Embed Size (px)
Citation preview

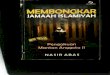
Figure 1: Participant is driving in a closedcircuit while experiencing the breathingexercise; and breathing waveform beforeand during the haptic guidance breathingintervention (bottom).
On-road guided slow breathinginterventions for car commuters
Stephanie BaltersSchool of MedicineStanford UniversityStanford, CA, [email protected]
James A. LandayComputer ScienceStanford UniversityStanford, CA, [email protected]
Pablo E. ParedesSchool of MedicineStanford UniversityStanford, CA, [email protected]
ABSTRACTThis is the first on-road study testing the efficacy and safety of guided slow breathing interventions ina car. This paper presents design and experimental implications when evolving from prior simulatorto on-road scenarios. We ran a between subjects controlled study (N=40) testing a haptic guidedbreathing system in a closed circuit. We contrasted both stress and not-stressed driving conditions.Preliminary results validate prior findings about the efficacy and safety of the simulator studies. Initialqualitative analysis shows an overall positive acceptance ratio, and no safety-critical incidents (e.g.,hard brakes or severe lane departures) – all participants graded the intervention as safe for real trafficapplications. Going further, quantitative and statistical analyses need to validate these early findingsbefore exposing commuters to the intervention on public roads.
SIGCHI’ 19, May 2019, Glasgow, UK© 2019 Association for Computing Machinery.This is the author’s version of the work. It is posted here for your personal use. Not for redistribution. The definitive Version ofRecord was published in Proceedings of ACM CHI Conference (SIGCHI’ 19), https://doi.org/10.1145/nnnnnnn.nnnnnnn.

On-road guided slow breathing interventions for car commuters SIGCHI’ 19, May 2019, Glasgow, UK
CCS CONCEPTS• Human-centered computing → Haptic devices; Ubiquitous and mobile computing systems andtools; •Applied computing→Consumer health; Psychology ; •Computer systems organization→ Sensors and actuators.
KEYWORDSSlow breathing; Deep breathing; Stress management; Just in time intervention; Health; Mental health;Commute; On the road; Road safety.
ACM Reference Format:Stephanie Balters, James A. Landay, and Pablo E. Paredes. 2019. On-road guided slow breathing interventionsfor car commuters. In Proceedings of ACM CHI Conference (SIGCHI’ 19). ACM, New York, NY, USA, 6 pages.https://doi.org/10.1145/nnnnnnn.nnnnnnn
MOTIVATIONA successful in-car breathing intervention iseffective in reducing breathing rate and physi-ological arousal, while not endangering drivingsafety nor inducing critical changes in drivingbehavior, e.g., major reduction in speed. We callthose subtle in-car interventions.
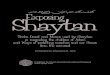
Figure 2: Seat-mat configuration coveringa back space of 12x18 inch grid, able toproduce a variety of different haptic stim-ulation patterns. In this experiment, thesystem delivered a swiping (up and down)sensation to guide participants’ breathingrhythm.
Breathing plays a fundamental role in regulating the autonomic nervous system and reducing au-tonomic arousal. First HCI studies have shown the efficacy of seat-embedded breathing guidancesystems to reduce breathing rate and physiological arousal in a simulator setting [1, 9]. In the nextstep, we need to evaluate applied systems under ecologically valid circumstances for the followingreasons (among others). Firstly, automotive studies show that the realness of potential physical harmin on-road driving, leads to a shift in focus compared to simulator driving – away from a secondarytask (e.g., phone dialing) and towards the actual driving task [10]. Hence, people might no longerengage with the intervention. Secondly, our embodied interaction design [6] not only requires cognitiveprocesses but aims at inducing actual changes in physiology. Those changes, itself, might induce risk.Hence, interventions might no longer be safe in a real car. Further, compared to the simulator, physicaldriving induces vibrations, visceral cues, and driving forces that could superimpose the guidancestimuli or impede a driver’s physical engagement with the intervention. Hence, the system designmight no longer be effective.The reasons stated above let us formulate the following research questions: RQ1: Is the in-car
on-road breathing guidance system effective in lowering driver’s breathing rate and, in turn, arousal levels?RQ2: Are in-car on-road guided breathing interventions safe and, if so, would it be safe to test them onpublic roads? RQ3: Are there any resulting changes in driving behavior, e.g., in speed or acceleration?The contribution of this paper is two-fold:
(1) Early qualitative findings that demonstrate the feasibility of in-car on-road guided slow breath-ing interventions with respect to both efficacy and safety.

On-road guided slow breathing interventions for car commuters SIGCHI’ 19, May 2019, Glasgow, UK
(2) A series of design and methodology considerations when testing intervention systems in risk-critical environments, e.g., driving.
No part of this paper currently includes quantitative and statistical analysis, which would be requiredbefore exposing commuters to the intervention on public roads.Driving Course. To provide a safe test en-
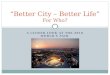
vironment, we conducted the experiment inan empty underground parking garage, withno additional traffic. A 0.65 miles long driv-ing course included four left and four rightturns. We placed four stop signs to resemblecity/neighborhood driving. Arrow-signs guidedthe way. We marked lanes with white duct tapeat a distance of 12 feet, which falls within therange of a typical city road configuration [13].At an approximate six-feet distance from bothlanes, structural pillars bordered the drivingcourse.
.
Figure 3: Experimental driving course inthe garage. Red lines show positions ofstop sings, and circles represent structuralpillars.
SYSTEM ANDMETHODOLOGYOur main objective was to reach high ecological validity with respect to commuting. We adapteda series of methodological parameters accordingly. Firstly, we invited only frequent commuters (afew times a week at minimum) to study habituated drivers. We pursued gender balance, and anaverage age of aboutM = 42.4 years (SD = 14.4) to approximate the cohort of American commuters[7]. Secondly, we designed the apparatus setup to carry a participant as single passenger because themajority of US commuters drives alone, e.g., 76.4 % in 2013 [7]. Thirdly, during the entire experiment,participants drove in a closed circuit in the same direction to resemble familiarity and tediousness ofa commute route. The Institutional Review Board approved experimental procedures. Participantswere provided insurance against accidents upon approval of a valid drivers license.Participants.We recruited a total of forty commuters (N = 40, 20 females). Average age wasM = 41.0years (SD = 12.9), and reported years of driver’s license possession was M = 21.8 years (SD = 13.8).Daily commute time ranged from 30 minutes to 2 hours. Twenty-five percent of participants reportedto practise deep breathing on a regular basis, whereas another one-forth reported to have no priorexperience with breathing exercises. We instructed all participants to not eat, drink caffeinated orenergizing beverages, do heavy exercises, sleep, or take hot showers one hour before the experiment.
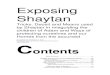
Figure 4: Experimental task procedure.
Apparatus. As experimental vehicle, we used an Infinity Q50. We equipped the car with cameras torecord participants in frontal and side angles, along with a frontal view of the road way (Figure 1). Ahaptic breathing guidance system integrated in a car seat described in [1, 8, 9] served as a templateto design an actuator system blent into a seat-mat. The system consisted of forty-one 2–3.6 V linearresonant actuator vibration motors, arranged as shown in Figure 2. We covered vibrators with a 0.2inches thin foam layer to cushion the actuators without lowering the vibrating stimuli. As participantsreported that a simple guidance pattern would be most intuitive and helpful to follow slow breathingrhythm [8, 9], we chose to stick to a simple pattern that swiped up and down the user’s back. Lastly,if applicable, experimenter (E1) asked participants to take off thick jackets to allow sensitivity in theback.Procedure and Experimental Tasks. We alternately divided participants into two groups (eachN = 20 with gender balance): an intervention and control group. E1 introduced participants of theintervention group to the haptic seat system and asked them to follow the breathing guidance forat least 30 seconds, and until they felt comfortable. The scenario of commuting home from work

On-road guided slow breathing interventions for car commuters SIGCHI’ 19, May 2019, Glasgow, UK
guided the design of the experimental tasks. All participants experienced two different modes ofpre-driving activities while being seated in the parked car (engine running): (1) stress-inducing and(2) neutral pre-condition. During the stressful pre-driving condition, we administered a variation ofthe Trier Social Math Task [5]: for a duration of three minutes, participants had to count backwardsfrom 1521 in steps of 13. In case a wrong answer was given or a time limit of four seconds wasviolated, the experimenter prompted the participants to start over again. During the neutral pre-driving condition (three minutes long), E1 asked the participants to wait in the car pretending abattery had to be exchanged in the trunk. We decided to include the latter “neutral” task to provide asimilar experimental length across participants. After each pre-condition, participants drove in theone-directional circuit for eight minutes. The intervention group experienced the guidance after twominutes of driving for a duration of two minutes in both conditions (Figure 4). The control group didnot experience any intervention. After the first driving task, a three minutes rest period followed toallow washing out of the prior stimulus. We randomized the order of stress-inducing and neutralconditions across participants to avoid bias. Experimental tasks were preceded by a baseline taskthat included watching a soothing video of a beach setting in the parked car (engine running) aswell as a familiarization with the driving course during ten laps (average duration M = 13 min 49 secwith SD = 1 min 47 sec). We randomized baseline and familiarization tasks across participants. Wechose a between subject study design because research indicates that a repeated exposure to a similararithmetic task reduces stress responses in participants [14].
Figure 5: Derived from the SAE Standardsfor Operational Definitions of DrivingPerformance Measures [12]. Lane depar-tures (option B) occur once a tire touchesthe inside of a lanemarking. Once the cen-ter of the vehicle touches and/or crosses alanemarking, lane departures become “se-vere”. While mild lane departures mightbe less risky on empty roads, severe lanedepartures are considered to violate driv-ing safety, especially since our driving cir-cuit is surrounded by structural pillars.
Quantitative Measures. To assess the (1) efficacy, (2) safety, and (3) potential changes in drivingbehavior upon on-road breathing interventions, we collected a variety of physiological, subjective, andcar-related measures. Psycho-physiological Measures: We captured breathing waveform (18 Hz) andelectrocardiogram (ECG) (250 Hz) with a Zephyr BioModule device worn around the torso. Electro-dermal Activity (EDA) (4Hz) was measured with an Empathica E4 bracelet worn around participants’non-dominant arm wrist. Subjective Measure: After each sub-task (baseline, familiarization, 2 x pre-stimulus, 2 x driving, and rest), we measured subjective stress responses via a simplified version of thePerceived Stress Scale (PSS) [11]: “How stressed do you feel right now?” with a 10-point scale from 1= “low” to 10 = “high”. Car-related Measures: From the CAN bus data stream, we collected speed (50Hz, mph), steering angle (100 Hz, degrees), and acceleration pedal position (50 Hz, degrees). Further,we positioned two cameras on the frontal fenders of the car, to capture spacing between tires andlane markings on each side. Because driving safety is highly context-dependent and often defined incorrespondence to other driving parties or incidents, e.g., time to collision measures [12], we define thefollowing safety violations suited to a closed circuit that is free of additional traffic: number of hardbraking in response to a sudden driving incident [4]) and number of severe lane departures (Figure 5).With respect to changes in driving behavior, we will analyze the following metrices according to the

On-road guided slow breathing interventions for car commuters SIGCHI’ 19, May 2019, Glasgow, UK
SAE recommendations [12]: number and rate of steering reversals, standard deviation of lane position,as well as average speed, and acceleration.Qualitative Measures. We surveyed subjective experiences of the intervention, specifically with re-spect to the perceived efficacy, safety, and changes in driving behavior, bymeans of a post-experimentalquestionnaire.
PRELIMINARY FINDINGS
Figure 6: Raw breathing waveform beforeand during the breathing intervention.
A first visual inspection of the raw breathing waveform validates a breathing rate of nine breathsper minutes (brpm) that was a participant-specific administered system pace during the breathingexercise (Figure 6). Secondly, two experimenters inspected lane capturing videos with respect to safetyviolations. Specifically they counted the observed number of hard brakes in response to a suddendriving incident, and the number of severe lane departures. No safety violations were observed. Lastly,an early analysis of qualitative user feedback indicates that participants experienced the interventionas helpful to reduce breathing pace, and that this reduction further led to a decrease in perceivedstress. Further, all participants of the intervention group (20/20) reported that the system wouldbe safe for real traffic applications. Two participants noted their concerns regarding applying theintervention in a drowsy driver state, as the intervention would further “add calming effects”.
FURTHER ANALYSIS AND FOLLOW-UP STUDYFurther analysis will comprise the processing (including e.g. artefact correction) of psycho-physiologicaldata, including breathing rate (brpm), heart rate (bpm), RMSSD (ms) as measure of short-term heartrate variability [9], EDA (amount of phasic peaks [2]), and self-reported stress. From CAN bus data, wewill derive occurrence of hard brakes (measured as one standard deviation of maximum deceleration),number and rate of steering reversals, and changes in speed (mph) and acceleration (m/s2) [12]. Viaimage processing we will calculate the amount, duration, and severeness of lane departures, as wellas mean standard deviation of lane positions (Figure 7). We aim to test following hypotheses: H1:
Figure 7: Image processing of videostreams C1 and C2 (60 frames per second),will allow us to automatically derivedriving safety and behavior measuressuch as amount and duration of severeand mild lane departures, and standarddeviation from center line.
Breathing rate and arousal levels will be lower during the intervention compared to before administration;H2: The decrease in breathing rate and arousal levels during the intervention is higher compared to thecontrol group; and H3: The intervention is safe to apply while driving; and does not induce major changesin driving behavior. Additionally, we will analyze qualitative results using thematic analysis [3] todistill main conclusions from the user feedback.
Upon validation, we will assess the guided slow breathing system/apparatus within commute trafficin a follow-up study. For safety reasons, we will give participants time to familiarize themselves withthe slow breathing system in an empty parking lot before entering public roads. A 12.3 miles longdriving course will comprise urban, mountain, and highway roads to test the system in differentdriving contexts. Commuters will follow a provided GPS route. We will conduct the experiment during

On-road guided slow breathing interventions for car commuters SIGCHI’ 19, May 2019, Glasgow, UK
evening commute hours (3.30 to 8.00 pm). We will use the same between subject design, measurements,and stressor. At different time points, the system will automatically administer breathing interventionsfor a duration of two minutes. We will set the breaks between interventions to randomly last betweenfour and six minutes to capture potential sustaining intervention effects. Via a post-questionnaires, wewill interrogate participants’ overall reaction and receptivity, with particular interest in understandingperceived impacts on efficacy, focus, safety, and opinions on beneficial or inappropriate drivingscenarios. To reduce risk, we will instruct participants to always prioritize safe driving. Drowsyparticipants will not be allowed to take part in the study. The experiment requires IRB approval, andvalidity of drivers’ licenses has to be approved to provide full insurance by the risk managementdepartment.
Figure 8: Driving course for follow-upstudy.ACKNOWLEDGEMENTSWe thank the Stanford Precision Health andIntegratedDiagnostics (PHIND) Center and theCenter for Automotive Research at Stanford(CARS) for supporting this work.
REFERENCES[1] Stephanie Balters, Elizabeth Murnane, James A. Landay, and Pablo E. Paredes. 2018. Breath Booster! Exploring In-car,
Fast-paced Breathing Interventions to Enhance Driver Arousal State. Proceedings of the PervasiveHealth Conference (2018).[2] Mathias Benedek and Christian Kaernbach. 2011. Physiological correlates and emotional specificity of human piloerection.
Biological psychology 86, 3 (2011), 320–329.[3] Richard E. Boyatzis. 1998. Transforming qualitative information: Thematic analysis and code development. Sage.[4] Joanne L. Harbluk, Y. Ian Noy, Patricia L. Trbovich, and Moshe Eizenman. 2007. An on-road assessment of cognitive
distraction: Impacts on drivers’ visual behavior and braking performance. Accident Analysis & Prevention 39, 2 (2007).[5] Clemens Kirschbaum, Karl-Martin Pirke, and Dirk H. Hellhammer. 1993. The Trier Social Stress Test–a tool for investigating
psychobiological stress responses in a laboratory setting. Neuropsychobiology 28, 1-2 (1993), 76–81.[6] Scott R. Klemmer, Björn Hartmann, and Leila Takayama. 2006. How bodies matter: five themes for interaction design. In
Proceedings of the 6th conference on Designing Interactive systems. ACM, 140–149.[7] Brian McKenzie. 2015. Who drives to work? Commuting by automobile in the United States: 2013. American Community
Survey Reports (2015).[8] Pablo E. Paredes, Nur Hamdan, Dav Clark, Carrie Cai, Wendy Ju, and James A. Landay. 2017. Evaluating in-car movements
in the design of mindful commute interventions: exploratory study. Journal of medical internet research 19, 12 (2017).[9] Pablo E. Paredes, Yijun Zhou, Nur Al-Huda Hamdan, Stephanie Balters, Elizabeth Murnane, Wendy Ju, and James A.
Landay. 2018. Just Breathe: In-Car Interventions for Guided Slow Breathing. Proceedings of the ACM on Interactive, Mobile,Wearable and Ubiquitous Technologies 2, 1 (2018), 28.
[10] Matthew P. Reed and Paul A. Green. 1999. Comparison of driving performance on-road and in a low-cost simulator usinga concurrent telephone dialling task. Ergonomics 42, 8 (1999), 1015–1037.
[11] Jonathan W. Roberti, Lisa N. Harrington, and Eric A. Storch. 2006. Further psychometric support for the 10-item versionof the perceived stress scale. Journal of College Counseling 9, 2 (2006), 135–147.
[12] SAE ISO Standards. 2015. Operational Definitions of Driving Performance Measures and Statistics. Society of AutomotiveEngineers (2015). https://doi.org/10.4271/J2944_201506
[13] William J. Stein and Timothy R. Neuman. 2007. Mitigation strategies for design exceptions. U.S. Department of Transporta-tion.
[14] Joe Tomaka, Jim Blascovich, Robert M. Kelsey, and Christopher L. Leitten. 1993. Subjective, physiological, and behavioraleffects of threat and challenge appraisal. Journal of personality and social psychology 65, 2 (1993), 248.