Embed Size (px)
Citation preview

On the CUSP: Stop CAUTI in ICU National Content Webinar
Today’s Topic:
Urine Culture Practices in the ICU; Antibiotic Stewardship; Practical ICU Tools; Using Results from
the Safety Culture Surveys
Access slides of today’s webinar on the national project website:
http://www.onthecuspstophai.org/on-the-cuspstop-cauti/cohort-9-icu-initiative/
1

Webinar Evaluation
Your feedback is important!Please take a moment to fill out an evaluation
of today’s webinar:
http://www.cvent.com/d/xrqmmq

Today’s Presenters
Mohamad Fakih, MD, MPH
Medical Director, Infection Prevention and Control
St John Hospital and Medical Center
Professor of Medicine,
Wayne State University School of Medicine
Detroit, MI
Pat Posa, RN, BSN, MSA, FAAN
System Performance Improvement Leader
St. Joseph Mercy Hospital3

Today’s Presenters
William Miles, MD, FACS, FCCM, FAPWCA
Director of Surgical Critical Care
Clinical Professor of Surgery
University of North Carolina, Chapel Hill-Charlotte Campus
Carolinas Medical Center
Surgical Trauma ICU
Misty Wheeler, RN, NE-BC, CCRN
Lacey Spangler, RN, BSN, RN, CCRN
Neurosurgical ICU
Julia Retelski, MSN, RN, CCRN, SCRN, CCNS4

Improving the Culture of Culturing (aka, Culturing Stewardship)
Mohamad Fakih, MD, MPH
Medical Director, Infection Prevention and Control
St John Hospital and Medical Center
Professor of Medicine,
Wayne State University School of Medicine
Detroit, MI
5

6
Polling #1
A 45 year old male who is an active intravenous drug user is admitted with fever of 103°F, confusion and respiratory distress. The patient is intubated and admitted to the intensive care unit; the CXR shows multiple pulmonary emboli and the blood cultures grow methicillin resistant Staphylococcus aureus. On day 3, he is still febrile with a temperature of 101.8°F. His blood cultures are still growing gram-positive cocci and the patient has a urinary catheter since intensive care unit admission.
1. Urine culture2. No urine culture3. N/A – HRET Staff

7
Polling #2
A 73 year old patient with prostatic hypertrophy was admitted to the hospital with abdominal discomfort. On admission, he was afebrile with normal vital signs and blood white cell count. A bladder scan showed a significantly distended urinary bladder. A urinary catheter was placed and 1200 ml of urine was drained. His abdominal pain improved and he did not complain of any respiratory symptoms. The patient spiked a fever of 102°F the next day. His blood pressure was 100 systolic and heart rate 110.
1. Urine culture2. No urine culture3. N/A – HRET Staff

8
Clinical Evaluation
The clinical evaluation of the patient is key to best care, and the optimal use
of tests

Bacteriuria with Catheter Use(Garibaldi et al, Infect Control 1982; 3: 466-70)
Daily bacteriologic monitoring of 1140 cases: • Bacteriuria at insertion: 99/1,140 (8.7%)
catheterizations• 1,041 had no colonization at insertion, 433
removed within 24 hours• Of 608 catheterizations >24 hours, 76 (12.5%)
developed bacteriuria• Risk of bacteriuria was 3% per catheter-day
9

10
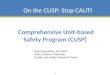
Picture of Routes of Entry
Maki and Tambyah, Emerg Infect Dis 2001; 7: 1-6

11
Catheter Associated Bacteriuria in ICU(Clec’h et al, Infect Control Hosp Epidemiol 2007; 28: 1367-73)
• 12 ICUs: weekly urine cultures or if symptoms in catheterized patients
• CAUTI defined as urine culture >103 CFU/ml• CAUTI (bacteriuria) rate= 12.9/ 1000 catheter-days• Median time to CAUTI 11 days (range 6-19 days)• Median ICU LOS longer for those with CAUTI (28
days) vs. those without (7 days)

Common Inappropriate Triggers For Urine Culture In Patients With Urinary Catheters
• Urine color, consistency and smell• Pyuria
12

Resident Physicians (N=106) and Nurses (N=159): Triggers For Cultures In Catheterized Patients
(Sibai et al, ID Week 2013, presentation 205 )
Trigger for Urine Culture
Resident Physicians (Answered Yes)
Nurses(Answered Yes)
Foul smelling urine 75 (70.8%) 146 (94.8%)Cloudy urine 84 (79.2%) 146 (94.8%)Sediments in urine 57 (53.8%) 129 (84.3%)Darker urine 39 (36.8%) 72 (47.7%)Chronic UC on admission
46 (43.4%) 115 (74.2%)
All of the above should NOT trigger a urine culture in catheterized patients!13

Resident Physicians and Pyuria: Obtain A Urine Culture In Catheterized Patients
(Sibai et al, ID Week 2013, presentation 205 )
Trigger for Urine Culture Answered Yes
Urine WBC 25 cells 71 (67%)
Urine WBC 100 cells 94 (88.7%)
Urine WBC 500 cells 101 (95.3%)
Pyuria in an asymptomatic patient with an indwelling urinary catheter should not be a
trigger for culture or antimicrobials
14

Pyuria Is Not Diagnostic Of CAUTI(Hooton, Clin Infect Dis 2010; 50:625–663)
• Pyuria does NOT help differentiate asymptomatic bacteriuria from CAUTI
• Pyuria + bacteria ≠ CAUTI
15

16
Pyuria and Bacteriuria(Tambyah, Arch Intern Med. 2000;160:673-677)
• 761 patients with newly inserted catheters, 10.8% developed bacteriuria or candiduria
• Defined bacteriuria as >103 CFUs.• Women had more bacteriuria (21.2%) than
men (7.2%)

17
Pyuria and Bacteriuria(Tambyah, Arch Intern Med. 2000;160:673-677)
Pyuria more common with bacteriuria related to gram negatives than gram positives or funguria

18
Pyuria and Bacteriuria(Tambyah, Arch Intern Med. 2000;160:673-677)
Pyuria cannot predict bacteriuria

Absence of Pyuria (Hooton, Clin Infect Dis 2010; 50:625–663)
• IDSA guidelines: “The absence of pyuria in a symptomatic patient suggests a diagnosis other than CA-UTI”
19

20
Color or Odor(Hooton, Clin Infect Dis 2010; 50:625–663)
• IDSA guidelines:“In the catheterized patient, the presence or absence of odorous or cloudy urine alone should not be used to differentiate CA-ASB from CA-UTI or as an indication for urine culture or antimicrobial therapy.”

21
Screening Urine Cultures!!
The practice: “screening culture on admission”, “standing orders” or “reflex orders” for urine cultures based on urinalysis results 1. May not help the hospital avoid non-
reimbursement2. May increase utilization of additional
resources (testing, antibiotics, consults)3. May adversely affect patients by exposing
them to inappropriate testing and treatments

PRE-PRINTED ORDERSFOLEY CATHETER PROTOCOL
22

23
How to Reduce Unnecessary Urine Cultures
1. Evaluate current processes for obtaining urine cultures (avoid automatic triggers or screening cultures with no appropriate indications)
2. Evaluate practice patterns (avoid PAN culturing)
3. Provide education on when it is appropriate to obtain urine cultures

24
How to Reduce Unnecessary Urine Cultures
4. Have periodic audits on urine culture use in the intensive care units to look for trends
5. Promote appropriate urinary catheter use to reduce risk of bacteriuria/ funguria

Discourage Urine Culture Use
25

Appropriate Urine Culture Use
26

Key Points Related to Obtaining Urine Cultures
http://www.onthecuspstophai.org/on-the-cuspstop-cauti/toolkits-and-resources/additional-resources/27

28
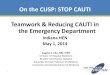
Culturing Stewardship and Other Preventative Measures: Large Hospital ICUs
Jul-Sep13 Oct-Dec13 Jan-Mar14 Apr-Jun14 Jul-Sep14 Oct-Dec140
0.5
1
1.5
2
2.5
CAUTI SIR for 50 Adult ICU Beds
CAUTI SIR
Influenza epidemic (more fever, more cultures)
ICU team only responsible for urine culture ordering

Antibiotic Stewardship in the ICU
William Miles, MD, FACS, FCCM, FAPWCA
Director of Surgical Critical Care
Clinical Professor of Surgery
University of North Carolina, Chapel Hill-Charlotte Campus
Carolinas Medical Center

Disclosures
Nothing to disclose
30

Antibiotic Stewardship in the ICU
Some Points to Consider• Resistance to antibiotics exists in nature before
medicine actually discovers or uses them• Antibiotics have societal impacts• Pressure from antibiotic mismanagement forces
significant resistance• 70% of antibiotics in America go to Food
production
31

Antibiotic Stewardship in the ICU
Antimicrobial Treatment Considerations
• Must be timely: any delay in starting them increases mortality significantly
• Appropriate: must cover spectrum of pathogens• Pharmacokinetics: adequate dose and intervals• Narrowing and Discontinuation: based on clinical
data, ICU microbiology data, and clinical response
32

Antibiotic Stewardship
33

Antibiotic Stewardship in the ICU
Novel Antibiotic Development
• 1980’s: 16 new antibiotics released• 1990’s: 10 new antibiotics released• 2000’s: 5 new antibiotics released
• 2008-2012: ONLY 1 new antibiotic developed!
34

Antibiotic Stewardship in the ICU
What is Antimicrobial Stewardship
• Systematic approach to optimize clinical outcomes while minimizing consequence of antibiotic use:– Toxicity– Selection of Resistance– Selection of virulent organisms– C. diff resistance
• Combine with infection control practices to limit emergence and transmission of resistance
• Reduces healthcare costs without impacting care• Patient safety!
Dellit T et al Clin Infect Dis 2007; 44:15935

Antibiotic Stewardship
• IDSA• Joint Commission• CMS-California mandate• CDC• Physician Leadership Forum• ATS /ACCP/SCCM

Antibiotic Stewardship in the ICU
Goals of Antibiotic Stewardship
Combat the Emergence
of resistance
Control CostsImprove Clinical
Outcomes
37

Antibiotic Stewardship in the ICU
Stewardship StrategiesPatient Evaluation Education/Guidelines
Choice of Antimicrobial Formulary Restrictions
Prescription OrderingComputer assisted strategies
Dispensing AntimicrobialReview and Feedback-includes all
38

Antibiotic Stewardship in the ICU
Economic Considerations for Antibiotic Stewardship
• Antibiotic use restriction and costs should not be the only focus
• Antibiotic costs are a small percentage of treatment costs
• Costs from hospital LOS, total Healthcare costs and Infection Prevention should be considered
• Patients’ Quality and return to a functional life
39

Antibiotic Stewardship in the ICU
Prescribing Antibiotics
• Day 1: Empiric Antibiotics– Based on disease and ICU’s biogram
• Day 3: Narrowing/De-escalation– Based on culture results– Infection vs. leukocytosis– What is clinical picture– Base it on Antibiogram of unit
40

Antibiotic Stewardship in the ICU
• Antimicrobial Stewardship Principles important
• Utilize Pharm D, Infection Preventionist
• Prevent MDROs
41

Antibiotics in UTI
• Pyuria either in the setting of negative urine cultures or in patients with asymptomatic bacteriuria usually requires no treatment. If pyuria persists consider other causes (e.g. interstitial nephritis or cystitis, fastidious organisms).
• Follow-up urine cultures or U/A are only warranted for ongoing symptoms. They should NOT be acquired routinely to monitor response to therapy.
• The prevalence of asymptomatic bacteriuria is high: 1%-5% in premenopausal women, 3%-9% in postmenopausal women, 40%-50% in long-term care residents and 9%-27% in women with diabetes.
http://www.hopkinsmedicine.org/amp/guidelines/Antibiotic_guidelines.pdf-2015
42

Duration UTI Treatment
• The duration of treatment has not been well studied for CA-UTI and optimal duration is not known.
• 7 days if prompt resolution of symptoms• 10–14 days if delayed response• 3 days if catheter removed in female patient </= 65 years
with lower tract infection.
http://www.hopkinsmedicine.org/amp/guidelines/Antibiotic_guidelines.pdf-2015
43

Treatment Notes UTI
• Remove the catheter whenever possible• Replace catheters that have been in >/= 2 weeks if still indicated
• Prophylactic antibiotics at the time of catheter removal or replacement are NOT recommended due to low incidence of complications and concern for development of resistance.
• Catheter irrigation should not be used routinely
http://www.hopkinsmedicine.org/amp/guidelines/Antibiotic_guidelines.pdf-2015
44

Antibiotic Stewardship
Must coincide with Infection Control/Prevention• Prevention
– Optimal management of urinary catheters
• Control– Hand hygiene– Contact precautions– Active surveillance– Education– Environmental Cleaning Standards– Improved Communication between Facilities
www.cdc.gov45

As The Wheels Turn
Antibiotic Stewardship
Micro Lab
Providers
Pharmacy
QI/QA
PATIENTS
Infection Control
46

Multi-Drug Resistant Organisms
• CRE• MRSA• C Diff Colitis• All possible in ICU management and prolonged
urinary catheter and long term antibiotic use• Antibiotic stewardship and Urinary Catheter
removal protocols are essential tools for prevention of MDROs
47

Antibiotic Stewardship
48

Practical Implementation of Antibiotic Stewardship
2 ICUs Work In Implementing Antibiotic Stewardship And Appropriate Urinary Culturing
49

Practical Implementation of Proper Culturing2 ICUs Experience
Surgical Trauma ICUMisty Wheeler, RN, NE-BC, CCRNLacey Spangler, RN, BSN, RN, CCRN
Neurosurgical ICUJulia Retelski, MSN, RN, CCRN, SCRN, CCNS
50

51
Carolinas Medical CenterSurgical Trauma ICU
• Carolinas Medical Center is part of Carolinas HealthCare System in Charlotte, NC
• 874 licensed beds, quaternary referral hospital• Level 1 Trauma Center, Largest teaching hospital
in NC
Surgical-Trauma ICUNeurosurgical ICU
• 29 bed multispecialty trauma and surgical unit including transplant and immunotherapy patients
• 29 bed multispecialty Neurology and Neurosurgical unit

52
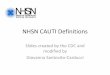
Surgical-Trauma ICU CAUTI Reduction 2014-2015
Jan Feb Mar Apr May Jun July Aug Sept Oct Nov Dec Jan Feb Mar0
1
2
3
4
5
6
7
8
9
# of
CAU
TIs
Daily UCP/Nec audits and IUC care focus
Urine Culture Initia-tive

53
NSICU CAUTI Reduction 2014-2015

54
ICU Urine Culture Initiatives
• Oct. 2014 – Do not PAN Culture, culture based on patient clinical picture
• Nov. 2014– Correct Order Entry for Source by Provider and support for nursing
to change order if necessary – Education for correct urine collection
• Preservative tube, DO NOT use specimen cup
– Send Urinalysis prior to sending culture– Lab and nursing policy rewritten
• Feb. 2015– Lab to reject cultures not sent in correct tube
• March 2015– Lab to complete Reflex Testing on Urine Specimen

Antibiotic Stewardship
Conclusions• Providers need better tools on how to initiate and
terminate antibiotics• Stewardship teams are just 1 step to regulate antibiotic
prescribing• Start based on national standards and Institutional
Antibiograms• De-escalate/narrow agents ASAP• Stop Antimicrobials based on clinical picture and do NOT
use Football Scores to decide length of treatment
55

Antibiotic Stewardship and Proper Culturing
• They go hand in hand• Synergy with Teamwork• With team effort and following CUSP CAUTI
Policies and Guidelines can be achieved
56

Safety Culture:Interpreting the Results
Pat Posa, RN, BSN, MSA, FAAN
System Performance Improvement Leader
St. Joseph Mercy Hospital
57

58
What is a Culture?
Represents a set of shared attitudes, values, goals, practices and behaviors that makes
one until distinct from the next.
Unspoken, implicit, taken for grantedLargely invisible
Measure culture at the unit level

Institute of Medicine
“ The biggest challenge to moving toward a safer health system is changing the culture from one of blaming individuals for errors to one in which errors are treated not as personal failures, but as opportunities to improve the system and prevent harm”
59

A Positive Culture of Safety
…..recognizes the inevitability of error and proactively seeks to identify latent threats
Nieva, V F Qual Saf Health Care 2003;12(suppl)60

Chaos, Culture, and Predictability
• Improve predictability = less chaos = better safety– Standardized interactions, checklists, familiarity
• Reduce predictability = more chaos = worse safety– New Manager, New Location, New Technology
61

Why Measure Unit Culture?
• Determine how bedside staff are feeling related to communication and recognizing defects– Diagnose and assess the current status of patient safety culture.– Identify strengths and areas for patient safety culture improvement.– Examine trends in patient safety culture change over time.– Measure/evaluate the cultural impact of patient safety initiatives and
interventions.
• CUSP is the intervention that will help you improve culture results
62

Survey Action Planning
Assessment data is likely to point to many different area of culture that can be improved
There will be many different ideas regarding potential actions
Incremental changes can be implemented and tested on a small scale, changing one process or practice at a time
Remember—in patient safety this is no one “silver bullet”
63

64
Safety Culture Drill Down
• If low on teamwork – what pulled the score down?– Difficulty Speaking Up– Breakdowns in Interdisciplinary Care Coordination– Difficulty Resolving Conflicts– Difficulty Asking Questions
• If low on safety norms – what pulled the score down?– Lack of trust– Lack of feedback– Lack of engagement

Changing the Culture Related to CAUTI
• Belief that any harm is not acceptable: – If this is present it will show up in categories of ‘non punitive
response to error’ and ‘feedback and communication about error’• Mindfully choose interventions:
– Don’t do things because “it is always how we have done it here” IE: pan culturing for any fever; indwelling urinary catheter in place because they are in the ICU
– Interdisciplinary discussion of risk vs benefit of starting antibiotics --- not just a routine, but thoughtful decisions
– This requires good interdisciplinary communication between team where each member of the healthcare team input is heard and valued
65

Teamwork Climate is the Consensus of Frontline Caregiver Assessments Related to Collaboration
Example Teamwork Climate Scale Items: • In this clinical area, it is difficult to speak up if
I perceive a problem with patient care• Disagreements in this clinical area are
resolved appropriately (i.e. not who is right, but what is best for the patient)
• The physicians and nurses here work together as a well-coordinated team
66

Safety Culture Debriefing
• Review results with staff• One strategy is to focus on:
– 5 areas with the most positive results– 5 areas with the most opportunities
67

Summarize 5 MOST Positive
Supervisor/manager expectations/actions promoting safetyConsiders staff suggestions for improving pt safety-76%*My supervisor overlooks pt safety problems that happen
over and over—76% disagree Organizational Learning—Continuous Improvement
We are actively doing things to improve patient safety-80% Teamwork
People support one another in this unit-86%When a lot of work needs to be done quickly, we work together as a team-85% In this unit, people treat each other with respect-78%
68

Summarize 5 LEAST Positive
Communication Openness Staff feel free to question the decisions or actions of those with more
authority-39% Feedback and Communication about Error
We are given feedback about changes put into place based on event reports—46%
Nonpunitive Response to Error *Staff feel like their mistakes are held against them—46% disagree *When an event is reported, it feels like the person is being written
up, not the problem—43% disagree *Staff worry that mistakes they make are kept in their personnel file-
33% disagree
69

Summarize 5 least Positive
Hospital Handoffs and transitions*Things “fall between the cracks” when transferring
patients from one unit to another-33% disagree*Problems often occur in the exchange of information
across hospital units-38% disagree Teamwork Across Hospital Units
*Hospital units do not coordinate well with each other-39% disagree
70

Evidence Based Local Solutions: Teamwork “If-Then”
If staffing levels inadequate/info lost at shift change: Then Morning/Shift Briefings
If interdisciplinary patient management issues: Then Daily Goals
If conflicts unresolved/role clarity lacking: Then Shadowing Exercise
If difficulty speaking up: Then standardizing with SBAR or Critical Language
71

Evidence Based Local Solutions:Safety “If-Then”
If staff lack consensus about quality and safety issues? Then educate on the science of safety
If staff feel unengaged in safety and quality?Then build grassroots with Learning from Defects
If staff feel unengaged, unsafe, & unresourced for quality?
Then build infrastructure & capacity with Psychological Safety and Executive Partnerships
72

Questions?
Your feedback is important!Please take a moment to fill out an evaluation
of today’s webinar:
http://www.cvent.com/d/xrqmmq