Embed Size (px)
Citation preview
Olmesartan Medoxomil-Based AntihypertensiveTherapy Evaluated by Ambulatory Blood PressureMonitoringEfficacy in High-Risk Patient Subgroups
Steven G. Chrysant,1 F. Wilford Germino2 and Joel M. Neutel3
1 Oklahoma Cardiovascular and Hypertension Center and the University of Oklahoma School of Medicine, Oklahoma City, OK, USA
2 Department of Internal Medicine, Orland Primary Care Specialists, Orland Park, IL, USA
3 Orange County Research Center, Tustin, CA, USA
Contents
Abstract. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 375
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 376
1.1 Importance of Blood Pressure (BP) Goals. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 376
1.2 Role of 24-Hour BP Monitoring . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 377
1.3 Treatment Recommendations and Rationale. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 378
1.4 Objective of this Review . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 378
1.5 Search Strategy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 378
2. Efficacy of Olmesartan Medoxomil-Based Therapy on Ambulatory BP Parameters . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 378
2.1 Ambulatory BP Lowering from Baseline . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 381
2.1.1 Olmesartan Medoxomil-Based Therapy Regimens . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 381
2.1.2 Impact of Time of Administration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
2.1.3 Olmesartan Medoxomil versus Comparator Antihypertensives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 383
2.2 24-Hour Systolic BP/Diastolic BP Goal Attainment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384
2.3 Adverse Events. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 384
3. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 385
4. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 387
Abstract Hypertension affects approximately 26% of the world’s adult population and is a recognized major risk
factor for morbidity and mortality associated with cardiovascular, cerebrovascular, and renal diseases.
However, despite the availability of a range of effective antihypertensive agents and a growing awareness of
the consequences of high blood pressure (BP), the treatment and control of hypertension remains sub-
optimal. A number of patient subgroups are categorized as ‘high risk’ and may have hypertension that is
more difficult to treat, including obese individuals, patients with stage 2 hypertension, those with type 2
diabetes mellitus (T2DM), patients with coronary artery disease or a history of stroke, and Black patients.
As the benefits of lowering BP in patients with hypertension are unequivocal, particularly in high-risk
patients, treating high-risk patients with hypertension to BP goals and maintaining 24-hour BP control is
important to help reduce cardiovascular risk and improve outcomes. Although the BP goals recommended
in current consensus guidelines for the management of patients with hypertension are based on cuff BP
measurements, ambulatory BP monitoring (ABPM) provides a valuable diagnostic tool and allows a more
accurate assessment of BP levels throughout the 24-hour dosing period. ABPM is a better predictor of
REVIEWARTICLEAm J Cardiovasc Drugs 2012; 12 (6): 375-389
1175-3277/12/0006-0375/$49.95/0
Adis ª 2012 Springer International Publishing AG. All rights reserved.

prognosis than office BP measurement and is also useful for assessing whether antihypertensive therapy
remains effective in the critical last few hours of the dosing period, which usually coincides with the morning
BP surge associated with arousal and arising.
ABPM has been adopted by new evidence-based guidelines in the United Kingdom to confirm a sus-
pected diagnosis of hypertension, which is an indication of the growing importance of ABPM in the
management of hypertension. This review provides an overview of the efficacy and safety of anti-
hypertensive therapy based on olmesartan medoxomil – hydrochlorothiazide and amlodipine/olmesartan
medoxomil in high-risk patient populations enrolled in studies that reported ambulatory BP endpoints. The
studies identified in this review showed that a titrate-to-BP goal strategy using olmesartan medoxomil- or
amlodipine/olmesartan medoxomil-based antihypertensive therapy was an effective and well-tolerated ap-
proach for maintaining BP control throughout the full 24-hour dosing period in high-risk patients with
difficult-to-treat hypertension.
1. Introduction
Hypertension is highly prevalent globally and a recognized
major risk factor for morbidity and mortality associated with
cardiovascular (CV), cerebrovascular, and renal diseases.[1-3] Hy-
pertension affects approximately 26% of the world’s adult popu-
lation, ranging from 20% to 40% of adults inWestern countries,[4]
and approximately one-third of the adult US population.[5]
There is a linear correlation between blood pressure (BP)
and the risk of death from ischemic heart disease and stroke,
regardless of age, with a doubling of the risk for each 20-mmHg
increase in systolic BP (SBP) or 10-mmHg increase in diastolic
BP (DBP).[3,6] Despite the availability of a range of effective
antihypertensive agents and a growing awareness of the con-
sequences of high BP, treatment and control of hypertension
remain suboptimal.[5] As a consequence of the low rate of BP
goal achievement, current guidelines recognize that most pa-
tients will require combination therapy to achieve their BP
goal.[6-8] The need for multiple drug therapy to achieve a BP
goal of <130/80mmHg for patients with diabetes mellitus is
supported by the American Diabetes Association and American
Association of Clinical Endocrinologists guidelines.[9,10] More-
over, for Black patients, the International Society on Hyper-
tension in Blacks 2010 Consensus Statement also recommends
combination therapy if BP is >15/10mmHg over their recom-
mended target, and BP ‡135/85mmHg if no target organ
damage, preclinical CV disease (CVD), or CVD are present, or
BP <130/80mmHg if target organ damage, preclinical CVD,
and/or history of CVD are present.[11]
Specific subgroups of patients with hypertension are considered
to be high risk, including obese individuals, patients with either
more severe (stage 2) or isolated systolic hypertension, those
with type 2 diabetes mellitus (T2DM), patients with coronary
artery disease or a history of stroke, and Black patients. Such
patients are considered to be more challenging to treat and
manage because of a high incidence of co-morbidities and other
clinical issues.[6,7,12] Hypertension is highly prevalent in patients
with T2DM, occurring at a rate approximately 1.5 to 3 times
higher than in the age-matched non-diabetic population.[13]
Also, the risk of CVD (including coronary artery disease, pe-
ripheral arterial disease, myocardial infarction, heart failure,
and stroke) and renal insufficiency in patients with both dia-
betes and hypertension is greatly increased.[13] Other compli-
cations in patients with diabetes and hypertension include
diabetic nephropathy, retinopathy, and neuropathy.[14,15]
Someminority populationswith hypertension are also at higher
risk than the general population. Specifically, in the United States,
hypertension ismore common inBlacks, develops at an earlier age,
is more severe, and is associated with a higher rate of clinical
complications than in age-matched non-Hispanic Whites.[6] In
addition, higher rates of other CV risk factors, such as obesity and
diabetes, increase the risk of fatal and non-fatal stroke, congestive
heart failure, and end-stage kidney disease in Blacks.[6,12,16,17]
In addition to predisposing patients to diabetes, obesity is in
itself a major independent CV risk factor[6] and influences prog-
nosis in hypertensive patients.[7] Finally, more severe (stage 2)
hypertension is more difficult to treat[6] and is associated with a
higher risk of CVD and stroke than less severe hypertension.[3,16]
However, the clinical benefits of lowering BP in patients with
hypertension are unequivocal, particularly in high-risk patients.[6,7]
Therefore, treating high-risk patients with hypertension to BP
goals and maintaining 24-hour BP control are important fac-
tors to reduce CV risk and improve outcomes.
1.1 Importance of Blood Pressure (BP) Goals
Current consensus practice guidelines for the management
of hypertension are based on clinical trial evidence demon-
376 Chrysant et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)

strating that treating patients with hypertension to defined BP
thresholds, or goals, improves long-term outcomes.[6,7,18] To
maximize CV protection, the guidelines recommend a seated
cuff BP goal of <140/90mmHg in the general hypertensive
population, with a more stringent goal of <130/80mmHg for
patients with diabetes, established CVD, or chronic kidney
disease.[6,7] There is reasonably strong clinical evidence for
this more stringent goal in patients with diabetes. However,
lower levels of evidence supporting this lower goal exist
for Black patients, patients with obesity, or those with stage 2
hypertension.[6,7]
1.2 Role of 24-Hour BP Monitoring
The limitations of traditional office BP measurement are
increasingly recognized, as measuring BP in a clinical setting
may be inadequate or misleading for the following reasons:
(i) the inherent variability of BP together with the small number
of readings typically taken in the office and ‘white coat’ or
‘masked’ effects resulting in increased or decreased BP, re-
spectively; (ii) observer bias; (iii) poor measurement technique,
including incorrect choice of cuff size, terminal digit preference,
rapid cuff deflation, and bladder size; (iv) improper sphyg-
momanometry equipment maintenance and/or calibration; and(v) varying levels of technical expertise in BP measurement
amongst the clinic staff.[18-20] Ambulatory BP monitoring
(ABPM) allows the collection of multiple BP measurements
on a regular basis. Consequently, ABPM provides a more ac-
curate assessment of mean BP levels, and thus better reflects
prevailing BP than office BP readings, and reveals masked
hypertension.[18] ABPM also provides important additional
clinical value, as clinic BP has a weak relationship with 24-hour
BP, and ambulatory BP (ABP) is relatively unaffected by ‘white
coat’ hypertension and has a better correlation with hyper-
tension-related organ damage and the effect of antihypertensive
treatment than do clinic BP readings.[6,7,18] Furthermore, com-
parison of the impact of office andABP on long-term prognosis
shows that ABP better predicts prognosis, even after adjust-
ment for associated risk factors.[19,21-23] For example, over
a 5-year follow-up period of 1963 adult patients (mean age
57 years), those with mean 24-hour SBP ‡135mmHg on anti-
hypertensive therapy were almost twice as likely to have a CV
event as patients with mean 24-hour SBP of <135mmHg, re-
gardless of office BP values.[21] In another study, ABPM was
also a more accurate predictor of CV mortality than was clinic
BP in 1144 elderly patients (mean age 73 years) with hyper-
tension.[24] After adjusting for clinic BP, night-time BP in this
study was a better predictor than daytime BP; there was an 18%
increase in the relative risk of CV death for each 10-mmHg
increase in night-time SBP, compared with a 10% mortality
increase for each 10-mmHg increase in daytime SBP. In con-
trast, for a corresponding increase in clinic SBP, there was no
significant increase in mortality.[24] Therefore, in order to re-
duce CV events and improve the CV risk profile of patients with
hypertension, optimal antihypertensive therapy should main-
tain BP control throughout the full 24-hour dosing period.
The availability of automated, non-invasive ABPM devices
that measure BP throughout the 24-hour period has demon-
strated that BP generally follows a distinct and reproducible
circadian pattern, with BPmaintained at its highest level during
the daytime and declining during the night-time to reach a
trough between approximately midnight and 03:00 hours.[25]
A slow and steady increase in BP is then observed until ap-
proximately 06:00 hours, at which point an abrupt and steep
surge in BP occurs that coincides with arousal and arising.[25,26]
This is particularly important because the end of the 24-hour
drug-dosing period usually coincides with the morning BP
surge, which is linked to an increased risk of CV events.[25,27]
Therefore, ABPM is also a useful approach for assessing the
ability of an antihypertensive agent to control BP throughout
the entire 24-hour dosing interval.
In addition to its prognostic value in predicting clinical
outcomes, ABP may provide additional predictive informa-
tion.[19,22] There is increasing evidence that BP variability
in itself is an independent predictor of clinical outcomes, and
ABPMprovides information on aspects of the circadian profile
of BP, including BP variability, the morning surge in BP noted
above, dipping status, and nocturnal BP patterns.[18,19] This
allows the identification of high-risk patients, independent of
BP measurement obtained in the office setting. False-positive
diagnoses (‘white coat’ hypertension) and false-negative diag-
noses (masked hypertension) are reduced, avoiding either un-
necessary treatment or undertreatment. ABPM is also the most
effective method of determining BP values during the sleep
cycle when nocturnal hypertension or a non-dipping pattern of
diurnal BP variation (<10% reduction from daytime to night-
time BP) are suspected.[19] This pattern is of relevance in the
treatment of high-risk patients because an increased prevalence
of non-dipper status has been reported in obese patients,
patients with sleep apnea, patients with T2DM or stage 2 hy-
pertension, and in Black patients.[28,29] Furthermore, there is
some evidence that non-dippers are at greater CV risk than
those with a normal nocturnal dipping pattern (typically SBP is
10–20mmHg lower at night-time than during the day),[22,28]
and a treatment that promotes a switch from non-dipper to
dipper status may facilitate a reduction in CV risk.
Efficacy of Olmesartan-Based Therapy in High-Risk Patients 377
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)

Although there are currently no specific practice guideline
recommendations for ABP goals, the American Heart Associ-
ation and the European Society of Hypertension suggest target
levels of <135/85, <120/70, and <130/80mmHg as normal for
daytime, night-time, and 24-hour average ABP, respectively, and
<130/80, <115/65, and <125/75mmHg as optimal values.[22,30]
A daytimeABPof 135/85mmHg corresponds approximately to
a clinic BP of 140/90mmHg, which is the threshold abovewhich
CV risk appears to substantially increase.[23,31]
The recent evidence-based guidelines from the National In-
stitute for Health and Clinical Excellence (NICE)[18] in the
United Kingdom include ABPM guidance that is expected
to have far-reaching implications. They recommend that if
hypertension is suspected (clinic BP of ‡140/90mmHg), the
patient should be offered ABPM to confirm the diagnosis of
hypertension, and ensure that they do not have masked hy-
pertension, determine their dipping status, and check for BP
variability.[18] Although this is not currently the standard of
care in the USA, it does provide an additional rationale for the
use of ABPM. Furthermore, the NICE recommendations are
supported by robust evidence that ABPM is superior to clinic
BP measurement for the cost-effective diagnosis of hyper-
tension in patients with suspected BP of >140/90mmHg, re-
sulting in improved health outcomes for men and women with
hypertension regardless of age.[32] It should be noted that there
are currently no specific ABP target recommendations for pa-
tients with difficult-to-treat hypertension such as Black patients,
patients with diabetes, elderly patients, etc.
1.3 Treatment Recommendations and Rationale
A titrate-to-BP goal approach is usually used to manage
hypertension, starting with the appropriate class and com-
bination of antihypertensives according to the degree of
hypertension and other risk factors.[6] If more than one anti-
hypertensive agent is required to achieve BP control, selecting
agents with complementary mechanisms of action is a rational
and recommended treatment approach.[6-8] For example,
the antihypertensive effects of angiotensin II type I receptor
blockers (ARBs) can be enhanced by the addition of a diuret-
ic.[33] Combination therapy may be more effective than
increasing the dose of a single agent, and may also alleviate ad-
verse events[30] associated with any of the component mono-
therapies, contributing to long-term compliance.[6-8,34]
The efficacy and safety of treatment regimens based on the
ARB olmesartan medoxomil, alone or in combination with
hydrochlorothiazide (HCTZ) or the dihydropyridine calcium
channel blocker (CCB) amlodipine, has been demonstrated in a
number of clinical trials and/or subgroup analyses in a variety
of high-risk patient populations, such as those with stage 2
hypertension, obesity, T2DM, and in Black patients.[34-40] The
24-hour BP-lowering efficacy of olmesartan medoxomil anti-
hypertensive therapy has also been compared with the ARB tel-
misartan in Japanese patients with hypertension and T2DM.[41]
1.4 Objective of this Review
This article reviews the efficacy and safety of olmesartan
medoxomil –HCTZ and amlodipine/olmesartan medoxomil
combination therapy in high-risk patient populations (Blacks,
patients with obesity, stage 2 hypertension, or T2DM) enrolled
in studies that reported ABP endpoints.
1.5 Search Strategy
A search of the medical literature using MEDLINE and
EMBASE (English-language articles only) was conducted
using the keywords ‘olmesartan’ and ‘hypertension’ and ‘am-
bulatory’ for the search period of January 1995–December
2011. The full articles were retrieved and the results were then
manually filtered to identify studies in which the efficacy of
olmesartan medoxomil-based antihypertensive therapies in
high-risk patients was assessed using ABPM. Additional ref-
erences were identified from the reference list of published ar-
ticles. Searches were last updated on 20 December 2011. It
should be noted that, although the search results did include
a phase III trial against azilsartan wherein some patients
had stage 2 hypertension, no subgroup results were provided,
and thus those findings could not be included in the present
review.[42]
2. Efficacy of Olmesartan Medoxomil-Based Therapy
on Ambulatory BP Parameters
Table I summarizes the study design, patients, interventions,
and endpoints of studies of olmesartan medoxomil-based
therapy in which changes in ABP parameters were reported in
the high-risk patient subgroups included in this review (Blacks,
stage 2 hypertension, T2DM, and obesity). Although not a
specific focus of this review, studies of elderly patient cohorts
were included if they reported ABP data and included analysis
of data from high-risk patient subgroups of interest. In cases
where reported data for a high-risk subgroup or groups was
part of a subgroup analysis, results for the total study popu-
lation are not included but only data for the high-risk sub-
group(s) in order to keep within the scope of the review.
378 Chrysant et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)
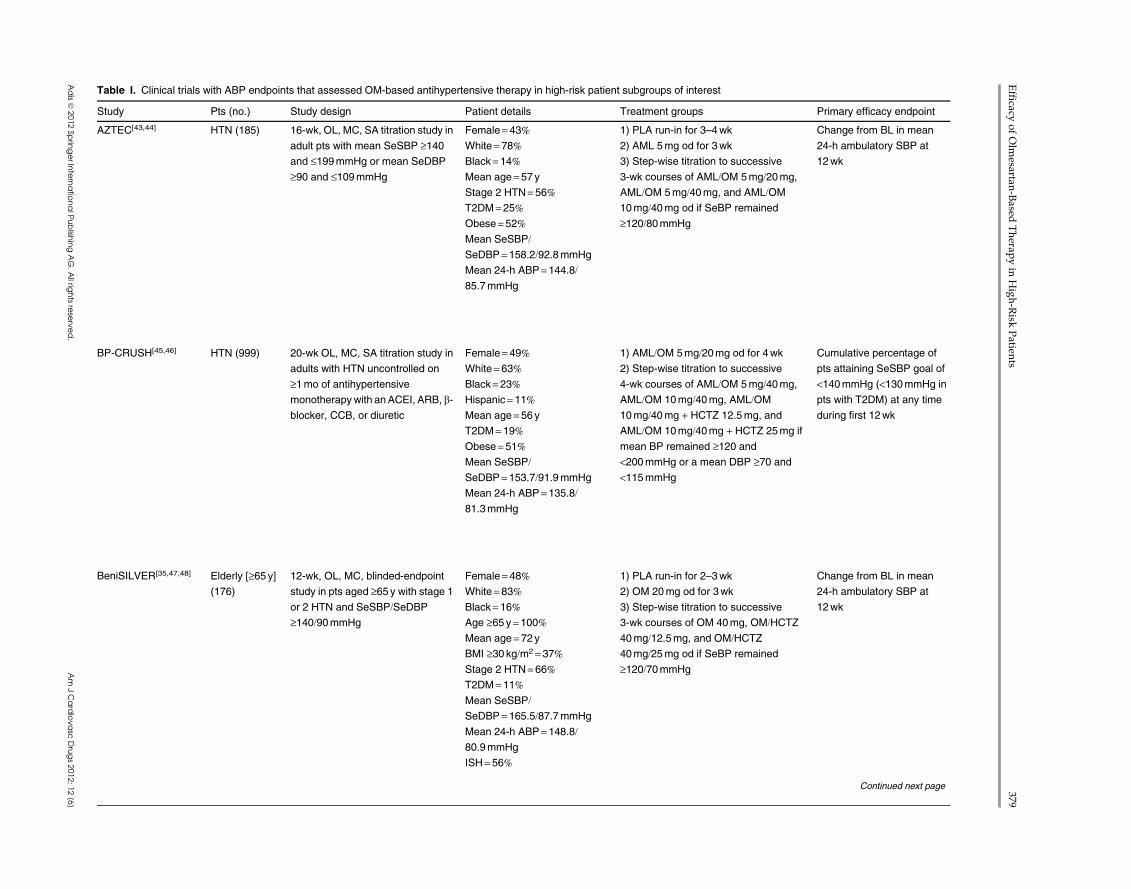
Table I. Clinical trials with ABP endpoints that assessed OM-based antihypertensive therapy in high-risk patient subgroups of interest
Study Pts (no.) Study design Patient details Treatment groups Primary efficacy endpoint
AZTEC[43,44] HTN (185) 16-wk, OL, MC, SA titration study in
adult pts with mean SeSBP ‡140and £199mmHg or mean SeDBP
‡90 and £109mmHg
Female= 43%White = 78%Black= 14%Mean age=57 yStage 2 HTN= 56%T2DM =25%Obese= 52%Mean SeSBP/SeDBP = 158.2/92.8mmHg
Mean 24-h ABP=144.8/85.7mmHg
1) PLA run-in for 3–4wk
2) AML 5mg od for 3wk
3) Step-wise titration to successive
3-wk courses of AML/OM 5mg/20mg,
AML/OM 5mg/40mg, and AML/OM
10mg/40mg od if SeBP remained
‡120/80mmHg
Change from BL in mean
24-h ambulatory SBP at
12wk
BP-CRUSH[45,46] HTN (999) 20-wk OL, MC, SA titration study in
adults with HTN uncontrolled on
‡1mo of antihypertensive
monotherapywith anACEI, ARB, b-
blocker, CCB, or diuretic
Female= 49%White = 63%Black= 23%Hispanic = 11%Mean age=56 yT2DM =19%Obese= 51%Mean SeSBP/SeDBP = 153.7/91.9mmHg
Mean 24-h ABP=135.8/81.3mmHg
1) AML/OM 5mg/20mg od for 4wk
2) Step-wise titration to successive
4-wk courses of AML/OM 5mg/40mg,
AML/OM 10mg/40mg, AML/OM
10mg/40mg + HCTZ 12.5mg, and
AML/OM 10mg/40mg + HCTZ 25mg if
mean BP remained ‡120 and
<200mmHg or a mean DBP ‡70 and
<115mmHg
Cumulative percentage of
pts attaining SeSBP goal of
<140mmHg (<130mmHg in
pts with T2DM) at any time
during first 12wk
BeniSILVER[35,47,48] Elderly [‡65 y](176)
12-wk, OL, MC, blinded-endpoint
study in pts aged ‡65 y with stage 1
or 2 HTN and SeSBP/SeDBP‡140/90mmHg
Female= 48%White = 83%Black= 16%Age ‡65 y= 100%Mean age=72 yBMI ‡30 kg/m2 = 37%Stage 2 HTN= 66%T2DM =11%Mean SeSBP/SeDBP = 165.5/87.7mmHg
Mean 24-h ABP=148.8/80.9mmHg
ISH= 56%
1) PLA run-in for 2–3wk
2) OM 20mg od for 3wk
3) Step-wise titration to successive
3-wk courses of OM 40mg, OM/HCTZ40mg/12.5mg, and OM/HCTZ40mg/25mg od if SeBP remained
‡120/70mmHg
Change from BL in mean
24-h ambulatory SBP at
12wk
Continued next page
Efficacy
ofOlm
esartan-Based
Therap
yin
High-Risk
Patien
ts379
Adisª
2012Sp
ringerInternatio
nalP
ublish
ingAG.Allrig
htsrese
rved.
Am
JCardiovasc
Drugs2012;12(6)
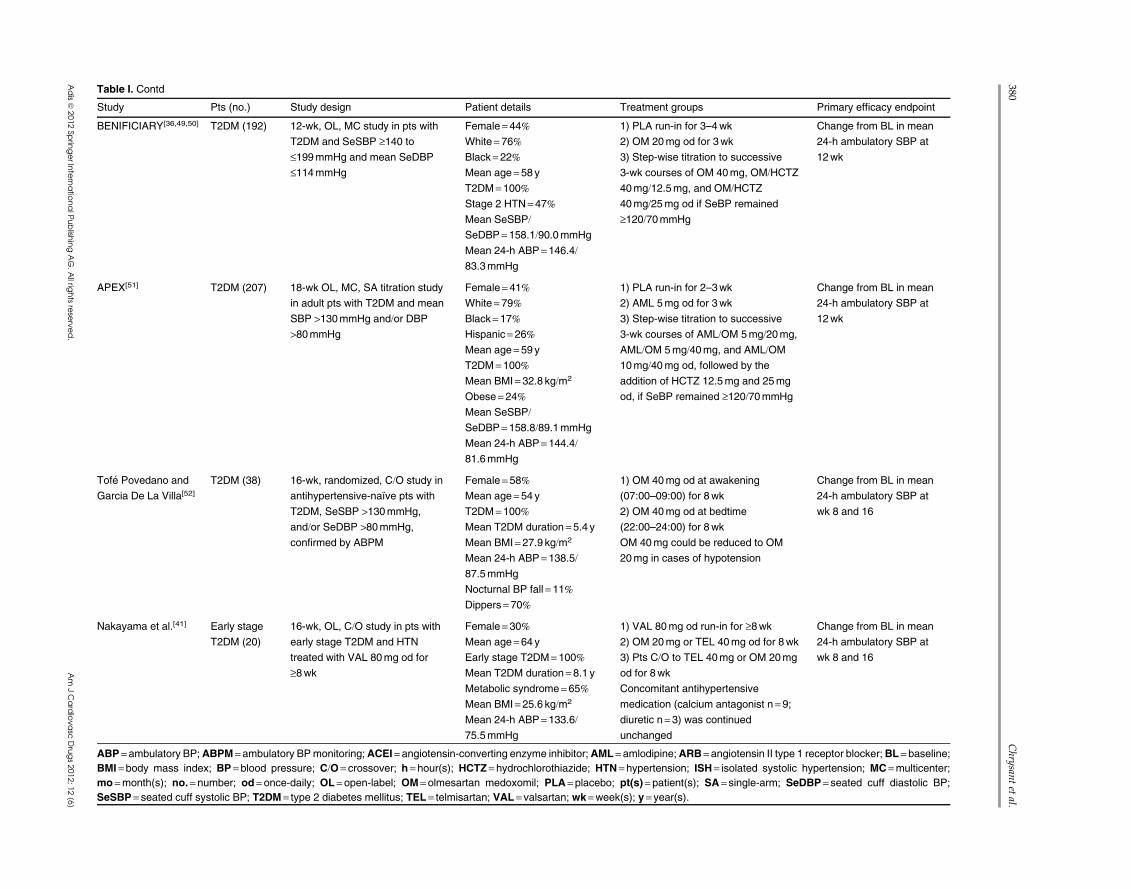
Table I. Contd
Study Pts (no.) Study design Patient details Treatment groups Primary efficacy endpoint
BENIFICIARY[36,49,50] T2DM (192) 12-wk, OL, MC study in pts with
T2DM and SeSBP ‡140 to
£199mmHg and mean SeDBP
£114mmHg
Female= 44%White = 76%Black= 22%Mean age=58 yT2DM =100%Stage 2 HTN= 47%Mean SeSBP/SeDBP = 158.1/90.0mmHg
Mean 24-h ABP=146.4/83.3mmHg
1) PLA run-in for 3–4wk
2) OM 20mg od for 3wk
3) Step-wise titration to successive
3-wk courses of OM 40mg, OM/HCTZ40mg/12.5mg, and OM/HCTZ40mg/25mg od if SeBP remained
‡120/70mmHg
Change from BL in mean
24-h ambulatory SBP at
12wk
APEX[51] T2DM (207) 18-wk OL, MC, SA titration study
in adult pts with T2DM and mean
SBP >130mmHg and/or DBP>80mmHg
Female= 41%White = 79%Black= 17%Hispanic = 26%Mean age=59 yT2DM =100%Mean BMI= 32.8 kg/m2
Obese= 24%Mean SeSBP/SeDBP = 158.8/89.1mmHg
Mean 24-h ABP=144.4/81.6mmHg
1) PLA run-in for 2–3wk
2) AML 5mg od for 3wk
3) Step-wise titration to successive
3-wk courses of AML/OM 5mg/20mg,
AML/OM 5mg/40mg, and AML/OM
10mg/40mg od, followed by the
addition of HCTZ 12.5mg and 25mg
od, if SeBP remained ‡120/70mmHg
Change from BL in mean
24-h ambulatory SBP at
12wk
Tofe Povedano and
Garcia De La Villa[52]T2DM (38) 16-wk, randomized, C/O study in
antihypertensive-naıve pts with
T2DM, SeSBP >130mmHg,
and/or SeDBP >80mmHg,
confirmed by ABPM
Female= 58%Mean age=54 yT2DM =100%Mean T2DM duration= 5.4 yMean BMI= 27.9 kg/m2
Mean 24-h ABP=138.5/87.5mmHg
Nocturnal BP fall =11%Dippers = 70%
1) OM 40mg od at awakening
(07:00–09:00) for 8wk
2) OM 40mg od at bedtime
(22:00–24:00) for 8wk
OM 40mg could be reduced to OM
20mg in cases of hypotension
Change from BL in mean
24-h ambulatory SBP at
wk 8 and 16
Nakayama et al.[41] Early stage
T2DM (20)
16-wk, OL, C/O study in pts with
early stage T2DM and HTN
treated with VAL 80mg od for
‡8wk
Female= 30%Mean age=64 yEarly stage T2DM= 100%Mean T2DM duration= 8.1 yMetabolic syndrome = 65%Mean BMI= 25.6 kg/m2
Mean 24-h ABP=133.6/75.5mmHg
1) VAL 80mg od run-in for ‡8wk2) OM 20mg or TEL 40mg od for 8wk
3) Pts C/O to TEL 40mg or OM 20mg
od for 8wk
Concomitant antihypertensive
medication (calcium antagonist n = 9;diuretic n =3) was continued
unchanged
Change from BL in mean
24-h ambulatory SBP at
wk 8 and 16
ABP =ambulatory BP;ABPM =ambulatory BPmonitoring;ACEI= angiotensin-converting enzyme inhibitor;AML= amlodipine;ARB=angiotensin II type 1 receptor blocker;BL = baseline;BMI =body mass index; BP = blood pressure; C/O= crossover; h = hour(s); HCTZ = hydrochlorothiazide; HTN= hypertension; ISH= isolated systolic hypertension; MC=multicenter;
mo=month(s); no.= number; od = once-daily; OL= open-label; OM= olmesartan medoxomil; PLA= placebo; pt(s)= patient(s); SA = single-arm; SeDBP = seated cuff diastolic BP;
SeSBP = seated cuff systolic BP; T2DM = type 2 diabetes mellitus; TEL = telmisartan; VAL= valsartan; wk =week(s); y = year(s).
380Chrysan
tetal.
Adisª
2012Sp
ringerInternatio
nalP
ublish
ingAG.Allrig
htsrese
rved.
Am
JCardiovasc
Drugs2012;12(6)
2.1 Ambulatory BP Lowering from Baseline
2.1.1 Olmesartan Medoxomil-Based Therapy Regimens
The ABP-lowering efficacy of olmesartan medoxomil-based
therapy from studies with subgroup analyses of Blacks or pa-
tients with stage 2 hypertension, T2DM, or obesity are shown in
tables II, III, and IV. Five of the studies that used ABP param-
eters to evaluate the efficacy of olmesartan medoxomil-based
dose-titration antihypertensive regimens in high-risk patient
subgroups were identified and summarized below.
AZTEC
TheAZORTrial Evaluating Blood Pressure Reductions and
Control (AZTEC) (ClinicalTrials.gov identifier: NCT00527514)
was conducted in 185 patients with hypertension who were
treated with a fixed-dose combination of amlodipine and ol-
mesartanmedoxomil, using step-wise dose titration to achieve a
seated cuff BP goal of <120/80mmHg (table I).[43,44] ABP re-
sults stratified by obesity and T2DM are presented in table II.
After treatment for 12 weeks, the results of the subgroup anal-
ysis paralleled those shown in the primary study of patients
with stage 1 or 2 hypertension. Amlodipine/olmesartan me-
doxomil combination therapy reduced 24-hour mean ABP by
-21.4/-12.7mmHg in the overall study population, compared
with -21.6/-13.4mmHg in obese patients and -21.5/-12.6mmHg
in patients with T2DM. Changes from baseline in mean day-
time and night-time BP were also similar in the overall study
population, obese patients, and patients with T2DM (table II).
ABP changes from baseline during the last hours of the
dosing interval were also comparable (table II). For example,
mean BP changes during the last 6 hours were -18.8/-11.1mmHg
overall, and -18.0/-11.1 and -18.7/-10.3mmHg in obese patients
and patients with T2DM, respectively.
BP-CRUSH
The Blood Pressure Control in All Subgroups With Hy-
pertension (BP-CRUSH) study (ClinicalTrials.gov identifier:
NCT00791258) enrolled 999 patients with hypertension uncon-
trolled on one or more antihypertensive monotherapies with an
angiotensin-converting enzyme inhibitor, ARB, b-adrenoceptorblocker (b-blocker), CCB, or diuretic. This was a dose-titration
study wherein patients were treated with amlodipine/olmesartan
medoxomil–HCTZ for 12 weeks, and uptitrated to achieve BP
goals of <120/70mmHg (table I).[45] A subgroup analysis was
conducted in patients stratified by obesity (table II).[46]
Treatment with amlodipine/olmesartanmedoxomil –HCTZ
reduced 24-hour mean ABP by 14.8/9.4mmHg in non-obese
patients and by 13.6/8.8mmHg in obese patients. In both non-
obese and obese patients, there were also significant changes
from baseline in mean daytime and night-time BP (table II).
This treatment regimen produced significant changes from
baseline in ABP during the last hours of the dosing inter-
val (table II). During the last 6 hours, mean changes were
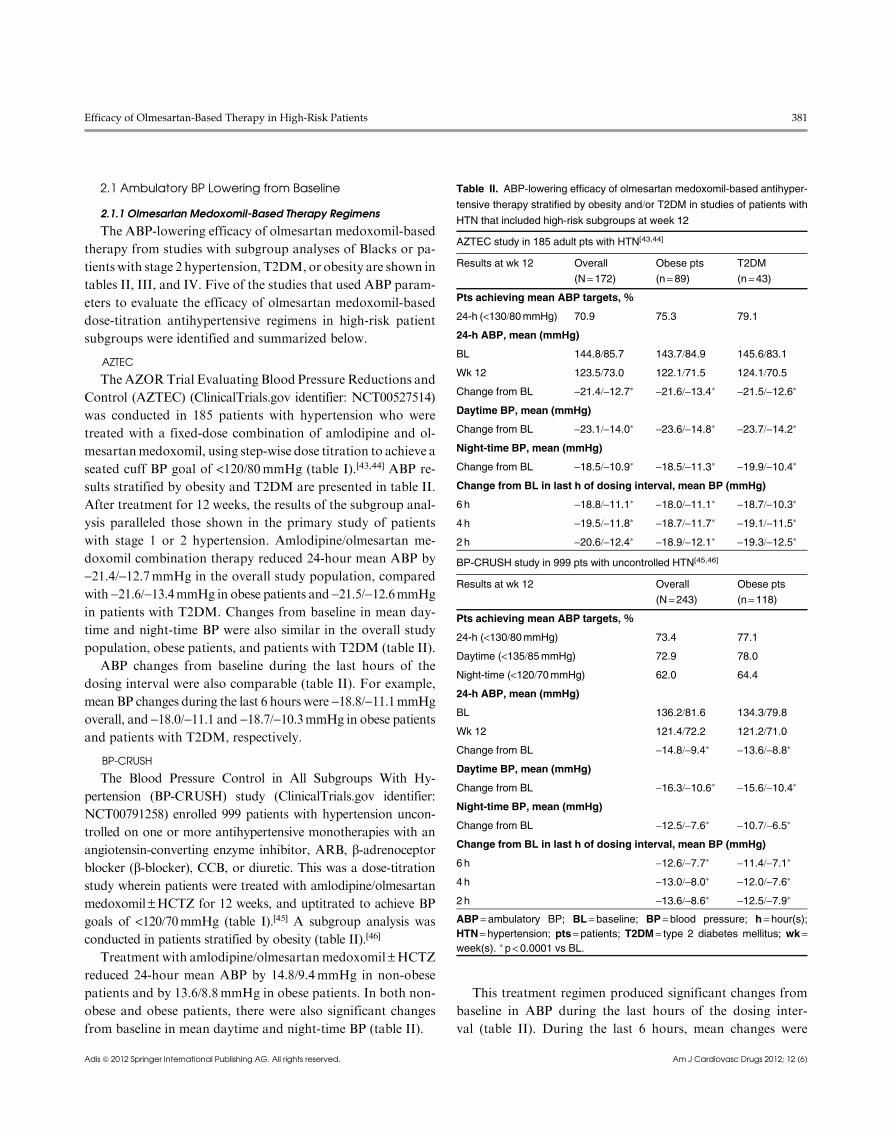
Table II. ABP-lowering efficacy of olmesartan medoxomil-based antihyper-
tensive therapy stratified by obesity and/or T2DM in studies of patients with
HTN that included high-risk subgroups at week 12
AZTEC study in 185 adult pts with HTN[43,44]
Results at wk 12 Overall
(N= 172)Obese pts
(n= 89)T2DM
(n= 43)
Pts achieving mean ABP targets, %
24-h (<130/80mmHg) 70.9 75.3 79.1
24-h ABP, mean (mmHg)
BL 144.8/85.7 143.7/84.9 145.6/83.1
Wk 12 123.5/73.0 122.1/71.5 124.1/70.5
Change from BL -21.4/-12.7* -21.6/-13.4* -21.5/-12.6*
Daytime BP, mean (mmHg)
Change from BL -23.1/-14.0* -23.6/-14.8* -23.7/-14.2*
Night-time BP, mean (mmHg)
Change from BL -18.5/-10.9* -18.5/-11.3* -19.9/-10.4*
Change from BL in last h of dosing interval, mean BP (mmHg)
6 h -18.8/-11.1* -18.0/-11.1* -18.7/-10.3*
4 h -19.5/-11.8* -18.7/-11.7* -19.1/-11.5*
2 h -20.6/-12.4* -18.9/-12.1* -19.3/-12.5*
BP-CRUSH study in 999 pts with uncontrolled HTN[45,46]
Results at wk 12 Overall
(N=243)Obese pts
(n= 118)
Pts achieving mean ABP targets, %
24-h (<130/80mmHg) 73.4 77.1
Daytime (<135/85mmHg) 72.9 78.0
Night-time (<120/70mmHg) 62.0 64.4
24-h ABP, mean (mmHg)
BL 136.2/81.6 134.3/79.8
Wk 12 121.4/72.2 121.2/71.0
Change from BL -14.8/-9.4* -13.6/-8.8*
Daytime BP, mean (mmHg)
Change from BL -16.3/-10.6* -15.6/-10.4*
Night-time BP, mean (mmHg)
Change from BL -12.5/-7.6* -10.7/-6.5*
Change from BL in last h of dosing interval, mean BP (mmHg)
6 h -12.6/-7.7* -11.4/-7.1*
4 h -13.0/-8.0* -12.0/-7.6*
2 h -13.6/-8.6* -12.5/-7.9*
ABP= ambulatory BP; BL= baseline; BP =blood pressure; h= hour(s);HTN= hypertension; pts= patients; T2DM= type 2 diabetes mellitus; wk =week(s). * p< 0.0001 vs BL.
Efficacy of Olmesartan-Based Therapy in High-Risk Patients 381
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)
-12.6/-7.7mmHg overall and -11.4/-7.1mmHg in obese
patients.
BeniSILVER
The Benicar Efficacy: New Investigation Shows Olmesartan
Medoxomil Treatment Increasingly Leads Various Elderly
Populations to Safe BP Reductions (BeniSILVER) study
(ClinicalTrials.gov identifier: NCT00412932) treated 176 elder-
ly hypertensive patients (aged ‡65 years) with olmesartan me-
doxomil –HCTZ, and uptitrated in a step-wise manner to
achieve BP goals of <120/70mmHg (table I). Patients were
stratified by race and hypertension severity (table III).[35,47,48]
At week 12, changes from baseline in 24-hour mean ABP
were -25.7/-12.3mmHg overall, -26.7/-11.8mmHg in Black
patients, and -26.5/-12.6mmHg in the stage 2 hypertension
subgroup (table III). ABP was significantly reduced from
baseline in the daytime and night-time intervals and in the last
hours of the dosing interval. Changes from baseline in mean
daytime and night-time ABP were similar across patient sub-
groups (table III), and similar significant changes in ABP
during the last hours of the dosing interval were also achieved.
During the last 6 hours, mean changes were -24.1/-11.6mmHg
overall, and -25.6/-11.4 and -24.6/-11.6mmHg in Black
patients and patients with stage 2 hypertension, respectively.
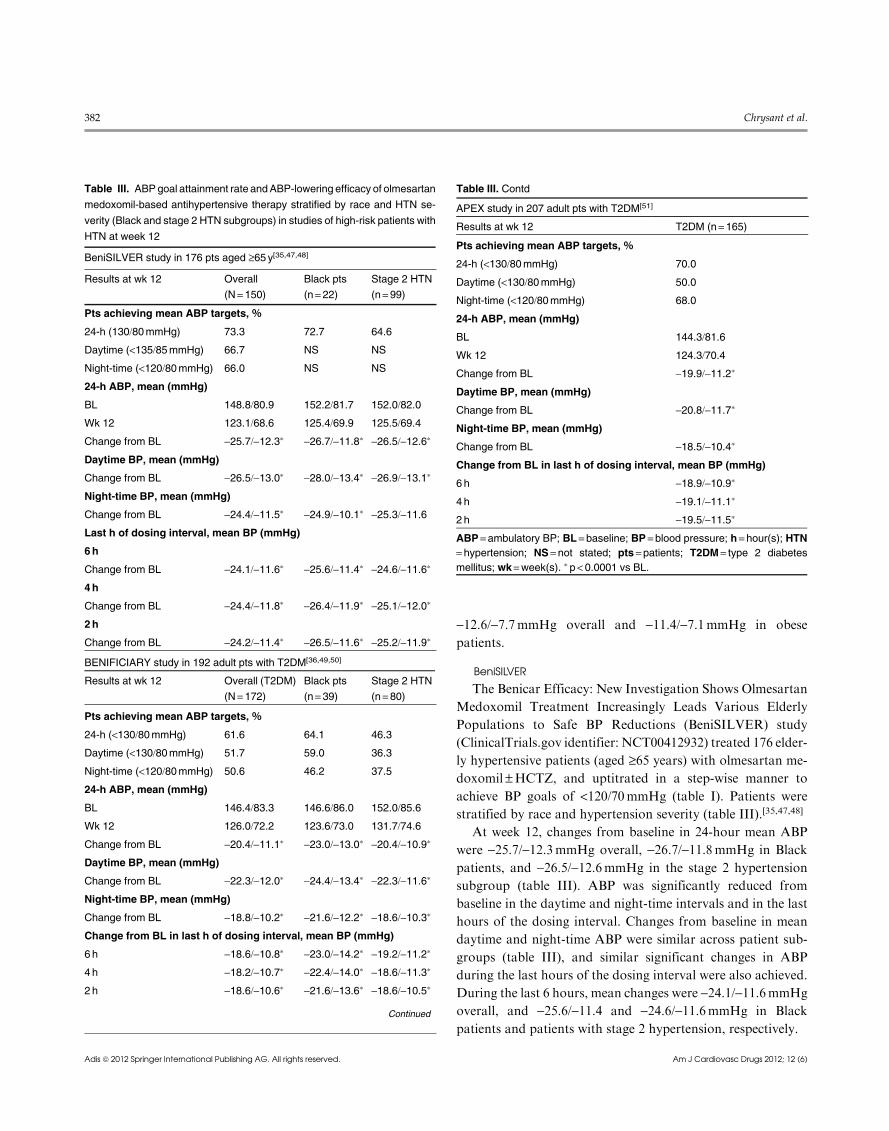
Table III. ABPgoal attainment rate andABP-lowering efficacy of olmesartan
medoxomil-based antihypertensive therapy stratified by race and HTN se-
verity (Black and stage 2 HTN subgroups) in studies of high-risk patients with
HTN at week 12
BeniSILVER study in 176 pts aged ‡65 y[35,47,48]
Results at wk 12 Overall
(N= 150)Black pts
(n= 22)Stage 2 HTN
(n= 99)
Pts achieving mean ABP targets, %
24-h (130/80mmHg) 73.3 72.7 64.6
Daytime (<135/85mmHg) 66.7 NS NS
Night-time (<120/80mmHg) 66.0 NS NS
24-h ABP, mean (mmHg)
BL 148.8/80.9 152.2/81.7 152.0/82.0
Wk 12 123.1/68.6 125.4/69.9 125.5/69.4
Change from BL -25.7/-12.3* -26.7/-11.8* -26.5/-12.6*
Daytime BP, mean (mmHg)
Change from BL -26.5/-13.0* -28.0/-13.4* -26.9/-13.1*
Night-time BP, mean (mmHg)
Change from BL -24.4/-11.5* -24.9/-10.1* -25.3/-11.6
Last h of dosing interval, mean BP (mmHg)
6h
Change from BL -24.1/-11.6* -25.6/-11.4* -24.6/-11.6*
4h
Change from BL -24.4/-11.8* -26.4/-11.9* -25.1/-12.0*
2h
Change from BL -24.2/-11.4* -26.5/-11.6* -25.2/-11.9*
BENIFICIARY study in 192 adult pts with T2DM[36,49,50]
Results at wk 12 Overall (T2DM)
(N= 172)Black pts
(n= 39)Stage 2 HTN
(n= 80)
Pts achieving mean ABP targets, %
24-h (<130/80mmHg) 61.6 64.1 46.3
Daytime (<130/80mmHg) 51.7 59.0 36.3
Night-time (<120/80mmHg) 50.6 46.2 37.5
24-h ABP, mean (mmHg)
BL 146.4/83.3 146.6/86.0 152.0/85.6
Wk 12 126.0/72.2 123.6/73.0 131.7/74.6
Change from BL -20.4/-11.1* -23.0/-13.0* -20.4/-10.9*
Daytime BP, mean (mmHg)
Change from BL -22.3/-12.0* -24.4/-13.4* -22.3/-11.6*
Night-time BP, mean (mmHg)
Change from BL -18.8/-10.2* -21.6/-12.2* -18.6/-10.3*
Change from BL in last h of dosing interval, mean BP (mmHg)
6 h -18.6/-10.8* -23.0/-14.2* -19.2/-11.2*
4 h -18.2/-10.7* -22.4/-14.0* -18.6/-11.3*
2 h -18.6/-10.6* -21.6/-13.6* -18.6/-10.5*
Continued
APEX study in 207 adult pts with T2DM[51]
Results at wk 12 T2DM (n= 165)
Pts achieving mean ABP targets, %
24-h (<130/80mmHg) 70.0
Daytime (<130/80mmHg) 50.0
Night-time (<120/80mmHg) 68.0
24-h ABP, mean (mmHg)
BL 144.3/81.6
Wk 12 124.3/70.4
Change from BL -19.9/-11.2*
Daytime BP, mean (mmHg)
Change from BL -20.8/-11.7*
Night-time BP, mean (mmHg)
Change from BL -18.5/-10.4*
Change from BL in last h of dosing interval, mean BP (mmHg)
6 h -18.9/-10.9*
4 h -19.1/-11.1*
2 h -19.5/-11.5*
ABP= ambulatory BP; BL= baseline; BP = blood pressure; h= hour(s); HTN= hypertension; NS = not stated; pts =patients; T2DM= type 2 diabetes
mellitus; wk =week(s). * p < 0.0001 vs BL.
Table III. Contd
382 Chrysant et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)

In BeniSILVER, 36.4% of Black patients were non-dippers
and 63.6%were dippers at baseline, while at the end of the study
37.5% of the non-dippers became dippers. For non-Black
patients, 31.3% were non-dippers at baseline and 68.8% were
dippers, with 52.5% of the non-dippers becoming dippers after
12 weeks of treatment.[47]
BENIFICIARY
In the Benicar Safety and Efficacy Evaluation (BENIFI-
CIARY) study (ClinicalTrials.gov identifier: NCT00403481),
192 patients with T2DM and hypertension were treated with
olmesartan medoxomil –HCTZ, titrated to achieve a BP
goal of <120/70mmHg (table I). Patients were stratified by race
and hypertension severity (table III).[36,49,50] At week 12, the
changes from baseline in 24-hour mean ABP for the total,
Black, and stage 2 hypertension cohorts were -20.4/-11.1,-23.0/-13.0, and -20.4/-10.9mmHg, respectively (table III).
There were statistically significant daytime and night-time ABP
reductions from baseline overall, in Black patients, and in
patients who entered the study with stage 1 or 2 hypertension.
ABP changes from baseline during the last hours of the
dosing interval were similar in the overall study population and
in patients with stage 2 hypertension (table III). However,
changes in ABP during the final hours of the dosing periodwere
numerically greater in Black patients than in other patient
groups. During the last 6 hours, mean ABP changes were
-18.6/-10.8mmHg overall, -19.2/-11.2 in patients with stage 2
hypertension, and -23.0/-14.2mmHg in Black patients.
At baseline in the BENIFICIARY study, 44.8% of patients
overall, 56.4% of Black patients, and 47.5% of patients with
stage 2 hypertension were non-dippers. After 12 weeks of treat-
ment, 36.4% of all non-dippers at baseline had converted to
dippers, as had 31.8% of Black non-dippers and 31.6% of
patients with stage 2 hypertension who were non-dippers at
baseline.[49]
APEX
APEX was A Prospective, open-label, ABPM study (Clin-
icalTrials.gov identifier: NCT00654745) to evaluate the safety
and Efficacy of an olmesartan medoXomil- and amlodipine-
based treatment titration regimen in patients with T2DM and
hypertension (table I). In this study, 207 patients with T2DM
and hypertension were treated with amlodipine/olmesartan
medoxomil –HCTZ to achieve a BP goal of <120/70mmHg
(table III).[51]
At 12 weeks, the change from baseline in 24-hour mean ABP
was -19.9/-11.2mmHg, and ABP was significantly reduced in
the daytime, night-time, and last hours of the dosing interval
(table III). During the last 6 hours of the dosing interval, mean
ABP changes were -18.9/-10.9mmHg.
2.1.2 Impact of Time of Administration
The impact of morning versus night-time dosing on ABP
lowering with olmesartan medoxomil monotherapy was
studied in patients with T2DM and hypertension (table I).
The results are presented in table IV.[52] Significant changes
from baseline in 24-hour, daytime, and night-time mean ABP
were achieved regardless of the time of dosing. For 24-hour
mean ABP, there was a change of -13.7/-8.6mmHg with
morning dosing and -14.4/-10.1mmHg with night-time dosing
(table IV). However, although there was no statistically sig-
nificant difference between dosing regimens in daytime mean
ABP, night-time administration of olmesartan medoxomil
produced a significantly larger decrease in night-time mean
ambulatory SBP (-16.2 vs -11.9mmHg) compared with morn-
ing administration.
At baseline, 68% of patients were dippers; morning admin-
istration of olmesartan medoxomil increased the proportion of
dipper patients to 74%, while 82% of patients had dipper status
with nocturnal administration (p = 0.012).[52]
2.1.3OlmesartanMedoxomil versusComparator Antihypertensives
Only one study was found that treated patients with olme-
sartan medoxomil-based therapy versus an active comparator
Table IV. Effects on ABP of morning vs evening dosing of olmesartan
medoxomil in patients with T2DM at week 8
Study in 38 hypertensive patients with T2DM[52]
Results after 8wk Morning dose
(n= 38)Night-time dose
(n= 38)
24-h ABP, mean (mmHg)
BL 138.5/87.5 138.5/87.5
Wk 8 124.8/78.9* 124.1/77.4*
Change from BL -13.7/-8.6 -14.4/-10.1
Daytime BP, mean (mmHg)
BL 142.2/89.5 142.2/89.6
Wk 8 128.7/81.4* 129.5/81.1*
Change from BL -13.5/-8.1 -12.7/-8.5
Night-time BP, mean (mmHg)
BL 124.3/80.8 124.3/80.8
Wk 8 112.4/74.0* 108.1-/71.0*--
Change from BL -11.9/-6.8 -16.2/-9.8
ABP= ambulatory BP; BL =baseline; BP =blood pressure; h = hour(s);T2DM= type 2 diabetes mellitus; wk=week(s). * p <0.0001 vs BL;
- p =0.007 vs morning dose; -- p = 0.069 vs morning dose.
Efficacy of Olmesartan-Based Therapy in High-Risk Patients 383
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)
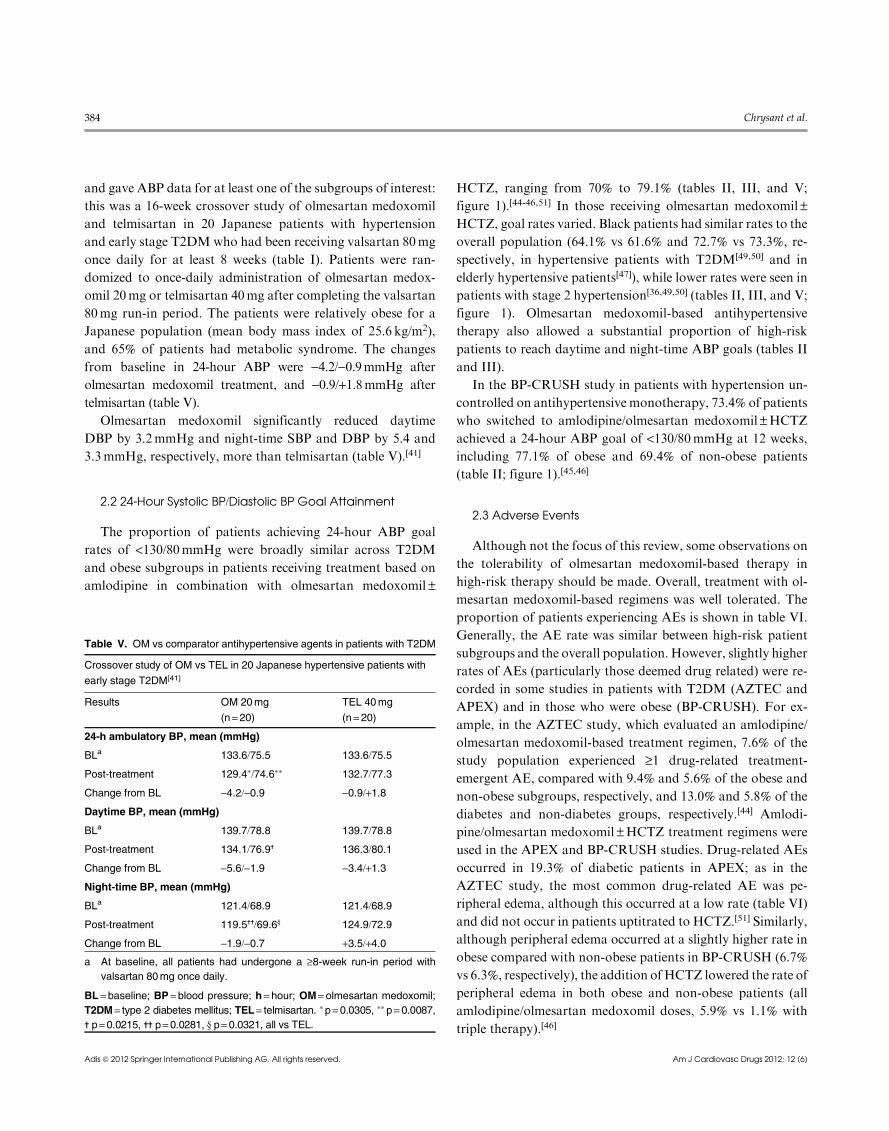
and gave ABP data for at least one of the subgroups of interest:
this was a 16-week crossover study of olmesartan medoxomil
and telmisartan in 20 Japanese patients with hypertension
and early stage T2DMwho had been receiving valsartan 80mg
once daily for at least 8 weeks (table I). Patients were ran-
domized to once-daily administration of olmesartan medox-
omil 20mg or telmisartan 40mg after completing the valsartan
80mg run-in period. The patients were relatively obese for a
Japanese population (mean body mass index of 25.6 kg/m2),
and 65% of patients had metabolic syndrome. The changes
from baseline in 24-hour ABP were -4.2/-0.9mmHg after
olmesartan medoxomil treatment, and -0.9/+1.8mmHg after
telmisartan (table V).
Olmesartan medoxomil significantly reduced daytime
DBP by 3.2mmHg and night-time SBP and DBP by 5.4 and
3.3mmHg, respectively, more than telmisartan (table V).[41]
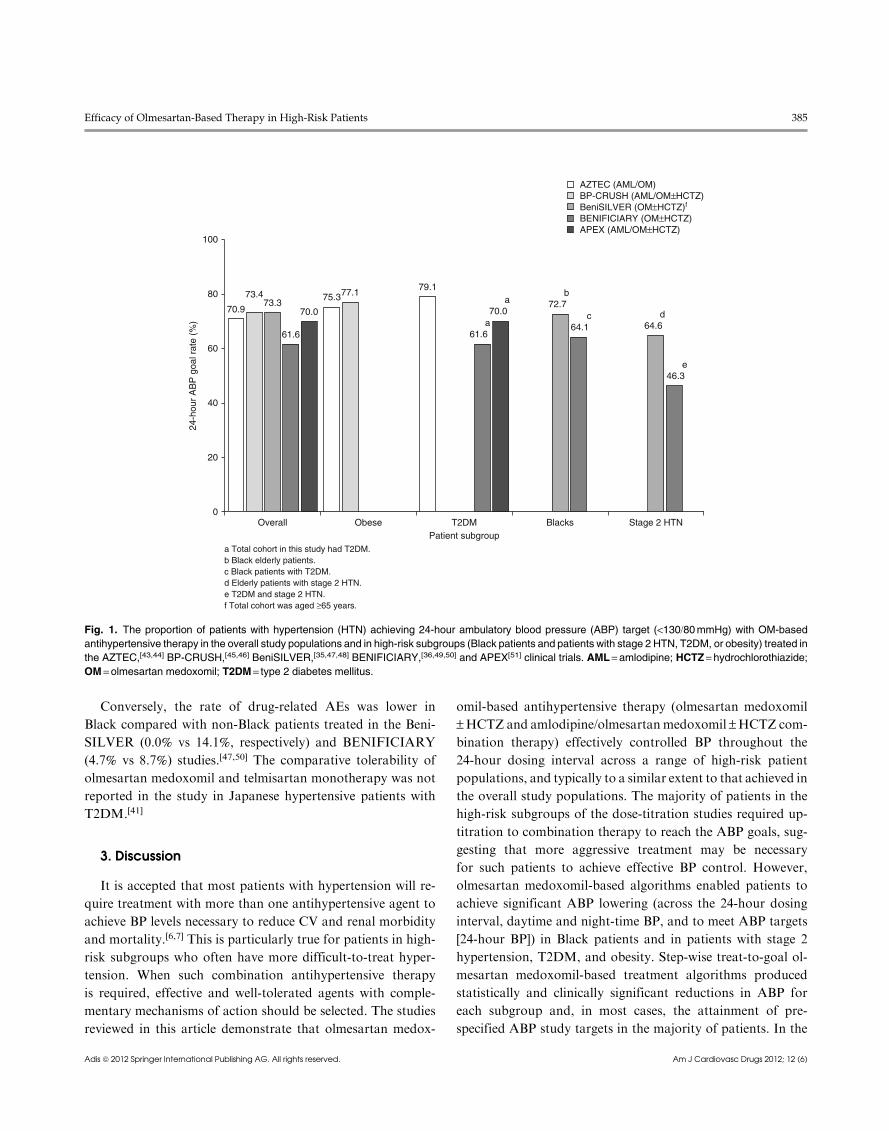
2.2 24-Hour Systolic BP/Diastolic BP Goal Attainment
The proportion of patients achieving 24-hour ABP goal
rates of <130/80mmHg were broadly similar across T2DM
and obese subgroups in patients receiving treatment based on
amlodipine in combination with olmesartan medoxomil –
HCTZ, ranging from 70% to 79.1% (tables II, III, and V;
figure 1).[44-46,51] In those receiving olmesartan medoxomil –HCTZ, goal rates varied. Black patients had similar rates to the
overall population (64.1% vs 61.6% and 72.7% vs 73.3%, re-
spectively, in hypertensive patients with T2DM[49,50] and in
elderly hypertensive patients[47]), while lower rates were seen in
patients with stage 2 hypertension[36,49,50] (tables II, III, and V;
figure 1). Olmesartan medoxomil-based antihypertensive
therapy also allowed a substantial proportion of high-risk
patients to reach daytime and night-time ABP goals (tables II
and III).
In the BP-CRUSH study in patients with hypertension un-
controlled on antihypertensive monotherapy, 73.4% of patients
who switched to amlodipine/olmesartan medoxomil –HCTZ
achieved a 24-hour ABP goal of <130/80mmHg at 12 weeks,
including 77.1% of obese and 69.4% of non-obese patients
(table II; figure 1).[45,46]
2.3 Adverse Events
Although not the focus of this review, some observations on
the tolerability of olmesartan medoxomil-based therapy in
high-risk therapy should be made. Overall, treatment with ol-
mesartan medoxomil-based regimens was well tolerated. The
proportion of patients experiencing AEs is shown in table VI.
Generally, the AE rate was similar between high-risk patient
subgroups and the overall population. However, slightly higher
rates of AEs (particularly those deemed drug related) were re-
corded in some studies in patients with T2DM (AZTEC and
APEX) and in those who were obese (BP-CRUSH). For ex-
ample, in the AZTEC study, which evaluated an amlodipine/olmesartan medoxomil-based treatment regimen, 7.6% of the
study population experienced ‡1 drug-related treatment-
emergent AE, compared with 9.4% and 5.6% of the obese and
non-obese subgroups, respectively, and 13.0% and 5.8% of the
diabetes and non-diabetes groups, respectively.[44] Amlodi-
pine/olmesartan medoxomil –HCTZ treatment regimens were
used in the APEX and BP-CRUSH studies. Drug-related AEs
occurred in 19.3% of diabetic patients in APEX; as in the
AZTEC study, the most common drug-related AE was pe-
ripheral edema, although this occurred at a low rate (table VI)
and did not occur in patients uptitrated to HCTZ.[51] Similarly,
although peripheral edema occurred at a slightly higher rate in
obese compared with non-obese patients in BP-CRUSH (6.7%vs 6.3%, respectively), the addition ofHCTZ lowered the rate of
peripheral edema in both obese and non-obese patients (all
amlodipine/olmesartan medoxomil doses, 5.9% vs 1.1% with
triple therapy).[46]
Table V. OM vs comparator antihypertensive agents in patients with T2DM
Crossover study of OM vs TEL in 20 Japanese hypertensive patients with
early stage T2DM[41]
Results OM 20mg
(n= 20)TEL 40mg
(n = 20)
24-h ambulatory BP, mean (mmHg)
BLa 133.6/75.5 133.6/75.5
Post-treatment 129.4*/74.6** 132.7/77.3
Change from BL -4.2/-0.9 -0.9/+1.8
Daytime BP, mean (mmHg)
BLa 139.7/78.8 139.7/78.8
Post-treatment 134.1/76.9- 136.3/80.1
Change from BL -5.6/-1.9 -3.4/+1.3
Night-time BP, mean (mmHg)
BLa 121.4/68.9 121.4/68.9
Post-treatment 119.5--/69.6y 124.9/72.9
Change from BL -1.9/-0.7 +3.5/+4.0
a At baseline, all patients had undergone a ‡8-week run-in period with
valsartan 80mg once daily.
BL= baseline; BP = blood pressure; h= hour; OM= olmesartan medoxomil;
T2DM= type 2 diabetes mellitus; TEL= telmisartan. *p=0.0305, **p= 0.0087,- p= 0.0215, -- p= 0.0281, y p= 0.0321, all vs TEL.
384 Chrysant et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)
Conversely, the rate of drug-related AEs was lower in
Black compared with non-Black patients treated in the Beni-
SILVER (0.0% vs 14.1%, respectively) and BENIFICIARY
(4.7% vs 8.7%) studies.[47,50] The comparative tolerability of
olmesartan medoxomil and telmisartan monotherapy was not
reported in the study in Japanese hypertensive patients with
T2DM.[41]
3. Discussion
It is accepted that most patients with hypertension will re-
quire treatment with more than one antihypertensive agent to
achieve BP levels necessary to reduce CV and renal morbidity
and mortality.[6,7] This is particularly true for patients in high-
risk subgroups who often have more difficult-to-treat hyper-
tension. When such combination antihypertensive therapy
is required, effective and well-tolerated agents with comple-
mentary mechanisms of action should be selected. The studies
reviewed in this article demonstrate that olmesartan medox-
omil-based antihypertensive therapy (olmesartan medoxomil
–HCTZ and amlodipine/olmesartanmedoxomil –HCTZ com-
bination therapy) effectively controlled BP throughout the
24-hour dosing interval across a range of high-risk patient
populations, and typically to a similar extent to that achieved in
the overall study populations. The majority of patients in the
high-risk subgroups of the dose-titration studies required up-
titration to combination therapy to reach the ABP goals, sug-
gesting that more aggressive treatment may be necessary
for such patients to achieve effective BP control. However,
olmesartan medoxomil-based algorithms enabled patients to
achieve significant ABP lowering (across the 24-hour dosing
interval, daytime and night-time BP, and to meet ABP targets
[24-hour BP]) in Black patients and in patients with stage 2
hypertension, T2DM, and obesity. Step-wise treat-to-goal ol-
mesartan medoxomil-based treatment algorithms produced
statistically and clinically significant reductions in ABP for
each subgroup and, in most cases, the attainment of pre-
specified ABP study targets in the majority of patients. In the
100
70.9
73.473.3
61.6
70.0
Overall Obese T2DM Blacks Stage 2 HTNPatient subgroup
a Total cohort in this study had T2DM.b Black elderly patients.c Black patients with T2DM.d Elderly patients with stage 2 HTN.e T2DM and stage 2 HTN. f Total cohort was aged ≥65 years.
75.377.179.1
a61.6
a70.0
b72.7
c64.1
d64.6
e46.3
24-h
our
AB
P g
oal r
ate
(%)
80
60
40
20
0
AZTEC (AML/OM)BP-CRUSH (AML/OM±HCTZ)BeniSILVER (OM±HCTZ)f
BENIFICIARY (OM±HCTZ)APEX (AML/OM±HCTZ)
Fig. 1. The proportion of patients with hypertension (HTN) achieving 24-hour ambulatory blood pressure (ABP) target (<130/80mmHg) with OM-based
antihypertensive therapy in the overall study populations and in high-risk subgroups (Black patients and patients with stage 2 HTN, T2DM, or obesity) treated in
the AZTEC,[43,44] BP-CRUSH,[45,46] BeniSILVER,[35,47,48] BENIFICIARY,[36,49,50] and APEX[51] clinical trials. AML= amlodipine; HCTZ= hydrochlorothiazide;OM=olmesartan medoxomil; T2DM= type 2 diabetes mellitus.
Efficacy of Olmesartan-Based Therapy in High-Risk Patients 385
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)

BP-CRUSH study, this was also achieved in high-risk pa-
tients previously uncontrolled on antihypertensive mono-
therapy.[45,46]
Furthermore, BP reductions persisted during the critical last
6, 4, and 2 hours of the dosing interval, which corresponds with
the morning BP surge, indicating that olmesartan medoxomil-
based therapy provided antihypertensive effect throughout the
full dosing interval in high-risk populations.
In the BENIFICIARY study in patients with T2DM, ABP
goal rates achieved with olmesartan medoxomil –HCTZ ther-
apy in patients with stage 2 hypertension were 46.3%, compared
with 64.1% in Black patients and 61.6% in the overall patient
population with T2DM.[36,49,50] This suggests that T2DM in
conjunction with more severe hypertension is a condition that
may particularly benefit from amore intensive antihypertensive
strategy. The use of a more intensive olmesartan medoxomil-
based strategy (amlodipine/olmesartan medoxomil –HCTZ)
achieved better goal rates in the T2DM population in the
APEX study (in which a greater proportion of patients with
T2DM achieved the prespecified ABP targets of <130/80mmHg than patients without T2DM)[51] than in patients with
T2DM in the BENIFICIARY study who received olmesartan
medoxomil –HCTZ.[49,50] This suggests that the lower goal
achievement rate in patients with stage 2 hypertension and
T2DM in the BENIFICIARY study may possibly be increased
with the use of amlodipine/olmesartan medoxomil –HCTZ.
However, there are differences in study design, patients, and
treatments, so no extrapolation can be drawn from such an
indirect comparison. This requires further investigation in a
randomized controlled trial.
One limitation of this analysis is that the studies identified
were all of relatively short duration (8–12 weeks of active
treatment), which does not allow conclusions to be made on
long-term efficacy in these patient subgroups. Nevertheless, the
long-term efficacy of the component antihypertensive agents
has been established in a number of studies.[53-57] A second
limitation is that, although nocturnal BP has been shown to be
a predictor of CV outcomes, the use of ABPM to determine
dipping patterns must be interpreted with caution as dipping
patterns can demonstrate variability and patients may spon-
taneously shift from a non-dipping pattern to a dipping pattern
and vice versa. Thirdly, all of the titrate-to-goal studies were of
an open-label design, and patient outcomes were not analyzed
to determine the statistical significance of differences between
subgroups. In addition, a few studies had a relatively small
number of patients in some subgroups. However, the studies
provide a reflection of real-world clinical practice where struc-
tured dose titration is recommended to achieve and maintain
Table VI. Proportion of patients experiencing AEs in ABPM studies of
olmesartan medoxomil-based antihypertensive therapy
Study TEAE Drug-
related
AEs
Drug-related AEs
occurring in ‡2%of pts
Discontinuations
due to TEAE
BeniSILVER study in 176 pts aged ‡65 y[35,47,48]
Overall 32.6 11.8 Dizziness: 3.4
Hypotension: 2.2
5.1
Black pts 31.0 0.0 Dizziness: 0.0
Hypotension: 0.0
3.4
Non-Black pts 32.9 14.1 Dizziness: 4.0
Hypotension: 2.7
5.4
Stage 2 disease 32.8 12.1 Dizziness: 2.6
Hypotension: 2.6
NS
Isolated systolic
HTN
32.7 15.3 Dizziness: 4.1
Hypotension: 2.3
Headache: 2.0
Nausea: 2.0
NS
BENIFICIARY study in 192 pts with T2DM[36,50]
Overall 34.9 7.8 NS NS
Black pts 39.5 4.7 NS NS
Non-Black pts 33.6 8.7 NS NS
Stage 2 disease 33.0 5.5 NS NS
AZTEC study in 185 pts with HTN[43,44]
Overall 31.4 7.6 Peripheral
edema: 2.2
1.6
Obese pts 34.4 9.4 Peripheral
edema: 4.2
1.0
T2DM 45.7 13.0 Peripheral
edema: 2.2
Dizziness: 2.2
2.2
APEX study in 207 pts with HTN and T2DM[51]
Overall 57.0 19.0 Peripheral
edema: 6.0
Dizziness: 3.0
Hypotension: 2.0
6.0
BP-CRUSH study in 999 pts with uncontrolled HTN[45,46]
Overall 53.0 25.5 Dizziness: 7.6
Peripheral
edema: 6.5
Hypotension: 2.3
Headache: 2.0
Fatigue: 2.0
8.6
Obese pts 53.9 26.1 Peripheral
edema: 6.7
Dizziness: 5.1
Hypotension: 2.4
Headache: 2.4
7.7
ABPM= ambulatory blood pressure monitoring; AE= adverse event; HTN=hypertension; NS = not stated; pts= patients; TEAE= treatment-emergent
AE; T2DM= type 2 diabetes mellitus; y= years.
386 Chrysant et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)

BP control, an approach especially relevant in high-risk
patients who may have difficult-to-treat hypertension. Apart
from the small study by Nakayama et al., which compared
olmesartanmedoxomil and telmisartanmonotherapy in Japanese
patients with T2DM,[41] no ABP studies directly comparing
olmesartanmedoxomil-based and other ARB-based antihyper-
tensive regimens were identified. Furthermore, it is beyond the
scope of this article to review the ABP efficacy in high-risk
patient subgroups of antihypertensive therapy based on other
ARBs.
4. Conclusion
A titrate-to-BP goal strategy using olmesartan medoxomil-
or amlodipine/olmesartan medoxomil-based antihypertensive
therapy has been shown to be an effective approach in man-
aging hypertension throughout the full 24-hour dosing period
in difficult-to-treat high-risk patients, including Blacks,
obese patients, patients with T2DM, and those with stage 2
hypertension. The reductions in ABP and achievement of
ABP targets may potentially translate into improvements in
the overall CV risk profile. The good tolerability of olmesartan
medoxomil, amlodipine, and HCTZ as components of
combination antihypertensive regimens may also potentially
lead to improvements in patient compliance during long-term
therapy.
Acknowledgments
This study was supported by Daiichi Sankyo, Inc. Manuscript prepa-
ration, editing, andmedical writing support were provided byRayHill and
Alan J. Klopp, PhD, of inScience Communications, Springer Healthcare,
and funded by Daiichi Sankyo, Inc.
Steven G. Chrysant, MD, has received research grants from Daiichi
Sankyo, Inc., Novartis, Boehringer Ingelheim, Merck, Bristol-Myers
Squibb, and Takeda Pharmaceuticals and serves as a consultant for
Daiichi Sankyo, Inc., Novartis, and Boehringer Ingelheim.
F. Wilford Germino, MD, has received research grants from Daiichi
Sankyo, Inc., Novartis, and Sanofi and honoraria from Bristol-Myers
Squibb, AstraZeneca, Forest Laboratories, Takeda, and Pfizer Inc.
Joel Neutel, MD, is a member of the speaker’s bureau for Novartis,
Boehringer Ingelheim, Daiichi Sankyo, Inc., the Bristol-Myers Squibb/Sanofi Pharmaceutical Partnership, Takeda, and Pfizer Inc.
References1. Rosendorff C, Black HR, Cannon CP, et al. Treatment of hypertension in the
prevention and management of ischemic heart disease: a scientific statement
from the American Heart Association Council for High Blood Pressure
Research and the Councils on Clinical Cardiology and Epidemiology and
Prevention. Circulation 2007 May 29; 115 (21): 2761-88
2. Vasan RS, Larson MG, Leip EP, et al. Impact of high-normal blood pressure
on the risk of cardiovascular disease. N Engl J Med 2001 Nov 1; 345 (18):
1291-7
3. Lewington S, Clarke R, Qizilbash N, et al. Age-specific relevance of usual
blood pressure to vascular mortality: a meta-analysis of individual data for
one million adults in 61 prospective studies. Lancet 2002 Dec 14; 360 (9349):
1903-13
4. Kearney PM, Whelton M, Reynolds K, et al. Global burden of hypertension:
analysis of worldwide data. Lancet 2005 Jan 15-21; 365 (9455): 217-23
5. Egan BM, Zhao Y, Axon RN. US trends in prevalence, awareness, treat-
ment, and control of hypertension, 1988–2008. JAMA 2010May 26; 303 (20):
2043-50
6. Chobanian AV, Bakris GL, Black HR, et al. The Seventh Report of the Joint
National Committee on Prevention, Detection, Evaluation, and Treatment
of High Blood Pressure: the JNC 7 report. JAMA 2003 May 21; 289 (19):
2560-72
7. Mancia G, De Backer G, Dominiczak A, et al. 2007 ESH-ESC Practice
Guidelines for the Management of Arterial Hypertension: ESH-ESC Task
Force on the Management of Arterial Hypertension. J Hypertens 2007 Sep;
25 (9): 1751-62
8. Mancia G, Laurent S, Agabiti-Rosei E, et al. Reappraisal of European
guidelines on hypertensionmanagement: a European Society ofHypertension
Task Force document. J Hypertens 2009 Nov; 27 (11): 2121-58
9. American Diabetes Association. Standards of medical care in diabetes – 2012.
Diabetes Care 2012 Jan; 35 Suppl 1: S11-63
10. Handelsman Y, Mechanick JI, Blonde L, et al. American Association of
Clinical Endocrinologists Medical Guidelines for Clinical Practice for de-
veloping a diabetes mellitus comprehensive care plan. Endocr Pract 2011
Mar-Apr; 17 Suppl 2: 1-53
11. Flack JM, Sica DA, Bakris G, et al. Management of high blood pressure in
Blacks: an update of the International Society on Hypertension in Blacks
consensus statement. Hypertension 2010 Nov; 56 (5): 780-800
12. Douglas JG, Bakris GL, Epstein M, et al. Management of high blood pressure
in African Americans: consensus statement of the Hypertension in African
Americans Working Group of the International Society on Hypertension in
Blacks. Arch Intern Med 2003 Mar 10; 163 (5): 525-41
13. Arauz-Pacheco C, Parrott MA, Raskin P. The treatment of hypertension in
adult patients with diabetes. Diabetes Care 2002 Jan; 25 (1): 134-47
14. Pessina AC. Target organs of individuals with diabetes caught between arterial
stiffness and damage to the microcirculation. J Hypertens Suppl 2007 Jun;
25 (1): S13-8
15. American Diabetes Association. Standards of medical care in diabetes – 2009.
Diabetes Care 2009 Jan; 32 Suppl 1: S13-61
16. Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke sta-
tistics – 2009 update: a report from the American Heart Association Statistics
Committee and Stroke Statistics Subcommittee. Circulation 2009 Jan 27;
119 (3): e21-181
17. Rosamond W, Flegal K, Furie K, et al. Heart disease and stroke statistics –
2008 update: a report from the American Heart Association Statistics Com-
mittee and Stroke Statistics Subcommittee. Circulation 2008 Jan 29; 117 (4):
e25-146
18. National Institute for Health and Clinical Excellence. Hypertension: the
clinical management of primary hypertension in adults. Clinical Guideline
127, Methods, evidence, and recommendations, August 2011: National In-
stitute for Health and Clinical Excellence (NICE); 2011 [online]. Available
from http://www.nice.org.uk/nicemedia/live/13561/56007/56007.pdf [Accessed
2011 Dec 14]
19. Pickering TG, White WB. ASH position paper: when and how to use self
(home) and ambulatory blood pressuremonitoring. J AmSocHypertens 2008
May-Jun; 2 (3): 119-24
20. Frohlich ED. Blood pressure measurement. Can J Cardiol 1995 Nov; 11 Suppl.
H: 35H-7H
Efficacy of Olmesartan-Based Therapy in High-Risk Patients 387
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)

21. Clement DL, De Buyzere ML, De Bacquer DA, et al. Prognostic value of
ambulatory blood-pressure recordings in patients with treated hypertension.
N Engl J Med 2003 Jun 12; 348 (24): 2407-15
22. Pickering TG, Hall JE, Appel LJ, et al. Recommendations for blood pressure
measurement in humans and experimental animals. Part 1: blood pressure
measurement in humans. A statement for professionals from the Sub-
committee of Professional and Public Education of the American Heart As-
sociation Council on High Blood Pressure Research. Circulation 2005 Feb 8;
111 (5): 697-716
23. Verdecchia P. Prognostic value of ambulatory blood pressure: current evidence
and clinical implications. Hypertension 2000 Mar; 35 (3): 844-51
24. Burr ML, Dolan E, O’Brien EW, et al. The value of ambulatory blood
pressure in older adults: the Dublin outcome study. Age Ageing 2008 Mar;
37 (2): 201-6
25. White WB. Cardiovascular risk and therapeutic intervention for the early
morning surge in blood pressure and heart rate. Blood PressMonit 2001 Apr;
6 (2): 63-72
26. Gosse P, Lasserre R, Minifie C, et al. Blood pressure surge on rising. J Hy-
pertens 2004 Jun; 22 (6): 1113-8
27. Muller JE, Tofler GH, Stone PH. Circadian variation and triggers of onset of
acute cardiovascular disease. Circulation 1989 Apr; 79 (4): 733-43
28. Pickering TG,KarioK.Nocturnal non-dipping: what does it augur? Curr Opin
Nephrol Hypertens 2001 Sep; 10 (5): 611-6
29. Routledge F, McFetridge-Durdle J. Nondipping blood pressure patterns
among individuals with essential hypertension: a review of the literature. Eur J
Cardiovasc Nurs 2007 Mar; 6 (1): 9-26
30. O’Brien E, Asmar R, Beilin L, et al. Practice guidelines of the European Society
of Hypertension for clinic, ambulatory and self blood pressure measurement.
J Hypertens 2005 Apr; 23 (4): 697-701
31. Pickering TG, Shimbo D, Haas D. Ambulatory blood-pressure monitoring.
N Engl J Med 2006 Jun 1; 354 (22): 2368-74
32. Lovibond K, Jowett S, Barton P, et al. Cost-effectiveness of options for the
diagnosis of high blood pressure in primary care: a modelling study. Lancet
2011 Oct 1; 378 (9798): 1219-30
33. Kjeldsen SE, Os I, Hoieggen A, et al. Fixed-dose combinations in the
management of hypertension: defining the place of angiotensin receptor
antagonists and hydrochlorothiazide. Am J Cardiovasc Drugs 2005; 5 (1):
17-22
34. Chrysant SG, Izzo JL Jr, Kereiakes DJ, et al. Efficacy and safety of
triple-combination therapy with olmesartan, amlodipine, and hydrochloro-
thiazide in study participants with hypertension and diabetes: a sub-
population analysis of the TRINITY study. J Am Soc Hypertens 2012 Mar-
Apr; 6 (2): 132-41
35. Kereiakes DJ, Neutel J, Stoakes KA, et al. The effects of an olmesartan me-
doxomil-based treatment algorithm on 24-hour blood pressure levels in eld-
erly patients aged 65 and older. J Clin Hypertens (Greenwich) 2009 Aug;
11 (8): 411-21
36. Neutel JM, Kereiakes DJ, Waverczak WF, et al. Effects of an olmesartan
medoxomil based treatment algorithm on 24-hour blood pressure control in
patients with hypertension and type 2 diabetes. CurrMedResOpin 2010Mar;
26 (3): 721-8
37. Fogari R, Taddei S, Holm-Bentzen M, et al. Efficacy and safety of olmesartan
medoxomil 40mg/hydrochlorothiazide 12.5mg combination therapy versus
olmesartan medoxomil 40mg monotherapy in patients with moderate to se-
vere hypertension: a randomized, double-blind, parallel-group, multicentre,
multinational, phase III study. Clin Drug Investig 2010; 30 (9): 581-97
38. Izzo Jr JL, Neutel JM, Silfani T, et al. Efficacy and safety of treating stage 2
systolic hypertension with olmesartan and olmesartan/HCTZ: results
of an open-label titration study. J Clin Hypertens (Greenwich) 2007 Jan; 9 (1):
36-44
39. Oparil S, Pimenta E. Efficacy of an olmesartan medoxomil-based treatment
algorithm in patients stratified by age, race, or sex. J Clin Hypertens
(Greenwich) 2010 Jan; 12 (1): 3-13
40. Kereiakes DJ, Chrysant SG, Izzo Jr JL, et al. Long-term efficacy and safety of
triple-combination therapy with olmesartan medoxomil and amlodipine be-
sylate and hydrochlorothiazide for hypertension. J Clin Hypertens 2012Mar;
14 (3): 149-57
41. Nakayama S, Watada H, Mita T, et al. Comparison of effects of olmesartan
and telmisartan on blood pressure and metabolic parameters in Japanese
early-stage type-2 diabetics with hypertension. Hypertens Res 2008 Jan;
31 (1): 7-13
42. WhiteWB,WeberMA, SicaD, et al. Effects of the angiotensin receptor blocker
azilsartan medoxomil versus olmesartan and valsartan on ambulatory and
clinic blood pressure in patients with stages 1 and 2 hypertension. Hyper-
tension 2011 Mar; 57 (3): 413-20
43. Punzi H, Neutel JM, Kereiakes DJ, et al. Efficacy of amlodipine and olme-
sartan medoxomil in patients with hypertension: the AZOR Trial Evaluating
Blood Pressure Reductions and Control (AZTEC) study. Ther Adv Cardio-
vasc Dis 2010 Aug; 4 (4): 209-21
44. Punzi H, Shojaee A, Waverczak WF, et al. Efficacy of amlodipine and olme-
sartan medoxomil in hypertensive patients with diabetes and obesity. J Clin
Hypertens (Greenwich) 2011 Jun; 13 (6): 422-30
45. Weir MR, Hsueh WA, Nesbitt SD, et al. A titrate-to-goal study of switching
patients uncontrolled on antihypertensive monotherapy to fixed-dose com-
binations of amlodipine and olmesartan medoxomil +/- hydrochlorothiazide.J Clin Hypertens (Greenwich) 2011 Jun; 13 (6): 404-12
46. Hsueh WA, Shojaee A, Maa J-F, et al. Efficacy of amlodipine/olmesartan
medoxomil –HCTZ in obese patients uncontrolled on antihypertensive
monotherapy. Curr Med Res Opin. Epub. DOI: 10.1185/03007995.
2012.740632
47. Neutel J, Kereiakes DJ, Stoakes KA, et al. Blood pressure-lowering efficacy of
an olmesartan medoxomil/hydrochlorothiazide-based treatment algorithm in
elderly patients (age >/=65 years) stratified by age, sex and race: subgroup
analysis of a 12-week, open-label, single-arm, dose-titration study. Drugs
Aging 2011 Jun 1; 28 (6): 477-90
48. Germino FW, Neutel JM, Dubiel R, et al. Efficacy of olmesartan medoxomil
and hydrochlorothiazide fixed-dose combination therapy in patients aged 65
years and older with stage 1 and 2 hypertension or isolated systolic hyper-
tension. Am J Cardiovasc Drugs 2012 Oct; 12 (5): 325-33
49. Kereiakes DJ, Neutel J. Efficacy of an olmesartan medoxomil-based treat-
ment algorithm in patients with hypertension and type 2 diabetes: anal-
ysis of diurnal blood pressure control as assessed by 24-hour ambulatory
blood pressure monitoring. Ther Adv Cardiovasc Dis 2010 Oct; 4 (5):
285-93
50. Neutel JM, Kereiakes DJ. An olmesartan medoxomil-based treatment algo-
rithm is effective in achieving 24-hour BP control in patients with type 2
diabetes mellitus, regardless of age, race, sex, or severity of hypertension:
subgroup analysis of the BENIFICIARY study. Am J Cardiovasc Drugs
2010; 10 (5): 289-303
51. Ram CV, Sachson R, Littlejohn T, et al. Management of hypertension in pa-
tients with diabetes using an amlodipine-, olmesartan medoxomil-, and hy-
drochlorothiazide-based titration regimen. Am JCardiol 2011May 1; 107 (9):
1346-52
52. Tofe Povedano S, Garcia De LaVilla B. 24-hour and nighttime blood pressures
in type 2 diabetic hypertensive patients following morning or evening ad-
ministration of olmesartan. J Clin Hypertens (Greenwich) 2009 Aug; 11 (8):
426-31
53. VolpeM,Miele C, HaagU. Efficacy and safety of a stepped-care regimen using
olmesartan medoxomil, amlodipine and hydrochlorothiazide in patients with
moderate-to-severe hypertension: an open-label, long-term study. Clin Drug
Investig 2009; 29 (6): 381-91
388 Chrysant et al.
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)

54. Chrysant SG, Oparil S, MelinoM, et al. Efficacy and safety of long-term treatment
with the combinationof amlodipinebesylate andolmesartanmedoxomil inpatients
with hypertension. J Clin Hypertens (Greenwich) 2009 Sep; 11 (9): 475-82
55. Ichikawa S, Takayama Y. Long-term effects of olmesartan, an Ang II receptor
antagonist, on blood pressure and the renin-angiotensin-aldosterone system
in hypertensive patients. Hypertens Res 2001 Nov; 24 (6): 641-6
56. Oparil S, Chrysant SG, Melino M, et al. Long-term efficacy of a combination
of amlodipine and olmesartan medoxomil +/- hydrochlorothiazide in patients
with hypertension stratified by age, race and diabetes status: a substudy of the
COACH trial. J Hum Hypertens 2010 Dec; 24 (12): 831-8
57. Kereiakes DJ, Izzo J, Chrysant S, et al. The long-term safety and tolerability of
combination olmesartanmedoxomil/amlodipine besylate+hydrochlorothiazide inpatients with hypertension: the TRINITY study [abstract]. 23rd Scientific
Meeting of the International Society of Hypertension (ISH); 26 Sep 2010;
Vancouver; 2010; A1994
Correspondence: Dr Steven G. Chrysant, Director, Oklahoma Cardiovascular
and Hypertension Center, 5850 West Wilshire Blvd, Oklahoma City,
OK 73132, USA. E-mail: [email protected]
Efficacy of Olmesartan-Based Therapy in High-Risk Patients 389
Adis ª 2012 Springer International Publishing AG. All rights reserved. Am J Cardiovasc Drugs 2012; 12 (6)