-
* FDA EVIDENCE LEVELS: 1. Companion diagnostic; 2. Cancer
mutations with evidence of clinical significance; 3. Cancer
mutations with potential clinical significance (Per FDA: Level 3
“mutations may be informational or used to direct patients towards
clinical trials for which they may be eligible.”)2
OmniSeq AdvanceSM AssayA SINGLE TEST TO INFORM CANCER
TREATMENT
Your single-source laboratory solution
ACTIONABLE RESULTS SHOWN BY OMNISEQ TESTING DATA1
● 52% of patients tested to date have had targeted
and/or immuno evidence Level 1/Level 2 results,*1,2
notably higher than rate of targeted therapy tests.
● Actionability reaches 99% by combining indicated
and contraindicated biomarker results for targeted
therapy and immunotherapy.
● Overexpression of immune markers, measured by
RNA-seq gene expression, highlight rational targets
for immuno-oncology clinical trials.
● Where applicable, summary interpretation will
include response rates where patients have multiple
Level 1 or Level 2 indications*1,2 to guide treatment
decisions.
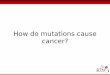
OmniSeq Advance Retrospective Results by Status, All
Histologies*1,2
Targeted Only Level 3 Evidence
Targeted AND Immuno Level 1 & 2 Evidence
Immuno OnlyLevel 1 & 2 Evidence
Immuno Only Level 3 Evidence
No Actionable Markers
Targeted AND Immuno
Level 3 Evidence
Targeted Only Level 1 & 2 Evidence
1%
33%
12%
22%
18%8%
6%
Number of samples, n=1,212
A single test with 99% actionability.1 Combine both targeted
therapy and immune-oncology biomarkers in a single test.
Genomic Profiling● Evaluates 144 genes● Measures SNVs, CNVs,
Fusions● 2% QNS rate
Immune Profiling● Evaluate entire cancer-immunity cycle● TMB,
TILs, MSI, PD-L1 and RNA-Seq
OmniSeq AdvanceSM
● One Test● One Sample● One Report
-
* FDA EVIDENCE LEVELS: 1. Companion diagnostic; 2. Cancer
mutations with evidence of clinical significance; 3. Cancer
mutations with potential clinical significance (Per FDA: Level 3
“mutations may be informational or used to direct patients towards
clinical trials for which they may be eligible.”)2
COMPONENTS OF OMNISEQ ADVANCESM
● PD-L1 IHC according to histology
● CD8 IHC to characterize tumor-infiltrating lymphocytes
(TILs)
● MSI by NGS, no normal tissue required
● Tumor mutational burden (TMB) – 409 genes
● RNA-sequencing of over 50 critical immune markers to
characterize the tumor micro-environment (TME)
● Somatic genomic profiling of 144 genes
● Personalized summary of findings written by a pathologist
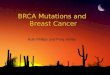
OMNISEQ ADVANCE FOR NON-SMALL CELL LUNG CANCER (NSCLC)
Due to the high prevalence of PD-L1 staining above 1% TPS, and
the number of targeted therapies available across multiple genetic
alterations, 82% of NSCLC patients were found to have Level 1 or 2
biomarkers.*1,2
The NCCN NSCLC Guidelines® recommendcomprehensive genomic
profiling to assess the full
spectrum of treatment
options.3
Number of samples, n=597
OMNISEQ ADVANCE RETROSPECTIVE RESULTS BY STATUS FOR
NSCLC*1,2
100%
Level 1 or 2 Targeted Therapy Markers*1,2
Percentages based on 302 samples
Immuno OnlyLevel 1 & 2 Evidence
Targeted AND ImmunoLevel 3 Evidence
Targeted Only Level 3 EvidenceImmuno Only Level 3 Evidence
No Actionable Markers: 0%
Targeted AND Immuno Level 1 & 2 Evidence
Targeted Only Level 1 & 2 Evidence
ALK or EGFR positive Level 1 & 2 Evidence
34%
12%
9%
3%
27%
12%
3%
ERBB2
65%
21%
KRAS
EGFR
ALK
3%
MET4%
BRAF1%
RET2%
3%
ROS11%
-
INTERROGATES THE CANCER-IMMUNITY CYCLE
Tumor Antigen Production● Tumor Mutational Burden (TMB)●
Microsatellite Instability (MSI)
T-Cell Receptor Signaling● RNA-Sequencing (RNA-Seq)● PD-L1
Immunohistochemistry (IHC)
Tumor Infiltrating Lymphocytes● RNA-Sequencing (RNA-Seq)● CD8
Immunohistochemistry (IHC)
Priming and activation
(APCs & T cells)
Trafficking of T cells to tumors (CTLs)
Cancer antigen presentation
(dendritic cells/APCs)
Release of cancer cell antigens
(cancer cell death)
Killing of cancer cells (Immune and cancer cells)
Infiltration of T cells into tumors (CTLs, endothelial
cells)
Recognition of cancer cells by T cells (CTLs, cancer cells)
Source: Adapted from Immunity, Volume 39, Chen, Daniel S et al.,
Oncology Meets Immunology: The Cancer-Immunity Cycle, 1-10.
Copyright 2013, with permission from Elsevier.
http:/dx.doi.org/10.1016/j.immuni.2013.07.012
BIOMARKERS THAT INDICATE AN INFLAMED TUMOR MICROENVIRONMENT MAY
MORE ACCURATELY PREDICT RESPONSE TO IMMUNOTHERAPY4
48%
27%
10%
12%
3%
No Highly Expressed Markers (Immune Desert)
High Expression of Other Immune Markers, but not TMB or PD-L1
High
TMB High
PD-L1 High (IHC)
TMB High & PD-L1 High IHC
IMMUNOTHERAPY ACTIONABILITY PERCENTAGE BY BIOMARKER
~50% of patients with negative results by standard markers had
high expression of secondary immune markers. These overexpressed
markers are direct targets for therapies commercially available or
in clinical trials.
Initial Immune Report Card Reference Population by Status
Source: Initial OmniSeq® Assay Reference Population, 2016
Number of samples, n=167
1 MarkerOverexpressed
2 MarkersOverexpressed
3+ MarkersOverexpressed
● GITR● CD40● ADORA2A● CCR2● CTLA4● PD-1● VISTA● CD38● FOXP3●
TIM3● IDO1● TGFβ1● OX40● TNF
Actionable Targets48%
The OmniSeq Advance assay was developed by OmniSeq® and is
performed by OmniSeq as a send-out from Integrated Oncology, part
of LabCorp Specialty Testing Group, its US distributor.
-
OmniSeq AdvanceSM is a service mark of OmniSeq, Inc.NCCN
Guidelines® is a trademark owned by the National Comprehensive
Cancer Network, Inc.
©2019 Laboratory Corporation of America® Holdings. All rights
reserved. | onc-999-v3-0519 | L18846-0519-3
REFERENCES1. Based on OmniSeq Internal data. 2. FDA Fact Sheet,
CDRH’s Approach to Tumor Profiling Next
Generation Sequencing Tests, U.S. Food and Drug Administration.
FDA website,
https://www.fda.gov/downloads/MedicalDevices/ProductsandMedicalProcedures/InVitroDiagnostics/UCM584603.pdf.
Accessed 5/10/18.
3. National Comprehensive Cancer Network. Non-Small Cell Lung
Cancer Version 4.2018. http://www.nccn.org. Published April 26,
2018. Accessed May 21, 2018.
4. Ott, PA et al., T-Cell-Inflamed Gene-Expression Profile,
Programmed Death Ligand Expression, and Tumor Mutational Burden
Predict Efficacy in Patients Treated With Pembrolizumab Across 20
Cancers: KEYNOTE-028. J Clin Oncol 2018:
DOI:10.1200/JCO.2018.78.2276.
www.integratedoncology.com
SPECIMEN REQUIREMENTS
Tissue Submission Guidelines
All blocks and slides must at a minimum be labeled with the
pathology case number and part. Reports and other provided
materials must be labeled with the pathology case number and at
least two patient identifiers, such as name, medical record number,
or date of birth. Please include the pathology report.
Recommended Specimen Submission
**DO NOT SUBMIT Decalcified Specimens or Cytology Smears**The
preferred specimen is at least one formalin-fixed,
paraffin-embedded (FFPE) block. If a block cannot be provided, see
slide requirements below. Specimens with very small amounts of
tumor and/or less than requested number of slides will be accepted
with the caveat that complete testing may not be possible.
Slide Requirements
Preferred: FFPE blockAlternate: send 20 unbaked, positively
charged, unstained slides cut at 5 μm plus one H&E.
Transportation Requirements
FFPE blocks: Stored at room temperature and shipped with no
special precautions, except when daily outside temperatures exceed
35°C, and then ship with cool packs to avoid paraffin meltdown.
FIND OUT MORELearn more about Integrated
Oncology’s comprehensive
menu of testing services.
Contact your local Integrated
Oncology territory manager,
call client services at
800.447.5816, or visit
www.integratedoncology.com.
LAB LOCATIONSArizonaIntegrated Oncology5005 South 40th
StreetPhoenix, AZ 85040800.710.1800 • Fax 800.481.4151
Connecticut/New YorkIntegrated Oncology3 Forest ParkwayShelton,
CT 06484800.447.5816 • Fax 212.258.2143
North CarolinaLabCorp Center for Molecular Biology and
Pathology1912 Alexander DriveResearch Triangle Park, NC
27709800.345.4363 • Fax 919.361.7798
TennesseeIntegrated Oncology201 Summit View Drive, Suite
100Brentwood, TN 37027800.874.8532 • Fax 615.370.8074
Integrated Oncology – a LabCorp Specialty Testing Group
More than 541,000 tests performed on 387,000+ patients
annually
1,600 contractual relationships with plans, payors, and other
health care organizations across the US, some of which are on an
exclusive basis
More than 700 connectivity solutions that integrate >250 EMR,
LIS, and PMS systems
Menu of more than 550 genetic, pathology, IHC, and FISH tests,
including both somatic and hereditary testing
Staff of more than 75 pathologists, PhDs, and genetic counselors
dedicated to oncology and familial cancer testing
More than 95 oncology- and pathology-specific publications and
presentations since 2013