Embed Size (px)
Citation preview

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 1/27
The Brachial plexus

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 2/27
The Brachial plexus

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 3/27
The Brachial plexus
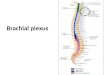
1. The brachial plexus is formedby the union of the anterior rami of C5-C8 & T1 (the rootsof the BP).
2. The roots pass laterallybetween the anterior andmiddle scalene muscles withthe subclavian artery.
3. Sympathetic fibers from themiddle and inferior cervical
ganglia join the roots as theypass between the scalenes.
Fig 6.29 p 775

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 4/27
In the supraclavicular area the roots unite to form trunks:1. Superior trunk ± C5& C62. Middle trunk ± C7 continues
3. Inferior trunk ± C8 & T1
Fig 6.28 p 774

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 5/27
As the trunks pass lateral to the 1st rib each trunk splits into anterior and posterior divisions as they pass beneath the clavicle and enter the cervicoaxillary canal: ± Anterior divisions innervate the muscles of the anterior compartment in
the arm and forearm.
± Posterior divisions innervate muscles of the posterior compartment of the arm and forearm
Fig 6.28 p 774

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 6/27
Divisions form cords in the area superior to the pectoral minor: ± Superior & middle anterior divisions unite the from the lateral cord
± Inferior division of the inferior trunk forms the medial cord
± Posterior divisions unite to form the posterior cord.
Fig 2.08 p 21 Grant¶s Dissector 13th Ed., PatrickTank

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 7/27
To simplify understanding and remembering the BP incan be divided into supraclavicular & infraclavicular segments by the clavicle
Fig 6.28 p 774

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 8/27
Supraclavicular branchesThere are four, they arise from roots, a trunk and a division*Root branches Dorasl scapular nerve:pierces middle scalene and passes
inferiorly to the rhomboids Long thoracic nerve: from C5,6,7 roots passes inferiorly on to the
surface of the Serratus anterior
Trunk branch Nerve to subclavius: passes directly to the inferior surface of
clavicle gives branch to sternoclavicular jointDivision branch Suprascapular nerve: runs parallel to the suprascapular artery to
the suprascapular notch (beneath the suprascapular ligament)
supplies the supraspinatus m. around the greater scapular notch tothe infraspinatus m.*Small braches arise from all roots to supply the scalene and longus
coli muscles. C5 gives a root to the Phrenic nerve (C3-5)

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 9/27
Supraclavicular branches
Fig 6.29 p 775

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 10/27
Infraclavicular Branches - -arise from the cords and can be
divided into branches and little branches (very unscientific).
Fig 6.28 p 774

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 11/27
Infraclavicular Branches
Cords BIG branches little
Lateral MusculocutaneousLateral
Lateral pectoral
Posterior Axillary
Radial
Upper Subscapular
Lower Subscapular Thoracodorsal
Medial Ulnar
Medial
Medial pectoral
Medial brachial cutaneous
Medial ante brachial cutaneous
The lateral & medial braches join to form theMedian nerve

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 12/27
Cords Big Branches Little Branches
Lateral Musculocutaneous
Lateral branch
Lateral pectoral
Fig 6.31 p 785

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 13/27
Cords Big Branches Little branchesPosterior Axillary
Radial
Upper subscapular
Lower subscapular
Thoracodorsal
Fig 2.09 p 21, Grant¶s Dissector 13th Ed., Patrick Tank

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 14/27
Cords Big branches Little branches
Medial Ulnar
Medial branch
Medial pectoral
Medial brachial cutaneous
Medial antebrachial cutaneous
Fig. 6.31, p 785

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 15/27
Figure 206.1.² Schematic representation of the brachial plexus nerves and muscles. (PS): paraspinal muscles; (R): rhomboid muscle; DS: dorsoscapular nerve; LT: long thoracic nerve: (SA): serratus anterior muscle; SF:
sympathetic fibers for the eye; (M of M) muscle of Muller: (DP) dilator of the pupil; (SS): supraspinatus muscle; (IS): infraspinatus muscle; SPS:suprascapular nerve; PL: pectoralis lateralis nerves; (P): pectoralis muscle;PM: pectoralis medialis nerve; (TM): teres major muscle; (SBS): subscapularismuscle; SBS: subscapularis nerve; TD: thoracodorsal nerve; (LD): latissimusdorsi muscle; MC: musculocutaneous nerve; (Bi): biceps muscle; (Br):brachialis muscle; M: median nerve; U: ulnar nerve; A: axillary nerve; (TMi):teres minor muscle; (D): deltoid muscle; R: radial nerve.

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 16/27
Brachial Plexus Root Injuries
Upper brachial plexus injury
± Erb-Duchenne Palsy C5&C6 root injury, caused by stretch between the head and
shoulder, shoulder stops head/neck don¶t. The most commonly involved nerves are the suprascapular
nerve, musculocutaneous nerve, and the axillary nerve.
Waiter¶s tip deformity- arm adducted, medially rotated andpronated. Why?
Sensory loss where? Major cause is obstetric injury ($$$$$$$$)

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 17/27
Figure 216.1.² Typical posture of a neonate with Duchenne-Erb palsy [A and B]. The posture consists of arm adduction and internal rotation, extended elbow, forearm pronation, palmar flexion of the wrist, and good finger movements. The presence of wrist flexion indicates minimal or noinvolvement of C7
.

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 18/27
Figure 216.2.² Schematic representation of the brachial plexus and itsnerves and muscles. Site of injury. A: C5 root and C6 spinal nerve; B: upper trunk; (PS): paraspinal muscles; (R): rhomboid muscle; DS: dorsoscapular
nerve; LT: long thoracic nerve; (SA): serratus anterior muscle; (SS):supraspinal muscle; (IS): infraspinal muscle; SPS: suprascapular nerve; PL: pectoral lateralis nerve; (P): pectoralis muscle; PM: pectoralis medialis nerve;SF: sympathetic fibers to the eyes; (M of M): muscle of Müller; (DP): dilator pupillary muscle; (TM): teres major muscle; (SBS): subscapularis muscle;SBS: subscapularis nerves; TD: thoracodorsal nerve; (LD): latissimus dorsi muscle; MC: musculocutaneous nerve; (Bi): biceps muscle; (Br): brachialismuscle; M: median nerve; U: ulnar nerve; A: axillary nerve; (TMi): teres minor
muscle; (D): deltoid muscle; R: radial nerve.

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 19/27
Brachial Plexus Injuries
Lower brachial plexus injury
± Klumpke palsy
C7,C8&T1 injury
Arm abduction injury
Paralysis of the muscles of the distal forearm andhand (all ulnar innervated) plus distal radial &median innervated muscles.
Horner's syndrome (ptosis,meiosis, anhydrosis) if T1 sympathetics involved.

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 20/27
Figure 220.2.² Site of injury in Klumpke palsy. [A] Root of T1 and spinal nerve of C8. [B] Lower trunk. The green lines at T1 represent the most frequent origin of sympathetic fibers for the eyes. (PS): paraspinal muscles; (R): rhomboid muscle; DS: dorsoscapular nerve; LT: long thoracic nerve; (SA): serratus anterior muscle; (SS): supraspinal muscle; (IS): infraspinal muscle; SPS: suprascapular nerve; PL: pectoral lateralis nerve; (P): pectoralis muscle; PM:
pectoralis medialis nerve; SF: sympathetic fibers to the eyes; (M of M): muscle of Müller; (DP):dilator pupillary muscle; (TM): teres major muscle; (SBS): subscapularis muscle; SBS:subscapularis nerves; TD: thoracodorsal nerve; (LD): latissimus dorsi muscle; MC:musculocutaneous nerve; (Bi): biceps muscle; (Br): brachialis muscle; M: median nerve; U:ulnar nerve; A: axillary nerve; (TMi): teres minor muscle; (D): deltoid muscle; R: radial nerve.

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 21/27
Brachial Plexus Injuries
Lower brachial plexus injury
± Klumpke palsy
C7,C8&T1 injury
Arm abduction injury
Paralysis of the muscles of the distal forearm andhand (all ulnar innervated) plus distal radial &median innervated muscles.
Horner's syndrome (ptosis,meiosis, anhydrosis) if T1 sympathetics involved.

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 22/27

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 23/27
Brachial Plexus Variations
Brachial Plexus Variations in Human Fetuses.ANATOMIC REPORTS
Neurosurgery. 53(3):676-684, September 2003.Uysal, Ismihan Ilknur M.D.; Seker, Muzaffer Ph.D.;
Karabulut, Ahmet Kagan M.D., Ph.D.; Buyukmumcu,Mustafa Ph.D.; Ziylan, Taner Ph.D.
This study was performed with 200 BPs fromspontaneously aborted fetuses without detectablemalformations. The BPs were composed mostly of theC5, C6, C7, and C8 nerves and the T1 nerve (71.5%). A
prefixed plexus was observed in 25.5% of cases, and apostfixed plexus was observed in 2.5% of cases.
Another study BPs noted phrenic nerve formation byC5,6&7 in 20% of specimens***

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 24/27
BP Anomalies

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 25/27

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 26/27
Brachial Plexus
Really cool procedure, do the same in lab!

8/8/2019 Old Brachial
http://slidepdf.com/reader/full/old-brachial 27/27
End