Embed Size (px)
Citation preview
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | II
ON-ROAD VERSUS OFF-ROAD
MOTORCYCLE ACCIDENTS IN
WESTERN AUSTRALIA
Steven J.G. Leeuwerke Master’s thesis Medicine
Student number: s1727044
Period: September 2013 – April 2014
Institutions and supervisors:
Department of Orthopaedic and Trauma Surgery of the Royal Perth Hospital, Western Australia Professor René Zellweger, MD, FRACS, FACS
Doctor Manimaran Sinnathamby, MBBS
University Medical Centre Groningen, Groningen, the Netherlands Miss Inge H.F. Reininga, PhD
Doctor Roeland H. den Boer, MD
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | I
Foreword After months of hard work, the end result is finally there: a comprehensive report on 180
cases of motorcycle accidents that were reviewed or admitted by the trauma team in the Royal
Perth Hospital (RPH) between 18 September 2013 and 5 March 2014. Up to 50% of all
motorcycle accidents have been reported to occur off-road and yet, most literature and
prevention campaigns are targeted solely at on-road motorcyclists. The primary aim was
therefore to assess the injury severity, injury profiles and outcomes in terms of health and
return to work three months after the accident in off-road motorcyclists compared to on-road
motorcyclists, in order to emphasise the need for action towards reducing trauma in this
group. This thesis, which is part of an ongoing project, is one of the final stages in becoming a
doctor and has been a wonderful experience for me. However, it has not been without
challenges and I would like to thank all who played a role in this project, in particular the
following persons.
First of all, I would like to thank my local supervisors, Professor René Zellweger and Doctor
Manimaran Sinnathamby. Prof., you have been supportive in many ways and have
encouraged me from the start to make the most of my stay here. You have a strong, unique
personality and have challenged me to think critically about a variety of subjects. For me
personally, my stay has been a success and I hope the feeling is mutual. Maran, you have
given me the freedom to explore my own ideas and were available when needed to steer me in
the right direction. Thank you for allowing me to take responsibility of the project and to fully
experience what it means to do a scientific research project. Also, I would like to thank
Maxine Burrell and the people from Medical Records in RPH, who have put effort in making
part of the data available in time, which was a successful challenge in the end. Further thanks
go to Katrin Zellweger, for casting a critical eye on my writing and providing important
suggestions towards improvement.
Secondly, I would like to thank my supervisors in the Netherlands, especially Ms. Inge
Reininga who has been an invaluable help with constructive comments and her expertise on
statistical analyses. Inge, you drove the necessary reshaping of this thesis to make it a
comprehensive whole and you have put a lot of effort into helping me understand how to
analyse the data. It all makes more sense now! Further, I would like to thank Doctor Roeland
den Boer, who was available at the start for advice with the content of the study.
Lastly, but most importantly, I would like to thank all patients that participated in this study,
not only by taking the time to answer all the questions with patience, but also by providing
insight in your passion for motorcycling and willingness to share graphic material of your
motorcycles, injuries and equipment. Your input has been an inspiration and at least one other
project has sprouted from your suggestions.
Enjoy the read and do not hesitate to contact me for questions or critical notes on the content!
Kind regards,
Steven Leeuwerke
Final year medical student at the Rijksuniversity Groningen, the Netherlands

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | II
Summary
Introduction Roughly 15,500 serious injuries and over 200 deaths occur on Australian roads annually
following motorcycle accidents, which equals to approximately 26% of all serious road
trauma. While the incidence of off-road motorcycle trauma is gradually increasing and up to
50% of all motorcycle accidents have been reported to occur off-road, preventive strategies
have almost been solely aimed at on-road motorcyclists. Earlier literature suggests differences
between both groups in terms of risk factors, injury severity, injury profiles and the use and
effect of motorcycle clothing, but results remain inconclusive. Further, differences in health
outcomes and return to work have not been investigated previously.
Objective This study primarily aimed to compare on-road and off-road motorcyclists with respect to
injury severity, injury profiles, the use and effect of motorcycle clothing and outcomes in
terms of physical and emotional health, as well as return to work. Secondary objectives
included a comparison of rider demographics and contributing factors to both the cause and
severity of an accident.
Methods
A prospective cohort study was undertaken at a level 1 trauma centre of Royal Perth Hospital,
Western Australia, collecting data from interviews and medical records. All motorcycle
accidents (two-wheeled and all-terrain vehicles) that were reviewed by trauma surgery during
a 6 month period ending on the 5th
of March 2014 were approached for inclusion.
Results There were no significant differences between on-road (n=108, 60.0%) and off-road (n=72,
40.0%) motorcyclists in terms of injury severity, hospital length of stay and discharge location
(home or rehabilitation facility). Injury profiles were similar between both groups, with the
exception of soft tissue injuries, which occurred more frequently in on-road motorcyclists (on-
road n=93, 89.4% versus off-road n=52, 74.3%; p=0.01). Only motorcycle clothing with body
armour was found to be significantly protective against soft tissue injuries. A protective effect
of gloves was not found. Although protective, the use of motorcycle clothing was low with
only 6.5% of on-road and 15.3% of off-road motorcyclists wearing full equipment with body
armour imbedded in all parts. Physical and emotional health outcomes three months after the
accident were generally worse in on-road motorcyclists. Return to work was overall low with
46.7% of patients unable to return to partial or full-time employment three months after the
accident. Return to work was not significantly different between both groups.
Conclusion Off-road motorcyclists sustain equally severe injuries with mostly similar injury profiles and
form a significant group of trauma. These findings emphasise the implications of off-road
motorcycling trauma to patient and society and reinforce the need to take action to reduce
trauma in this group of motorcyclists. Further research is needed to formulate ways to
effectively implement new injury prevention strategies specifically targeted at off-road
motorcyclists.
Key terms: motorcycle accidents, off-road motorcycles, motorcycle clothing, health
outcomes, return to work.

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | III
Samenvatting
Introductie Jaarlijks vinden er ruim 15,000 ernstige en meer dan 200 fatale motorongevallen plaats op
Australische wegen en vormen daarmee ongeveer 26% van alle ernstige verkeersongevallen.
Hoewel de incidentie van off-road ongevallen gestaag toeneemt en tot wel 50% van alle
motorongevallen off-road plaatsvinden, zijn preventie campagnes tot nu toe vrijwel
uitsluitend gericht op on-road motorrijders. Eerdere literatuur suggereert verschillen tussen
on-road en off-road motorrijders betreft risicofactoren, letsel ernst, letsel profielen en het
gebruik en effect van motorkleding, maar resultaten zijn tot nu toe niet eenduidig. Verschillen
in gezondheidsuitkomsten en werk hervatting na het ongeval zijn niet eerder onderzocht.
Doel Het primaire doel was het vergelijken van on-road en off-road motorrijders op het gebied van
letsel ernst, letsel profielen, het gebruik en effect van motorkleding, fysieke en emotionele
gezondheidsuitkomsten en werk hervatting drie maanden na het ongeval. Secondaire doelen
waren onder meer het vergelijken van demografische gegevens en bijdragende factoren in
zowel de oorzaak en de ernst van het ongeval.
Methoden Dit prospectieve cohort onderzoek verzamelde gegevens afkomstig uit interviews en
medische dossiers in het Royal Perth Hospital, West Australië, een level 1 trauma centrum.
Alle motorongevallen (twee-wielers en all-terrain voertuigen) die werden beoordeeld door het
trauma team binnen een periode van 6 maanden (t/m 5 maart 2014), werden benaderd voor
deelname.
Resultaten Er werden geen significante verschillen gevonden tussen on-road (n=108, 60.0%) en off-road
(n=72, 40.0%) motorrijders op het gebied van letsel ernst, ziekenhuisverblijf of ontslag locatie
(huis of rehabilitatie centrum). Letsel profielen waren vergelijkbaar tussen beide groepen, met
uitzondering van weke delen letsels, welke vaker voorkwamen in on-road motorrijders (on-
road n=93, 89.4% versus off-road n=52, 74.3%; p=0.01). Motorkleding met body armour
bleek significant te beschermen tegen weke delen letsels. Er werd geen beschermend effect
gevonden van handschoenen. Het gebruik van motorkleding was infrequent, slechts 6.5% on-
road en 15.3% off-road motorrijders droegen een complete uitrusting met body armour.
Fysieke en emotionele gezondheidsuitkomsten waren slechter in on-road motorrijders drie
maanden na het ongeval. Werkhervatting was laag, 46.7% van alle patiënten was niet in staat
om het werk gedeeltelijk of volledig te hervatten. Er waren geen significante verschillen in
werkhervatting tussen on-road en off-road motorrijders.
Conclusie
Off-road motorrijders lopen letsels op van gelijke ernst en tonen grotendeels gelijke letsel
profielen en vormen daarmee een belangrijke groep trauma patiënten. De resultaten
benadrukken de gevolgen van off-road ongevallen voor zowel de patiënt en de maatschappij
en de noodzaak om trauma in deze groep motorrijders te verminderen. Toekomstig onderzoek
gericht op de invoer van preventie stragieën zijn
Sleutelwoorden: motorongevallen, off-road motorrijders, motorkleding,
gezondheidsuitkomsten, werkhervatting.

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | IV
Definitions and abbreviations
1. Definitions used by the WHO ICD-10[1]
Motorcycle: a motorcycle is a two-wheeled motor vehicle with one or two riding saddles and
sometimes with a third wheel for the support of a sidecar. The sidecar is considered part of the
motorcycle. A motorcycle rider is any person riding on a motorcycle or in a sidecar or trailer
attached to such a vehicle.
All-terrain vehicle (ATV): a special all-terrain vehicle is a motor vehicle of special design
to enable it to negotiate rough or soft terrain or snow. Examples of special design are high
construction, special wheels and tyres, tracks, and support on a cushion of air.
Traffic accident: a traffic accident is any vehicle accident occurring on the public highway
[i.e. originating on, terminating on, or involving a vehicle partially on the highway]. A vehicle
accident is assumed to have occurred on the public highway unless another place is specified,
except in the case of accidents involving only off-road motor vehicles, which are classified as
non-traffic accidents unless the contrary is stated.
Public highway or street: a public highway [trafficway] or street is the entire width between
property lines (or other boundary lines) of land open to the public as a matter of right or
custom for purposes of moving persons or property from one place to another. A roadway is
that part of the public highway designed, improved and customarily used for vehicular traffic.
Non-traffic accident: a non-traffic accident is any vehicle accident that occurs entirely in any
place other than a public highway.
2. Definitions used in the present study
Motorcycle: two wheeled motor vehicles and ATVs (as per WHO ICD-10 definition)
Motorcycle accident: any fall or collision whilst riding on a motorcycle as motorcycle rider
or passenger.
On-road: as per WHO ICD-10 definition of a traffic accident, or if involving an off-road
motorcycle on a public highway or street.
Off-road: as per WHO ICD-10 definition of a non-traffic accident, or if occurring on an
unsealed road.
Abbreviations:
ATV All-terrain vehicle
BA Body armour
ED Emergency Department
ICD-10 International Classification of Diseases version 10
ICU Intensive Care Unit
ISS Injury Severity Score
LOS Length of stay
MCA Motorcycle accident
RPH Royal Perth Hospital
TBI Traumatic Brain Injury
WA Western Australia
WHO World Health Organisation
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | V
List of figures and tables
Box 1 – Criteria for ED to involve trauma surgery in the line of care (Appendix I – page 35).
Box 2 – WHO ICD-10 definitions for motorcycles (page 9).
Figure 1 – Details of 36 excluded patients (Appendix I – page 35).
Figure 2 – A motorcycle handlebar penetrating the left thigh (page 18).
Figure 3 – Anterior-posterior view of a traumatic amputation of the thumb (page 18).
Figure 4 – Off-road impaling injury with a branch (page 18).
Table 1 – Demographics and admission details (page 12).
Table 2 – Rider characteristics (page 13).
Table 3 – Mechanism of injury by crash type (page 14).
Table 4 – Injury profiles of on-road and off-road motorcyclists (page 16).
Table 5 – Frequency of motorcycle clothing that was worn and owned, but not worn in on-
road and off-road motorcyclists (page 20).
Table 6 – Risk of not wearing any motorcycle clothing compared to wearing motorcycle
clothing with or without body armour (reference) (page 20).
Table 7a – Physical outcomes three months after the accident (page 22).
Table 7b – Physical outcomes three months after the accident between on-road and off-road
motorcyclists (reference), adjusted for possible confounders (age, gender, impact
speed, crash type and ISS) (page 23).
Table 8a – Emotional outcomes three months after the accident (page 24).
Table 8b – Emotional outcomes three months after the accident between on-road and off-road
motorcyclists (reference), adjusted for possible confounders (age, gender, impact
speed, crash type and ISS) (page 24).
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | VI
Contents FOREWORD ............................................................................................................................. I
SUMMARY/SAMENVATTING .....................................................................................II, III
DEFINITIONS AND ABBREVIATIONS ........................................................................... IV
LIST OF FIGURES AND TABLES ...................................................................................... V
CONTENTS .................................................................................................................... VI, VII
1. INTRODUCTION .................................................................................................... page 1-7
1.1 – Background ................................................................................................................... 1-6 1.1.1 – Definitions and classification systems in motorcycling ................................................. 1
1.1.2 – Popularity of motorcycling in Australia ......................................................................... 1
1.1.3 – Injury and mortality rates ........................................................................................... 1, 2
1.1.4 – Injury profiles ................................................................................................................. 2
1.1.5 – Burden to patient and society ..................................................................................... 2, 3
1.1.6 – Who gets hurt: contributing factors to the cause and mechanism of injury ............... 3, 4
1.1.7 – Who gets hurt: contributing factors to the severity and outcome of injury .................... 5
1.1.8 – On-road versus off-road motorcycle accidents .......................................................... 5, 6
1.2. – Study objectives ............................................................................................................ 6, 7 1.2.1 – Aim of this study ....................................................................................................... 6, 7
1.2.2 – Hypotheses .................................................................................................................... 7
2. METHODS ............................................................................................................. page 8-10
2.1 – Setting ............................................................................................................................... 8
2.2 – Study design ................................................................................................................. 8-10 2.2.1 – Definitions ...................................................................................................................... 8
2.2.2 – Study population, case identification and sample size ............................................... 8, 9
2.2.3 – Data collection and study variables .......................................................................... 9, 10
2.3 – Ethics approval ............................................................................................................... 10
2.4 – Statistical analyses .......................................................................................................... 10
3. RESULTS .............................................................................................................. page 11-24
3.1 – Study population ............................................................................................................. 11
3.2 – Demographics and injury severity ................................................................................. 11
3.3 – Rider characteristics, accident cause and mechanism ............................................. 12-15 3.3.1 – Rider characteristics ............................................................................................... 12, 13
3.3.2 – Cause and mechanism ............................................................................................. 13-15
3.4 – Injury profiles ............................................................................................................ 15-17 3.4.1 – Traumatic brain and neurological injuries ................................................................... 15
3.4.2 – Internal injuries ............................................................................................................ 15
3.4.3 – Fractures ................................................................................................................. 15, 17
3.4.4 – Soft tissue injuries ........................................................................................................ 17
3.5 – Motorcycle clothing ................................................................................................... 17-21 3.5.1 – Frequency of use ..................................................................................................... 17-19
3.5.2 – Effectiveness in preventing injury ........................................................................... 19-21
3.6 – Outcomes three months after the accident ............................................................... 21-24 3.6.1 – Demographics ............................................................................................................... 21
3.6.2 – Physical health ......................................................................................................... 21-23
3.6.3 – Emotional health .......................................................................................................... 23
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | VII
3.6.4 – Return to work and financial loss ................................................................................. 24
4. DISCUSSION ....................................................................................................... page 25-29
4.1 – Rider characteristics, accident cause and mechanism ............................................ 25, 26
4.2 – Injury severity and injury profiles ........................................................................... 26, 27
4.3 – Motorcycle clothing ........................................................................................................ 27
4.4 – Outcomes three months after the accident .................................................................... 28
4.5 – Recommendations .......................................................................................................... 29
4.6 – Strengths and limitations ............................................................................................... 29
5. CONCLUSION .......................................................................................................... page 30
REFERENCES .................................................................................................................. 31-34
APPENDICES ........................................................................................................................ 35
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | 1
1. Introduction
1.1 Background
1.1.1 Definitions and classification systems in motorcycling
Motorcycles are engine-powered machines used primarily for recreation and transportation.
Various vehicles may be regarded as motorcycles and the literature is subject to inconsistently
used terminology. Whereas some studies use the term ‘motorcycle’ to indicate only one
specific type of motorcycles (e.g. street bikes), in others this term also includes other
motorcycle types, such as quad bikes and dirt bikes. Two commonly used definitions to
classify motorcycles more accurately are ‘powered two-wheelers’ and ‘All-terrain vehicles’
(ATVs). However, although these definitions differentiate between the general build of the
motorcycle (e.g. frame and number of wheels), this does not take into account the intended
location of use of the motorcycle. This is important, as rider characteristics and the
environment in which in is ridden may influence the risk of having an motorcycle accident
(MCA), as well as the injury severity and injury profile of persons victim to such accidents.
Arguably the best method to define motorcycles and MCAs may be the classification system
used by the World Health Organisation (WHO), the International Classification of Diseases
(ICD), which is revised on a regular basis. The latest version, the ICD 2010 (ICD-10),
classifies motorcycles separately into two-wheeled motorcycles and ATVs and further
separates them into ‘traffic’ and ‘non-traffic’ accidents. Traffic accidents refer to accidents
occurring on public highways or streets, which are defined by the ICD-10 as ‘the entire width
between property lines (or other boundary lines) of land open to the public as a matter of right
or custom for purposes of moving persons or property from one place to another’, which is in
most definitions largely consistent with the term ‘on-road’. Non-traffic accidents are defined
as ‘any vehicle accident that occurs entirely in any place other than a public highway’ and is
in most definitions largely consistent with the term ‘off-road’.
The definitions used in this study deviate slightly from the definitions used by the
ICD-10 and are discussed in detail in the methods section, paragraph 2.2.1. The terminology
in this chapter is subject to the differences in terminology throughout the literature and is
specified where possible.
1.1.2 Popularity of motorcycling in Australia
The popularity of motorcycling as a method of recreation and transportation has steadily
increased in Australia over the years. With 115,488 new motorcycles (including scooters) sold
in 2012 of which over half (53.1%) were intended for off-road use, an overall increase in sales
of 5.4% compared to 2011 was observed [2]. This seems consistent with the average annual
increase in motorcycle registrations of 6.8% and 5.8% from 2002 to 2008 and 2008 to 2013
respectively [3,4], which is much higher than the increase in registrations of other road
vehicles [5]. Furthermore, whereas motorcycles comprised 3.7% of all road vehicle
registrations in 2008, this percentage had grown to 4.3% in 2013 [3]. These trends predict a
continuing increase in the use of both on-road and off-road motorcycles, with an associated
increase in future motorcycle trauma.
1.1.3 Injury and mortality rates
Although motorcyclists represent a relatively small proportion of all Australian road users,
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 2
they show the highest morbidity and mortality rates due to crashes [5-7]. From 2008 to 2009,
14,493 hospital admissions due to serious motorcycle injuries were recorded in Australia,
which accounted for 26.3% of all hospital admissions for serious injuries following traffic
accidents during that year [7]. In 2012, 224 MCA associated deaths were recorded [8]. The
fact that motorcyclists are a vulnerable group of road users becomes even more evident when
comparing injury and death rates per 100,000 registered vehicles and per distance travelled.
Compared to other road users, motorcyclists show a 10-fold higher injury rate and a 5- to 6-
fold higher death rate per 100,000 registered vehicles [4,5,7]. Per distance travelled,
motorcyclists show an approximately 41-fold higher rate of serious injury and a 30- to 34-fold
higher death rate compared with car occupants [5,9]. Furthermore, although the death rate per
distance travelled has decreased for car occupants over the last decade, for motorcyclists it has
not [5], despite an average decrease in the number of deaths per 10,000 registered
motorcycles [8]. Although motorcyclists account for less than 1% of the distance travelled of
all Australian road users, the proportion of deaths due to MCAs is increasing and was near
15% of all road fatalities in 2007 [5]. Similar trends are observed in the United Kingdom
(UK) and Europe, where motorcyclists comprise less than 1% of all road users (UK) [10], but
account for 14% and 16% of all traffic fatalities respectively [10,11]. The fact that
motorcyclists are much more exposed compared to most other road users, may explain the
higher risk of serious and fatal injuries observed in motorcyclists.
1.1.4 Injury profiles
The type and severity of sustained injuries following a MCA (and any other accident) are
related to the impact force that is inflicted upon the body. The impact force is roughly
determined by the mass (kilograms) times the deceleration of the crashing object (meters per
second), the latter of which is determined by the change in velocity over a certain time period.
Both deceleration and mass are directly proportional with the impact force. In other words, a
large and rapid decrease in velocity and a high mass result in a high impact force. Effective
measures to prolong the deceleration time and subsequently decrease the impact force have
been implemented in cars for decades and include seatbelts, airbags and crumple zones. The
absence of such measures due to the difficulty to implement them on motorcycles may
explain the high morbidity and mortality observed in motorcyclists.
Because MCAs usually involve a significant impact force, many MCAs result in
multi-trauma patients with multiple injured body regions [12] (up to 88% in major trauma
patients [13]). Injured body regions most commonly involving the extremities [12,14],
followed by the head or neck and chest in non-fatal accidents [12,14-16]. In patients admitted
to trauma units, over 95% of patients sustained one or more fractures [15], which most
commonly involves the lower extremity [12,14-16]. Of these, the tibia, followed by the femur
[15], foot and patella are most frequently involved and have shown to have a large impact on
disability, economic costs and return to work [12]. Fatal accidents predominantly occur in on-
road motorcyclists (94%) [16] and are mainly the result of the head injuries [12,16], followed
by internal thoracic and abdominal injuries [12]. With roughly 26% of all hospital admissions
due to serious injuries following traffic accidents consisting of motorcyclists [7], the potential
burden to both patient and society are considerable.
1.1.5 Burden to patient and society
By 2020, traffic accidents are expected to be the third leading cause of long-term disability
and impairment worldwide [17]. With MCAs accounting for roughly 26% of all traffic
accidents that result in serious injury and hospital admission [7], both short- and long-term
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 3
disability rates are likely to be high in motorcyclists. Recently, a large study investigating
functional outcomes of MCA victims in eight European countries, reported that 46.4% of
patients was expected to experience some functional limitation as a result of their injuries at
least one year after hospital discharge [14]. The most common injuries involved the lower and
upper extremity, accounting for 26 and 21% of the total number of injuries respectively. The
expected long-term disability rates for these body regions were high at 80 and 47%
respectively. A more dated study looking at MCA victims that received compensation for
disability during that year (57.6%), reported that 68% had a mechanical impairment of a limb
and 80% were reported to have disfiguring impairments [18]. Disability mostly involved
problems with locomotion and dexterity at work.
Not only the burden to the patient, but also the burden to society is an important
consideration. As stated earlier, motorcyclists are prone to more severe injuries compared to
most other road users and may subsequently require more surgical procedures, require a
prolonged length of stay in hospitals and specialised rehabilitation centers and record a longer
absence from work, all of which have a financial impact on both the patient and society.
When looking at this more closely, the costs of MCAs to society are considerable. An
American study looking into the costs of medical care and lost productivity following fatal
and non-fatal traffic accidents, found that motorcyclists account for 12% (12 billion USD) of
all costs due to traffic accidents in 2005 [19]. Although motor vehicle accidents had the
largest share in cost (70 billion USD), motorcyclists showed disproportionally higher costs
with respect to their injury incidence [19]. An earlier American study investigating the costs
of motor vehicle accidents showed that the majority (74%) of these costs are paid by society
through insurance and taxes [20]. These are strong indicators that MCAs are a considerable
burden to both the patient and society in terms of disability, lost working days, productivity
and (ongoing) health care costs.
1.1.6 Who gets hurt: contributing factors to the cause and mechanism of injury
Age and sex
Most frequently involved in MCAs are young males [12,21,22], especially motorcyclists in
their twenties [11,21]. Young motorcyclists are more often inexperienced [22], which has
been related to the risk of a MCA [12,23]. Furthermore, they have been shown to be more
likely to engage in risk/taking behaviour, such as dangerous driving and breaking the law (e.g.
speeding, drink-riding, not wearing a helmet) [12]. Despite the higher risk of MCAs in young
motorcyclists, another peak is reported in motorcyclists in their forties and fifties [12,21,22].
It has been suggested that this is related to decreased physical resiliency and slower reaction
times [21,22].
A disturbing note is the increasing number of children involved in MCAs, especially
off-road. Between 2009 and 2010, 10.2% and 30.3% of reported MCAs occurred in persons
under the age of 15 and 25 respectively [24]. Another study even found that 56% of off-road
MCAs occurred in children under the age of 12, and 8% of children were only 5 years old or
even younger [25]. Bevan et al. reported a similar distribution and showed an annual increase
of juvenile MCAs with almost 10% during the study period (2000 to 2004) [26]. Multiple
studies show that off-road MCAs in children are associated with significant morbidity and
mortality [25-28] and disability rates up to 24% following head injuries [27,29,30]. The large
number of juvenile motorcyclists may in part be explained by the absence of minimum age
requirements, obligatory licensing or obligatory registering of motorcycles when riding on
private lands [13].

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 4
Inexperience and training
Although inexperienced motorcyclists show an increased risk of being involved in a MCA
[12], a significant lower risk of MCAs in trained motorcyclists versus untrained motorcyclists
has not been clearly demonstrated [12,31]. A recent Cochrane review concluded that no clear
statements could be made as to the effect of motorcycle training on crash, injury or offence
rates, due to the poor quality of the studies currently available [32]. A possible explanation for
the absence of clear evidence that motorcycle training has any influence on MCA rates may
be that not experience, but rather age is the main determinant for the risk of a MCA due to the
higher occurrence of risk taking behaviour in young motorcyclists, as was stated earlier [12].
Another possible explanation is that motorcyclists adapt their riding behaviour because of
increased confidence in their operating skills following motorcycle training [12].
Single- and multi vehicle accidents
As explained in paragraph 1.1.4, the type and severity of sustained injuries following a MCA
are related to the impact force that is inflicted upon the body. Keeping this in mind, one may
understand how sudden loss of velocity (e.g. due to hitting a moving or static solid object)
results in a short deceleration time and subsequently, a high impact force. It is therefore not
surprising that collisions are reported to result in a greater injury severity [6,22]. Cassell et al.
reported that 58% of all fatal accidents were attributable to collisions with other road users,
and 12% to collisions with fixed objects [16]. In collisions with cars at intersections, the car
driver is usually responsible for the accident [22]. This has been found to be attributable to
drivers not seeing the motorcycle either due to the shape and colour of the motorcycle or
having a strong set to only see other cars [22]. Although most MCAs are single vehicle
accidents [6,33], a considerable proportion of accidents involves other vehicles and a
significant proportion of single vehicle MCAs result from swerving to avoid impact with
another vehicle [12].
Intoxication
Intoxication with alcohol and/or drugs is a widely accepted risk factor for traffic accidents and
is associated with decreased riding skills [22]. Especially amongst motorcyclists, the rate of
alcohol use is high [12]. Further, fatal accidents involving alcohol occur more frequently in
motorcyclists than in drivers of any other motor vehicles [12,22]. Alcohol use is associated
with speeding, lower rates of helmet use [34] and more severe head injuries in both helmeted
and unhelmeted patients, likely due to increased susceptibility to haemorrhagic shock [12].
The use of other drugs, such as cannabis and cocaine, has been reported to be higher in
motorcyclists as well [12]. It has been suggested that intoxicated riding occurs more
frequently in off-road motorcyclists than in on-road motorcyclists [35].
Environmental factors: road conditions and weather
Both road conditions and weather may be a causative contributor in a small proportion of
MCAs. While most fatal and non-fatal traffic accidents occur on dry, sealed roads [35], loss
of surface grip, which is influenced by wet roads, road markings, loose materials, potholes,
and surface irregularities, seem to be the main causative contributors [22]. Further, many
motorcyclists lose control in curves [22] and roadside objects such as crash barriers and
guardrails have been shown to increase mortality rates [6]. Weather does not appear to be an
important contributing factor in the majority of MCAs, likely due to the fact that motorcycling
is mainly a recreational activity reserved for favourable weather conditions [22]. When used
for transportation, motorcyclists may switch to alternative transport options during bad
weather [22].
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 5
1.1.7 Who gets hurt: contributing factors to the severity and outcome of injury
Speeding
Not only is it more difficult to remain in control of the motorcycle at high speeds due to faster
required reaction times and may therefore be a causative factor in an accident, higher speeds
also contribute to the impact force and subsequently the injury severity of a MCA (paragraph
1.1.4). Indeed, higher impact speeds have been associated with more severe injuries in
motorcyclists [6,12]. Speeding is reported to account for almost two thirds of fatal MCAs
involved in single vehicle accidents [12], possibly due to a reported reduction in helmet
effectiveness at high speeds [6,12]. Not only excessive speed, but also the appropriate speed
for the traffic conditions in which in is ridden is an important consideration [12].
Protective equipment
In most countries including Australia, the use of a helmet is mandatory. Helmets reduce the
risk of injury by absorbing the impact force through an energy absorbent liner and resisting
penetration of sharp objects through a hard outer shell [36]. Their protective benefit is well
established and a reduction of head injury and mortality by 42 and 69% respectively is
reported in the literature [37]. Nonetheless, some controversy remained because of observed
cervical spine injuries in helmeted MCA patients [12]. It was thought that the added head
mass might increase the chance of hyper-flexion or -extension during a MCA. Most of these
studies, however, had limitations in their designs and their findings have been contradicted by
many other studies that did not find such a relationship [12]. Controversially, a protective
effect of helmets on cervical spine injuries has also been reported [38]. Despite their
irrefutably proven benefit, helmet compliance remains an issue in a small group of MCAs and
it has been suggested that the rate of helmet non-compliance is higher in off-road MCAs
[26,39].
Additional protective equipment, such as special motorcycle jackets, pants, boots and
gloves, may also decrease the risk of injury following an accident. An additional protective
effect against the weather has been argued, which may decrease the risk of an accident by
minimizing distraction and discomfort from the weather [40]. The use of protective equipment
other than helmets is optional and not bounded by Australian law. Many variations in clothing
material, thickness and the presence and location of additional body armour exist,
complicating the assessment of their protective properties. Few studies have looked into the
effect of protective equipment on injury prevention. A recent study by de Rome et al. showed
a significant reduction in soft tissue damage, in particular open wounds, when wearing
protective equipment during a MCA [41]. A protective effect on fractures, however, could not
be demonstrated. Nonetheless, motorcyclists wearing protective equipment spent less time in
hospital and reported less severe pain scores, impairment and disability two months after the
accident.
1.1.8 On-road versus off-road motorcycle accidents
As stated in the beginning of this chapter, on-road and off-road motorcyclists may differ with
respect to rider characteristics, risk factors, injury severity and injury profiles following a
MCA. The focus has mainly been on on-road motorcyclists, despite the fact that more than
half of all motorcycles sold in Australia are intended for off-road use [2] and the proportion of
MCAs occurring in off-road locations have been reported to be 24 to 50% in adults or adults
and children combined [13,16,24,33,39,42] and as high as 89% in children ≤16 years [26].
Furthermore, multiple studies show that the incidence of off-road MCAs is increasing [13,24-
26,28,39,43-45]. To the authors knowledge, only three studies have reported on differences
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 6
between on-road and off-road motorcyclists with respect to injury severity and injury profiles
[13,16,42]. Cassell et al., comparing both fatal and non-fatal on-road and off-road MCAs,
found that although most on-road fatalities are the result of a collision with another road user
(49%) or fixed object (25%), off-road fatalities were more frequently caused by non-collision
accidents (67%) [16]. Injury profiles in fatal accidents were similar between on-road and off-
road MCAs and most commonly involved head injuries, followed by thoracic injuries.
Further, no differences in injury profiles between both groups were found in non-fatal
injuries, with fractures being the most common type of injury followed by open wounds. For
severe cases, injury profiles were similar as well with the most common type of injury being
fractures, followed by internal organ injuries, intracranial injuries and injury to the nerve and
spinal cord. On-road motorcyclists, however, involved generally more severe injuries in terms
of hospital length of stay. Mikocka-Walus et al., looking exclusively at major trauma patients,
found comparable results [13]. They found that on-road motorcyclists were more commonly
admitted to rehabilitation facilities, had longer admission lengths and longer stays in Intensive
Care Units (ICU) [13]. Further, the incidence of serious head and extremity injuries was
higher in on-road motorcyclists. In both on-road and off-road motorcyclists, thoracic injuries
were the most common type of injury [13]. Grange et al., investigating crashed motorcyclists
in a level 1 trauma centre and an Emergency Department (ED) in California, reported no
significant differences in injury severity between on-road and off-road motorcyclists in terms
of Injury Severity Scores (ISS), admission rates and admission to ICUs [42]. They did find
differences in injury profiles, with the incidence of blunt chest, abdominal and skin trauma
being higher in on-road motorcyclists. Further, on-road motorcyclists were more likely to
require transfusions and die from their injuries [42].
With regards to risk factors, all three studies found that off-road motorcyclists are
generally younger [13,16,42]. Bevan et al. investigated ED presentations and trauma
admissions related to motorcycling in paediatric patients (≤16 years) and found that only 72%
of patients in which helmet-wearing status was recorded were wearing a helmet [26]. The
high non-compliance of helmet use in off-road motorcyclists has been reported previously and
higher rates of alcohol and/or drug use in off-road motorcyclists have been reported as well
[39].
To date, the only data on the differences between on-road and off-road MCAs with
respect to injury severity and injury profiles comes from three studies that report partially
conflicting results [13,16,42]. As all of these studies were retrospective studies based on
hospital codings, the recording of less severe injuries such as soft tissue injuries were likely
underreported or were not reported at all. None of these studies have adjusted the found
differences for possible confounding factors such as impact speed and worn motorcycle
clothing. More research is needed to provide a more detailed insight into the differences
between both groups.
1.2 Study objectives
1.2.1 Aim of this study
Western Australia (WA) is the largest state of Australia and encompasses a large area of rural
and remote regions. Of all Australian states, WA has shown the largest increase in motorcycle
registrations (47.8% from 2008 to 2013) [3]. Further, WA has been reported to have the
second smallest average annual decrease in fatal MCAs from 2003 to 2012 [8] and the
number of seriously injured people following MCAs keeps increasing [46]. Royal Perth
Hospital (RPH) houses the only level 1 trauma centre in the state and subsequently receives
near 80% of all major (motorcycling) trauma. The experience of local doctors is that off-road
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 7
motorcycling is a increasingly popular recreational activity in WA and that a high proportion
of all MCAs occur off-road. Many of these accidents are of at least equal severity compared
to on-road MCAs and often no protective equipment is worn. As stated earlier, previous
studies investigating differences between on-road and off-road MCAs with respect to injury
severity and injury profiles remain partly inconclusive and the impact speed and use of
motorcycle clothing in this group of motorcyclists remains uninvestigated. Furthermore,
although there have been studies reporting on disability rates following MCAs [14,18], these
focused on on-road motorcyclists and a comparison with on-road motorcyclists has not been
made. More research is needed to supplement the existing literature and to emphasise the
implications of off-road motorcycle trauma on both patient and society, so that new
prevention campaigns specifically targeted at off-road motorcyclists may be implemented.
The primary aim of this study was therefore to compare on-road and off-road motorcyclists
with respect to:
1. injury severity and injury profiles;
2. the use of motorcycle clothing and their effect on injury prevention;
3. outcomes in terms of physical and emotional health, as well as return to work three
months after the accident.
Secondary study objectives included a comparison of rider demographics and contributing
factors to both the cause and severity of the injury, including intoxication, (impact) speed and
environmental factors.
1.2.2 Hypotheses
For primary study objectives, the following hypotheses were formulated and tested:
1. Injury profiles and injury prevention
H0: off-road motorcycle accidents are of equal severity compared to on-road
motorcyclists following an accident, measured using ISS and hospital length of stay
H0: off-road motorcyclists show similar injury profiles compared to on-road
motorcyclists following an accident.
2. Use of protective equipment and their effect on injury prevention
H0: the use of motorcycle clothing is similar in on-road and off-road motorcyclists that
are involved in an accident.
H0: motorcycle clothing in on-road and off-road motorcyclists is equally protective.
3. Outcome
H0: off-road motorcyclists show similar outcomes in terms of physical health,
emotional health and return to work three months after the accident compared to on-
road motorcyclists following an accident.
H0: off-road motorcyclists show similar return to work rates three months after the
accident compared to on-road motorcyclists following an accident.
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 8
2. Methods
2.1 Setting
The Royal Perth Hospital (RPH) is a level 1 major trauma service provider and includes a
specialised trauma centre with a 30-bed capacity and four high acuity beds. RPH provides
care for an area of approximately 2.5 million km2 and 2.2 million people [6]. As the only level
1 trauma centre in the state, RPH receives approximately 80% of all major trauma cases in
WA [47]. MCAs account for 8% of all trauma cases admitted to RPH, which translates into
roughly 400 RPH admissions following MCAs annually [48]. All (acute) trauma cases that
are presented to RPH are admitted to the Emergency Department (ED), where the initial
resuscitation, diagnostic investigations and treatment take place. The decision to involve the
trauma team is predominantly based on the physical signs, mechanism and anatomical area of
injury of the patient (appendix I – box 1). From the ED, trauma patients may be admitted
under trauma surgery, orthopaedics, plastic surgery, spinal surgery or other specialties.
2.2 Study design
2.2.1 Definitions
The definitions used in this study were based on the WHO ICD-10 definitions and were
adapted to include a slightly different range of motorcycles and road locations. In this study,
the term ‘motorcycle’ was used to indicate both two-wheeled motor vehicles and ATVs,
which were defined in concordance with the WHO ICD-10 definitions (box 2) [1] and
included street bikes, dirt bikes, scooters, mopeds, motorized bicycles, quad bikes and buggies
respectively. A MCA was defined as any fall or collision whilst riding on a motorcycle as
motorcycle rider or passenger. The accident was considered to have occurred ‘on-road’ if it
fulfilled the criteria of a traffic accident or involved an off-road motorcycle that was ridden on
a public highway or street. The accident was considered to occur ‘off-road’, if the accident
occurred anywhere else or occurred on an unsealed road.
Injury severity was assessed using the Injury Severity Score (ISS), an internationally accepted
tool to grade injury severity in trauma patients. In concordance with the classification used by
the American College of Surgeons [49], injury severity was further classified based on ISS
score into minor (ISS 1 – 9), moderate (10 – 15), severe (ISS 16 – 24) and very severe (>24)
trauma. Trauma was considered ‘major’ in case of an ISS of 16 or greater.
Motorcyclists were considered to wear full equipment if all worn parts were
specifically designed for motorcycling and included at least a helmet, a jacket or impact
protector, pants, boots and gloves. The use of neck braces, shin guards/knee pads and kidney
belts were considered to be additional protective equipment. Equipment was considered to
contain body armour if this included multiple reinforcements over physically vulnerable areas
(e.g. foam pads over shoulders or elbows, Kevlar lining in pants). Although potentially
protective, the use of equipment not designed for motorcycling (e.g. steel-capped work boots)
was not considered to be protective equipment in this study.
2.2.2 Study population, case identification and sample size
A prospective cohort design was chosen for this study. Over a six month period (September
2013 to March 2014), all MCA cases that were reviewed or admitted by the trauma team were
considered to be eligible for this study. Eligible cases were identified from the hospital’s
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 9
patient management system (iSOFT Clinical Manager) and were approached by the student-
investigator for participation in the study. Patients deficient of the English language or with an
altered consciousness throughout admission (Glasgow Coma Scale <15) were excluded from
the study, as were MCAs that did not involve a review of the trauma team or resulted from an
(alleged) assault whilst on the motorbike. Written informed consent was obtained with
additional parental consent in case of under aged patients (<18 years). The sample size was
estimated at 100 – 150 patients, based on findings of an earlier RPH study [6] and annual
statistics on the number of MCAs in RPH [48].
2.2.3 Data collection and study variables
Data collection was separated into three occasions. First, a structured questionnaire-based
interview was conducted during admission, capturing data on demographics, substance use,
cause and mechanism of injury, use of protective equipment and details about the motorcycle
and riding behaviour. Secondly, the medical record of eligible patients was audited, capturing
data on admission and discharge details, accident location, sustained injuries and
management. Unconfirmed injuries were excluded from the analyses. ISS scores were
provided by a trained research nurse. Third, in a subgroup of patients, a structured
questionnaire-based follow-up interview was conducted over the telephone three months after
the accident, comprising of questions regarding the physical, emotional, social and
occupational impact of the accident. Time restrictions prevented completing the follow-up
interview in all patients.
Data from the questionnaire and the medical record were compared and conjoined into
a single database. Details on impact speed and riding while intoxicated were collected from
both the questionnaire and the medical record to increase accuracy. Discrepancies were
Box 2 – WHO ICD-10
1 definitions for motorcycles [49].
Motorcycle:
A motorcycle is a two-wheeled motor vehicle with one or two riding saddles and sometimes with a third wheel for
the support of a sidecar. The sidecar is considered part of the motorcycle. A motorcycle rider is any person riding
on a motorcycle or in a sidecar or trailer attached to such a vehicle.
All-terrain vehicle:
A special all-terrain vehicle is a motor vehicle of special design to enable it to negotiate rough or soft terrain or
snow. Examples of special design are high construction, special wheels and tyres, tracks, and support on a cushion
of air.
Traffic accident:
A traffic accident is any vehicle accident occurring on the public highway [i.e. originating on, terminating on, or
involving a vehicle partially on the highway]. A vehicle accident is assumed to have occurred on the public
highway unless another place is specified, except in the case of accidents involving only off-road motor vehicles,
which are classified as non-traffic accidents unless the contrary is stated.
Public highway or street:
A public highway [trafficway] or street is the entire width between property lines (or other boundary lines) of land
open to the public as a matter of right or custom for purposes of moving persons or property from one place to
another. A roadway is that part of the public highway designed, improved and customarily used for vehicular
traffic.
Non-traffic accident:
A non-traffic accident is any vehicle accident that occurs entirely in any place other than a public highway.
1 World Health Organisation, International Classification of Diseases version 10.
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 10
resolved by finding evidence to support the data (e.g. measured blood ethanol level), or were
marked unknown when the accuracy of the data remained questionable. For variables that
involved an estimation (e.g. impact speed, years of riding experience), a mean value was
calculated if estimations were within a reasonable range (e.g. ± 20 km/h for impact speed).
2.2 Ethics approval
Ethics approval for this study was obtained from the Royal Perth Hospital Human Research
Ethics Committee prior to commencement of this study. All included images were used with
the consent of the patients.
2.3 Statistical analyses
Data were analysed using IBM SPSS Statistics for Windows (version 21.0 Armonk, NY: IBM
Corp). Descriptive statistics generally included frequency with percent distribution for
binomial data. Quantitative data were assessed for normality using plots and the Shapiro-Wilk
test and were presented as mean with standard deviation for normally distributed data or
median with range for non-normally distributed data. Inferential statistics were performed
using Fisher’s exact test for binomial data and the Pearson’s Chi-squared test for trends for
categorical data. Binomial and categorical quantitative data were tested using the T-test and
Mann-Whitney U test for normally distributed data and ANOVA and Kruskall-Wallis test for
non-normally distributed data respectively. Single injuries were categorized by injury type
and were analysed as binomial data (injury present or absent) in two steps. First, potential
differences in the incidence of injury between on-road and off-road motorcyclists were
identified using Fisher’s exact test. Secondly, a multivariate logistic regression model was
calculated, adjusting for possible confounders. Theoretical confounders included age, gender,
impact speed, crash type (single versus multiple vehicle accident) and motorcycle clothing
and were selected using univariate logistic regression models using a broad alpha (≤0.30).
Identified confounders were then entered into the final model (forward method) using the
likelihood ratio. The protective effect of motorcycle clothing and outcomes were analysed in a
similar manner, with potential confounders that were taken into account being age, gender,
impact speed, crash type and ISS. Multivariate logistic regression models were presented as
regression coefficient with odds ratio (OR) and 95% confidence interval (95% CI). All
inferential analyses used two-tailed significance levels of p≤0.05.

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 11
3. Results
3.1 Study population
A total of 247 MCA cases were identified during the study period, of which 222 met the
inclusion criteria. Of the 222 patients eligible for participation, 180 (81.1%) patients agreed to
be interviewed and were included in the study (details of excluded patients are presented in
Appendix I – figure 1). The medical records of 174 (96.7%) patients were available for audit,
in the remaining six cases data from the questionnaire was used exclusively. In addition, a
total of 101 (56.1%) patients were approached three months after the accident to partake in
the follow-up interview. Of these, 89 (88.1%) patients completed the interview, 10 (9.9%)
patients could not be reached and 2 (2.0%) patients refused participation.
3.2 Demographics and injury severity
Of the total of 180 accidents, 108 (60.0%) accidents occurred on-road and 72 (40.0%)
accidents occurred off-road. Patients were predominantly male (n=160, 88.9%) with ages
ranging from 14 to 84 years (median 30.5 years) (Table 1). Most patients were single (n=80,
44.4%), followed by married (n=46, 25.6%), defacto (n=22.2, 40.0%) and divorced or
separated (n=14, 7.8%). The majority of patients were admitted under trauma surgery (n=100,
55.6%) or orthopedic surgery (n=53, 29.4%). Other admitting specialties included spinal
surgery, plastic surgery, burns, neurosurgery, maxillofacial surgery and urology. Injury
severity varied greatly among motorcyclists and ISS ranged from 1 to 38 (median ISS 9.0).
Most patients were considered minor traumas (n=104, 57.8%) and 27 (15%) patients were
considered major traumas (ISS > 15). Overall, including re-admissions a total of 1358 RPH
admission days were recorded (median length of stay (LOS) 5.0 days, range 1 – 76 days).
Twelve patients required admission to an Intensive Care Unit (ICU) (median LOS 3.0 days,
range 1 – 9 days). Ninety-nine (55.0%) patients required injury management by means of one
or more surgical interventions (minor interventions such as suturing small lacerations were
considered conservative management). Most patients were discharged home following
admission (n=127, 70.6%), a smaller proportion required rehabilitation in a specialised center
(n=37, 20.6%) or were discharged to another hospital (n=15, 8.3%). Patients spent a total of
850 days in rehabilitation centers, ranging from 4 to 86 days (median LOS 17.0 days). An
additional 114 days were spent in other hospitals (median LOS 5.0 days, range 1 – 30 days).
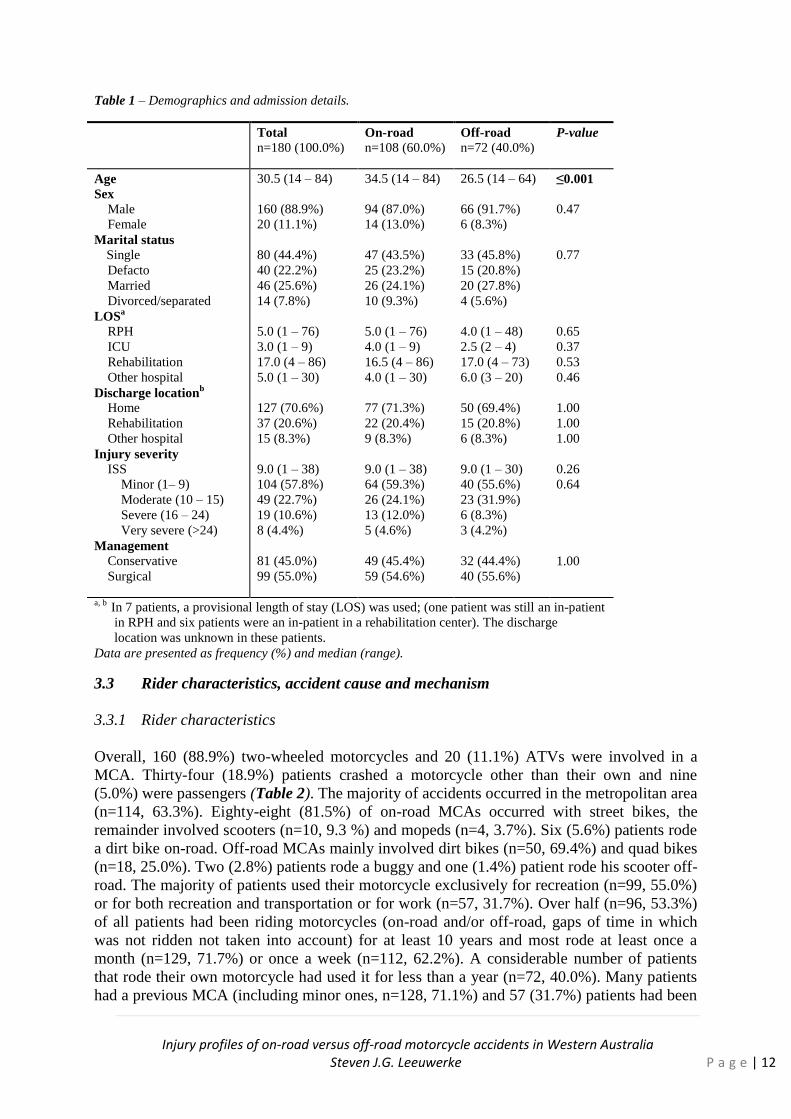
When comparing on-road and off-road MCAs, off-road motorcyclists were generally
younger than on-road motorcyclists (p≤0.001) (Table 1). Injury severity (ISS) did not differ
significantly between both groups (p=0.26), nor was the proportion of motorcyclists in each
trauma category significantly different (p=0.64). The proportion of major trauma cases (ISS
category severe and very severe) were statistically similar for on-road and off-road MCAs
(on-road n=18, 16.7% versus off-road n=9, 12.5%; p=0.53). LOS between on-road and off-
road motorcyclists did not differ significantly for RPH (p=0.65), ICU (p=0.37), rehabilitation
facilities (p=0.37) or other hospitals (p=0.46). The proportion of patients that required
surgical intervention was related to injury severity (p=0.05), but did not differ between both
groups (p=1.00). Statistically similar proportions of patients were discharged home (p=1.00),
to a rehabilitation facility (p=1.00) or to another hospital (p=1.00).
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 12
Table 1 – Demographics and admission details.
Total n=180 (100.0%)
On-road
n=108 (60.0%) Off-road
n=72 (40.0%) P-value
Age
Sex Male
Female
Marital status
Single
Defacto
Married
Divorced/separated
LOSa
RPH
ICU
Rehabilitation
Other hospital
Discharge locationb
Home
Rehabilitation
Other hospital
Injury severity
ISS
Minor (1– 9)
Moderate (10 – 15)
Severe (16 – 24)
Very severe (>24)
Management Conservative
Surgical
30.5 (14 – 84)
160 (88.9%)
20 (11.1%)
80 (44.4%)
40 (22.2%)
46 (25.6%)
14 (7.8%)
5.0 (1 – 76)
3.0 (1 – 9)
17.0 (4 – 86)
5.0 (1 – 30)
127 (70.6%)
37 (20.6%)
15 (8.3%)
9.0 (1 – 38)
104 (57.8%)
49 (22.7%)
19 (10.6%)
8 (4.4%)
81 (45.0%)
99 (55.0%)
34.5 (14 – 84)
94 (87.0%)
14 (13.0%)
47 (43.5%)
25 (23.2%)
26 (24.1%)
10 (9.3%)
5.0 (1 – 76)
4.0 (1 – 9)
16.5 (4 – 86)
4.0 (1 – 30)
77 (71.3%)
22 (20.4%)
9 (8.3%)
9.0 (1 – 38)
64 (59.3%)
26 (24.1%)
13 (12.0%)
5 (4.6%)
49 (45.4%)
59 (54.6%)
26.5 (14 – 64)
66 (91.7%)
6 (8.3%)
33 (45.8%)
15 (20.8%)
20 (27.8%)
4 (5.6%)
4.0 (1 – 48)
2.5 (2 – 4)
17.0 (4 – 73)
6.0 (3 – 20)
50 (69.4%)
15 (20.8%)
6 (8.3%)
9.0 (1 – 30)
40 (55.6%)
23 (31.9%)
6 (8.3%)
3 (4.2%)
32 (44.4%)
40 (55.6%)
≤0.001
0.47
0.77
0.65
0.37
0.53
0.46
1.00
1.00
1.00
0.26
0.64
1.00
a, b In 7 patients, a provisional length of stay (LOS) was used; (one patient was still an in-patient
in RPH and six patients were an in-patient in a rehabilitation center). The discharge
location was unknown in these patients.
Data are presented as frequency (%) and median (range).
3.3 Rider characteristics, accident cause and mechanism
3.3.1 Rider characteristics
Overall, 160 (88.9%) two-wheeled motorcycles and 20 (11.1%) ATVs were involved in a
MCA. Thirty-four (18.9%) patients crashed a motorcycle other than their own and nine
(5.0%) were passengers (Table 2). The majority of accidents occurred in the metropolitan area
(n=114, 63.3%). Eighty-eight (81.5%) of on-road MCAs occurred with street bikes, the
remainder involved scooters (n=10, 9.3 %) and mopeds (n=4, 3.7%). Six (5.6%) patients rode
a dirt bike on-road. Off-road MCAs mainly involved dirt bikes (n=50, 69.4%) and quad bikes
(n=18, 25.0%). Two (2.8%) patients rode a buggy and one (1.4%) patient rode his scooter off-
road. The majority of patients used their motorcycle exclusively for recreation (n=99, 55.0%)
or for both recreation and transportation or for work (n=57, 31.7%). Over half (n=96, 53.3%)
of all patients had been riding motorcycles (on-road and/or off-road, gaps of time in which
was not ridden not taken into account) for at least 10 years and most rode at least once a
month (n=129, 71.7%) or once a week (n=112, 62.2%). A considerable number of patients
that rode their own motorcycle had used it for less than a year (n=72, 40.0%). Many patients
had a previous MCA (including minor ones, n=128, 71.1%) and 57 (31.7%) patients had been
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 13
hospitalized before following a MCA.
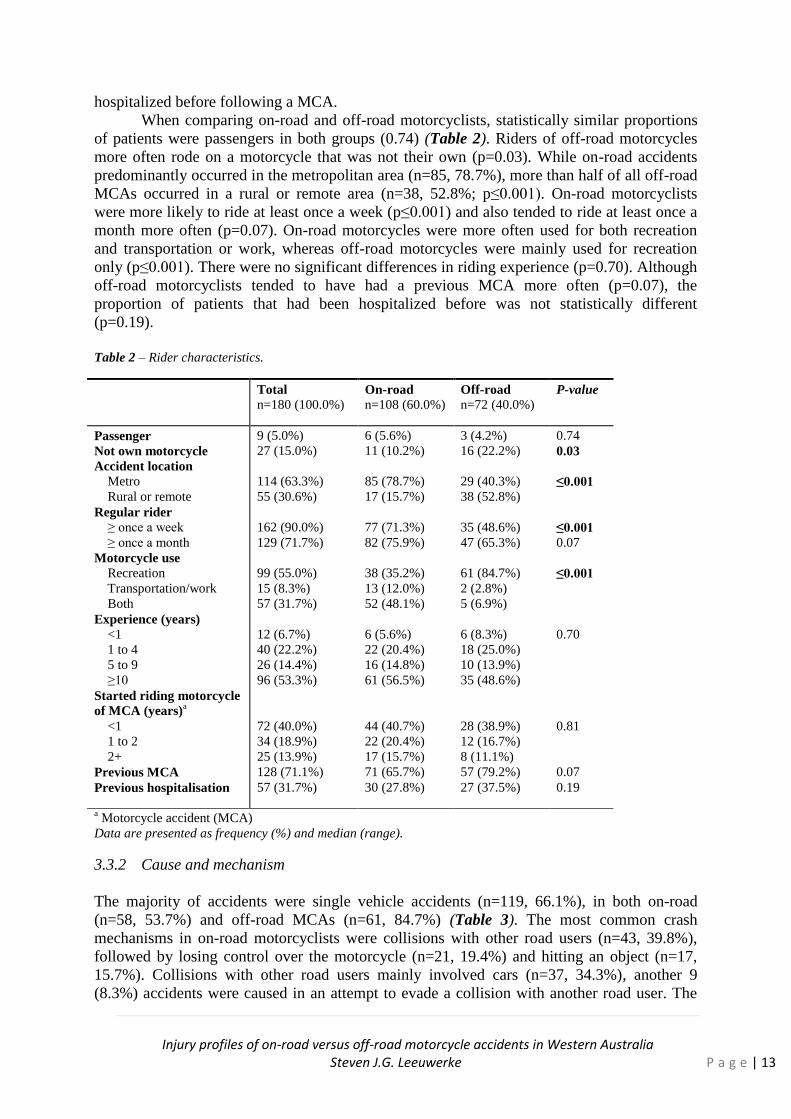
When comparing on-road and off-road motorcyclists, statistically similar proportions
of patients were passengers in both groups (0.74) (Table 2). Riders of off-road motorcycles
more often rode on a motorcycle that was not their own (p=0.03). While on-road accidents
predominantly occurred in the metropolitan area (n=85, 78.7%), more than half of all off-road
MCAs occurred in a rural or remote area (n=38, 52.8%; p≤0.001). On-road motorcyclists
were more likely to ride at least once a week (p≤0.001) and also tended to ride at least once a
month more often (p=0.07). On-road motorcycles were more often used for both recreation
and transportation or work, whereas off-road motorcycles were mainly used for recreation
only (p≤0.001). There were no significant differences in riding experience (p=0.70). Although
off-road motorcyclists tended to have had a previous MCA more often (p=0.07), the
proportion of patients that had been hospitalized before was not statistically different
(p=0.19).
Table 2 – Rider characteristics.
Total n=180 (100.0%)
On-road
n=108 (60.0%) Off-road
n=72 (40.0%) P-value
Passenger
Not own motorcycle
Accident location Metro
Rural or remote
Regular rider ≥ once a week
≥ once a month
Motorcycle use
Recreation
Transportation/work
Both
Experience (years)
<1
1 to 4
5 to 9
≥10
Started riding motorcycle
of MCA (years)a
<1
1 to 2
2+
Previous MCA
Previous hospitalisation
9 (5.0%)
27 (15.0%)
114 (63.3%)
55 (30.6%)
162 (90.0%)
129 (71.7%)
99 (55.0%)
15 (8.3%)
57 (31.7%)
12 (6.7%)
40 (22.2%)
26 (14.4%)
96 (53.3%)
72 (40.0%)
34 (18.9%)
25 (13.9%)
128 (71.1%)
57 (31.7%)
6 (5.6%)
11 (10.2%)
85 (78.7%)
17 (15.7%)
77 (71.3%)
82 (75.9%)
38 (35.2%)
13 (12.0%)
52 (48.1%)
6 (5.6%)
22 (20.4%)
16 (14.8%)
61 (56.5%)
44 (40.7%)
22 (20.4%)
17 (15.7%)
71 (65.7%)
30 (27.8%)
3 (4.2%)
16 (22.2%)
29 (40.3%)
38 (52.8%)
35 (48.6%)
47 (65.3%)
61 (84.7%)
2 (2.8%)
5 (6.9%)
6 (8.3%)
18 (25.0%)
10 (13.9%)
35 (48.6%)
28 (38.9%)
12 (16.7%)
8 (11.1%)
57 (79.2%)
27 (37.5%)
0.74
0.03
≤0.001
≤0.001 0.07
≤0.001
0.70
0.81
0.07
0.19
a Motorcycle accident (MCA)
Data are presented as frequency (%) and median (range).
3.3.2 Cause and mechanism
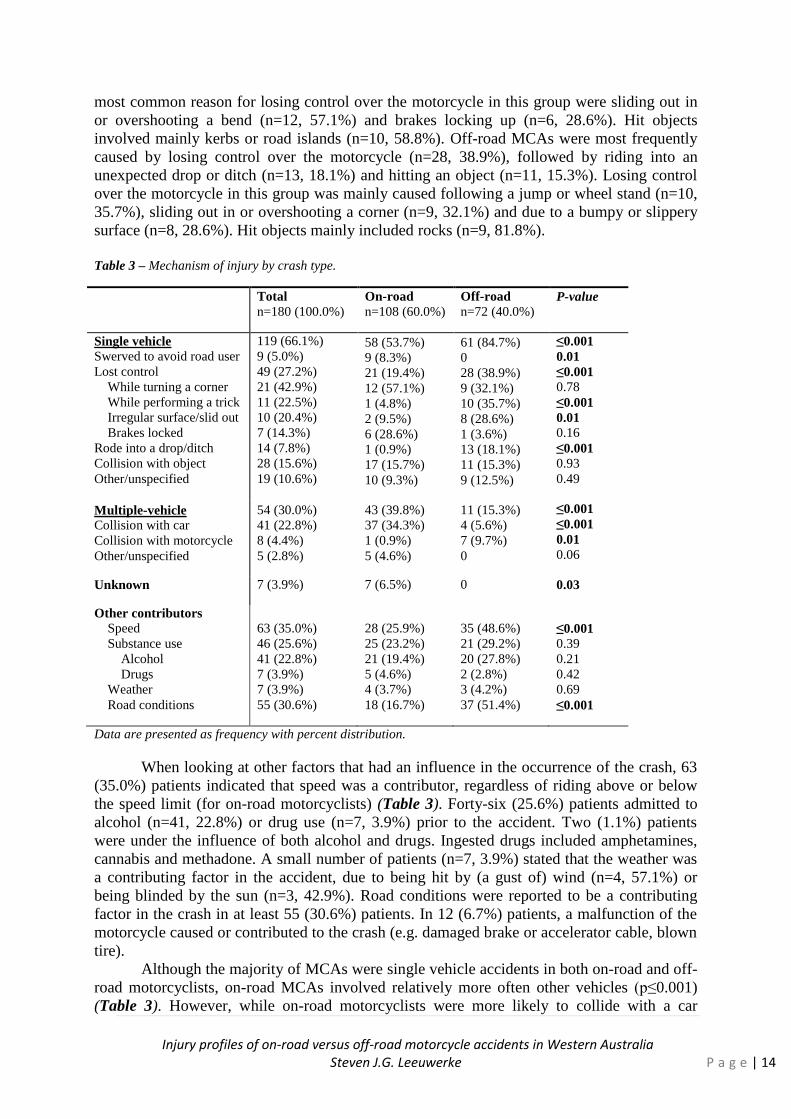
The majority of accidents were single vehicle accidents (n=119, 66.1%), in both on-road
(n=58, 53.7%) and off-road MCAs (n=61, 84.7%) (Table 3). The most common crash
mechanisms in on-road motorcyclists were collisions with other road users (n=43, 39.8%),
followed by losing control over the motorcycle (n=21, 19.4%) and hitting an object (n=17,
15.7%). Collisions with other road users mainly involved cars (n=37, 34.3%), another 9
(8.3%) accidents were caused in an attempt to evade a collision with another road user. The
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 14
most common reason for losing control over the motorcycle in this group were sliding out in
or overshooting a bend (n=12, 57.1%) and brakes locking up (n=6, 28.6%). Hit objects
involved mainly kerbs or road islands (n=10, 58.8%). Off-road MCAs were most frequently
caused by losing control over the motorcycle (n=28, 38.9%), followed by riding into an
unexpected drop or ditch (n=13, 18.1%) and hitting an object (n=11, 15.3%). Losing control
over the motorcycle in this group was mainly caused following a jump or wheel stand (n=10,
35.7%), sliding out in or overshooting a corner (n=9, 32.1%) and due to a bumpy or slippery
surface (n=8, 28.6%). Hit objects mainly included rocks (n=9, 81.8%).
Table 3 – Mechanism of injury by crash type.
Total
n=180 (100.0%)
On-road
n=108 (60.0%)
Off-road
n=72 (40.0%) P-value
Single vehicle Swerved to avoid road user
Lost control
While turning a corner
While performing a trick
Irregular surface/slid out
Brakes locked
Rode into a drop/ditch
Collision with object
Other/unspecified
119 (66.1%)
9 (5.0%)
49 (27.2%)
21 (42.9%)
11 (22.5%)
10 (20.4%)
7 (14.3%)
14 (7.8%)
28 (15.6%)
19 (10.6%)
58 (53.7%)
9 (8.3%)
21 (19.4%)
12 (57.1%)
1 (4.8%)
2 (9.5%)
6 (28.6%)
1 (0.9%)
17 (15.7%)
10 (9.3%)
61 (84.7%)
0
28 (38.9%)
9 (32.1%)
10 (35.7%)
8 (28.6%)
1 (3.6%)
13 (18.1%)
11 (15.3%)
9 (12.5%)
≤0.001
0.01
≤0.001
0.78
≤0.001
0.01
0.16
≤0.001
0.93
0.49
Multiple-vehicle
Collision with car
Collision with motorcycle
Other/unspecified
54 (30.0%)
41 (22.8%)
8 (4.4%)
5 (2.8%)
43 (39.8%)
37 (34.3%)
1 (0.9%)
5 (4.6%)
11 (15.3%)
4 (5.6%)
7 (9.7%)
0
≤0.001
≤0.001
0.01
0.06
Unknown 7 (3.9%) 7 (6.5%) 0 0.03
Other contributors
Speed
Substance use
Alcohol
Drugs
Weather
Road conditions
63 (35.0%)
46 (25.6%)
41 (22.8%)
7 (3.9%)
7 (3.9%)
55 (30.6%)
28 (25.9%)
25 (23.2%)
21 (19.4%)
5 (4.6%)
4 (3.7%)
18 (16.7%)
35 (48.6%)
21 (29.2%)
20 (27.8%)
2 (2.8%)
3 (4.2%)
37 (51.4%)
≤0.001
0.39
0.21
0.42
0.69
≤0.001
Data are presented as frequency with percent distribution.
When looking at other factors that had an influence in the occurrence of the crash, 63
(35.0%) patients indicated that speed was a contributor, regardless of riding above or below
the speed limit (for on-road motorcyclists) (Table 3). Forty-six (25.6%) patients admitted to
alcohol (n=41, 22.8%) or drug use (n=7, 3.9%) prior to the accident. Two (1.1%) patients
were under the influence of both alcohol and drugs. Ingested drugs included amphetamines,
cannabis and methadone. A small number of patients (n=7, 3.9%) stated that the weather was
a contributing factor in the accident, due to being hit by (a gust of) wind (n=4, 57.1%) or
being blinded by the sun (n=3, 42.9%). Road conditions were reported to be a contributing
factor in the crash in at least 55 (30.6%) patients. In 12 (6.7%) patients, a malfunction of the
motorcycle caused or contributed to the crash (e.g. damaged brake or accelerator cable, blown
tire).
Although the majority of MCAs were single vehicle accidents in both on-road and off-
road motorcyclists, on-road MCAs involved relatively more often other vehicles (p≤0.001)
(Table 3). However, while on-road motorcyclists were more likely to collide with a car
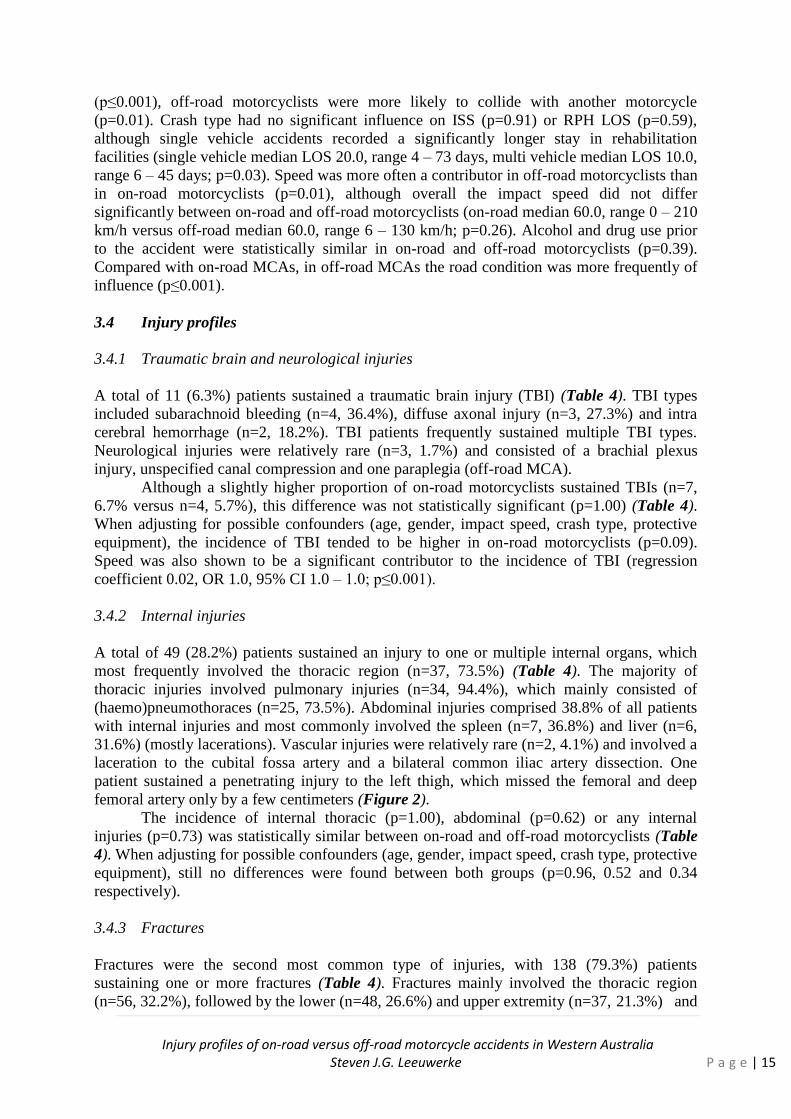
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 15
(p≤0.001), off-road motorcyclists were more likely to collide with another motorcycle
(p=0.01). Crash type had no significant influence on ISS (p=0.91) or RPH LOS (p=0.59),
although single vehicle accidents recorded a significantly longer stay in rehabilitation
facilities (single vehicle median LOS 20.0, range 4 – 73 days, multi vehicle median LOS 10.0,
range 6 – 45 days; p=0.03). Speed was more often a contributor in off-road motorcyclists than
in on-road motorcyclists (p=0.01), although overall the impact speed did not differ
significantly between on-road and off-road motorcyclists (on-road median 60.0, range 0 – 210
km/h versus off-road median 60.0, range 6 – 130 km/h; p=0.26). Alcohol and drug use prior
to the accident were statistically similar in on-road and off-road motorcyclists (p=0.39).
Compared with on-road MCAs, in off-road MCAs the road condition was more frequently of
influence (p≤0.001).
3.4 Injury profiles
3.4.1 Traumatic brain and neurological injuries
A total of 11 (6.3%) patients sustained a traumatic brain injury (TBI) (Table 4). TBI types
included subarachnoid bleeding (n=4, 36.4%), diffuse axonal injury (n=3, 27.3%) and intra
cerebral hemorrhage (n=2, 18.2%). TBI patients frequently sustained multiple TBI types.
Neurological injuries were relatively rare (n=3, 1.7%) and consisted of a brachial plexus
injury, unspecified canal compression and one paraplegia (off-road MCA).
Although a slightly higher proportion of on-road motorcyclists sustained TBIs (n=7,
6.7% versus n=4, 5.7%), this difference was not statistically significant (p=1.00) (Table 4).
When adjusting for possible confounders (age, gender, impact speed, crash type, protective
equipment), the incidence of TBI tended to be higher in on-road motorcyclists (p=0.09).
Speed was also shown to be a significant contributor to the incidence of TBI (regression
coefficient 0.02, OR 1.0, 95% CI 1.0 – 1.0; p≤0.001).
3.4.2 Internal injuries
A total of 49 (28.2%) patients sustained an injury to one or multiple internal organs, which
most frequently involved the thoracic region (n=37, 73.5%) (Table 4). The majority of
thoracic injuries involved pulmonary injuries (n=34, 94.4%), which mainly consisted of
(haemo)pneumothoraces (n=25, 73.5%). Abdominal injuries comprised 38.8% of all patients
with internal injuries and most commonly involved the spleen (n=7, 36.8%) and liver (n=6,
31.6%) (mostly lacerations). Vascular injuries were relatively rare (n=2, 4.1%) and involved a
laceration to the cubital fossa artery and a bilateral common iliac artery dissection. One
patient sustained a penetrating injury to the left thigh, which missed the femoral and deep
femoral artery only by a few centimeters (Figure 2).
The incidence of internal thoracic (p=1.00), abdominal (p=0.62) or any internal
injuries (p=0.73) was statistically similar between on-road and off-road motorcyclists (Table
4). When adjusting for possible confounders (age, gender, impact speed, crash type, protective
equipment), still no differences were found between both groups (p=0.96, 0.52 and 0.34
respectively).
3.4.3 Fractures
Fractures were the second most common type of injuries, with 138 (79.3%) patients
sustaining one or more fractures (Table 4). Fractures mainly involved the thoracic region
(n=56, 32.2%), followed by the lower (n=48, 26.6%) and upper extremity (n=37, 21.3%) and
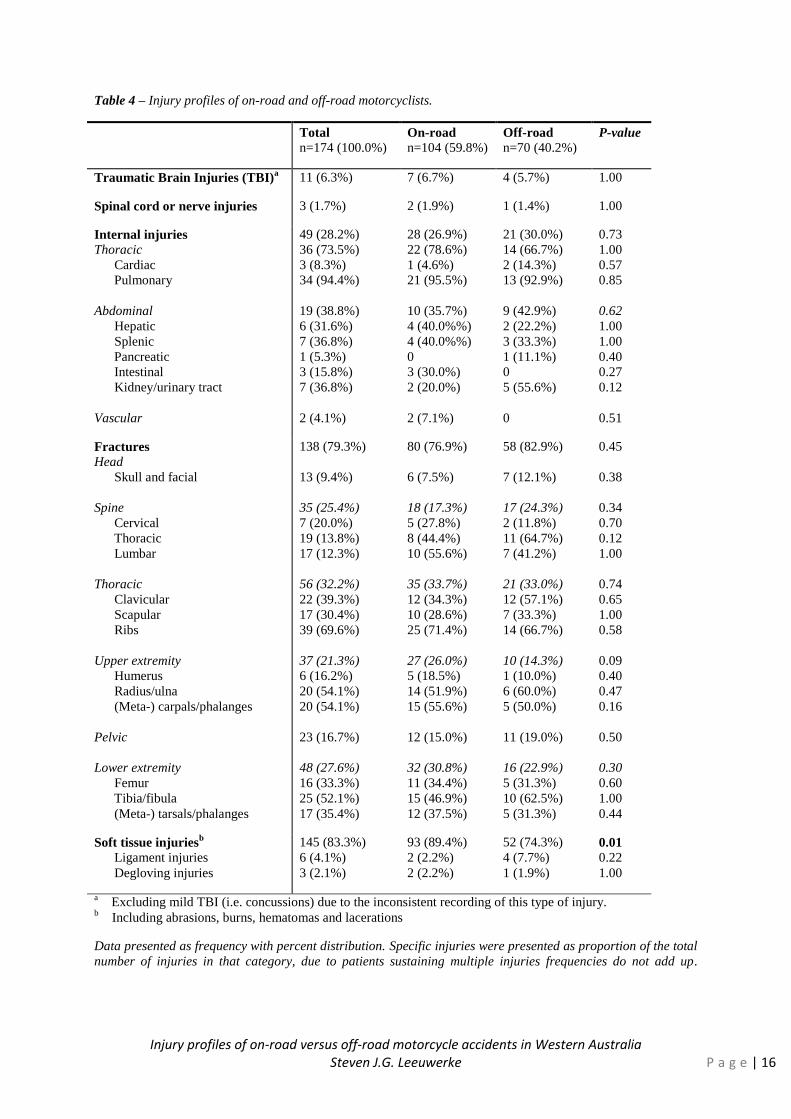
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | 16
Table 4 – Injury profiles of on-road and off-road motorcyclists.
Total n=174 (100.0%)
On-road n=104 (59.8%)
Off-road n=70 (40.2%)
P-value
Traumatic Brain Injuries (TBI)a 11 (6.3%) 7 (6.7%) 4 (5.7%) 1.00
Spinal cord or nerve injuries 3 (1.7%) 2 (1.9%) 1 (1.4%) 1.00
Internal injuries Thoracic
Cardiac
Pulmonary
Abdominal
Hepatic
Splenic
Pancreatic
Intestinal
Kidney/urinary tract
Vascular
49 (28.2%)
36 (73.5%)
3 (8.3%)
34 (94.4%)
19 (38.8%)
6 (31.6%)
7 (36.8%)
1 (5.3%)
3 (15.8%)
7 (36.8%)
2 (4.1%)
28 (26.9%)
22 (78.6%)
1 (4.6%)
21 (95.5%)
10 (35.7%)
4 (40.0%%)
4 (40.0%%)
0
3 (30.0%)
2 (20.0%)
2 (7.1%)
21 (30.0%)
14 (66.7%)
2 (14.3%)
13 (92.9%)
9 (42.9%)
2 (22.2%)
3 (33.3%)
1 (11.1%)
0
5 (55.6%)
0
0.73
1.00
0.57
0.85
0.62
1.00
1.00
0.40
0.27
0.12
0.51
Fractures
Head
Skull and facial
Spine
Cervical
Thoracic
Lumbar
Thoracic
Clavicular
Scapular
Ribs
Upper extremity
Humerus
Radius/ulna
(Meta-) carpals/phalanges
Pelvic
Lower extremity
Femur
Tibia/fibula
(Meta-) tarsals/phalanges
138 (79.3%)
13 (9.4%)
35 (25.4%)
7 (20.0%)
19 (13.8%)
17 (12.3%)
56 (32.2%)
22 (39.3%)
17 (30.4%)
39 (69.6%)
37 (21.3%)
6 (16.2%)
20 (54.1%)
20 (54.1%)
23 (16.7%)
48 (27.6%)
16 (33.3%)
25 (52.1%)
17 (35.4%)
80 (76.9%)
6 (7.5%)
18 (17.3%)
5 (27.8%)
8 (44.4%)
10 (55.6%)
35 (33.7%)
12 (34.3%)
10 (28.6%)
25 (71.4%)
27 (26.0%)
5 (18.5%)
14 (51.9%)
15 (55.6%)
12 (15.0%)
32 (30.8%)
11 (34.4%)
15 (46.9%)
12 (37.5%)
58 (82.9%)
7 (12.1%)
17 (24.3%)
2 (11.8%)
11 (64.7%)
7 (41.2%)
21 (33.0%)
12 (57.1%)
7 (33.3%)
14 (66.7%)
10 (14.3%)
1 (10.0%)
6 (60.0%)
5 (50.0%)
11 (19.0%)
16 (22.9%)
5 (31.3%)
10 (62.5%)
5 (31.3%)
0.45
0.38
0.34
0.70
0.12
1.00
0.74
0.65
1.00
0.58
0.09
0.40
0.47
0.16
0.50
0.30
0.60
1.00
0.44
Soft tissue injuriesb
Ligament injuries
Degloving injuries
145 (83.3%)
6 (4.1%)
3 (2.1%)
93 (89.4%)
2 (2.2%)
2 (2.2%)
52 (74.3%)
4 (7.7%)
1 (1.9%)
0.01 0.22
1.00
a Excluding mild TBI (i.e. concussions) due to the inconsistent recording of this type of injury.
b Including abrasions, burns, hematomas and lacerations
Data presented as frequency with percent distribution. Specific injuries were presented as proportion of the total
number of injuries in that category, due to patients sustaining multiple injuries frequencies do not add up.
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 17
spine (n=35, 20.1%). Pelvic and skull or facial fractures were slightly less common (n=23,
13.2% and n=13, 7.5% respectively). Thoracic fractures mainly involved rib fractures (n=39,
69.6%), followed by clavicular fractures (n=22, 39.3%). A slightly smaller proportion of
patients sustained a scapular fracture (n=17, 30.4%). Lower extremity fractures mainly
involved a tibial or fibular fracture (n=25, 52.1%). Upper extremity fractures most frequently
involved radial/ulnar and (meta)carpal fractures (both n=20, 54.1%). Spinal fractures mainly
involved fractures of the thoracic (n=19, 54.3%) and lumbar spine (n=17, 48.6%). A smaller
proportion involved cervical spine fractures (n=7, 20.0%). Additionally, 3 (1.7%) patients
sustained amputations (all on-road), which involved a traumatic amputation of a phalanx
(Figure 3), a traumatic amputation of the leg and an open tibial/fibial fracture combined with
a degloving injury which required surgical amputation of the lower leg.
No significant differences were observed in the occurrence of fractures between on-
road and off-road motorcyclists, although there was a tendency for on-road motorcyclists to
sustain more upper extremity fractures (p=0.09) (Table 4). When adjusting for possible
confounders (age, gender, impact speed, crash type, protective equipment), no differences
between both groups were found with respect to skull or facial fractures (p=0.32), spinal
fractures (p=0.26), thoracic fractures (p=0.29), upper extremity (p=0.13) or lower extremity
fractures (p=0.23). The incidence of upper extremity fractures was higher in multi vehicle
accidents (regression coefficient 1.1, OR 3.1, 95% CI 1.4 – 6.8; p=0.01) and was related to
impact speed, although not statistically significantly (p=0.06).
3.3.4 Soft tissue injuries
Soft tissue injuries (including abrasions, (full thickness) burns, lacerations and hematomas)
were the most common type of injury with 145 (83.3%) patients sustaining one or multiple
soft tissue injuries in at least one body region (Table 4). Most of these injuries were caused by
friction of the skin against the impact surface. A small proportion of accidents was caused by
other mechanisms such as penetrating injuries (Figure 4). The body regions that most
commonly sustained soft tissue injuries were the legs (n=107, 73.8%) and thorax, abdomen or
back (n=104, 71.7%), followed by the hands and wrists (n=59, 40.7%), the head and neck
(n=46, 31.7%) and feet and ankles (n=35, 24.1%). Ligament and degloving injuries occurred
relatively infrequent (n=6, 3.4% and n=3, 1.7% respectively).
Compared to on-road motorcyclists, a lower incidence of soft tissue injuries to any
body region (p≤0.001) was seen in off-road motorcyclists (Table 4). When adjusting for
possible confounders (age, gender, impact speed, crash type, protective equipment), the
incidence of soft tissue injuries to any body region were statistically similar between on-road
and off-road motorcyclists (p=0.24). The occurrence of soft tissue injuries was related to
speed (regression coefficient 0.03, OR 1.0, 95% CI 1.0 – 1.0) and multi vehicle accidents
(regression coefficient 2.0, OR 7.0, 95% CI 1.5 – 33.1).
3.4 Motorcycle clothing
3.4.1 Frequency of use
Overall, only a minority of patients wore full protective equipment at the time of the accident
(n=24, 13.3%) and even less patients had body armour imbedded in all parts of clothing
(n=18, 10.0% of total) (Table 5). Helmets were the most common type of motorcycle clothing
worn (n=156, 86.7%), followed by gloves (n=90, 50.0%), jackets or impact protectors (n=67,
37.2%), boots (n=65, 36.1%) and pants (n=51, 28.3%). A considerable proportion of patients
owned, but did not wear (parts of) motorcycle clothing at the time of the accident (full

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | 18
Figure 2 – A near-miss: this multi vehicle accident
(on-road) resulted in the motorbike’s handlebar
penetrating the left thigh, barely missing the
femoral and deep femoral artery. From left to right:
A. the handlebar entered the left medial thigh in
anterior-posterior direction and is penetrating the
skin and quadriceps muscle. B. the entry wound
after extraction of the handlebar. C. the wound
after debridement. Visible are the left femoral and
deep femoral artery which was missed a few
centimetres. D. a vacuum dressing was applied,
with negative pressure on the wound surface to
promote healing. The wound was closed by a few
days later . E. the handlebar after extraction from
the wound.
Figure 3 – Anterior-posterior (AP) and lateral view
of the left hand following a motorcycle versus car
(on-road) at 80 km/h. The x-ray clearly shows a
traumatic amputation of the left thumb. An avulsion
fracture of the left ulnar styloid process can also be
seen.
Figure 4 – this patient lost control over his dirt
bike after hitting a rock and subsequently swerved
into a bush, impaling his right hip on a branch
equipment n=3, 1.7%; jacket/impact protector n=45, 25.0%; pants n=30, 16.7%; boots n=26,
14.4% and gloves n=40, 22.2%).
When comparing any motorcycle clothing (with and without body armour) worn
between on-road and off-road motorcyclists, off-road motorcyclists wore full equipment
(p=0.02), pants (≤0.001) and boots (≤0.001) significantly more often than on-road
motorcyclists did (Table 5). Only 7 (6.5%) on-road and 11 (15.3%) off-road motorcyclists
wore full equipment with body armour embedded in all parts. Controversially, off-road
motorcyclists less frequently wore helmets (off-road n=56, 77.8% versus on-road n=100,
92.6%; p=0.01). The use of any jackets/impact protectors and any gloves was similar in both
groups (p=0.27 and 0.65 respectively). There were relatively more off-road motorcyclists that
owned, but did not wear full equipment (any) or a helmet, but neither of these differences
were statistically significant (p=0.06 and 0.07 respectively). On-road motorcyclists owned,
but did not wear gloves significantly more often than did off-road motorcyclists (p≤0.001),
although off-road motorcyclists tended to own, but not wear gloves with body armour more
frequently (p=0.09). The main reasons for patients not wearing motorcycle clothing that they
owned were: too much effort to put it on or only going for a short ride (n=40, 44.0%), too hot
(n=18, 19.9%), inconvenient (n=8, 8.8%), did not expect to ride (n=6, 6.6%), lost/lend out

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 19
(n=3, 3.3%) or other/unspecified (n=15, 16.5%). Fifty-five (30.6%) patients expressed a
regret not to have worn more motorcycle clothing (on-road n=33, 30.6% versus off-road
n=22, 30.6%; p=1.00).
Additional protection that was worn exclusively by off-road motorcyclists included
neck braces (n=8, 11.1%) and knee pads or shin guards (n=15, 20.8%) (Table 5). A small
number of patients owned, but did not wear a neck brace (n=4, 5.6%) or knee pads/shin
guards (n=7, 9.7%) at the time of the accident. Kidney belts were mostly worn by off-road
motorcyclists (off-road n=9, 12.5% versus on-road n=1, 0.9%; p=0.05), although statistically
similar proportion of patients owned, but did not wear a kidney belt (on-road n=5, 4.6%
versus off-road n=5, 6.9%; p=0.52).
3.4.2 Effectiveness in preventing injuries
Full equipment
When adjusting for possible confounders (age, gender, impact speed, crash type), patients not
wearing full equipment did not sustain significantly more internal injuries than did patients
that were wearing full equipment with full or partial body armour (p=0.38), but tended to
sustain less fractures (p=0.06) and soft tissue injuries (p=0.08) in any body region (Table 6).
Helmets
Patients that did not wear a helmet were more at risk of TBI (regression coefficient 2.4, OR
11.3, 95% CI 1.9 – 69.3; p=0.04), facial or skull fractures (regression coefficient 1.9, OR 6.4,
95% CI 1.8 – 22.6; p=0.01) and facial soft tissue injuries (regression coefficient 1.3, OR 3.6
1.2 – 11.2; p=0.03) compared with those that did wear a helmet (Table 6).
Jackets/impact protectors
Jackets without body armour were not shown to be protective against thoracic and abdominal
internal injuries (p=0.46), thoracic fractures (p=0.28) or soft tissue injuries in that body area
(including the back and arms) (p=0.53) (Table 6). Although jackets and impact protectors
with body armour were also not protective against thoracic and abdominal internal injuries
(p=0.74) or thoracic fractures (p=0.48), they were protective against soft tissue injuries in that
body region (regression coefficient 1.5, OR 4.3, 95% CI 2.0 – 9.1; p≤0.001).
Pants
Pants without body armour were not shown to be protective against lower extremity fractures
(femoral, tibial or fibular) (p=0.22) or soft tissue injuries in that body region (p=0.61) (Table
6). Pants with body armour were shown to be protective against soft tissue injuries of the
lower extremity (regression coefficient 1.2, OR 3.2, 95% CI 1.4 – 7.5; p=0.01), but also did
not protect against lower extremity fractures (p=0.22).
Boots
Although boots were not shown to protect against lower extremity fractures (tibial, fibial or
and (meta-)tarsal) (p=0.65), they did protect against soft tissue injuries of the ankle and feet
(regression coefficient 2.7, OR 14.9, 95% CI 3.1 – 70.9; p≤0.001) (Table 6).
Gloves
Gloves without body armour were not shown to protect against (meta-)carpal and phalangeal
fractures (p=0.55), nor protected against soft tissue injuries of the hands (p=0.10) (Table 6).
Further, gloves with body armour were also not found to protect against fractures (p=0.10) or
soft tissue injuries (p=0.10). Speed was identified as a risk factor for both (meta-)carpal and

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | 20
Table 5 – Frequency of motorcycle clothing that was worn and not worn in on-road and off-road motorcyclists.
Total (n=180, 100%) Worn Not worn
On-road (n=108, 60.0%) Worn Not worn
Off-road (n=72, 40.0%) Worn Not worn
P-value
Worn Not worn
Full equipment (any)
With full BA
Helmet
Jacket/impact protector (any)
With BA
Pants (any)
With BA
Boots
Gloves (any)
With BA
24 (13.3%) 3 (1.7%)
18 (75.0%) 2 (66.7%)
156 (86.7%) 16 (8.9%)
67 (37.2%) 45 (25.0%)
59 (88.1%) 38 (84.4%)
51 (28.3%) 30 (16.7%)
41 (80.4%) 24 (80.0%)
65 (36.1%) 26 (14.4%)
90 (50.0%) 40 (22.2%)
69 (76.7%) 28 (70.0%)
9 (8.3%) 0
7 (77.8%) 0
100 (92.6%) 6 (5.6%)
44 (40.7%) 32 (29.6%)
36 (81.8%) 26 (81.3%)
15 (13.9%) 20 (18.5%
14 (93.3%) 15 (75.0%)
25 (23.1%) 15 (13.9%)
52 (48.1%) 32 (29.6%)
41 (78.9%) 21 (65.6%)
15 (20.8%) 3 (4.2%)
11 (73.3%) 2 (66.7%)
56 (77.8%) 10 (13.9%)
23 (31.9%) 13 (18.1%)
23 (100.0%) 12 (92.3%)
36 (50.0%) 10 (13.9%)
27 (75.0%) 9 (90.0%)
40 (55.6%) 11 (15.3%)
38 (52.8%) 8 (11.1%)
28 (73.7%) 7 (87.5%)
0.02 0.06
0.07 0.16
0.01 0.07
0.27 0.08
0.87 0.27
≤0.001 0.54
≤0.001 0.83
≤0.001 0.83
0.65 ≤0.001
0.75 0.09
Data are presented as frequency with percent distribution. With and without body armour distributions are presented as proportion of any protective equipment of that type.
Table 6 – Risk of not wearing any motorcycle clothing compared to wearing motorcycle clothing with or without body armour (BA, reference) in sustaining internal injuries,
fractures and soft tissue injuries in the corresponding body region, adjusting for possible confounders (age, gender, impact speed and crash type).
Protection worn (reference) Regression
coefficient
Internal injuries
Adj. OR (95% CI)
P-value Regression
coefficient
Fractures
Adj. OR (95% CI) P-value Regression
coefficient
Soft tissue injuries Adj. OR (95% CI)
P-value
Full equipment without BA or partial
Full equipment with BA
Helmet
Jacket without BA
Jacket with BA or impact protector
Pants without BA
Pants with BA
Boots
Gloves without BA
Gloves with BA
n/s
n/s
2.4
n/s
n/s
-
-
-
-
-
n/s
n/s
11.3 (1.9 – 69.3)
n/s
n/s
-
-
-
-
-
0.38
0.38
0.01
0.46
0.74
-
-
-
-
-
n/s
n/s
1.9
n/s
n/s
n/s
n/s
n/s
n/s
n/s
n/s
n/s
6.4 (1.8 – 22.6)
n/s
n/s
n/s
n/s
n/s
n/s
n/s
0.06
0.06
≤0.001
0.28
0.48
0.22
0.22
0.06
0.55
0.10
n/s
n/s
1.3
n/s
1.5
n/s
1.2
2.7
n/s
n/s
n/s
n/s
3.6 (1.2 – 11.2)
n/s
4.3 (2.0 – 9.1)
n/s
3.2 (1.4 – 7.5)
14.9 (3.1 – 70.9)
n/s
n/s
0.08
0.08
0.03 0.53
≤0.001 0.61
0.01
≤0.001 0.10
0.10
Data are presented as regression coefficient and odds ratio (OR) with 95% confidence interval (CI), comparing wearing protective equipment (reference) with wearing no
protection.
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia Steven J.G. Leeuwerke P a g e | 21
phalangeal fractures (regression coefficient 0.02, OR 1.0, 95% CI 1.0 – 1.0; p=0.01) and soft
tissue injuries of the hands (regression coefficient 0.01, OR 1.0, (95% CI 1.0 – 1.0; p=0.03).
Although multi vehicle accidents were shown to be a risk factor for soft tissue injuries
(regression coefficient 0.01, OR 3.7, 95% CI 1.8 – 7.8; p≤0.001), crash type was not of
statistical significant influence for fractures (p=0.11).
3.5 Outcomes three months after the accident
3.5.1 Demographics
Eighty-seven (48.3%) of the total of 180 included patients that reached 3 months after the
accident within the study period completed the follow-up interview. Of these, 51 (58.6%)
accidents occurred on-road and 36 (41.4%) accidents occurred off-road. Patients were
predominantly male (n=76, 87.4%) with ages ranging from 14 to 68 years (median 30.0
years). Most patients were single (n=38, 43.7%), followed by married (n=23, 26.4%), defacto
(n=18, 20.7%) or divorced or separated (n=8, 9.2%).
Although off-road motorcyclists tended to be younger, this difference was not
significant (off-road median 27.5, range 14 – 53 years versus on-road median 34.0, range 14 –
68 years; p=0.064). Injury severity was not significantly different between on-road and off-
road motorcyclists (on-road median ISS 9.00, range 1 – 38 versus off-road median ISS 9.50,
range 1 – 29; p=0.597). Impact speed was statistically similar between both groups (p=0.74).
3.5.2 Physical health
Overall, 66 (75.9%) patients reported to be in good to excellent general health three months
after the accident, although 58 (66.7%) patients indicated to be in a worse condition compared
to the situation prior to the accident (Table 7a). Twenty-two (25.3%) patients indicated no
health change and in 7 (8.0%) patients health was even improved, because they felt stronger
or fitter due to increased exercise (n=2, 28.6%), losing weight (n=2, 28.6%), getting life back
on track (n=2, 28.6%) or stopped smoking (n=1, 14.3%). Most patients still experienced
problems during daily activities (n=55, 63.2%), mostly minor in nature (n=47, 85.5%). A
minority of patients experienced many problems (n=8, 14.6%). Pain or discomfort during rest
or activities was reported in 63 (72.4%) patients. Increased fatigue compared to the situation
prior to the accidents was reported in 35 (40.2%) patients, mostly throughout the day (n=20,
57.1%) or after light or heavy activities (n=15, 42.9%). Thirty-nine (44.8%) patients reported
to have (almost) completely recovered, 25 (28.7%) to have recovered for a great part and 23
(26.4%) patients felt they had only recovered a bit or not recovered at all.
Compared with on-road motorcyclists, off-road motorcyclists generally reported to be
in better general health (p=0.02), reported better health compared to the situation prior to the
accident (p=0.05), reported less often problems with daily activities (p≤0.001) and reported
overall a better recovery (p≤0.001) (Table 7a). Off-road motorcyclists also tended to report
pain less frequently and reported less frequently an increase in fatigue, although these
difference did not reach statistical significance (p=0.06 and 0.08 respectively). When
adjusting for possible confounders (age, gender, impact speed, crash type and ISS), on-road
motorcyclists still showed a higher risk of reporting daily problems (regression coefficient
1.9, OR 6.6, 95% CI 1.9 – 14.5; p≤0.001) (Table 7b). ISS also was a risk factor for daily
problems (regression coefficient 0.1, OR 1.1, 95% CI 1.0 – 1.3; p=0.02). Speed tended to be a
risk factor for daily problems, but this did not reach statistical significance (p=0.09). Reported
pain was not significantly different between on-road and off-road motorcyclists after adjusting
(p=0.35), but was related to age (regression coefficient 0.1, OR 1.1, 95% CI 1.0 – 1.1;
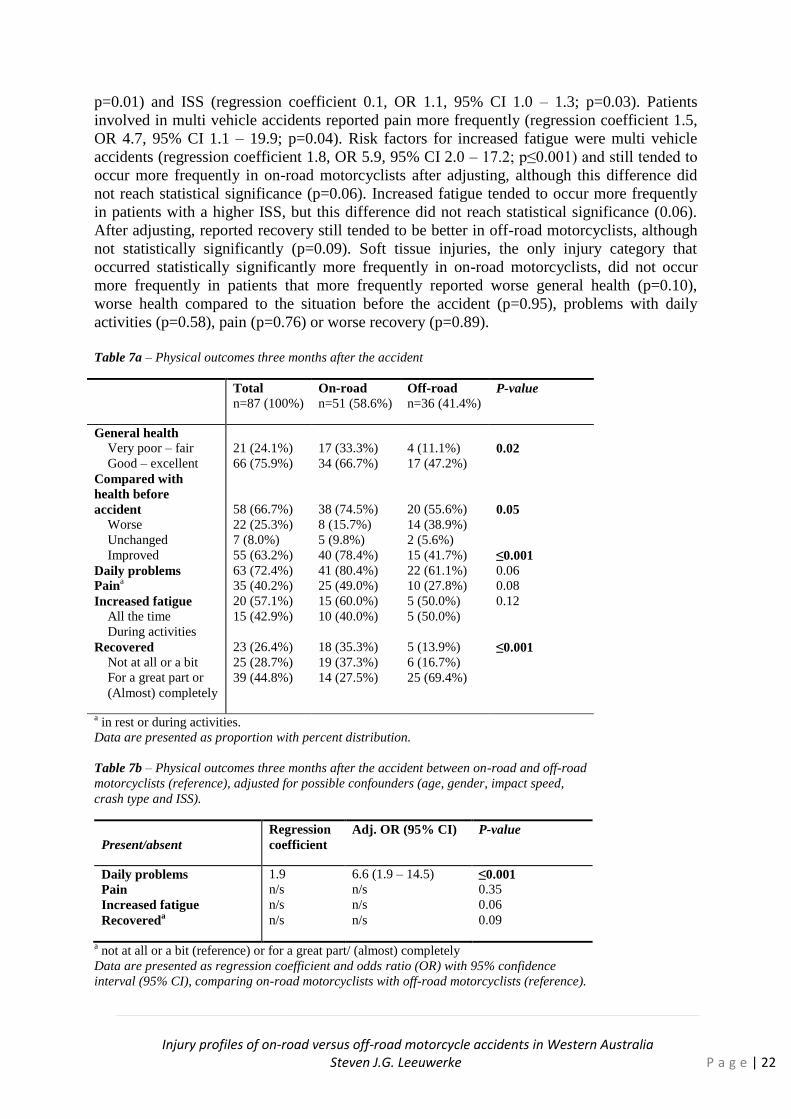
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 22
p=0.01) and ISS (regression coefficient 0.1, OR 1.1, 95% CI 1.0 – 1.3; p=0.03). Patients
involved in multi vehicle accidents reported pain more frequently (regression coefficient 1.5,
OR 4.7, 95% CI 1.1 – 19.9; p=0.04). Risk factors for increased fatigue were multi vehicle
accidents (regression coefficient 1.8, OR 5.9, 95% CI 2.0 – 17.2; p≤0.001) and still tended to
occur more frequently in on-road motorcyclists after adjusting, although this difference did
not reach statistical significance (p=0.06). Increased fatigue tended to occur more frequently
in patients with a higher ISS, but this difference did not reach statistical significance (0.06).
After adjusting, reported recovery still tended to be better in off-road motorcyclists, although
not statistically significantly (p=0.09). Soft tissue injuries, the only injury category that
occurred statistically significantly more frequently in on-road motorcyclists, did not occur
more frequently in patients that more frequently reported worse general health (p=0.10),
worse health compared to the situation before the accident (p=0.95), problems with daily
activities (p=0.58), pain (p=0.76) or worse recovery (p=0.89).
Table 7a – Physical outcomes three months after the accident
Total
n=87 (100%)
On-road
n=51 (58.6%)
Off-road
n=36 (41.4%) P-value
General health
Very poor – fair
Good – excellent
Compared with
health before
accident Worse
Unchanged
Improved
Daily problems
Paina
Increased fatigue All the time
During activities
Recovered Not at all or a bit
For a great part or
(Almost) completely
21 (24.1%)
66 (75.9%)
58 (66.7%)
22 (25.3%)
7 (8.0%)
55 (63.2%)
63 (72.4%)
35 (40.2%)
20 (57.1%)
15 (42.9%)
23 (26.4%)
25 (28.7%)
39 (44.8%)
17 (33.3%)
34 (66.7%)
38 (74.5%)
8 (15.7%)
5 (9.8%)
40 (78.4%)
41 (80.4%)
25 (49.0%)
15 (60.0%)
10 (40.0%)
18 (35.3%)
19 (37.3%)
14 (27.5%)
4 (11.1%)
17 (47.2%)
20 (55.6%)
14 (38.9%)
2 (5.6%)
15 (41.7%)
22 (61.1%)
10 (27.8%)
5 (50.0%)
5 (50.0%)
5 (13.9%)
6 (16.7%)
25 (69.4%)
0.02
0.05
≤0.001 0.06
0.08
0.12
≤0.001
a in rest or during activities.
Data are presented as proportion with percent distribution.
Table 7b – Physical outcomes three months after the accident between on-road and off-road
motorcyclists (reference), adjusted for possible confounders (age, gender, impact speed,
crash type and ISS).
Present/absent
Regression
coefficient
Adj. OR (95% CI) P-value
Daily problems
Pain
Increased fatigue
Recovereda
1.9
n/s
n/s
n/s
6.6 (1.9 – 14.5)
n/s
n/s
n/s
≤0.001
0.35
0.06
0.09
a not at all or a bit (reference) or for a great part/ (almost) completely
Data are presented as regression coefficient and odds ratio (OR) with 95% confidence
interval (95% CI), comparing on-road motorcyclists with off-road motorcyclists (reference).
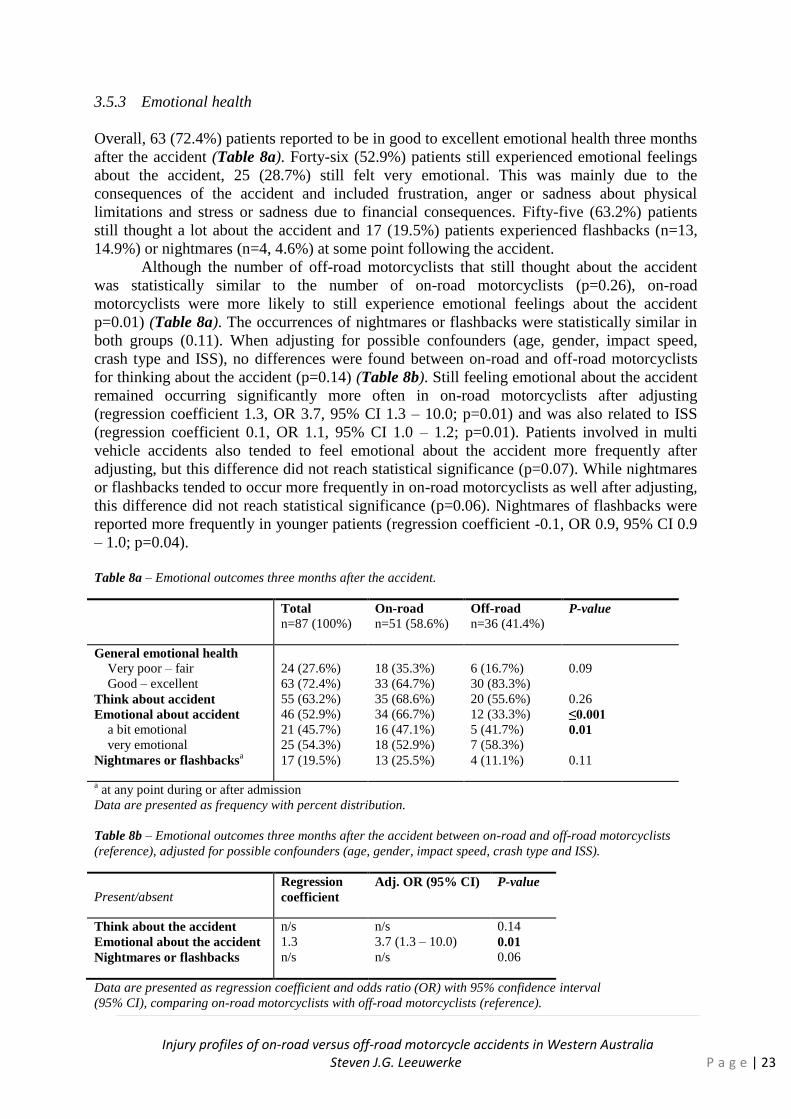
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 23
3.5.3 Emotional health
Overall, 63 (72.4%) patients reported to be in good to excellent emotional health three months
after the accident (Table 8a). Forty-six (52.9%) patients still experienced emotional feelings
about the accident, 25 (28.7%) still felt very emotional. This was mainly due to the
consequences of the accident and included frustration, anger or sadness about physical
limitations and stress or sadness due to financial consequences. Fifty-five (63.2%) patients
still thought a lot about the accident and 17 (19.5%) patients experienced flashbacks (n=13,
14.9%) or nightmares (n=4, 4.6%) at some point following the accident.
Although the number of off-road motorcyclists that still thought about the accident
was statistically similar to the number of on-road motorcyclists (p=0.26), on-road
motorcyclists were more likely to still experience emotional feelings about the accident
p=0.01) (Table 8a). The occurrences of nightmares or flashbacks were statistically similar in
both groups (0.11). When adjusting for possible confounders (age, gender, impact speed,
crash type and ISS), no differences were found between on-road and off-road motorcyclists
for thinking about the accident (p=0.14) (Table 8b). Still feeling emotional about the accident
remained occurring significantly more often in on-road motorcyclists after adjusting
(regression coefficient 1.3, OR 3.7, 95% CI 1.3 – 10.0; p=0.01) and was also related to ISS
(regression coefficient 0.1, OR 1.1, 95% CI 1.0 – 1.2; p=0.01). Patients involved in multi
vehicle accidents also tended to feel emotional about the accident more frequently after
adjusting, but this difference did not reach statistical significance (p=0.07). While nightmares
or flashbacks tended to occur more frequently in on-road motorcyclists as well after adjusting,
this difference did not reach statistical significance (p=0.06). Nightmares of flashbacks were
reported more frequently in younger patients (regression coefficient -0.1, OR 0.9, 95% CI 0.9
– 1.0; p=0.04).
Table 8a – Emotional outcomes three months after the accident.
Total
n=87 (100%)
On-road
n=51 (58.6%)
Off-road
n=36 (41.4%) P-value
General emotional health
Very poor – fair
Good – excellent
Think about accident
Emotional about accident a bit emotional
very emotional
Nightmares or flashbacksa
24 (27.6%)
63 (72.4%)
55 (63.2%)
46 (52.9%)
21 (45.7%)
25 (54.3%)
17 (19.5%)
18 (35.3%)
33 (64.7%)
35 (68.6%)
34 (66.7%)
16 (47.1%)
18 (52.9%)
13 (25.5%)
6 (16.7%)
30 (83.3%)
20 (55.6%)
12 (33.3%)
5 (41.7%)
7 (58.3%)
4 (11.1%)
0.09
0.26
≤0.001
0.01
0.11
a at any point during or after admission
Data are presented as frequency with percent distribution.
Table 8b – Emotional outcomes three months after the accident between on-road and off-road motorcyclists
(reference), adjusted for possible confounders (age, gender, impact speed, crash type and ISS).
Present/absent
Regression
coefficient
Adj. OR (95% CI) P-value
Think about the accident
Emotional about the accident
Nightmares or flashbacks
n/s
1.3
n/s
n/s
3.7 (1.3 – 10.0)
n/s
0.14
0.01
0.06
Data are presented as regression coefficient and odds ratio (OR) with 95% confidence interval
(95% CI), comparing on-road motorcyclists with off-road motorcyclists (reference).
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 24
3.5.4 Return to work and financial loss
A total of 75 (86.2%) patients were employed prior to the accident and had recorded a total of
677 weeks of absence until three months after the accidents. Of these, thirty-five (46.7%)
patients were unable to return to full or partial employment within three months after the
accident. Most employed patients lost income (n=53, 70.7%), with most patients losing more
than 2000 AUD per month (<500 AUD n=2, 2.7%; 500-1000 AUD n=2, 2.7%; 1000-2000
n=12, 16.0%; >2000 n=36, 48.0%). Multiple patients lost over 10.000 AUD per month.
Return to work was similar between on-road and off-road motorcyclists (on-road
n=25, 49.0% versus off-road n=15, 41.7%; p=0.65), as was lost income (p=0.58). Return to
work was associated with ISS (returned median ISS 5.00 (1 – 29) versus not returned median
ISS 11.0 (1 – 38); p≤0.001).
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 25
4. Discussion
The primary objective of this study was to investigate the differences between on-road and
off-road MCAs with respect to injury severity, injury profiles, and the impact on perceived
health status three months after the accident. The aim was to increase awareness on the
gravity of off-road motorcycle trauma and to provide suggestions towards trauma prevention
in this group of patients.
4.1 Rider characteristics, accident cause and mechanism
Although the primary aim was not to compare on-road and off-road MCAs with respect to
cause, mechanism or risk factors, some interesting differences were found. A considerable
proportion of off-road motorcyclists rode on someone else’s motorcycle in the present study
(22.2%) which was significantly more often than on-road motorcyclists. Further, 40.0% of all
patients that had an accident on their own motorcycle had ridden this specific motorcycle for
less than a year. Only 6.3% of all motorcyclists had been riding motorcycles for less than a
year. Although no conclusions on risk factors for having an accident can be drawn from the
present study due to the absence of motorcyclists that did not have an accident, this may
suggest that unfamiliarity with the motorcycle may be a risk factor for having an accident,
which would be in keeping with previous literature [50].
While similar proportions of off-road MCAs were single vehicle accidents, the
proportion of single vehicle MCAs in on-road accidents was considerably higher than
previously reported by Cassell et al. (39.8% versus 53.7% in the present study) [16]. The
observed difference may be explained by the fact that 26.8% of accidents in their study were
unspecified (versus 3.9% in the present study). Although off-road motorcyclists still more
often involved single vehicle accidents than on-road motorcyclists, they were more likely to
collide with other motorcyclists, a finding that is supported by Cassell et al. [16].
Losing control in a corner, which has previously been identified as a risk factor for
MCAs [22], also caused a considerable number of on-road and off-road MCAs in the current
study (11.7%), often in combination with speed. Road conditions in general were much more
often an accident contributor in off-road motorcyclists than in on-road motorcyclists, as may
be expected due to the differences in terrain. However, an alarming proportion of off-road
accidents were caused by riding into an unexpected drop or ditch, which stresses the
importance of knowledge about the terrain in which in is ridden. Rider education through
general campaigns or local motorcycling clubs may be an effective way of achieving this.
When looking at preventable causes or contributors to the accident, an alarming
proportion of patients (25.6%) were found to have consumed alcohol or drugs prior to the
accident. Although comparison is difficult because of differences in definitions, other studies
also found intoxication to be of influence to the crash in a considerable number of accidents.
Cunningham et al. found that 6% of all accidents in their study were solely caused by alcohol
or drug intoxication and Steinhardt et al. reported that up to 53% and 40% of off-road and on-
road motorcyclists respectively had used alcohol 24 hours before the accident [6,39].
Although Steinhardt et al. found illicit drug use to be higher in off-road motorcyclists, the
results from the present study did not show a significant difference between both groups. With
the true number of accidents influenced by substance use probably lying somewhere in the
middle, it remains a completely preventable cause of a considerable number of accidents and
should remain an important focus for injury prevention in both on-road and off-road
motorcyclists. Another important finding was the higher contribution of speed in off-road
MCAs (off-road 48.6% versus on-road 25.9%). Although it has been suggested that off-road

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 26
motorcyclists usually ride at lower speeds [16,42], the present study did not find significant
differences in impact speed between both groups. This is surprising, given the fact that off-
road motorcyclists usually ride in much rougher terrain and it is more difficult to stay in
control at high speeds in such conditions. This suggest that misappropriate speeds for the
condition in which in is ridden is a bigger factor off-road than it is on-road and may be related
to risk-taking behaviour, which has been found to occur more frequently in younger people
[12]. Indeed, off-road motorcyclists were found to be younger than on-road motorcyclists in
the present study, which is consistent with earlier findings [13,16,42]. Although
misappropriate speed for conditions in which in is ridden has been related to a higher risk of
multiple vehicle collisions [12], this effect has not been reported previously in off-road
motorcyclists. Another completely preventable cause were motorcycle malfunctions, which
contributed to or caused 6.7% of all accidents.
A considerable proportion of patients had been involved in previous MCAs (71.1%)
and many had been hospitalized before due to a MCA before (31.7%). Because the present
study did not differentiate between the location where the previous accidents had occurred,
some on-road motorcyclists also rode an off-road motorcycle (and vice versa) and some
accidents occurred during racing, conclusions on the risk for off-road motorcyclists to crash
compared to on-road motorcyclists could not be drawn. Nonetheless, off-road motorcyclists
still tended to have been involved in an accident before more frequently than on-road
motorcyclists. Although no difference in previous hospitalization was found between both
groups, Meuleners et al. found that off-road motorcyclists have a higher risk of hospitalization
compared to on-road motorcyclists in patients presenting to the ED [33]. In contrast, Grange
et al. found no differences in the proportion of patients that were admitted between both
groups [42]. With accurate data on the number of off-road motorcyclists that have an accident
in relation to the exposure and distance travelled being absent, the relative accident rate
between on-road and off-road motorcyclists remains unclear.
4.2 Injury severity and injury profiles
Most importantly, no significant differences between on-road and off-road motorcyclists were
found in terms of ISS, hospital length of stay (including ICU and rehabilitation facilities) or
discharge location. These results contradict the findings from Cassell et al. and Mikocka-
Walus et al., who both found a shorter hospital length of stay in off-road motorcyclists
[13,16]. Further, Mikocka-Walus et al. found that off-road motorcyclists had a lower ISS, a
shorter ICU stay and were more likely to be discharged home, whereas on-road motorcyclists
were more likely to be discharged to a rehabilitation facility [13]. Although Grange et al. also
did not detect a significant difference in ISS between both groups, there was a tendency for
on-road motorcyclists to have a higher ISS. The observed differences with the present study
may reflect local differences and are likely unrelated to the fact that the patient population in
the present study tended to include more severely injured patients, as the study of Mikocka-
Walus et al. focused on major trauma patients.
Injury profiles were not statistically significantly different between on-road and off-
road motorcyclists with the exception of soft tissue injuries, which were overall the most
common type of injuries (83.3%). The higher incidence of soft tissue injuries in on-road
motorcyclists is consistent with the findings of Grange et al. and is likely to be related to the
higher proportion of off-road motorcyclists that wore motorcycle clothing. Indeed, when
adjusting for possible confounders (including motorcycle clothing), the difference between
both groups disappeared. Although all traumatic amputations occurred in on-road
motorcyclists, no statistically significant differences were found between on-road and off-road
motorcyclists due to the low incidence of this injury type. Similar incidences between both
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 27
groups have been reported by Cassell et al. [16]. Although also not statistically significant, the
incidence of TBIs tended to be higher in on-road motorcyclists after adjusting, despite the
higher proportion of off-road motorcyclists that did not wear a helmet, as did the incidence of
upper extremity fractures, which was shown to be related to multi vehicle accidents. Overall,
the incidence of TBI, nerve or spinal cord injuries was relatively low compared to other
studies [14,15,42], but was consistent with the findings of Cassell et al. [16]. Fractures were
the second most common injury with 79.3% of patients sustaining one or more fractures.
Thoracic fractures were the most common (32.2%), followed by lower extremity (27.6%),
spinal (25.4%) and upper extremity fractures (21.3%). Ankarath et al., who reported injury
profiles in a similar fashion, found similar incidences of internal injuries, although they
reported a higher incidence of fractures (94.3%) and a lower incidence of spinal fractures
(10.4% versus 25.4% in the present study) [15]. The present study also found a higher
proportion of cervical spine fractures compared with other studies (20.0% versus
approximately 10%) [14,15]. Although not entirely comparable due to the different
classification systems, Mikocka-Walus found similar injury profiles with thoracic injuries
being the most common, followed by lower extremity injuries [13]. However, they found that
on-road motorcyclists sustained upper extremity, lower extremity and head injuries
significantly more often than off-road motorcyclists [13]. As discussed, the present study also
found that on-road motorcyclists tended to sustain upper extremity fractures and TBIs more
frequently, although this difference did not reach statistical significance.
4.3 Motorcycle clothing
Due to relatively low incidences of certain injury categories, the protective effect of
motorcycle clothing was analyzed for on-road and off-road motorcyclists combined. Overall,
no protective effect of motorcycle clothing was shown in preventing internal injuries or
fractures, with the exception of helmets. Although the incidence of lower extremity fractures
was lower when boots were worn, this effect was not statistically significant. However, with
the exception of gloves, all motorcycle clothing with body armour imbedded in it was shown
to protect significantly against soft tissue injuries, whereas clothing without body armour had
no significant effect on the incidence of soft tissue injuries. These findings are largely
consistent with findings of de Rome et al., with the exception of gloves which were found to
protect in their study [41]. Although the present study did not separate between any soft tissue
injuries and open wounds, the results from this study also suggest an effect of motorcycling
clothing with or without body armour in preventing open wounds [41].
Despite the observed protective effect, only 13.3% of all patients wore full protective
equipment during the accident of which only 75.0% had body armour embedded in all parts of
the equipment. Off-road motorcyclists wore full protective equipment considerably more
often than did on-road motorcyclists (20.8% versus 8.3% of on-road motorcyclists), which
may be related to a general higher anticipation of having an accident in off-road
motorcyclists. Although most patients did not own full equipment, a considerable proportion
of patients owned, but did not wear (all) motorcycle clothing during the accident, for which
the main reasons were that it was too much effort to put on, they were only going for a short
ride or that it was too hot. Helmet use was considerably lower in off-road motorcyclists
(77.8% versus 92.6% in on-road motorcyclists), which supports earlier literature [26,39]. This
is concerning, especially considering that impact speed was found to be similar in on-road and
off-road motorcyclists, in contrast to what has been thought previously. Helmets have been
found to be less effective in preventing fatal head injuries at higher speeds [12], although this
may be due to differences in road characteristics [6]. Controversially, on-road motorcyclists
tended to sustain TBIs more often when adjusting for helmet use and speed.

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 28
4.4 Outcomes three months after the accident
Overall, many patients reported worse health than before the accident (66.7%), problems with
daily activities (63.2%) and pain (72.4%) and a considerable proportion of patients reported
no recovery or only to have recovered a bit (26.4%). Fatigue was also very common (40.2%
of patients) and most of these patients felt tired throughout the day (57.1%). Many patients
felt emotional about the accident (52.9%) and a considerable proportion of patients reported
inconvenience or distress by flashbacks or nightmares (19.5%). The financial burden for the
patient was high as well, with 70.7% of patients losing income, of which almost half (48.0%)
lost more than 2000 AUD each month. With approximately half (50.6%) of all patients that
were followed up being single or divorced/separated men, who are likely to be the sole
breadwinner in their household, the financial impact on patients was likely high. A substantial
proportion (46.7%) were not able to return to partial or full employment three months after
the accident and were therefore at risk of losing their job. Although employees can not be
dismissed due to temporary absence or illness under Australian law, after 3 months this right
expires [51]. Not only may this have a big influence on patient’s personal situation, it may
also be a financial burden to society in terms of unemployment benefits, which add up to the
societal costs for hospital admission and treatment. Further, earlier research has shown that
most long-term disability following MCAs involve problems with locomotion or dexterity at
work, which seems to be in keeping with the large proportion of patients reporting increase
fatigue. Earlier findings of de Rome et al. 2012, although limited to on-road MCAs, support
the findings that MCAs have a big influence on the patient. They reported that less than half
of all patients were riding pain free 6 months after the accident, that 8% reporting some
extend of disability and 13% still had not returned to the work role they occupied before the
accident [52]. They also found that patients that wore motorcycle clothing had a generally
better health outcome compared with patients that had not [52].
Although no differences between on-road and off-road motorcyclists were seen with
respect to return to work and lost income, off-road motorcyclists showed better physical and
emotional outcomes three months after the accident. This is surprising, when considering that
both groups sustained equally severe injuries and similar injury profiles were seen with the
exception of soft tissue injuries. When looking at motorcycle clothing, de Rome et al. showed
lower rates of hospitalization in patients wearing motorcycle clothing [41] and implied that
the potential reduction in soft tissue injuries may reduce complications such as opportunistic
infections, scarring and disability, which has been found to result in a high rate of impairment
[18,41]. Indeed, in a separate publication the same authors found better health outcomes in
protected patients [52]. Although soft tissue injuries in the present study were not related to
physical outcomes, it must be noted that these were not quantified or assessed based on
extend and severity and this might have influenced the results. Keeping this in mind, a lower
proportion of on-road motorcyclists wore motorcycle clothing, which may partly explain the
observed difference. Not only did on-road motorcyclists report worse physical health, they
also felt more frequently emotional (e.g. frustrated, sad) about the accident than did off-road
motorcyclists. As patients that were involved in a multi vehicle accidents were found to feel
emotional about the accident more frequently than patients involved in single vehicle
accidents, the observed difference may in part be explained by the person at fault in these
accidents. It has been found that collisions with cars at intersections are generally the fault of
the car driver [22], which may lead to patients feeling more often frustrated about the
situation than when the accident was caused by themselves or no one was at fault.

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 29
4.5 Recommendations
Although preventive campaigns have been successfully implemented for on-road
motorcyclists and have reduced the number of accidents in this group [13], similar campaigns
for off-road motorcyclists are generally lacking. This should change, considering the high
proportion of off-road motorcyclists that sustain serious trauma. Some important issues were
raised by the present study, including high proportions of patients with substance use prior to
the accident in both groups, the relatively big contribution of speed in off-road accidents and
the high incidence of off-road accidents due to riding into an unexpected drop or ditch. These
issues may be addressed by educating riders on the importance of knowledge of the terrain.
Other interventions to reduce trauma in off-road motorcyclists have been suggested, including
age restrictions, special licensing, skills and risk awareness courses and mentoring schemes
for novice riders [16]. Although the most effective way to reduce to morbidity and mortality
due to MCAs is to prevent accidents from happening, another important consideration is
altering the outcome. Motorcycle clothing has shown to reduce the incidence of soft tissue
injuries and may improve patient outcome and costs, especially in accidents of relatively low
severity [52]. Although off-road motorcyclists were shown to wear motorcycle clothing more
frequently than on-road motorcyclists, the majority of patients did not wear full protective
clothing and this remains an important issue to be addressed. Another important consideration
is the encouragement and enforcement of helmet use in off-road motorcyclists, as a
considerable proportion of off-road motorcyclists did not wear a helmet. Future research
should focus on formulating ways to effectively implement new injury prevention strategies
specifically targeted at off-road motorcyclists, in order to reduce the burden of trauma to both
patient and society in this specific group of riders.
4.6 Strengths and limitations
A strength of this study was the combined prospective cohort design and retrospective audit,
which allowed a very detailed collection of patient demographics, accident details and
outcome three months after the accident. Further, by collecting possible sensitive data from
two sources, the accuracy of the data was maximized. Nonetheless, several limitations must
be addressed. The most important limitation was the relatively small sample size, which may
have compromised the detection of statistically significant differences between on-road and
off-road motorcyclists for some variables. Previous studies comparing both groups generally
used larger sample sizes and the fact that no differences in injury severity were found may be
attributable to this. Therefore, the results of this study should be interpreted with some
caution. Another obvious limitation was the possible selection bias towards more severely
injured patients, as this study only included patients that were reviewed or admitted by the
trauma team. Lastly, despite the effort to maximize accuracy of the data, the data were subject
to the willingness of the patient to answer the questions. Although every effort was taken to
increase the accuracy of possible sensitive subjects such as substance, the data was limited by
the honesty of the patients and the limited availability of objective measures such as a routine
blood alcohol level. Nonetheless, this study provided some important insights into the
characteristics of accidents in both on-road and off-road motorcyclists and reported some
findings that have not been found previously.

Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 30
4. Conclusion
The results from this study showed no significant differences in injury severity between on-
road and off-road motorcyclists in terms of ISS, hospital length of stay or discharge location.
Injury profiles were similar between both groups, with the exception of soft tissue injuries
which were higher in on-road motorcyclists. This higher incidence is likely related to the
lower rate of motorcycle clothing worn in this group. Although off-road motorcyclists
generally wore more protective equipment, a relatively low proportion of patients in both
groups wore full motorcycle equipment. Only motorcycle clothing with body armour was
shown to protect against soft tissue injuries and helmets were the only form of protection that
protected significantly against internal (traumatic brain) injuries and fractures. The effect of
motorcycle clothing on internal injuries has not previously been reported. This is the first
study to compare outcomes of on-road and off-road motorcyclists and showed that despite
similar injury severity and largely similar injury profiles, on-road motorcyclists reported
worse physical and emotional health outcomes three months after the accident. Nonetheless,
return to work was similar in on-road and off-road motorcyclists and was generally low with
nearly half of previously employed patients unable to return to partial or full employment
three months after the accident. The financial impact for patient and society are likely be
considerable. These findings emphasise the implications of off-road motorcycling trauma to
both patient and society and reinforce the need of taking action to reduce trauma in this
specific group of motorcyclists.
The present study highlighted important issues to be addressed in terms of both
primary and secondary prevention, including substance use, knowledge of the terrain,
speeding and the use of motorcycle clothing. Further research is needed to formulate ways to
effectively implement new injury prevention strategies specifically targeted at off-road
motorcyclists.
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 31
References
[1] World Health Organisation, International Classification of Diseases version 2010.
Definitions related to transport accidents.
(http://apps.who.int/classifications/apps/icd/icd10online2004/defs.htm)
[2] Federal Chamber of Automotive Industries (FCAI), National Sales Report 2012.
[3] Australian Bureau of Statistics. Motor vehicle census. 2013; 9309.0.
[4] Henley G, Harrison JE. Trends in serious injury due to land transport accidents, Australia
2000-01 to 2008-09. Injury and statistics series no. 66 2012; INJCAT 142. Canberra: AIHW.
[5] Johnston P, Brooks C, Savage H. Fatal and serious road crashes involving motorcyclists.
2008; Monograph 20.
[6] Cunningham G, Chenik D, Zellweger R. Factors influencing motorcycle crash victim
outcomes: a prospective study. ANZ J.Surg. 2012; 82 551-4.
[7] Henley G, Harrison G. Serious injury due to land transport, Australia 2008-09. 2012;
INJCAT 143. Canberra: AIHW.
[8] Bureau of Infrastructure, Transport and Regional Economics (BITRE). Road Deaths
Australia, 2012. Statistical Summary BITRE, Canberra ACT 2013.
[9] National Highway Traffic Safety Administration. Traffic Safety Facts 2005: Motorcycles.
National Highway Traffic Safety Administration 2007, Washington, DC.
[10] Department of Environment, Transport and the Regions. Tomorrow's Roads - Safer for
Everyone: The Government's Road Safety Strategy and Casualty Reduction Targets for
2010. London: Department of Environment, Transport and the Regions, 2000.
[11] European Co-operation in the Field of Scientific and Technical Research. European
Commission, Directorate Gerenal for Energy and Transport. Motorcycle Safety Helmets.
(ec.europa.eu/transport/roadsafety_library/.../cost327_final_report.pdf 2001; COST 327 final
report)
[12] Lin MR, Kraus JF. A review of risk factors and patterns of motorcycle injuries.
Accid.Anal.Prev. 2009; 41 710-22.
[13] Mikocka-Walus A, Gabbe B, Cameron P. Motorcycle-related major trauma: on-road
versus off-road incidence and profile of cases. Emerg.Med.Australas. 2010; 22 470-6.
[14] Forman JL, Lopez-Valdes FJ, Pollack K et al. Injuries among powered two-wheeler users
in eight European countries: a descriptive analysis of hospital discharge data.
Accid.Anal.Prev. 2012; 49 229-36.
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 32
[15] Ankarath S, Giannoudis PV, Barlow I, Bellamy MC, Matthews SJ, Smith RM. Injury
patterns associated with mortality following motorcycle crashes. Injury 2002; 33 473-7
[16] Cassell E, Clapperton A, O'Hare M, Congiu M. On- and off-road motorcycling injury in
Victoria. Hazard 2006; 64.
[17] Mathers C, Boerma T, Ma Fat D. The global burden of disease: 2004 update. Geneva,
Switzerland: World Health Organisation 2008, 160.
[18] Clarke JA, Langley JD, Disablement resulting from motorcycle crashes. Disabil.Rehabil.
1995; 17 377-85.
[19] Naumann RB, Dellinger AM, Zaloshnja E, Lawrence BA, Miller TR. Incidence and total
lifetime costs of motor vehicle-related fatal and nonfatal injury by road user type, United
States, 2005. Traffic Inj.Prev. 2010; 11 353-60.
[20] L. Blincoe, A. Seay, E. Zaloshnja, T. .Miller, E. Romano, S.Luchter, R.Spicer. National
Highway Traffic safety Administration. The Economic Impact of Motor Vehicle Crashes,
2000.
[21] Brown JB, Bankey PE, Gorczyca JT, Cheng JD, Stassen NA, Gestring ML. The aging
road warrior: national trend toward older riders impacts outcome after motorcycle injury.
Am.Surg. 2010; 76 279-86.
[22] Vlahogianni EI, Yannis G, Golias JC. Overview of critical risk factors in Power-Two-
Wheeler safety. Accid.Anal.Prev. 2012; 49 12-22.
[23] Harrison WA, Christie R. Exposure survey of motorcyclists in New South Wales.
Accid.Anal.Prev. 2005; 37 441-51.
[24] Tovell A, McKenna K, Bradey C, Pointer S. Hospital separations due to injury and
poisoning, Australia 2009–10. Injury research and statistics series no. 69. INJCAT 145.
Canberra: AIHW 2012.
[25] Soundappan SS, Holland A, Lam L et al. Off-road vehicle trauma in children: a New
South Wales perspective. Pediatr.Emerg.Care 2010; 26 909-13.
[26] Bevan CA, Babl FE, Bolt P, Sharwood LN. The increasing problem of motorcycle
injuries in children and adolescents. Med.J.Aust. 2008; 189 17-20.
[27] Ramakrishnaiah RH, Shah C, Parnell-Beasley D, Greenberg BS. Motorized dirt bike
injuries in children. J.Emerg.Med. 2013; 44 806-10.
[28] Clapperton AJ, Herde EL, Lower T. Quad bike related injury in Victoria, Australia.
Med.J.Aust. 2013; 199 418-22.
[29] Weiss H, Agimi Y, Steiner C, Youth. Motorcycle-related hospitalizations and traumatic
brain injuries in the United States in 2006. Pediatrics 2010; 126 1141-8.
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 33
[30] Shah CC, Ramakrishnaiah RH, Bhutta ST et al. Imaging findings in 512 children
following all-terrain vehicle injuries. Pediatr.Radiol. 2009; 39 677-84.
[31] Sexton B, Baughan C, Elliott M, Maycock G. The Accident Risk of Motorcyclists. Road
Safety Division, Department for Transport, London 2004.
[32] Kardamanidis K, Martiniuk A, Ivers RQ, Stevenson MR, Thistlethwaite K. Motorcycle
rider training for the prevention of road traffic crashes. Cochrane Database Syst.Rev. 2010;
(10):CD005240. doi CD005240.
[33] Meuleners LB, Lee AH, Haworth C. Road environment, crash type and hospitalisation of
bicyclists and motorcyclists presented to emergency departments in Western Australia.
Accid.Anal.Prev. 2007; 39 1222-5.
[34] Haworth NL, Greig K, Nielson AL. A comparison of risk taking in moped and
motorcycle crashes. 2009; Transportation Research Record 2140 182-7.
[35] Siskind V, Steinhardt D, Sheehan M et al. Risk factors for fatal crashes in rural Australia.
Accid.Anal.Prev. 2011; 43 1082-8.
[36] Fernandes FA, Alves de Sousa RJ. Motorcycle helmets--a state of the art review.
Accid.Anal.Prev. 2013; 56 1-21.
[37] Liu BC, Ivers R, Norton R et al. Helmets for preventing injury in motorcycle riders.
Cochrane Database Syst.Rev. 2008; (1):CD004333. doi CD004333.
[38] Philip AF, Fangman W, Liao J, Lilienthal M, Choi K. Helmets prevent motorcycle
injuries with significant economic benefits. Traffic Inj.Prev. 2013; 14 496-500.
[39] Steinhardt D, Mary S, Siskind V. A comparison of offroad and onroad crashes in rural
and remote Queensland. Proceedings 2006 Australian Road Safety Research, Policing,
Education Conference, Gold Coast. 2006.
[40] Motorcycle Council of NSW Inc. (MCC). (http://www.roadsafety.mccofnsw.org.au/).
[41] de Rome L, Ivers R, Fitzharris M, Du W., Haworth N, Heritier S, Richardson D.
Motorcycle protective clothing: protection from injury or just the weather? Accid.Anal.Prev.
2011; 43 1893-900.
[42] Grange JT, Corbett SW, Cotton A. Street bikes versus dirt bikes: a comparison of injuries
among motorcyclists presenting to a regional trauma center. J.Trauma 2004; 57 591-4.
[43] Blackman R, Cheffins T, Veitch C, O'Connor T. At work or play: a comparison of
private property vehicle crashes with those occurring on public roads in north Queensland.
Aust.J.Rural Health 2009; 17 189-94.
[44] Meuleners LB, Lee AH, Haworth C. Emergency presentations by vulnerable road users:
implications for injury prevention. Inj.Prev. 2006; 12 12-4.
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 34
[45] Lower T, Egginton N, Owen R. Agricultural motorcycle injuries in WA adolescents.
Aust.N.Z.J.Public Health 2003; 27 333-6.
[46] Thompson P, Hill D, Beidatsch K, Bramwell J. Road Safety Council of Western
Australia. Reported Road Crashes in Western Australia 2011.
[47] Trauma Services, Royal Perth Hosptial, 2013
(http://www.rph.wa.gov.au/traumaservices.html).
[48] Royal Perth Hospital. Trauma Registry Report - 2010 and 2011 Combined.
[49] American College of Surgeons. National Trauma Data Bank (NTDB): Annual Report
2005.
[50] Mullin B, Jackson R, Langley J, Norton R. Increasing age and experience: are both
protective against motorcycle injury? A case-control study. Inj.Prev. 2000; 6 32-5.
[51] Australian Government., Fair Work Act 2009.
(http://www.austlii.edu.au/au/legis/cth/consol_reg/fwr2009223/index.html#s3.01)
[52] de Rome L, Ivers R, Fitzharris M, Haworth N, Heritier S, Richardson D. Effectiveness of
motorcycle protective clothing: riders' health outcomes in the six months following a crash.
Injury 2012; 43 2035-45.
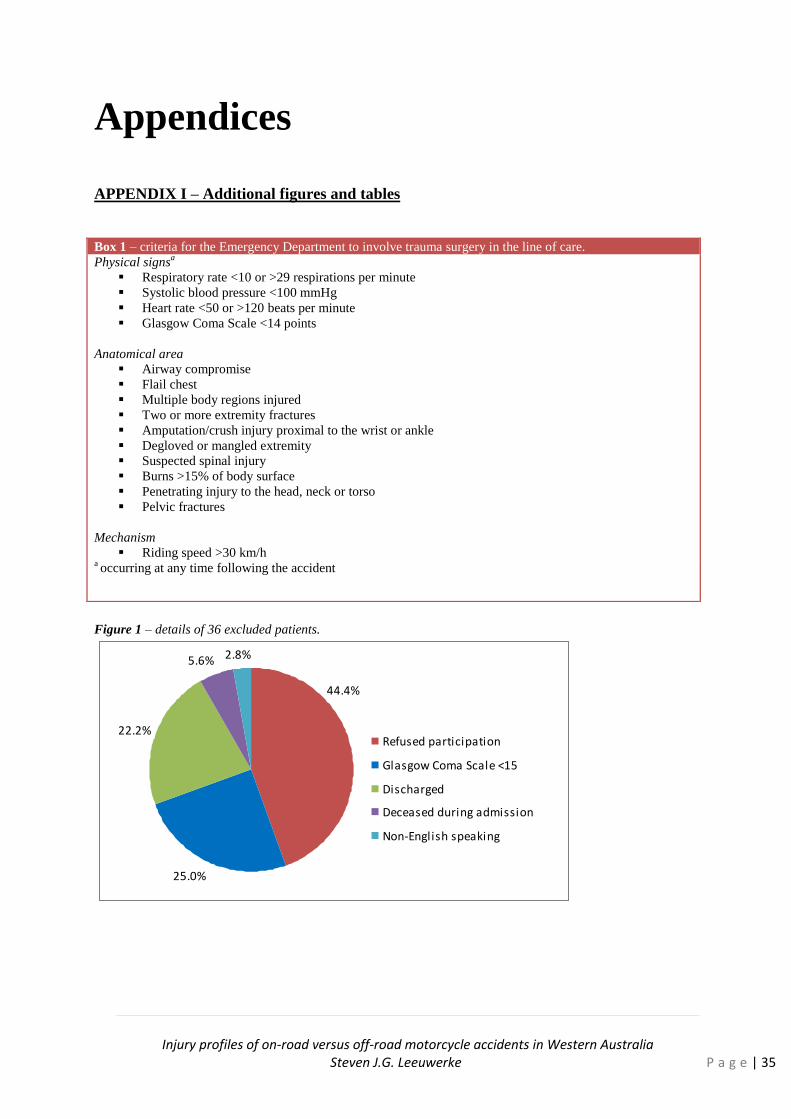
Injury profiles of on-road versus off-road motorcycle accidents in Western Australia
Steven J.G. Leeuwerke P a g e | 35
Appendices
APPENDIX I – Additional figures and tables
Figure 1 – details of 36 excluded patients.
25.0%
22.2%
5.6% 2.8%
44.4%
Refused participation
Glasgow Coma Scale <15
Discharged
Deceased during admission
Non-English speaking
Box 1 – criteria for the Emergency Department to involve trauma surgery in the line of care.
Physical signsa
Respiratory rate <10 or >29 respirations per minute
Systolic blood pressure <100 mmHg
Heart rate <50 or >120 beats per minute
Glasgow Coma Scale <14 points
Anatomical area
Airway compromise
Flail chest
Multiple body regions injured
Two or more extremity fractures
Amputation/crush injury proximal to the wrist or ankle
Degloved or mangled extremity
Suspected spinal injury
Burns >15% of body surface
Penetrating injury to the head, neck or torso
Pelvic fractures
Mechanism
Riding speed >30 km/h a occurring at any time following the accident