Embed Size (px)
Citation preview
On the frequency and reproducibility of orthostatic blood pressure changes in healthy community-dwelling elderly during 60-degree head-up tilt
The postural effects of 20 minutes of 60-degree head-up tilt on systolic, diastolic, and mean arterial blood pressures (BPs), heart rate, and rhythm were studied in 70 healthy, community-dwelling volunteer subjects of both sexes, divided into three age groups. Group A consisted of 30 subjects, with a mean age of 76 years (range 65 to 95 years); group B had 19 subjects, with a mean age of 54 years (range 45 to 64 years); and group C had 21 subjects, with a mean age of 33 years (range 24 to 44 years). To qualify, subjects had to have a systolic BP of 150 mm Hg or less and a diastolic BP of < 90 mm Hg, be taking no prescribed medications, have had no previous syncopal episodes, and have absence of any significant medical illness. Nine of 30 (30%) subjects in group A, 1 of 19 (5%) subjects in group B, and 2 of 21 (9.5%) subjects in group C exhibited asymptomatic postural drops in systolic blood pressure > 20 mm Hg (p < 0.05). The mean time for the systolic blood pressure drops in group A was 9.2 minutes. Results were reproducible upon retesting after 1 week. (AM HEART J 1993;126:184-188.)
Archana Patel, MD, Anne Maloney, and Anthony N. Damato, MD Jersey City, N.J.
Orthostatic hypotension is defined as a drop in systolic blood pressure > 20 mm Hg or a drop in diastolic blood pressure > 10 mm Hg upon the subject's assuming an upright position.^ The incidence of orthostatic hypotension in the elderly has been reported to vary between 4 % and 33 % .^'^^ Mader,^ in his review of this subject, has enumerated several possible reasons for this variability, which include: types of patients studied (inpatients versus outpatients); presence of coexisting diseases; use of medications by study subjects; baseline blood pressure criteria; methods of blood pressure measurements; and differing study protocols. Several investigators have noted a direct correlation between the presence of supine hypertension and the frequency of postural hypotension.^'^' ̂ "̂ *
In an attempt to better define the frequency of orthostatic hypotension in the older population, Mader et al.^ studied supine to standing blood pressure
From the Division of Cardiology and Geriatric Medicine, Department of Medicine, Jersey City Medical Center; and Seton Hall University School of Graduate Medical Education.
Received for publication Aug. 10, 1992; accepted Jan. 6, 1993.
Reprint requests: Anthony N. Damato, MD, Jersey City Medical Center, Jersey City, NJ 07304.
Copyright ® 1993 by Mosby-Year Book, Inc. 0002-8703/93/$1.00 + .10 4 / 1 / 4 6 2 8 8
changes in 300 community-dwelling elderly individuals (mean age 69.3 years) and found the overall incidence of postural hypotension to be 10.7%. However, in the group without risk factors, the prevalence was 6.4%, compared with 13.7% in the group with risk factors. Data from this and other reports have suggested that postural hypotension in older subjects is not a normal finding in the absence of identified risk factors and most often is the result of associated diseases or medications.^' '̂ ̂ ^ The present study was undertaken to determine postural changes to a 60-degree head-up tilt in a group of healthy, community-dwelling elderly persons and to compare these changes with those obtained in a group of young and middle-aged healthy individuals. Additionally, we proposed to test the reproducibility of our findings by restudying any individual with a postural drop of systolic blood pressure > 20 mm Hg after 1 week of the original study.
METHODS
Seventy normal, healthy, community-dwelling volunteers of both sexes were recruited for this study. There were 28 men and 42 women, whose ages ranged from 24 to 95 years. Subjects were divided into three age groups (see below). Patients were screened for the absence of systemic hypertension, other cardiovascular diseases, diabetes, pulmonary and renal diseases, neurologic diseases, lower
184
Volume 126, Number 1
American Heart Journal Patel, Maloney, and Damato 185
a: E E
A
Mean Values Systoiic BP
k T k
Supine 1
1 k
Time (min)
V, k
10 15 20 Supine
• Group A
0 Group B
O Group C
* p < 0.001
Mean Values Diastolic BP
I 40
fo ia JA li, fe fef^ i i
Supine 1 5 10 IS 20 Supine
Time (min)
• Group A O Group B H Group C » p < 0.001
X E E
Mean Values MABP
L u, k ik fa
Supine 1 20 Supine
Time (min)
• Group A Q Groups D Group C * p < 0 05
Mean Values for HR
^M^ '̂
Supme S 10 15 Time (min)
20 Supme
• Group A Q Groups @ Group C • p < 0.05
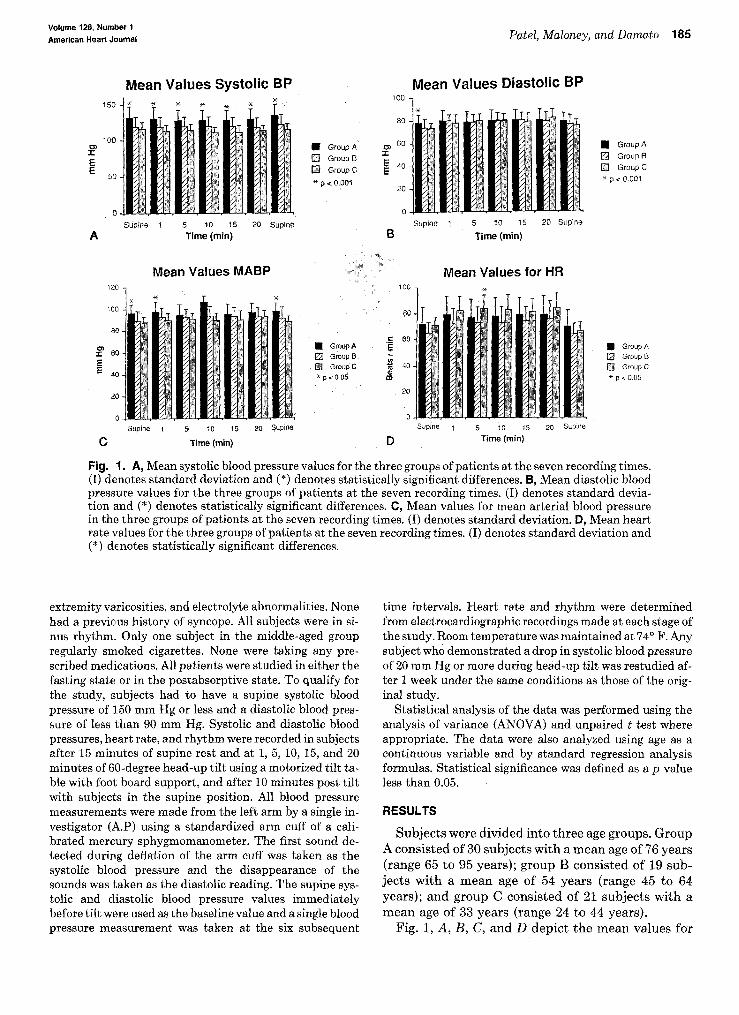
Fig. 1. A, Mean systolic blood pressure values for the three groups of patients at the seven recording times. (I) denotes standard deviation and (*) denotes statistically significant differences. B, Mean diastolic blood pressure values for the three groups of patients at the seven recording times. (I) denotes standard deviation and (*) denotes statistically significant differences. C, Mean values for mean arterial blood pressure in the three groups of patients at the seven recording times. (I) denotes standard deviation. D, Mean heart rate values for the three groups of patients at the seven recording times. (I) denotes standard deviation and (*) denotes statistically significant differences.
extremity varicosities, and electrolyte abnormalities. None had a previous history of syncope. All subjects were in sinus rhythm. Only one subject in the middle-aged group regularly smoked cigarettes. None were taking any prescribed medications. All patients were studied in either the fasting state or in the postabsorptive state. To qualify for the study, subjects had to have a supine systolic blood pressure of 150 mm Hg or less and a diastolic blood pressure of less than 90 mm Hg. Systolic and diastolic blood pressures, heart rate, and rhythm were recorded in subjects after 15 minutes of supine rest and at 1, 5, 10, 15, and 20 minutes of 60-degree head-up tilt using a motorized tilt table with foot board support, and after 10 minutes post tilt with subjects in the supine position. All blood pressure measurements were made from the left arm by a single investigator (A.P) using a standardized arm cuff of a calibrated mercury sphygmomanometer. The first sound detected during deflation of the arm cuff was taken as the systolic blood pressure and the disappearance of the sounds was taken as the diastolic reading. The supine systolic and diastolic blood pressure values immediately before tilt were used as the baseline value and a single blood pressure measurement was taken at the six subsequent
time intervals. Heart rate and rhythm were determined from electrocardiographic recordings made at each stage of the study. Room temperature was maintained at 74° F. Any subject who demonstrated a drop in systolic blood pressure of 20 mm Hg or more during head-up tilt was restudied after 1 week under the same conditions as those of the original study.
Statistical analysis of the data was performed using the analysis of variance (ANOVA) and unpaired t test where appropriate. The data were also analyzed using age as a continuous variable and by standard regression analysis formulas. Statistical significance was defined as a p value less than 0.05.
RESULTS
Subjects were divided into three age groups. Group A consisted of 30 subjects with a mean age of 76 years (range 65 to 95 years); group B consisted of 19 subjects with a mean age of 54 years (range 45 to 64 years); and group C consisted of 21 subjects with a mean age of 33 years (range 24 to 44 years).
Fig. 1, A, B, C, and D depict the mean values for
186 Patel, Maloney, and Damato July 1993
American Heart Journal
Table I. Mean changes during tilt
Group A Group B Group C
Mean systolic BP change (mm Hg)
Mean time for systolic BP change (min)
Mean heart rate change (beats/min)
Mean time for heart rate change (min)
Mean diastolic BP change (mm Hg)
Mean time for diastolic BP change (min)
Mean of mean BP change (min)
Mean time of mean BP change (min)
- 8 (+20 to -30)
8.1 (1 to 20)
+9.6 (+1 to +27)
7.4 (1 to 20)
+2.6 (+14 to -20)
9.4 (1 to 20)
+0.7 (+16 to -22)
10.6 (1 to 20)
-2 .9 (+14 to -22)
7.6 (1 to 20) +10.8
(+30 to -20) 10.4
(1 to 20) +8.8
(+20 to -4 ) 9.2
(1 to 20) +5.0
(+14 t o - 6 ) 9.9
(1 to 20)
- 6 (+10 to -24)
8.4 (1 to 20) +16.1
(+1 to +40) 8.8
(1 to 20) +7.8
(+1 to +20) 8.8
(1 to 20) +5.4
(+16 to - 9 ) 9.0
(1 to 20)
BP, Blood pressure; bracketed values are the ranges.
Table II. Decreases in systolic blood pressure greater than 20 mm Hg
Patient No.
3
15
18
22
23
24
26
27
30
Group A
Maximum decrease
Study 1&2
- 2 4 mm Hg - 2 4 mm Hg - 3 0 mm Hg - 2 0 mm Hg - 3 0 mm Hg - 2 4 mm Hg - 2 0 mm Hg - 3 0 mm Hg - 2 6 mm Hg - 3 4 mm Hg - 2 0 mm Hg - 2 0 mm Hg - 2 6 mm Hg - 2 2 mm Hg - 3 0 mm Hg
-22 mm Hg - 2 0 mm Hg
Time of maximum decrease
20 min 20 min
5 min 6 min
15 min 15 min
1 min 1 min
10 min 10 min
1 min 1 min 5 min 5 min
15 min
15 min 20 min
Patient No.
6
Group B
Maximum decrease
Study 1&2
-22 mm Hg - 2 0 mm Hg
Time of maximum decrease
20 min 20 min
Patient No.
20
21
Group C
Maximum decrease
Study 1&2
- 2 4 mm Hg - 1 6 mm Hg - 2 0 mm Hg -12 mm Hg
Time of maximum decrease
15 min 10 min 20 min 10 min
systolic, diastolic, and mean arterial pressures and heart rate, respectively. For all seven recording times, mean systolic blood pressures for group A were significantly higher than those for the other two groups (p < 0.001). Only the pre tilt supine mean diastolic blood pressure in group A was significantly higher (p < 0.001). Group A showed statistically significant increases in mean values of mean arterial blood pressures for the pre and post tilt supine periods and at the 1-minute tilt stage compared with groups B and
C. Group C had a statistically higher mean heart rate value at the 5-minute tilt period compared with the other two groups.
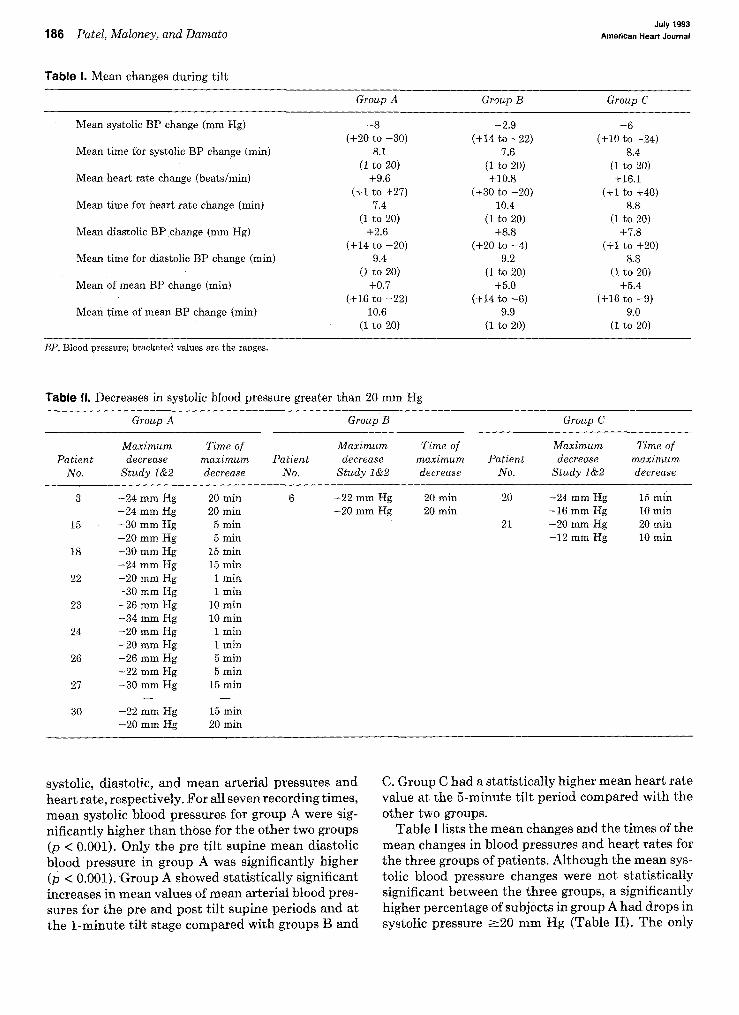
Table I lists the mean changes and the times of the mean changes in blood pressures and heart rates for the three groups of patients. Although the mean systolic blood pressure changes were not statistically significant between the three groups, a significantly higher percentage of subjects in group A had drops in systolic pressure >20 mm Hg (Table II). The only
Volume 126, Number 1
American Heart Journal Patel, Moloney, and Damato 187
significant changes were in the mean heart rate changes (group C changes were significantly higher [p < 0.02] than group A changes) and the mean diastolic blood pressure changes (group A changes were significantly less [p < 0.01] than group B and C changes).
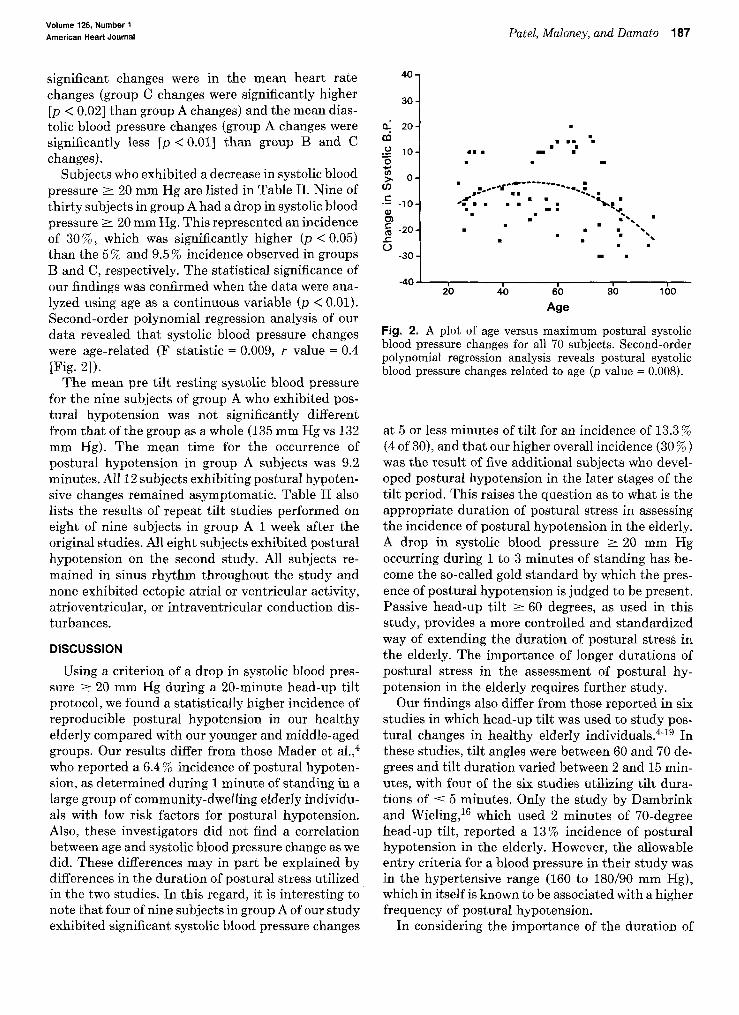
Subjects who exhibited a decrease in systolic blood pressure > 20 mm Hg are listed in Table II. Nine of thirty subjects in group A had a drop in systolic blood pressure > 20 mm Hg. This represented an incidence of 30%, which was significantly higher (p < 0.05) than the 5 % and 9.5 % incidence observed in groups B and C, respectively. The statistical significance of our findings was confirmed when the data were analyzed using age as a continuous variable (p < 0.01). Second-order polynomial regression analysis of our data revealed that systolic blood pressure changes were age-related (F statistic = 0.009, r value = 0.4 [Fig. 2]).
The mean pre tilt resting systolic blood pressure for the nine subjects of group A who exhibited postural hypotension was not significantly different from that of the group as a whole (135 mm Hg vs 132 mm Hg). The mean time for the occurrence of postural hypotension in group A subjects was 9.2 minutes. All 12 subjects exhibiting postural hypotensive changes remained asymptomatic. Table II also lists the results of repeat tilt studies performed on eight of nine subjects in group A 1 week after the original studies. All eight subjects exhibited postural hypotension on the second study. All subjects remained in sinus rhythm throughout the study and none exhibited ectopic atrial or ventricular activity, atrioventricular, or intraventricular conduction disturbances.
DISCUSSION
Using a criterion of a drop in systolic blood pressure > 20 mm Hg during a 20-minute head-up tilt protocol, we found a statistically higher incidence of reproducible postural hypotension in our healthy elderly compared with our younger and middle-aged groups. Our results differ from those Mader et al.,* who reported a 6.4% incidence of postural hypotension, as determined during 1 minute of standing in a large group of community-dwelling elderly individuals with low risk factors for postural hypotension. Also, these investigators did not find a correlation between age and systolic blood pressure change as we did. These differences may in part be explained by differences in the duration of postural stress utilized in the two studies. In this regard, it is interesting to note that four of nine subjects in group A of our study exhibited significant systolic blood pressure changes
40
30
20
y 10-
0. cd o
•5
t 0 w e -10 <u
ra -20 sz O
-30
-40 20 40
1
60 Age
— I — 80 100
Fig. 2. A plot of age versus maximum postural systolic blood pressure changes for all 70 subjects. Second-order polynomial regression analysis reveals postural systolic blood pressure changes related to age (p value = 0.008).
at 5 or less minutes of tilt for an incidence of 13.3% (4 of 30), and that our higher overall incidence (30 %) was the result of five additional subjects who developed postural hypotension in the later stages of the tilt period. This raises the question as to what is the appropriate duration of postural stress in assessing the incidence of postural hypotension in the elderly. A drop in systolic blood pressure > 20 mm Hg occurring during 1 to 3 minutes of standing has become the so-called gold standard by which the presence of postural hypotension is judged to be present. Passive head-up tilt > 60 degrees, as used in this study, provides a more controlled and standardized way of extending the duration of postural stress in the elderly. The importance of longer durations of postural stress in the assessment of postural hypotension in the elderly requires further study.
Our findings also differ from those reported in six studies in which head-up tilt was used to study postural changes in healthy elderly individuals.''"^^ In these studies, tilt angles were between 60 and 70 degrees and tilt duration varied between 2 and 15 minutes, with four of the six studies utilizing tilt durations of < 5 minutes. Only the study by Dambrink and Wieling,^^ which used 2 minutes of 70-degree head-up tilt, reported a 13% incidence of postural hypotension in the elderly. However, the allowable entry criteria for a blood pressure in their study was in the hypertensive range (160 to 180/90 mm Hg), which in itself is known to be associated with a higher frequency of postural hypotension.
In considering the importance of the duration of
188 Patel, Maloney, and Damato July 1993
American Heart Journal
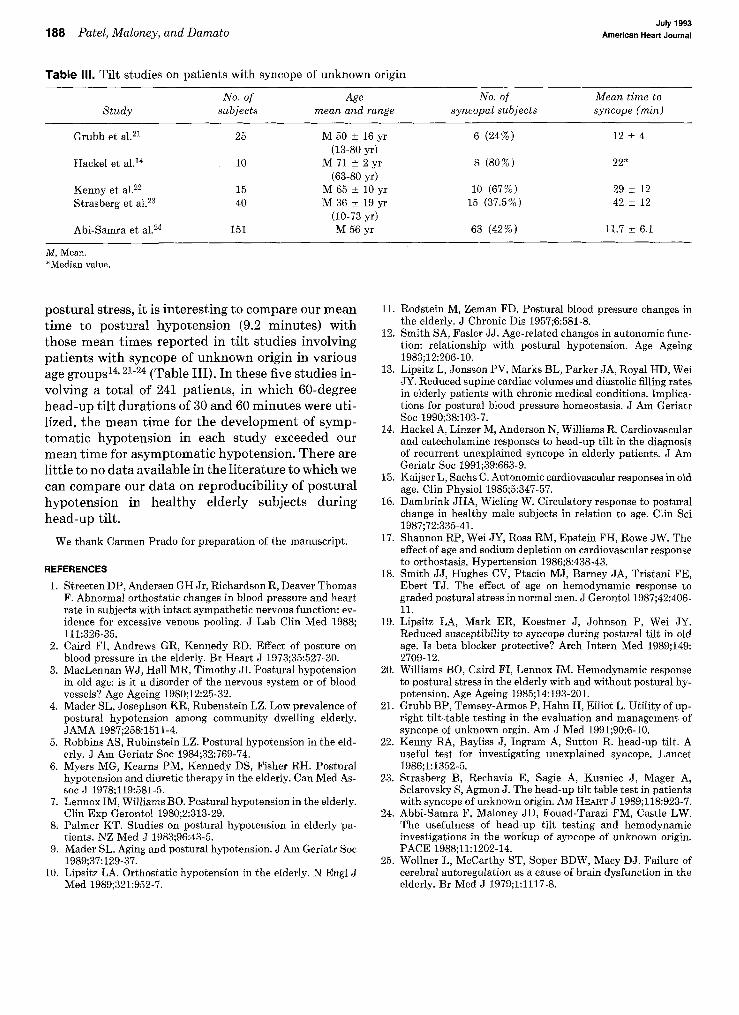
Table III. T i l t s tud ies on p a t i e n t s wi th syncope of u n k n o w n origin
Study
Grubb et al.^i
Hackel et a l . "
Kenny et al.^^ Strasberg et al.^^
Abi-Samra et al .^
No. of subjects
25
10
15 40
151
Age mean and range
M 50 ± 16 yr (13-80 yr)
M 71 ± 2 yr (63-80 yr)
M 65 ± 10 yr M 36 ± 19 yr
(10-73 yr) M 5 6 y r
No. of syncopal subjects
6 (24%)
8 (80%)
10 (67%) 15 (37.5%)
63 (42%)
Mean time to syncope (min)
12 ± 4
22*
29 ± 12 42 ± 12
11.7 ± 6.1
M, Mean. •Median value.
postural stress, it is interesting to compare our mean time to postural hypotension (9.2 minutes) with those mean times reported in tilt studies involving patients with syncope of unknown origin in various age groups^^' ̂ "̂̂ * (Table III). In these five studies involving a total of 241 patients, in which 60-degree head-up tilt durations of 30 and 60 minutes were utilized, the mean time for the development of symptomatic hypotension in each study exceeded our mean time for asymptomatic hypotension. There are little to no data available in the literature to which we can compare our data on reproducibility of postural hypotension in healthy elderly subjects during head-up tilt.
We thank Carmen Prado for preparation of the manuscript.
REFERENCES
1. Streeten DP, Andersen GH Jr, Richardson R, Deaver Thomas F. Abnormal orthostatic changes in blood pressure and heart rate in subjects with intact sympathetic nervous function: evidence for excessive venous pooling. J Lab Clin Med 1988; 111:326-35.
2. Caird FI, Andrews GR, Kennedy RD. Effect of posture on blood pressure in the elderly. Br Heart J 1973;35:527-30.
3. MacLennan WJ, Hall MR, Timothy JI. Postural hypotension in old age: is it a disorder of the nervous system or of blood vessels? Age Ageing 1980;12:25-32.
4. Mader SL, Josephson KR, Rubenstein LZ. Low prevalence of postural hypotension among community dwelling elderly. JAMA 1987;258:1511-4.
5. Robbins AS, Rubinstein LZ. Postural hypotension in the elderly. J Am Geriatr Soc 1984;32:769-74.
6. Myers MG, Kearns PM, Kennedy DS, Fisher RH. Postural hypotension and diuretic therapy in the elderly. Can Med Assoc J 1978;119:581-5.
7. Lennox IM, Williams BO. Postural hypotension in the elderly. Clin Exp Gerontol 1980;2:313-29.
8. Palmer KT. Studies on postural hypotension in elderly patients. NZ Med J 1983;96:43-5.
9. Mader SL. Aging and postural hypotension. J Am Geriatr Soc 1989;37:129-37.
10. Lipsitz LA. Orthostatic hypotension in the elderly. N Engl J Med 1989;321:952-7.
11. Rodstein M, Zeman FD. Postural blood pressure changes in the elderly. J Chronic Dis 1957;6:581-8.
12. Smith SA, Fasler JJ . Age-related changes in autonomic function: relationship with postural hypotension. Age Ageing 1983;12:206-10.
13. Lipsitz L, Jonsson PV, Marks BL, Parker JA, Royal HD, Wei JY. Reduced supine cardiac volumes and diastolic filling rates in elderly patients with chronic medical conditions. Implications for postural blood pressure homeostasis. J Am Geriatr Soc 1990;38:103-7.
14. Hackel A, Linzer M, Anderson N, Williams R. Cardiovascular and catecholamine responses to head-up tilt in the diagnosis of recurrent unexplained syncope in elderly patients. J Am Geriatr Soc 1991;39:663-9.
15. Kaijser L, Sachs C. Autonomic cardiovascular responses in old age. Clin Physiol 1985;5:347-57.
16. Dambrink JHA, Wieling W. Circulatory response to postural change in healthy male subjects in relation to age. Clin Sci 1987;72;335-41.
17. Shannon RP, Wei JY, Rosa RM, Epstein FH, Rowe JW. The effect of age and sodium depletion on cardiovascular response to orthostasis. Hypertension 1986;8:438-43.
18. Smith JJ , Hughes CV, Ptacin MJ, Barney JA, Tristani FE, Ebert TJ. The effect of age on hemodynamic response to graded postural stress in normal men. J Gerontol 1987;42:406-11.
19. Lipsitz LA, Mark ER, Koestner J, Johnson P, Wei JY. Reduced susceptibility to syncope during postural tilt in old age. Is beta blocker protective? Arch Intern Med 1989;149: 2709-12.
20. Williams BO, Caird FI, Lennox IM. Hemodynamic response to postural stress in the elderly with and without postural hypotension. Age Ageing 1985;14:193-201.
21. Grubb BP, Temsey-Armos P, Hahn H, Elliot L. Utility of upright tilt-table testing in the evaluation and management of syncope of unknown orgin. Am J Med 1991;90:6-10.
22. Kenny RA, Bayliss J, Ingram A, Sutton R. head-up tilt. A useful test for investigating unexplained syncope. Lancet 1986;1:1352-5.
23. Strasberg B, Rechavia E, Sagie A, Kusniec J, Mager A, Sclarovsky S, Agmon J. The head-up tilt table test in patients with syncope of unknown origin. A M HEAET J 1989;118:923-7.
24. Abbi-Samra F, Maloney JD, Fouad-Tarazi FM, Castle LW. The usefulness of head-up tilt testing and hemodynamic investigations in the workup of syncope of unknown origin. PACE 1988;11:1202-14.
25. WoUner L, McCarthy ST, Soper BDW, Macy DJ. Failure of cerebral autoregulation as a cause of brain dysfunction in the elderly. Br Med J 1979;1:1117-8.