Embed Size (px)
Citation preview
Klassische Experimente derPsychologie
On Being Sane in InsanePlaces
Author: D. L. Rosenhan (1973)
Presentation by:Student: Stavroula Vasiliadi
Professor: Michael Niedeggend
Contents
Criteria of Normal-Abnormal behaviour Rosenhan’s biography Rosenhan’s experiment Hypothesis Theoritical Propositions Method Results The normal are not detectably sane- Type I and type II errors The stickiness of psychodiagnostic labels The experience of psychiatric hospitalization Powerlessness and Depersonalization Recent Applications Critique Summary-Conclusion Bibliography
“Normality and abnormality are notuniversal. What is viewed as normal in oneculture may be seen quite aberrant inanother.”
Benedict (1934)
NORMAL ABNORMAL(Effective (Mental
functioning) illness)
“All behaviour can be seen to lie on a continuum with normal at one end, andabnormal at the other”
Distinguishing “normal” from “abnormal”behaviour:
CriteriaCortex of Behaviour
Persistence of Behaviour
Social Deviance
Subjective Distress
Psychological Handicap
Effect on Functioning
Are mental health professionals truly ableto distinguish between the mentally ill andthe mentally healthy?
What are the consequences of mistakes?
David L. Rosenhan
received his Bacelor ofArts degree in YeshinaUniversity
1953 Master Degree atColumbia University and5 years later his Ph.D inpsychology.
1970 joined the StanfordLaw School faculty
1972 RosenhanExperiment
ROSENHAN EXPERIMENT(1972)
Hypothesis
Do the characteristics that lead to psychologicaldiagnoses reside in the patients themselves or inthe environments and cortex in which observersfind them?
If the established criteria and the training mentalhealth professionals have received fordiagnosing mental illness are adequate, thenwould those professionals be able to distinguishbetween the insane and the sane?
Theoretical Propositions
Rosenhan proposed to have normalpeople admitted to psychiatric hospitalsand then determining whether they werediscovered to be sane and, if so, how?
If these “pseudopatients” were notdiscovered to be normal, this would beevidence that diagnoses of the mentally illare depend more from the situation thanfrom the patient.
Method
8 sane people (3 psychologists, a psychiatrist, apediatrician, a housewife and a painter) - 3women & 5 men
in 12 different hospitals in United States called the hospital and made an appointment all of them followed the same instructions changed their names and occupations complained only of hearing voices that said
“empty”, “hollow” and “thud” all subjects acted normally and gave truthful
information
Method
all except one admitted with the diagnoses of“schizophrenia”
apart from their nervousness the“pseudopatients“ behaved “normally” andcooperated with the staff and accepted allmedications (not swallowed)
all took notes of their experience
their aim was to convince the staff that theywere healthy enough to be discharged
Results
length of hospital stay: an average of 19 days( min. 7 max. 52)
no one of the “pseudopatients” was detected bythe hospital staff
1 was diagnosed with “schizophrenia” 7 were diagnosed with “schizophrenia in
remission” 35 out of 118 real patients voiced suspicions that
3 of the subjects were not actually mentally ill contacts between patients and staff were
minimal and often bizarre
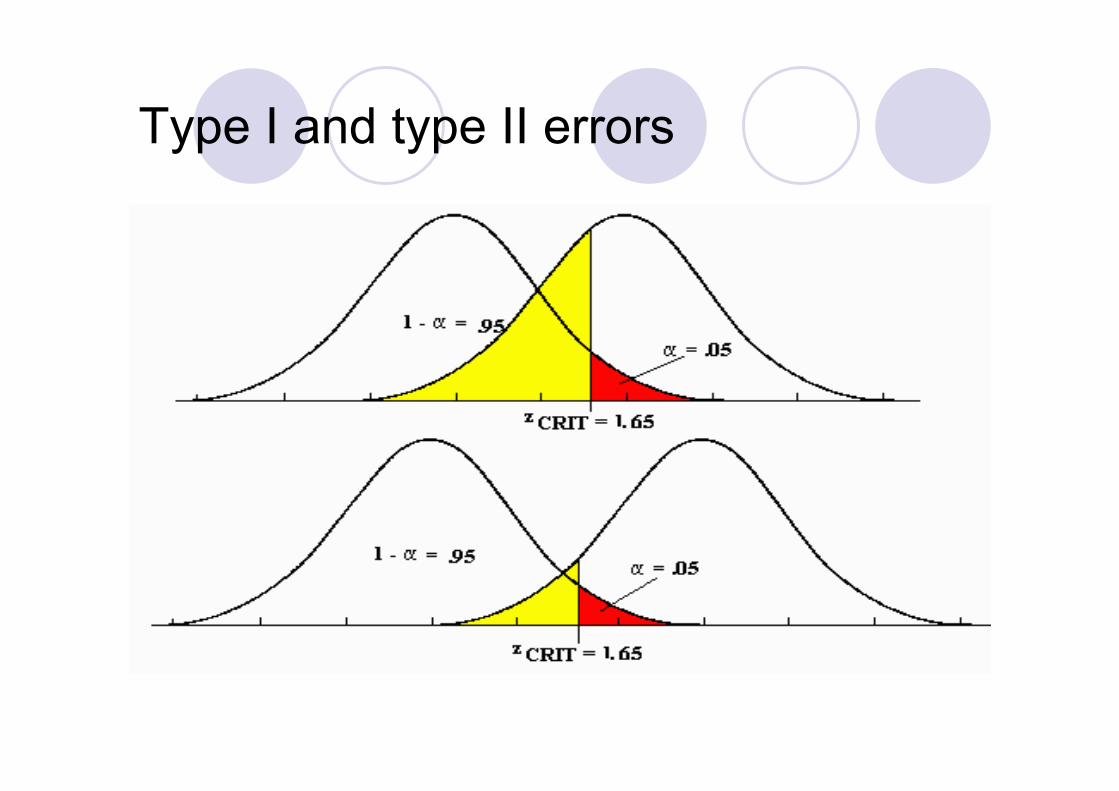
The normal are not detectably sane
Rosenhan believed that this happened becauseof what statisticians call “type error 2”
What is the “type error 2” ? the error of accepting a hypothesis that
should have been rejected This error says that physicians are more incline to call a
healthy person sick than a sick person healthy. This isbecause it is better to err on the side of caution, tosuspect illness even among the healthy.
The difference between medical and psychiatricdiagnose is that psychiatric diagnoses carry thepersonal, legal and social stigma.
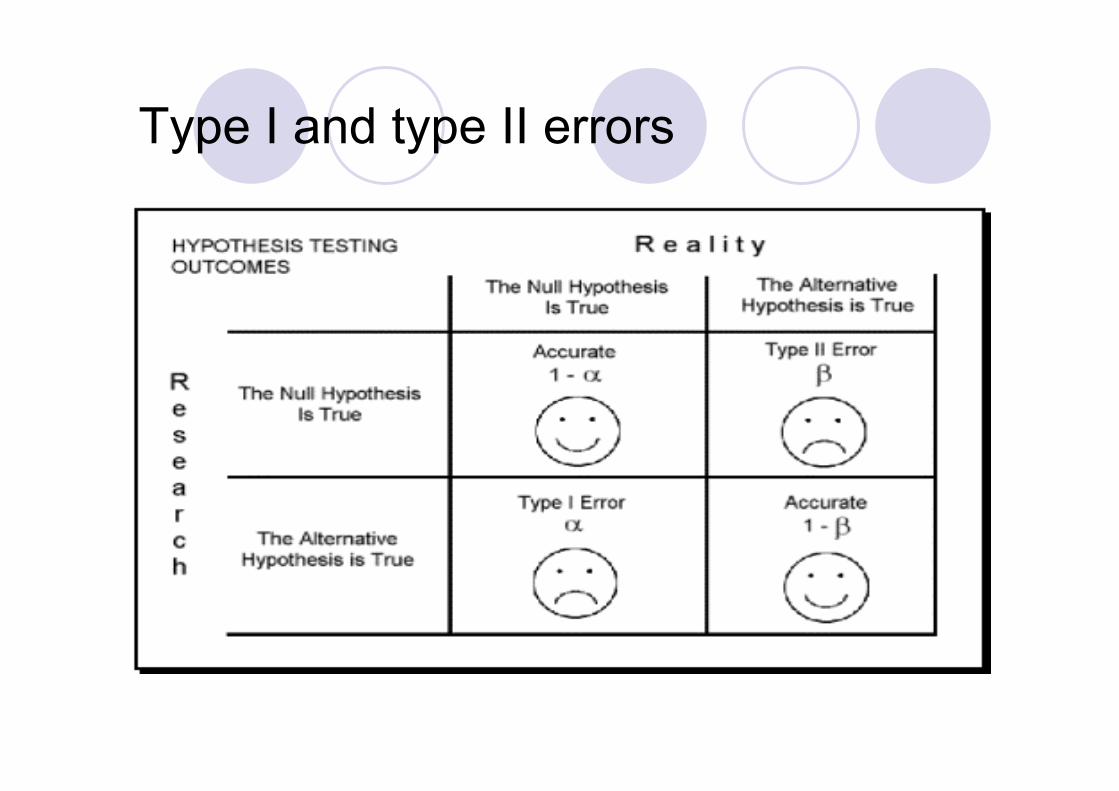
Type I and type II errors
Type I and type II errors
The stickiness of psychodiagnostic labels
When a patient is labeled as schizophrenicit becomes his/her central personality traitsand it colours all his/her behaviouralcharacteristics.
The label is so powerful that many of thepseudopatients’ normal behaviours wereoverlooked entirely or profoundlymisinterpreted.
Example from the Rosenhan’s researchof a pseudopatient’s stated history
The pseudopatient had had a close relationshipwith his mother but was rather remote from hisfather during his early childhood. Duringadolescence and beyond, however, his fatherbecame a close friend while his relationship withhis mother cooled. His present relationship withhis wife was characteristically close and warm.Apart from occasional angry exchanges, frictionwas minimal. The children had rarely beenspanked
The director’s interpretation of this rathernormal history
“This white 39-year-old male manifests a longhistory of considerable ambivalence in closerelationships which begins in early childhood. Awarm relationship with his mother cools duringhis adolescence. A distant relationship with hisfather is described as becoming very intense.Affective stability is absent. His attempts tocontrol emotionality with his wife and childrenare punctuated by angry outbursts and, in caseof the children, spankings. And while he says hehas several good friends, one senseconsiderable ambivalence embedded in thoserelationships also.”
The experience of psychiatrichospitalization
staff and patients are strictly segregated
those with the most power have least todo with patients and those with the leastpower are most involve with them
contacts between patients and staff areoften minimal
Pseudopatients test
the “pseudopatients” test to approach staffmembers and attempt to make a verbal contactby asking common questions
the most common response from the staff was abrief response to the question, offered while theywere “on the move” and with head averted or noresponse at all
pseudopatient: “Pardon me, Dr…..,could you tell me when I am eligible forground privileges?”psychiatrist: “Good morning, Dave. How are you today?”the doctor moved on without waiting for a response
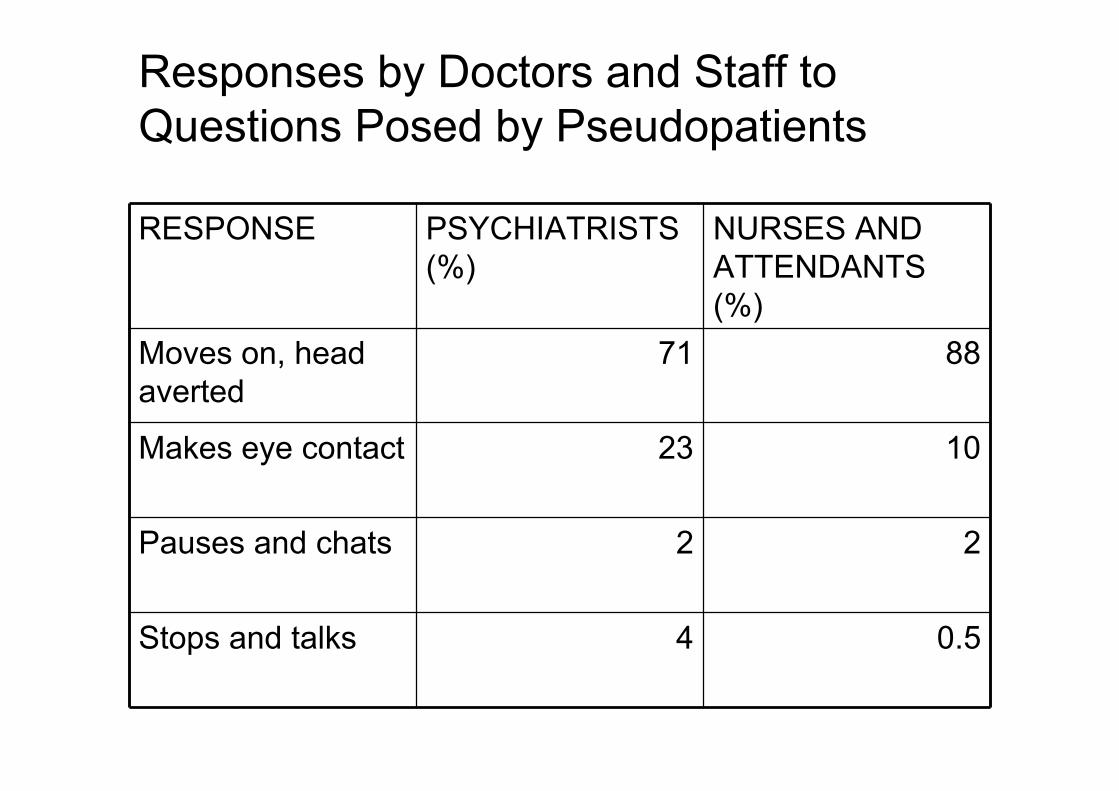
Responses by Doctors and Staff toQuestions Posed by Pseudopatients
RESPONSE PSYCHIATRISTS(%)
NURSES ANDATTENDANTS(%)
Moves on, headaverted
71 88
Makes eye contact 23 10
Pauses and chats 2 2
Stops and talks 4 0.5
Powerlessness and Depersonalization
The absence of eye and verbal contact reflectavoidance and depersonalization
Powerlessness was evident everywhere:
The freedom of movement is restricted. Patients cannot initiate contact with the staff. Personal privacy is minimal. Patients personal history and anguish is available to any
staff member.
The Sources of Depersonalization
The attitude that all have toward thementally ill
(Fear, distrust, horrible expectations andbenevolent intentions)
The hierarchical structure of thepsychiatric hospital
(Patients do not spend much time ininterpersonal contact with doctoral staff and thismodel inspires the rest of the staff )
Recent Applications
Studies that have used Rosenhan’s research inchallenging the validity of diagnoses made by mentalhealth professionals
Thomas Szasz (early 1970):Mental illness are notdiseases, but problems in living that have social andenvironmental causes.
Wahl (1999): People feel the effects of the stigmasurrounding mental illness from various sources.
Biosvert & Faust (1999): The tolerance andunderstanding of mental illness is incrising.
Broughton & Chesterman (2001): People mayfabricate symptoms of mental illness (e.g.criminals)
Critique
Spitzer’s belief is that Rosenhan’s studydid not really invalidate psychologicaldiagnostic systems.(1976)
3 possible ways of detecting the sanity ofa “pseudopatient”:
Detecting sanity before admission Detecting sanity after admission The patient was no longer insane
1. Detecting sanity before admission
The symptom of hallucinations does havediagnostic signification even though there wasnot in the literature
The clinical picture includes not only thesymptom but also the desire to enter apsychiatric hospital.
From that is reasonable to conclude that thesymptom is a source of significant distress.
With all the other conditions ruled out there isonly one possible diagnoses left: Schizophrenia
2. Detecting sanity after admission
Diagnostic conditions are not alwayschronic and unremitting
Mental illnesses endure forever (APA’s DSM)The diagnoses of schizophrenia does not
mean that all the patient’s behavior isschizophrenic
3. The patient was no longer insane
The diagnoses “schizophrenic in remission”is extremely unusual because:
a) Patients with the diagnosis ofschizophrenia are rarely completelyasymptomatic when discharged.
b) The discharged diagnosis associatedwith the admission to the hospital withoutany reference to the condition of thepatient when discharged
Summary-Conclusion
Rosenhan“It is clear that we cannotdistinguish the sane fromthe insane in psychiatrichospitals.(…)In a morebenign environment, onethat was less attached toglobal diagnosis, theirbehaviours andjudgments might havebeen more benign andeffective.”
Spitzer has argued that
psychological diagnosticsystems are invalidated.
Such symptom variationin psychiatric disorders iscommon and does notmean that the staff wasincompetent in failing todetect the ruse.
Bibliography
Roger R. Hock, Forty Studies that ChangedPsychology, Pearson Prentice Hall, 2005, p.226-234
D.L.Rosenhan, On Being Sane in Insane Places,Science, New Series, Vol.179, No 4070, (Jan.19,1973), p.250-258
Robert L. Spitzer, More on Pseudoscience inScience and the Case for Psychiatric Diagnosis,Arch Gen Psychiatry, Vol.33, April 1976
Internet
Thank you for your attention