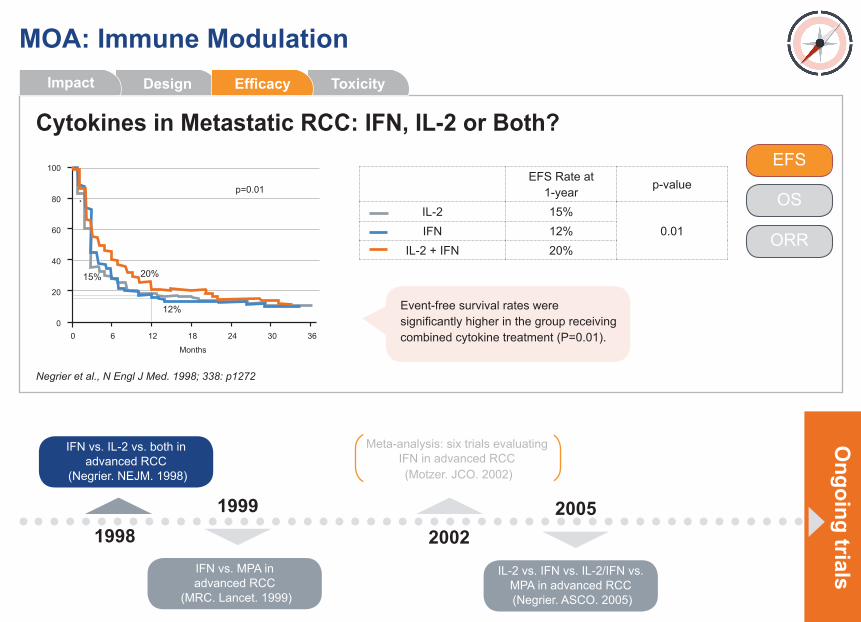
Cytokines in Metastatic RCC: IFN, IL-2 or Both?
Negrier et al., N Engl J Med. 1998; 338: p1272
ToxicityEfficacyDesignImpact
• Cytokines involved in activation of the host immune response are moderately active in metastatic RCC; interferon and IL-2 have been part of standard treatment since the 1990’s• Groupe Français d’Immunothérapie hypothesized that the combination of both cytokines could improve outcome in this randomized phase III trial• Lack of improvement of OS with the combination as well as poor toxicity profile associated with both combination and single agent IL-2; consequently, IFN considered SOC and comparator for future phase III trials
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
Ongoing trials
MOA: Immune Modulation
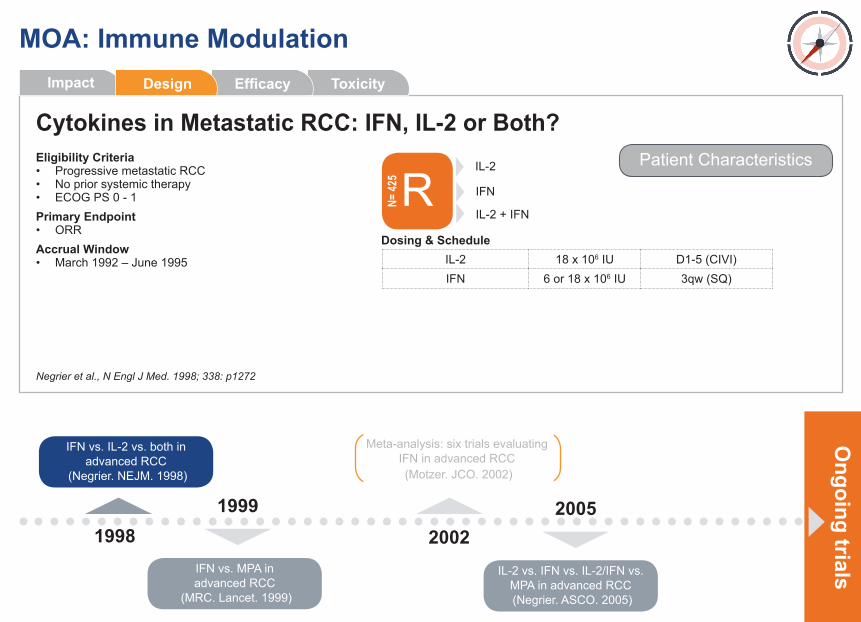
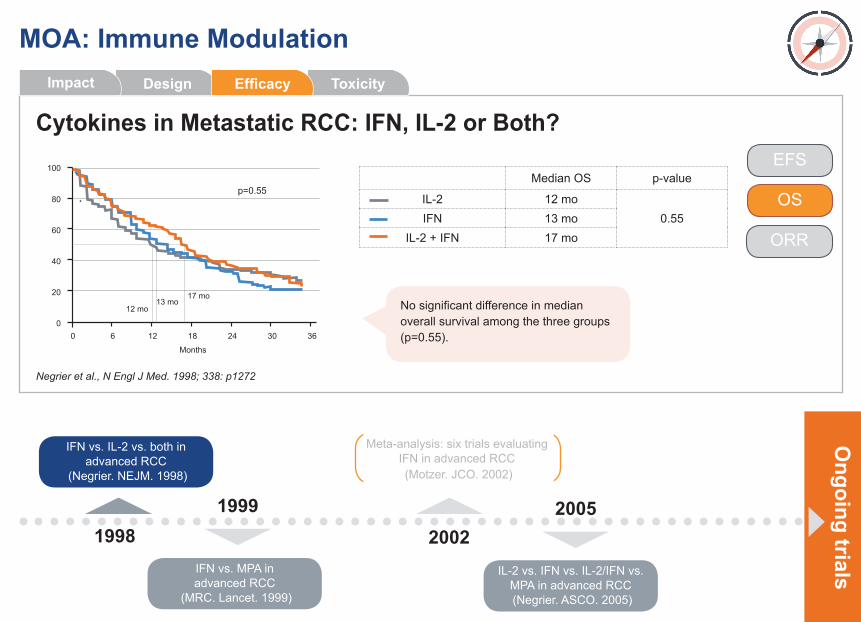
Cytokines in Metastatic RCC: IFN, IL-2 or Both?
Negrier et al., N Engl J Med. 1998; 338: p1272
Eligibility Criteria• Progressive metastatic RCC• No prior systemic therapy• ECOG PS 0 - 1Primary Endpoint• ORRAccrual Window• March 1992 – June 1995
Patient Characteristics
R IFN
IL-2
IL-2 + IFN
N= 42
5
IL-2 18 x 106 IU D1-5 (CIVI)IFN 6 or 18 x 106 IU 3qw (SQ)
Dosing & Schedule
ToxicityEfficacyImpact Design
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
Ongoing trials
MOA: Immune Modulation
Cytokines in Metastatic RCC: IFN, IL-2 or Both?
Negrier et al., N Engl J Med. 1998; 338: p1272
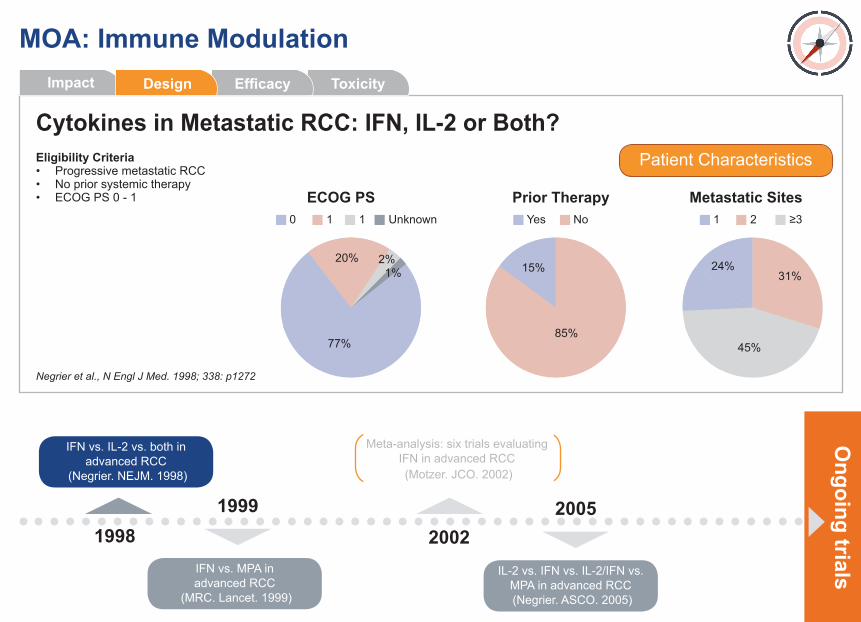
Eligibility Criteria• Progressive metastatic RCC• No prior systemic therapy• ECOG PS 0 - 1
Patient Characteristics
Prior TherapyYes No
15%
85%
Metastatic Sites
31%24%
45%
1 2 ≥3
ToxicityEfficacyImpact Design
ECOG PS0 1 1 Unknown
77%
20% 2%1%
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
Ongoing trials
MOA: Immune Modulation
Cytokines in Metastatic RCC: IFN, IL-2 or Both?
Negrier et al., N Engl J Med. 1998; 338: p1272
EFS Rate at 1-year
p-value
IL-2 15%0.01IFN 12%
IL-2 + IFN 20%
0
60
80
40
20
100
Months
0 186 12 3024 36
EFS
OS
ORR
ToxicityDesign EfficacyImpact
Event-free survival rates were significantly higher in the group receiving combined cytokine treatment (P=0.01).
p=0.01
12%
20%15%
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
Ongoing trials
MOA: Immune Modulation
Cytokines in Metastatic RCC: IFN, IL-2 or Both?
Negrier et al., N Engl J Med. 1998; 338: p1272
EFSMedian OS p-value
IL-2 12 mo0.55IFN 13 mo
IL-2 + IFN 17 mo
0
60
80
40
20
100
Months
0 186 12 3024 36
OS
ORR
ToxicityDesign EfficacyImpact
No significant difference in median overall survival among the three groups (p=0.55).
p=0.55
12 mo13 mo
17 mo
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
Ongoing trials
MOA: Immune Modulation
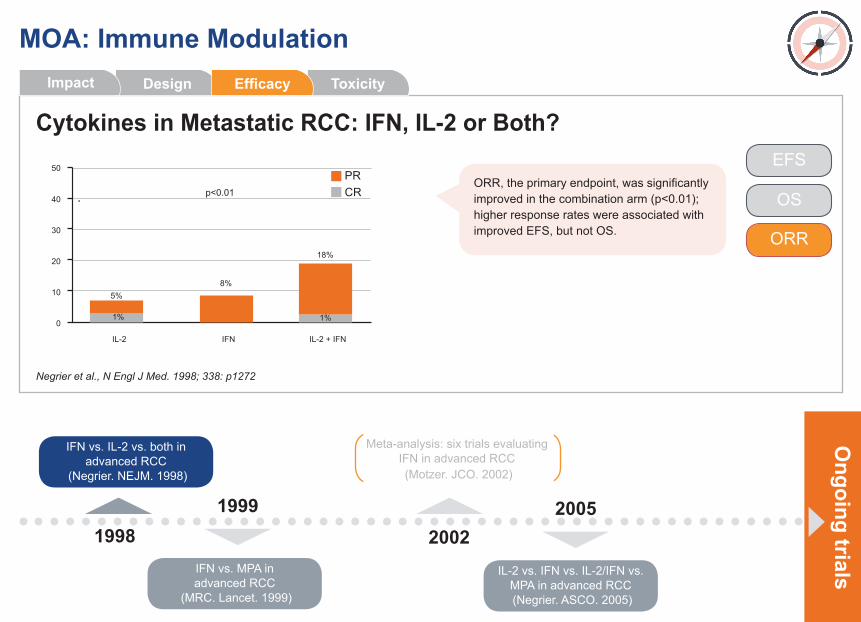
Cytokines in Metastatic RCC: IFN, IL-2 or Both?
Negrier et al., N Engl J Med. 1998; 338: p1272
OS
ORR
0
30
40
20
10
50
IL-2 IFN IL-2 + IFN
8%5%
18%
1% 1%
EFS
ToxicityDesign EfficacyImpact
ORR, the primary endpoint, was significantly improved in the combination arm (p<0.01); higher response rates were associated with improved EFS, but not OS.
p<0.01
PRCR
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
Ongoing trials
MOA: Immune Modulation
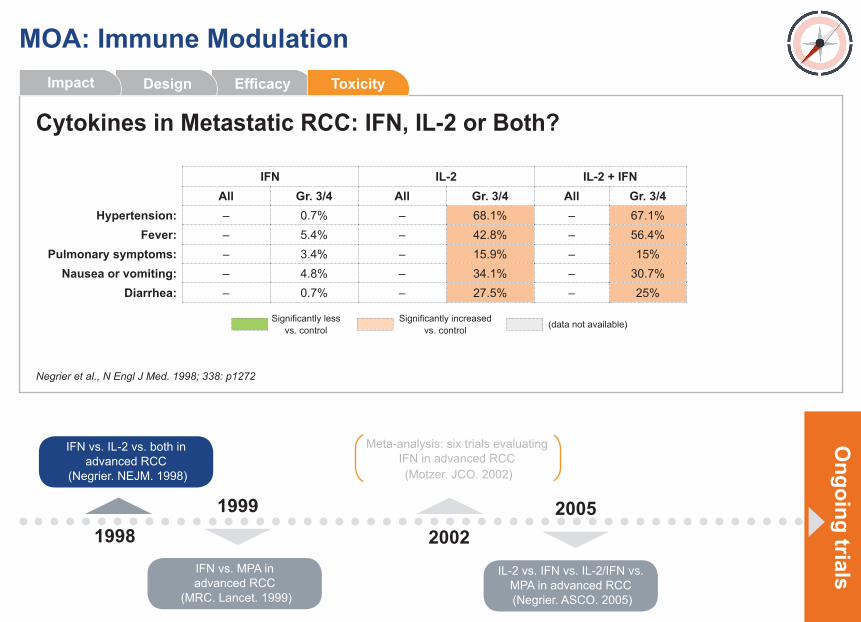
Cytokines in Metastatic RCC: IFN, IL-2 or Both?
Negrier et al., N Engl J Med. 1998; 338: p1272
IFN IL-2 IL-2 + IFN All Gr. 3/4 All Gr. 3/4 All Gr. 3/4
Hypertension: – 0.7% – 68.1% – 67.1%Fever: – 5.4% – 42.8% – 56.4%
Pulmonary symptoms: – 3.4% – 15.9% – 15%Nausea or vomiting: – 4.8% – 34.1% – 30.7%
Diarrhea: – 0.7% – 27.5% – 25%
Efficacy ToxicityDesignImpact
Significantly less vs. control
Significantly increased vs. control (data not available)
Ongoing trials
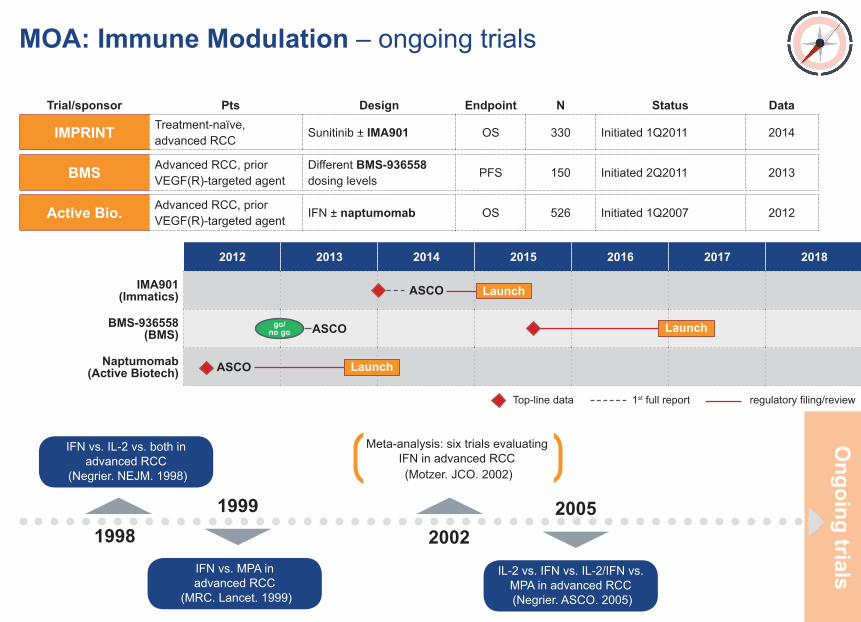
MOA: Immune Modulation – ongoing trials
Trial/sponsor RE Pts-3 Design Endpoint N Status Data
IMPRINT Treatment-naïve, advanced RCC
Sunitinib ± IMA901 OS 330 Initiated 1Q2011 2014
BMS Advanced RCC, prior VEGF(R)-targeted agent
Different BMS-936558 dosing levels
PFS 150 Initiated 2Q2011 2013
Active Bio. Advanced RCC, prior VEGF(R)-targeted agent
IFN ± naptumomab OS 526 Initiated 1Q2007 2012
2012 2013 2014 2015 2016 2017 2018
IMA901 (Immatics) ASCO
BMS-936558(BMS) ASCO
Naptumomab(Active Biotech) ASCO
Launch
Launch
Launchgo/no go
Top-line data 1st full report regulatory filing/review
1998 2002IFN vs. MPA in advanced RCC
(MRC. Lancet. 1999)
IL-2 vs. IFN vs. IL-2/IFN vs. MPA in advanced RCC (Negrier. ASCO. 2005)
IFN vs. IL-2 vs. both in advanced RCC
(Negrier. NEJM. 1998)
Meta-analysis: six trials evaluating IFN in advanced RCC (Motzer. JCO. 2002)
1999 2005
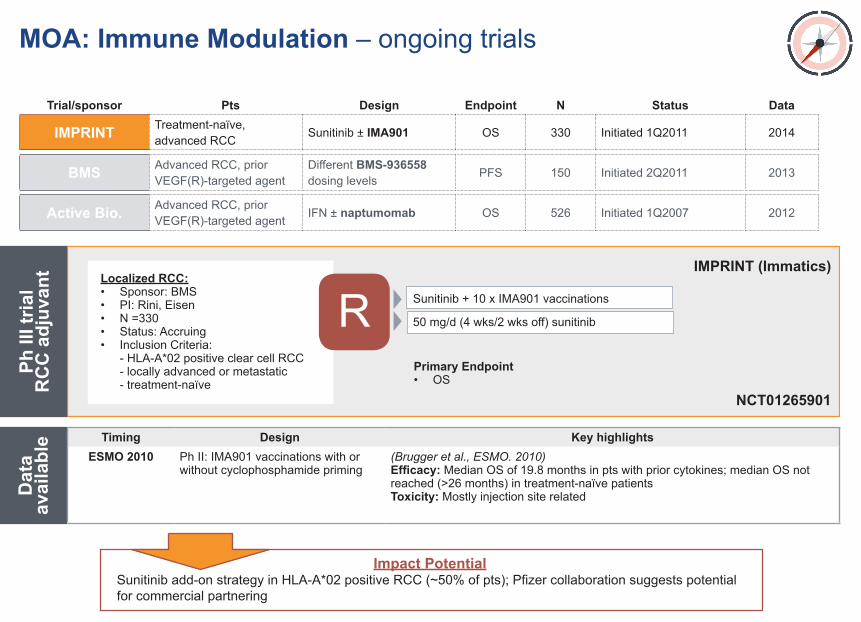
R
Impact PotentialSunitinib add-on strategy in HLA-A*02 positive RCC (~50% of pts); Pfizer collaboration suggests potential for commercial partnering
Ph II
I tria
l
RC
C a
djuv
ant
Dat
a av
aila
ble
Localized RCC:• Sponsor: BMS• PI: Rini, Eisen• N =330• Status: Accruing• Inclusion Criteria: - HLA-A*02 positive clear cell RCC - locally advanced or metastatic - treatment-naïve
Primary Endpoint• OS
IMPRINT (Immatics)
NCT01265901
MOA: Immune Modulation – ongoing trials
Trial/sponsor RE Pts-3 Design Endpoint N Status Data
IMPRINT Treatment-naïve, advanced RCC
Sunitinib ± IMA901 OS 330 Initiated 1Q2011 2014
BMS Advanced RCC, prior VEGF(R)-targeted agent
Different BMS-936558 dosing levels
PFS 150 Initiated 2Q2011 2013
Active Bio. Advanced RCC, prior VEGF(R)-targeted agent
IFN ± naptumomab OS 526 Initiated 1Q2007 2012
Timing Design Key highlightsESMO 2010 Ph II: IMA901 vaccinations with or
without cyclophosphamide priming(Brugger et al., ESMO. 2010)Efficacy: Median OS of 19.8 months in pts with prior cytokines; median OS not reached (>26 months) in treatment-naïve patientsToxicity: Mostly injection site related
Sunitinib + 10 x IMA901 vaccinations
50 mg/d (4 wks/2 wks off) sunitinib
R
MOA: Immune Modulation – ongoing trials
Trial/sponsor RE Pts-3 Design Endpoint N Status Data
IMPRINT Treatment-naïve, advanced RCC
Sunitinib ± IMA901 OS 330 Initiated 1Q2011 2014
BMS Advanced RCC, prior VEGF(R)-targeted agent
Different BMS-936558 dosing levels
PFS 150 Initiated 2Q2011 2013
Active Bio. Advanced RCC, prior VEGF(R)-targeted agent
IFN ± naptumomab OS 526 Initiated 1Q2007 2012
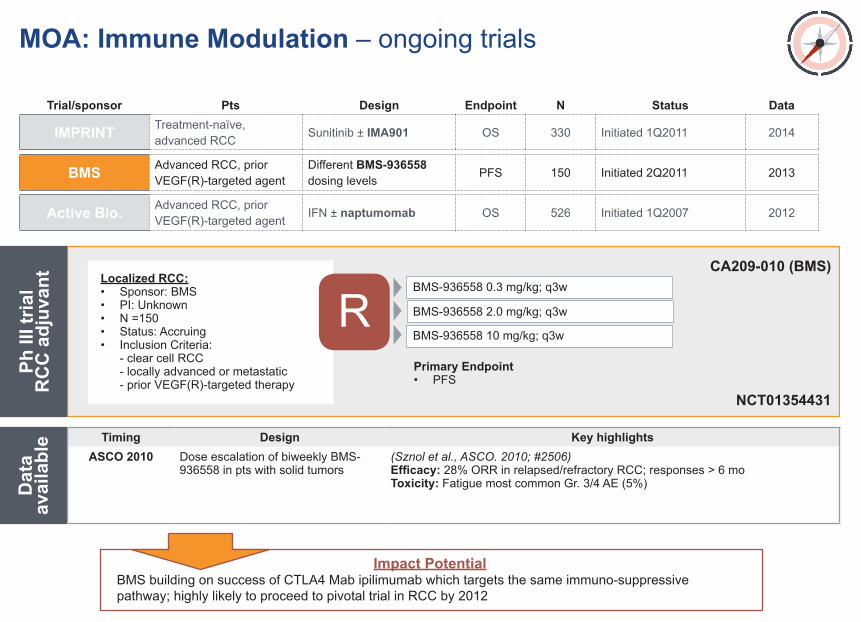
Impact PotentialBMS building on success of CTLA4 Mab ipilimumab which targets the same immuno-suppressive pathway; highly likely to proceed to pivotal trial in RCC by 2012
Ph II
I tria
l
RC
C a
djuv
ant
Dat
a av
aila
ble
Localized RCC:• Sponsor: BMS• PI: Unknown• N =150• Status: Accruing• Inclusion Criteria: - clear cell RCC - locally advanced or metastatic - prior VEGF(R)-targeted therapy
Primary Endpoint• PFS
CA209-010 (BMS)
NCT01354431
Timing Design Key highlightsASCO 2010 Dose escalation of biweekly BMS-
936558 in pts with solid tumors(Sznol et al., ASCO. 2010; #2506)Efficacy: 28% ORR in relapsed/refractory RCC; responses > 6 mo Toxicity: Fatigue most common Gr. 3/4 AE (5%)
BMS-936558 0.3 mg/kg; q3w
BMS-936558 2.0 mg/kg; q3w
BMS-936558 10 mg/kg; q3w
R
MOA: Immune Modulation – ongoing trials
Trial/sponsor RE Pts-3 Design Endpoint N Status Data
IMPRINT Treatment-naïve, advanced RCC
Sunitinib ± IMA901 OS 330 Initiated 1Q2011 2014
BMS Advanced RCC, prior VEGF(R)-targeted agent
Different BMS-936558 dosing levels
PFS 150 Initiated 2Q2011 2013
Active Bio. Advanced RCC, prior VEGF(R)-targeted agent
IFN ± naptumomab OS 526 Initiated 1Q2007 2012
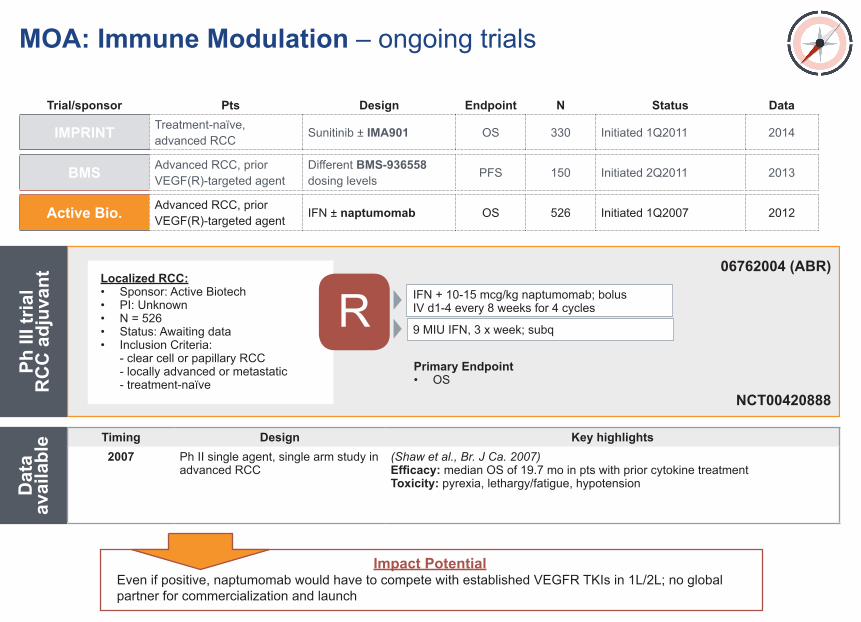
Impact PotentialEven if positive, naptumomab would have to compete with established VEGFR TKIs in 1L/2L; no global partner for commercialization and launch
Ph II
I tria
l
RC
C a
djuv
ant
Dat
a av
aila
ble
Localized RCC:• Sponsor: Active Biotech• PI: Unknown• N = 526• Status: Awaiting data• Inclusion Criteria: - clear cell or papillary RCC - locally advanced or metastatic - treatment-naïve
Primary Endpoint• OS
06762004 (ABR)
NCT00420888
Timing Design Key highlights2007 Ph II single agent, single arm study in
advanced RCC(Shaw et al., Br. J Ca. 2007)Efficacy: median OS of 19.7 mo in pts with prior cytokine treatmentToxicity: pyrexia, lethargy/fatigue, hypotension
IFN + 10-15 mcg/kg naptumomab; bolus IV d1-4 every 8 weeks for 4 cycles
9 MIU IFN, 3 x week; subq
MOA: Anti-angiogenesis
Ub Ub
Ub
Ub
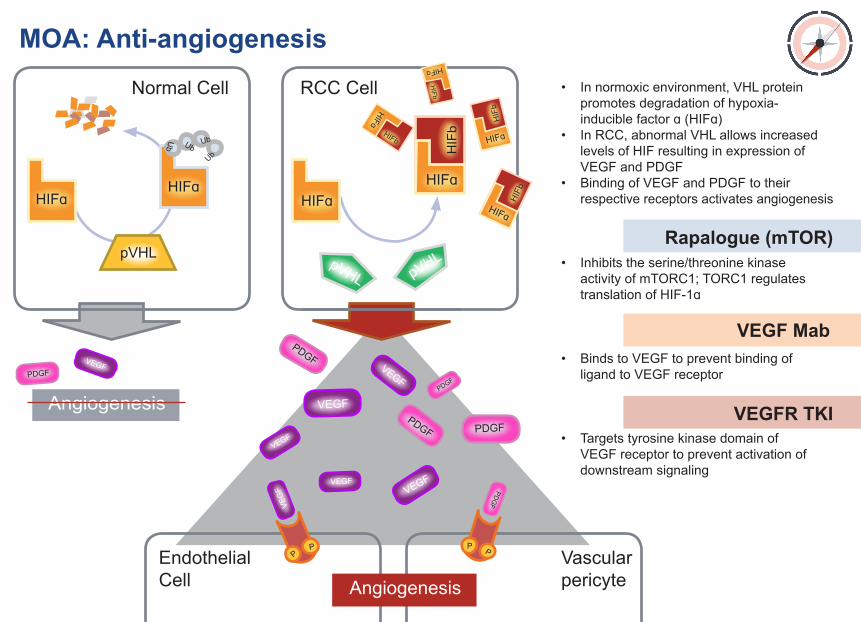
• Innormoxicenvironment,VHLprotein promotesdegradationofhypoxia- induciblefactorɑ(HIFɑ)• InRCC,abnormalVHLallowsincreased levelsofHIFresultinginexpressionof VEGFandPDGF• BindingofVEGFandPDGFtotheir respectivereceptorsactivatesangiogenesis
• Inhibitstheserine/threoninekinase activityofmTORC1;TORC1regulates translationofHIF-1ɑ
• BindstoVEGFtopreventbindingof ligandtoVEGFreceptor
• Targetstyrosinekinasedomainof VEGFreceptortopreventactivationof downstreamsignaling
NormalCell
EndothelialCell
RCCCell
Rapalogue (mTOR)
VEGF Mab
VEGFR TKI
VascularpericyteAngiogenesis
PP P P
Angiogenesis
HIFɑHIFɑ
HIFɑHIFɑ
HIFɑ
HIFɑ
HIFɑ
HIFɑ
pVHL pVHL
HIF
bHIFb
HIFb
HIF
b
HIFb
pVHL
PDGFVEGF
VEGF
VEGF
VEGF VEG
F
VEGF
VEGF
PDGFPDGF
PDGFPDG
F
PDGF
VEGFR TKIs: TolerabilityVEGFR TKIs: Efficacy
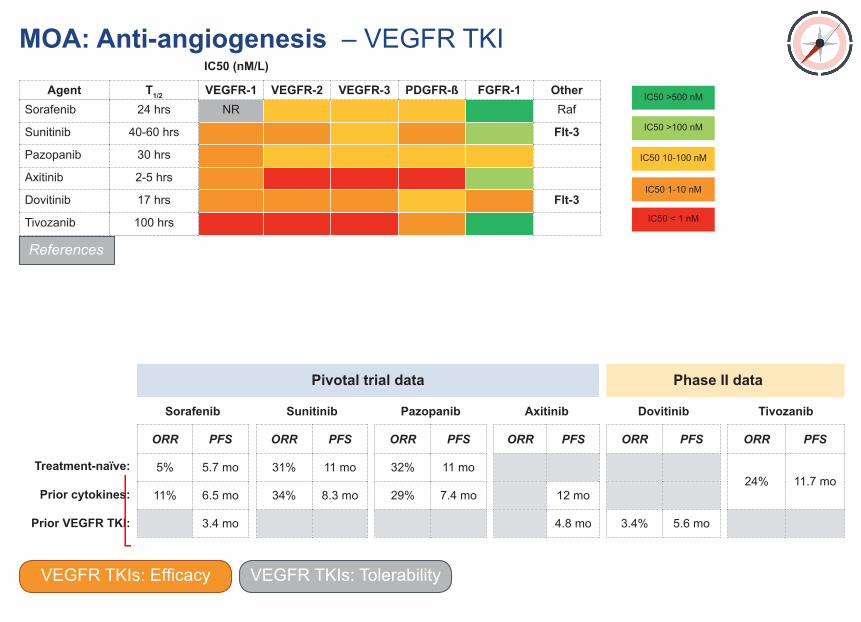
MOA: Anti-angiogenesis – VEGFR TKI
Sorafenib
ORR PFS
5% 5.7 mo
11% 6.5 mo
3.4 mo
Sunitinib
ORR PFS
31% 11 mo
34% 8.3 mo
Pazopanib
ORR PFS
32% 11 mo
29% 7.4 mo
Axitinib
ORR PFS
12 mo
4.8 mo
Dovitinib
ORR PFS
3.4% 5.6 mo
Tivozanib
ORR PFS
24% 11.7 mo
Pivotal trial data Phase II data
Treatment-naïve:
Prior cytokines:
Prior VEGFR TKI:
References
IC50 (nM/L)
Agent T1/2 VEGFR-1 VEGFR-2 VEGFR-3 PDGFR-ß FGFR-1 OtherSorafenib 24 hrs NR Raf
Sunitinib 40-60 hrs Flt-3
Pazopanib 30 hrs
Axitinib 2-5 hrs
Dovitinib 17 hrs Flt-3
Tivozanib 100 hrs
IC50 >500 nM
IC50 >100 nM
IC50 10-100 nM
IC50 1-10 nM
IC50 < 1 nM
VEGFR TKIs: TolerabilityVEGFR TKIs: Efficacy
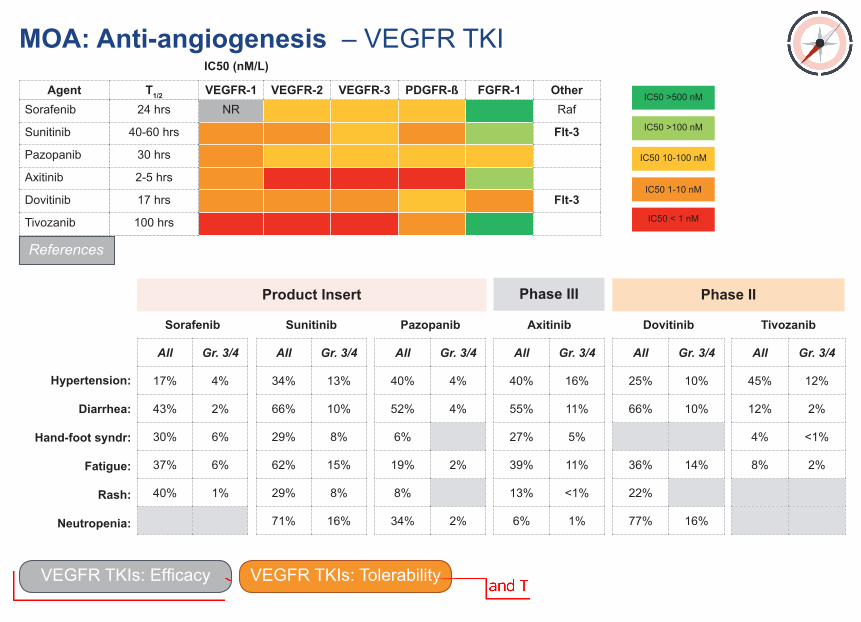
MOA: Anti-angiogenesis – VEGFR TKI
Sorafenib
All Gr. 3/4
17% 4%
43% 2%
30% 6%
37% 6%
40% 1%
Sunitinib
All Gr. 3/4
34% 13%
66% 10%
29% 8%
62% 15%
29% 8%
71% 16%
Pazopanib
All Gr. 3/4
40% 4%
52% 4%
6%
19% 2%
8%
34% 2%
Axitinib
All Gr. 3/4
40% 16%
55% 11%
27% 5%
39% 11%
13% <1%
6% 1%
Dovitinib
All Gr. 3/4
25% 10%
66% 10%
36% 14%
22%
77% 16%
Tivozanib
All Gr. 3/4
45% 12%
12% 2%
4% <1%
8% 2%
Product Insert Phase IIPhase III
Hypertension:
Diarrhea:
Hand-foot syndr:
Fatigue:
Rash:
Neutropenia:
References
IC50 (nM/L)
Agent T1/2 VEGFR-1 VEGFR-2 VEGFR-3 PDGFR-ß FGFR-1 OtherSorafenib 24 hrs NR Raf
Sunitinib 40-60 hrs Flt-3
Pazopanib 30 hrs
Axitinib 2-5 hrs
Dovitinib 17 hrs Flt-3
Tivozanib 100 hrs
IC50 >500 nM
IC50 >100 nM
IC50 10-100 nM
IC50 1-10 nM
IC50 < 1 nM
VEGFR TKIs: TolerabilityVEGFR TKIs: Efficacy
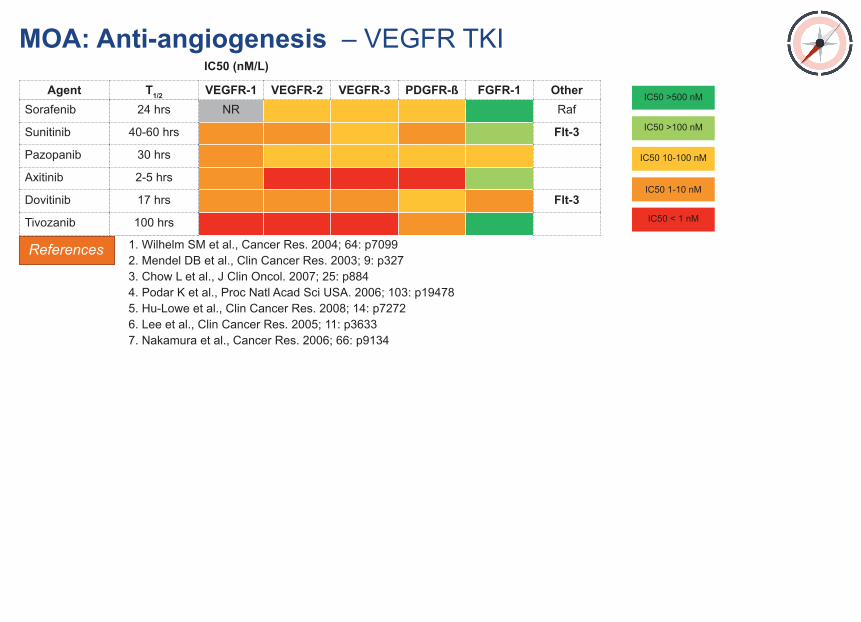
MOA: Anti-angiogenesis – VEGFR TKI
References 1. Wilhelm SM et al., Cancer Res. 2004; 64: p70992. Mendel DB et al., Clin Cancer Res. 2003; 9: p3273. Chow L et al., J Clin Oncol. 2007; 25: p884 4. Podar K et al., Proc Natl Acad Sci USA. 2006; 103: p194785. Hu-Lowe et al., Clin Cancer Res. 2008; 14: p72726. Lee et al., Clin Cancer Res. 2005; 11: p36337. Nakamura et al., Cancer Res. 2006; 66: p9134
IC50 (nM/L)
Agent T1/2 VEGFR-1 VEGFR-2 VEGFR-3 PDGFR-ß FGFR-1 OtherSorafenib 24 hrs NR Raf
Sunitinib 40-60 hrs Flt-3
Pazopanib 30 hrs
Axitinib 2-5 hrs
Dovitinib 17 hrs Flt-3
Tivozanib 100 hrs
IC50 >500 nM
IC50 >100 nM
IC50 10-100 nM
IC50 1-10 nM
IC50 < 1 nM
Ongoing trials
MOA: Anti-angiogenesis – VEGFR TKI – sorafenib
FDA & EMEA approval
2005 20102011
Ph IIb: sorafenib vs. IFN in 1L
(Escudier. JCO. 2009)
Ph II: sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
Ph II: sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009
Sorafenib Expanded Access Program (EU-ARCCS)
(Beck. Ann Oncol. 2011)
Sorafenib Expanded Access Program (NA-ARCCS)
(Stadler. Cancer. 2010)
Pivotal ph III: sorafenib in cytokine-refractory RCC (Escudier. JCO. 2009)
2009
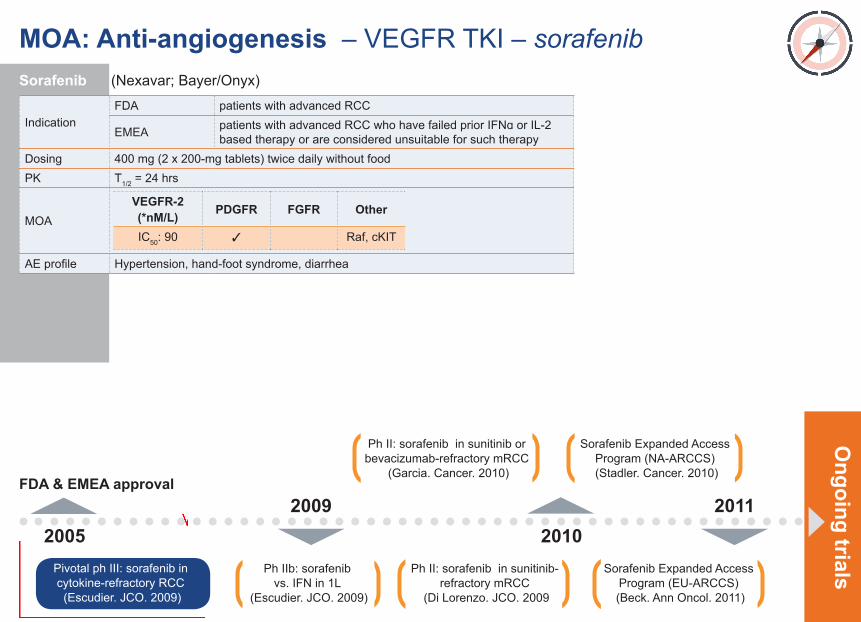
Sorafenib (Nexavar; Bayer/Onyx)
IndicationFDA patients with advanced RCC
EMEA patients with advanced RCC who have failed prior IFNɑ or IL-2 based therapy or are considered unsuitable for such therapy
Dosing 400 mg (2 x 200-mg tablets) twice daily without foodPK T1/2 = 24 hrs
MOA
AE profile Hypertension, hand-foot syndrome, diarrhea
VEGFR-2 (*nM/L) PDGFR FGFR Other
IC50: 90 ✓ Raf, cKIT
Ongoing trials
FDA & EMEA approval
2005 20102011
Ph IIb: sorafenib vs. IFN in 1L
(Escudier. JCO. 2009)
Ph II: sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
Ph II: sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009
Sorafenib Expanded Access Program (EU-ARCCS)
(Beck. Ann Oncol. 2011)
Sorafenib Expanded Access Program (NA-ARCCS)
(Stadler. Cancer. 2010)
Pivotal ph III: sorafenib in cytokine-refractory RCC (Escudier. JCO. 2009)
MOA: Anti-angiogenesis – VEGFR TKI – sorafenib
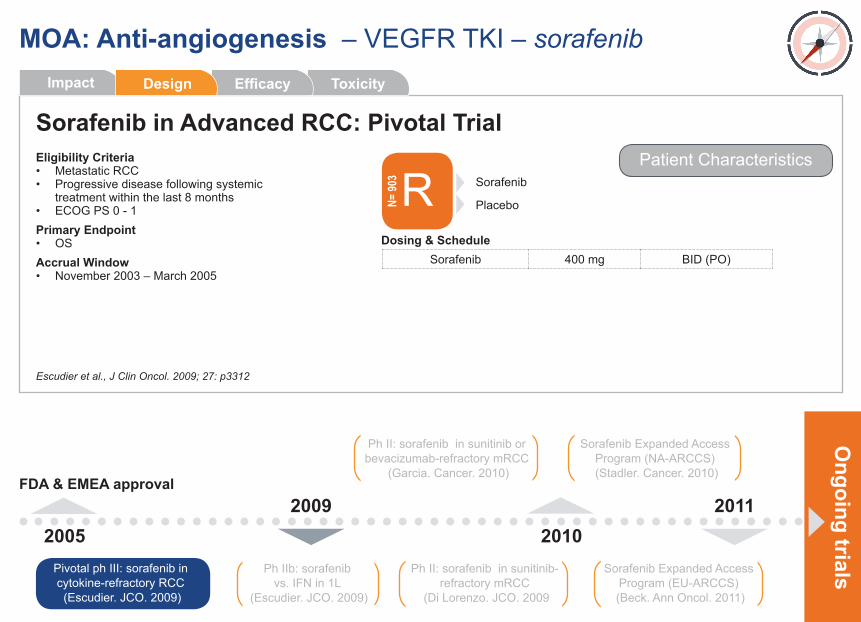
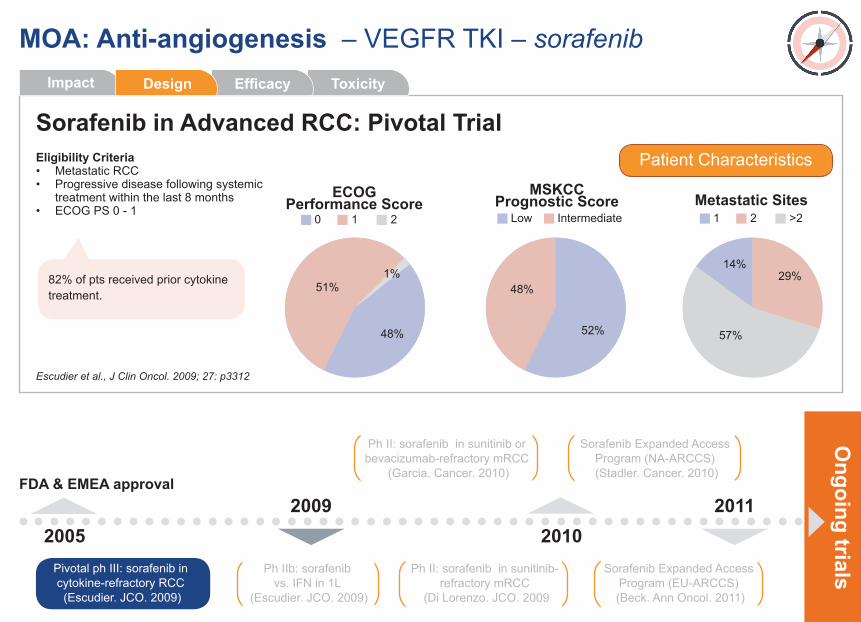
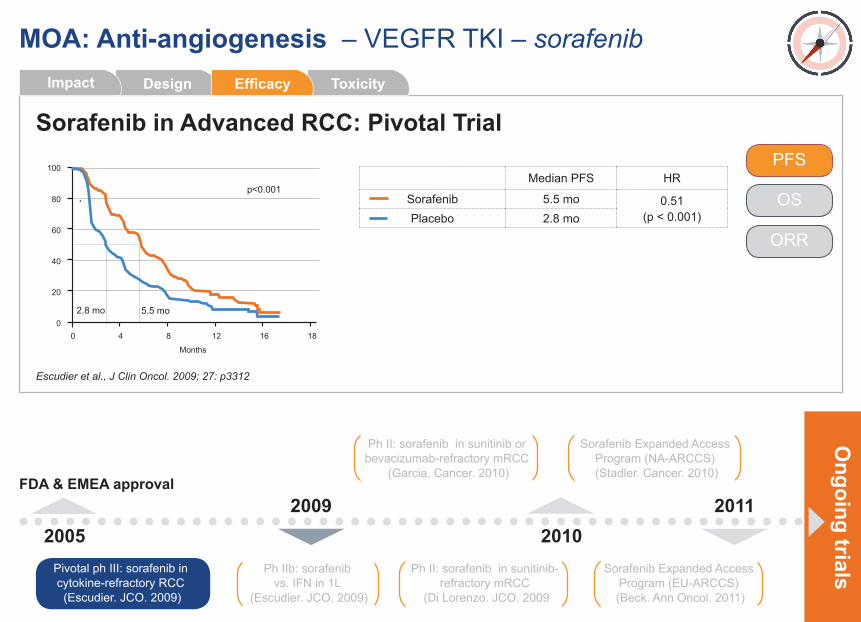
Sorafenib in Advanced RCC: Pivotal Trial
Escudier et al., J Clin Oncol. 2009; 27: p3312
2009
ToxicityEfficacyDesignImpact
• RCC tumors are highly vascularized as angiogenesis is driven by HIF-1ɑ, a protein over-expressed in clear cell RCC due to aberrant expression of VHL; HIF-1ɑ upregulates expression of VEGF• Sorafenib, a VEGFR-targeted tyrosine kinase inhibitor, was compared to placebo in this randomized phase III trial which enrolled pts with prior cytokines• FDA approved sorafenib for “advanced RCC” in 2006; EMEA indication limited to pts with prior cytokines
Ongoing trials
FDA & EMEA approval
2005 20102011
Ph IIb: sorafenib vs. IFN in 1L
(Escudier. JCO. 2009)
Ph II: sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
Ph II: sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009
Sorafenib Expanded Access Program (EU-ARCCS)
(Beck. Ann Oncol. 2011)
Sorafenib Expanded Access Program (NA-ARCCS)
(Stadler. Cancer. 2010)
Pivotal ph III: sorafenib in cytokine-refractory RCC (Escudier. JCO. 2009)
MOA: Anti-angiogenesis – VEGFR TKI – sorafenib
Sorafenib in Advanced RCC: Pivotal Trial
Escudier et al., J Clin Oncol. 2009; 27: p3312
2009
Eligibility Criteria• Metastatic RCC• Progressive disease following systemic treatment within the last 8 months• ECOG PS 0 - 1Primary Endpoint• OSAccrual Window• November 2003 – March 2005
Patient Characteristics
R Sorafenib
PlaceboN= 90
3
Sorafenib 400 mg BID (PO)Dosing & Schedule
ToxicityEfficacyImpact Design
Ongoing trials
FDA & EMEA approval
2005 20102011
Ph IIb: sorafenib vs. IFN in 1L
(Escudier. JCO. 2009)
Ph II: sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
Ph II: sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009
Sorafenib Expanded Access Program (EU-ARCCS)
(Beck. Ann Oncol. 2011)
Sorafenib Expanded Access Program (NA-ARCCS)
(Stadler. Cancer. 2010)
Pivotal ph III: sorafenib in cytokine-refractory RCC (Escudier. JCO. 2009)
MOA: Anti-angiogenesis – VEGFR TKI – sorafenib
Sorafenib in Advanced RCC: Pivotal Trial
Escudier et al., J Clin Oncol. 2009; 27: p3312
2009
Eligibility Criteria• Metastatic RCC• Progressive disease following systemic treatment within the last 8 months• ECOG PS 0 - 1
Patient Characteristics
MSKCC Prognostic Score
Low Intermediate
48%
52%
Metastatic Sites
29%14%
57%
1 2 >2
ToxicityEfficacyImpact Design
ECOG Performance Score
0 1 2
48%
51%1%82% of pts received prior cytokine
treatment.
Ongoing trials
FDA & EMEA approval
2005 20102011
Ph IIb: sorafenib vs. IFN in 1L
(Escudier. JCO. 2009)
Ph II: sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
Ph II: sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009
Sorafenib Expanded Access Program (EU-ARCCS)
(Beck. Ann Oncol. 2011)
Sorafenib Expanded Access Program (NA-ARCCS)
(Stadler. Cancer. 2010)
Pivotal ph III: sorafenib in cytokine-refractory RCC (Escudier. JCO. 2009)
MOA: Anti-angiogenesis – VEGFR TKI – sorafenib
Sorafenib in Advanced RCC: Pivotal Trial
Escudier et al., J Clin Oncol. 2009; 27: p3312
2009
Median PFS HR
Sorafenib 5.5 mo 0.51(p < 0.001)Placebo 2.8 mo
0
60
80
40
20
100
Months
0 124 8 16 18
PFS
OS
ORR
ToxicityDesign EfficacyImpact
p<0.001
2.8 mo 5.5 mo
Ongoing trials
FDA & EMEA approval
2005 20102011
Ph IIb: sorafenib vs. IFN in 1L
(Escudier. JCO. 2009)
Ph II: sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
Ph II: sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009
Sorafenib Expanded Access Program (EU-ARCCS)
(Beck. Ann Oncol. 2011)
Sorafenib Expanded Access Program (NA-ARCCS)
(Stadler. Cancer. 2010)
Pivotal ph III: sorafenib in cytokine-refractory RCC (Escudier. JCO. 2009)
MOA: Anti-angiogenesis – VEGFR TKI – sorafenib
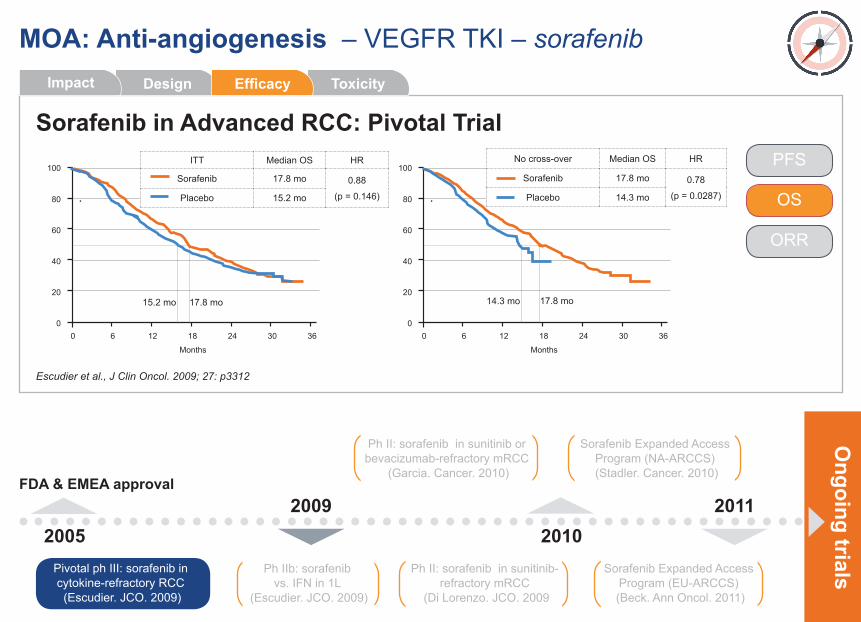
Sorafenib in Advanced RCC: Pivotal Trial
Escudier et al., J Clin Oncol. 2009; 27: p3312
2009
PFS
OS
ORR
ToxicityDesign EfficacyImpact
0
60
80
40
20
100
Months
0 186 12 30 36240
60
80
40
20
100
Months
0 186 12 30 3624
ITT Median OS HR
Sorafenib 17.8 mo 0.88
(p = 0.146)Placebo 15.2 mo
No cross-over Median OS HR
Sorafenib 17.8 mo 0.78
(p = 0.0287)Placebo 14.3 mo
17.8 mo 17.8 mo15.2 mo 14.3 mo
Ongoing trials
FDA & EMEA approval
2005 20102011
Ph IIb: sorafenib vs. IFN in 1L
(Escudier. JCO. 2009)
Ph II: sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
Ph II: sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009
Sorafenib Expanded Access Program (EU-ARCCS)
(Beck. Ann Oncol. 2011)
Sorafenib Expanded Access Program (NA-ARCCS)
(Stadler. Cancer. 2010)
Pivotal ph III: sorafenib in cytokine-refractory RCC (Escudier. JCO. 2009)
MOA: Anti-angiogenesis – VEGFR TKI – sorafenib
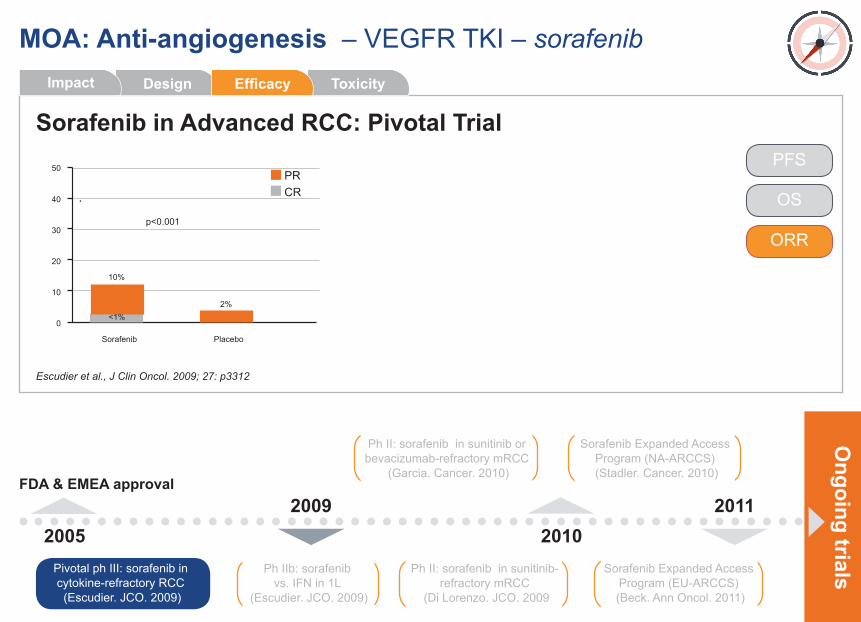
Sorafenib in Advanced RCC: Pivotal Trial
Escudier et al., J Clin Oncol. 2009; 27: p3312
2009
0
30
40
20
10
50
Sorafenib Placebo
2%
10%
<1%
PFS
OS
ORR
ToxicityDesign EfficacyImpact
p<0.001
PRCR
Ongoing trials
FDA & EMEA approval
2005 20102011
Ph IIb: sorafenib vs. IFN in 1L
(Escudier. JCO. 2009)
Ph II: sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
Ph II: sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009
Sorafenib Expanded Access Program (EU-ARCCS)
(Beck. Ann Oncol. 2011)
Sorafenib Expanded Access Program (NA-ARCCS)
(Stadler. Cancer. 2010)
Pivotal ph III: sorafenib in cytokine-refractory RCC (Escudier. JCO. 2009)
MOA: Anti-angiogenesis – VEGFR TKI – sorafenib
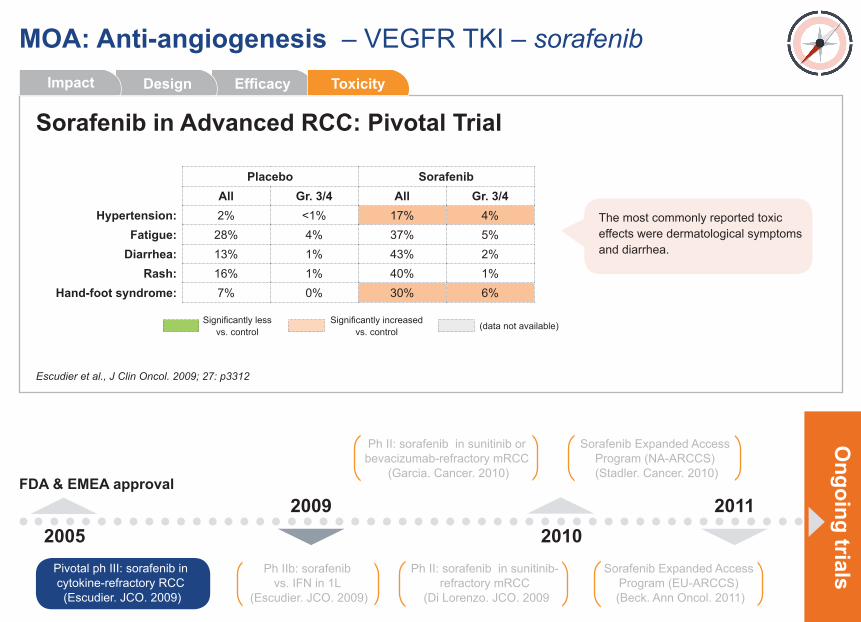
Sorafenib in Advanced RCC: Pivotal Trial
Escudier et al., J Clin Oncol. 2009; 27: p3312
2009
Placebo Sorafenib All Gr. 3/4 All Gr. 3/4
Hypertension: 2% <1% 17% 4%Fatigue: 28% 4% 37% 5%
Diarrhea: 13% 1% 43% 2%Rash: 16% 1% 40% 1%
Hand-foot syndrome: 7% 0% 30% 6%
Efficacy ToxicityDesignImpact
The most commonly reported toxic effects were dermatological symptoms and diarrhea.
Significantly less vs. control
Significantly increased vs. control (data not available)
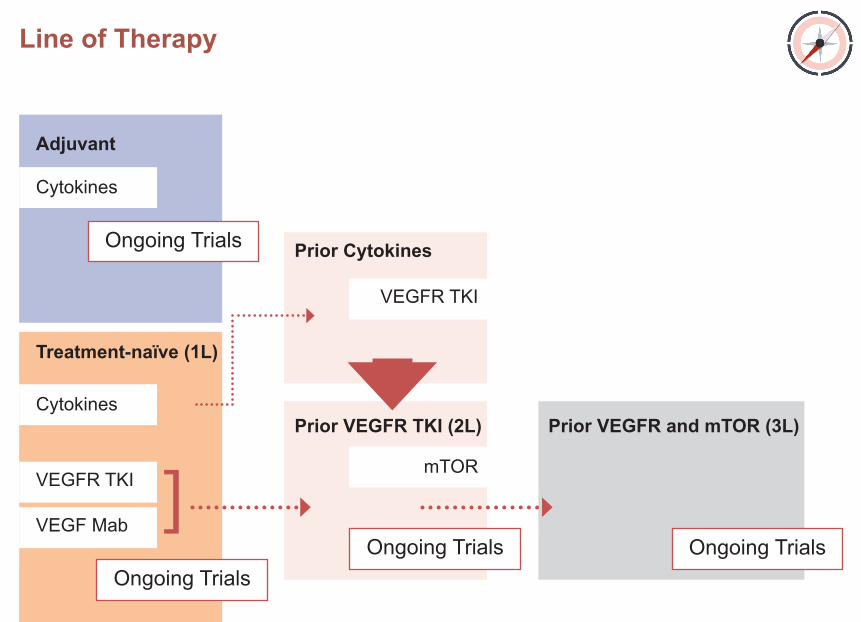
Line of Therapy
Adjuvant
Prior Cytokines
Prior VEGFR TKI (2L) Prior VEGFR and mTOR (3L)
Treatment-naïve (1L)
Cytokines
VEGFR TKI
mTOR
Cytokines
VEGFR TKI
VEGF Mab
Ongoing Trials
Ongoing TrialsOngoing Trials Ongoing Trials
]
Trials INTORACTUS (ECOG): Interferon vs. Observation Messing. JCO. 2003; 21: p1214UK (Cytokine Working Group): Interleukin-2 vs. Observation Clark. JCO. 2003; 21: p3133
Key
Ongoing Trials
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
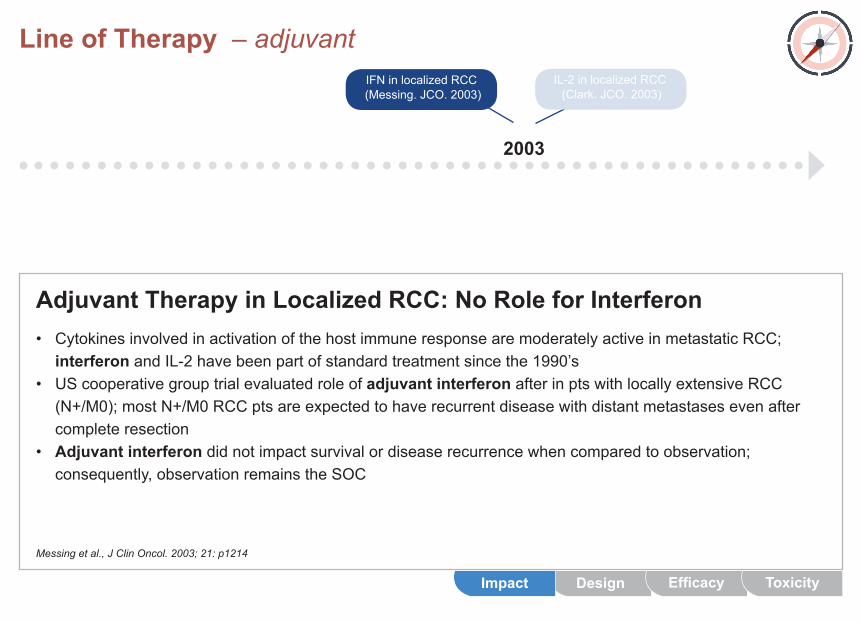
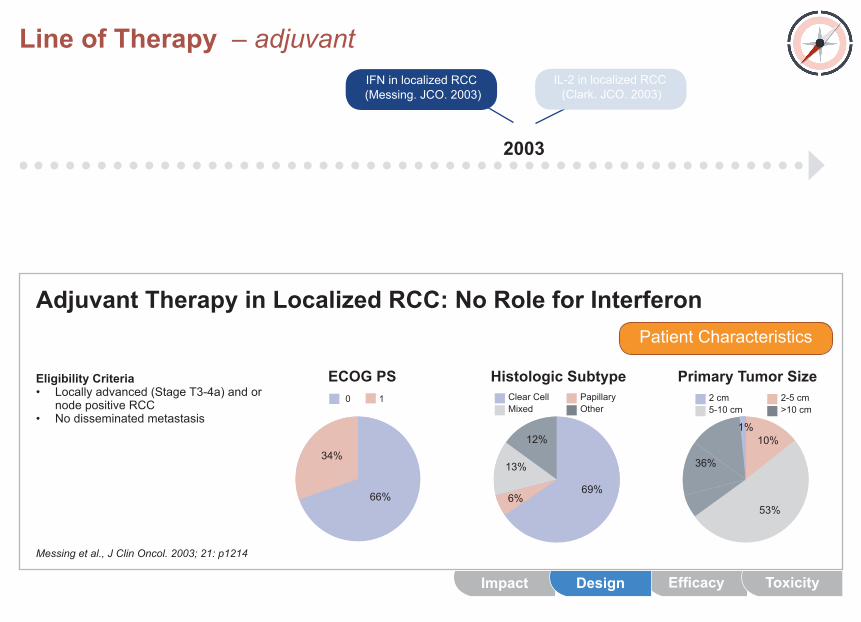
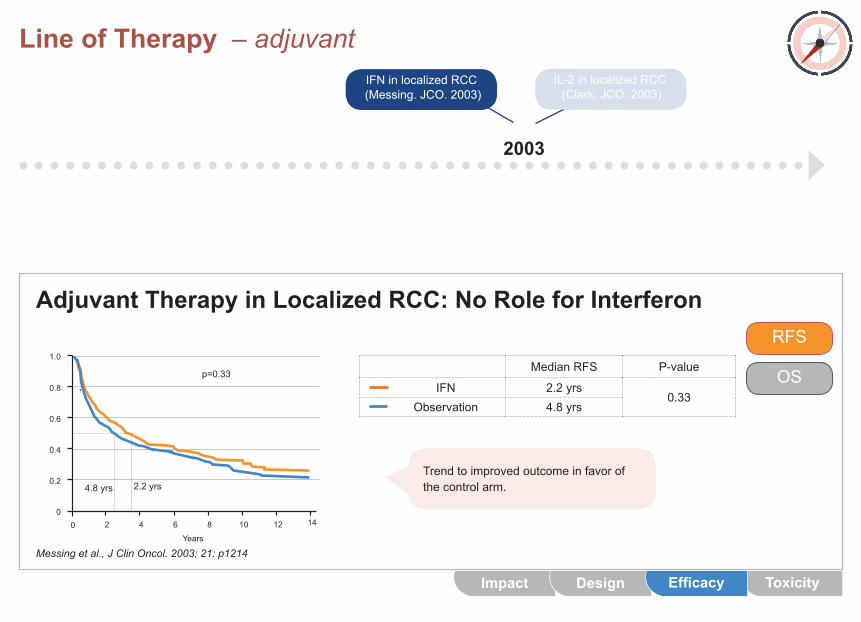
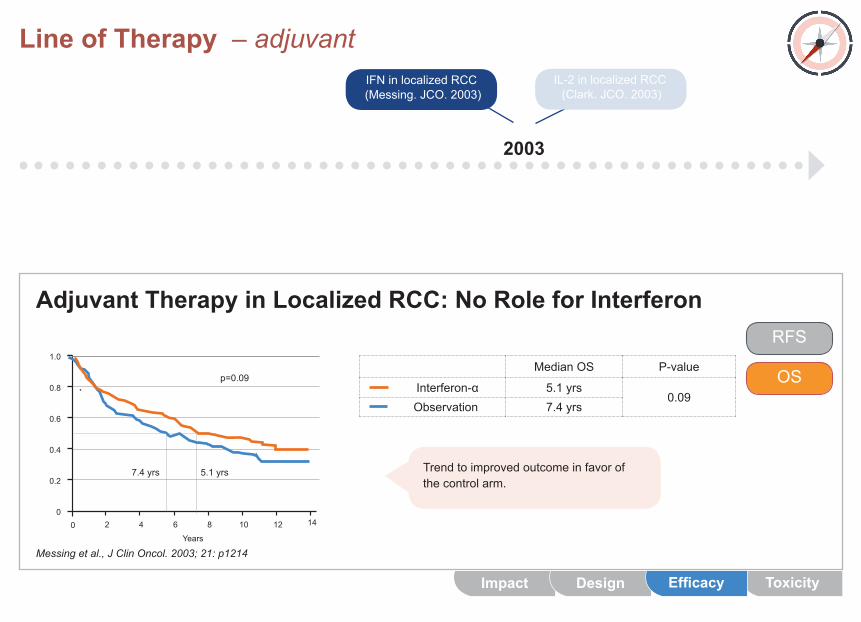
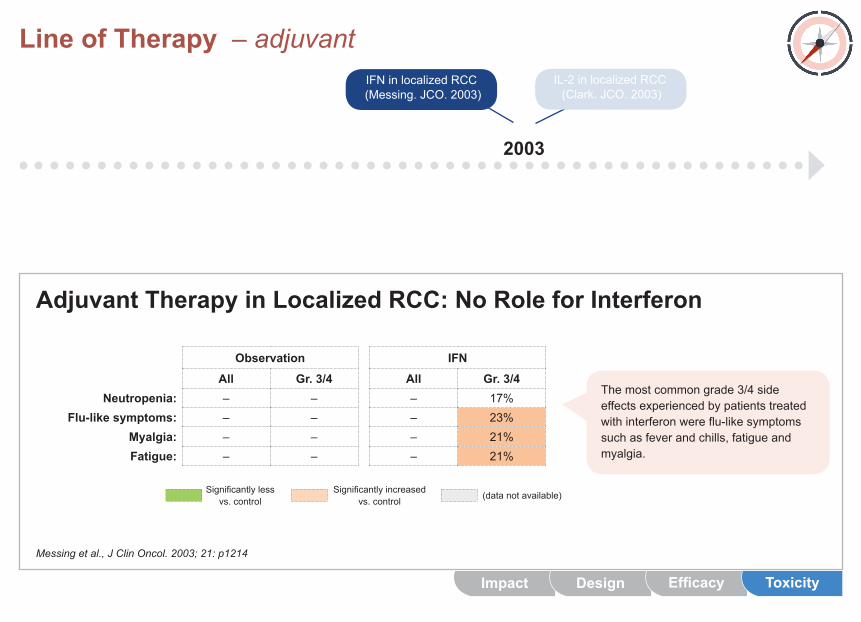
Adjuvant Therapy in Localized RCC: No Role for Interferon
Messing et al., J Clin Oncol. 2003; 21: p1214
• CytokinesinvolvedinactivationofthehostimmuneresponsearemoderatelyactiveinmetastaticRCC; interferonandIL-2havebeenpartofstandardtreatmentsincethe1990’s• UScooperativegrouptrialevaluatedroleofadjuvant interferon afterinptswithlocallyextensiveRCC (N+/M0);mostN+/M0RCCptsareexpectedtohaverecurrentdiseasewithdistantmetastasesevenafter complete resection• Adjuvant interferondidnotimpactsurvivalordiseaserecurrencewhencomparedtoobservation; consequently,observationremainstheSOC
DesignImpact Efficacy Toxicity
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
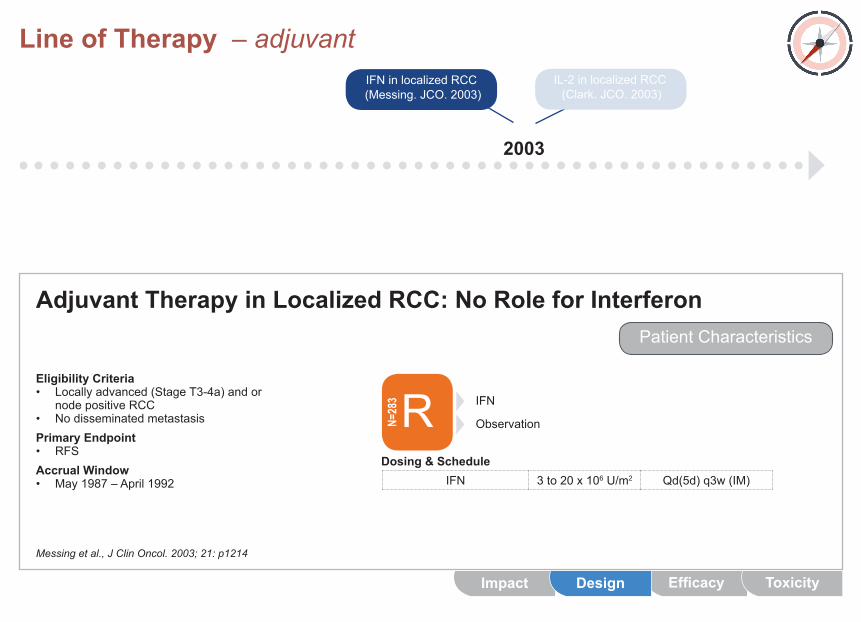
Adjuvant Therapy in Localized RCC: No Role for Interferon
Messing et al., J Clin Oncol. 2003; 21: p1214
Eligibility Criteria• Locallyadvanced(StageT3-4a)andor node positive RCC• NodisseminatedmetastasisPrimary Endpoint• RFSAccrual Window• May1987–April1992
PatientCharacteristics
RN=283
IFN 3to20x106 U/m2 Qd(5d) q3w (IM)Dosing & Schedule
Observation
IFN
EfficacyImpact Design Toxicity
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
Adjuvant Therapy in Localized RCC: No Role for Interferon
Messing et al., J Clin Oncol. 2003; 21: p1214
PatientCharacteristics
Eligibility Criteria• Locallyadvanced(StageT3-4a)andor node positive RCC• Nodisseminatedmetastasis
ECOG PS0 1
66%
34%
Histologic SubtypeClear CellMixed
PapillaryOther
12%
13%
69%6%
2 cm5-10 cm
2-5 cm>10 cm
Primary Tumor Size
10%
36%
53%
1%
EfficacyImpact Design Toxicity
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
Adjuvant Therapy in Localized RCC: No Role for Interferon
Messing et al., J Clin Oncol. 2003; 21: p1214
RFS
OSMedian RFS P-value
IFN 2.2 yrs0.33
Observation 4.8yrs
0
0.6
0.8
0.4
0.2
1.0
Years0 6 12102 4 8 14
Trend to improved outcome in favor of thecontrolarm.
Impact ToxicityDesign Efficacy
4.8yrs 2.2 yrs
p=0.33
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
Adjuvant Therapy in Localized RCC: No Role for Interferon
Messing et al., J Clin Oncol. 2003; 21: p1214
Median OS P-value
Interferon-α 5.1 yrs0.09
Observation 7.4yrs
Trend to improved outcome in favor of thecontrolarm.
0
0.6
0.8
0.4
0.2
1.0
Years0 6 12102 4 8 14
RFS
OS
Impact ToxicityDesign Efficacy
5.1 yrs7.4yrs
p=0.09
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
Adjuvant Therapy in Localized RCC: No Role for Interferon
Messing et al., J Clin Oncol. 2003; 21: p1214
Observation IFN All Gr. 3/4 All Gr. 3/4
Neutropenia: – – – 17%Flu-like symptoms: – – – 23%
Myalgia: – – – 21%Fatigue: – – – 21%
Themostcommongrade3/4sideeffectsexperiencedbypatientstreatedwithinterferonwereflu-likesymptomssuchasfeverandchills,fatigueandmyalgia.
Impact Design Efficacy Toxicity
Significantlyless vs. control
Significantlyincreased vs. control (data not available)
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
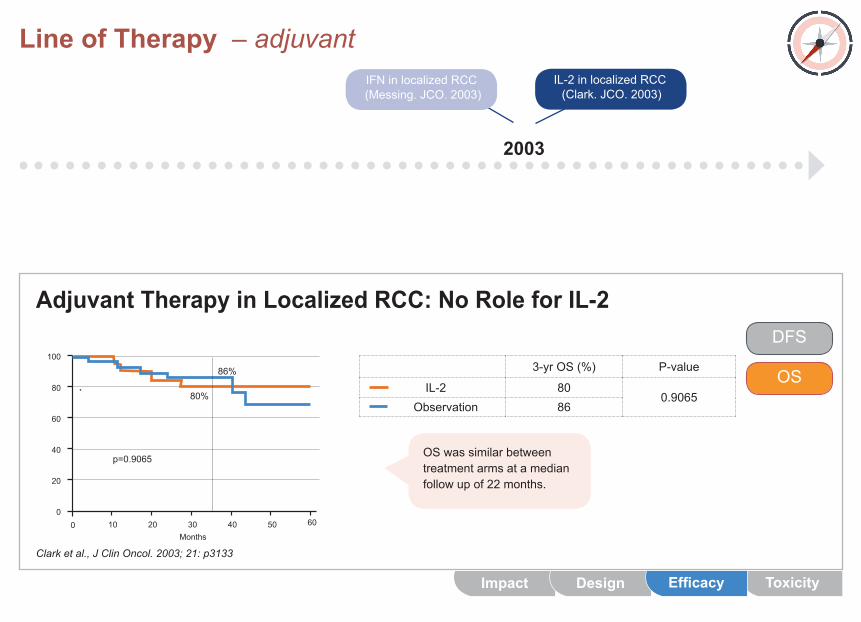
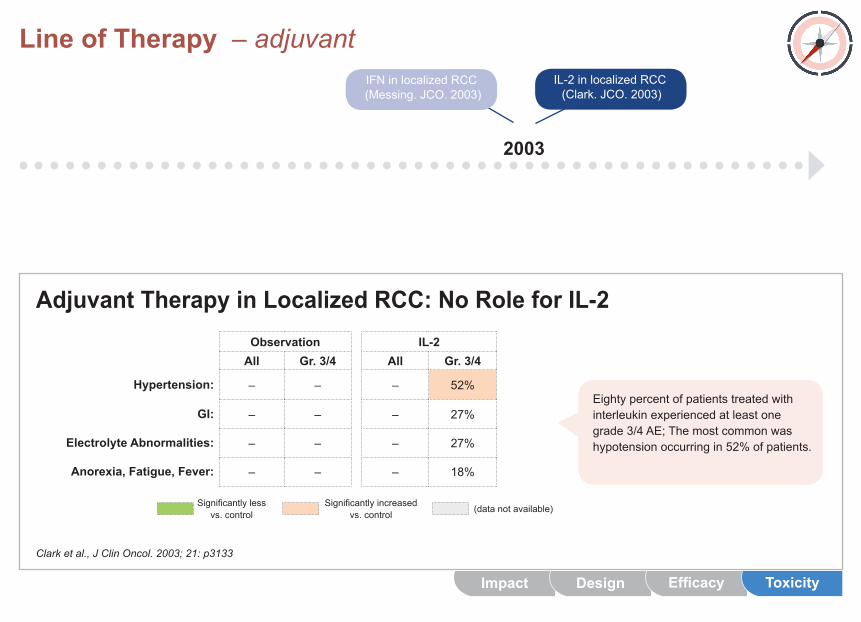
Adjuvant Therapy in Localized RCC: No Role for IL-2
Clark et al., J Clin Oncol. 2003; 21: p3133
• CytokinesinvolvedinactivationofthehostimmuneresponsearemoderatelyactiveinmetastaticRCC; interferon and IL-2havebeenpartofstandardtreatmentsincethe1990’s• Small,randomizedtrialevaluatesroleforIL-2,onlyFDA-approvedsystemictherapyformetastaticRCCat thattime,inptswithlocallyextensiveRCC• Likeadjuvantinterferon,IL-2didnotimpactsurvivalordiseaserecurrencewhencomparedtoobservation; observationafterresectionremainstheSOC
DesignImpact Efficacy Toxicity
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
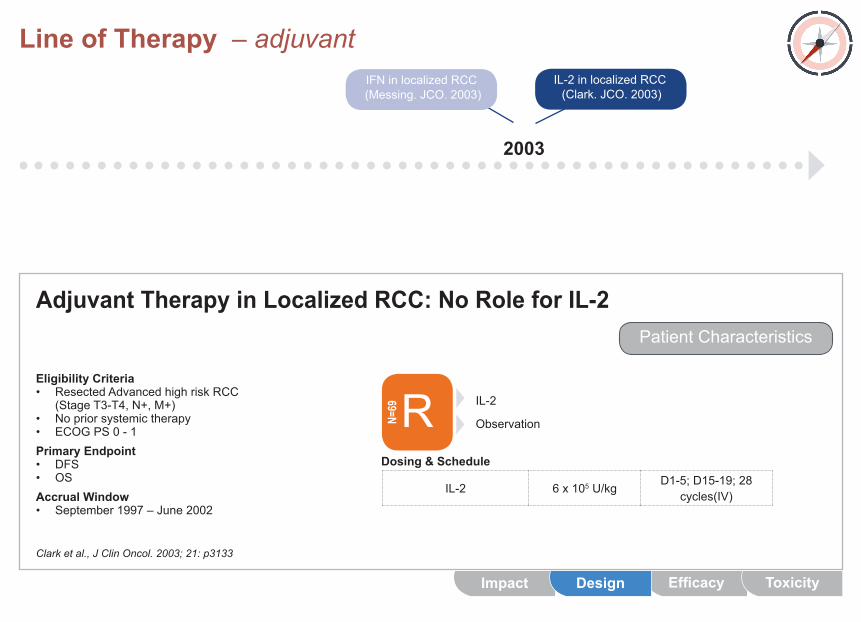
Adjuvant Therapy in Localized RCC: No Role for IL-2
Clark et al., J Clin Oncol. 2003; 21: p3133
Eligibility Criteria• ResectedAdvancedhighriskRCC (Stage T3-T4, N+, M+)• Nopriorsystemictherapy• ECOGPS0-1Primary Endpoint• DFS• OSAccrual Window• September1997–June2002
PatientCharacteristics
RN=69
IL-2 6x105 U/kgD1-5;D15-19;28
cycles(IV)
Dosing & Schedule
Observation
IL-2
EfficacyImpact Design Toxicity
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
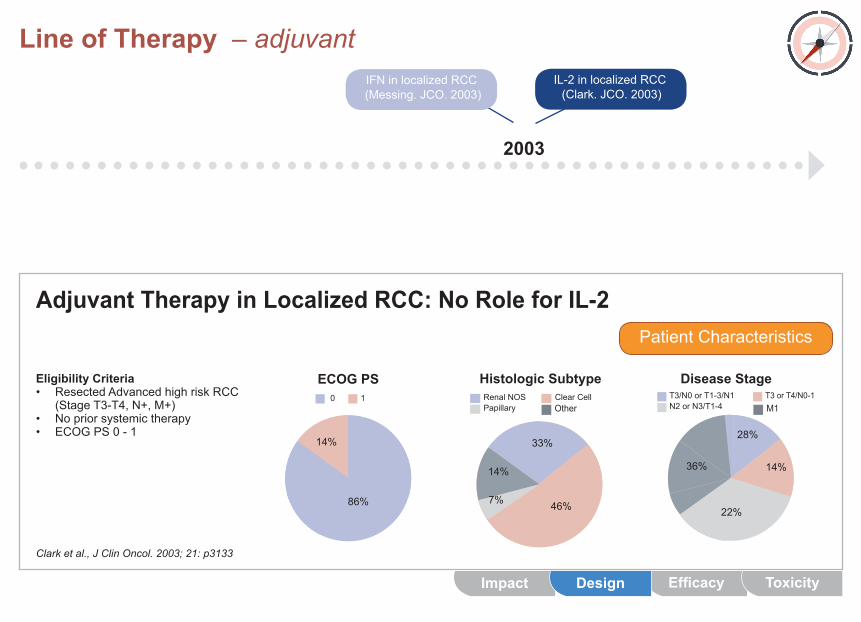
Adjuvant Therapy in Localized RCC: No Role for IL-2
Clark et al., J Clin Oncol. 2003; 21: p3133
Eligibility Criteria• ResectedAdvancedhighriskRCC (Stage T3-T4, N+, M+)• Nopriorsystemictherapy• ECOGPS0-1
PatientCharacteristics
ECOG PS0 1
86%
14%
EfficacyImpact Design Toxicity
T3/N0 or T1-3/N1N2 or N3/T1-4
T3 or T4/N0-1
Disease Stage
36%
28%
22%
14%
M1
Histologic SubtypeRenal NOSPapillary
Clear Cell
14%
33%
46%7%
Other
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
Adjuvant Therapy in Localized RCC: No Role for IL-2
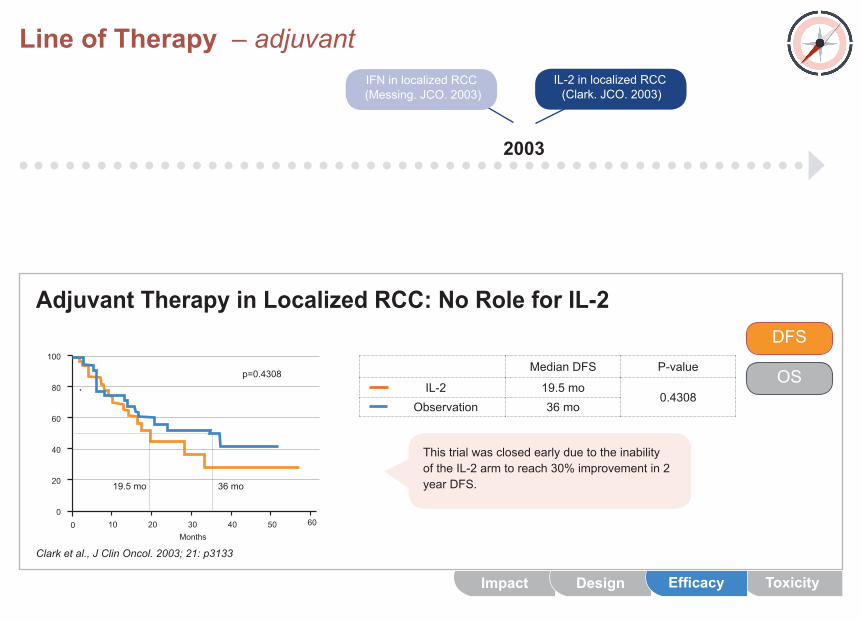
Clark et al., J Clin Oncol. 2003; 21: p3133
Median DFS P-value
IL-2 19.5mo0.4308
Observation 36 mo
0
60
80
40
20
100
Months0 502010 4030 60
ThistrialwasclosedearlyduetotheinabilityoftheIL-2armtoreach30%improvementin2year DFS.
DFS
OS
Impact ToxicityDesign Efficacy
19.5mo 36 mo
p=0.4308
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
Adjuvant Therapy in Localized RCC: No Role for IL-2
Clark et al., J Clin Oncol. 2003; 21: p3133
3-yr OS (%) P-value
IL-2 800.9065
Observation 86
0
60
80
40
20
100
Months0 502010 4030 60
OS was similar between treatment arms at a median followupof22months.
DFS
OS
Impact ToxicityDesign Efficacy
86%
80%
p=0.9065
Line of Therapy – adjuvantIL-2 in localized RCC (Clark. JCO. 2003)
IFN in localized RCC (Messing. JCO. 2003)
2003
Adjuvant Therapy in Localized RCC: No Role for IL-2
Clark et al., J Clin Oncol. 2003; 21: p3133
Observation IL-2 All Gr. 3/4 All Gr. 3/4
Hypertension: – – – 52%
GI: – – – 27%
Electrolyte Abnormalities: – – – 27%
Anorexia, Fatigue, Fever: – – – 18%
Eightypercentofpatientstreatedwithinterleukinexperiencedatleastonegrade3/4AE;Themostcommonwashypotensionoccurringin52%ofpatients.
Impact Design Efficacy Toxicity
Significantlyless vs. control
Significantlyincreased vs. control (data not available)
Line of Therapy – adjuvant – ongoing trials
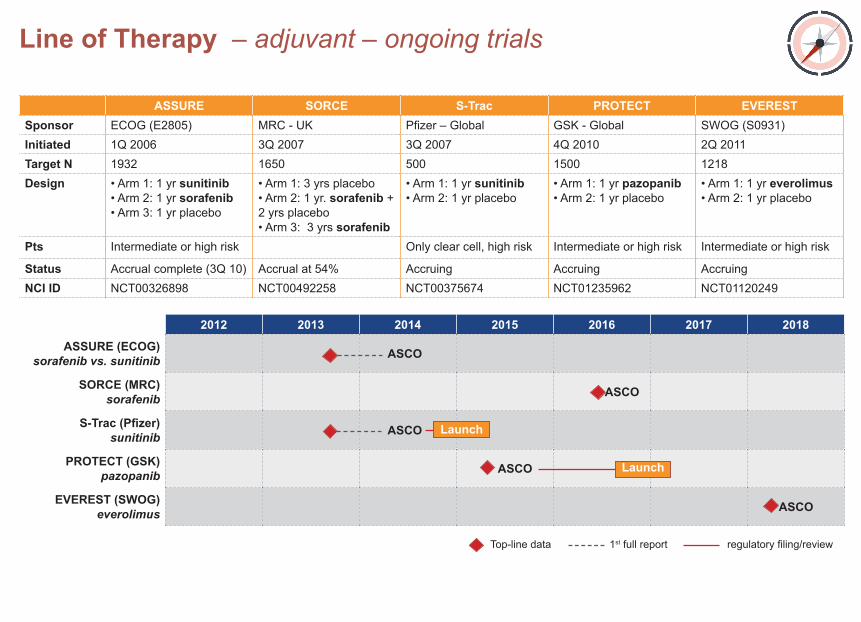
ASSURE SORCE S-Trac PROTECT EVERESTSponsor ECOG(E2805) MRC - UK Pfizer–Global GSK - Global SWOG(S0931)Initiated 1Q 2006 3Q2007 3Q2007 4Q 2010 2Q 2011Target N 1932 1650 500 1500 1218Design •Arm1:1yrsunitinib
•Arm2:1yrsorafenib•Arm3:1yrplacebo
•Arm1:3yrsplacebo•Arm2:1yr.sorafenib + 2 yrs placebo•Arm3:3yrssorafenib
•Arm1:1yrsunitinib•Arm2:1yrplacebo
•Arm1:1yrpazopanib•Arm2:1yrplacebo
•Arm1:1yreverolimus•Arm2:1yrplacebo
Pts Intermediateorhighrisk Onlyclearcell,highrisk Intermediateorhighrisk Intermediateorhighrisk
Status Accrual complete (3Q 10) Accrual at 54% Accruing Accruing AccruingNCI ID NCT00326898 NCT00492258 NCT00375674 NCT01235962 NCT01120249
2012 2013 2014 2015 2016 2017 2018
ASSURE (ECOG) sorafenib vs. sunitinib ASCO
SORCE (MRC) sorafenib ASCO
S-Trac (Pfizer) sunitinib ASCO
PROTECT (GSK) pazopanib ASCO
EVEREST (SWOG) everolimus ASCO
Launch
Top-line data 1st full report regulatoryfiling/review
Launch
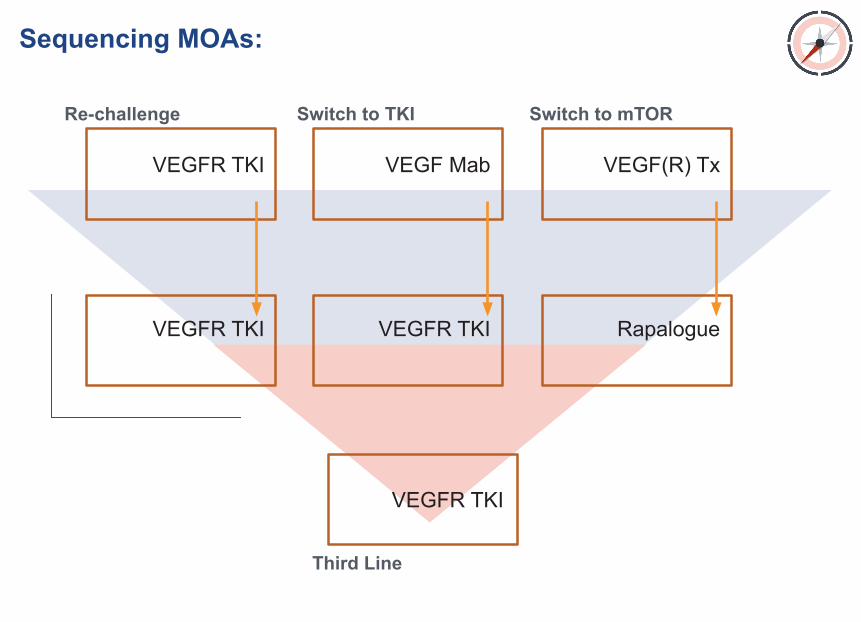
Sequencing MOAs:
Re-challenge Switch to TKI Switch to mTOR
Third Line
VEGFR TKI
VEGFR TKI
VEGF Mab
VEGFR TKI
VEGFR TKI
VEGF(R) Tx
Rapalogue
Ongoing trials
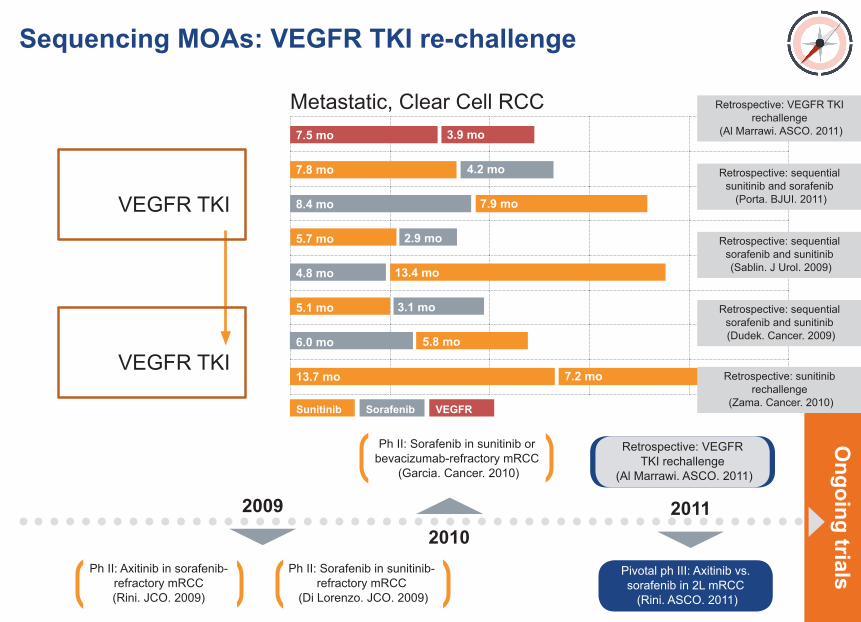
Sequencing MOAs: VEGFR TKI re-challenge
2010Pivotal ph III: Axitinib vs. sorafenib in 2L mRCC (Rini. ASCO. 2011)
Ph II: Sorafenib in sunitinib or bevacizumab-refractory mRCC
(Garcia. Cancer. 2010)
2009 2011
Ph II: Axitinib in sorafenib-refractory mRCC(Rini. JCO. 2009)
Ph II: Sorafenib in sunitinib-refractory mRCC
(Di Lorenzo. JCO. 2009)
VEGFR TKI
VEGFR TKI
Metastatic, Clear Cell RCC
7.8 mo 4.2 mo
7.5 mo 3.9 mo
8.4 mo 7.9 mo
5.7 mo 2.9 mo
4.8 mo 13.4 mo
5.1 mo 3.1 mo
6.0 mo 5.8 mo
Sunitinib Sorafenib VEGFR
13.7 mo 7.2 mo
Retrospective: VEGFR TKI rechallenge
(Al Marrawi. ASCO. 2011)
Retrospective: sequential sunitinib and sorafenib
(Porta. BJUI. 2011)
Retrospective: sequential sorafenib and sunitinib (Sablin. J Urol. 2009)
Retrospective: sequential sorafenib and sunitinib (Dudek. Cancer. 2009)
Retrospective: sunitinib rechallenge
(Zama. Cancer. 2010)
Retrospective: VEGFR TKI rechallenge
(Al Marrawi. ASCO. 2011)
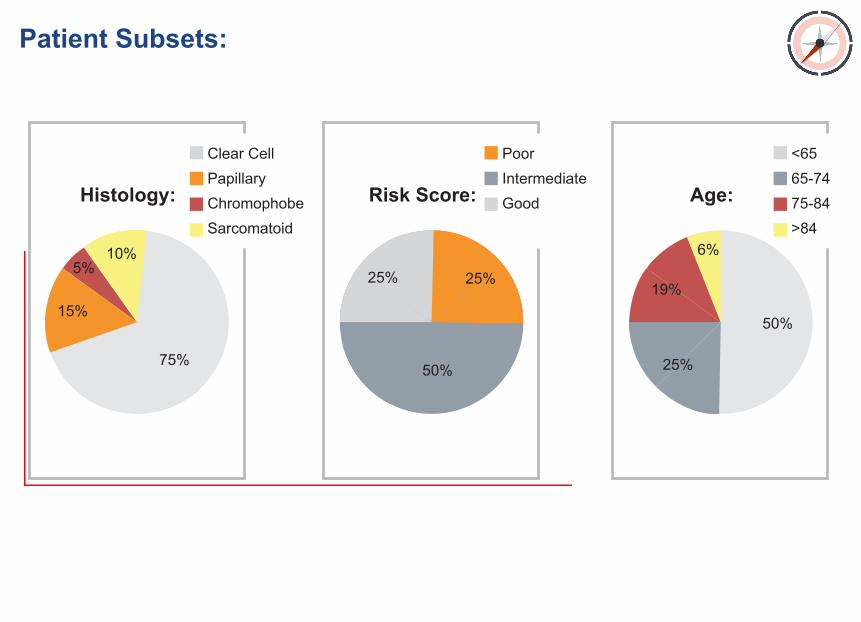
Patient Subsets:
Histology:
Clear CellPapillaryChromophobeSarcomatoid
10%5%
75%
15%
Age:
<6565-7475-84>84
6%
25%
50%
19%
Risk Score:
PoorIntermediateGood
50%
25% 25%
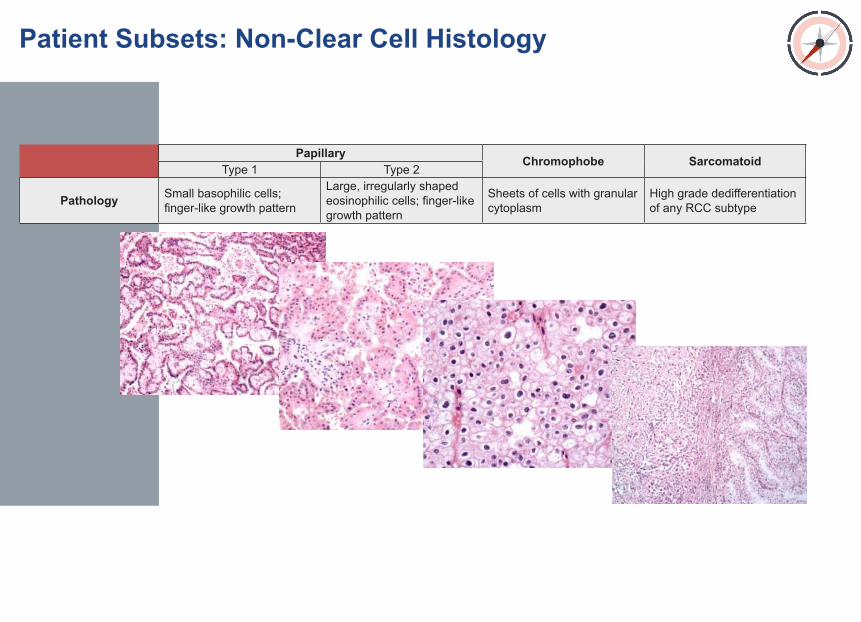
Papillary Chromophobe SarcomatoidType 1 Type 2
Pathology Small basophilic cells; finger-like growth pattern
Large, irregularly shaped eosinophilic cells; finger-like growth pattern
Sheets of cells with granular cytoplasm
High grade dedifferentiation of any RCC subtype
Patient Subsets: Non-Clear Cell Histology
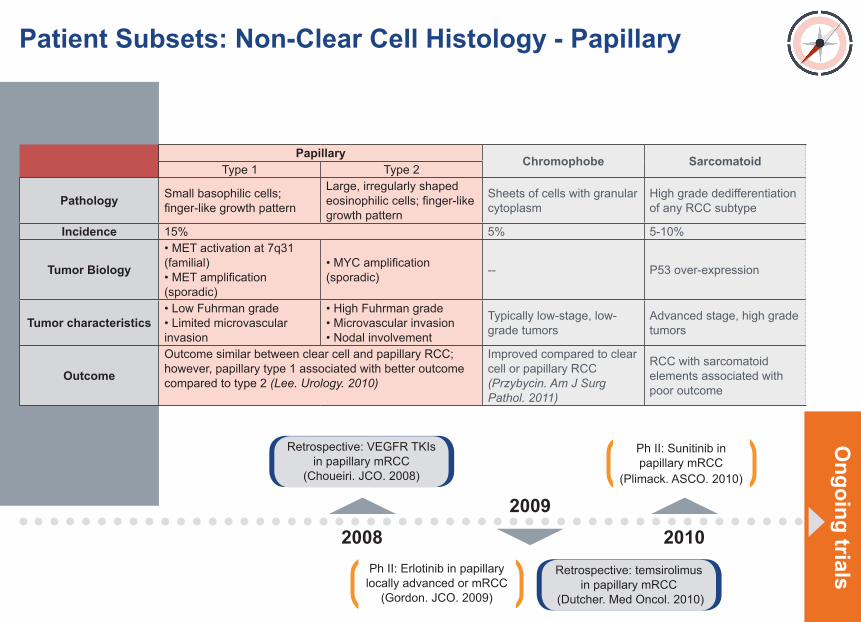
Papillary Chromophobe SarcomatoidType 1 Type 2
Pathology Small basophilic cells; finger-like growth pattern
Large, irregularly shaped eosinophilic cells; finger-like growth pattern
Sheets of cells with granular cytoplasm
High grade dedifferentiation of any RCC subtype
Incidence 15% 5% 5-10%
Tumor Biology
• MET activation at 7q31 (familial)• MET amplification (sporadic)
• MYC amplification (sporadic) -- P53 over-expression
Tumor characteristics• Low Fuhrman grade• Limited microvascular invasion
• High Fuhrman grade• Microvascular invasion• Nodal involvement
Typically low-stage, low-grade tumors
Advanced stage, high grade tumors
Outcome
Outcome similar between clear cell and papillary RCC; however, papillary type 1 associated with better outcome compared to type 2 (Lee. Urology. 2010)
Improved compared to clear cell or papillary RCC (Przybycin. Am J Surg Pathol. 2011)
RCC with sarcomatoid elements associated with poor outcome
Patient Subsets: Non-Clear Cell Histology - PapillaryO
ngoing trials
Retrospective: VEGFR TKIs in papillary mRCC
(Choueiri. JCO. 2008)
Retrospective: temsirolimus in papillary mRCC
(Dutcher. Med Oncol. 2010)
2008 20102009
Ph II: Sunitinib in papillary mRCC
(Plimack. ASCO. 2010)
Ph II: Erlotinib in papillary locally advanced or mRCC
(Gordon. JCO. 2009)
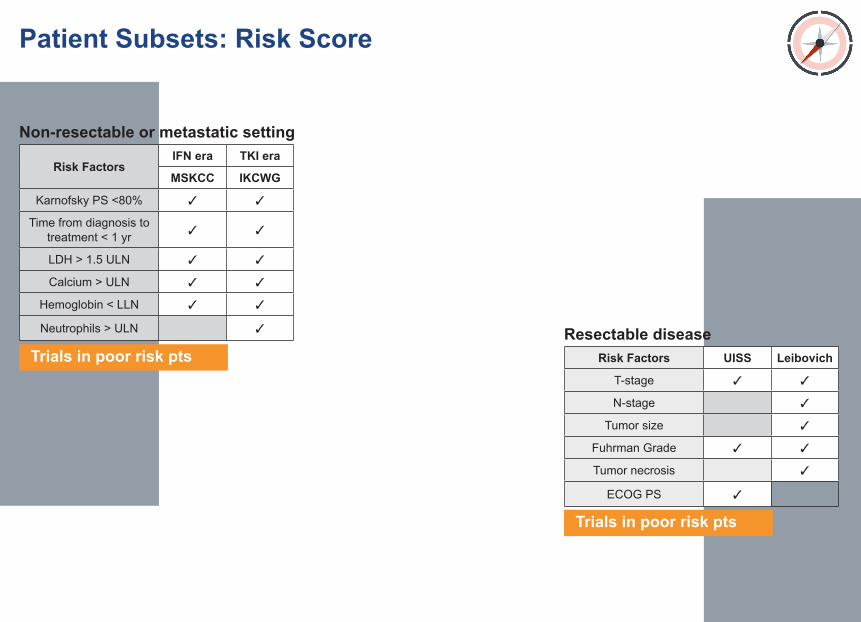
Risk FactorsIFN era TKI era
MSKCC IKCWG
Karnofsky PS <80% ✓ ✓
Time from diagnosis to treatment < 1 yr ✓ ✓
LDH > 1.5 ULN ✓ ✓
Calcium > ULN ✓ ✓
Hemoglobin < LLN ✓ ✓
Neutrophils > ULN ✓
Risk Factors UISS Leibovich
T-stage ✓ ✓
N-stage ✓
Tumor size ✓
Fuhrman Grade ✓ ✓
Tumor necrosis ✓
ECOG PS ✓
Patient Subsets: Risk Score
Non-resectable or metastatic setting
Resectable diseaseTrials in poor risk pts
Trials in poor risk pts
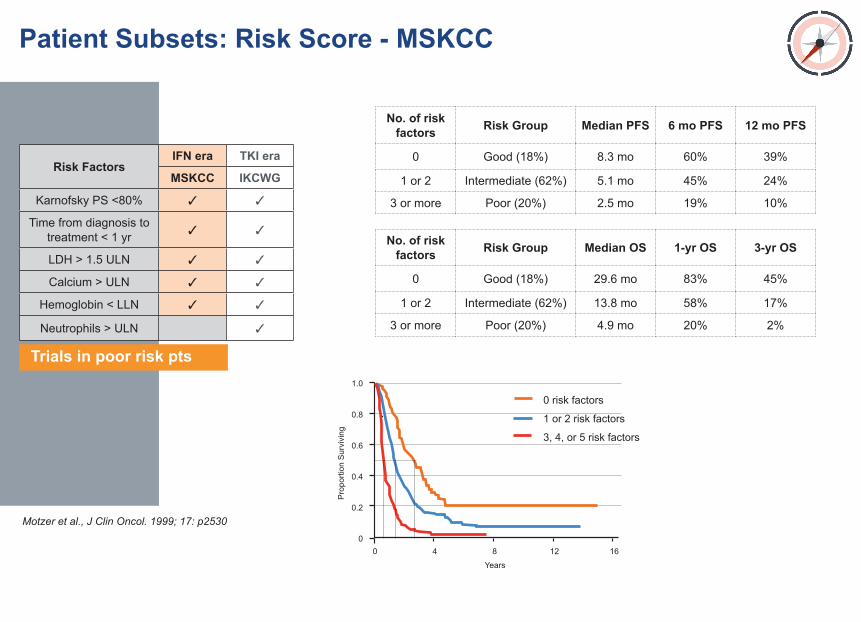
Risk FactorsIFN era TKI era
MSKCC IKCWG
Karnofsky PS <80% ✓ ✓
Time from diagnosis to treatment < 1 yr ✓ ✓
LDH > 1.5 ULN ✓ ✓
Calcium > ULN ✓ ✓
Hemoglobin < LLN ✓ ✓
Neutrophils > ULN ✓
No. of risk factors Risk Group Median PFS 6 mo PFS 12 mo PFS
0 Good (18%) 8.3 mo 60% 39%
1 or 2 Intermediate (62%) 5.1 mo 45% 24%
3 or more Poor (20%) 2.5 mo 19% 10%
No. of risk factors Risk Group Median OS 1-yr OS 3-yr OS
0 Good (18%) 29.6 mo 83% 45%
1 or 2 Intermediate (62%) 13.8 mo 58% 17%
3 or more Poor (20%) 4.9 mo 20% 2%
Patient Subsets: Risk Score - MSKCC
Trials in poor risk pts
Motzer et al., J Clin Oncol. 1999; 17: p25300
0.6
0.8
0.4
0.2
1.0
Years
0 124 8 16
0 risk factors
1 or 2 risk factors
3, 4, or 5 risk factors
Pro
porti
on S
urvi
ving
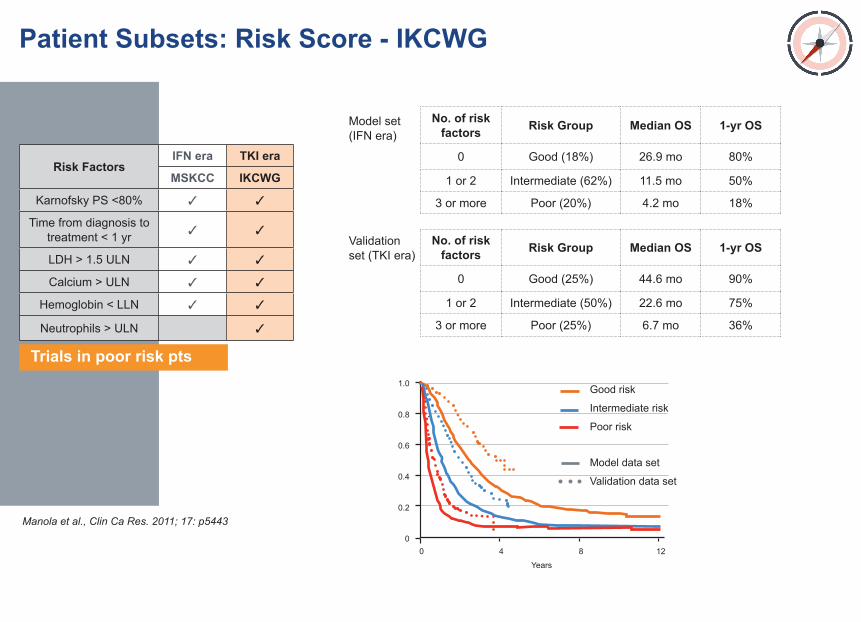
Risk FactorsIFN era TKI era
MSKCC IKCWG
Karnofsky PS <80% ✓ ✓
Time from diagnosis to treatment < 1 yr ✓ ✓
LDH > 1.5 ULN ✓ ✓
Calcium > ULN ✓ ✓
Hemoglobin < LLN ✓ ✓
Neutrophils > ULN ✓
No. of risk factors Risk Group Median OS 1-yr OS
0 Good (18%) 26.9 mo 80%
1 or 2 Intermediate (62%) 11.5 mo 50%
3 or more Poor (20%) 4.2 mo 18%
No. of risk factors Risk Group Median OS 1-yr OS
0 Good (25%) 44.6 mo 90%
1 or 2 Intermediate (50%) 22.6 mo 75%
3 or more Poor (25%) 6.7 mo 36%
Patient Subsets: Risk Score - IKCWG
Trials in poor risk pts
Manola et al., Clin Ca Res. 2011; 17: p54430
0.6
0.8
0.4
0.2
1.0
Years
0 4 8 12
Good risk
Intermediate risk
Poor risk
Model data set
Validation data set
Model set (IFN era)
Validation set (TKI era)
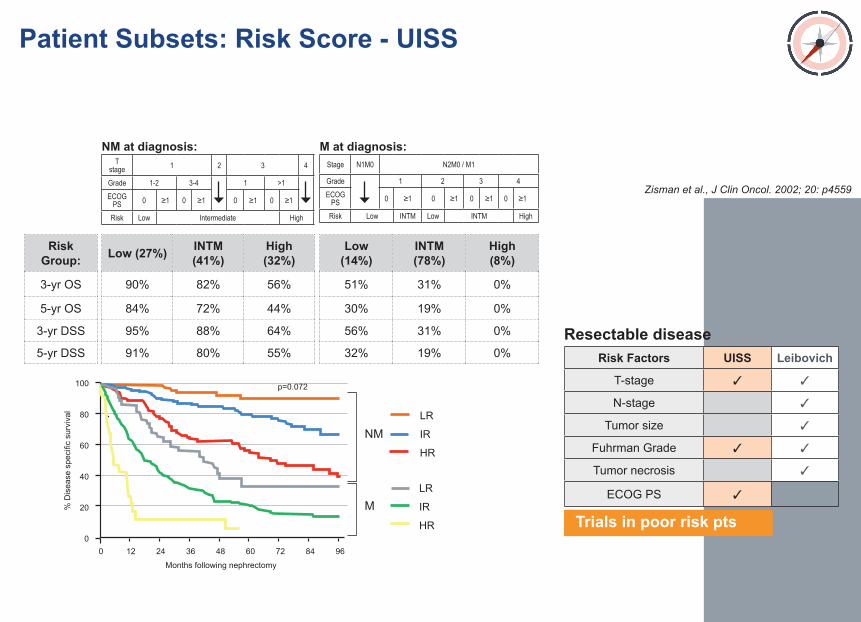
Risk Factors UISS Leibovich
T-stage ✓ ✓
N-stage ✓
Tumor size ✓
Fuhrman Grade ✓ ✓
Tumor necrosis ✓
ECOG PS ✓
Resectable disease
Trials in poor risk pts
Low (27%) INTM (41%)
High (32%)
90% 82% 56%
84% 72% 44%
95% 88% 64%
91% 80% 55%
Low (14%)
INTM (78%)
High (8%)
51% 31% 0%
30% 19% 0%
56% 31% 0%
32% 19% 0%
Risk Group:
3-yr OS
5-yr OS
3-yr DSS
5-yr DSS
968472600
60
80
40
20
100
Months following nephrectomy
0 2412 4836
LR
IR
HR
Patient Subsets: Risk Score - UISS
T stage 1 2 3 4
Grade 1-2 3-4 1 >1ECOG
PS 0 ≥1 0 ≥1 0 ≥1 0 ≥1
Risk Low Intermediate High
Stage N1M0 N2M0 / M1
Grade 1 2 3 4ECOG
PS 0 ≥1 0 ≥1 0 ≥1 0 ≥1
Risk Low INTM Low INTM High
NM at diagnosis: M at diagnosis:
NM
M LR
IR
HR
% D
isea
se s
peci
fic s
urvi
val
p=0.072
Zisman et al., J Clin Oncol. 2002; 20: p4559
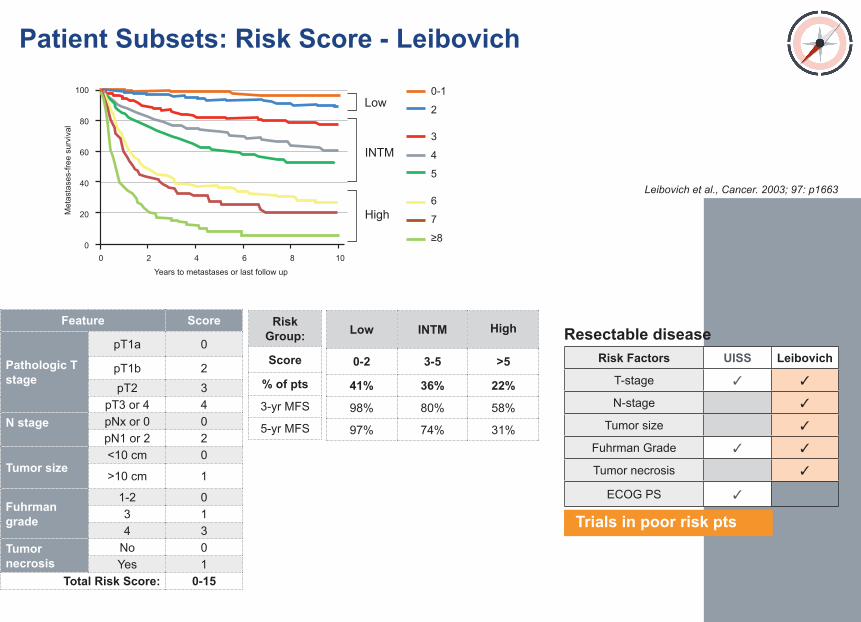
Risk Factors UISS Leibovich
T-stage ✓ ✓
N-stage ✓
Tumor size ✓
Fuhrman Grade ✓ ✓
Tumor necrosis ✓
ECOG PS ✓
Resectable disease
Trials in poor risk pts
Low INTM
High
0-2 3-5 >5
41% 36% 22%
98% 80% 58%
97% 74% 31%
Feature Score
Pathologic T stage
pT1a 0
pT1b 2pT2 3
pT3 or 4 4N stage pNx or 0 0
pN1 or 2 2
Tumor size<10 cm 0
>10 cm 1
Fuhrman grade
1-2 03 14 3
Tumor necrosis
No 0Yes 1
Total Risk Score: 0-15
Risk Group:
Score
% of pts
3-yr MFS
5-yr MFS
Patient Subsets: Risk Score - Leibovich
Leibovich et al., Cancer. 2003; 97: p1663
100
60
80
40
20
100
Years to metastases or last follow up
0 42 86
0-1
2Low
INTM
HighMet
asta
ses-
free
surv
ival
3
4
5
6
7
≥8
ITT intent to treatIU international unitsIV intravenousJAMA Journal of the American Medical AssociationJCO Journal of Clinical OncologyMab monoclonal antibodyMIU million international unitsMo monthMOA mechanism of actionMPA medroxyprogesterone acetate MRC Medical Research CouncilmRCC metastatic renal cell carcinomaMSKCC Memorial Sloan-Kettering Cancer Center mTOR mammalian target of rapamycinMU million unitsNCC non-clear cellNED no evidence of diseaseNEJM New England Journal of MedicineNS not shown (value not listed in reference)ORR overall response rateOS overall survivalPDGF Platelet-derived growth factorPFS progression free survivalPh phasePI principal investigatorPK pharmacokineticsPO per os (by mouth)PR partial response
1L first lineAE adverse event ALT alanine aminotransferaseASCO American Society of Clinical OncologyBID bis in die (twice a day)CALGB Cancer and Leukemia Group BCDD continuous daily dosingCI confidence intervalCIVI continuous intravenous infusionCR complete responseDFS disease free survivalECOG Eastern Cooperative Oncology GroupEFS event free survivalEMEA European Medicines Evaluation Agency ESMO European Society of Medical OncologyEU European UnionFDA Food and Drug AdministrationFGFR fibroblast growth factor receptorFLT-3 Fms-like tyrosine kinase 3GI gastrointestinalGr. gradeGS Gleason score HIF-1α hypoxia-inducible factor-1 alphaHR hazard ratiohrs hoursIFN interferon IL-2 interleukin-2
Glossary
PS performance statuspt patientq3w quaque 3 weeks (every 3 weeks) qd quaque daily (every day)QOL quality of life RCC renal cell carcinomaSD stable diseaseSOC standard of careSubq subcutaneousSQ subcutaneousTKI tyrosine kinase inhibitorTTP time to progressionUK United KingdomUS United StatesVEGF vascular endothelial growth factorVEGFR vascular endothelial growth factor receptorVHL Von Hippel-LindauWHO World Health Organizationwks weeksw.o. withoutyr year
DAVAOncology, LP...facilitating successful drug development





























